Embed Size (px)
Citation preview

Cochrane Database of Systematic Reviews
Chest physiotherapy for reducing respiratory morbidity in
infants requiring ventilatory support (Review)
Hough JL, Flenady V, Johnston L, Woodgate PG
Hough JL, Flenady V, Johnston L, Woodgate PG.
Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support.
Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.: CD006445.
DOI: 10.1002/14651858.CD006445.pub2.
www.cochranelibrary.com
Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Active chest physiotherapy vs no active chest physiotherapy, Outcome 1 Weight of secretions
cleared per procedure per day (g). . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Analysis 1.2. Comparison 1 Active chest physiotherapy vs no active chest physiotherapy, Outcome 2 Intraventricular
haemorrhage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Analysis 1.3. Comparison 1 Active chest physiotherapy vs no active chest physiotherapy, Outcome 3 IVH grade 3 or 4. 21
Analysis 2.1. Comparison 2 Comparison of active chest physiotherapy techniques (percussion vs cupping), Outcome 1
Hypoxaemia per procedure per baby. . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Analysis 2.2. Comparison 2 Comparison of active chest physiotherapy techniques (percussion vs cupping), Outcome 2 %
change in FiO2 per procedure per baby. . . . . . . . . . . . . . . . . . . . . . . . . . 22
Analysis 3.1. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome 1 Non-
resolution of atelectasis after initial intervention. . . . . . . . . . . . . . . . . . . . . . . 22
Analysis 3.2. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome 2 Secretions
cleared (<0.2 ml) per procedure per baby. . . . . . . . . . . . . . . . . . . . . . . . . 23
Analysis 3.3. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome 3 IVH grade
3 or 4 after commencement of CPT. . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Analysis 3.4. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome 4
Periventricular leucomalacia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
24WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iChest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Chest physiotherapy for reducing respiratory morbidity ininfants requiring ventilatory support
Judith L Hough1, Vicki Flenady2, Leanne Johnston3 , Paul G Woodgate4
1Physiotherapy Department, Mater Hospital, South Brisbane, Australia. 2Centre for Clinical Studies-Women’s and Children’s Health,
Women’s and Children’s Health Service, South Brisbane, Australia. 3School of Health and Rehabilitation Sciences, University of
Queensland, St Lucia, Australia. 4Department of Neonatology, Mater Mother’s Hospital, Brisbane, Australia
Contact address: Judith L Hough, Physiotherapy Department, Mater Hospital, Raymond Terrace, South Brisbane, Queensland, 4101,
Australia. [email protected].
Editorial group: Cochrane Neonatal Group.
Publication status and date: New, published in Issue 1, 2010.
Review content assessed as up-to-date: 27 November 2007.
Citation: Hough JL, Flenady V, Johnston L, Woodgate PG. Chest physiotherapy for reducing respiratory morbidity in
infants requiring ventilatory support. Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.: CD006445. DOI:
10.1002/14651858.CD006445.pub2.
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Chest physiotherapy (CPT) has been used in many neonatal nurseries around the world to improve airway clearance and treat lung
collapse; however, the evidence to support its use has been conflicting. Despite the large number of studies there is very little evidence
of sufficiently good quality on which to base current practice.
Objectives
To assess the effects of active CPT techniques, such as percussion and vibration followed by suction compared with suction alone, on
the respiratory system in infants receiving mechanical ventilation. Additionally, differences between types of active CPT techniques
were assessed.
Search methods
Our search included The Cochrane Library (Issue 2, 2007), MEDLINE (1966 to 2007), EMBASE (1988 to 2007), CINAHL, Science
Citation Index, previous reviews including cross-references, abstracts, conference proceedings and grey literature.
Selection criteria
Trials in which ventilated newborn infants up to four weeks of age were randomly or quasi-randomly assigned to receive active CPT or
suction alone. Infants receiving CPT for the extubation period were excluded.
Data collection and analysis
Two review authors independently conducted quality assessments and data extraction for included trials. We analysed data for individual
trial results using relative risk (RR) and mean difference (MD). Results are presented with 95% confidence intervals (CI). Due to
insufficient data, we could not undertake meta-analysis.
1Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Main results
Three trials involving 106 infants were included in this review. In one trial (n = 20) CPT was no better than standard care in clearing
secretions. No increase in the risk of intraventricular haemorrhage was noted. Two trials compared different types of active CPT. One
trial (n = 56) showed that non-resolved atelectasis was reduced in more neonates receiving the lung squeezing technique (LST) when
compared to postural drainage, percussion and vibration (PDPV) (RR 0.25; 95% CI 0.11 to 0.57). No difference in secretion clearance
or in the rate of intraventricular haemorrhage or periventricular leucomalacia was demonstrated. The other trial (n = 30) showed that the
use of percussion or ’cupping’ resulted in an increased incidence of hypoxaemia (RR 0.53; 95% CI 0.28 to 0.99) and increased oxygen
requirements (MD -9.68; 95% CI -14.16 to -5.20) when compared with contact heel percussion. There was insufficient information
to adequately assess important short and longer-term outcomes, including adverse effects.
Authors’ conclusions
The results of this review do not provide sufficient evidence on which to base clinical practice. There is a need for larger randomised
controlled trials to address these issues.
P L A I N L A N G U A G E S U M M A R Y
Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
There is not enough evidence to determine whether active chest physiotherapy is of benefit to neonates on mechanical ventilation. Babies
who require mechanical ventilation are at risk of lung collapse from increased secretions. Chest physiotherapy (patting or vibrating the
chest) is used to improve clearance of secretions from the airway to try to prevent lung collapse. This review found no clear overall
benefit or harm from chest physiotherapy. Some individual chest physiotherapy techniques were more beneficial than others in resolving
atelectasis and maintaining oxygenation. These results do not support one technique over another. Due to the limited number, poor
quality and age of trials in this review, there is not enough evidence to determine whether or not chest physiotherapy is beneficial or
harmful in the treatment of infants being ventilated in today’s intensive care units. Further good quality trials are needed to address
this issue.
B A C K G R O U N D
Approximately two to three per cent of all babies born in Australia
and New Zealand require admission to a level three neonatal in-
tensive care unit (NICU) (ANZNN 2005). In this group of high-
risk infants, 89% require assisted ventilation. Chest physiotherapy
(CPT) techniques are used in many NICUs throughout the world
to improve airway clearance and treat lung collapse in infants on
ventilatory support.
The application of CPT in airway management of mechanically
ventilated adults has been shown to improve total lung/thoracic
compliance and cardiorespiratory function (Mackenzie 1985);
however, little is known about its effect on neonates. Acute lo-
bar atelectasis is a common problem in infants receiving mechan-
ical ventilation. Atelectasis contributes to morbidity in the neona-
tal nursery, necessitating prolongation of oxygen administration
(Ehrlich 1972). Although CPT has been shown to be effective in
the treatment of both non-ventilated children (Zach 1987) and
intubated adults (Stiller 1990) with acute lobar collapse, studies
of the effectiveness in the neonatal population are conflicting. In
the neonatal population, CPT is used to prevent and treat lung
collapse and consolidation. Some studies in the neonatal popu-
lation have shown positive effects of CPT, including improved
oxygenation (Finer 1978; Curran 1979) and increased removal of
secretions (Etches 1978). However, the use of CPT has also re-
ceived much criticism, largely as a result of reports of adverse out-
comes. Documented adverse outcomes include hypoxaemia (Fox
1978), bruising, rib fractures (Purohit 1975; Dabezies 1997) and
intracranial lesions such as intraventricular haemorrhage (Raval
1987) and porencephalic cysts (Cross 1992; Harding 1998).
CPT in the preterm infant consists of a variety of techniques that
include positioning, active techniques such as percussion and vi-
bration, and suction. Percussion involves a rhythmical cupping ac-
tion applied to the chest wall performed with a full cupped hand,
tented fingers, or by using an infant resuscitation face mask (cup-
2Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ping). The technique of vibration can be performed manually by
using the fingers to cause a fine shaking motion of the chest wall.
Alternatively, an electric toothbrush or other vibrating device can
be used.
The use of these techniques, in varying combinations and frequen-
cies, has become standard treatment for a variety of pulmonary
conditions. Since there are many combinations of treatments that
constitute CPT, it is difficult to determine the exact effects of any
particular treatment technique. There has been some attempt in
the past to ascertain which techniques produced the most clinically
relevant results, but the results are equivocal. One study found
percussion to be better than vibration (Tudehope 1980), while an-
other has found the opposite to be the case (Curran 1979). A third
study found that there was no difference between the techniques
(Hartrick 1982). In clinical practice, percussion and vibration are
rarely used in isolation; most often percussion and vibration are
given in combination with positioning, postural drainage and air-
way suction. Therefore, it is difficult to assess separately the effi-
cacy of each treatment component.
Previous Cochrane reviews have investigated the positioning
(Balaguer 2006) and suctioning (Pritchard 2001; Woodgate 2001;
Spence 2003) components of CPT. Only one review has assessed
the effect of active CPT on preterm infants, and this study in-
volved a population of infants who were being extubated (Flenady
2002). This review could not recommend guidelines for clinical
practice due to small numbers of infants studied and the insuffi-
cient information on outcomes other than the reduction in post-
extubation atelectasis (Flenady 2002). In light of the results of
this review and the amount of conflicting information from other
studies, it is important to investigate the wider use of the tech-
niques of percussion and vibration in the preterm population.
Since the issue of the effectiveness of physiotherapy is still a con-
troversial topic, it is anticipated that this review will provide evi-
dence on which to base guidelines regarding the provision of the
chest physiotherapy techniques of percussion and vibration in the
infant on ventilatory support.
