Embed Size (px)
Citation preview

10/15/2012
1
Chemotherapy in Luminal Breast Cancer: Choice of Regimen
Andrew D. Seidman, MDAttending Physician
Breast Cancer Medicine ServiceMemorial Sloan‐Kettering Cancer Center
Professor of MedicineWeill Cornell Medical College
Question
• Which of the following chemotherapy regimens are optimal options as adjuvant therapy for a 59 year old woman with a 1.7 cm., ER+, PR+, HER2 negative, node negative breast cancer with an 21‐Gene Recurrence Score of 30?
1. doxorubicin, cyclophosphamide and docetaxel (“TAC”)
2. cyclophosphamide + methotrexate + fluorouracil (CMF)
3. doxorubicin + cyclophosphamide followed by a taxane (AC‐T)
4. docetaxel + cyclophosphamide (“TC”)
5. doxorubicin + cyclophosphamide (AC)
6. FEC or FAC
The Questions: Choice of Chemotherapy for Luminal Breast Cancer
• Chemotherapy or Not?
• Anthracycline or Not?y
• Taxane or Not?
• Does Density Matter?

10/15/2012
2
It’s All About …The “Talk”
Metastatic Breast Cancer
5
Historical Perspective1985 NIH Consensus Conference:
Premenopausal, node (+) : Chemotherapy
Premenopausal, node (‐) : treatment not recommended,consider chemotherapy if "high risk"
Postmenopausal, node (+), ER (+) : tamoxifen
Postmenopausal, node (+), ER (‐) : consider chemotherapy,but cannot be recommended as standard practice
Postmenopausal, node (‐) : no routine adjuvant therapy,may be considered for certain "high‐risk" patients

10/15/2012
3
S1007: A Phase III, Randomized Clinical Trial of Standard S1007: A Phase III, Randomized Clinical Trial of Standard Adjuvant Endocrine Therapy +/Adjuvant Endocrine Therapy +/-- Chemotherapy in Patients Chemotherapy in Patients with 1with 1--3 Positive Nodes, Hormone Receptor3 Positive Nodes, Hormone Receptor--Positive and Positive and
HER2HER2--Negative Breast Cancer with Recurrence Score of 25 Negative Breast Cancer with Recurrence Score of 25 or Lessor Less
Ana M. GonzalezAna M. Gonzalez‐‐Angulo, M.D.Angulo, M.D.
Primary ObjectivePrimary Objective
To determine the effect of chemotherapy in To determine the effect of chemotherapy in patients with node positive breast cancer who patients with node positive breast cancer who do not have high RS by 21do not have high RS by 21--Gene RS AssayGene RS Assay
•• Patients with 1Patients with 1--3 positive nodes and HR+ and HER23 positive nodes and HR+ and HER2--•• Patients with 1Patients with 1--3 positive nodes, and HR+ and HER23 positive nodes, and HR+ and HER2--breast cancer with RS ≤ 25breast cancer with RS ≤ 25
•• DFS for patients treated with chemotherapy compared to DFS for patients treated with chemotherapy compared to no chemotherapy and dependence on the magnitude of no chemotherapy and dependence on the magnitude of RS. RS.
•• Determine the optimal Determine the optimal cutpointcutpoint for recommending for recommending chemotherapy or not.chemotherapy or not.
ChemotherapyChemotherapy
Second Generation RegimensSecond Generation Regimens
Third Generation RegimensThird Generation Regimens

