Embed Size (px)
Citation preview

Chronic Kidney Disease
Christos Argyropoulos MD, PhDUniversity of New Mexico School of Medicine

Overview• Chronic Kidney Disease Basics• Review ACP guidelines for CKD care• Interface between Primary Care &
Nephrology – Special considerations in diabetes,
hypertension, CVD and CKD– Drug dosing considerations– What do nephrologists/CKD clinic do?– CKD “cheat-sheet”

CKD BASICS

1. Burden of chronic kidney disease (CKD) and kidney
failure
2. Back to the basics
Renal anatomy, physiology, and functional
assessment
“Numerology” of Nephrology (eGFR/proteinuria)
Identify and monitor CKD progression
Chronic kidney disease basics

BURDEN OF CKD

Chronic Kidney Disease
− Kidney function
Glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 for > 3
months with or without kidney damage
AND/OR
− Kidney damage
> 3 months, with or without decreased GFR, manifested by either
− Pathological abnormalities
− Markers of kidney damage, i.e., proteinuria (albuminuria)
» Urine albumin-to-creatinine ratio (UACR) > 30 mg/g
CKD is reduced kidney function and/or kidney damage
Reference: National Kidney Foundation Kidney Disease Outcome Quality Initiative (KDOQI). Clinical practice guidelines for chronic kidney disease: evaluation,
classification, and stratification. Amer J Kid Dis 2002; 39(2 suppl 1):S18–S266.
Kidneys cannot maintain homeostasis.
Kidney failure is associated with fluid, electrolyte,
and hormonal imbalances and metabolic
abnormalities.
ESRD means the patient is on dialysis or has a
kidney transplant.
Kidney failure is an eGFR < 15

Incidence of ESRD is increasing (and appears to be following obesity trends)
Reference: USRDS Annual Data Report (NIDDK, 2010)
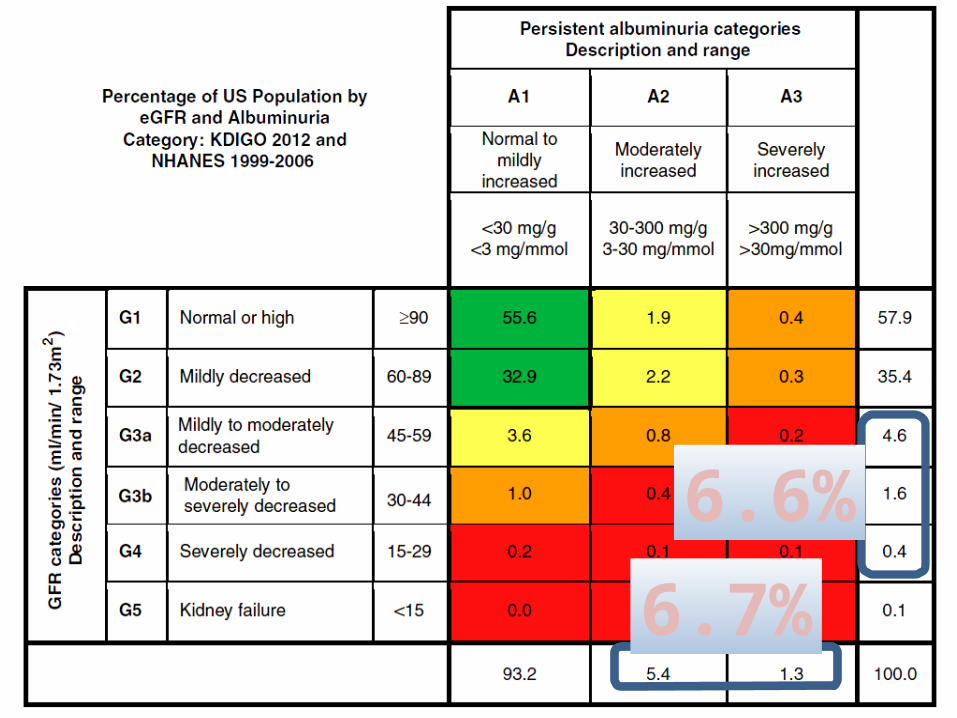
6.7%
6.6%

Diabetes is the leading cause of ESRD, followed by hypertension
Reference: Adapted from USRDS Annual Data Report (NIDDK, 2011)

New Mexico And Hawai Are Sister States(for Diabetic CKD)

Diabetes is an even more common cause of CKD in Sandoval County

Diabetes
Hypertension
Family history of kidney disease
Cardiovascular disease
Recurrent urinary tract infections
HIV infection
Autoimmune diseases
Risk factors for CKD

Historical cohort study (Kaiser) found that body
mass index (BMI) > 25 is an independent predictor
for ESRD.
A retrospective 20-year study in Norway found the
risk for CKD increases for pre-hypertensive patients
with BMI > 30.
Overweight may be an independent risk factor for CKD
References: Hsu et al. Ann Intern Med 2006; 144(1):21–28; Munkhaugen et al. Am J Kid Dis 2009; 54(4):638–646.



