Embed Size (px)
Citation preview

2012/03/28
1
Mechanism of HIV drug resistance .Rodrigo Brindeiro / Amilcar Tanuri
Laboratório de Virologia MolecularUFRJ
2-Asso ciate Research Scientist, In ternatio nal Center fo r Aids Care and Treatment Programs-ICAP, Mailman Scho ol of Public Health, Co lumbia Univ ersity, NY, USA.
Sic Transit Gloria Mundi.Ad Majorem Dei GloriamIn Hoc Signo Vinces.
HIV virus and infected CD4+ T cells
Nobel 2008
HPVHIV
Harald zur HausenFrançoise Barré-SinoussiLuc Montagnier
Ciclo replicativo do HIV
Fusion Inhibitors
CCR5 Inhibitors
NRTI and NNRTI Inhibitors
Integrase Inhibitors
Protease Inhibitors
HIV life cycle and Classes of ARV Available
25 drugs approved to treat HIV/AIDS
Hunt R at all 2002 Microbiol & Immun
Mortality Rate Tendency Related to Aids Brazil, 1990-1999.
R 2 = 0,8156Year
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
90 91 92 93 94 95 96 97 98 99
(x 1
00
.00
0h
ab
.)
2012/03/28
2
Nucleoside/Nucleotide AnaloguesAbacavir (Ziagen, ABC)Didanosine (Videx, ddI)Emtricitabine (Emtriva, FTC)Lamivudine (Epivir, 3TC)Stavudine (Zerit, d4T)Tenofovir (Viread, TDF)Zalcitabine (Hivid, ddC) Discontinued by manufacturer 12/31/06Zidovudine (Retrovir, AZT, ZDV)
Nonnucleoside Reverse Transcriptase InhibitorsDelavirdine (Rescriptor, DLV)Efavirenz (Sustiva, Stocrin, EFV)Etravirine (Intelence, TMC 125)Nevirapine (Viramune, NVP)Rilpivirine (Edurant, TMC 278)
Protease InhibitorsAmprenavir (Agenerase, APV) Discontinued by manufacturer 10/07Atazanavir (Reyataz, ATV)Darunavir (Prezista, DRV, TMC 114)Fosamprenavir (Lexiva, Telzir, FPV)Indinavir (Crixivan, IDV)Lopinavir/Ritonavir (Kaletra)Nelfinavir (Viracept, NFV)Ritonavir (Norvir, RTV)Saquinavir (Invirase, SQV)Tipranavir (Aptivus, TPV)
Fusion InhibitorsEnfuvirtide (Fuzeon, ENF, T-20)
Chemokine Coreceptor AntagonistsMaraviroc (Selzentry, Celsentri, MVC)
Integrase InhibitorsRaltegravir (Isentress, RAL)
List of ARV FDA Approved
HIV Genetic Diversity
• HIV displays large genetic variability and two viruses can be causative agent of AIDS (HIV-1 and HIV-2). RT has no proofreading mechanisms and poses a mutations rate of 1 error per 10000 nt synthesized.
• Every day in a infected individual we have a huge replication burden (1010 particles daily) and all kind mutations appears. Most of them are lost and few are fixed in the viral population.
• HIV-2 can differ from HIV-1 in 50% of the aa of the main genes (gag, pol, and env).
• HIV-2 is less pathogenic and less transmissible by horizontal and vertical routes.
HIV quasispecies
Why HIV get resistant to ARV?
