Embed Size (px)
Citation preview

Childhood Chronic Conditions, Changing Epidemiology and Implications for Care
James M. Perrin, MD, FAAPImmediate Past President, American Academy of PediatricsProfessor of Pediatrics, Harvard Medical SchoolJohn C. Robinson Chair, MassGeneral Hospital for ChildrenCongreso Argentino de Pediatria, Septiembre 2015

Dr. Perrin has no financial or other conflicts of interest to disclose
2
Presentation Overview Childhood chronic
conditions – Huge growth in rates
Childhood poverty– Effect on health and wellbeing
Transforming health care to address chronic care
3
EpidemicsOf Childhood ChronicHealth Conditions
Children with Special Health Care Needs
Children with special health care needs are those who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally - Maternal and Child Health Bureau
Chronic condition ≠ Disability

Measuring Prevalence Rates Limitation of activity due to health condition – 7-8%
Diagnostic codes from billing data – 11-12%
Children with special health care needs MCHB definition –15-18%
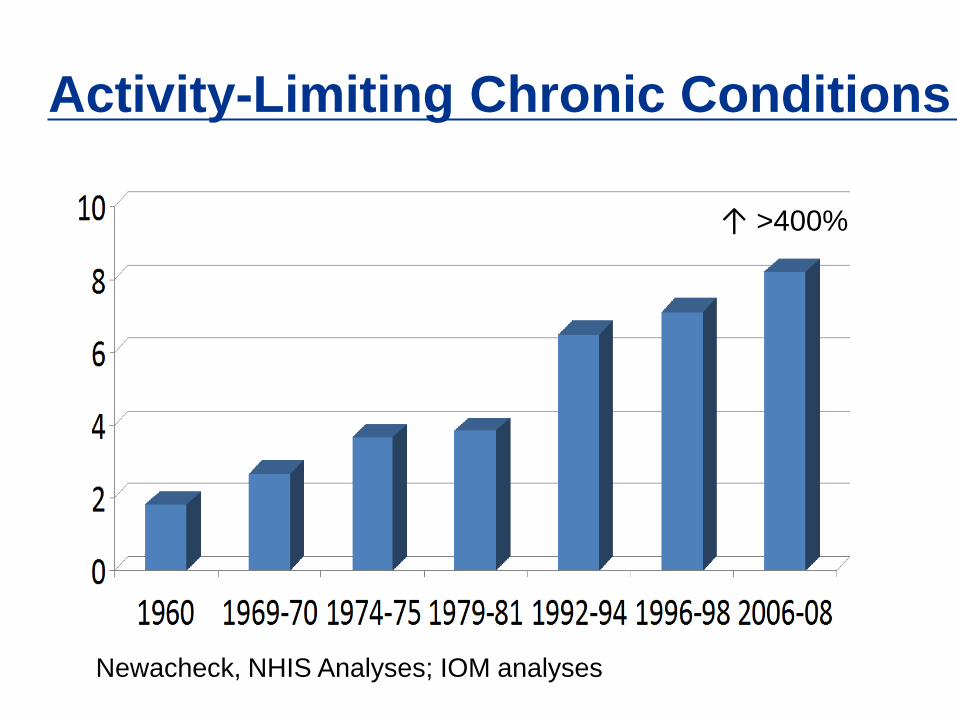
Activity-Limiting Chronic Conditions
Newacheck, NHIS Analyses; IOM analyses
>400%↑

All Chronic Conditions
0
5
10
15
20
25
30
1988-1994 1994-2000 2000-2006
Initial PrevEnd Prev
↑ 236%
Cohorts of 2-8 year olds followed for six years; initial and end chronic condition prevalence; Van Cleave, Gortmaker, Perrin, JAMA, 2010

Chronic Conditions: Children and Adults
Adult conditions:– small number of common conditions
Child conditions:– large number of (mainly) rare conditions
Most conditions more common in males, especially before puberty
Most children survive, although developmental, physical, and psychological outcomes vary
Changing Patterns of Childhood Chronic Conditions
1960-1980: Improvements in survival led to increased rates of several chronic conditions– >80% survival in 1980; >95% survival today– Marginal impact of newer conditions VLBW, in utero toxins, AIDS
1980-now: New epidemics of common chronic conditions
Perrin, Bloom, Gortmaker, JAMA, 2007
Less Common Chronic Conditions
Cystic fibrosisSpina bifidaSickle cell anemiaHemophilia
22,500 (3:10,000)60,000 (7.5:10,000)37,500 (5:10,000)7,500 (1:10,000)
80,000,000 children/youth in US

