Embed Size (px)
Citation preview

Chronic Pain: an overview of mechanisms and management
Dr Helen CohenConsultant Rheumatology & Chronic Pain
Royal National Orthopaedic Hospital

∗ How pain works∗ Pain mechanisms∗ Guidelines∗ Pharmacologic treatment∗ Interventional treatment∗ Pain management & rehabilitation
Overview

∗ Multiple types of pain∗ Evolutionary survival system

∗ Primary afferent small myelinated A-δ and unmyelinated C-fibre nociceptors
∗ Transmit impulses to the dorsal horn of the spinal cord. ∗ A- δ terminate primarily on neurones in laminas I, V and X ∗ C-fibres terminate in laminas I – V (mainly I and II).∗ C-fibres transmit to spinal second order interneurones
∗ wide dynamic range (WDR) respond to pain & touch∗ nociceptive specific neurones
Nociception

Nociceptive impulses ascend by two main pathways:
∗ The more modern neospinothalamic anterolateral system∗ A-delta fibres∗ Pain & non-painful temperature∗ connects to spinothalamic tracts; pass to the lateral thalamus ∗ connections to the sensory cortex allowing the localisation of pain ∗ Discriminative pain – quality, intensity, location; ‘fast pain’
∗ The primitive spino-reticulo-diencephalic tract in the posterolateral cord∗ c-fibres∗ connects to reticular system of the brainstem ∗ other connections to the thalamus and hypothalamus∗ Affective/arousal/emotional aspects of pain; ‘slow pain’∗ Sympathetic outflow connections
Ascending tracts

Descending control
∗ Periaqueductral gray-rostral ventromedial medulla (PAG-RVM) system ∗ Dorsal reticular nucleus (DRt) and ventrolateral medulla (VLM). ∗ Nucleus raphe magnus (NRM) and locus coeruleus in the pons
∗ These systems can be inhibitory or facilitatory∗ Deficits of descending inhibition may be operating in
some chronic pain syndromes eg. fibromyalgia∗ Many different neurotransmitters
∗ Serotonin∗ Noradrenaline

Nociceptive neurotransmission∗ Primary afferent neurones:
∗ Glutamate∗ Other excitatory neuropeptides include calcitonin gene related peptide
(cGRP) and substance P (SP), & many more∗ Glutamate binds to NMDA and AMPA receptors∗ GABA-ergic inhibitory neurones throughout spinal cord
∗ also activated by glycine∗ Opiate receptors∗ Nociceptive ion channels TRVP1, NaV1.7 – expressed in DRG
and nociceptive cells∗ Nerve growth factor – activation & sensitization of
nociceptors∗ Cannabinoid receptors – CB1, CB2∗ Endocannabinoids – inc. anadamide; degraded by FAA(fatty
acid amide hydrolase)

Central Processing∗ Chronic pain as a network dysfunction∗ No single ‘pain centre’
∗ Many brain areas can be activated including: thalamus, reticular system, hypothalamus, periaqueductal grey, S1, S2 and cingulate cortex
∗ Thalamic connections to many cortical areas including limbic and anterior cingulate mediate the affective/emotional aspects of pain.
∗ Autonomic connections

Nociceptors∗ reduction in threshold ∗ increase in responsiveness∗ Previously ‘silent’ c-fibres become active
∗ Nociceptor & ion channel modulation; changes in gene expression
Peripheral sensitisation

∗ Central sensitization is an increase in the excitability of neurons within the central nervous system, so that normal inputs begin to produce abnormal responses.
∗ WDR spinal neurones: ∗ increased excitability, ∗ decreased thresholds, ∗ widened receptive field
∗ Neuronal synaptic plasticity∗ Enhanced presynaptic neurotransmitter release, recruitment of
post synaptic NMDA receptors; changes in microglia, astrocytes, gap junctions, membrane excitability and gene transcription
Central sensitisation

‘Centralised’ pain
Central Sensitization in Chronic Pain
Pain itself can change how pain works, resulting in more pain with less provocation


Neuroplasticity∗ The process in which the brain's neural synapses and
pathways are altered as an effect of environmental, behavioral, and neural changes
∗ Can be observed at multiple scales, from microscopic changes in individual neurons to larger-scale changes such as cortical remapping
∗ Maladaptive neuroplasticity in chronic pain conditions eg. phantom limb pain, CRPS
Kuner R, Flor H. Structural plasticity and reorganisation in chronic pain. Nat Rev Neurosci. 2016 Dec 15;18(1):20-30.
Kumbhare DA, Elzibak AH, Noseworthy MD. Evaluation of Chronic Pain Using Magnetic Resonance (MR) Neuroimaging Approaches: What the Clinician Needs to Know. Clin J Pain. 2017 Apr;33(4):281-290.

