Embed Size (px)
Citation preview
The American College of Osteopathic Family Physicians is accredited by the American Osteopathic Association Council to sponsor continuing medical education for osteopathic physicians.
The American College of Osteopathic Family Physicians designates the lectures and workshops for Category 1-A credits on an hour-for-hour basis, pending approval by the AOA CCME, ACOFP is not responsible for the content.
ACOFP / AOA’s 122nd Annual Osteopathic Medical Conference & Exposition
OCTOBER 7 - 10PHILADELPHIA, PENNSYLVANIA29.5 Category 1-A CME credits anticipated
OMED 17®
ACOFP - The Heart of the Matter - An Evidence Based Approach to Common Cardiovascular Concerns:
Primary Care Approach to Hypertension - Sorting Out the Latest Treatment Guideline
Michael Levin, DO
9/25/2017
1
The Management of Hypertension
in 2017
Targets and Therapies
Michael Levin, D.O., FA.C.O.I.
Chair: Division of Nephrology
Philadelphia College of Osteopathic Medicine
Metropolitan Nephrology Associates
www.metroneph.com
@MetroNephro
Objectives
Review recent evidence affecting the diagnosis and
management of patients with elevated blood pressure
Discuss the therapeutics of various antihypertensive
agents used in managing patients with hypertension
Compare and contrast BP targets and first-line therapy
options from various clinical practice hypertension
guidelines ( e.g., JNC , ADA)

9/25/2017
2
The Renal Continuum of Care
Nephrologist
Primary Care Physician
ESRDCKD
At Risk
Population
Diabetes
Hypertension
Obesity
CVD
26,000,000+ People500,000+ People
~375,000 Dialysis
~125,000 Transplant
9/25/2017
3
Patient Background
60 y/o African American Male evaluated for challenging to control blood pressure issues
Diagnosed during routine examination in Primary Care office 4 years prior and has been a challenge for the Medical team to control
PMHx: HTN, CAD with stent, CKD stage 3, Obesity, DM x 4 years
