Embed Size (px)
Citation preview
Chemotherapy in Advanced Gastric Cancer: A SystematicReview and Meta-Analysis Based on Aggregate DataAnna D. Wagner, Wilfried Grothe, Johannes Haerting, Gerhard Kleber, Axel Grothey, and Wolfgang E. Fleig
A B S T R A C T
PurposeThis systematic review and meta-analysis were performed to assess the efficacy and tolerabilityof chemotherapy in patients with advanced gastric cancer.
MethodsRandomized phase II and III clinical trials on first-line chemotherapy in advanced gastric cancerwere identified by electronic searches of Medline, Embase, the Cochrane Controlled TrialsRegister, and Cancerlit; hand searches of relevant abstract books and reference lists; and contactto experts. Meta-analysis was performed using the fixed-effect model. Overall survival, reportedas hazard ratio (HR) with 95% CI, was the primary outcome measure.
ResultsAnalysis of chemotherapy versus best supportive care (HR � 0.39; 95% CI, 0.28 to 0.52) andcombination versus single agent, mainly fluorouracil (FU) -based chemotherapy (HR � 0.83; 95%CI � 0.74 to 0.93) showed significant overall survival benefits in favor of chemotherapy andcombination chemotherapy, respectively. In addition, comparisons of FU/cisplatin-containingregimens with versus without anthracyclines (HR � 0.77; 95% CI, 0.62 to 0.95) and FU/anthracycline-containing combinations with versus without cisplatin (HR � 0.83; 95% CI, 0.76 to0.91) both demonstrated a significant survival benefit for the three-drug combination.Comparing irinotecan-containing versus nonirinotecan-containing combinations (mainly FU/cisplatin) resulted in a nonsignificant survival benefit in favor of the irinotecan-containingregimens (HR � 0.88; 95% CI, 0.73 to 1.06), but they have never been compared against athree-drug combination.
ConclusionBest survival results are achieved with three-drug regimens containing FU, an anthracycline,and cisplatin. Among these, regimens including FU as bolus exhibit a higher rate of toxicdeaths than regimens using a continuous infusion of FU, such as epirubicin, cisplatin, andcontinuous-infusion FU.
J Clin Oncol 24:2903-2909. © 2006 by American Society of Clinical Oncology
INTRODUCTION
Despite a sharp decline of its incidence during thesecond half of the 20th century, gastric cancerremains the second leading cause of cancer mor-tality in the world.1 Infection with Helicobacterpylori, atrophic gastritis, intestinal metaplasia,and dysplasia have been identified as importantsteps in the pathogenesis of gastric adenocarcino-ma,2 whereas Barrett’s esophagus and dysplasiaare associated with the development of esopha-geal adenocarcinoma.3 The incidence of this can-cer in white males increased more than 3.5-foldbetween 1974 and 1994 in the United States,which is more than that of any other malignancy.Similar observations have been made in otherWestern countries.4,5 Because it is difficult to
determine whether these cancers are gastroesoph-ageal junction tumors or distal esophageal malig-nancies, they are usually treated in the samemanner in clinical trials for advanced disease.
In the Western world, most gastric cancerpatients are diagnosed when the tumor is in-operable. For these patients, systemic chemother-apy is the main treatment option. Although alarge number of chemotherapy regimens havebeen tested in randomized studies, there is nointernationally accepted standard of care, and un-certainty remains regarding the choice of the reg-imen. Therefore, we performed a systematicreview and meta-analysis of randomized phase IIand III treatment trials to assess the efficacy andtolerability of chemotherapy in patients with ad-vanced gastric cancer.
From the First Department of Medicine,Coordinating Centre for Clinical Trials,Department of Medicine IV, and Insti-tute of Medical Epidemiology, Biostatis-tics and Informatics, Martin-Luther-University Halle-Wittenberg, Halle/Saale, Germany; and Mayo ClinicCollege of Medicine, Rochester, MN.
Submitted November 22, 2005; acceptedMarch 8, 2006.
Support for the Coordinating Centre forClinical Trials, Halle, Germany by theGerman Ministry of Education andResearch Grant No. BMBF/FKZ:01GH0105 KKS, Halle, Germany.
