Embed Size (px)
Citation preview

Journal of Hepatology, 1988; 7: 169-174 169 Elsevier
HEP 00456
Chronic hepatitis D in intravenous drug addicts and non-addicts
A comparative clinico-pathological study
M. Buti, A. Mas, J.M. S~.nchez-Tapias, R. Esteban, M. Bruguera, H. Allende, J. Costa, J. Guardia and J. Rod6s
Liver Unit. Ho~7)ital Clinic, Univer~idad de Barcelona a .d Departme.ts of lmer.al Medici.e and Pathology, Ciudad Sa.itaria "Valle de Hebron', Universidad A uto.oma de Barcelona, Barcelo.a (Spain)
(Received 27 October 1987) (Accepted 17 May 1988)
Summary
In recent years chronic infection by the hepatit is delta virus (HDV) has become an important cause of chronic
liver disease among drug addicts. To evaluate the influence of addict ion to i.v. drugs on the course of this disease
we have analyzed the clinicaL, his topathological , virological and evolutive features in 18 addicts and 11 non-ad-
dicts with chronic delta infection. Recent acute hepatit is D, documented as H D V superinfect ion, was observed in
14 addicts (77%) and in 2 non-addicts (18%) (P < 0.02). At the time of evaluat ion for chronic liver disease, the
frequency of symptoms, the degree of biochemical disturbances and the histopathological severity were similar in
the two groups but the durat ion of HDV infection was probably shorter in drug addicts. HBV replicat ion, as indi-
cated by the presence of H B e A g and H B V - D N A in serum and HBcAg in liver, was more frequent in addicts. The
amount of H D A g in liver tissue was also greater in addicts (P < 0.005). Antib.odies against the human immuno-
deficiency virus were detected in all of the addicts (P < 0.001). Al though most patients remained asymptomat ic ,
significant histological worsening occurred in one half of the cases after a relatively short period of follow-up
(25.1 + 16.3 months) . The tendency to deter iora te in addicts (61% of cases) was greater than in non-addicts
(36%). These observat ions suggest that the prognosis of chronic H D V infection is part icularly poor in drug ad-
dicts in whom rapid deter iora t ion may be related to s imultaneous and inadequately control led replication of hep-
a totropic viruses.
Supported in part by grants 2017/84 from FI of the Seguridad Social and A R/85-41 from CIRIT of the Generalitat de Catalunya. J .C. is the recipient of a grant from Fundacio Catalana per a I'Estudi de Its Malaties del Fetgc. Corresponde.ce: J.M. Sanchez-Tapias, Liver Unit, Hospital Clinic. Villarroel 170. I)8036 Barcelona. Spain. Tel. 3231414, ext. 2208.
I) 168-8278/88/$03.50 © 1988 Elsevier Science Publishers B.V. (Biomedical Division)

170 M. BUTI et al.
Introduction
The hepatitis delta virus (HDV) is a defective pa-
thogen that may cause acute and chronic infection in man in close association with the hepatitis B virus
(HBV) [1]. Previous studies have demonstrated that the majority of patients with chronic H D V infection
have severe forms of liver disease with a greater ten- dency to progress than those with pure HBV infec-
tion [2,3].
The epidemiology of H D V infection is rather com- plex [1]. It is endemic in some areas but epidemics
and sporadic cases may also occur. In recent years, the use of contaminated needles has become a very important cause of HDV hepatitis among drug ad-
dicts in the Western world and epidemics have been
described [4-6], Indeed, addiction to i.v. drugs is currently the main route by which HDV infection is
spread in these countries [7]. Addicts to i.v. drugs are exposed to repeated bac-
terial, fungal and viral infections and may have an al- tered immune response that could modify the course
of HDV infection [8,9]. To ascertain whether paren- teral drug abuse may modify the course of chronic
hepatitis D, the clinical, pathological, virological and
evolutive features of this disease in addicts and non- addicts have been compared in this study.
Patients and Methods
Twenty-nine consecutive patients (24 men and 5
women) with HBsAg-positive, histologically proven
chronic liver disease and HDV superinfection were included in the study. None was alcoholic and all had
shown sustained hypertransaminasemia and had been positive for HBsAg for at least 6 months and
their anti-HD antibody titer was 1:1000 or higher. Sixteen patients came to hospital early in the course of an acute hepatitis attack with jaundice, amino-
transferase serum levels higher than ten times the normal values, a lack of anti-HBc IgM and the pres-
sence of markers of H D V in the serum ( H D A g in ten cases and anti-HD antibody in six), which was fol- lowed by persistently disturbed liver function tests
that led to a diagnostic liver biopsy. The remaining 13 cases were referred for liver biopsy because they had shown long-lasting abnormahties of liver function tests and positivity for HBsAg.