PSH: Cardiac PTCA with DES Circumflex
Medications: Lisinopril 40 mg Daily, Coreg 25 mg Twice per day, Hydrochlorthiazide 25 mg per day
FamHx: Father; deceased, MI at 50
SocHx: Smoker, 15 pack years; quit 10 years ago. Factory worker.
Physical Exam
BP: 168/94 HR: 84 BMI: 44
Neck: supple, no goiter, but circumference > 18 inches
Heart: 84 per minute, no gallop or rub
Lungs: clear
Extremities: reduced pinprick b/l, no peripheral edema
Eyes: dilated exam background retinopathy changes
9/25/2017
4
Labs at Evaluation
Hgb 14.8 Hct 36%
Hgb A1C: 8.6%
Na: 140 K: 5.5 Cl: 104 CO2: 26
BUN: 31 Cr: 2.2 eGFR: 36 cc/min
UA: 1+ protein, no RBC’s
9/25/2017
5

9/25/2017
6

9/25/2017
7
Hypertension:
A Brief Snapshot
Most common modifiable CVD/Renal risk
factor
Contributed to > 50 % of adverse CVD outcomes
BP Control
Reduces Heart Failure by 50%; CVA by 40%; MI
25%
33 % of adults will be affected
60 % increase by 2025
US Renal Data System: Annual Data Report, US Department of Public Health and Human
Services, NIH 2007
9/25/2017
8
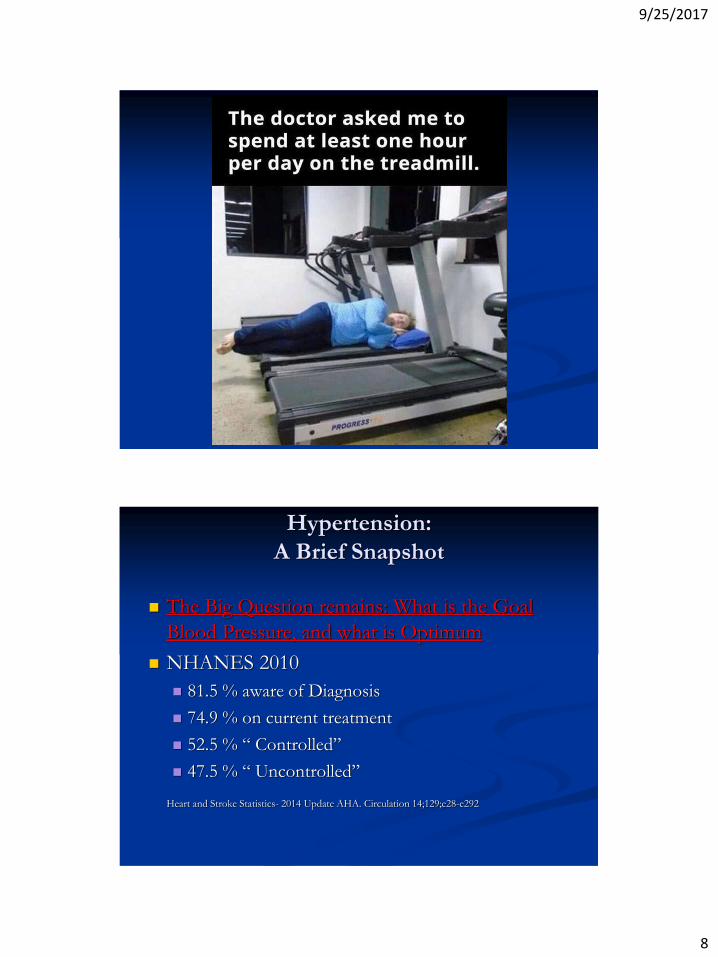
Hypertension:
A Brief Snapshot
The Big Question remains: What is the Goal
Blood Pressure, and what is Optimum
NHANES 2010
81.5 % aware of Diagnosis
74.9 % on current treatment
52.5 % “ Controlled”
47.5 % “ Uncontrolled”
Heart and Stroke Statistics- 2014 Update AHA. Circulation 14;129;e28-e292
9/25/2017
9
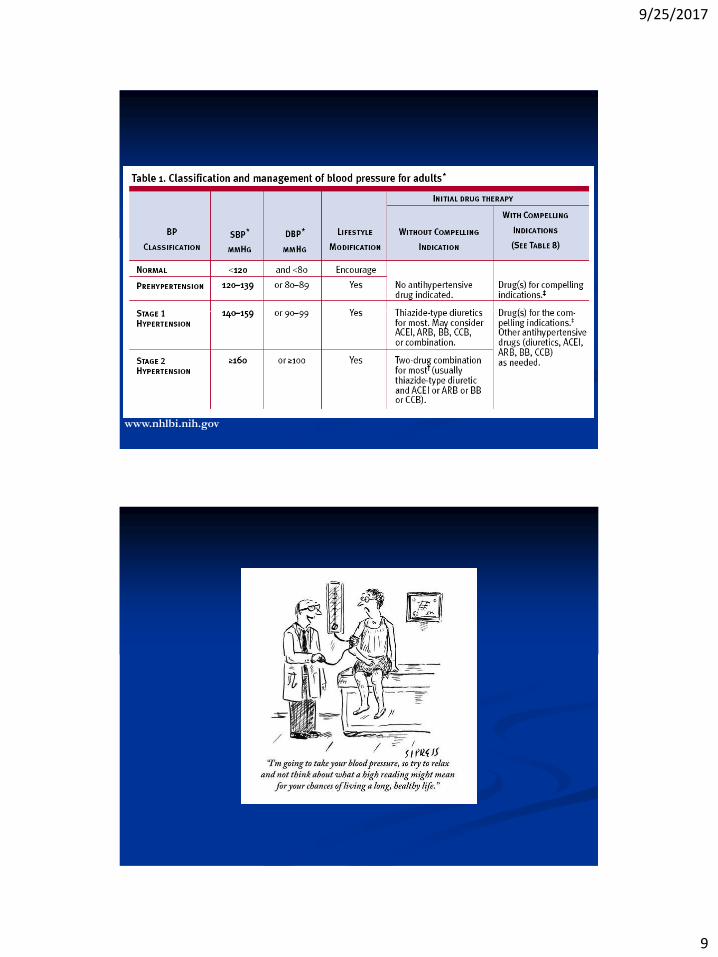
www.nhlbi.nih.gov
9/25/2017
10
9/25/2017
11
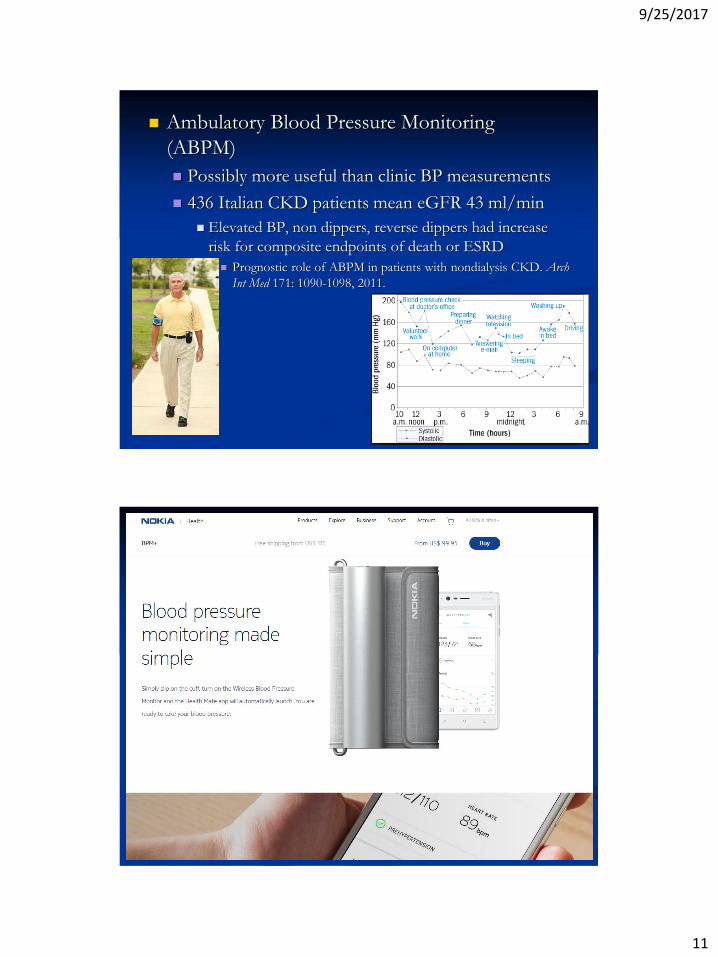
Ambulatory Blood Pressure Monitoring
(ABPM)
Possibly more useful than clinic BP measurements
436 Italian CKD patients mean eGFR 43 ml/min
Elevated BP, non dippers, reverse dippers had increase
risk for composite endpoints of death or ESRD
Prognostic role of ABPM in patients with nondialysis CKD. Arch
Int Med 171: 1090-1098, 2011.

9/25/2017
12
9/25/2017
13
9/25/2017
14