CKD (And ESRD) are costly
• Cost of treating ESRD : almost $50B/year• Cost of treating all CKD: $45.5B/year• Cost of treating diabetic CKD: $24.6B/year
Reference: Adapted from USRDS Annual Data Report (NIDDK, 2013)
BACK TO THE BASICS

The functions include: Filtration
− Glomeruli generate
ultrafiltrate of the plasma. Reabsorption
− Tubules selectively
reabsorb substances from
the ultrafiltrate. Secretion
− Tubules secrete
substances into the urine.
The nephron functions to maintain balance

Regulatory function
− Control composition and volume of blood
Maintain stable concentrations of inorganic anions such as
sodium (Na), potassium (K), and calcium (Ca)
− Maintain acid-base balance
Excretory function
− Produce urine
− Remove metabolic wastes
Including nitrogenous waste
The kidneys maintain homeostasis

Hormone function
− Produce renin for blood pressure control
− Produce erythropoietin which stimulates marrow
production of red blood cells
− Activate 25(OH)D to 1,25 (OH)2D (active vitamin D)
Metabolic function
− Gluconeogenesis
− Metabolize drugs and endogenous substances
(e.g., insulin)
The kidneys have other functions

We have a large physiologic reserve.
Slow, progressive loss of functioning nephrons may
not be noticeable.
The person with CKD may not feel different.
Each kidney has about 1 million nephrons; slow loss may not be noticeable

The composition of the urine changes.
Most people do not notice any difference in urine
volume.
Slow, progressive loss of function may not be
noticeable.
People with CKD still make urine

Damage to the filter allows larger molecular weight
substances such as albumin into the ultrafiltrate.
Increased urine protein may be a cause as well as a
sign of kidney injury.
Glomerular injury may result in urinary excretion of larger molecules

Urine volume may not change
− Composition of the urine changes
Reduced waste excretion
− May not be apparent until CKD is advanced
Altered hormone production
− Anemia (erythropoietin) and mineral & bone disorders
(vitamin D)
Reduced catabolism
− Examples: Insulin, glucagon, drugs
Fewer nephrons disrupt the balance

Reduced renal clearance and accumulation of:
− Advanced glycation end products
− Pro-inflammatory cytokines
− Reactive oxygen species (oxidation)
− Metabolic acids
Insulin resistance (even in people without diabetes)
− Reduces insulin-mediated glucose uptake in skeletal
muscles
− May be associated with inflammation as well
Fewer nephrons disrupt the balance

NUMEROLOGYeGFR and Albuminuria

GFR is equal to the sum of the filtration rates in all of
the functioning nephrons.
GFR is not routinely measured in clinical settings.
Estimation of the GFR (eGFR) gives a rough measure
of the number of functioning nephrons.
What is the glomerular filtration rate (GFR)?
A typical “normal” reference range of
0.6–1.2 mg/dL listed on many lab reports does not
account for muscle mass, age, gender,
and race.
A 28-year-old African American man with serum
creatinine of 1.2 has an eGFR > 60.
A 78-year-old white woman with serum creatinine of
1.2 has an eGFR of 43.
“Normal” serum creatinine may not be normal
eGFR is not the measured GFR.
The formula to estimate GFR was derived from a
population-based study.
eGFR is based on serum creatinine levels.
Previous methods to estimate kidney function also
are based on serum creatinine.
Creatinine assays are now standardized.
− Isotope Dilution Mass Spectrometry (IDMS)
eGFR estimates the measured GFR

Reference Table for Population Mean eGFR from NHANES III
Kidney function and eGFR decline with age
Reference: http://nkdep.nih.gov/professionals/gfr_calculators/gfr_faq.htm
Age (years) Mean eGFR (mL/min/1.73 m2)
20–29 116
30–39 107
40–49 99
50–59 93
60–69 85
70+ 75

Odds Ratio of Nephrology referral in the absence of automatic eGFR
reporting
PLoS ONE 9(11): e112767. doi:10.1371/journal.pone.0112767 (2014)http://www.plosone.org/article/info:doi/10.1371/journal.pone.0112767
1.13
(mg/dl)
2.26 3.40 4.52
1.7 – 2.8

Do not use with:
− Rapidly changing creatinine levels
Example: acute kidney injury
− Extremes in muscle mass, body size, or altered diet
patterns
− Medications that interfere with the measurement of
serum creatinine
Not all estimating equations are created equal
− MDRD is “blind” above 60 ml/min/1.73m2
Creatinine-based estimates of kidney function have limitations

Cystatin – C v.s. Creatinine• Cystatin – C is a “novel”
measure of renal function
• Estimating equations have been developed to use Cys-C alone or with SCr
• These equations do not always agree !