10/15/2012
4
Biologic Heterogeneity Mandates Individualized
Treatment Approaches
21‐GeneRecurrence Score (RS) Assay
PROLIFERATIONKi‐67STK15SurvivinCyclin B1
ESTROGENERPRBcl2SCUBE2
16 Cancer and 5 Reference Genes From 3 Studies
RS = + 0.47 x HER2 Group Score - 0.34 x ER Group Score + 1.04 x Proliferation Group Score+ 0.10 x Invasion Group Score + 0.05 x CD68- 0.08 x GSTM1- 0.07 x BAG1Cyclin B1
MYBL2
SCUBE2
INVASIONStromelysin 3Cathepsin L2
HER2GRB7HER2
BAG1GSTM1
REFERENCEBeta‐actinGAPDHRPLPOGUSTFRC
CD68 Category RS (0-100)Low risk RS <18
Int risk RS ≥18 and <31
High risk RS ≥31
Paik et al. N Engl J Med. 2004;351:2817‐2826.
0.07 x BAG1
•
Standardized Quantitative 21‐Gene RS Assay: Node ‐, ER +
15%
20%
25%
30%
35%
40%
Recurr
ence a
t 10 Y
ears
Low Risk Group High Risk Group Intermediate Risk Group
0%
5%
10%
0 5 10 15 20 25 30 35 40 45 50
Recurrence Score
Dis
tant
1) Paik et al NEJM 2004, 2) Habel et al Breast Cancer Research 2006 3) Paik et al JCO 2006, 4) Gianni et al JCO 2005
Lower RS’s••Lower likelihood of recurrenceLower likelihood of recurrence••Greater magnitude of TAM benefitGreater magnitude of TAM benefit••Minimal, if any, chemotherapy benefitMinimal, if any, chemotherapy benefit
Higher RS’s••Greater likelihood of recurrenceGreater likelihood of recurrence••Lower magnitude of TAM benefitLower magnitude of TAM benefit••Clear chemotherapy benefitClear chemotherapy benefit

10/15/2012
5
Adjuvant Chemotherapy Regimens
CMF = AC
AC → P/DCAF/FAC CEF/FEC
DC
ddAC → P
// /
FEC → P/D
Differential Benefits by Subtype?
DAC(Tac)
AC ‐> wkly P
The Anthracyclines Have Been a Mainstay: Clear Benefits in Unselected Patients
3.7%
4.6%
EBCTCG, Lancet 2005
OS
Gennari A et al, JNCI 2008
OS

10/15/2012
6
Anthracycline sensitivity in HER2‐positives
TOP2Deleted
TOP2Normal
DiLeo SABCS 2008 (abs 705)
Normal
TOP2Amplified
Anthracycline for Luminals?
• Unique, serious, potential late toxicities (cardiac, AML, MDS)
• Total/near total alopecia
• Increased likelihood of nausea
• Some evidence of effectiveness in all subgroups
• Limited prospective, reproducible data demonstrating a lack of differential benefit in any subset
• Mixed retrospective, data demonstrating effectiveness limited to subsets
• Biomarker identification and testing is evolving
Adjuvant CMF or AC vs Capecitabine in women >65Capecitabine Alone for Selected Luminals?
Muss et al, NEJM 2009

10/15/2012
7
Meta‐analysis: Adjuvant taxane vs no taxane: DFS
Copyright © American Society of Clinical OncologyDe Laurentiis, M. et al. J Clin Oncol; 26:44‐53 2008
Meta‐analysis: Adjuvant taxane vs no taxane: OS
Copyright © American Society of Clinical Oncology
De Laurentiis, M. et al. J Clin Oncol; 26:44‐53 2008
Disease-free Survival among Patients Treated with or without Paclitaxel According to
Estrogen-Receptor Status and HER2 Expression
21Hayes DF et al. N Engl J Med 2007;357:1496-1506

10/15/2012
8
No paclitaxelbenefit
Each of these 3 subsets shows a statistically significant benefit from paclitaxel with small sample size
E1199: Best Taxane for Luminal BC?
Secondary Comparisons:Docetaxel Paclitaxel
q3w q1w q3w q1w
5-Year DFS 81.2% 77.6% 76.9% 81.5%
d t lit l 3HR: 1.23 HR: 1.09 HR: 1.0 HR: 1.27
Primary Comparisons:Paclitaxel vs. Docetaxel: HR: 1.032; P = 0.61
q3w vs. q1w: HR: 1.062; P = 0.33
compared to paclitaxel q3wP = 0.02 NS NS P = 0.006
Hormone Receptor Positive*
HR: 1.28
P = 0.03
HR: 1.15
NS
HR: 1.0
NS
HR: 1.20
NS
Hormone Receptor Negative*
HR: 1.08
NS
HR: 0.96
NS
HR: 1.0
NS
HR: 1.40
P = 0.02
5-Year OS 87.3% 86.2% 86.5% 89.7%
compared to paclitaxel q3wHR: 1.13
NS
HR: 1.02
NS
HR: 1.0
NS
HR: 1.32
P = 0.01
* Exploratory analysis
Meta‐analysis of disease‐free survival (DFS) according to ER status for Taxanes
Copyright © American Society of Clinical Oncology De Laurentiis, M. et al. J Clin Oncol; 26:44‐53 2008