After liver biopsy all patients were followed pro-
spectively at 2 -4-month intervals. A complete clini- cal examination, routine liver function tests, and de-
terminations of HBsAg, HBe antigen and antibody
and total anti-HD antibody were done at each visit. No patient received immunosuppressive or antiviral
therapy. A liver biopsy was repeated after 1-5 years of follow-u p.
HBsAg, HBeAg, anti-HBe and total anti-HD anti- body were examined by radioimmunoassay with commercial reagents (Ausria II, HBe and Anti-Del-
ta, Abbot t Labs, U.S.A_). Serum H D A g , anti-HBc
lgM and anti-HIV antibodies were investigated by
enzyme immunoanalysis with commercial kits (Del- tassay, Nochtech, Ireland; Corezyme and Anti-
HTLV3, Abbot t Labs, U_S.A., respectively) and
anti-HIV antibodies were confirmed by western blot analysis. Serum H B V - D N A was sought by a spot hy-
bridization technique with an estimated detection limit of 0.3 pg D N A [10].
Percutaneous liver biopsies were obtained with a
Tru-cut needle. Liver sections were examined after
staining with Masson's trichrome and hematoxylin/ eosin. The pathological diagnosis was done accord-
ing to international criteria [11] and the index of his-
tological activity was determined according to Kno- dell et al. [12]. HBcAg and H D A g were sought in 5,u thick liver sections fixed in formalin and embedded in
paraffin. Proteolytic digestion was not performed
and each batch included appropriate positive and negative controls. HD antigen was investigated by indirect immunoperoxidase, using as primary anti-
body a high dilution (1:5000) of the lgG fraction puri-
fied from a human serum with high anti-delta but low anti-HBc titer and free of rheumatoid factor and or- gan non-specific autoantibodies [10,13]. An estima-
tion of the amount of H D A g present in liver was
made by grading from 0 to 4+ the number of positive nuclei observed in the whole section. HBcAg was in- vestigated by a peroxidase-antiperoxidase proce- dure, with commercial rabbit anti-HBc (Dako Labs,

CHRONIC HEPATITIS D IN ADDICTS AND NON-ADDICTS 171
U . S . A . ) .
C o m p a r i s o n s we re m a d e us ing the c h i - s q u a r e tes t
wi th Y a t e s ' c o r r e c t i o n and the s t a n d a r d t test .
R e s u l t s
Data at diagnosis
E i g h t e e n p a t i e n t s w e r e a d d i c t e d to i n t r a v e n o u s
drugs and 11 we re not . A r e c e n t e p i s o d e of acu te
hepa t i t i s occu r r i ng wi th in the p r e v i o u s 7 - 1 2 m o n t h s
and wi th the se ro log ic f e a t u r e s of H D V s upe r i n f ec -
t ion was d o c u m e n t e d in 14 add ic t s a n d in two n o n - a d -
dicts ( P < 0.02). T w o a d d i t i o n a l add ic t s and five n o n -
addic ts r e p o r t e d a h i s to ry of acu te hepa t i t i s . T h e r e
were no d i f f e r ences in age or sex b e t w e e n these two
g roups ( T a b l e 1).
W h e n the init ial l iver b iopsy was p e r f o r m e d , the
sever i ty of the u n d e r l y i n g l iver d i sease in add ic t s and
non -add i c t s was s imi la r , as assessed by c o m p a r i s o n of
the f r e q u e n c y of s y m p t o m s , d e g r e e of b i o c h e m i c a l
d i s t u r b a n c e s and h i s to log ica l diagnosis_ T h e in tens i ty
of por ta l i n f l a m m a t i o n , the s eve r i t y of p e r i p o r t a l and
TABLE 1
CLINICAL, BIOCHEMICAL DATA AT DIAGNOSIS
AND HISTOLOGICAL
Addicts Non- P (n = 18) addicts value
01 = 11)
Age (yrs) 21 + 3 25 + 12 n.s. Sex (M/F) 17/1 7/4 n.s. Recent acute hepatitis 14 2 <0.02 Acute hepatitis in the past 2 5 n.s. Jaundice 3 1 n.s. ALAT (IU/I) ~' 156 + 86 107 + 72 n.s. y-Globulin (g/I) 20.7 + 6.9 17.6 + 4.9 n.s.