Normal: ≥ 60 mL/min/1.73 m2
Kidney disease: 15–59 mL/min/1.73 m2
Kidney failure: < 15 mL/min/1.73 m2
How to explain eGFR results to patients

Stable eGFR levels may mean non-progressive
disease or current therapy is working.
A rapid decline in eGFR may indicate rapid
progression of kidney disease.
A decline within the “>60” range may not always be
benign (even if the eGFR is technically “normal”)
Monitor the eGFR trends

Proteinuria/Albuminuria
• Though not a measure of GFR, it is a marker of kidney damage that independently predicts cardiovascular disease.
• It is in the definition of stage 1 and stage 2 CKD.
• Controversial whether microalbuminuria always represents kidney disease (CKD stage 1) or whether it could reflect endothelial dysfunction without kidney damage.
• Generally use spot urine for albumin/creatinine ratio- but can use total protein/creatinine for significant proteinuria (>500-1000 mg/g).

Standard of diabetes care (annual screen)
Diagnosis
− Forty percent of people are identified with CKD on the basis of
urine albumin alone.
− 50% of diabetics with CKD will NOT have abnormal albuminuria
Prognosis
− Important prognostic marker, especially in diabetes mellitus
(DM)
− Used to monitor and guide therapy (but note ACP guidelines)
Tool for patient education and self-management (such as
A1C or eGFR)
Urine albumin results are used for screening, diagnosing, and treating CKD

Definition of Albuminuria
Method Normal Micro-albuminuria
Overt/Macro-albuminuria
24 hour excretion <30 mg/day 30-300 mg/day >300 mg/day
Timed urine specimen <20 g/min 20-200 g/min >200 g/min
Spot-urine albumin specific dipstick
(screening)<3 mg/dl >3 mg/dl N/A
Spot urine albumin/ creatinine ratio (ADA) < 30 mg/g 30-300 mg/g >300 mg/g
Spot urine albumin/ creatinine ratio (gender
specific) (K/DOQI)
<17 mg/g (men)<25 mg/g (women)
17-250 (men)25-355 (women)
>250 (men)>355 (women)
K/DOQI and ADA
Dipstick
− Semi-quantitative, screening only
Affected by urine concentration, highly variable
− Detection of urine albumin > 300 mg/day
(1+ approximates albumin excretion of 30 mg/day)
Urine protein/creatinine ratio
‒ All proteins, not just albumin (myeloma/CIN)
Urine albumin-to-creatinine ratio (UACR)
‒ Quantifies urine albumin
− Steps toward standardization currently in progress
− Standard for public health, clinical care, and research
Which urine test to use?

Urinary ACR is NOT perfect
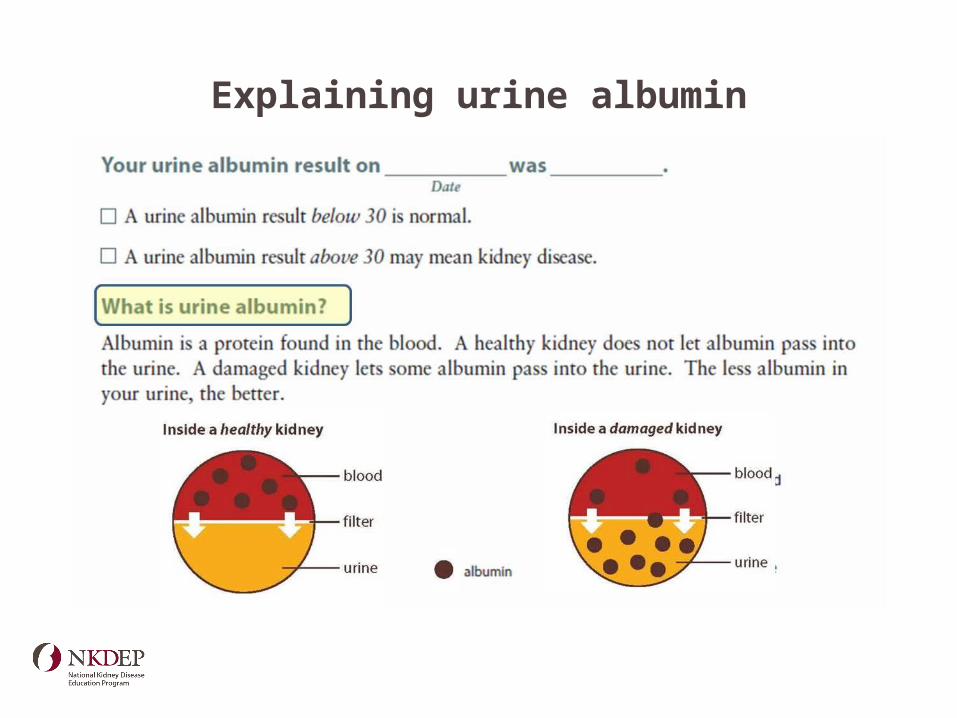
Explaining urine albumin