10/15/2012
9
Meta‐analysis of disease‐free survival (DFS) according to HER‐2 status
Copyright © American Society of Clinical Oncology
De Laurentiis, M. et al. J Clin Oncol; 26:44‐53 2008
Weekly Paclitaxel was “equally superior” to every 3 Week Paclitaxel in Luminal or Triple Negs in E1199
HRHR HER2HER2 No. No. DFSDFS OSOS
Pos Neg 1213 1.31 1.36
(0.97, 1.72) p=0.05
(0.92, 2.00)
p=0.12
Neg Neg 462 1.37
(0.98, 1.93
P=0.07
1.33
(0.91, 1.94)
P=0.14
Taxane OR Anthracycline for Luminal BC?: US Oncology 9735
AC x 4 q3w
Doxorubicin (60 mg/m2)Cyclophosphamide (600 mg/m2)
n=510
• N=1016• 71% ER+• 48% N–
TC x 4 q3w
Docetaxel (75 mg/m2) Cyclophosphamide (600 mg/m2)
n=506
Eligibility: Stage I, II, or III disease
R
Jones et al. J Clin Oncol. 2006;24:5381‐5387.

10/15/2012
10
TC vs AC: DFS and OS
Copyright © American Society of Clinical Oncology
From: Jones, S. et al. J Clin Oncol; 27:1177‐1183 2009
Summary of unplanned, exploratory analyses of disease-free survival hazard ratios (HR) and CI
Docetaxel/cyclophosphamide (TC) is favored left of 1.
Jones S et al. JCO 2009;27:1177-1183
©2009 by American Society of Clinical Oncology
US Oncology 06090TC versus TAC in HER2 (‐):
(Relative Contribution of A added to to T in Luminals?)
N = 2000
From: http://www.usoncology.com/portal/page/portal/PubWeb/2CancerCareNetwork/03USOncologyResearch/X_ClinicalResearch/X_ClinicalTrialsDetail?PSTUDYNUM=06090PI: J. Blum
80% power to detect a 3.4% DFS advantage for the anthracycline
10/15/2012
11
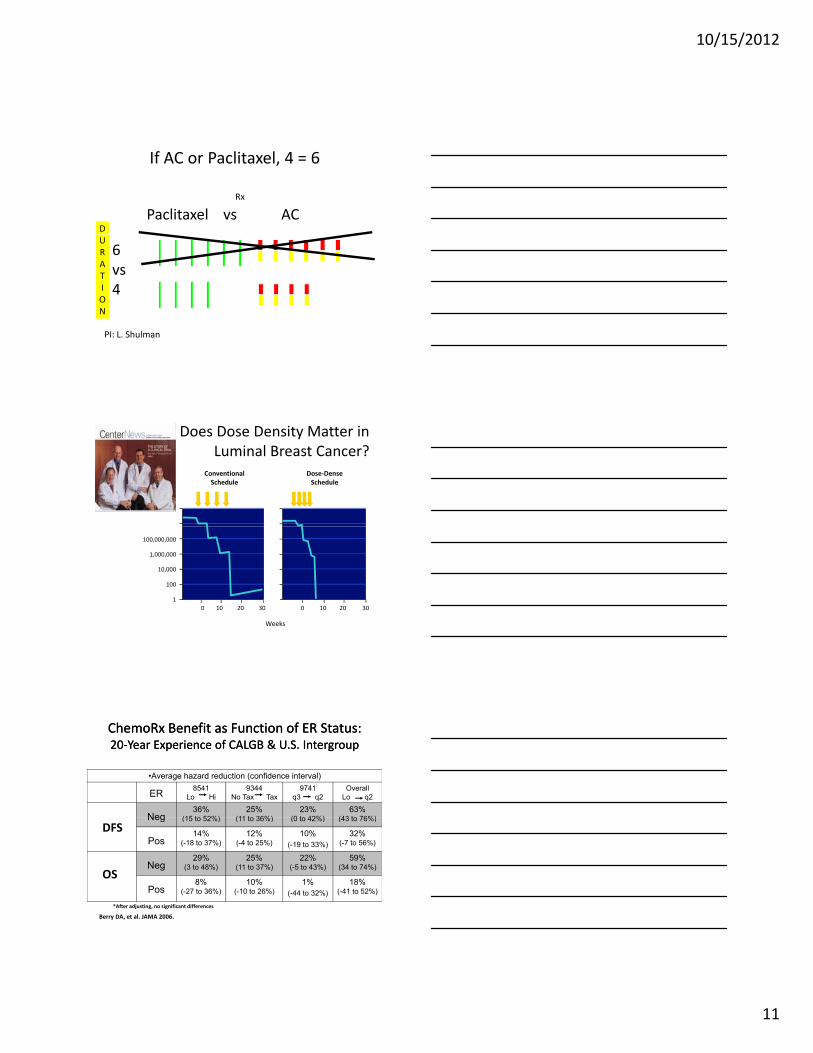
If AC or Paclitaxel, 4 = 6
Rx
Paclitaxel vs ACD
PI: L. Shulman
6vs 4
URATION
Does Dose Density Matter in Luminal Breast Cancer?
1,000,000,000,000
10,000,000,000
ConventionalSchedule
Dose‐DenseSchedule
10,000,000,000
100,000,000
1,000,000
10,000
100
1
0 10 20 30 0 10 20 30
Weeks
Cell number
ChemoRx Benefit as Function of ER Status: 20‐Year Experience of CALGB & U.S. IntergroupChemoRx Benefit as Function of ER Status: 20‐Year Experience of CALGB & U.S. Intergroup
•Average hazard reduction (confidence interval)
ER8541
Lo Hi9344
No Tax Tax9741
q3 q2Overall
Lo q2
Neg36%
(15 to 52%)25%
(11 to 36%)23%
(0 to 42%)63%
(43 to 76%)
*After adjusting, no significant differences
Berry DA, et al. JAMA 2006.
Neg (15 to 52%) (11 to 36%) (0 to 42%) (43 to 76%)
Pos14%
(-18 to 37%)12%
(-4 to 25%)10%
(-19 to 33%)
32%(-7 to 56%)
Neg29%
(3 to 48%)25%
(11 to 37%)22%
(-5 to 43%)59%
(34 to 74%)
Pos8%
(-27 to 36%)10%
(-10 to 26%)1%
(-44 to 32%)
18%(-41 to 52%)
DFS
OS