• Low aderance to treatment.• On-and-off ARV therapy.• Infection with a isolate carrying DRM.
The main message here is: “ HIV needs to replicate to accumulate mutations.” The best way to prevent DR is keeping the VL undetectable during ARV treatment .
The drug does not produce or induce DR it just select pre-existing mutant viruses
WT
MUT
2012/03/28
3
3TC
Days in culture7 14 21 28 35 42 49 56 63 70 77 84 91 98
HIV
vira
l loa
d
105
106
107
108
109
1010
1011
RT CRT B
0.02 0.04 0.08 0.16 0.32 0.64 1.2 2.4 4.8 9.6 19.2 38.4 76.8 3TC concentrations (µM)
M184IM184I
3TC
Days in culture7 14 21 28 35 42 49 56 63 70 77 84 91 98
HIV
vira
l loa
d
105
106
107
108
109
1010
1011
RT CRT B
0.02 0.04 0.08 0.16 0.32 0.64 1.2 2.4 4.8 9.6 19.2 38.4 76.8 3TC concentrations (µM)
3TC
Days in culture7 14 21 28 35 42 49 56 63 70 77 84 91 98
HIV
vira
l loa
d
105
106
107
108
109
1010
1011
RT CRT B
0.02 0.04 0.08 0.16 0.32 0.64 1.2 2.4 4.8 9.6 19.2 38.4 76.8 3TC concentrations (µM)
M184IM184I
In vitro selection B and C virus with 3TC .
M184VM184V
M184VVM184VV
Types of HIV Resistance
• Primary or transmitted drug resistance: Drug resistance in previously untreated persons. Primary drug resistance implies that a virus with drug resistance mutations was transmitted either directly, or through one or more intermediates, from a person with acquired drug resistance. In the first case, ‘primary’ is used to describe persons who have recently been infected. In the second case, ‘primary’ is used to describe persons with transmitted resistance.
Types of HIV Resistance
• Acquired or secondary drug resistance: Drug resistance developing in a person who has received antiretroviral therapy. Acquired drug resistance results from the generation of genetic variation in the population of viruses within a person followed by the selection of drug-resistant variants during HAART therapy.
Types of HIV Resistance
• Polymorphism: Polymorphisms are mutations occurring frequently in viruses not exposed to selective drug pressure. A nonpolymorphicmutation is one that does rarely occur in the absence of therapy.
How ARV drugs work?NRTI
2012/03/28
4
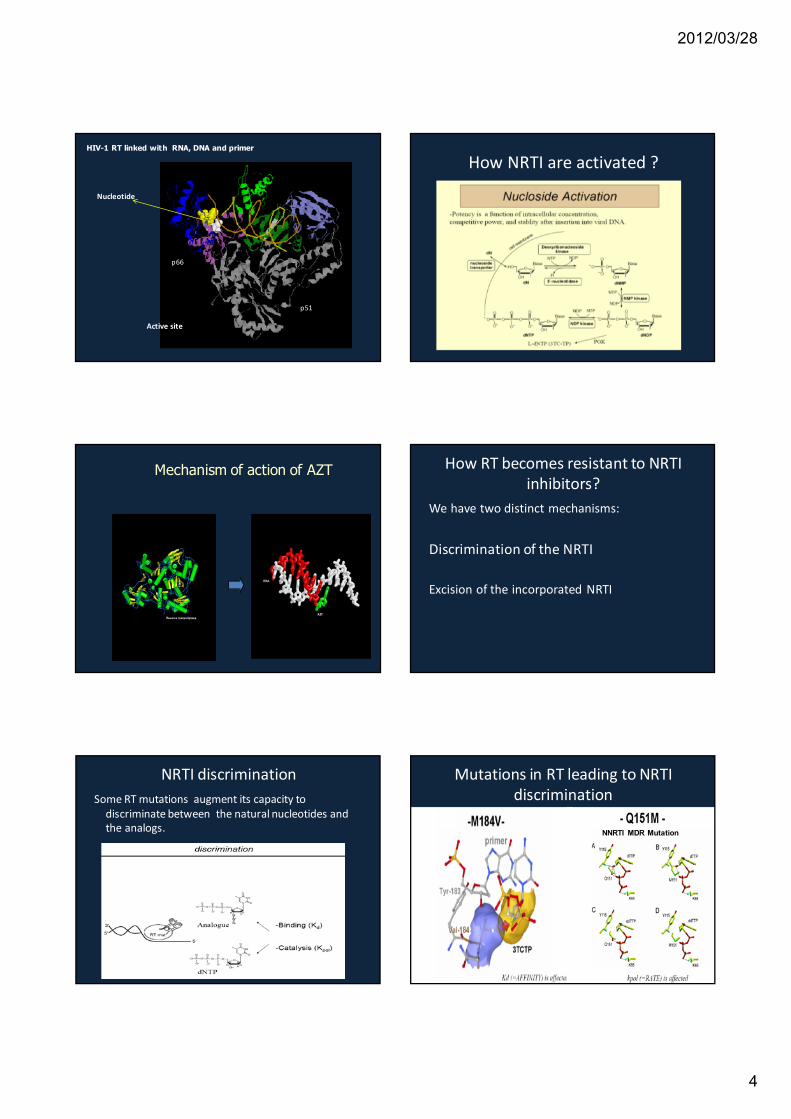
HIV-1 RT linked with RNA, DNA and primer
p51
p66
Active site
Nucleotide
How NRTI are activated ?
Mechanism of action of AZT How RT becomes resistant to NRTI inhibitors?
We have two distinct mechanisms:
Discrimination of the NRTI
Excision of the incorporated NRTI
NRTI discriminationSome RT mutations augment its capacity to
discriminate between the natural nucleotides and the analogs.
Mutations in RT leading to NRTI discrimination
NNRTI MDR Mutation

