Embed Size (px)
Citation preview
Philip Barter
The Heart Research Institute
Sydney, Australia
Cholesteryl ester transfer protein
inhibitors - what have we learnt?

Philip Barter Disclosures
Received honorariums for lectures, consultancies or
membership of advisory boards from:
AstraZeneca, CSL, MSD, Novartis, Pfizer, Roche,
Sanofi Aventis

QUESTION
Why continue the development of
CETP inhibitors after the failures of
torcetrapib and dalcetrapib?

What do we know about the relationship
between CETP and atherosclerosis?

Rabbits have high level of activity of CETP
Rabbits naturally highly susceptible to the
development of atherosclerosis
Inhibition of CETP in rabbits decreases
atherosclerosis in all models, including genetic
manipulation to inhibit CETP, use of an anti-
CETP vaccine or by administration of small
molecule CETP inhibitors
CETP and Atherosclerosis in Rabbits
Sugano et al. J Biol Chem.1998;273:5033. Rittershaus et al. ATVB. 2000;20:2106.
Okamoto et al. Nature. 2000;406:203. Morehouse et al. J Lipid Res. 2007;48:1263.

Two very large meta-analyses and one large
study of 18,245 initially healthy American
women all concluded that CETP gene
polymorphisms associated with lower CETP
mass and/or lower CETP activity had higher
levels of HDL-C, lower levels of LDL-C and a
significantly reduced coronary risk.
CETP Polymorphisms and Cardiovascular
Risk in Humans
Thompson et al JAMA2008;299:2777-278
Voight et al Lancet, online ahead of publication, 17 May 2012
Ridker et al. Circ Cardiovasc Genet 2009; 2: 26

So, given the evidence that:
(i) Inhibiting CETP in rabbits inhibits
atherosclerosis
(ii) Genetic variants of CETP in humans are
accompanied by higher HDL-C, lower LDL-C and
reduced CV risk and
(iii) Inhibition of CETP in humans increases HDL-C
and, in some cases, decreases LDL-C
There is a strong case for developing CETP
inhibitors as agents to reduce cardiovascular risk
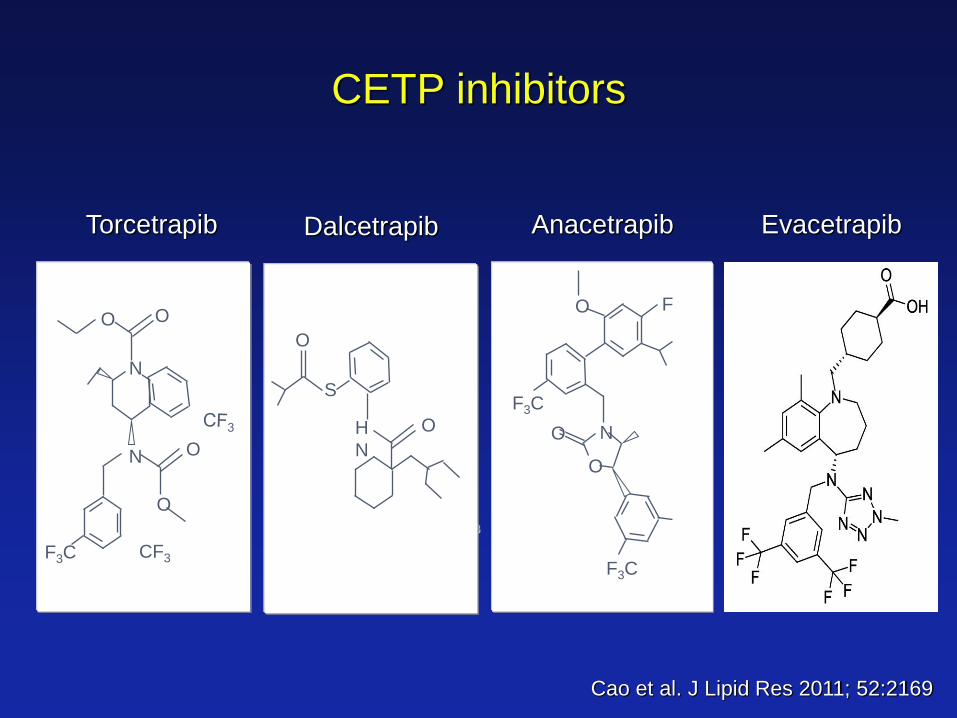
Torcetrapib
CF3
F3C
N O
O
N
O O
CF3
Dalcetrapib
S
O
O
H
N
Anacetrapib
O
F3C
O
N
O
F3C
F
CETP inhibitors
Evacetrapib
Cao et al. J Lipid Res 2011; 52:2169

