Embed Size (px)
DESCRIPTION
Child Abuse. Naminder Sandhu & Dr. Bela Sztukowski September 1, 2011. Video: Infant beat to death by father - PowerPoint PPT Presentation
Citation preview
Child Abuse
Naminder Sandhu& Dr. Bela Sztukowski
September 1, 2011

Video: Infant beat to
death
by father
BATTLEFORD — A 25-year-old
Lloydminster man who “sn
apped” while
changing his infant so
n’s diaper, fa
tally
injuring the child, has received a priso
n
sentence of 5 1/2 years for
manslaughter.
APRIL 26, 2011
Toddler dies in hospital;
police to charge
Medicine Hat day home
worker
BY CALGARY HERALD, GLOBAL TV CALGARY
JULY 22, 2010
NEWS CANADABaby girl savagely beaten by woman before rescue CHRIS KITCHING, SUN MEDIA
FIRST POSTED: WEDNESDAY, SEPTEMBER 2,
2009

Emotional abuse 19%
Physical abuse31%
Sexual abuse10%
Neglect40%
Objectives
• Identify suspicious injury patterns – Consider ddx and mimics
• Review appropriate investigations• Explore management options• Know your medical and legal responsibilities
Epidemiology
Canadian Incidence Study of Reported Child abuse and Neglect, 1998
•22 investigations/1000 children (2.2%) •45% of cases confirmed by child welfare workers (9.9 cases/1000)