Hypertension, diabetes and elevated creatinine
• 75 y/o female with long standing hypertension and diabetes.
• To her knowledge, she has not had any kidney problems previously.
• MRI/MRA small kidney approximately 9 cm bilaterally.
Lab parameter Value
Serum Creatinine 1.9 mg/dL
BUN 46 mg/dL
Hemoglobin 12.1 g/dL
HbA1c 8.1%
Albumin:Creatinine Ratio
250

Patient with hypertensionand elevated creatinine
What is her kidney function?Lab parameter ValueSerum Creatinine 1.9 mg/dLBUN 46 mg/dL
Pick your preferred equation to calculate her GFR…
• 100/Scr = 45.4• Cockroft-Gault = 25
ml/min• CKD-EPI = 25 ml/min• MDRD = 28 ml/min• 24-hour urine collection
= 27 ml/min

Patient with hypertensionand elevated creatinine
How can we characterize her kidney function?– Cause: Type 2 Diabetes
Albumin• 135 mg/gGFR• 100/Scr = 45.4 • C-G = 25 ml/min• CKD-EPI = 28 ml/min• MDRD = 28 ml/min• 24-hour urine = 27 ml/min
High Risk of Progression

ACP GUIDELINES

ACP Guidelines• Recommendation 1: ACP recommends against screening for chronic kidney
disease in asymptomatic adults without risk factors for chronic kidney disease. – (Grade: weak recommendation, low-quality evidence)

• Recommendation 2: ACP recommends against testing for proteinuria in adults with or without diabetes who are currently taking an angiotensin-converting enzyme inhibitor or an angiotensin II–receptor blocker. – (Grade: weak
recommendation, low-quality evidence)
– Residual albuminuria in fixed dose ARB trials: increased renal risk
ACP Guidelines
ACP Guidelines
• Recommendation 3: ACP recommends that clinicians select pharmacologic therapy that includes either an angiotensin-converting-enzyme inhibitor (moderate-quality evidence) or angiotensin II–receptor blocker (high-quality evidence) in patients with hypertension and stage 1 to 3 chronic kidney disease. – (Grade: strong recommendation)
• The risk for ESRD was not reduced in patients with only microalbuminuria or impaired GFR.
• Pooled data from 10 trials showed that mortality risk was reduced in patients with microalbuminuria, although most of the data were derived from a large study that showed no difference in mortality between patients with and without microalbuminuria.
• Therapy with ACE inhibitors did not reduce the risk for cardiovascular mortality, myocardial infarction (MI), stroke, or other vascular outcomes.

Benazepril effective in advanced CKD
• Findings consistent with earlier results from REIN Trial (Ruggenenti 2001) and systematic review (Bakris 2000).
• Cough 17% in run in period, >30% bump in creatinine 2%.
• NNT with benazepril 5-6 for composite outcome of doubling creatinine, ESRD, death (Hsu ACP Journal Club).
• Shows that benazepril safe and effective in advanced non-DM CKD.Hou NEJM 2006

ACP Guidelines• Recommendation 4: ACP recommends that clinicians
choose statin therapy to manage elevated low-density lipoprotein in patients with stage 1 to 3 chronic kidney disease.– (Grade: strong recommendation, moderate-quality evidence)

Moderately Elevated Systolic Blood Pressure Combined With Normal Diastolic Blood
Pressure Had Consistently Lower Mortality Rates Among U.S. Veterans With CKD
• Kovesdy CP, Bleyer AJ, Molnar MZ, et al. Blood pressure and mortality in U.S. veterans with chronic kidney disease: a cohort study. Ann Intern Med. 2013;159:233-42.
• The BP targets for patients with CKD have been unclear and may differ by severity of proteinuria or diabetes status.