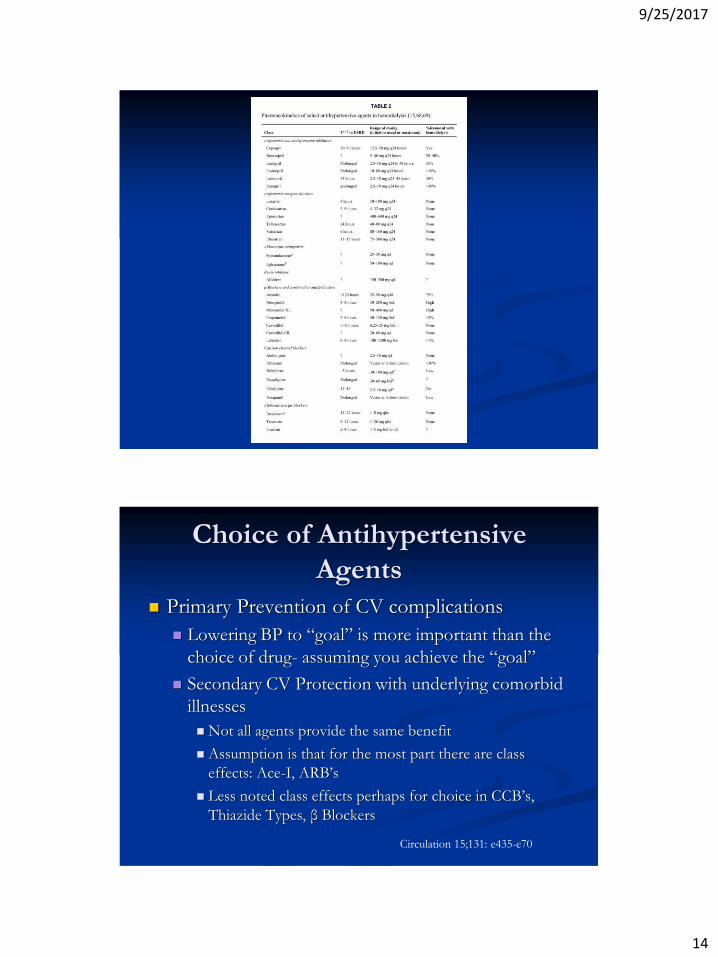
Choice of Antihypertensive
Agents
Primary Prevention of CV complications
Lowering BP to “goal” is more important than the
choice of drug- assuming you achieve the “goal”
Secondary CV Protection with underlying comorbid
illnesses
Not all agents provide the same benefit
Assumption is that for the most part there are class
effects: Ace-I, ARB’s
Less noted class effects perhaps for choice in CCB’s,
Thiazide Types, β Blockers
Circulation 15;131: e435-e70

9/25/2017
15
Thiazide (Type/Like) Diuretic
Class
HCTZ vs. Chlorthalidone(CTD)

9/25/2017
16
Beta Blockade as Initial Therapy
9/25/2017
17
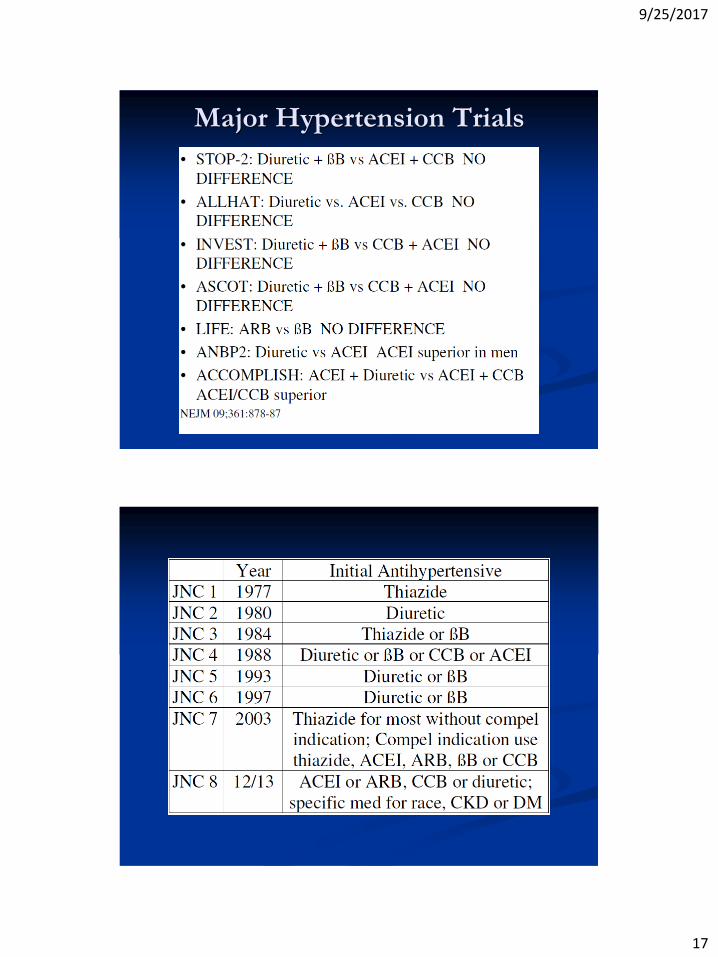
Major Hypertension Trials
9/25/2017
18

9/25/2017
19
Lifestyle modifications
www.nhlbi.nih.gov
9/25/2017
20
9/25/2017
21
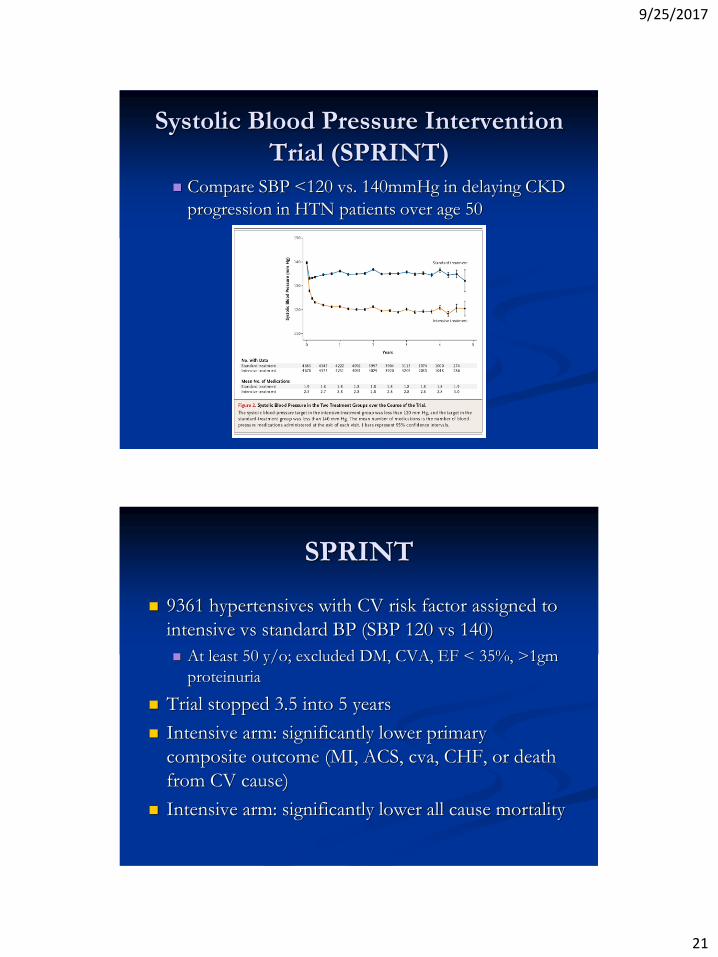
Systolic Blood Pressure Intervention
Trial (SPRINT)
Compare SBP <120 vs. 140mmHg in delaying CKD
progression in HTN patients over age 50