Who’s at risk?
Socioeconomic stressors
Parent stressors
Triggering situations
Child stressors
What and how to ask: the history
Think twice if….
1) Sounds crazy but explains injury2) Sounds reasonable but doesn’t explain injury• 30 degrees out and “she ran bare feet
onto the hot pavement”… but arches of feet also burned!
Consider child’s development!
“Those who can’t cruise don’t bruise”
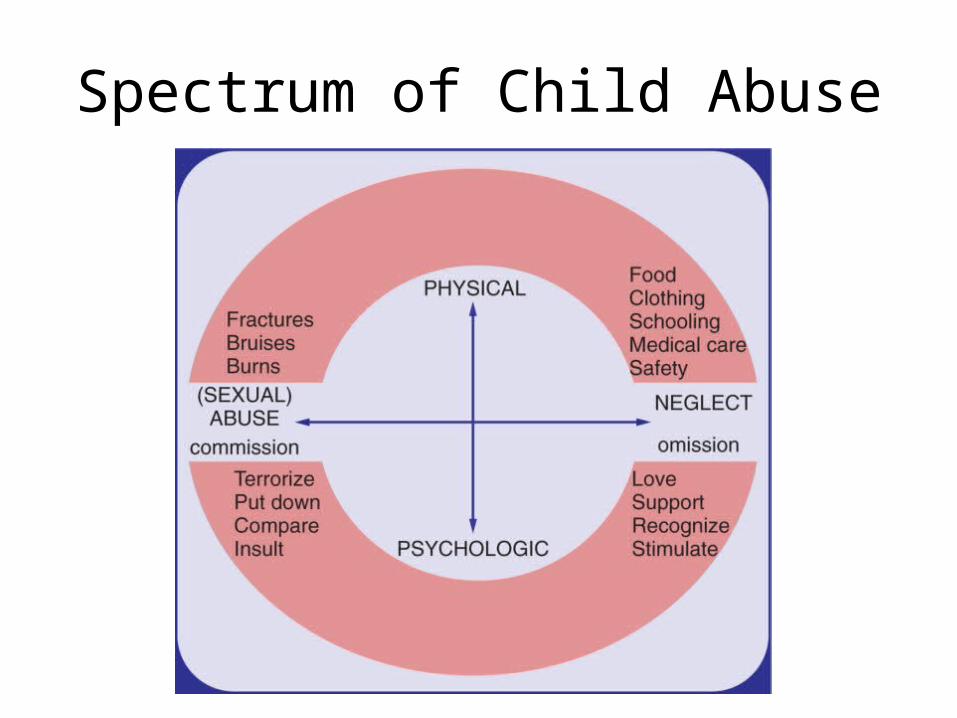
Spectrum of Child Abuse
General assessment• Behavioural indicators– Age appropriate? Regression?– Emotional attachments– School– Drugs – Mood, sleep– Trouble with law
• Physical indicators– Hygeine – Growth– Injuries
Case 1: 3 month old colicky, irritable
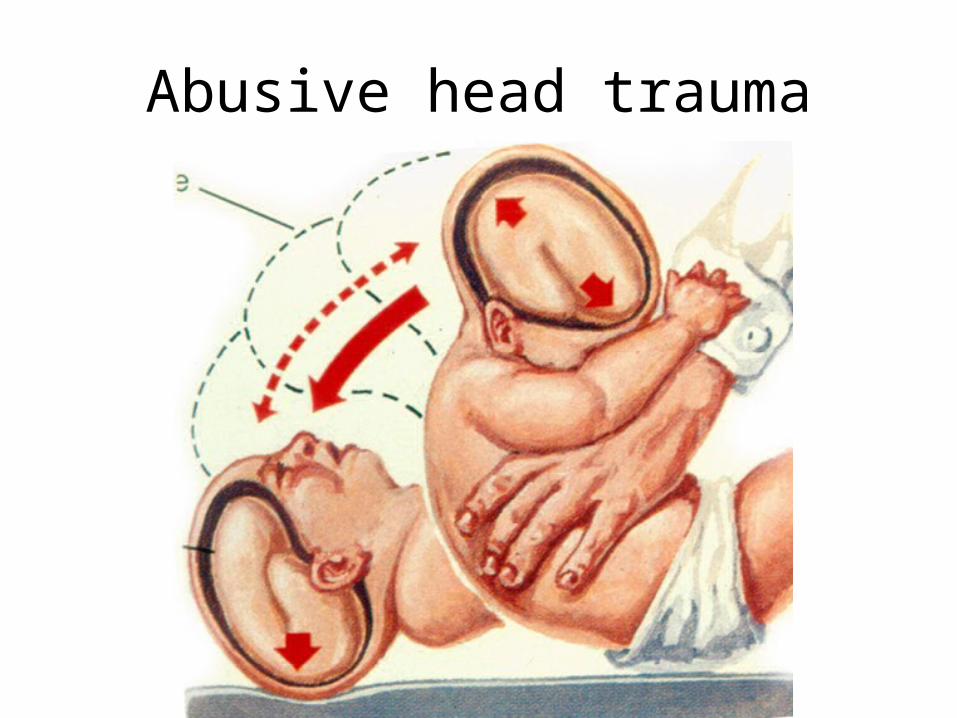
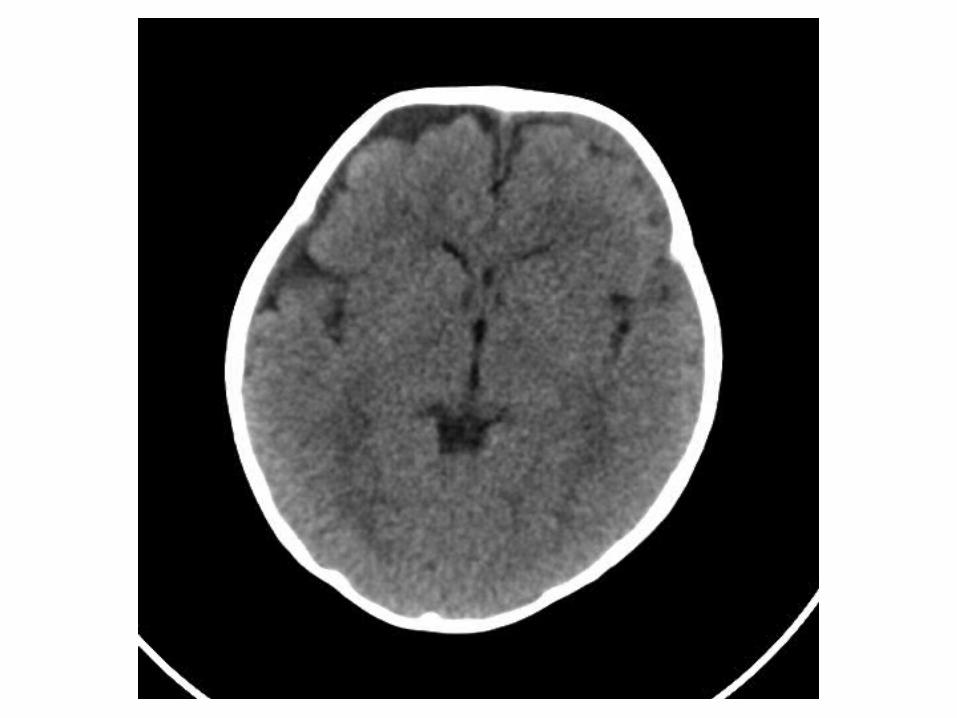
Abusive head trauma
Which is not in ddx for SDH?
• Accidental short fall• Birth trauma • MVC• Minor or no trauma with F13 deficiency• Minor trauma with Marfan• Abusive head trauma• Other: Vit K defic, hemophilia A, vWD, platelet
function disorders, platelet number disorders, metabolic disorders (glutaric aciduria type 1)
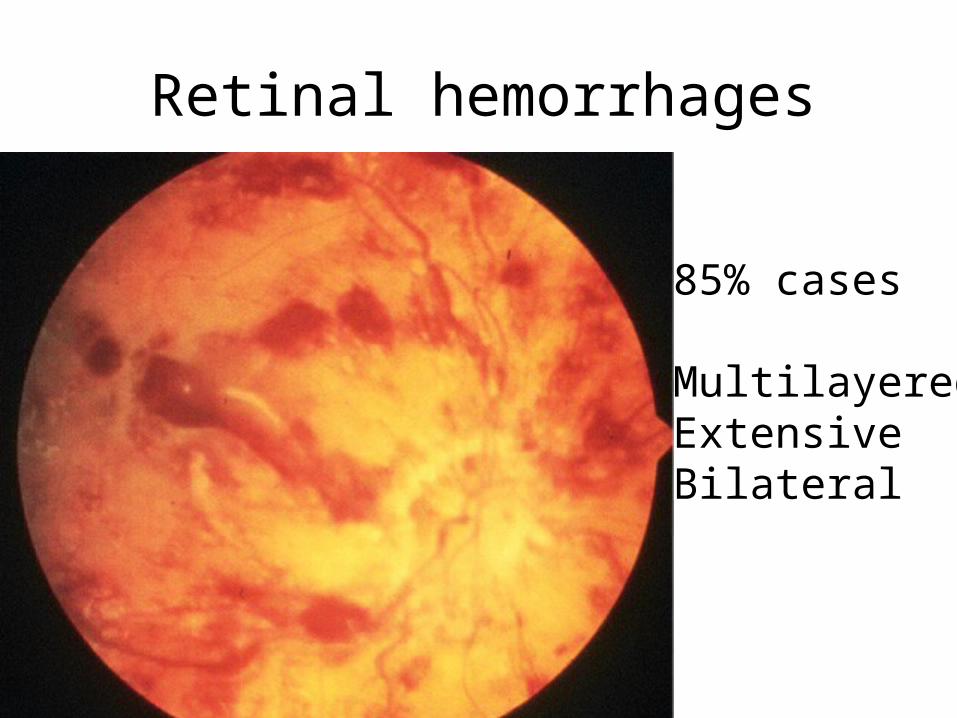
Retinal hemorrhages
85% cases
MultilayeredExtensiveBilateral