Torcetrapib
Torcetrapib increased HDL-C by more
than 60% and reduced LDL-C by more
than 20% over and above the changes
achieved by using high doses of statins.
Barter et al, NEJM 2007;357:2109
Inhibiting CETP with torcetrapib in
humans did not reduce atherosclerosis in
three imaging trials and in a large-scale
clinical end-point trial (ILLUMINATE)
increased CV events and both CV and
non-CV mortality
But

What was the reason for the adverse outcome with
torcetrapib in the ILLUMINATE trial?
Possible explanations
Inhibiting CETP is pro-atherogenic
Inhibiting CETP generates dysfunctional HDL
Torcetrapib had adverse off-target effects unrelated to CETP
inhibition
What was the reason for the adverse outcome with
torcetrapib in the ILLUMINATE trial?
Possible explanations
Inhibiting CETP is pro-atherogenic
Inhibiting CETP generates dysfunctional HDL
Torcetrapib had adverse off-target effects unrelated to CETP
inhibition

Effects of torcetrapib on HDL function
HDLs isolated from patients treated with anacetrapib
have an enhanced ability to promote the efflux of
cholesterol from macrophages.
Yvan-Charvet et al. ATVB 2007;27:1132

What was the reason for the adverse outcome with
torcetrapib in the ILLUMINATE trial?
Possible explanations
Inhibiting CETP is pro-atherogenic
Inhibiting CETP generates dysfunctional HDL
Torcetrapib had adverse off-target effects
unrelated to CETP inhibition

In patients receiving torcetrapib in the ILLUSTRATE, RADIANCE 1 & 2 and ILLUMINATE studies there was a significant: Increase in blood pressure Decrease in serum potassium Increase in serum bicarbonate Increase in serum sodium Increase in serum aldosterone
Off-target effects of torcetrapib
Barter et al, NEJM 2007;357:2109. Nissen et al. NEJM. 2007;356:1304.
Kastelein et al. NEJM, 2007; 356:16. Bots et al. Lancet. 2007; 370:153

Torcetrapib induced synthesis and secretion of both aldosterone and cortisol from human adrenal cells in tissue culture. Torcetrapib reduced expression of endothelial nitric oxide synthase mRNA and protein, reduces nitric oxide release, increases expression of endothelin-1 and induces endothelial dysfunction animals independent of CETP inhibition Other CETP inhibitors do not have these off-target effects
Forrest et al. Br J Pharmacol. 2008;154:1465-1473. Hu et al. Endocrinology 2009;150:2211-
2219. Capponi et al. Circulation 2008;118:S:452.
Connelly et al. J Cardiovasc Pharmacol 2010; 55:459.
Simic et al. Eur Heart J. 2012 (in press)
Off-target effects of torcetrapib
unrelated to CETP inhibition

So, off-target adverse effects of torcetrapib
(unrelated to CETP inhibition) MAY have
been responsible for the adverse outcome in
the ILLUMINATE trial
Dalcetrapib
Inhibits CETP activity by about 50%
Increases HDL-C by about 30%
Minimal effect on LDL-C levels
Luscher et al. European Heart J, 2012;33:857
Effects of dalcetrapib in humans

15,600 patients 4-12 weeks
after an index ACS event
dal-OUTCOMES Trial
Dalcetrapib 600 mg Statin therapy to optimal LDL-C level
Placebo
Primary End Point
CHD death, non-fatal MI, atherothrombotic stroke, unstable angina requiring hospitalization or resuscitated cardiac arrest
2.5-year follow-up
Schwartz et al. Am Heart J. 2009;158:896-901.

It was announced in early May 2012 that the dal-OUTCOMES
trial had been terminated on the basis of futility.
dal-OUTCOMES Trial
http://www.roche.com/media_releases/med-cor-2012-05-07.htm

Two possible explanations are:
(i) The increase in HDL-C concentration induced
by dalcetrapib was not accompanied by an
enhancement of the protective functions of
HDL or
(ii) that the inverse relationship between HDL-C
concentration and cardiovascular risk observed
in population studies is an epiphenomenon
rather than being reflective of an ability of HDL
to protect against cardiovascular disease.
Why did dalcetrapib fail to reduce CV events?