US VA CKD Cohort Outcomes • The relationship of both SBP and
DBP with mortality was U-shaped.
• Various combinations of lower SBPs and DBPs were associated with lower mortality rates as long as the DBP remained greater than approximately 70 mm Hg.
• Patients with SBP of 130-159 mm Hg and DBP of 70-89 mm Hg had the lowest mortality rates.
• Patients with “ideal” BP (<130/80 mm Hg) had increased mortality rates because the study included patients with low SBPs and DBPs.

Implications
• This study challenges guidelines recommending lower BP targets for patients with CKD.
• These findings are consistent with the Eighth Joint National Committee recommendations. – Recommendation 4 in the population aged ≥18 years with
CKD, initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to goal SBP <140 mm Hg and DBP <90 mm Hg. (Expert Opinion – Grade E)
• Further information on BP targets will be provided by SPRINT (Systolic Blood Pressure Intervention), an ongoing trial by the National Institutes of Health that examines BP targets in older adults with and without CKD.

Relaxation of CKD BP Target Guidelines
Group Goal BP Initial Therapy
Group Goal BP Initial Therapy
ADA 2009 <130/80 ACE/ARB ADA 2013 ≤140/90 ACE/ARB
JNC 7 <130/80 ACE/ARB JNC 8 <140/90 ACE/ARB
KDOQI (2007)
<130/80 ACE/ARB KDIGO 2013
<140/90 ACE/ARB
<130/80 proteinuria
Am Society of HTN 2008
≤130/80 ACE/ARB ASH/ISH 2013
<140/90 ACE/ARB
<130/80 Some experts for proteinuria

SPRINT Important Goals https://sprint.phs.wfubmc.edu
• SPRINT will test whether a treatment strategy aimed at reducing SBP to a lower goal (< 120 mm Hg) than currently recommended (< 140 mm Hg) will reduce the occurrence of cardiovascular (CVD) and CKD events.
• SPRINT Memory and cognition In Decreased Hypertension (MIND) will test whether the lower SBP goal influences the occurrence of dementia, change in cognition, and change in brain structure.

INTERFACE BETWEEN PRIMARY CARE AND NEPHROLOGY

Lifestyle modifications help lower blood pressure in the general population
References: Chobanian et al. J Am Med Assoc 2003; 289(19):2560–2571; Neter et al. Hypertension 2003; 42(5):878–884; Dietary Guidelines, 2010
Modification Recommendation Lowers Systolic Blood Pressure by (Range)
Weight reduction •Maintain normal body weight•Body mass index (BMI) 18.5–24.9 kg/m2
5–20 mm Hg / 10 kg 4 mm Hg / 5 kg
DASH •Increase potassium (fruits and vegetables) and calcium (dairy)•DASH may be too high in protein, potassium and phosphorus for CKD
8–14 mm Hg
Physical activity •At least 30 minutes most days 4–9 mm Hg
Moderate alcohol consumption
•Women: ≤ 1 drink per day •Men: ≤ 2 drinks per day
2–4 mm Hg
Sodium restriction •2,300 mg per day•1,500 mg per day for hypertension, diabetes, and CKD
2–8 mm Hg
Modification Recommendation Lowers Systolic Blood Pressure by (Range)
Weight reduction •Maintain normal body weight•Body mass index (BMI) 18.5–24.9 kg/m2
5–20 mm Hg / 10 kg 4 mm Hg / 5 kg
DASH •Increase potassium (fruits and vegetables) and calcium (dairy)•DASH may be too high in protein, potassium and phosphorus for CKD
8–14 mm Hg
Physical activity •At least 30 minutes most days 4–9 mm Hg
Moderate alcohol consumption
•Women: ≤ 1 drink per day •Men: ≤ 2 drinks per day
2–4 mm Hg
Sodium restriction •2,300 mg per day•1,500 mg per day for hypertension, diabetes, and CKD
2–8 mm Hg
Have not been extensively studied in CKD !!