Case 2
• 2 year old developmentally delayed tripped on rug and fell onto left side; cried right away, been grabbing ear since
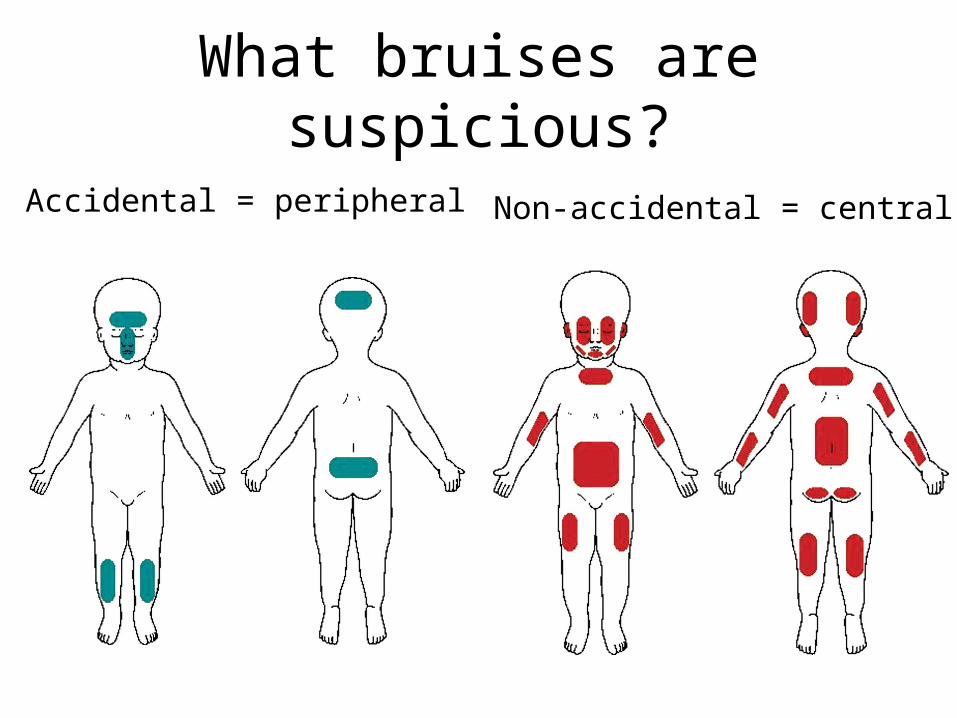
What bruises are suspicious?
Accidental = peripheral Non-accidental = central