Chronic persistent hepatitis 3 1 n.s. Chronic active hepatitis 12 9 n.s. Liver cirrhosis 3 1 n.s.
lndex of histological activity 13.1 +4.5 12.6+3.2 n.s. Portal inflammation 4.1 + 1.7 3.7 + 0.7 n.s. Periportallesions 3.1 + 1.2 4.0 +__ 1.7 n.s. Lobula~changes 3.0 + 0.8 2.7 + 1.1 n.s. Liver fibrosis 2.7 + 0.8 2.0 + 1.4 n.s.
p a r e n c h y m a l les ions and t he d e g r e e of l iver f ibros is
as well as t h e K n o d e l l ' s i ndex of h i s to logica l ac t iv i ty
were also s imi la r ( T a b l e 1)_
E l e v e n add ic t s ( 6 1 % ) but on ly o n e n o n - a d d i c t
( 9 % ) were H B e A g - s e r o p o s i t i v e ( P < 0.02). A n t i -
H B e a n t i b o d i e s we re d e t e c t e d in six add ic t s ( 3 3 % )
and in n ine n o n - a d d i c t s ( 8 2 % ) ( P < 0.02) . H B e A g
and a n t i - H B e were nega t i ve in o n e p a t i e n t f r o m e a c h
g roup . I gM a n t i - H B c a n t i b o d i e s a n d s e r u m H D A g
were nega t ive in all cases. H B V - D N A was d e t e c t e d
in s e r u m in e igh t add ic t s and in two n o n - a d d i c t s .
A n t i - H I V a n t i b o d i e s w e r e pos i t ive in all t h e add ic t s
bu t were nega t i ve in t he n o n - a d d i c t s ( P < 0 .001)
(Tab le 2).
H D A g was f o u n d in l iver t i ssue in 15 add ic t s ( 8 3 % )
and in 10 n o n - a d d i c t s ( 9 0 % ) bu t t he a m o u n t of
H D A g p r e s e n t in l iver was g r e a t e r in add ic t s ( P <
TABLE 2
VIROLOGICAL DATA AT DIAGNOSIS
Addicts Non- P (n = 18) addicts value
01 = 11)
Serum HBeAg+ 11 1 <0.02 anti-HBe+ 6 9 <0.02 negative HBe markers 1 I n.s. HBV-DNA+ 8 2 n.s. anti-HIV+ 18 0 <0.001
Liver HDAg+ alone 9 7 n.s. HBcAg+ alone 2 0 n.s. HDAg and HBcAg+ 6 2 n.s. HDAg and HBcAg- 1 I n.s.
Amount of HDAg in liver tissue 4+ 10 1 3+ 4 l 2+ I 3 I+ 0 5 absent 3 I
Amount of HBcAg in liver tissue 4+ 6 0 3+ 1 1 2+ 1 1 1+ 0 0 absent 10 9
<0.005
n.d.
Normal value up to 20 IU/I. n.d. = not done.

172 M. BUTI et al.
0.005) (Table 2). HBcAg was detected in eight ad-
dicts (44%) and only two non-addicts (27%)_ The amount of this antigen present in liver seemed great-
er in addicts but statistical analysis was not possible because the number of non-addicts with detectable HBcAg in liver was too low. Other details on the
presence of viral antigens in liver tissue are given in Table 2.
Follow-up Two patients, one from each group, died during
follow-up from complications of advanced liver dis-
ease. They were jaundiced and had cirrhosis at the
time of diagnosis. The HBc and HD antigens were still present in liver tissue at necropsy.
Twenty-seven patients remained asymptomatic or presented minor symptoms such as increased fatigue
or vague discomfort in the upper right quadrant_ Complete recovery was observed in only one case.
He was a non-addict with severe chronic active hep- atitis with bridging necrosis and abundant H D A g ex-
pression in whom liver function tests became normal,
HBsAg disappeared and anti-HBs developed after 4 years of follow-up. At this time, his liver biopsy
showed minimal, non-specific changes and immuno- - staining for viral antigens was negative.
A second liver biopsy was taken in 17 addicts and in nine non-addicts with persistently abnormal liver
function tests_ The time interval between biopsies was 20.6 + 7.3 (12-39) and 30.3 + 12.3 (14-52)
months, respectively. Among addicts, worsening of liver lesions was observed in three patients with
chronic persistent hepatitis who progressed to
chronic active hepatitis (one case) or to cirrhosis (two cases) and in eight patients with chronic active hep-
atitis who developed cirrhosis. Among non-addicts, progression to cirrhosis was noted in four patients
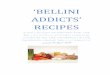
with previous chromc active hepatitis. Overall, histo- logical worsening was noted in 11 addicts (61%) and
in four non-addicts (36%), but this difference was not statistically significant (Fig. 1). The time elapsed be-
tween biopsies in patients who worsened was 20.4 + 6.1 months in addicts and 25.7 + 7.7 months in non-
addicts. Among patients with chronic hepatitis in the first biopsy, cirrhosis was documented in 10/15 ad-
ADDICTS
FIRST SECOND BIOPSY BIOPSY
Fig. I. Schematic representation
NON-ADDICTS !