2012/03/28
5
Other multidrug resistant mutations in RT
Two or more amino acid insertion S-A, S-S or S-G at HIV-1 RT codon 69(S) in conjunction with other RT mutations are associated with phenotypic resistance to multiple NRTIs
T69 Pos
TAM mutations
• Resistance to zidovudine (ZDV) results from thymidine analogue resistance mutations (TAMs) at HIV-1 reverse transcriptase (RT) codons 41, 67, 70, 210, 215 and 219. Two mutations are possible at codon 215: Y or F. Whereas 215Y occurs alone or with 41L and 210W (TAM-1), 215F rarely occurs with these mutations or by itself; it is usually found with 67N, 70R and 219Q (TAM-2). The 210W mutation most often occurs with 41L and 215Y and rarely occurs with 215F or TAM-2 mutations. We previously demonstrated that the 215F mutant is less fit than T215 wild-type or 215Y (Hu et al., Antiviral Therapy 2004; 9:S68). In the present study, we explored the virological basis for clustering of 210W with other TAM-1 but not TAM-2 mutants, and the clustering of 215F, but not 215Y, with TAM-2 mutants.
What is excision?What is pyrophosphorolisis?
How NRTI excision mechanism works?
For isolates carrying TAM
How TAM works in excision mechanism ? Nucleotide inhibitor (Tenofovir,
Gilead)• Tenofovir was approved by FDA in 2001.
This modif ication enables TDF to jump the 1st phosphorylation step making a favorable PK profile .

2012/03/28
6
Main TDF Resistance Mutation
Does K65R accumulatemore often in subtype C?
NRTI mutation list
NNRTI
NNRTI NNRTI mechanism of action.HIV-1 RT Linked with Nevirapine (NNRTI)
Active site
Nevirapine
HIV-1 RT linked with Nevirapine with mutations related with NNRTI mutations
Active sites
Nevirapine
NNRTI DR Mutations
Entravirine and its capability to inhibit NNRTI resistant strains specifically K103N
In Brazil The prevalence of 13 specific ETR RAMs in subtype B samples was V179T 2%, G190S 3.7%, Y181V 0,5%, V106I 6%, V179D 2.6%, K101P 3.0%, K101E 5.3%, Y181C 12%, A98G 6.9%, V90I 6.9%,Y181I 3.6%, G190A 15% and L100I 6.1%.

2012/03/28
7
NNRTI mutation list HIV GAG Maturation process
How protease inhibitors work
Protease inhibitor
HIV ProteaseMajor Mutations Positions 30, 32, 33, 46, 48, 50,
54, 76, 82, 84, 88, 90
HIV Drug Resistance Database, Los Alamos National Laboratoryhttp://resdb.lanl.gov/Resist_DB
Sampling of Minor PI Mutations commonly present in non-B isolates as natural polymorphism
Mutations Positions 20, 36, 63, 71, 77, 93

2012/03/28
8
New PIs
Atazanavir Tipranavir Darunavir
DRV interacts with more aa in protease active site
Ritonavir enhances the blood levels of
other protease inhibitors
Kempf, et al, 1997
With ritonavirWithout ritonavir
(mg
/ml)
.01
.1
1
10
0 1 2 3 4 5 6 7 8Hours
S
NelfinavirAmprenavirIndinaviraquinavir
.01
.1
10
1
0 1 2 3 4 5 6 7 8
Hours
(mg
/ml)
Genetic Barrier
NRTI PI RTV/PI
Genotipic Res
How a MDR protease looks like
PI mutation list New classes of ARV drugs

2012/03/28
9
Integrase inhibitors
Mutations N155H, alone and combinations withQ148K/H/R and Y143R/C/H
Maraviroc
Fuseon – T20
Final Remarks • The best way to prevent the spread of HIV DR is to
prevent HIV infection.• The best other way to prevent the spread of HIV DR is
to keep the patients in ARV with undetectable VL.• In RLS the VL is not available in large scale.• 2nd line potent regimens are not available in RLS.• We need to make an effort to implement VL and
make available potent 2nd line regimens to curb the spread of HIV DR.





