Bite marks

Slap marks

Hemophilia

Cord injuryErythema nodosum

Vasculitis:Henoch-Schonlein Purpura

Coining

Cupping
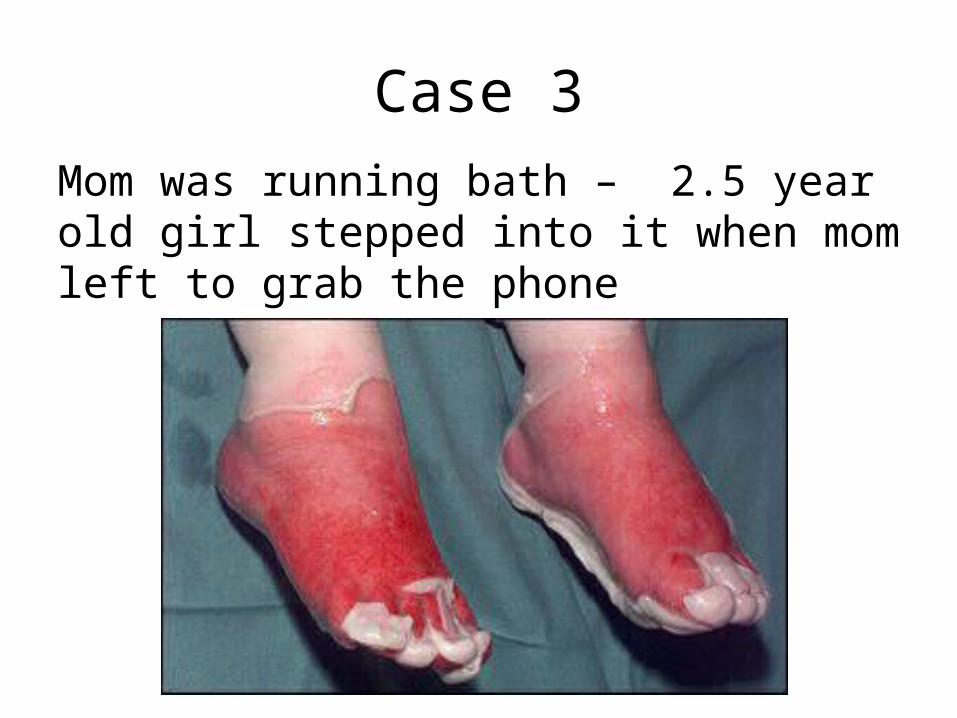
Case 3Mom was running bath – 2.5 year old girl stepped into it when mom left to grab the phone
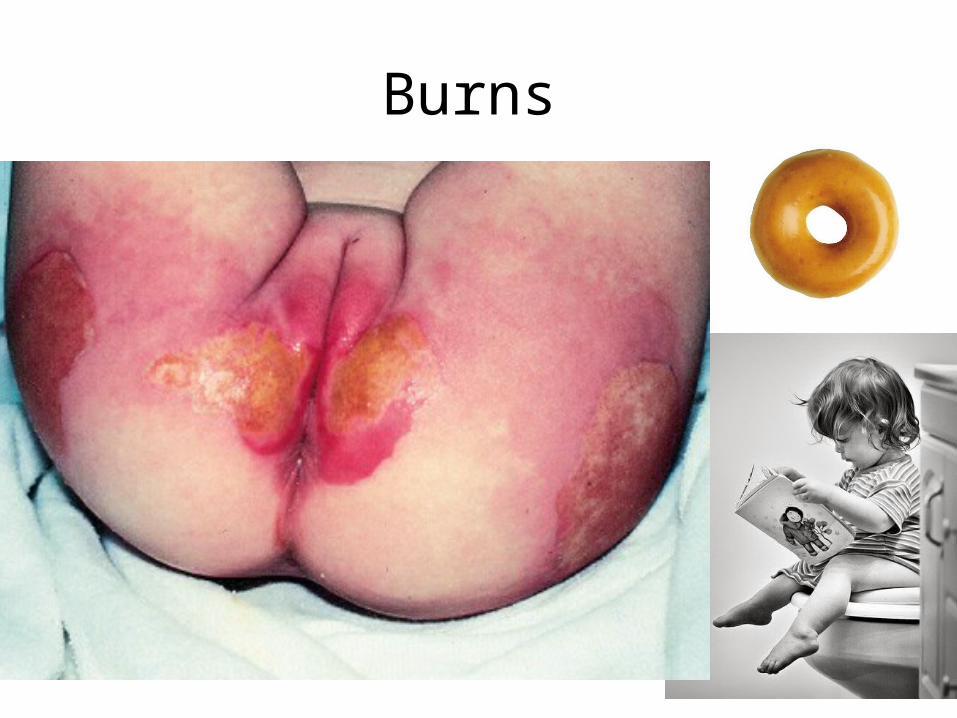
Burns


Staph scalded skin syndrome
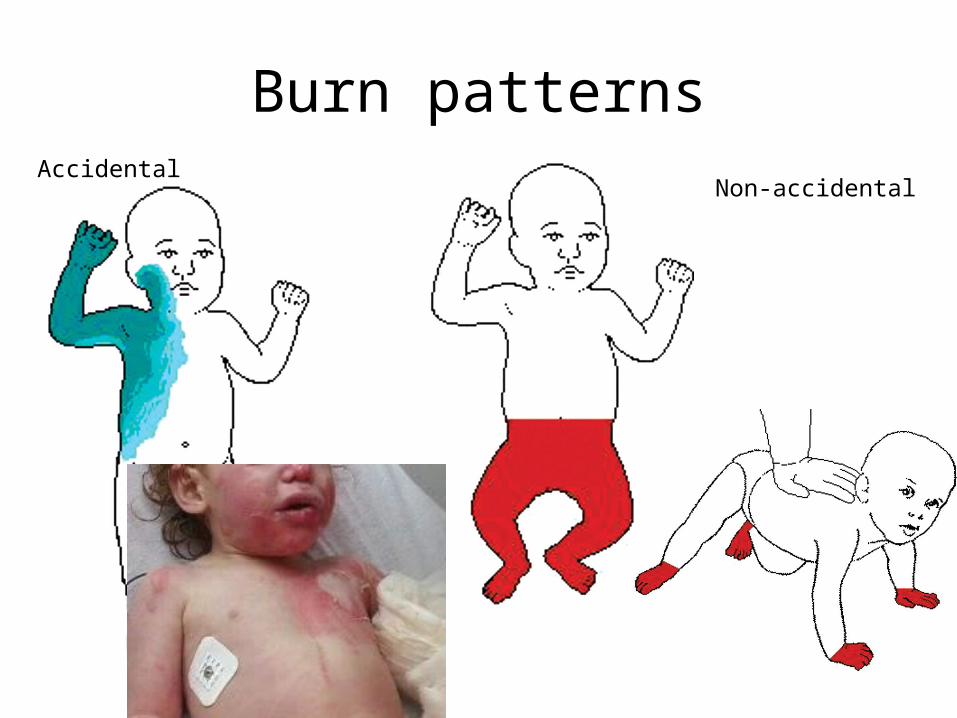
Burn patternsAccidental
Non-accidental

