Embed Size (px)
Citation preview

CHRONIC OBSTRUCTIVE PULMONARY DISEASE UPDATE 2002
O. D. Polk, Jr., M.D.Assistant Professor of MedicineHoward University College of
Medicine

IMPACT OF COPD IN THE US Affects 21.7 million Americans The fourth leading cause of death
– 112,000 deaths in 1998 Annual cost >$30 billion
– $14.7 billion in direct healthcare costs– $15.7 billion in indirect healthcare costs
It is estimated that by 2020 COPD will be the third leading cause of death in the world
Data on file (analysis of NHANES III data), GlaxoSmithKline.American Lung Association. Fact sheet: chronic obstructive pulmonary disease (COPD).Murphy SL. National Vital Statistics Reports; 48(11); 2000.Murray CJL and Lopez AD, eds. The Global Burden of Disease. Vol. 1. 1996:362.

COPD VS ASTHMA
Annual EstimateCondition mortality (N) annual
cost
COPD 100,000 $25 billion
Asthma 5000-6000 $12 billion
Martin RJ. American Academy of Allergy, Asthma, and Immunology 56th
Annual Meeting; March 4, 2000; San Diego, Calif.

DEFINITION OF COPD Airflow limitation that is
not fully reversible usually progressive
Chronic abnormal inflammatory response to environmental pollutants irritants tobacco smoke
American Thoracic Society. Am J Respir Crit Care Med. 1995;152(suppl, pt 2):S77-S120.

DIFFERENTIAL DIAGNOSIS
American Thoracic Society. Am J Respir Crit Care Med. 1995;152(suppl, pt 2):S77-S120.

RISK FACTORS FOR COPD Tobacco smoking (80% to 90%) Passive smoking Ambient air pollution Hyperresponsive airways Exposure to occupational dusts and chemicals Indoor/outdoor air pollution Alpha1-antitrypsin deficiency (<1%)
American Thoracic Society. Am J Respir Crit Care Med. 1995;152(suppl, pt 2):S77-S120. Mahadeva R and Lomas DA. Thorax. 1998;53:501-505. Global Initiative for Chronic Obstructive Lung Disease. NHLBI/WHO Workshop Report. April 2001. NIH publication 2701.

GENETIC RISK FACTORS FOR COPD
Accelerated decline in lung function 15% of whites 5% of Asians
Alpha-1-Antitrypsin Deficiency (PiZZ) Gentic polymorphisms of the TNF,
cytochrome p450, and miocrosomal epoxide hydrolase

ALPHA1 –ANTITRYPSIN DEFICIENCY (AAT) Patients with emphysema: <1% Common variants: S and Z
Point mutations in alpha1-antitrypsin gene S-variant (264GluVal) in 28% of Southern Europeans
Alpha1-antitrypsin levels = 60% no pulmonary effects
Z-variant (342Glu Lys) is associated with severe deficiency
Levels 10% of normal Accumulation of alpha1-antitrypsin in the rough
endoplasmic reticulum of the liver Predisposed to juvenile hepatitis, cirrhosis, and
hepatocellular carcinoma
Mahadeva R and Lomas DA. Thorax. 1998;53:501-505.

PATIENT SELECTION FOR SCREENING FOR THE DIAGNOSIS OF AAT
Onset of COPD before age 50 COPD without smoking history Family history of COPD under age 50 Smoker with family history of COPD Young adult asthmatic unresponsive
to therapy Patient with predominant lower lobe
emphysema

PATHOPHYSIOLOGY OF COPD Hallmark – limitation of expiratory flow with
relative preservation of inspiratory flow Bronchial hyperresponsiveness – strong
predictor of progression of airway obstruction
Nonuniform ventilation Hyperinflation Increased work of breathing and dyspnea

CLINICAL FEATURES OF COPD Typical smokers—mean 20
cigarettes/day for 20 years Usually present in fifth decade of life
with productive cough or acute chest illness
Dyspnea with exertion History of wheezing and dyspnea may
lead to an erroneous diagnosis of asthma

SYMPTOMS OF COPD
Chronic cough Sputum production Breathlessness (dyspnea with
exertion) Wheezing
American Thoracic Society. Am J Respir Crit Care Med. 1995;152(suppl, pt 2):S77-S120.Global Initiative for Chronic Obstructive Lung Disease. NHLBI/WHO Workshop Report. April 2001. NIH Publication 2701.

PHYSICAL EXAMINATION FOR COPD Airflow obstruction
Wheezing during auscultation Prolongation of forced expiratory time
Hyperinflation of lungs Low diaphragmatic position Decreased intensity of heart and breath
sounds Severe disease
Pursed-lip breathing Use of accessory respiratory muscles Retraction of intercostal spaces
American Thoracic Society. Am J Respir Crit Care Med. 1995;152(suppl, pt 2):S77-S120.Global Initiative for Chronic Obstructive Lung Disease. NHLBI/WHO Workshop Report. April 2001. NIH Publication 2701.

