Embed Size (px)
Citation preview

Abstract / Clinical Radiology 69 (2014) S11eS22S16
had been appropriately requested by the radiologist but not performedand the patients were recalled.1st action plan: These results were discussed at a local radiology meetingto ensure that radiologists request STIR when spondyloarthropathy issuspected. The results were then used in the formation of a new MRIprotocol for the scanning of spondyloarthropathy, in order to reduce thechance that STIR will fail to be performed in the future.
Imaging of the cervical spine injury in elderly patients
Authors: Divyashree Mysore*, Sharath R. Hosmane, Reda Braham
Background: The RCR and NICE recommends developing local protocol forprimary imaging modality for cervical spine (CSPN) assessment of bluntcervical injury in elderly patients (>65 yrs). Literature suggests youngelderly (65 e 75yrs) are less likely to need further imaging than old elderly(>75yrs). Distinction reflects observed differences in functional decline,trauma mortality rates and osteoporosisStandard, indicator and target: Standard: 100% images should be tech-nically adequateAims:Assess adequacy of CSPN x-rays in patients ¼ />65yrsAssess difference in young elderly (65 e 75 yrs) and old elderly (>75yrs)patientsMethodology: CSPN x-rays from 1/1/2011 to 31/3/2013, requested forblunt injury from A&E for patients ¼ />65yrs were obtained from PACSResults of 1st audit round: 193 CSPN x- rays were performed with meanage of 78 years78.8% of the images were of adequate quality and 21.2% CSPN x-rays wereinadequate to diagnose CSPN injury. 35pts in old elderly group had inad-equate CSPN x-rays compared to 6pts in young elderly group (p ¼ 0.005).37.3% patients had CT CSPN following x-rays of CSPN for reasons of in-adequacy (21.2%), inconclusive (11.4%) and abnormal (4.7%)1st action plan: The results were presented in clinical governancemeeting. The adequacy criteria was presented to increase awareness. Theradiologists were advised to mention in report if x-rays are inadequate. Itwas agreed to have low threshold to perform CT spine in elderly patients,especially in patients aged >75 yrs. Re-audit will be performed
Traumatic knee pain e adequacy of clinical information withreference to the Ottawa knee rules
Authors: Bilal A. Sethi*, Karen A. Duncan, John Lee
Background: Acute knee injuries are common presentation but not allrequire knee x-rays. The Ottawa Knee rules (OKR) state that for patientspresenting with a history of knee trauma knee radiographs are onlyrequired if
- age 55 yrs or older,- tenderness at head of fibula,- isolated tenderness of patella,- inability to flex knee to 90- inability to bear weight both immediately and in the emergencydepartment (ED)
Standard, indicator and target: All knee x- ray requests for traumaticknee pain should be in line with OKR and provide adequate clinical in-formation including point tenderness.Indicator: Percentage of referrals providing adequate clinical informationwith reference to the Ottawa knee rules Target 95% compliance.Methodology: Retrospective review of ED referral details as suppliedelectronically, for patients who were referred for knee imaging.Results of 1st audit round: 100 consecutive knee x-ray referrals from EDwere analysed, covering period from 02-30/11/2013.
* Guarantor and correspondent: Divyashree Mysore* Guarantor and correspondent: Bilal A. Sethi* Guarantor and correspondent: Nik M. Nik-Hussin* Guarantor and correspondent: Tharunniya Vamadevan
36 excludedAdequate information ¼ 38Inadequate information ¼ 25Only 60% of knee x-ray requests for traumatic knee pain provided adequateclinical information with reference to OKR.1st action plan: Presented at ED meeting highlighting areas of noncompliance.Following steps taken:
i) Knee examination demonstration in ED teaching sessionii) Introducing OKR during junior doctors induction.iii) agreement to improve documentation and clinical information on
referrals.Results of 2nd round: Currently in the process of re-auditing.
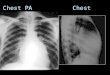
Chest staging in head and neck cancer patients: a multicentre regionalaudit
Authors: Nik M. Nik-Hussin*, Claire Barker, Niranjan Desai, SuzieBonington
Background: The chest is the commonest metastatic site for lar-yngopharyngeal cancers. The incidence of a 2nd synchronous tumour inthe thorax is between 4-30%. Sensitivity and specificity for detectinglung nodules is 100% and 95% for CT vs 33% and 97% for chest radiog-raphy. The Northwest Head & Neck Cancer Guidelines advocate CTthorax for staging prior to the multidisciplinary meeting to ensureefficient and timely management. The audit aimed to assess adherenceto regional guidelines.Standard, indicator and target: Standard: Northwest Head & Neck Im-aging Guidelines.Indicator: New patients should have a pre-MDT CT thorax.Target: 100%Methodology: Multicentre retrospective audit. New patients referred tothe regional MDTs from August-December 2013 were identified fromprospectively derived databases of the South and Central Manchester NHSTrusts and Pennine Acute Trust MDTs. Retrospective review of imaging onPACS was performed. Data was analysed as a combined cohort to reflectregional practice.Results of 1st audit round: 151 patients were identified. 70.2% hadappropriate chest imaging prior to the MDT. 14.5% only chest radiog-raphy.11.3% had imaging of the chest after the MDT and prior to surgery. Ofthese patients 7 patient had a chest radiograph and 10 patients had pre-operative CT. 4.0% had no chest imaging performed before or after theMDT. The target of 100% was not achieved.1st action plan: The results of the audit were presented at each RegionalMDT.Re-audit will be undertaken in a year.
The use of CT trauma protocols for patients with head injury in amajor trauma centre
Authors: Tharunniya Vamadevan*, Daniel Warren, JeremyMacmullen-Price, Ian Craven
Background: Leeds Teaching Hospitals recently became a Major TraumaCentre with a subsequent increase in trauma imaging. Standardised headtrauma protocols were introduced in September 2013 stating a volumeacquisition with 5mm soft tissue and 1mm bony reformats sent to PACS.Supervising Consultants were concerned that bony reformats were un-available at the time of reporting - either a discrepancy of the Radiogra-pher or on-call Radiologist. The audit originated following a discrepancy ofa missed skull base fracture on 3 mm reconstructions that later becameapparent on higher resolution imaging (case will be shown).