Burn from diarrhea

Healing impetigo
Cigarette burns
Cigarette burns

Curling iron
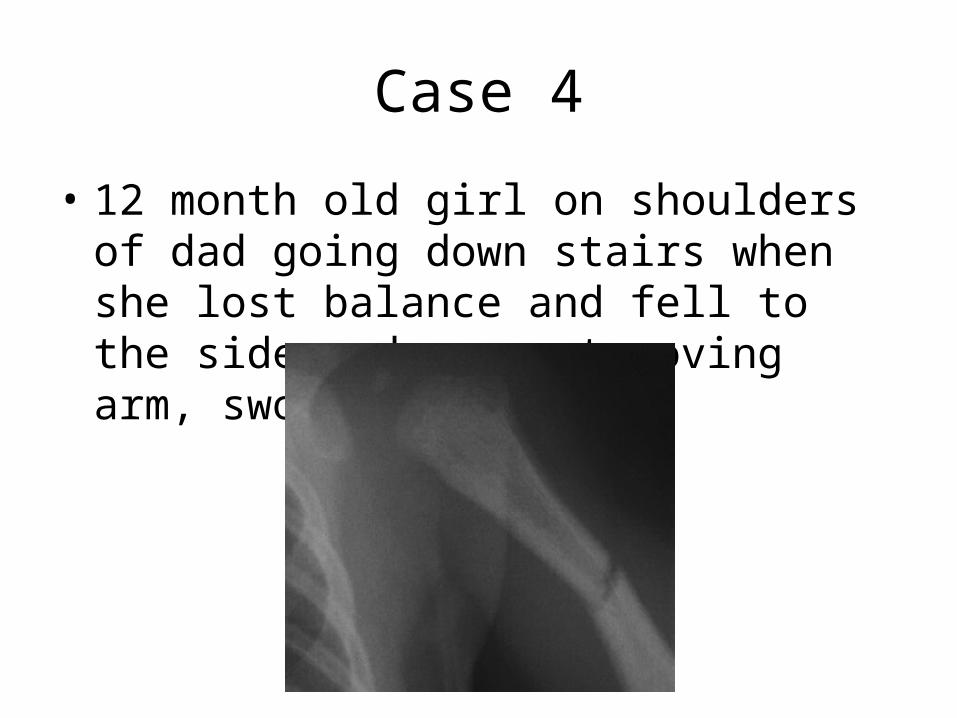
Case 4
• 12 month old girl on shoulders of dad going down stairs when she lost balance and fell to the side and now not moving arm, swollen
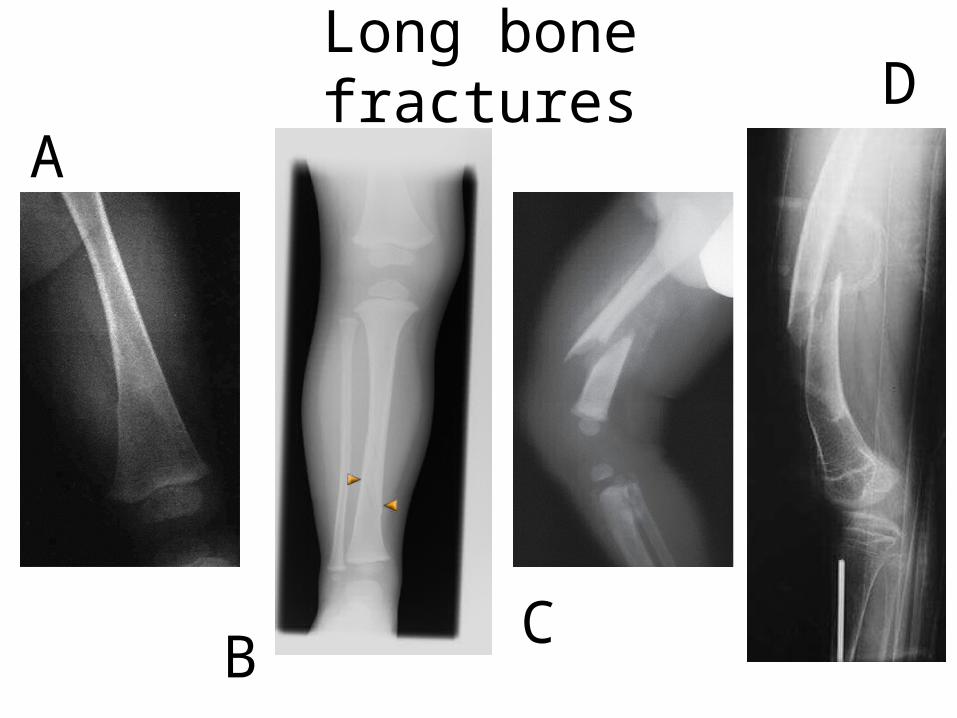