CKD and hypertension
BP ≤ 140/90 may be
beneficial for many
Nephrologists like ≤ 130/80
for proteinuria (for now)
Multiple medications (>2-3)
Most will need a diuretic
Assessment:
Food–medication interaction
− Hyperkalemia
Intervention:
Limit sodium
− Keep to ≤ 1,500 mg/day (?
harm in DM w/o CKD)
− Avoid salt substitutes
Limit potassium when
serum level is elevated
− Individualized
Most CKD patients will not
become hypokalemic when
treated with a diuretic

Renal threshold for glucose is 180–200 mg/dL.
Sugars cross-linking to proteins changes their shapes and functions (AGEs).
A1C goal is individualized (≤ 7% in ADA 2014).
Spontaneous improvement in glycemic control may indicate CKD progression and medications may change.
Risk for hypoglycemia occurs with CKD (insulin is cleared from the kidneys, 20% of gluconeogenesis occurs in the kidney); risk for hyperkalemia occurs with ACEi and ARBs.
− Use low-potassium juice to treat hypoglycemia.
− Light-colored soda pop is lower in phosphorus than cola.
CKD and diabetes I

Any “juice” can treat hypoglycemia, even those low in potassium
mg

Urine albumin excretion is associated with diabetic kidney
disease, but not all people will have high urine albumin
levels.
High levels of urine albumin may mean more rapid
progression of CKD.
Good control of diabetes early may help reduce the risk of
albuminuria later.
Tight versus good control may not slow progression
Potential dangers associated with very tight control and
sodium restriction
CKD and diabetes II

Same traditional factors as the general population
Also Nontraditional risk factors which include:
− Albuminuria
− Anemia
− Abnormal calcium and phosphorus metabolism
Statins are used in CKD patients with some caution
(ezetimibe/simvastatin may be more beneficial: off label)
Some foods rich in soluble fiber may be higher in K and P
than recommended for CKD patients.
Phosphorus in food additives is absorbed much more readily.
CKD and CVD

Control blood pressure (ACEi/ARB)
Reduce sodium intake (but note emerging data
about possible harms in diabetics)
Achieve good control of diabetes early; may help
prevent albuminuria
Reduce weight (if obese)
Reduce protein intake, if excessive
Achieve tobacco cessation
Interventions for reducing urine albumin


Drug Dosing Considerations• Renal impairment may alter both pharmacodynamics and
pharmacokinetics• There is a higher risk for Adverse Drug Reactions as a result of renal
functional impairment AND comorbidities in CKD patients• Drug development programs and the FDA lag behind clinical
practice when quantifying renal function and risk (MeDRA uses creatinine elevation, studies are designed based on Cockroft Gault)
• MOST DRUGS HAVE NEVER BE TESTED IN CKD POPULATIONS• Dosing recommendations are often based on post-hoc analyses or
PK/PD modeling using “general population” relationships• One is often conducting an RCT n=1 when prescribing a medication
in CKD

Cockroft Gault ≠ MDRD for drug dosing
Ann Pharmacother 2012;46:1174-87
For patients with advanced age, low weight, and modestly elevated serum creatinine, further work is needed before the MDRD equations can replace the CG equation for dose adjustment in the labeling.

Renal function estimation formulas for drug dosing
Pharmacotherapy. 2011;31(11):1130-1144.

The cautious approach to drug
dosing in CKD
Pharmacotherapy. 2011;31(11):1130-1144.

Glyburide
Metformin (US label SCr>1.4-
1.5 ex-US eGFR>30)
Alpha-glucosidase inhibitors
Exenatide
Glimepiride
Sitagliptin
Repaglinide
Insulin (dose decrease)
Glipizide
Pioglitazone
− Fluid retention (bladder cancer,
↑ risk of CKD?)
Nateglinide
Pramlintide
SGLT2 inhibitors:
− Canaglifozin
(Invokana)/empaglifozin
(Jardiance) (stop if eGFR<45)
− Dapaglifozin(Farxiga) (stop if
eGFR<60)
Diabetes medications may be discontinued or adjusted in CKD
Reference: Reilly & Berns Seminars in Dialysis 2010; 23(2):163–168.Farxiga/Invokana/Jardiance PIL

Alternatives to warfarin that are licensed for use without Therapeutic Drug Monitoring
− Rivaroxaban (Xarelto) : Xa inhibitor
− Apixaban (Eliquis): Xa inhibitor
− Dabigatran (Pradaxa): DRI
No dietary restrictions compared to Coumadin Rapidly expanding clinical use Safety signals for older individuals with renal
impairment They are removed by the kidneys Dialytic clearance substantial only for dabigatran
Novel Oral AntiCoagulants (NOACs) in CKD

Safety of NOACs in CKD (major or clinically relevant bleeding)
eGFR(50-79) eGFR(30-49)