Presented in part at the 6th Interna-tional Gastric Cancer Congress, Yoko-hama, Japan, May 4-7, 2005; and the13th European Cancer Conference,Paris, France, October 30-November 3,2005.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Address reprint requests to Anna D.Wagner, MD, First Department ofMedicine, Martin-Luther-UniversityHalle-Wittenberg, Ernst-Grube-Str 40,06120 Halle/Saale, Germany; e-mail:[email protected].
© 2006 by American Society of ClinicalOncology
0732-183X/06/2418-2903/$20.00
DOI: 10.1200/JCO.2005.05.0245
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 24 � NUMBER 18 � JUNE 20 2006
2903Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.
Copyright © 2006 American Society of Clinical Oncology. All rights reserved.

METHODS
We conducted this systematic review on the basis of a peer-reviewed, publishedprotocol in accordance with the guidelines of the Cochrane Collaboration.6
Study Selection
Trials were identified by electronic searches in the Cochrane ControlledTrials Register, Medline, Embase, and Cancerlit. The search strategy includedthe medical subject headings of “stomach neoplasms,” “drug therapy,” “che-motherapy,” “antineoplastic agents combined,” and “palliative care” and freetext searches. No language limits were applied. Initial searches were performedin February 2003, with updates in February 2004 and February 2005. Inaddition, we contacted drug manufacturers, asked experts in the field, andperformed manual searches in reference lists and conference proceedings ofUnited European Gastroenterology Week (1993 to 2004), Digestive DiseaseWeek (1981 to 2004), European Society for Medical Oncology (1978 to 2004),European Cancer Conference (1981 to 2004), and American Society for Clin-ical Oncology (1981 to 2005). Selection criteria were as follows: study design:randomized, controlled trials; participants: patients with histologically con-firmed, advanced, recurrent, or metastasized adenocarcinoma of the stomachor gastroesophageal junction; and interventions: systemic intravenous chemo-therapy and/or best supportive care (BSC).
Authors were contacted to obtain any missing information. Abstracts orunpublished data were included if sufficient information was available and iffinal results were confirmed by contacting the first author. Cross-over studieswere excluded because they dilute differences between study arms. Studyselection, data extraction, and data entry were performed by two authorsindependently. Differences were resolved by consensus with a third author.
Statistical Methods
Overall survival was the primary outcome measure. Hazard ratios (HRs)and 95% CIs as relevant effect measures were estimated directly or indirectlyfrom the given data.7 The fixed-effect model was used for meta-analysis. Toassess statistical heterogeneity between studies, the Cochran Q test was per-formed, with a predefined significance threshold of 0.1. The methodologicquality of all eligible studies was assessed according to a predefined qualityscore8 using the Cochrane Collaboration software (RevMan version 4.2.2;http://www.cochrane.org). This quality score was used as the basis for sensi-tivity analysis. Funnel plots were used to assess publication bias. Details ofstatistical analyses and trial selection have been described elsewhere.8 Here,results for overall survival as the primary outcome measure, toxicity, and,where available, quality of life are reported. Comparisons of chemotherapyversus BSC and combination versus single-agent chemotherapy were pre-specified in advance in the protocol for the review process.
In addition, eligible studies comparing different combination chemo-therapy regimens were classified into subcategories depending on whetherthey contained fluorouracil (FU), an anthracycline, or cisplatin. Because arational decision on which comparisons of different combination chemother-apy regimens were to be tested had to take into account the availability andeligibility of relevant studies, it was impossible to define these comparisonsbefore starting the review process. As a consensus among the reviewers, thefollowing two comparisons of chemotherapy regimens widely used in clinical
practice and serving as reference arms in ongoing trials were selected afterreview of the eligible studies: FU/cisplatin/anthracycline combinations versus FU/cisplatin combinations without anthracyclines; and FU/cisplatin/anthracyclinecombinations versus FU/anthracycline combinations without cisplatin. The com-parison of irinotecan-containing versus nonirinotecan-containing combinationswas added in 2005.