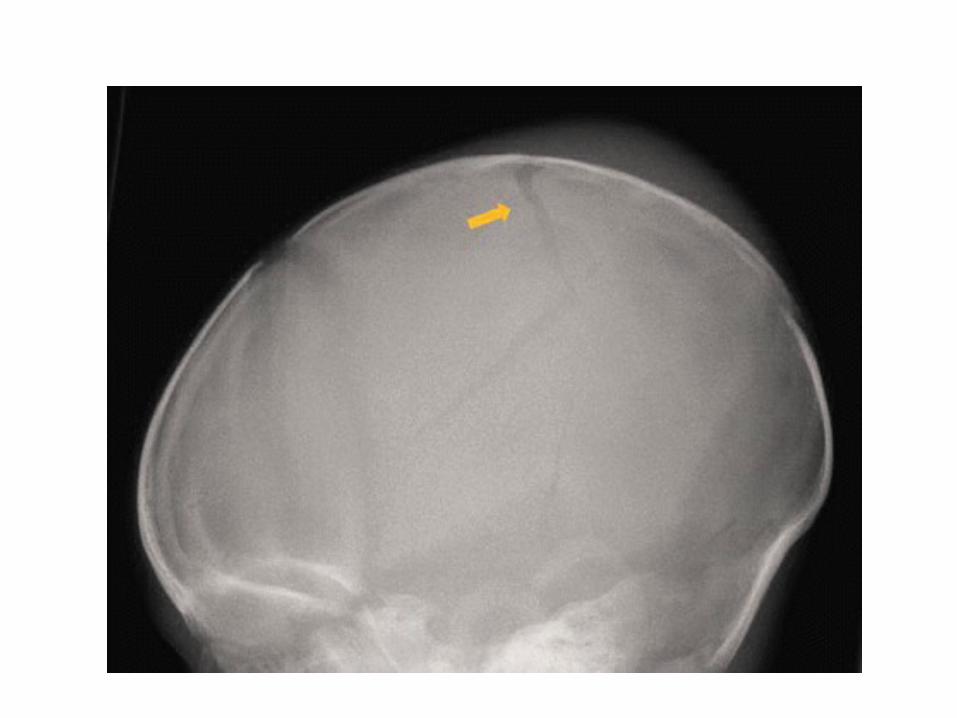
Long bone fractures
CB
AD
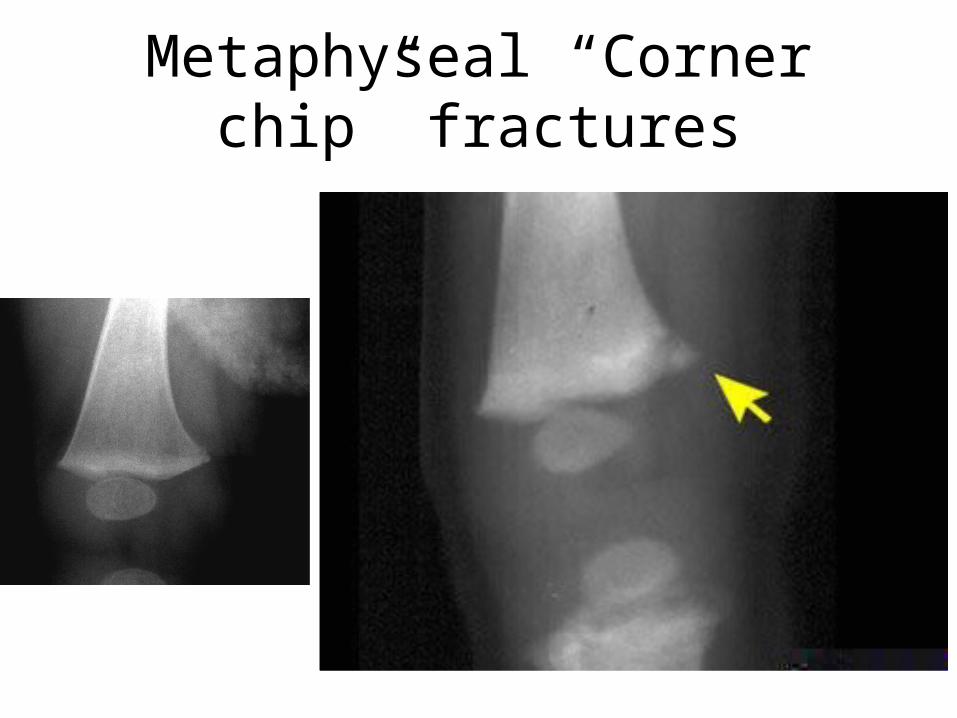
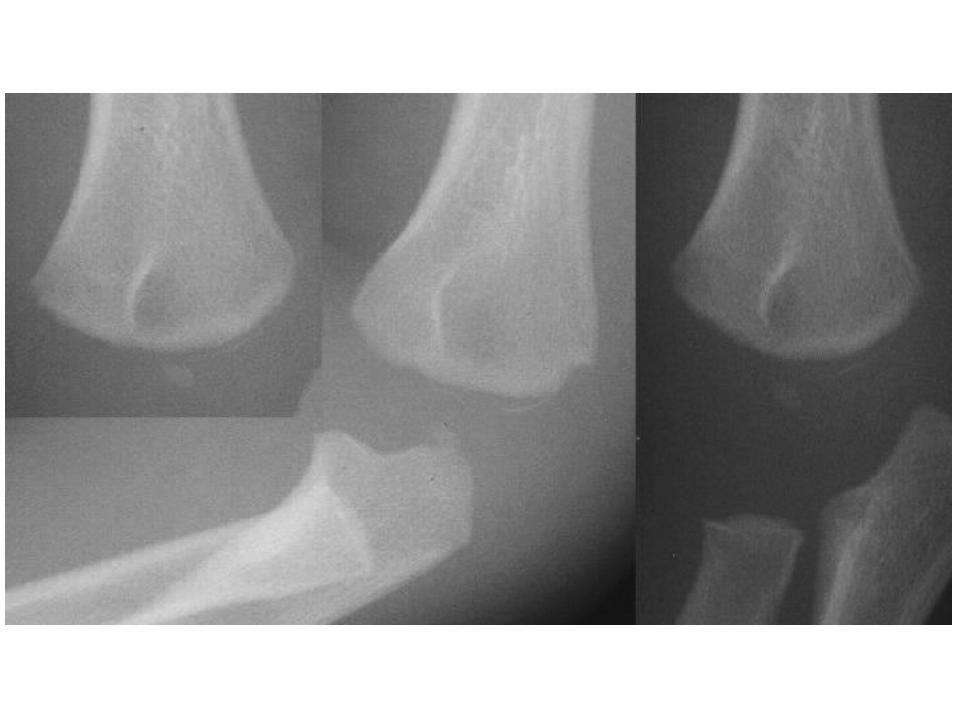
Metaphyseal “Corner chip” fractures
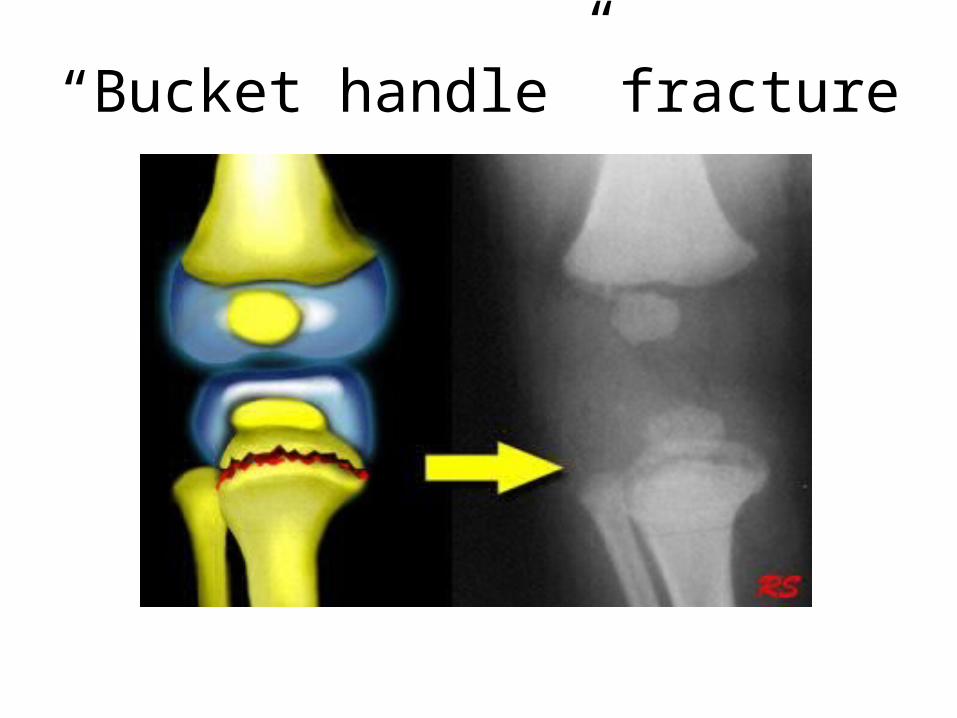
“Bucket handle” fracture
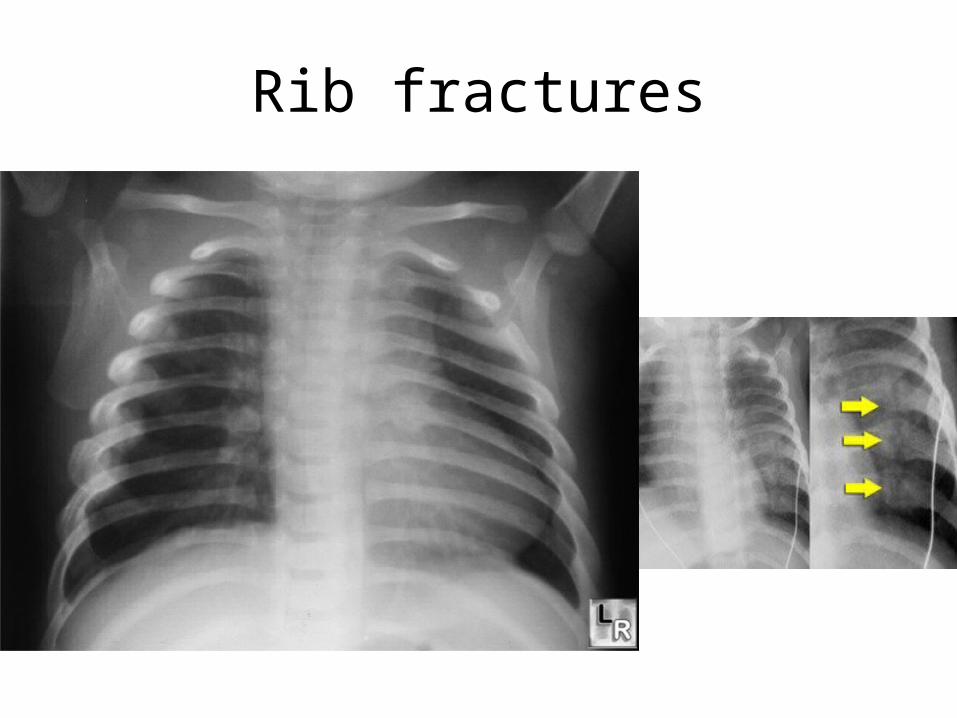
Rib fractures
Fractures from abuse• Non ambulatory child with fracture• Fracture from fall from bed/crib/couch• Strongly suggestive of:– Ribs– Long bone metaphyses– Scapula– Sternum– Vertebral spinous processes
• Moderately suggestive:– Multiple fractures– Fractures of different ages– Epiphyseal separation– Vertebral body fractures