O B J E C T I V E S
1. To determine the effects of active CPT, such as percussion and
vibration followed by suction, compared to nonactive techniques,
such as suction with or without the addition of positioning, in
newborn infants receiving mechanical ventilation:
a) electively for the prevention of atelectasis, consolidation or other
respiratory morbidity
b) therapeutically for the treatment of atelectasis or consolidation
2. To determine the effects of the different types of active CPT.
The following subgroup analyses are planned:
1. Population:
• Gestational age: < 30 weeks; < 37 weeks; 37 weeks and over
• Birth weight : < 1500 grams; < 2500 grams; 2500 grams
and over
• Underlying pulmonary disorder: respiratory distress
syndrome (RDS), aspiration, infection or chronic lung disease
(CLD)
2. Intervention - techniques:
• Type of technique: percussion (including cupping with a
face mask, contact heel percussion and finger percussion);
vibration (with fingers or mechanical vibrator)
• Frequency: four hours or less; > four hours
M E T H O D S
Criteria for considering studies for this review
Types of studies
All trials utilising random or quasi-random patient allocation that
met the inclusion criteria for types of participants, interventions
and at least one outcome were included. Cross-over trials were
included.
Types of participants
All newborn infants receiving mechanical ventilation for neonatal
respiratory disease with the intervention initiated in the first four
weeks of life. We excluded infants receiving prophylactic CPT for
the extubation period as this intervention is addressed in another
Cochrane review (Flenady 2002).
Types of interventions
Active CPT (vibration or percussion, with or without the use of
devices such as face masks and electric vibrators) followed by suc-
tion compared with standard care (suction with or without posi-
tioning).
Studies comparing two or more methods of CPT intervention
were eligible.
3Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Types of outcome measures
Primary outcomes
• Duration of mechanical ventilation (MV) (days)
• Duration of supplemental oxygen after intervention (days)
• Duration of hospital stay (days)
Secondary outcomes
Atelectasis or consolidation based on pre/post radiographs:
• incidence of atelectasis or consolidation (for prophylactic
group)
• resolution or extension of atelectasis or consolidation (for
treatment group)
Oxygenation:
• incidence of hypoxaemia (SaO2 < 90% or TcPO2 < 50
mmHg) during a single intervention
• per cent change PaCO2 and PaO2 pre and post a single
intervention
• per cent change inspired oxygen received (FiO2) pre and
post a single intervention
Secretion clearance:
• sputum weight (g) post a single intervention
• sputum volume (ml) post a single intervention
Rates and type of intracranial lesions diagnosed by ultrasound
scan:
• intraventricular haemorrhage (IVH) (any IVH, grade 3 and
4) (Papile 1978)
• periventricular leucomalacia (PVL) [any grade, and severe
(grades 3 and 4)] (Papile 1978)
Bradycardia (change in heart rate < 30% of baseline or < 100 beats
per minute) during intervention
Search methods for identification of studies
We used the standard search strategy for the Cochrane Neona-
tal Review Group (see: Cochrane Neonatal Review Group, search
strategy for Specialised Register in The Cochrane Library). The re-
view authors undertook a comprehensive search which included
searches of the following electronic databases: The Cochrane Cen-
tral Register of Controlled Trials (CENTRAL, The Cochrane Li-
brary, Issue 2, 2007), MEDLINE (1966 to June 2007), EMBASE
(1988 to June 2007), CINAHL (1982 to June 2007), PEDro
(1929 to June 2007) and Web of Science. The review authors
cross-referenced relevant literature including identified trials and
review articles.
Searches of the electronic databases were based on the following
search strategy:
1. physiotherapy OR physical therapy, AND
2. infant OR neonate OR newborn, AND
3. chest OR lung OR respiratory
4. NOT cystic fibrosis
The search also included searches of previous reviews including
cross-references, abstracts, conference and symposia proceedings,
expert informants and journal hand searching restricted to the En-
glish language. We handsearched conference Proceedings of the
Society for Pediatric Research (SPR) (1967 to 2007), the European
Society for Pediatric Research (ESPR) (2005), Pediatric Academic
Societies Abstracts 2006, Australasian Physiotherapy conference
abstracts (2003 to 2006), theses and dissertation lists, The Char-
tered Society of Physiotherapists (1988 to 2005) and trial registries
(Australia, UK, USA) for unpublished work. No other language
restrictions were applied.
We examined the title and abstract of each retrieved study to assess
eligibility. If there was uncertainty, we examined the full paper.
Data collection and analysis
We used the standard methods of the Neonatal Review Group of
the Cochrane Collaboration.Two review authors searched for and
considered trials for inclusion, evaluated methodological quality
and extracted data independently. Differences in interpretation
were resolved by discussion with a third review author.
Where necessary, we contacted investigators of identified trials
for additional information regarding trial methodology or out-
come data (Crane 1978; Etches 1978; Finer 1978; Curran 1979;
Tudehope 1980; Hartrick 1982; Peters 1983; Fiser 1985; Leung
1998; Main 2001). Since many of these studies were performed
quite a few years ago some of the authors either no longer had the
data available (Etches 1978; Finer 1978; Curran 1979; Tudehope
1980) or could not be contacted (Crane 1978; Hartrick 1982).
At the time of this review, additional data had been received from
Peters 1983, and was included in this review.
Quality assessment
We conducted quality assessment according to the methods de-
scribed in section six of the Cochrane Handbook for Systematic
Reviews of Interventions (Handbook 2007). We considered four
major sources of potential bias and methods of avoidance when
assessing the trial quality:
(1) selection bias - blinding of randomisation;
(2) performance bias - blinding of intervention;
(3) attrition bias - complete follow-up;
(4) detection bias - blinding of outcome assessment.
A quality rating was assigned to each trial for the criterion of
blinding of randomisation as follows: (A) adequate, (B) unclear,
(C) inadequate, or (D) not used. A quality rating of (A) yes, (B)
can’t tell, or (C) no, was assigned to the other quality components
(completeness of follow-up and blinding of outcome assessment).
High quality trials were defined as those receiving an A rating for
blinding of randomisation (central computerised randomisation
service or sealed opaque envelopes). The quality assessment rating
4Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

included in the Table of ’Characteristics of Included Studies’ refers
to blinding of randomisation (allocation concealment) only.
Data analysis
Two review authors independently extracted data using prepared
data extraction forms. We resolved any discrepancies by discussion
with a third review author.
We used the Review Manager software (RevMan 4.2.7) (RevMan
2003) for statistical analyses. In the cross-over trial (Peters 1983)
investigators provided individual patient data for each intervention
on oxygenation. From this data the authors derived the group
means and standard deviations for per cent change in oxygenation.
The numbers of infants who experienced one or more hypoxaemic
episode during each intervention were included for the outcome
of hypoxaemia.
Due to insufficient data it was not possible to conduct a meta-
analysis. For individual trials, where possible, mean differences
and 95% confidence intervals (CI) are reported for data measured
on a continuous scale. For categorical outcomes, relative risk and
95% confidence intervals are reported.
Methods for future updates of this review
We did not implement all of the methods outlined in the protocol
as there were insufficient data.
For future updates of the review, we will analyse categorical data
using relative risk (RR), risk difference (RD) and number needed
to treat (NNT) where appropriate. We will use a fixed-effect model
to pool results. We will use weighted mean differences (WMD)
for data measured on a continuous scale. We will report the 95%
confidence intervals (CI) for all estimates. We will perform sensi-
tivity analyses to evaluate the effect of the trial quality (excluding
quasi-randomised trials and considering trials with minimal bias).
We will assess heterogeneity by visual inspection of the outcomes
tables and by using an I-squared test of heterogeneity (Higgins
2002). Where statistical heterogeneity is found, the review authors
will look for an explanation using prespecified subgroup analyses.
The following subgroup analyses will be performed:
1. Population
• Gestational age: < 30 weeks; < 37 weeks; 37 weeks and over
• Birth weight : < 1500 grams, < 2500 grams, 2500 grams
and over
• Underlying pulmonary disorder: respiratory distress
syndrome (RDS), aspiration, infection or chronic lung disease
(CLD)
2. Intervention - techniques
• Type of technique: percussion (including cupping with a
face mask, contact heel percussion and finger percussion);
vibration (with fingers or mechanical vibrator)
• Frequency: four hours or less; > four hours
R E S U L T S
Description of studies
The search strategy initially retrieved 2036 references of which
1993 publications were excluded based upon title and abstract. We
identified the remaining 43 publications as potentially eligible for
inclusion in this review and requiring more detailed examination.
After examination of the publications, we excluded 40 publications
from the review. Thirty-one publications were excluded as they did
not fulfil the inclusion criteria. Of these 31, we excluded 23 trials
as they were not randomised or quasi-randomised controlled trials,
six trials because the participants were not newborn infants with
respiratory disease in the first four weeks of life, one because the
participants were not mechanically ventilated, and a further one
trial because the intervention was not a physiotherapy technique.
We excluded a further four trials (Crane 1978; Hartrick 1982;
Fiser 1985; Leung 1998) as the publications were in the form of
conference abstracts and despite attempts to do so no further data
could be obtained from the authors.
We excluded another five trials (Etches 1978; Finer 1978; Curran
1979; Tudehope 1980; Main 2001) as no useable data were re-
ported or could be obtained from the authors.
(For further details on excluded studies see the table of ’Charac-
teristics of Excluded Studies’).