It is also possible that inhibiting CETP with a
relatively weak inhibitor such as dalcetrapib is
not sufficient to have an impact on CV events.
In addition, it is possible that CETP inhibition is
not effective in patients treated soon after an
acute coronary event as was the case with dal-
OUTCOMES.
Why did dalcetrapib fail to reduce CV events?
In my view, there is a compelling case for
conducting new cardiovascular clinical outcome
trials with agents such as anacetrapib and
evacetrapib that do not have the off-target
adverse effects of torcetrapib and are much
more effective than dalcetrapib as inhibitors of
CETP and as HDL-raising and LDL-lowering
agents.

Anacetrapib
Anacetrapib is a potent CETP inhibitor that
has none of the off-target effects observed
with torcetrapib
Forrest et al. Br J Pharmacol. 2008;154:1465-1473. Hu et al. Endocrinology 2009;150:2211-2219
.
Effects of anacetrapib on HDL function
HDLs isolated from patients treated with
anacetrapib have an enhanced ability to
promote the efflux of cholesterol from
macrophages.
Yvan-Charvet L et al ATVB 2010;30:1430-1438

1620 patients with CHD or
CHD risk equivalents
DEFINE trial Determining the EFficacy and Tolerability of CETP
INhibition with AnacEtrapib
Anacetrapib 100 mg Statin therapy to achieve LDL-C <100 mg/dL
Placebo
Primary End Point
Lipid efficacy and the safety
76 week follow-up
Cannon et al. NEJM. 2010; 363:2406-2415 Forrest et al. Br J Pharmacol. 2008;154:1465-1473. Hu et al. Endocrinology 2009;150:2211-2219.

DEFINE trial
ApoA-I (mg/dL)
Study Week
O 24 76 0
40
80
120
160
200
240 Anacetrapib
Placebo
Cannon et al. NEJM. 2010; 363:2406
Study Week
O 24 76 0
20
40
60
80
100
120
Anacetrapib
Placebo
HDL-C (mg/dL)

DEFINE trial
LDL-C
Study Week
0 24 76 0
20
40
60
80
100
Anacetrapib
Placebo
Cannon et al. NEJM. 2010; 363:2406
mg
/dL

DEFINE trial
Study Week
O 24 76 0
20
40
60
80
100
120
Anacetrapib
Placebo
Cannon et al. NEJM. 2010; 363:2406
Non-HDL-C (mg/dL) ApoB (mg/ml)
Study Week
20
40
60
80
100
Anacetrapib
Placebo
O 24 76 0

DEFINE trial
Study Week
0 24 76 0
10
20
30
40
50
Anacetrapib
Placebo
Cannon et al. NEJM. 2010; 363:2406
Lp(a) n
mo
l/L

Anacetrapib had no effect on levels of aldosterone,
sodium, potassium or bicarbonate and did not raise
blood pressure
DEFINE trial
Cannon et al. NEJM. 2010; 363:2406

Anacetrapib had no effect on BP
SBP
DBP
mm
Hg
mm
Hg
Week
Anacetrapib
Placebo
200
160
120
80
40
0
120
80
40
0 0 6 12 18 24 30 38 46 54 62 70 76
0 6 12 18 24 30 38 46 54 62 70 76
Cannon et al. NEJM. 2010; 363:2406
The event distribution in DEFINE indicated a 94%
probability that treatment with anacetrapib does not
result in a torcetrapib type increase in CV events
DEFINE trial
Cannon et al. NEJM. 2010; 363:2406