10/15/2012
12
R Negative
20‐Year Experience of CALGB & U.S. Intergroup20‐Year Experience of CALGB & U.S. Intergroup
DFS CALGB 8541
DFSCALGB 9344
DFSCALGB 9741
ChemoRx Benefit as Function of ER Status:
ERER
Positive
Years Years Years
Berry DA, et al. JAMA 2006
Ultimately, It May Be What Comes AFTER ChemoRx That Matters Most in Luminal BCs!
COMPARISON OF TAILORX AND MINDACT TRIALS
TAILORx MINDACT
Groups TBCI BIG
Population Node‐neg, ER+ Node‐neg, ER+/‐
Assay 21 gene RS™ 70 gene Prognostic Signature
Utility Scale & Level of Evidence
+ or ++II
+ or ++IIILevel of Evidence II III
Tissue FPET Fresh or frozen
Accrual Goal ~10,500 ~6,000
Randomized group RS 11‐25 (40%) Discordant risk (32%)
RandomizationTreat with hormones+/‐ chemotherapy
Treat by clinical vs. genomic risk
Non‐randomized groupsRS < 11: HormonesRS > 25: Chemo+ hormones
Both low risk (13%):HormonesBoth high risk (55%): Chemo
hormones
10/15/2012
13
Question
• Which of the following chemotherapy regimens are optimal options as adjuvant therapy for a 59 year old woman with a 1.7 cm., ER+, PR+, HER2 negative, node negative breast cancer with an 21‐Gene Recurrence Score of 30?
1. doxorubicin, cyclophosphamide and docetaxel (“TAC”)
2. cyclophosphamide + methotrexate + fluorouracil (CMF)
3. doxorubicin + cyclophosphamide followed by a taxane (AC‐T)
4. docetaxel + cyclophosphamide (“TC”)
5. doxorubicin + cyclophosphamide (AC)
6. FEC or FAC
My Choice:
CMF
Take Home Points:Adjuvant Chemotherapy for Luminal A Breast Cancer
• Relative benefit of chemotherapy in this intrinsic subset is modest
• Anti‐estrogen therapy plays a (the) major role in risk reductionreduction
• Incremental differences in efficacy between 1st, 2nd, and 3rd generation regimens are negligible while differences in early and late toxicities may not be
• “First do no harm”, or at least “first do as little harm as possible”

10/15/2012
14
It’s Our Time





