One ongoing trial was identified (Hough 2007) (See table of
’Characteristics of Ongoing Studies’).
Three trials were included in the review.
The study by Raval 1987 compared the effects of CPT in 20 pre-
mature neonates with a gestational age of 28 to 32 weeks. Infants
who were intubated and ventilated for respiratory distress syn-
drome (RDS) were randomly assigned to two groups. The inter-
vention in the CPT group (n = 10) consisted of postural drainage
in the head up and head down position, percussion, vibration and
suction. The control group (n = 10) procedure consisted of suc-
tioning only. Each of these procedures was performed every two to
three hours in the first 24 hours of life. Outcomes measured used
were continuous TcPO2 monitoring, arterial blood gas (ABG)
sampling, weight of sputum cleared, mortality rate and rates of
intracranial lesions.
Peters 1983 evaluated the responses of critically ill neonates to two
different techniques of CPT administration. Thirty neonates (25
to 42 weeks gestational age) who were 28 days old or younger
were randomised in a two-period cross-over design to one of two
groups. Group 1 received postural drainage, endotracheal instilla-
tion of saline, suction and percussion consisting of cupping with a
Bennett face mask (Bennett percussion) followed by Boyd percus-
sion (contact heel percussion) an hour later. Group 2 received the
same interventions in the reverse order. The neonates’ responses
for heart rate, mean arterial pressure (MAP), intracranial pressure
(ICP), TcPO2 and TcPCO2 were recorded during the pre-CPT,
5Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

postural drainage, percussion, ETT instillation and suctioning,
and immediately post-CPT phases.
Wong 2003 enrolled 56 neonates who were aged less than 37 weeks
gestation and required mechanical ventilation if they met the in-
clusion criteria of the presence of a segmental or lobar collapse
confirmed on chest x-ray. Lung squeezing technique (LST), a form
of manual chest wall compression, was compared in a group of 26
neonates with conventional treatment of postural drainage, per-
cussion and vibration (PDPV). Therapy sessions were performed
twice daily at specified times until resolution of atelectasis oc-
curred. Re-expansion of atelectasis, recurrence of atelectasis, dura-
tion of ventilation, duration of oxygen dependency, occurrence of
bronchopulmonary dysplasia (BPD), rates of intracranial lesions
and mortality rate were the outcomes measured in this study.
Types of participants
A total of 106 infants were randomised in the three included trials
investigating CPT in neonates.
Participant recruitment and inclusion criteria varied between the
three trials; Raval 1987 included preterm infants with a birth
weight less than 2000 grams, Wong 2003 recruited mechanically
ventilated infants with a gestational age of less than 37 weeks,
and Peters 1983 included any newborn infant requiring intuba-
tion. Gestational ages varied from between 28 to 32 weeks (Raval
1987), 22 to 36 weeks (Wong 2003) and 25 to 42 weeks (Peters
1983). Birth weights varied correspondingly with one study not
stating birth weight (Raval 1987), the second ranging from 540
to 2900 grams (Wong 2003), and in third the study (Peters 1983)
the infants tending to be heavier (ranging in weight from 750 to
4030 grams). Postnatal age at the time of the study varied from
1 to 12 hours of age (Raval 1987) to 1 to 10 days (Peters 1983).
In the trial by Wong 2003, the postnatal age was not stated. The
primary diagnosis for enrolled infants in Raval 1987 was RDS,
whereas for the study by Wong 2003 the main diagnosis was at-
electasis. In the third study, the diagnoses included hyaline mem-
brane disease (HMD), pneumonia and transient tachypnoea of
the newborn (Peters 1983). All three studies included only infants
who were mechanically ventilated. Only two of the studies stated
exclusion criteria. Peters 1983 included infants requiring sedation
for irritability and/or restlessness, while Wong 2003 stated their
exclusion criteria as persistent pulmonary hypertension, meco-
nium aspiration syndrome, congenital heart defects, pneumonia
presenting with generalised patchy consolidation, post-cardiotho-
racic surgery, pleural effusion and pneumothorax.
Types of interventions
The types of interventions assessed differed across the included
studies. Raval 1987 compared CPT comprising postural drainage
in the head up and in the head down positions, percussion, vi-
bration and suctioning (PDPV) with a control group receiving
standard care. Each of these procedures was performed every two
to three hours throughout the first 24 hours of life. Wong 2003
also used the PDPV technique combination but compared this
with another CPT technique called the lung squeezing technique
(LST) until resolution of atelectasis. The remaining study com-
pared individual techniques of percussion with a face mask (cup-
ping) and contact heel percussion using a cross-over design (Peters
1983). Each infant received each technique once in a randomised
order over approximately a three hour period.
Types of outcome measures
Short-term physiological outcomes of oxygenation could be in-
cluded from one cross-over trial (Peters 1983). In this trial, tran-
scutaneous oxygenation, changes in oxygen requirements and hy-
poxic episodes were measured 10 minutes pre and post-interven-
tion. Although Peters 1983 measured PaCO2, we could not in-
clude this data in the analyses as the standard deviation data could
not be obtained from the author. In the trial by Raval 1987, oxy-
genation was reported in figure format and as the authors could
not be contacted, we could not include the data on oxygenation in
the review. Secretion clearance was also used as an outcome mea-
sure in two of the studies (Raval 1987; Wong 2003). Wong 2003
defined the secretions as obvious if the amount collected during
a single intervention was greater than 0.2 ml. Raval 1987 mea-
sured the amounts of secretions collected over a 24-hour period
and reported average secretion per procedure. Rates of intracra-
nial lesions diagnosed by ultrasound scan and mortality rate were
measured in the two parallel group studies. Ultrasound scans were
done at three to five days of postnatal life in one trial (Raval 1987)
and for three consecutive days after the first intervention in the
other (Wong 2003). For the purposes of this review the highest
grade of haemorrhage was included. Although the study by Peters
1983 did not include ultrasound findings, they did report changes
in intracranial pressure and mean arterial pressure; however, these
measurements were not included in our pre-specified outcomes.
Wong 2003 was the only study to document duration of venti-
lation, duration of oxygen dependency and bronchopulmonary
dysplasia, and the presence of atelectasis on chest radiographs.
(For further details on included studies see the table, ’Character-
istics of Included Studies’).
Risk of bias in included studies
Concealment of allocation
Of the three included studies, only one reported an adequate
method of allocation concealment (Wong 2003). This study used a
computerised random number allocation placed in sealed opaque
envelopes, and stratified by mode of ventilation [high frequency
oscillatory ventilation (HFOV) or conventional mechanical ven-
tilation (CMV)]. The other two reported randomly assigning par-
ticipants to groups but did not report on the method of allocation
concealment (Peters 1983; Raval 1987).
Blinding of intervention
Due to the nature of the intervention of CPT, blinding of inter-
vention was not employed in any of the included studies.
6Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Completeness of follow-up
There was no loss to follow-up reported in any of the included
studies. Only one study reported withdrawals (Wong 2003); how-
ever, outcomes for these infants were included in the analysis.
Blinding of outcome measures
In summary, only one study was of a high methodological quality
(Wong 2003). It is difficult to determine adequately the quality
of the remaining two trials (Peters 1983; Raval 1987) due to lack
of information in the reported studies and the inability to obtain
clarification from the authors.
Effects of interventions
The results of three trials are included in this review (Peters 1983;
Raval 1987; Wong 2003).
Active CPT versus nonactive techniques/standard care (Com-
parison 1)
One trial (Raval 1987) with a total of 20 infants compared active
CPT in the form of postural drainage, percussion and vibration
(PDPV) with the nonactive technique of suction alone.
Primary outcome measures
(Duration of mechanical ventilation, duration of supplemental
oxygen, duration of hospital stay):
Raval 1987 did not address any of the preplanned primary out-
come measures.
Secondary outcomes
Weight of secretions cleared per procedure per day (Outcome 1.1)
There was no statistical difference in the amount of sputum cleared
with CPT as compared to the amount cleared with suction alone
(MD 0.01 g; 95% CI -0.10 to 0.12).
Rates of IVH (Outcomes 1.2 - 1.3)
No statistically significant difference was found for either the rate
of any intraventricular haemorrhage (RR 2.33; 95% CI 0.83 to
6.54) or for the rate of a grade 3-4 IVH (RR 11.00; 95% CI 0.69
to 175.86).
Comparison of active CPT techniques (Comparison 2)
One trial (Peters 1983) (n = 30) reported change in oxygenation
comparing the techniques of percussion versus cupping.
Primary outcome measures
(Duration of mechanical ventilation, duration of supplemental
oxygen, duration of hospital stay):
Peters 1983 did not address any of the preplanned primary out-
come measures.
Secondary outcomes measures
Change in oxygenation per procedure per baby (Outcome 2.1 - 2.2)
An increase in the incidence of hypoxaemia was shown with cup-
ping when compared to contact heel percussion (RR 0.53; 95%
CI 0.28 to 0.99) and an associated increase in oxygen requirement
(MD -9.68; 95% CI -14.16 to -5.20).
Comparison of LST and PDPV (Comparison 3)
One trial (Wong 2003) (n = 56) compared the techniques of LST
and PDPV.
Primary outcome measures
(Duration of mechanical ventilation, duration of supplemental
oxygen, duration of hospital stay):
Wong 2003 did not address any of the preplanned primary out-
come measures.
Secondary outcomes
Non-resolution of atelectasis after initial intervention (Outcome 3.1)
When compared with PDPV, LST resulted in a reduction in the
numbers of infants with non resolution of atelectasis (RR 0.25;
95% CI 0.11 to 0.57).