ILLUMINATE Trial 2007 (torcetrapib)
DEFINE Trial 2010 (anacetrapib)
0.5 1.0 1.5
CVD/MI/S/UA
Revascularization
0.75 1.25
CETP-I Better CETP-I worse
DEFINE trial N = 1,623 - Anacetrapib
ILLUMINATE Trial N=15,067 - Torcetrapib
CVD/MI/S/UA
Revascularization
0.25
Cannon et al. NEJM. 2010; 363:2406-2415
Barter et al, NEJM 2007;357:2109-2122
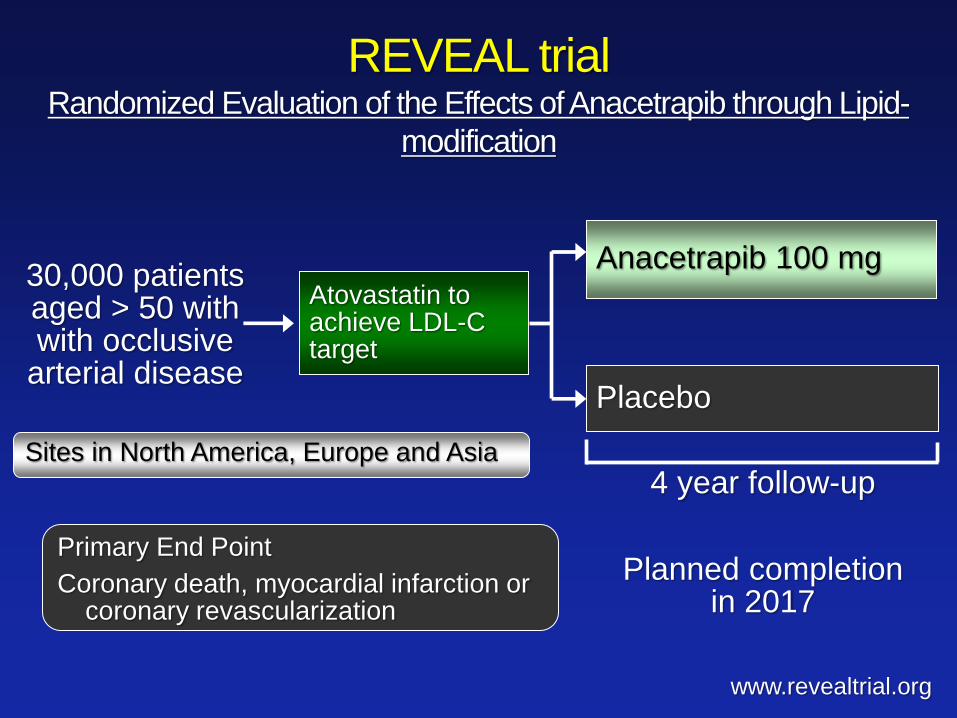
30,000 patients aged > 50 with with occlusive
arterial disease
REVEAL trial Randomized Evaluation of the Effects of Anacetrapib through Lipid-
modification
Anacetrapib 100 mg Atovastatin to achieve LDL-C target
Placebo
Primary End Point
Coronary death, myocardial infarction or coronary revascularization
4 year follow-up
www.revealtrial.org
Sites in North America, Europe and Asia
Planned completion in 2017
Evacetrapib

120%
100%
80%
60%
40%
20%
0%
Percent Change in HDL-C: Evacetrapib Plus statin
7.3%
86.6%* 79.9%*
94.0%*
1.4% 5.5%
Simvastatin 40 mg Atorvavastatin 20 mg Rosavastatin 10 mg
Statin plus placebo Statin plus evacetrapib 100 mg
* P<0.001 compared with placebo Nicholls et al. JAMA. 2011;306:2099

0%
20%
40%
60%
Percent Change in LDL-C: Evacetrapib Plus statin
-34.9%
-46.1%* -47.6%* -52.3%*
-33.6%
-38.8%
Simvastatin 40 mg Atorvavastatin 20 mg Rosavastatin 10 mg
Statin plus placebo Statin plus evacetrapib 100 mg
* P<0.001 compared with placebo Nicholls et al. JAMA. 2011;306:2099

• There is still a compelling case for further
testing the hypothesis that inhibiting CETP
will be anti-atherogenic in humans when
using inhibitors that have none of the
torcetrapib-like adverse effects and which
have substantially greater HDL-raising and
LDL-lowering than was achieved by
dalcetrapib.
• The hypothesis is currently being tested in
large CV clinical endpoint trials.






![Surface Properties of Cholesteryl Ester Liquid Crystalmint.uthm.edu.my/images/DOCUMENTS/PMiNT_Paper_3.pdf · literature [8]. However, the chemical compounds of the cholesteryl ester](https://img.dokumen.tips/doc/110x75/5f90eb74f0ec4316ef0bf1d2/surface-properties-of-cholesteryl-ester-liquid-literature-8-however-the-chemical.jpg)






