RESULTS
We identified 158 references through electronic searches and 55 refer-ences by manual searches and contact with experts. After exclusion ofduplicate publications, 194 unique references remained for furtherevaluation. Among these, 27 studies were eligible for analysis of thefive comparisons specified earlier. Trials including gastric and esoph-ageal or gastric and pancreatic cancer patients were included if suffi-cient information for the subgroup of patients with gastric cancerpatients was available. Because trials differed in how toxicity wasreported (eg, per number of patients or per number of cycles), only thepercentage of toxic deaths could be used for summarizing resultsacross different studies.
Chemotherapy Versus BSC
Three eligible studies9-11 including 184 patients were included inthis meta-analysis (Fig 1). All three studies used combination chemo-therapy. The overall HR of 0.39 (95% CI, 0.28 to 0.52) in favor of thechemotherapy arms demonstrates a convincing benefit in overall sur-vival over BSC alone, which translates to a benefit in weighted meanaverage survival of approximately 6 months. Heterogeneity was non-significant (P � .19). However, two of these three studies had substan-tial methodologic limitations. Murad et al9 interrupted randomassignment in the middle of the study because of “strong evidence ofbenefit for the treated patients.” The study by Pyrhönen et al10 wasterminated early because of slow accrual and “a conspicuous differ-ence in survival.” A sensitivity analysis according to the quality scoreincluding only studies with adequate allocation concealment10,11
changes the overall HR to 0.49 (95% CI, 0.36 to 0.67), but the resultretains statistical significance. An additional study,12 which was ex-cluded from the analysis because of cross over, provided importantinsights about the quality of life of patients in the chemotherapy andBSC arms. The average proportion of the total survival time with ahigh quality of life was significantly higher in the group of patientsrandomly assigned to chemotherapy compared with the BSC group(69% v 47%, respectively; P � .05).
Fig 1. Effect of chemotherapy versus bestsupportive care (BSC) on overall survival.Hazard ratios were analyzed with the fixed-effect model (reproduced with permission8).
Wagner et al
2904 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.Copyright © 2006 American Society of Clinical Oncology. All rights reserved.

Combination Versus Single-Agent Chemotherapy
Eleven studies13-23 with a total of 1,472 patients were included inthis analysis (Fig 2). Most of the studies used FU in the single-agentarm13-22; one study23 used doxorubicin. If studies included more thanone single agent13 or combination chemotherapy arm,12-15 their re-sults were combined. Seven of 11 combination chemotherapy regi-mens studied in this comparison contained FU and ananthracycline.13-15,19,20,22,23 Bouché et al17 included two combinationtherapy arms with FU/folinic acid/cisplatin and FU/folinic acid/irino-tecan. Non–FU-based combination chemotherapy regimens, whichinstead included etoposide, an anthracycline, and cisplatin, were in-vestigated in two studies.18,21 Treatment allocation was concealed ineight studies,13,16-18,20-23 and the analysis was done by intent-to-treat(ITT) in six studies.14-17,20,21 The resulting HR of 0.83 (95% CI, 0.74 to0.93) for survival in favor of combination chemotherapy providesevidence for a statistically significant survival benefit of combinationversus single-agent chemotherapy. This corresponds to a difference inweighted mean average survival of approximately 1 month. Again,results of the different studies were consistent in their findings; theCochran Q test for heterogeneity was nonsignificant (P � .27). Asensitivity analysis, which included only those studies with adequateallocation concealment,13,16-18,20-23 resulted in an overall HR of 0.82(95% CI, 0.71 to 0.93). However, because ITT analyses were notperformed in a relevant number of studies for this comparison, anoverestimation of the effect of combination chemotherapy cannot beexcluded. Overall treatment-associated toxicities were higher in thecombination chemotherapy arms, although this was usually not sta-tistically significant in the individual trials. Treatment-related deathswere reported in seven of 11 studies included in this comparison.Among these, six studies14-17,19,21 used FU in the single-agent arms.The overall rate of treatment-related deaths in these six studies com-bined was 1.7% for combination therapy versus 0.8% for single-agenttherapy with FU. This difference was not statistically significant (exactMantel-Haenszel odds ratio [OR] � 2.33; P � .28524). Quality of lifewas assessed in only one of these studies17; all patients in the singleagent and both combination chemotherapy arms had a significantimprovement in quality of life compared with pretreatment scores.