Secretion clearance per procedure per baby (Outcome 3.2)
There was no statistically significant difference between the LST
and PDPV groups in the numbers of infants who had less than
0.2 ml of secretions removed post-treatment (RR 0.96; 95% CI
0.62 to 1.49).
Rates of IVH grade 3-4 (Outcome 3.3)
There was no difference in the rate of progression of IVH to grade
3-4 when LST was compared to PDPV (RR 0.87; 95% CI 0.35
to 2.17).
Rates of any PVL (Outcome 3.4)
There was no difference in the rate of PVL (RR 0.87; 95% CI
0.21 to 3.52) between the techniques of LST and PDPV.
Due to small numbers, meta-analyses and planned subgroup anal-
yses could not be undertaken.
D I S C U S S I O N
This review includes the results of three trials that studied 106
infants. Due to insufficient data and differences in reporting of
outcome measures meta-analysis could not be undertaken.
Primary outcomes
The pre-specified primary outcomes of duration of mechanical
ventilation, duration of supplemental oxygen after intervention,
and duration of hospital stay were not reported in any of the three
trials included in this review.
Secondary outcomes
Data from one trial (Raval 1987) comparing active CPT (postural
drainage, percussion and vibration (PDPV)) with standard care
did not show any difference in the outcome of weight of secretions
cleared.
7Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The remaining two studies compared different types of active CPT
techniques. In one trial, the lung squeezing technique (LST) re-
sulted in a decrease in the number of infants with non-resolution
of atelectasis after the first treatment; however, LST did not re-
sult in a corresponding improvement in secretion clearance (Wong
2003). This study also reported that LST took significantly fewer
therapy sessions to attain full re-expansion of the atelectatic lung
than the PDPV group (p < 0.001). Despite LST being superior
to PDPV in attaining lung re-expansion, the rate of recurrence of
lung atelectasis was similar in both groups (p = 0.8) and there was
no difference in the number of infants whose lungs failed to re-ex-
pand (p = 0.7). In the analyses on change in oxygenation, cupping
resulted in more hypoxaemia and increased oxygen requirements
compared with contact heel percussion.
The results of this review indicate that although there was no clear
benefit for the use of CPT over standard care, LST was superior
to PDPV for the treatment of atelectasis, and neonates were kept
better oxygenated with contact heel percussion compared to cup-
ping. LST, although reportedly used in Asia, does not appear to
be used extensively throughout other parts of the world. Further
research is required to better understand the indications for and
outcomes of this technique.
CPT has come under much criticism due to adverse events such
as intracranial lesions (Harding 1998) and rib fractures (Purohit
1975). This review found that there was no difference in the risk
of developing intracranial lesions, either between active CPT and
standard care or between types of techniques. However, the analysis
between active CPT and standard care did approach significance
and therefore raises some concern as to whether this finding is
clinically significant. Practices described in the trial by Raval 1987
comparing active CPT and standard care are very different to those
currently used in most neonatal nurseries. Although there was no
evidence of adverse events or harm, the small numbers of infants
included in the review meant that important outcomes could not
be assessed. Due to insufficient data, planned subgroup analyses
of infants < 30 weeks gestation who are potentially more at risk
could not be undertaken.
The findings of this review highlight the limitations of the evidence
presently available from randomised trials.
These limitations include:
Methodological quality of included studies
Only one trial was considered to be of relatively high method-
ological quality (Wong 2003). As only one trial reported blinded
allocation to treatment, no trials blinded the intervention, and it
is unknown whether there was blinded assessment of outcome,
the potential for a high risk of bias in these studies cannot be ex-
cluded. Blinding of intervention is important when blinding of
outcome is not undertaken. This is an inherent problem in trials
investigating CPT (Wallis 1999).
Small numbers
Due to the small numbers of infants enrolled in the included trials,
all estimates of effect are imprecise resulting in the inability to
assess adequately the effects of this intervention. Subgroup analyses
of high risk infants (< 30 weeks) could not be undertaken. This is
an important deficiency in the evidence currently available.
Inconsistency in study design
The included trials employed different interventions and outcome
measures and, therefore, could not be combined. Even when oxy-
genation was the outcome measured, the three studies defined it
in slightly different ways, precluding the ability to combine the
results. Other factors which may have had an impact on the results
obtained could be differences in inclusion criteria and technique
delivery.
Applicability to present day practice
Two of these studies were conducted over 20 years ago. Applicabil-
ity of the results to present day practice may be compromised due
to changes in population characteristics and interventions includ-
ing: exogenous surfactant, changes in modes of ventilation, and
changes in how CPT is delivered. Importantly, two of the trials
included a head down tip for postural drainage, which is not used
today as it has been shown to increase the risk of IVH (Emery
1983; Cowan 1985). Since continuous positive airway pressure
(CPAP) is being used more frequently, the effect of CPT in infants
on CPAP should also be included in future reviews.
Absence of primary outcome measures in included studies
Clinically relevant long-term outcomes such as duration of me-
chanical ventilation, duration of supplemental oxygen, and dura-
tion of hospital stay have not been reported in any of the included
trials.
These limitations all highlight the need for further good quality
randomised trials. Due to insufficient data there is not enough
reliable evidence to support or refute the use of CPT
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
The results of this review do not provide sufficient evidence to
guide clinical practice on the use of CPT techniques in infants
on ventilatory support in today’s neonatal intensive care settings.
Although concern for the safety of active CPT in preterm infants
has been reported, possible adverse effects of CPT could not be
evaluated due to insufficient data. In view of this and the lack of
clear evidence for benefit, it would seem wise to use this interven-
tion cautiously.
8Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Implications for research
Further well-designed trials are required to assess the risks and ben-
efits of CPT in the treatment of respiratory diseases in ventilated
neonates. Future trials should be adequately powered to address
clinically important outcomes, particularly for the high risk pop-
ulation of infants < 30 weeks gestation. Clinically important out-
comes which should be assessed include duration of ventilation,
duration of oxygen therapy, length of hospital stay, and presence
of intracranial lesions. Shorter-term outcomes such as resolution
of atelectasis, oxygenation, and other lung function variables such
as ventilation distribution should also be included. Costs also need
to be considered.
Some of the important clinical and economic outcomes that re-
main unmeasured by current research are likely to require a very
large sample size, therefore, a large multicentre trial would be rec-
ommended.
A C K N O W L E D G E M E N T S
The authors would like acknowledge Dr K Peters, Assistant Pro-
fessor, Faculty of Nursing/Perinatal Research Centre, University
of Alberta, Edmonton, Alberta for providing further information
regarding her trial.
Although Dr C Curran, Dr P Etches, Dr N Finer and Dr D
Tudehope could not provide more data from their trials, we would
like to acknowledge their attempt to do so.
We would also like to thank Karen New for providing assistance
with the completion of this review.
R E F E R E N C E S
References to studies included in this review
Peters 1983 {published and unpublished data}
Peters, K. Neonatal unit - research studies. AARN News
Letter 1983;39:14–6.
Raval 1987 {published data only}
Raval D, Yeh TF, Mora A, Cuevas D, Pyati S, Pildes RS.
Chest physiotherapy in preterm infants with RDS in the
first 24 hours of life. Journal of Perinatology 1987;7:301–4.
Wong 2003 {published data only}
Wong I, Fok TF. Randomized comparison of two
physiotherapy regimens for correcting atelectasis in
ventilated pre-term neonates. Hong Kong Physiotherapy
Journal 2003;21:43–50.
References to studies excluded from this review
Andersen 1991 {published data only}
Andersen JB, Falk M. Chest physiotherapy in the pediatric
age group. Respiratory Care 1991;36:546–54.
Beaudoin 1973 {published data only}
Beaudoin J, Remondiere R. Chest therapy for newborn
children. Physiotherapy Canada 1973;25:152–4.
Becroft 1998 {published data only}
Becroft DM, Chan Y, Harding JE. Chest physiotherapy is
associated with encephaloclastic porencephaly in extremely
premature babies. Modern Pathology 1998;11:1P.
Bradbury 1996 {published and unpublished data}
Bradbury J. The effect of cupping on the cardiorespiratory
status of the neonate with respiratory distress syndrome.
Proceedings of the 1996 National Physiotherapy Congress.
1996:199–200.
Cabero 1987 {published data only}
Cabero Mendoza M, Farre Rosich T, Garcia-Margallo Paris
L, Lorente Lorente MJ, Pla Consuegra M, Rodes Meifren
C. Early respiratory physiotherapy in bronchopulmonary
dysplasia. Revista de Enfermería 1987;10:52–3.
Coradello 1979 {published data only}
Coradello H, Tauffkirchen E, Baar B. Effect of chest
physiotherapy on pO2 and pCO2 in premature and mature
babies with respiratory distress syndrome (author’s transl).
Padiatrie und Padologie 1979;14:37–42.
Coradello 1982 {published data only}
Coradello H, Simbruner G, Baar B. Influence of physical
chest therapy in mechanically ventilated newborn infants
on the amount of secretions removed from the trachea.
Klinische Padiatrie 1982;194:8–10.
Crane 1978 {published data only (unpublished sought but not used)}
Crane LD, Zombek M, Krauss AN, Auld PA. Comparison
of chest physiotherapy techniques in infants with HMD.
Pediatric Research 1978;12:559.
Crane 1986 {published data only}
Crane LD. Cardiorespiratory management of the high-risk
neonate: Implications for developmental therapists. Physical
and Occupational Therapy in Pediatrics 1986;6:255–81.