SPRINT
9361 hypertensives with CV risk factor assigned to
intensive vs standard BP (SBP 120 vs 140)
At least 50 y/o; excluded DM, CVA, EF < 35%, >1gm
proteinuria
Trial stopped 3.5 into 5 years
Intensive arm: significantly lower primary
composite outcome (MI, ACS, cva, CHF, or death
from CV cause)
Intensive arm: significantly lower all cause mortality
9/25/2017
22
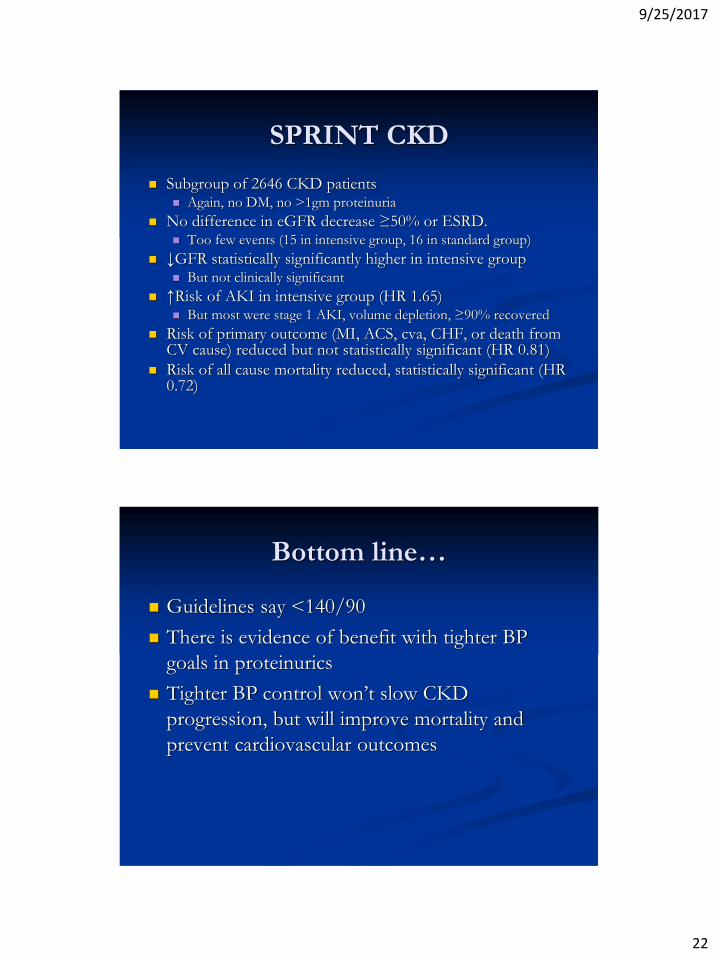
SPRINT CKD
Subgroup of 2646 CKD patients Again, no DM, no >1gm proteinuria
No difference in eGFR decrease ≥50% or ESRD. Too few events (15 in intensive group, 16 in standard group)
↓GFR statistically significantly higher in intensive group But not clinically significant
↑Risk of AKI in intensive group (HR 1.65) But most were stage 1 AKI, volume depletion, ≥90% recovered
Risk of primary outcome (MI, ACS, cva, CHF, or death from CV cause) reduced but not statistically significant (HR 0.81)
Risk of all cause mortality reduced, statistically significant (HR 0.72)