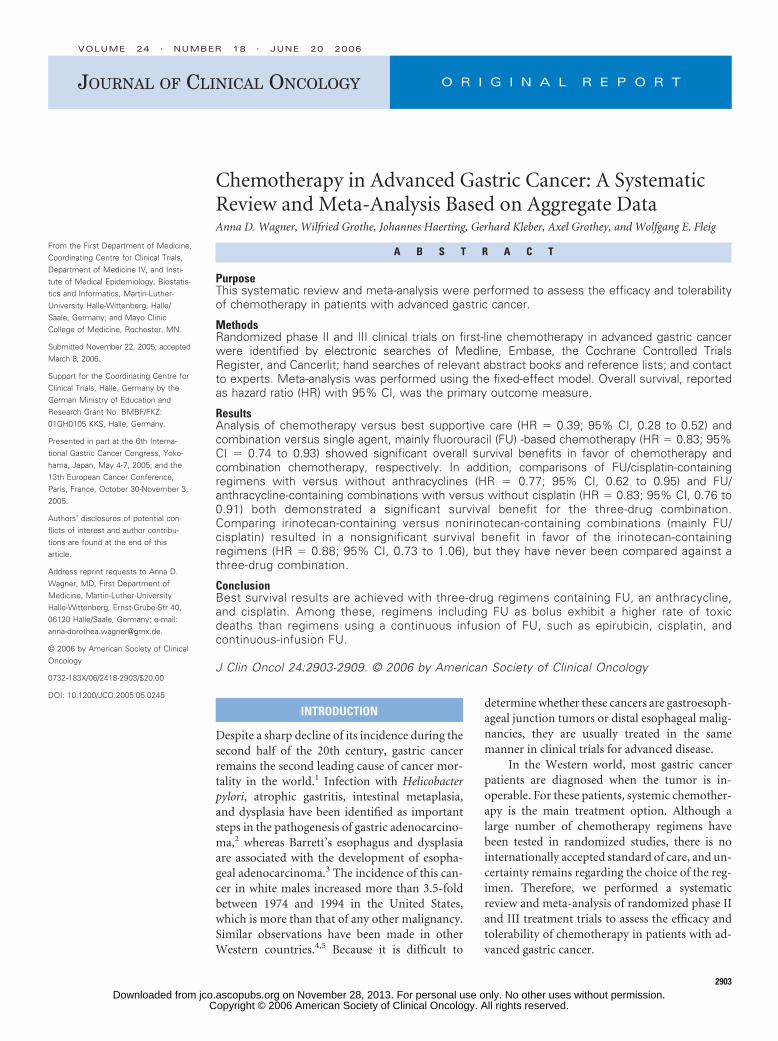
FU/Cisplatin/Anthracycline Versus
FU/Cisplatin Combinations
This meta-analysis was based on 501 patients in three random-ized trials25-27 (Fig 3). The resulting HR for overall survival of 0.77(95% CI, 0.62 to 0.91) demonstrates a statistically significant benefit inoverall survival in favor of the three-drug combination. The corre-sponding difference in weighted mean average survival between thesetwo categories of regimens is approximately 2 months. Allocationconcealment was adequate in all three studies included in this com-parison, and heterogeneity was nonsignificant (P � .71).