Curran 1979 {published data only (unpublished sought but not used)}
Curran CL, Kachoyeanos MK. The effects on neonates of
two methods of chest physical therapy. MCN. The American
Journal of Maternal Child Nursing 1979;4:309–13.
Duara 1983 {published data only}
Duara S, Bessard K, Keszler L, Artes D, Batzer K. Evaluation
of different percussion time intervals at chest physiotherapy
(CPT) on neonatal pulmonary function parameters.
Pediatric Research 1983;17:310A.
9Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Etches 1978 {published data only (unpublished sought but not used)}
Etches PC, Scott B. Chest physiotherapy in the newborn:
effect on secretions removed. Pediatrics 1978;62:713–5.
Finer 1978 {published data only (unpublished sought but not used)}∗ Finer NN, Boyd J. Chest physiotherapy in the neonate: a
controlled study. Pediatrics 1978;61:282–5.
Finer NN, Grace MG, Boyd J. Chest physiotherapy in the
neonate with respiratory distress. Pediatric Research 1977;
11:570.
Fiser 1985 {published data only (unpublished sought but not used)}
Fiser DH, Kluck W. The effect of chest physiotherapy and
tracheal suctioning on PaO2 in infants and children with
atelectasis. Chest 1985;88:S22.
Fitzpatrick 1988 {published data only}
Fitzpatrick MP, Bullock MI, Tudehope DI. Chest
physiotherapy for intubated infants with hyaline membrane
disease. New Zealand Journal of Physiotherapy 1988;16:
15–18.
Fox 1978 {published data only}
Fox WW, Schwartz JG, Shaffer TH. Pulmonary
physiotherapy in neonates: Physiologic changes and
respiratory management. Journal of Pediatrics 1978;92:
977–81.
Gajdosik 1985 {published data only}
Gajdosik CG. Transcutaneous monitoring of PO2 during
chest physical therapy in a premature infant. Physical and
Occupational Therapy in Pediatrics 1985;5:69–75.
Greisen 1985 {published data only}
Greisen G, Frederiksen PS, Hertel J, Christensen NJ.
Catecholamine response to chest physiotherapy and
endotracheal suctioning in preterm infants. Acta Paediatrica
Scandinavica 1985;74:525–9.
Hartrick 1982 {published data only (unpublished sought but not used)}
Hartrick J, Fluit L, Parrott J, Yu VY. A controlled-study
of chest physiotherapy methods in the newborn-infant.
Australian Paediatric Journal 1982;18:141.
Hartsell 1987 {published data only}
Hartsell MB. Chest physiotherapy and mechanical
vibration. Journal of Pediatric Nursing 1987;2:135–7.
Hough 1991 {published data only}
Hough A. Positioning vs vibrations in chest physiotherapy.
Chest 1991;100:1741.
James 1970 {published data only}
James J. The use of a mechanical vibrator during chest
physiotherapy. Physiotherapy 1970;56:31–2.
Kanarek 1980 {published data only}
Kanarek KS, Curran JS, Williams PR, Sidebottom RA,
Brown C. Changes in trans-cutaneous PO2 (TcPO2)
and transcutaneous PCO2 (TcPCO2) during chest
physiotherapy in neonates. Clinical Research 1980;28:A875.
Leung 1998 {published data only (unpublished sought but not used)}
Leung A. MSc dissertation abstract session. A study of
two different chest physiotherapy percussion techniques
on some physiological changes in neonates. Hong Kong
Physiotherapy Journal 1988;16:19.
Luther 1981 {published data only}
Luther U, Friedrich H, Schramm D. Physiotherapy in
intensive care of premature infants and newborns. Zeitschrift
fur Physiotherapie 1981;33:457–61.
Main 2001 {published data only (unpublished sought but not used)}∗ Main E. The effect of physiotherapy on respiratory
function in ventilated children. PhD thesis, University
College, London 2001.
Main E, Castle R, Newham D, Stocks J. Respiratory
physiotherapy vs suction: the effects on respiratory function
in ventilated infants and children. Intensive Care Medicine
2004;30:1144–51.
Main E, Stocks J. The influence of physiotherapy and
suction on respiratory deadspace in ventilated children.
Intensive Care Medicine 2004;30:1152–9.
Meier 1979 {published data only}
Meier P. CPT - which method, if any?. MCN American
Journal of Maternal Child Nursing 1979;4:310–1.
Meyer 1984 {published data only}
Meyer CL. Chest physiotherapy in infants requiring
ventilatory assistance. Respiratory Therapy 1984;14:27-9,
32-4.
Murai 1994 {published data only}
Murai D, Grant J. Continuous oscillation therapy improves
the outcome of intubated newborns: results of a prospective,
randomized controlled trial. Neonatal Intensive Care 1995;
8:18.∗ Murai DT, Grant JW. Continuous oscillation therapy
improves the pulmonary outcome of intubated newborns
- results of a prospective, randomized, controlled trial.
Critical Care Medicine 1994;22:1147–54.
Paratz 1994 {unpublished data only}
Paratz J. The effect of respiratory physiotherapy on
intracranial dynamics in preterm and term infants. PhD
thesis, University of Queensland, Brisbane. 1994.
Parker 1985 {published data only}
Parker AE. Chest physiotherapy in the neonatal intensive
care unit. Physiotherapy 1985;71:63–5.
Remondiere 1976 {published data only}
Remondiere R, Relier JP, Esclapez P, Beaudoin J. Value
of respiratory physiotherapy in the treatment of hyaline
membrane disease in the newborn. Annales de Pediatrie
1976;23:617–23.
Schultz 2005 {published data only}
Schultz TR, Lin R, Francis BA, Hales RL, Colborn S,
Napoli LA, et al. Kinetic therapy improves oxygenation
in critically ill pediatric patients. Pediatric Critical Care
Medicine 2005;6:428–34.
Stiller 1996 {published data only}
Stiller K, Jenkins S, Grant R, Geake T, Taylor J, Hall B.
Acute lobar atelectasis: a comparison of five physiotherapy
regimens. Physiotherapy Theory and Practice 1996;12:
197–209.
10Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Storni 2003 {published data only}
Storni V. Role of respiratory physiotherapy for diagnosed
infants. Revue Des Maladies Respiratoires 2003;20:
S189–S193.
Tudehope 1980 {published data only (unpublished sought but not
used)}
Tudehope DI, Bagley C. Techniques of physiotherapy in
intubated babies with the respiratory distress syndrome.
Australian Paediatric Journal 1980;16:226–8.
Unoki 2005 {published data only}
Unoki T, Kawasaki Y, Mizutani T, Fujino Y, Yanagisawa
Y, Ishimatsu S, Tet al. Effects of expiratory rib-cage
compression on oxygenation, ventilation, and airway-
secretion removal in patients receiving mechanical
ventilation. Respiratory Care 2005;50:1430–7.
Warner 1984 {published data only}
Warner A. Does chest physiotherapy move airway secretions?
. American Review of Respiratory Disease 1984;130:701–2.
Warwick 2004 {published data only}
Warwick W, Wielinski C, Hansen L. Comparison of
expectorated sputum after manual chest physical therapy
and high-frequency chest compression. Biomedical
Instrumentation and Technology 2004;38:470–5.
Wong 2006 {published data only}
Wong I, Fok TF. Effects of lung squeezing technique on
lung mechanics in mechanically-ventilated preterm infants
with respiratory distress syndrome. Hong Kong Physiotherapy
Journal 2006;24:39–46.
References to ongoing studies
Hough 2007 {unpublished data only}
Hough J, Johnston L, Brauer S, Woodgate P. The effect of
chest physiotherapy on lung function in preterm infants.
PhD thesis in progress: University of Queensland, Australia.
Additional references
ANZNN 2005
Abeywardana S. The report of the Australian and New
Zealand Network, 2003. Sydney: ANZNN, 2005.
Balaguer 2006
Balaguer A, Escribano J, Roque M. Infant position in
neonates receiving mechanical ventilation. Cochrane
Database of Systematic Reviews 2006, Issue 4. [Art. No.:
CD003668. DOI: 10.1002/14651858.CD003668.pub2]
Cowan 1985
Cowan F, Thoresen M. Changes in superior sagittal sinus
blood velocities due to postural alterations and pressure
on the head of the newborn infant. Pediatrics 1985;75:
1038–47.
Crane 1978
Crane LD, Zombek M, Krauss AN, Auld PAM. Comparison
of chest physiotherapy techniques in infants with HMD.
Pediatric Research 1978;12:559–9.
Cross 1992
Cross JH, Harrison CJ, Preston PR, Rushton DI, Newell SJ,
Morgan ME, et al. Postnatal encephaloclastic porencephaly
- a new lesion?. Archives of Disease in Childhood 1992;67:
307–11. [1468–2044]
Dabezies 1997
Dabezies EJ, Warren PD. Fractures in very low birth weight
infants with rickets. Clinical Orthopaedics Related Research
1997;Feb:233–9.
Ehrlich 1972
Ehrlich R, Arnon RG. The intermittent endotracheal
intubation technique for the treatment of recurrent
atelectasis. Pediatrics 1972;50:144–7.
Emery 1983
Emery JR, Peabody JL. Head position affects intracranial
pressure in newborn infants. Journal of Pediatrics 1983;103:
950–3.
Etches 1978
Etches PC, Scott B. Chest physiotherapy in the newborn:
effect on secretions removed. Pediatrics 1978;62:713–5.