Other signs of abuse
• Traction alopecia• Growth parameters• Extensive dental caries • Severe diaper dermatitis• Neglected wound care
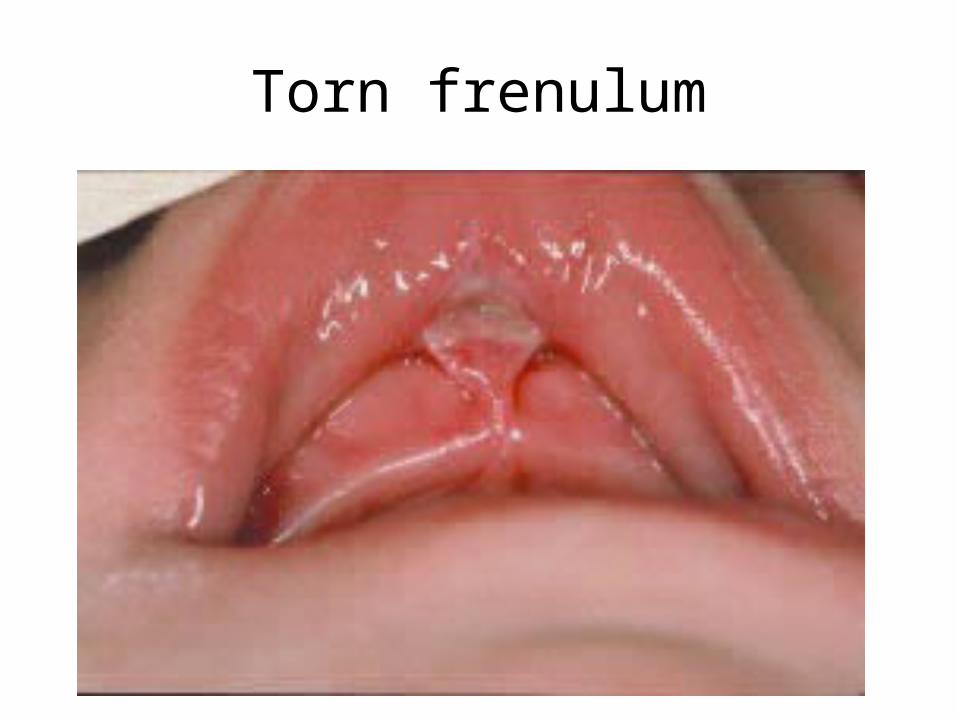
Torn frenulum
Other injuriesVisceral abdominal•predominantly in children > 2 years old•2nd most common cause fatalities •usually blunt trauma (punch or kick to abdomen, rapid deceleration after being thrown)
Investigations
• American Academy of Pediatrics/ Canadian Pediatric society guidelines– Skeletal survey: < 2yo
• Consider repeat in 10 – 14 days
– Head CT– Ophthalmology consult– CBC, coags
– Bone scan?– Bone mineralization labs? Metabolic work up?
Social work always available in the ED
If concerned….. Call:•Child & Family Services: 297-2995•Child abuse service: Dr. Neil Cooper•Sexual abuse clinic: Dr. Jen MacPherson (outpatient referrals)
What to do at the ACH
To admit or not to admit?
• Medical need• Inability to guarantee safety
Document document document
HPI:Mother states “… was washing the dishes when I heard a thud and I ran to the living room and saw her on the floor”…. “she had rolled off the couch”….
P/E:
It is an offence to fail to report suspected maltreatment
Take home points• Child abuse is not always
obvious know what to ask and what to look for
• Always keep in mind mimickers
• Document carefully and objectively
• If any suspicion, report and investigate, and consider admission
THE END




![Child Abuse[1]](https://img.dokumen.tips/doc/110x75/55847cc6d8b42a15768b50e9/child-abuse1.jpg)