J FIRST SECOND BIOPSY BIOPSY
of individual diagnosis in re- peated liver biopsies from addicts and non-addicts. (NL = nor- mal liver; CPH = chronic persistent hepatitis; CAH = chronic
active hepatitis: HC = hepatic cirrhosis.)
dicts (67%) and in 4/10 non-addicts (40%) after 20.1
+ 6.3 and 20.7 + 8 months of follow-up, respectively. During the period of follow-up, no patient had op-
portunistic infections, lymphadenopathy, fever, loss
of weight or other manifestations of AIDS or AIDS- related complex.
Discussion
Previous studies on the natural history of chronic HDV infection have shown that this condition is
usually associated with severe and rapidly progres- sive liver disease [2,3,14]. These observations have
been confirmed in the present study in which 75% of
the cases had chronic active hepatitis in the first liver biopsy and more than one half showed progression to
cirrhosis after a relatively short period of time. Inter-
estingly, this important 'histological deterioration oc- curred without symptoms of liver disease and only
two patients had major manifestations of hepatic de- compensation.
Chronic H D V infection is very common among
parenteral drug abusers [14-17] but studies to delin- eate the characteristics of the infection in these sub- jects in comparison with sporadic cases have not been
performed. The present study suggests that several
aspects of chronic H D V infection may be different in these two populations.
The majority of patients in this series reported a history of acute hepatitis, as in other studies [2,
13,14,17]. In 14 addicts but in only two non-addicts the acute episode was recent and had the serological

CHRONIC HEPATITIS D IN ADDICTS AND NON-ADDICTS 173
features of H D V super infec t ion in chronic H B V car-
riers [18], indicat ing that the dura t ion of H D V infec-
tion at the t ime of the first l iver biopsy was shor te r in
addicts. Since the degree of l iver d a m a g e was similar
in the two groups , it may be sugges ted that H D V - i n -
duced chronic l iver disease tends to progress m o r e
rapidly in addicts than in non-addic ts . The observa-
tions made at fo l low-up suppor t this p resump-
tion because r epea t ed biopsies d e m o n s t r a t e d that the
rate of his tological worsen ing was a lmost twice as
great in addicts. Progress ion to cirrhosts was also
more f r equen t in addicts. H o w e v e r , since these dif-
ferences did not ach ieve statistical s ignif icance, fur-
ther studies including m o r e pat ients are r equ i r ed to
e lucidate this ques t ion .
The reasons why chronic H D V infect ion-asso-
ciated hepat ic disease seems to progress m o r e rapidly
in drug addicts are not known. A c c e l e r a t e d worsen-
ing of l iver lesions might be re la ted to s imul t aneous
repl ica t ion of H B V , which was m o r e f r equen t in ad-
dicts, as indica ted by the h igher p r o p o r t i o n of pa-
tients with H B e A g and H B V - D N A in se rum and
H B c A g in liver. In ad.dition, the n u m b e r of hepa to -
cytes displaying H D A g was g rea te r in drug addicts ,
suggest ing that H D V repl ica t ion is more act ive in
these subjects_ A l t h o u g h the role of H D V repl ica t ion
in the pa thogenes i s of del ta hepat i t i s is u n k n o w n , it is
possible that the p resence of very act ive H D V repli-
cat ion might acce lera te the progress ion of the disease
because a great n u m b e r of hepa tocy tes would be sus-
cept ib le to d a m a g e e i ther by a direct cy topa th ic ef-
fect of H D V on infected l iver cells [19] or by the ac-
tion of the host ' s i m m u n e mechan i sms against hep-
a tocytes suppor t ing H D V repl ica t ion , as recent ly
sugges ted [20]. W h e t h e r a symptoma t i c H I V infec-
tton, which was present in all the drug addicts in-
c luded in this s tudy, plays some role in this comp lex
s i tuat ion is current ly unknown. Final ly, infect ion by
n o n - A , non-B hepat i t is virus or viruses, which is very
c o m m o n a m o n g drug addicts [8], might also account
for progress ive liver damage . W h a t e v e r the cause,
the acce le ra ted progress ion of chronic H D V infec-
t ion-associa ted l iver disease seen in drug addicts
seems re la ted to uncon t ro l l ed repl ica t ion of hepa to-
tropic viruses and suggests that early ant iviral thera-
py is par t icular ly necessary in these patients_
References
1 Rizzetto M. The delta agent. Hepatology 1983; 3: 729-737. 2 Rizzetto M, Verme G, Recchia S, et al. Chronic hepatitis in
carriers of hepatitis B surface antigen with intrahepatic ex- pression of the delta antigen. Ann Intern Med 1983; 98: 437-441.