Flenady 2002
Flenady VJ, Gray PH. Chest physiotherapy for preventing
morbidity in babies being extubated from mechanical
ventilation. Cochrane Database of Systematic Reviews
2002, Issue 2. [Art. No.: CD000283. DOI: 10.1002/
14651858.CD000283]
Handbook 2007
Higgins JPT, Green S, editors. Assessment of study
quality. Cochrane Handbook for Systematic Reviews of
Interventions 4.2.6 [updated September 2006]; Section 6.
The Cochrane Library 2007, issue 2.
Harding 1998
Harding JE, Miles FK, Becroft DM, Allen BC, Knight DB.
Chest physiotherapy may be associated with brain damage
in extremely premature infants. Journal of Pediatrics 1998;
132:440–4.
Higgins 2002
Higgins J, Thompson S. Quantifying heterogeneity in
meta-analysis. Statistics in Medicine 2002;21:1539–58.
Mackenzie 1985
Mackenzie CF, Shin B. Cardiorespiratory function before
and after chest physiotherapy in mechanically ventilated
patients with post-traumatic respiratory failure. Critical
Care Medicine 1985;13:483–6.
Papile 1978
Papile L, Burstein J, Burstein R, Koffler H. Incidence
and evolution of subependymal and intraventricular
hemorrhage: a study of infants with birth weights less than
1,500gm. The Journal of Pediatrics 1978;92:529–34.
Pritchard 2001
Pritchard M, Flenady V, Woodgate P. Preoxygenation for
tracheal suctioning in intubated, ventilated newborn infants.
Cochrane Database of Systematic Reviews 2001, Issue 1. [Art.
No.: CD000427. DOI: 10.1002/14651858.CD000427]
11Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Purohit 1975
Purohit DM, Caldwell C, Levkoff AH. Letter: Multiple rib
fractures due to physiotherapy in a neonate with hyaline
membrane disease. American Journal of Diseases of Children
1975;129:1103–4. [MEDLINE: medline; neonatal;
physiotherapy; 0002–922X]
Raval 1987
Raval D, Yeh TF, Mora A, Cuevas D, Pyati S, Pildes RS.
Chest physiotherapy in preterm infants with RDS in the
first 24 hours of life. Journal of Perinatology 1987;7:301–4.
RevMan 2003 [Computer program]
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). Version 4.2 for Windows.
Copenhagan: The Nordic Cochrane Centre, The Cochrane
Collaboration, 2003.
Spence 2003
Spence K, Gillies D, Waterworth L. Deep versus shallow
suction of endotracheal tubes in ventilated neonates and
young infants. Cochrane Database of Systematic Reviews
2003, Issue 3. [Art. No.: CD003309. DOI: 10.1002/
14651858.CD003309]
Stiller 1990
Stiller K, Geake T, Taylor J, Grant R, Hall B. Acute lobar
atelectasis: a comparison of two chest physiotherapy
regimens. Chest 1990;98:1336–40.
Tudehope 1980
Tudehope DI, Bagley C. Techniques of physiotherapy in
intubated babies with the respiratory distress syndrome.
Australian Paediatric Journal 1980;16:226–8.
Wallis 1999
Wallis C, Prasad A. Who needs chest physiotherapy?
Moving from anecdote to evidence. Archives of Disease in
Childhood 1999;80:393–7.
Woodgate 2001
Woodgate PG, Flenady V. Tracheal suctioning without
disconnection in intubated ventilated neonates. Cochrane
Database of Systematic Reviews 2001, Issue 2. [Art. No.:
CD003065. DOI: 10.1002/14651858.CD003065]
Zach 1987
Zach MS, Oberwaldner B. Chest physiotherapy - the
mechanical approach to antiinfective therapy in cystic
fibrosis. Infection 1987;15:381–4.∗ Indicates the major publication for the study
12Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
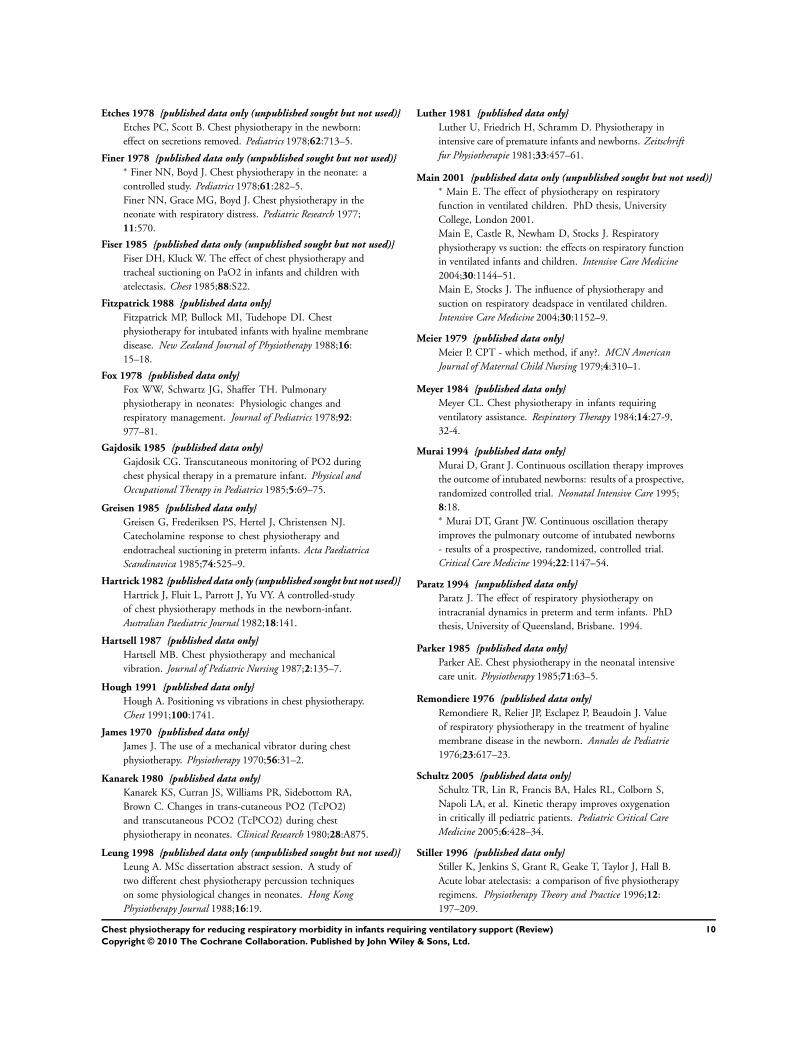
Peters 1983
Methods Blinding of randomisation - Unclear
Blinding of intervention - No
Blinding of outcome measure - Can’t tell
Complete follow-up - Yes
Participants 30 newborn infants who required intubation
Main diagnosis: 16 infants had HMD; the remainder had a variety of diagnoses
Gestational age: 25 to 42 weeks
Birth weight: 750 to 4030 grams
Postnatal age: 1 to 10 days
Conducted in Edmonton, Canada
Interventions Two period cross-over design with 2 CPT groups:
Bennett face mask
Contact heel percussion
Each technique was performed once only during postural drainage of both the upper and lower lobes and
was followed by saline instillation and suction of the ETT
Outcomes Heart rate
Mean arterial pressure (MAP)
Intracranial pressure (ICP)
TcpO2
TcpCO2
All taken pre and post CPT as well as post postural drainage, saline instillation and suctioning
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Allocation concealment? Unclear risk B - Unclear
Raval 1987
Methods Blinding of randomisation - Unclear. Randomly assigned to 2 groups
Blinding of intervention - No
Complete follow-up - Yes
Blinding of outcome measure - No
Participants 20 preterm infants who required endotracheal intubation and assisted ventilation
Main diagnosis: all infants had RDS
Gestation age: 28 to 32 weeks
13Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
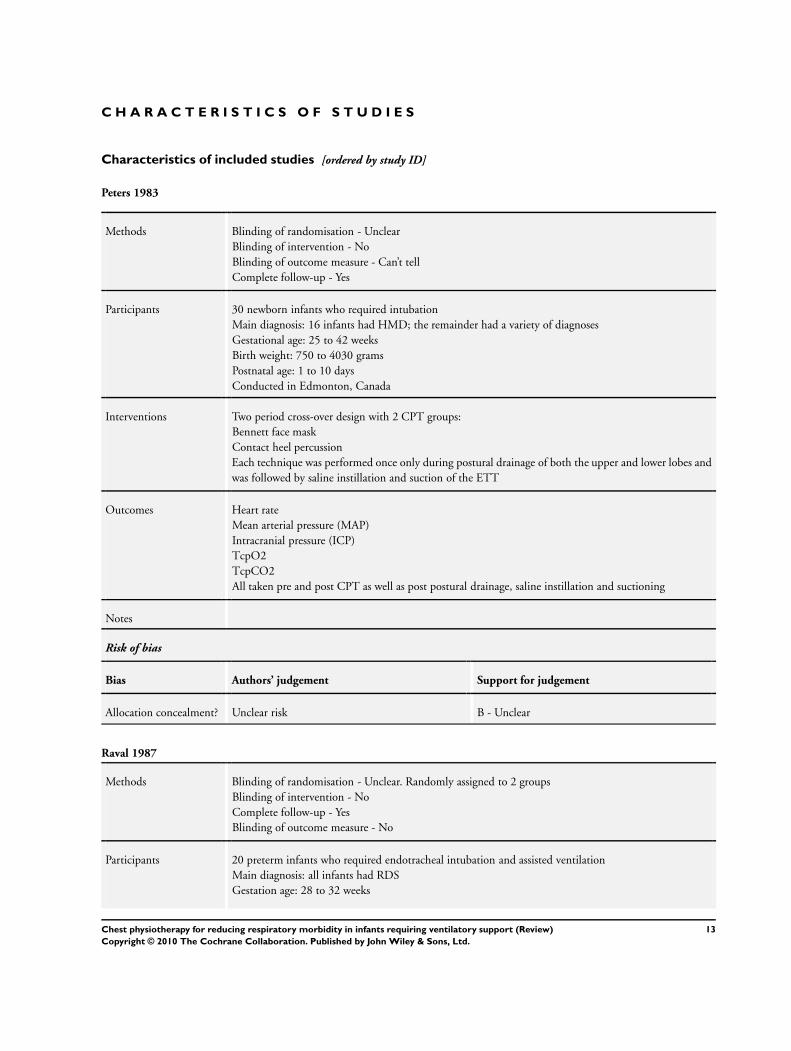
Raval 1987 (Continued)
Birth weight: 680 to 1870 grams
Postnatal age at study: 1 to 12 hours
Conducted in Chicago, USA
Interventions 2 arms - intervention, control
CPT group (n = 10): postural drainage with head up and head down, percussion, vibration and suctioning
All procedures performed every 2 to 3 hours in the first 24 hours of life
Control (n = 10): suctioning only
Outcomes Oxygenation: continuous TcPO2 monitoring, ABG samples
Secretion clearance: sputum weight per procedure
Rates of intracranial lesions by ultrasound scan
Mortality rate
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Allocation concealment? Unclear risk B - Unclear
Wong 2003
Methods Blinding of randomisation - Yes. Computerised random number allocation in sealed opaque envelopes,
stratified by mode of ventilation (HFOV or CMV)
Blinding of intervention - No
Complete follow-up - Yes
Blinding of outcome measure - Yes
Participants 56 neonates who required mechanical ventilation were randomised - 2 withdrawals due to critical condi-
tions (1 from each group)
Main diagnosis: atelectasis (segmental or lobar collapse)
Gestational age: 22 to 36 weeks
Birth weight: 540 to 2900 grams
Exclusions: persistent pulmonary hypertension, meconium aspiration syndrome, congenital heart defects,
pneumonia presenting with generalised patchy consolidation, post-cardiothoracic surgery, pleural effusion
and pneumothorax
Conducted in Shatin, Hong Kong
Interventions 2 arms - 2 intervention groups:
Lung squeezing technique (LST) (n = 26) - 3 or 4 sustained chest compressions lasting for about 5 seconds