Efficacy of NOACs in mild CKD (eGFR 50-79)
Stroke VTE or VTE related death

Efficacy of NOACs in moderate CKD (eGFR 30-49)
Stroke VTE or VTE related death
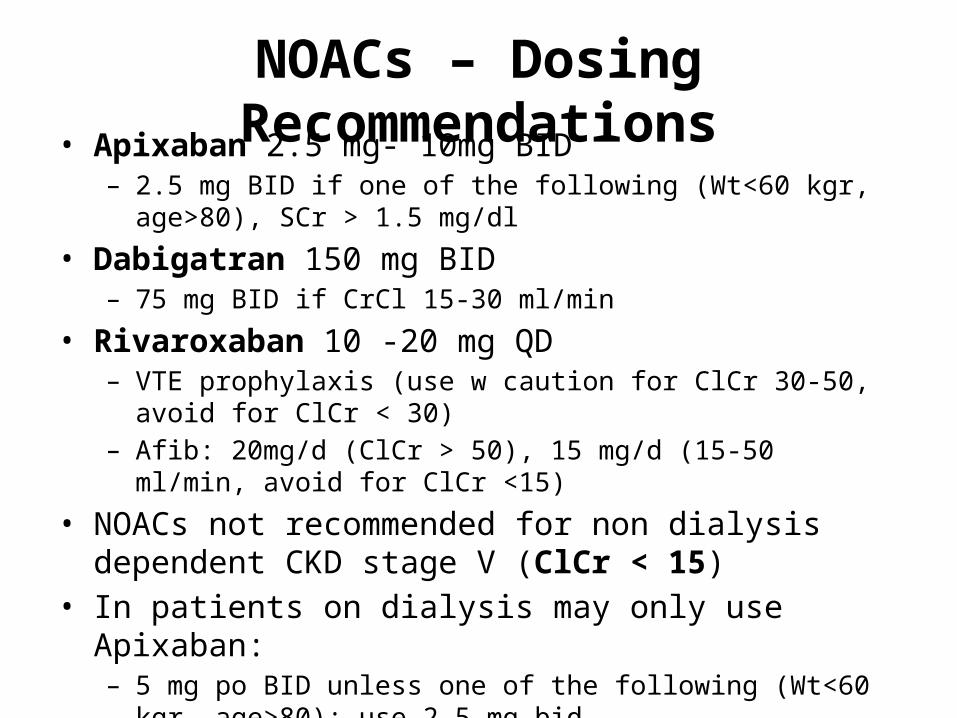
NOACs – Dosing Recommendations• Apixaban 2.5 mg- 10mg BID
– 2.5 mg BID if one of the following (Wt<60 kgr, age>80), SCr > 1.5 mg/dl
• Dabigatran 150 mg BID– 75 mg BID if CrCl 15-30 ml/min
• Rivaroxaban 10 -20 mg QD– VTE prophylaxis (use w caution for ClCr 30-50, avoid for ClCr < 30)– Afib: 20mg/d (ClCr > 50), 15 mg/d (15-50 ml/min, avoid for ClCr <15)
• NOACs not recommended for non dialysis dependent CKD stage V (ClCr < 15)
• In patients on dialysis may only use Apixaban:– 5 mg po BID unless one of the following (Wt<60 kgr, age>80): use 2.5
mg bid

Medications that increase risk for hyperkalemia in CKD
Referece: Chobanian et al. J Am Med Assoc 2003; 289(19):2560–2571
Commonly prescribed
Angiotensin-Converting
Enzyme Inhibitor (ACEi)
Angiotensin Receptor
Blockers (ARB)
Used cautiously in CKD
Aldosterone antagonists
Renin inhibitors
Potassium-sparing
diuretics
Whenever an ACEi/ARB/Aldo antagonist/DRI is started check K within 7-10 days (but not sooner than 7 or >14)K-sparing diuretics in CKD or diabetes (with normal eGFR/proteinuria): check K within 3-7 days (but not later)

The role of the nephrologist outside the dialysis unit
• Treating complications of CKD• Slowing progression• Preparation for renal replacement therapy:
– Outpatient hemodialysis– Home hemodialysis– Peritoneal dialysis (home therapy)– Pre-emptive renal transplantation

Fewer functioning nephrons may mean:
− Inadequate erythropoietin (anemia)
− Accumulation of potassium (K)
− Accumulation of hydrogen ion (metabolic acidosis)
− Inadequate activation of vitamin D (bone disease)
− Accumulation of phosphorus (P)
− Accumulation of pro-inflammatory cytokines Toxins build up in the blood.
Complications increase as kidney function declines