3 Fattovich G, Boscaro S, Noventa F, et al. Influence of hep- atitis Delta virus infection on progression to cirrhosis in chronic hepatitis B. J Infect Dis 1987; 155: 931-935.
4 Shattock AG, Kelly MG, Fielding J. Arthurs Y. Epidemic hepatitis B with delta antigenaemia among Dublin drug- abusers. IrJ Med Sci 1982; 151: 334-338.
5 Caredda F, Rossi E, Monforte AD. Farci P, Lavarini C. An outbreak of delta agent among a group of drug addicts and their close contacts. J Infect Dis 1984; 149: 286-287.
6 Lettau LA, McCarthy JG. Smith MH, et al. Outbreak of se- vere hepatitis due to delta and hepatitis B viruses in paten- feral drug abusers and their contacts. N Engl J Med 1987; 317: 1256-1262.
7 Raimondo G, Smedile A, Gallo L, Balbo A, Ponzeno A, Rizzetto M. Multicentre study of prevalence of HBV-asso- ciated delta infection and liver disease in drug-addicts. Lan- cet 1982; i: 2'49-251.
8 Weller IVD, Cohn D, Sierralta A. Clinical, biochemical,
serological, histological and ultrastructural features of liver disease in drug abusers. Gut 1984; 25: 417-423.
9 Fauci AS. Acquired immurlodeficiency syndrome: epide- miologic, clinical, immunologic and therapeutic consider- ations. Ann Intern Med 1984; 100: 92-106.
10 Genescfi J, Jardf R, But M, et al. Hepatitis B virus repli- cation in acute hepa'titis B, acute hepatitis B virus-hepatitis delta virus coinfection and acute hepatitis delta superinfec- tion. Hepatology 1987; 7: 569-572.
11 Diseases of the liver and biliary tract: standardization of no- menclature, diagnostic criteria and diagnostic methodolo- gy. DHEW publication. No. (NIH) 76-725. Sponsored by the International Association for the Study of the Liver. Proceedings N22. Washington, DC: U.S. Government Printing Office, 1976; 212.
12 Knodell RG, Ishak KG, Black WC, et al. Formulation and application of a numerical scoring system for assessing his- tological activity in asymptomatic chronic active hepatitis. Hepatology 1981 : 1 : 431-435.
13 S,Snchez-Tapias JM, Vilar JH, Costa J, et al. Natural histo- ry of chronic persistent hepatitis B. Relationship between hepatitis B virus replication and the course of the disease. J Hepatol 1984; 1: 15-27.
14 Govindarajan S, De Cok KV, Redeker AG. Natural course of delta superinfection in chronic hepatitis B virus infected

174 M. BUTI et al.
patients: histopathologic study with multiple liver biopsies. Hepatology 1986; 6: 640-644.
15 Ponzeno A, Seer LB, Buskell-Balles Z, et al. Hepatitis B markers in Unites States drug addicts with special emphasis on the Delta hepatitis virus. Hepatology 1984; 4: 1111-1115
16 Novick DM, Farci P. Karayiannis P, et al. Hepatitis D virus antibody in HBsAg positive and HBsAg negative substance abusers v,,ith chronic liver disease. J Med Virol 1985; 15: 351-356.
17 Colombo lVl, C~m'tbiere R, Rumi MG, et al. Long term delta superinfection in hepatitis B surface antigen carriers and its
relationship to the course of chronic hepatitis. Gastroenter- ology 1983; 85: 235-239.
18 Buti M. Esteban R, Jardi R, Esteban Jl, Guardia JJ. Sero- logical diagnosis of acute deha hepatitis..I Med Virol 1986: 18: 81-85.
19 Lefkowitch JH, Goldstein H, Yatto R, Gerber MA. Cyto- pathic liver injury in acute delta virus hepatitis. Gastro- enterology 1987; 92: 1262-1266.
20 Negro F, Baldi M, Bonino F, et al. Chronic HDV (hepatitis delta virus) hepatitis. Intrahepatic expression of delta anti- gen, histologic activity and outcome of liver disease. J Hep- atol 1988; 6: 8-14.