followed by a slow gentle release in the supine position with bed flat
Postural drainage, percussion, vibration (PDPV) (n = 30) - performed in alternate side lying with bed flat
Both techniques were proceeded by endotracheal suctioning
Sessions were performed twice daily
14Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wong 2003 (Continued)
Outcomes Re-expansion of atelectasis
Recurrence of atelectasis
Duration of ventilation
Duration of oxygen dependency
Oxygenation: oxygen saturation
Secretion clearance: sputum volume per procedure per baby
Rates of intracranial lesions by ultrasound scan
Mortality rate
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Allocation concealment? Low risk A - Adequate
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Andersen 1991 Not a randomised trial - review article
Beaudoin 1973 Not a randomised trial - review article
Becroft 1998 Not a randomised trial
Bradbury 1996 Babies on nasopharyngeal CPAP - not mechanically ventilated
Cabero 1987 Not a randomised trial
Coradello 1979 Not a randomised trial
Coradello 1982 Not a randomised trial - cross-over study
Crane 1978 Abstract only - unable to contact author for further information
Crane 1986 Not a randomised trial - review article
Curran 1979 Eligible for inclusion but did not have sufficient data to enable outcomes to be calculated. Primary author was
contacted but was unable to supply the information required
Duara 1983 Not a randomised trial - case control study
15Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Etches 1978 Eligible for inclusion but did have have standard deviations to enable outcomes to be calculated. Primary author
was contacted but was unable to supply the information required
Finer 1978 Eligible for inclusion but data supplied was combined for ventilated infants and infants on CPAP. Primary author
was contacted but was unable to supply the information required
Fiser 1985 Eligible for inclusion but despite contacting primary author no further data were supplied
Fitzpatrick 1988 Not a randomised trial - case control study
Fox 1978 Not a randomised trial - case control study
Gajdosik 1985 Not a randomised trial - case report
Greisen 1985 Not a randomised trial - case control study
Not assessing respiratory outcome measures
Hartrick 1982 Abstract only - unable to contact author for further information
Hartsell 1987 Not newborn infants - children and adults with cystic fibrosis and bronchiectasis
Hough 1991 Not a randomised trial or newborn infants
James 1970 Not a randomised trial - report on technique
Kanarek 1980 Not a randomised trial - case control study
Leung 1998 Eligible for inclusion but despite contacting primary author no further data were supplied
Luther 1981 Not a randomised trial - case reports
Main 2001 Not newborn infants with respiratory distress - any studied newborns had cardiac conditions
Meier 1979 Not a randomised trial - a letter
Meyer 1984 Not a randomised trial - review article
Murai 1994 Intervention not physiotherapy - postural therapy
Paratz 1994 Not a randomised trial - case control study
Parker 1985 Not a randomised trial - review article
Remondiere 1976 Not a randomised trial - case report
Schultz 2005 Not newborn infants - greater than 8 months of age
16Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Stiller 1996 Not newborn infants - adult population
Storni 2003 Not newborn infants with neonatal respiratory disease - infants had cystic fibrosis
Tudehope 1980 Eligible for inclusion but did not have have enough data for outcomes to be calculated. Primary author was
contacted but was unable to supply the information required
Unoki 2005 Not newborn infants
Warner 1984 Not a randomised trial - review article
Warwick 2004 Not newborn infants
Wong 2006 Not a randomised trial - cohort study
Characteristics of ongoing studies [ordered by study ID]
Hough 2007
Trial name or title The effect of chest physiotherapy on lung function in the preterm infant
Methods Blinding of randomisation - Yes. Computerised random number allocation in sealed opaque envelopes.
Blinding of intervention - No
Blinding of outcomes measures - Yes
Complete follow-up - Yes
Participants Ventilated preterm infants in whom active CPT is indicated
Main diagnosis: atelectasis
Gestation age: < 34 weeks
Birth weight: > 750 grams
Conducted in Brisbane, Australia
Interventions Cross-over design with 2 CPT groups:
Cupping with face mask
Vibration
Techniques performed 4 hours apart
After CPT, saline instillation and suction to be performed
Outcomes Ventilation distribution: measured by electrical impedance tomography
Oxygenation: saturation monitoring
Rates of intracranial lesions by ultrasound scan
Starting date October 2006
Contact information [email protected]
17Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hough 2007 (Continued)
Notes
18Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. Active chest physiotherapy vs no active chest physiotherapy
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Weight of secretions cleared per
procedure per day (g)
1 20 Mean Difference (IV, Fixed, 95% CI) 0.01 [-0.10, 0.12]
2 Intraventricular haemorrhage 1 20 Risk Ratio (M-H, Fixed, 95% CI) 2.33 [0.83, 6.54]
3 IVH grade 3 or 4 1 20 Risk Ratio (M-H, Fixed, 95% CI) 11.0 [0.69, 175.86]
Comparison 2. Comparison of active chest physiotherapy techniques (percussion vs cupping)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Hypoxaemia per procedure per
baby
1 60 Risk Ratio (M-H, Fixed, 95% CI) 0.53 [0.28, 0.99]
2 % change in FiO2 per procedure
per baby
1 60 Mean Difference (IV, Fixed, 95% CI) -9.68 [-14.16, -5.20]
Comparison 3. Comparison of active chest physiotherapy techniques (LST vs PDPV)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Non-resolution of atelectasis
after initial intervention
1 56 Risk Ratio (M-H, Fixed, 95% CI) 0.25 [0.11, 0.57]
2 Secretions cleared (<0.2 ml) per
procedure per baby
1 56 Risk Ratio (M-H, Fixed, 95% CI) 0.96 [0.62, 1.49]
3 IVH grade 3 or 4 after
commencement of CPT
1 56 Risk Ratio (M-H, Fixed, 95% CI) 0.87 [0.35, 2.17]
4 Periventricular leucomalacia 1 56 Risk Ratio (M-H, Fixed, 95% CI) 0.87 [0.21, 3.52]
19Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.1. Comparison 1 Active chest physiotherapy vs no active chest physiotherapy, Outcome 1
Weight of secretions cleared per procedure per day (g).