Complications may increase as estimated glomerular filtration rate (eGFR) decreases
Reference: Adapted from USRDS 2010 Annual Data Report (NIDDK, 2010)

• Delivered by a CKD educator (usually a RN) meeting face to face with the patient
• Increase number of pts. receiving early (stage 3 & 4) CKD education statewide.
• Prevent “traumatic dialysis starts”: decrease catheter placement rate, increase fistula placement and PD catheter placement rate.
• Increase number of pts. choosing Home Dialysis.• Slow progression of CKD and delay need for dialysis.• Prevent dialysis through pre-emptive transplant.
IT IS NOT JUST ABOUT THE NEPHROLOGIST: CKD EDUCATION PROGRAM OBJECTIVES

What else is out there?(all these are off label)
• VDRAs (calcitriol, paricalcitol, doxercalciferol) for proteinuria (GNs/DM)
• Uric acid modulation• Alkali therapy for acidosis• Pentoxifylline• SGLT2 (early stage DN: in clinical trials)• Aldosterone antagonists (in combination with ACEi/ARBs: not
undertaken lightly)• K-sparing diuretics for tx resistant volume overload in
proteinuria(not undertaken lightly – UNM clinical trial experience: NCT01804777)
• DRIs (Direct Renin Inhibitors)• ETR- A antagonists (in clinical trials)
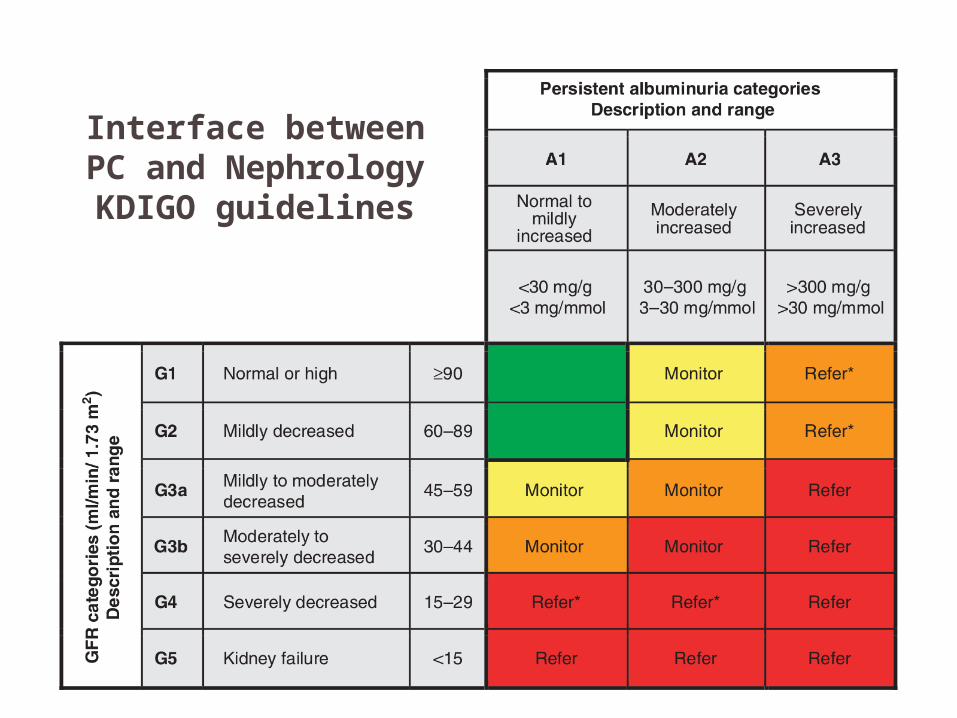
Interface between PC and NephrologyKDIGO guidelines

CKD Checklist for PCPs• Slowing Progression
– BP < 140/90– HBA1c ≤ 7% within 6 mos– Annual screen for proteinuria– On ACEi/ARB if DM or microalb
> 30mg/g– Smoking cessation– Discuss avoidance of
NSAIDs/nephrotoxins– LDL < 100 within the last year– 5 year pneumovax– Yearly flu
• Tx of Complications– CBC, iron studies within the
year– Ca, P, PTH (q 6 mo if eGFR <
60, q 3 mo if eGFR < 30)
• Nephrology Referral– GFR < 30– Persistent proteinuria
despite ACEi– Persistent hyperK– Resistant HTN (≥4 meds)– ↓GFR by 30% (“certain
drop”) irrespective of eGFR– Unclear etiology of CKD– Anemia requiring ESAs– ↑ P, PTH
CJASN 9:1526-1535, 2014