New Epidemics: Mainly Among School-age Children and YouthObesityAsthmaADHDDepression/AnxietyAutism Spectrum
Disorder
13.4 million (16.4:100)*7.2 million (9:100)4.8 million (6.4:100)3.2 million (4:100) 1 million (<1:100)
*Population estimates, late 2000s80 million children/youth in US
Estimated Numbers for Argentina
ObesityAsthmaADHDDepression/anxietyAutism Spectrum
Disorder
1.8 million 1.0 million 640,000 430,000 133,000
13
Argentine population: 42.5 million31.8% <age 20 years
Grouping Childhood Chronic Health Conditions Low prevalence, (usually) high severity
– (~2million)– Substantial involvement of pediatric subspecialists in care– CF, spina bifida, leukemia, arthritis, diabetes …
Very complex, multisystem conditions – (<.4 million)
Common, high prevalence, wide spectrum of severity – (~6-8 million)– Asthma– Obesity– Mental health conditions (anxiety, depression, ADHD)– Developmental conditions (incl. autism spectrum disorders)

Long-term Implications/ Prevention Critical Rapid rise in young
adult disability from:– Cardiovascular disease
(overweight and diabetes)– Pulmonary disease– Mental and developmental
conditions
Major increases in: – Health care costs– Unemployment– Reliance on disability
programs

Implications for Populations and Health Most adult chronic health
conditions have major antecedents in childhood
Children living in unhealthy environments have much higher rates of poor health as adults
A healthy and productive workforce requires healthy children prevented from toxic stress and poor health conditions
Why Are Childhood Chronic ConditionsMore Prevalent?
– Biomedical/surgical advances, coupled with
– Regressive social and environmental changes
Genes and Environment Genetics
– Many conditions have clear genetic disposition, usually requiring environmental triggers for manifestation
– But, genetic drift alone cannot explain these rates
Changing physical and toxic environments and the cleanliness hypothesis– Growth of autoimmune disorders in all age groups– Increasing evidence of toxins affecting fetus
Children’s social environments

Low Birthweight and Poverty Do Not Explain US Growth Increasing rates of very low
birth weight and survival
Poverty– Increases rates of most
conditions– Increases severity of many
conditions– Affects response to treatment
Little evidence for changes in US poverty rates

Children’s Social Environments have ChangedParentingMedia
– including phones
Physical activity and indoor timeDiet
Parental Stress
Changing employment patterns
Changing geography, esp. in urban areas
Migration patterns
Children have less time and attention from consistent adults

Television and Media Affect Child Health
75% of children have TV in room– 35% of children < 2 years old
Advertising fast, high-calorie food Children indoor, sedentary Fast-paced, rapid-cycling
visual, auditory stimulation Replaces tasks requiring more
attention– Reading, model-building
Violence presented as harmless; gratification immediate
Tracks from preschool to adolescence
Impact of Television
Fattening children in front of TV (Gortmaker, Dietz)
Dose-related effects of TV on initiation of smoking among 10-14 year olds (Gidwani et al.)

Children are Less Physically Active Limited recreation, parks,
playgrounds, sports programs
Dangerous neighborhoods– Effects on social
interactions
Decreased school physical education
Lower rates of walking, bicycling
More Time Indoors
More exposure to indoor pollutants– Smoke– Mites, roaches
Less time socializing with peers

Diet Increased use of fast food and take out
restaurants Increased portion size Nutrients from fortified drinks – sodas in schools Clear association with overweight and diabetes Association of asthma with
– Low levels of omega-3 fatty acids and antioxidant vitamins
– High levels of trans fatty acids
Sugar and ADHD (??)

Poverty and Child Health
28
Household Income in 2012
1 in 10 children live in homes with incomes less than $12,000 More than 1 in 5 with incomes
less than $24,000 Close to half with incomes under
$48,000
Federal Poverty Level: $24,250 for family of four (2015)
Health Consequences of Poverty Increased infant mortality Low birth weight, subsequent
problems Chronic diseases: asthma,
obesity, MH, development Food insecurity, poorer
nutrition and growth Less access to quality health
care Increased accidental injury,
mortality Higher exposure to toxic stress
Moore KA et al. Children in poverty: trends, consequences, and policy options. 2009. Child Trends Research Brief
Poverty and Well-Being Poorer educational outcomes
– Low academic achievement, higher HS dropouts
Less positive social and emotional development
More problem behaviors– Early unprotected sex with
increased teen pregnancy– Drug and alcohol abuse– Increased criminal behavior as
adolescents and adults
More likely to be poor adults