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 1 Active chest physiotherapy vs no active chest physiotherapy
Outcome: 1 Weight of secretions cleared per procedure per day (g)
Study or subgroup CPT Suction onlyMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Raval 1987 10 0.09 (0.11) 10 0.08 (0.14) 100.0 % 0.01 [ -0.10, 0.12 ]
Total (95% CI) 10 10 100.0 % 0.01 [ -0.10, 0.12 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.18 (P = 0.86)
Test for subgroup differences: Not applicable
-0.1 -0.05 0 0.05 0.1
Favours suction only Favours CPT
Analysis 1.2. Comparison 1 Active chest physiotherapy vs no active chest physiotherapy, Outcome 2
Intraventricular haemorrhage.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 1 Active chest physiotherapy vs no active chest physiotherapy
Outcome: 2 Intraventricular haemorrhage
Study or subgroup CPT Suction only Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Raval 1987 7/10 3/10 100.0 % 2.33 [ 0.83, 6.54 ]
Total (95% CI) 10 10 100.0 % 2.33 [ 0.83, 6.54 ]
Total events: 7 (CPT), 3 (Suction only)
Heterogeneity: not applicable
Test for overall effect: Z = 1.61 (P = 0.11)
0.2 0.5 1 2 5
Favours CPT Favours suction only
20Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 Active chest physiotherapy vs no active chest physiotherapy, Outcome 3 IVH
grade 3 or 4.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 1 Active chest physiotherapy vs no active chest physiotherapy
Outcome: 3 IVH grade 3 or 4
Study or subgroup CPT Suction only Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Raval 1987 5/10 0/10 100.0 % 11.00 [ 0.69, 175.86 ]
Total (95% CI) 10 10 100.0 % 11.00 [ 0.69, 175.86 ]
Total events: 5 (CPT), 0 (Suction only)
Heterogeneity: not applicable
Test for overall effect: Z = 1.70 (P = 0.090)
0.01 0.1 1 10 100
Favours CPT Favours suction only
Analysis 2.1. Comparison 2 Comparison of active chest physiotherapy techniques (percussion vs cupping),
Outcome 1 Hypoxaemia per procedure per baby.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 2 Comparison of active chest physiotherapy techniques (percussion vs cupping)
Outcome: 1 Hypoxaemia per procedure per baby
Study or subgroup Percussion Cupping Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Peters 1983 9/30 17/30 100.0 % 0.53 [ 0.28, 0.99 ]
Total (95% CI) 30 30 100.0 % 0.53 [ 0.28, 0.99 ]
Total events: 9 (Percussion), 17 (Cupping)
Heterogeneity: not applicable
Test for overall effect: Z = 1.98 (P = 0.048)
0.5 0.7 1 1.5 2
Favours percussion Favours cupping
21Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Comparison of active chest physiotherapy techniques (percussion vs cupping),
Outcome 2 % change in FiO2 per procedure per baby.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 2 Comparison of active chest physiotherapy techniques (percussion vs cupping)
Outcome: 2 % change in FiO2 per procedure per baby
Study or subgroup Percussion CuppingMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Peters 1983 30 -6.11 (9.16) 30 3.57 (8.52) 100.0 % -9.68 [ -14.16, -5.20 ]
Total (95% CI) 30 30 100.0 % -9.68 [ -14.16, -5.20 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.24 (P = 0.000023)
Test for subgroup differences: Not applicable
-10 -5 0 5 10
Favours percussion Favours cupping
Analysis 3.1. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome
1 Non-resolution of atelectasis after initial intervention.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 3 Comparison of active chest physiotherapy techniques (LST vs PDPV)
Outcome: 1 Non-resolution of atelectasis after initial intervention
Study or subgroup LST PDPV Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wong 2003 5/26 23/30 100.0 % 0.25 [ 0.11, 0.57 ]
Total (95% CI) 26 30 100.0 % 0.25 [ 0.11, 0.57 ]
Total events: 5 (LST), 23 (PDPV)
Heterogeneity: not applicable
Test for overall effect: Z = 3.34 (P = 0.00084)
0.2 0.5 1 2 5
Favours LST Favours PDPV
22Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome
2 Secretions cleared (<0.2 ml) per procedure per baby.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 3 Comparison of active chest physiotherapy techniques (LST vs PDPV)
Outcome: 2 Secretions cleared (<0.2 ml) per procedure per baby
Study or subgroup LST PDPV Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wong 2003 15/26 18/30 100.0 % 0.96 [ 0.62, 1.49 ]
Total (95% CI) 26 30 100.0 % 0.96 [ 0.62, 1.49 ]
Total events: 15 (LST), 18 (PDPV)
Heterogeneity: not applicable
Test for overall effect: Z = 0.17 (P = 0.86)
0.5 0.7 1 1.5 2
Favours LST Favours PDPV
Analysis 3.3. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome
3 IVH grade 3 or 4 after commencement of CPT.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 3 Comparison of active chest physiotherapy techniques (LST vs PDPV)
Outcome: 3 IVH grade 3 or 4 after commencement of CPT
Study or subgroup LST PDPV Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wong 2003 6/26 8/30 100.0 % 0.87 [ 0.35, 2.17 ]
Total (95% CI) 26 30 100.0 % 0.87 [ 0.35, 2.17 ]
Total events: 6 (LST), 8 (PDPV)
Heterogeneity: not applicable
Test for overall effect: Z = 0.31 (P = 0.76)
0.5 0.7 1 1.5 2
Favours LST Favours PDPV
23Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
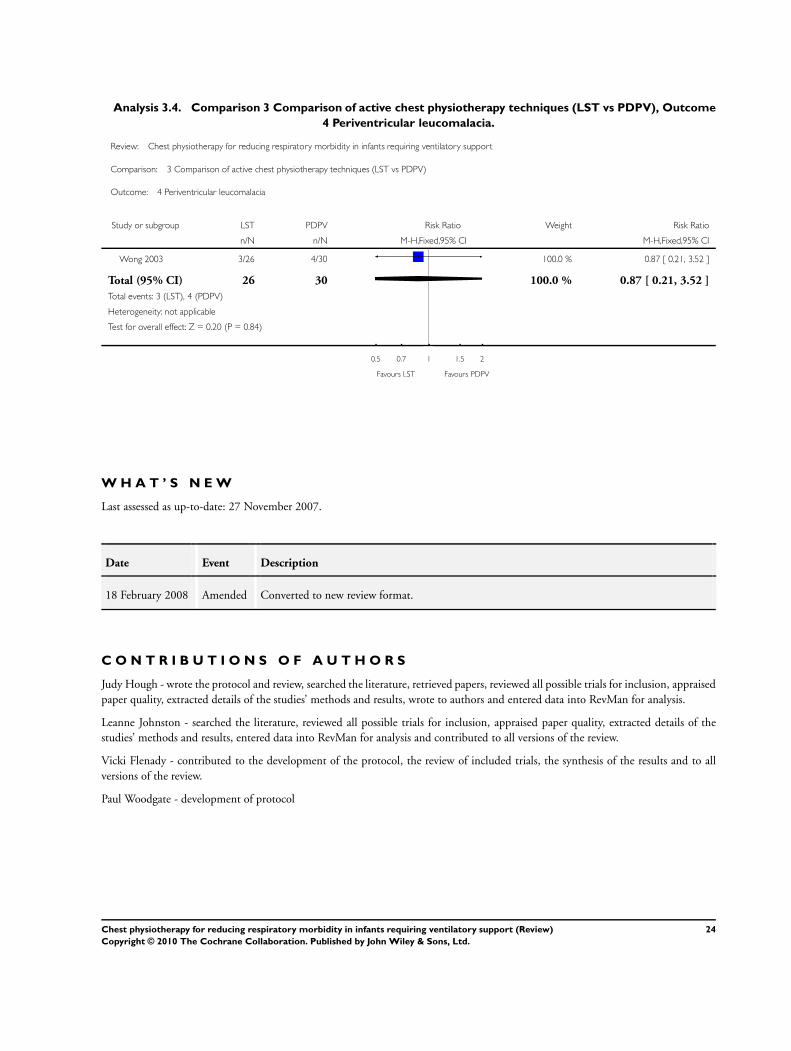
Analysis 3.4. Comparison 3 Comparison of active chest physiotherapy techniques (LST vs PDPV), Outcome
4 Periventricular leucomalacia.
Review: Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support
Comparison: 3 Comparison of active chest physiotherapy techniques (LST vs PDPV)
Outcome: 4 Periventricular leucomalacia
Study or subgroup LST PDPV Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Wong 2003 3/26 4/30 100.0 % 0.87 [ 0.21, 3.52 ]
Total (95% CI) 26 30 100.0 % 0.87 [ 0.21, 3.52 ]
Total events: 3 (LST), 4 (PDPV)
Heterogeneity: not applicable
Test for overall effect: Z = 0.20 (P = 0.84)
0.5 0.7 1 1.5 2
Favours LST Favours PDPV
W H A T ’ S N E W
Last assessed as up-to-date: 27 November 2007.
Date Event Description
18 February 2008 Amended Converted to new review format.
C O N T R I B U T I O N S O F A U T H O R S
Judy Hough - wrote the protocol and review, searched the literature, retrieved papers, reviewed all possible trials for inclusion, appraised
paper quality, extracted details of the studies’ methods and results, wrote to authors and entered data into RevMan for analysis.
Leanne Johnston - searched the literature, reviewed all possible trials for inclusion, appraised paper quality, extracted details of the
studies’ methods and results, entered data into RevMan for analysis and contributed to all versions of the review.
Vicki Flenady - contributed to the development of the protocol, the review of included trials, the synthesis of the results and to all
versions of the review.
Paul Woodgate - development of protocol
24Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
JH and LJ are co-investigators in a trial investigating the effect of CPT techniques on lung function in the preterm infant for JH’s PhD
thesis (2005 to 2007).
S O U R C E S O F S U P P O R T
Internal sources
• Centre for Clinical Studies, Mater Mothers’ Hospital, South Brisbane, Queensland, Australia.
• Mater Research Support Centre, Mater Health Services, South Brisbane, Queensland, Australia.
• School of Health and Rehabilitation Studies, University of Queensland, Australia.
External sources
• Evidence Based Practice Grant, Queensland Health, Australia.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Mucus [∗secretion]; Percussion [methods]; Pulmonary Atelectasis [∗therapy]; Randomized Controlled Trials as Topic; Respiration,
Artificial [∗adverse effects]; Respiratory Therapy [∗methods]; Suction; Vibration [therapeutic use]
MeSH check words
Humans; Infant; Infant, Newborn
25Chest physiotherapy for reducing respiratory morbidity in infants requiring ventilatory support (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.