Bottom line…
Guidelines say <140/90
There is evidence of benefit with tighter BP
goals in proteinurics
Tighter BP control won’t slow CKD
progression, but will improve mortality and
prevent cardiovascular outcomes
9/25/2017
23
9/25/2017
24
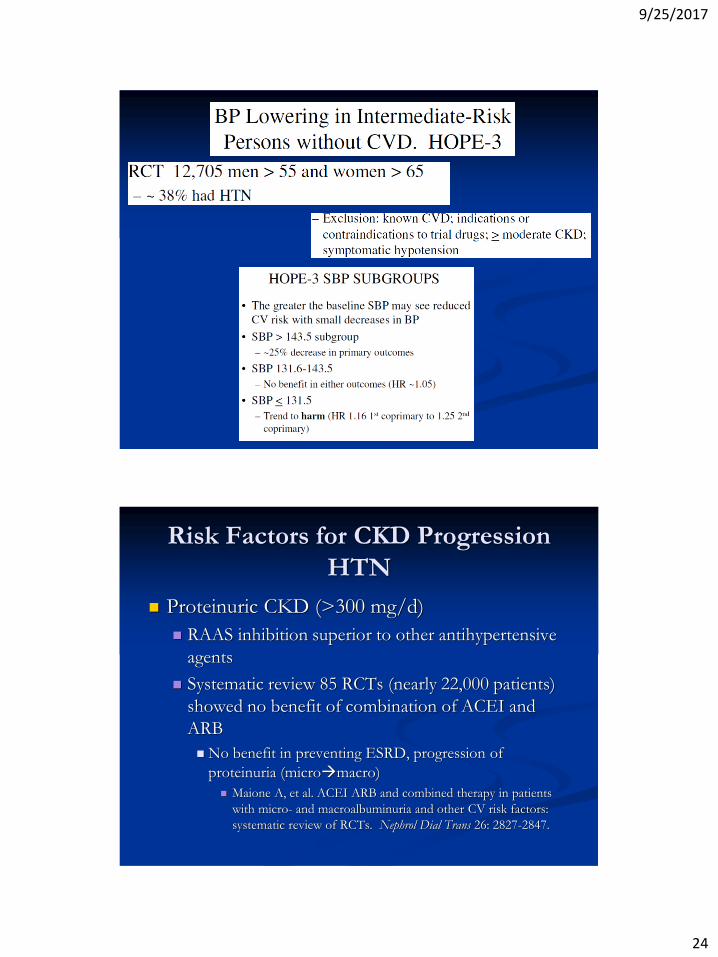
Risk Factors for CKD Progression
HTN
Proteinuric CKD (>300 mg/d)
RAAS inhibition superior to other antihypertensive
agents
Systematic review 85 RCTs (nearly 22,000 patients)
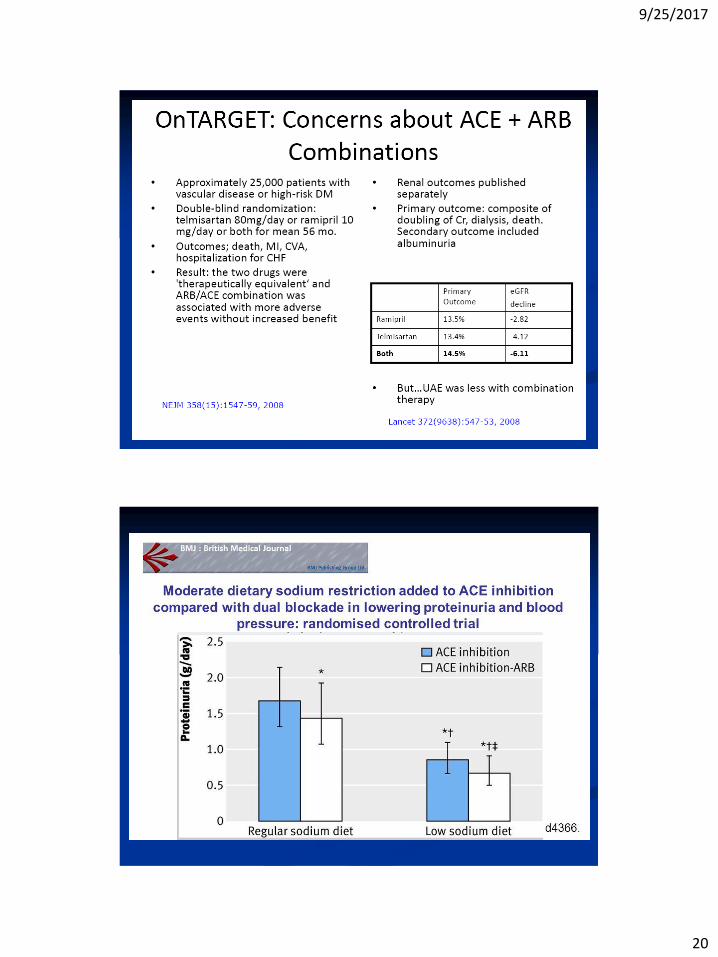
showed no benefit of combination of ACEI and
ARB
No benefit in preventing ESRD, progression of
proteinuria (micromacro)
Maione A, et al. ACEI ARB and combined therapy in patients
with micro- and macroalbuminuria and other CV risk factors:
systematic review of RCTs. Nephrol Dial Trans 26: 2827-2847.
9/25/2017
25
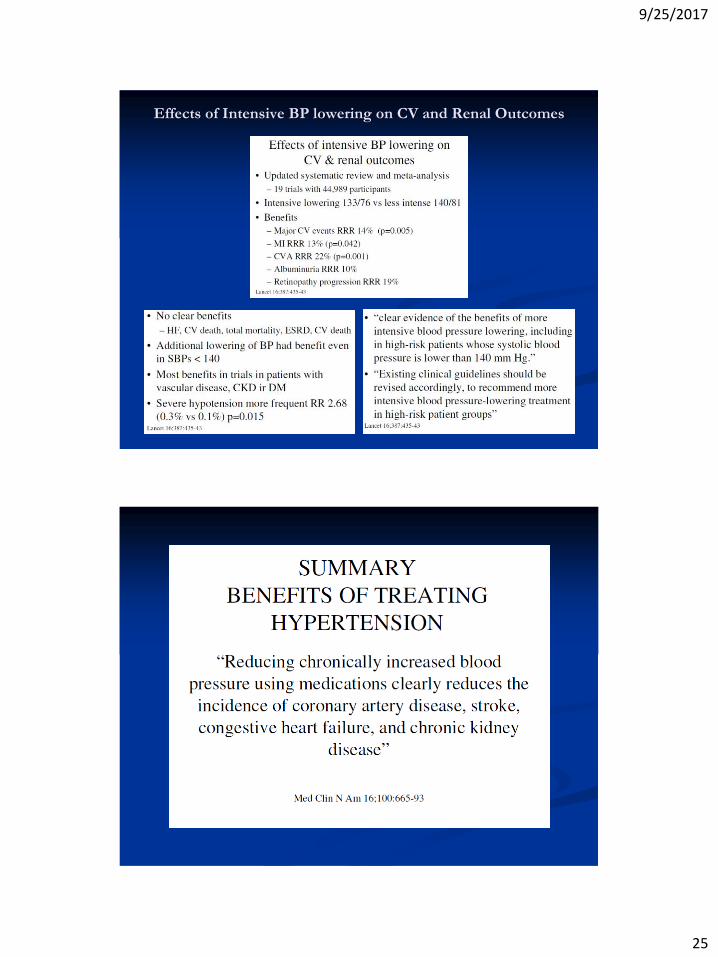
Effects of Intensive BP lowering on CV and Renal Outcomes
9/25/2017
26