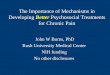
Cortical Representation
Somatotopic maps S1,S2, & beyond

Cortical remapping following hand amputation and 5 months post transplantation.
Face or hand, not both: perceptual correlates of reafferentation in a former amputee
∗ Article in Current Biology 12(15):1342-6 · September 2002
Farnè A1, Roy AC, Giraux P, Dubernard JM, Sirigu A.

Changes in cortical reorganisation in PLP after training in sensory discrimination
Pre-training. Representation of the mouth invades the hand area
Post training. Representation of the mouth moves to a more inferior lateral position
Hand Mouth
Flor H; The Lancet Neurology 2002
Neuromagnetic source imaging

Pain & geneticsPain plus syndromes∗ Gain of function: SCN9/Na1.7 channel
∗ Primary erythromelalgia∗ Paroxsysmal extreme pain disorder
∗ Familial hemiplegic migraine – loss & gain mutations in different genes
Congenital Insensitivity to Pain syndromes∗ SCN9 mutation / Nav1.7 channelopathy∗ FAA-OUT – mutation impairing FAA – increased
endocannabinoidsOther∗ COMT (Catechol-O-methyltransferase) – catecholamines have
a role in pain processing/perception; COMT degrades dopamine, nor-adrenaline and adrenaline – effect on pain & modulation of opioidergic activity
∗ OPRM1 (mu opioid receptor) – impaired opioid response

∗ Pain is both a sensationAnd
∗ A perception
∗ This can dramatically change behavioural and emotional responses to pain

Psychological factors
∗ Increased anxiety and depression∗ Also attention deficit (and hyperactivity) disorder, autism
spectrum disorders, obsessive-compulsive disorder, personality disorder, anorexia, self harm, PTSD, previous abuse
∗ Catastrophisation∗ Psychological stress makes pain worse & vice-versa

Guidelines for management of chronic pain
Scottish Intercollegiate Guidelines Network
U.S. Department of Health and Human Services
https://www.sign.ac.uk/assets/sign136_2019.pdf
Evidence based recs
Task force reviewGaps & recs
U.S. Department of Health and Human Services (2019, May). Pain Management Best Practices Inter-Agency Task ForceReport: Updates, Gaps, Inconsistencies, and Recommendations. Retrieved from U. S. Department of Health and HumanServices website: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html

Guidelines Neuropathic Pain
∗ International Association for the Study of Pain∗ Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and
meta-analysis. Lancet Neurol. 2015;14:162–73.∗ Haanpaa M, Attal N, Backonja M, et al. NeuPSIG guidelines on neuropathic pain assessment. Pain. 2011;152:14–27.
∗ European Federation of Neurological Societies (EFNS) ∗ Attal N, Cruccu G, Baron R, et al. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision.
Eur J Neurol.2010;17:1113.∗ Cruccu G, Sommer C, Anand P, et al. EFNS guidelines on neuropathic pain assessment: revised 2009. Eur J Neurol.
2010;17:1010–8.
∗ National Institute for Health and CareExcellence∗ National Institute for Health and Care Excellence (NICE). Neuropathic pain: the pharmacological management of
neuropathic pain in adults innon-specialist settings. 2013.
∗ Canadian Pain Society (CPS) ∗ Moulin D, Boulanger A, Clark AJ, et al. Pharmacological management of chronic neuropathic pain: revised consensus
statement from the Canadian Pain Society. Pain Res Manag. 2014;19:328–35.
Fibromyalgia: European League Against Rheumatism (EULAR) 2008; revised 2016
American Pain Society (APS) 2005 German (Association of the Scientific Medical Societies, AWMF) 2012 Israeli
Canadian Pain Society (CPS) 2013

Controversies and challenges in fibromyalgia: a review and a proposal.Cohen H. Ther Adv Musculoskelet Dis. 2017 May;9(5):115-127. doi: 10.1177/1759720X17699199. Epub 2017 Mar 26. Review.
Interventional Rx
Chronic pain

Why don’t drugs seem to work?
Causes of chronic painIt is suggested that:
• Multiple mechanisms involving various regions of entire neuraxis
• Pathophysiology may vary from one patient to another

Drug treatment∗ NSAIDs – inflammatory pain∗ Neuromodulatory medication
∗ Tricyclic antidepressants eg. amitriptyline – increase serotonin +/-noradrenaline,
∗ Gabapentin, pregabalin – increase GABA ∗ SNRI eg. Duloxetine – increase S, NA
∗ Ketamine, memantine – affect NMDA receptor∗ Opioids∗ Capsaicin – TRVP1∗ Anti-nerve growth factor Ab biologic drugs (tanezumab)∗ Cannabis & derivatives?
∗ BIA 10-2474 - FAA inhibitor – French drug trial 2016 – 1 death, 5 hospitalised.
∗ IF IT DOES NOT WORK OR CAUSES SIDE EFFECTS, STOP IT