31
Transforming Care and the Pediatric Medical Home
Organizing Care forChronic Conditions

Conceptual model of how interventions can affect early child developmentEngle, Black, Behrman, Cabral de Mello, Gertler, Kapiriri, Martorell, Young, Lancet, 2007
Practice Transformation in Pediatrics New practice arrangements
– Team based community care– Population health
Making payment work to change communities– Moving from FFS to various bundled arrangements
and incentives for performance– Linking pediatrics with public/private reform activities
Harnessing new technologies to strengthen care– Beyond EHRs to iPhones and telemedicine
Leadership training in change33
Changing Technologies – Beyond Electronic Records Home/community monitoring via iPhone, other
web methods – e.g., followup for IBD, monitoring ASD progress
Text messaging, follow up– Newborn care (Text for Babies)– Immunization reminders– Behavior guidance
Out of office diagnostic, treatment technologies– E.g., iPhone otoscopy
34

Disruptive Innovations New clinical arrangements
– Pharmacy clinics and others– Convenience and cost
Web-based clinical care
Other telehealth efforts– Direct care – in office or home– Shared care – in office– Distributing knowledge to local providers (Project ECHO)
35
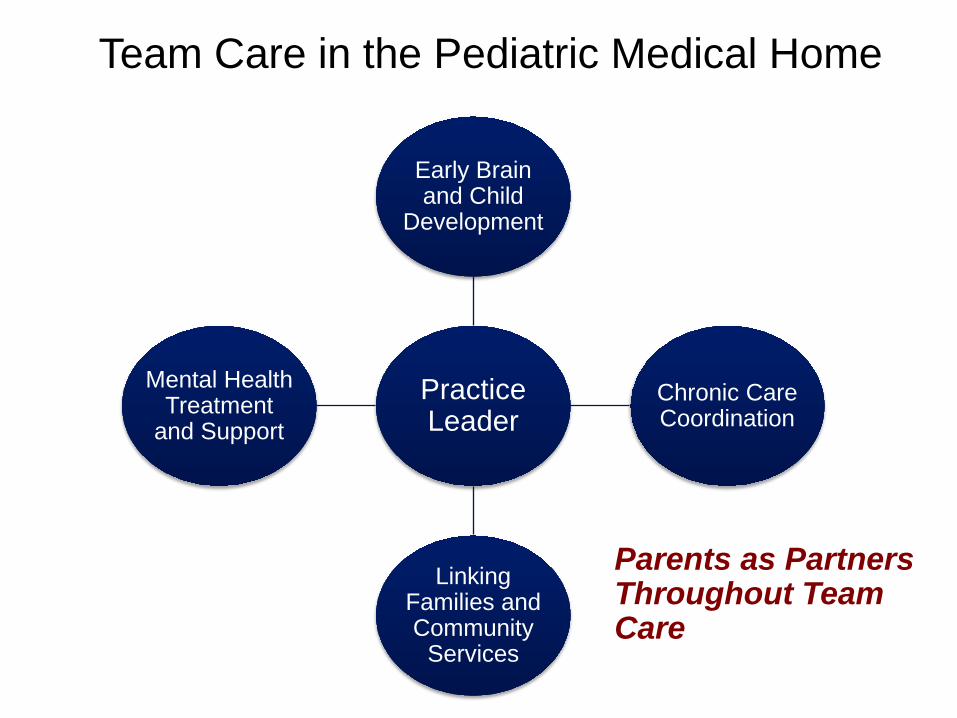
Practice Leader
Early Brain and Child
Development
Chronic Care Coordination
Linking Families and Community
Services
Mental Health Treatment
and Support
Team Care in the Pediatric Medical Home
Parents as Partners Throughout Team Care

Summary Alarming and growing rates of chronic health
conditions among children/youth
Poverty persists among children worldwide– Major impact on child health and development
Addressing prevention and community interventions will strengthen populations and countries’ economies
Transformation in health care– Team-based care– Addressing community needs and integration– Prevention and going beyond medicine to community health
37
Questions

![The challenge of transition in chronic respiratory diseases · with sex, pregnancy, work, and raising a family in the context of chronic ill health.[7] Respiratory conditions in childhood](https://img.dokumen.tips/doc/110x75/6062517502f8176669721179/the-challenge-of-transition-in-chronic-respiratory-with-sex-pregnancy-work-and.jpg)



