COPD – MANAGEMENT Smoking Cessation Pharmacologic Therapy Oxygen Therapy Pulmonary Rehabilitation Nutrition and COPD Noninvasive Positive Pressure Ventilation Surgery for COPD
Lung Volume Reduction Surgery (LVRS) Lung Transplantation

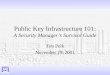
COPD RISK and SMOKING CESSATION
Fletcher C and Peto R. Br Med J. 1977;1:1645-1648.

SMOKING CESSATION Smoking cessation is the only measure
that will slow the progression of COPD (the Lung Health Study)
The presence of respiratory illness such as COPD is not a motivator for smoking cessation
Physician-delivered smoking cessation interventions can significantly increase smoking abstinence rates

SMOKING CESSATON INTERVENTION Physician Intervention – set a quit date Refer to group smoking cessation clinics Pharmacologic therapy with nicotine
replacement therapy (NRT) in highly dependent smokers Smokes a pack or more per day Requires 1st cigarette within 30 min of waking
up Finds it difficult refraining from smoking in
places where it is forbidden Consider therapy with bupropion alone or
in combination with NRT

HOWARD UNIVERSITY CANCER CENTER
Tobacco Control Program Ongoing Clinical Trial involving
Smoking Cessation We are recruiting patients Call
202-865-4036 202-806-5293

PHARMACOLOGIC THERAPY
Bronchodilators Short-acting Long-acting
Corticosteroids Mucolytics Antibiotics

SHORT-ACTING BRONCHODILATOR DRUGS
Beta2-agonists and anticholinergics Variable onset of action with duration of 4
to 6 h Improve symptoms and exercise capacity Safe 3 to 4 times daily Combining B2-agonists plus
anticholinergic drugs provides additional benefit to either drug alone

SHORTACTING BRONCHODILATORS

LONG-ACTING BRONCHODILATOR DRUGS Drugs
Salmeterol Formoterol Theophylline Oral beta2-agonists
Duration of action usually lasts 12-24 h
Commonly used as maintenance therapy in COPD

SYSTEMIC CORTICOSTEROIDS 10 TO 20% of patients with chronic
COPD improve Responders have more eosinophils in
induced sputum and bronchial biopsy Treatment of hospitalized patients
Fewer treatment failures Shorter stays More hyperglycemia Two (2) weeks of therapy is sufficient

INHALED CORTICOSTEROIDS
No short-term benefit Long-term use may
Improve lung function minimally Improve 6-muinute walk test Reduce moderate and severe (but not
mild) COPD exacerbations

MUCOLYTICS
Variable effects in patients with COPD
Ineffective at shortening the course or improving outcomes of patients with acute exacerbations

ANTIBIOTICS Multiple trials favor the use of
antibiotics for acute exacerbations of COPD Worsening dyspnea Increased sputum volume Sputum purulence
There is no evidence that prophylactic antibiotics prevent acute exacerbations.

OXYGEN THERAPY IN COPD

OXYGEN THERAPY Two controlled trials – MRC and NOTT
Death rates are lower Quality of life indexes improved Used for at least 15 hours/day
Oxygen should be prescribed when Arterial PaO2<55 mmHg or SaO2<88% PaO2 56 to 59 mmHg
ECG evidence of p pulmoonale Pedal Edema/CHF Secondary erythrocytosis

PULMONARY REHABILITATION
Improves dyspnea Improves QOL scores Reduces the number of
hospitalizations and days in the hospital
Effects on survival are not definite

NUTRITION AND COPD Malnutrition occurs in 1/4 to 1/3 of
patients with moderate to severe COPD Depletion of fat mass and fat-free mass Elevated resting energy expenditure
Nutritional supplements alone do not reverse weight loss
Megestrol acetate stimulates weight gain and ventilation in underweight COPD patients but did not improve respiratory muscle function

SURGERY FOR COPD Lung volume reduction surgery (LVRS)
Mortality 0 to 6% 30 days postop Mortality 0 to 8% 6 months postop Ongoing trials will provide cost-benefit
analysis Resection of large bullae Lung Transplantation
Procedure is costly Limited lack of organs Requires prolonged immunosuppression

NEW TREATMENTS Mediator Antagonists
Leukotriene antagonists TNF Antioxidants
Protease Inhibitors Antiinflammatory Drugs
Phosphodiesterase 4 inhibitors Drug Delivery

COPD: KEY POINTS Smoking cessation is extremely important. None of the existing medications for COPD
(with the exception of oxygen) are known to modify the long-term prognosis of this disease
Pharmacotherapy for COPD is used for the overall management of the disease (including improvement of lung function and QOL)
Bronchodilator medications are central to the symptom management of COPD. They are given on an as-needed basis or as maintenance therapy