∗ WHO pain ladder not appropriate – opiate rung
∗ Where are opiates are used –caution, monitoring, pain clinic involvement
Medication
http://www.sign.ac.uk/guidelines/fulltext/136/section5.html

∗ Not much difference between Chronic pain, FMS and NeuPain guidelines∗ Non-NeuPain – more use of NSAIDs, paracetamol, weak opioids, topical NSAIDs
∗ (Cruccu) “There is a broad agreement among the guidelines on pharmacological treatment of neuropathic pain”
∗ Three drug classes have received strong recommendations for first-line therapy in all guidelines: ∗ tricyclic antidepressants, particularly amitriptyline∗ serotonin-norepinephrine reuptake inhibitors (SNRIs) such as duloxetine∗ Gabapentinoids
∗ Tramadol “recommended by most guidelines for second-line treatment of neuropathic pain….......NICE recommend tramadol only for use in rescue therapy”
∗ “Drugs recommended for third- and fourth-line treatment commonly include”∗ strong opioids, ∗ anti-epileptic agents other than gabapentinoids, and ∗ cannabinoids.∗ Topical preparations of capsaicin and lidocaine are recommended for localized neuropathic pain.
BEYOND NNT AND NNH: QOL IMPROVEMENT IS A REAL NEED, NOT A BONUSCOMBINATION THERAPY: AN UNDER-RESEARCHED SOLUTION
Guidelines summary
www.hhs.gov/ash/advisory-committees/pain/reports/index.html

Interventional approaches
IASP. Dworkin RH, O’Connor AB, Kent J, et al. Interventional management of neuropathic pain: NeuPSIG recommendations. Pain. 2013;154:2249–61.
Cruccu G, Aziz TZ, Garcia-Larrea L, et al. EFNS guidelines on neurostimulation therapy for neuropathic pain. Eur J Neurol. 2007;14:952–70. Pain Ther (2017) 6 (Suppl 1):S35–S42 S41
CPS. Mailis A, Taenzer P. Evidence-based guideline for neuropathic pain interventional treatments: spinal cord stimulation, intravenous infusions, epidural injections and nerve blocks. Pain Res Manag. 2012;17:150–8.
Pain Clinic
U.S. Department of Health and Human Services (2019, May). Pain Management Best Practices Inter-Agency Task ForceReport: Updates, Gaps, Inconsistencies, and Recommendations. Retrieved from U. S. Department of Health and HumanServices website: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html

Interventional approaches∗ A comprehensive assessment by a skilled pain specialist is
necessary to identify which procedure is indicated for a given patient’s pain syndrome.
∗ Unfortunately, pain specialists are typically not involved in the multidisciplinary approaches of diagnosing and treating a pain patient early enough in his or her treatment, which can lead to suboptimal patient outcomes.
∗ The interventions are not curative; pt still needs non-pharmacologic coping skills
U.S. Department of Health and Human Services (2019, May). Pain Management Best Practices Inter-Agency Task ForceReport: Updates, Gaps, Inconsistencies, and Recommendations. Retrieved from U. S. Department of Health and HumanServices website: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html

Pain Management Programmes
https://www.britishpainsociety.org/static/uploads/resources/files/pmp2013_main_FINAL_v6.pdf

∗ Education∗ Rehabilitation
∗ Pain control∗ Physical and vocational rehabilitation∗ Psychological support
∗ Self-management∗ Goal focussed
∗ Rooted in a biopsychosocial model
Medical Rehabilitation Principles

Sessions include:∗ Making changes & maintaining change∗ Pacing∗ ‘Your move’ stretch programme∗ Pain education∗ Coping skills∗ Sport & recreation∗ Postural management∗ Anatomy & healing∗ Goal setting∗ Foiling a flare up∗ Relaxation∗ Nutrition∗ Work support∗ Medicines & future medical management∗ Friends & family group
Royal National Orthopaedic Hospital Pain management programme

∗ Functional Neurological Disorders∗ Focal dystonia∗ Non-epileptic seizures
∗ Ehlers-Danlos Syndrome/hypermobility∗ Chiari I∗ Postural Orthostatic Tachycardia Syndrome
∗ CRPS∗ Hereditary erythromelalgia
Challenging chronic pain: neurology, rheumatology,psychiatry interface

∗ Biopsychosocial model∗ Acute vs chronic
Can co-exist∗ Individualised∗ Sources of pain∗ Musculoskeletal factors∗ Psychological factors∗ Judicious and careful use of medication∗ Medication as an adjunct not the focus
Approach to chronic pain

https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html

Thank you for listening!