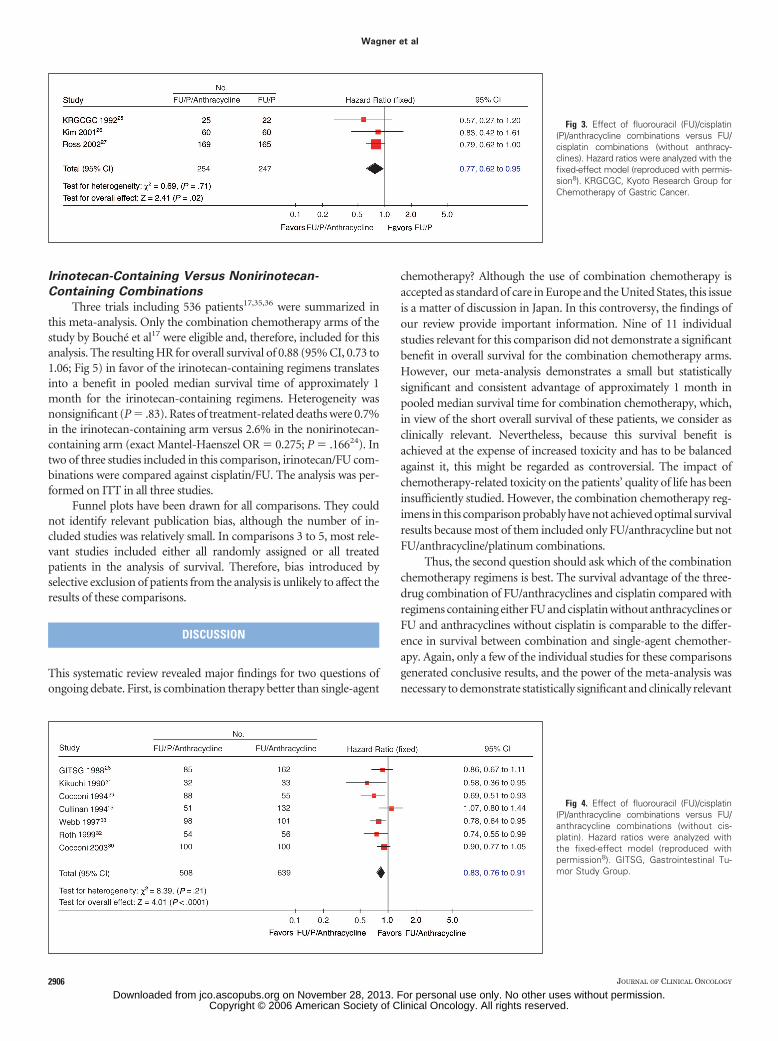
FU/Cisplatin/Anthracycline Versus
FU/Anthracycline Combinations
Summarizing the results for the comparison of FU/cispla-tin/anthracycline combinations versus FU/anthracycline (with-out cisplatin) results in an HR of 0.83 (95% CI, 0.76 to 0.91) infavor of the three-drug regimen (Fig 4). Combination chemother-apy arms only from the study by Cullinan et al15 were included in thiscomparison. This meta-analysis, which included 1,147 patients inseven studies,15,28-33 once more confirms a significant overall sur-vival benefit in favor of the three-drug combination, whichcorresponds to a difference in weighted mean average survival ofapproximately 1 month. A sensitivity analysis according to thequality score did not affect the resulting HR (HR � 0.81; 95% CI,0.72 to 0.90). There was no significant heterogeneity (P � .21).
Toxicity needs consideration. The two regimens containing FU,an anthracycline, and cisplatin that have been evaluated in the largestnumber of patients are cisplatin, epirubicin, leucovorin, and FU ad-ministered as bolus (PELF; 184 patients)29,30 and epirubicin, cisplatin,and protracted venous-infusion FU (ECF; 327 patients).26,27,33 Therate of treatment-related deaths was 3.3% for PELF versus 0.6% forECF (OR � 5.36; 95% CI, 1.1 to 27.4; Fisher’s exact test, P � .02834),suggesting an increased toxicity of PELF. Quality of life was analyzedin two studies evaluating ECF compared with FU, doxorubicin, andmethotrexate33 and mitomycin, cisplatin, and FU27 and was superiorin patients treated with ECF.
Fig 2. Effect of combination versussingle-agent chemotherapy on overall sur-vival. Hazard ratios were analyzed with thefixed-effect model.
Chemotherapy in Advanced Gastric Cancer
www.jco.org 2905Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.
Copyright © 2006 American Society of Clinical Oncology. All rights reserved.
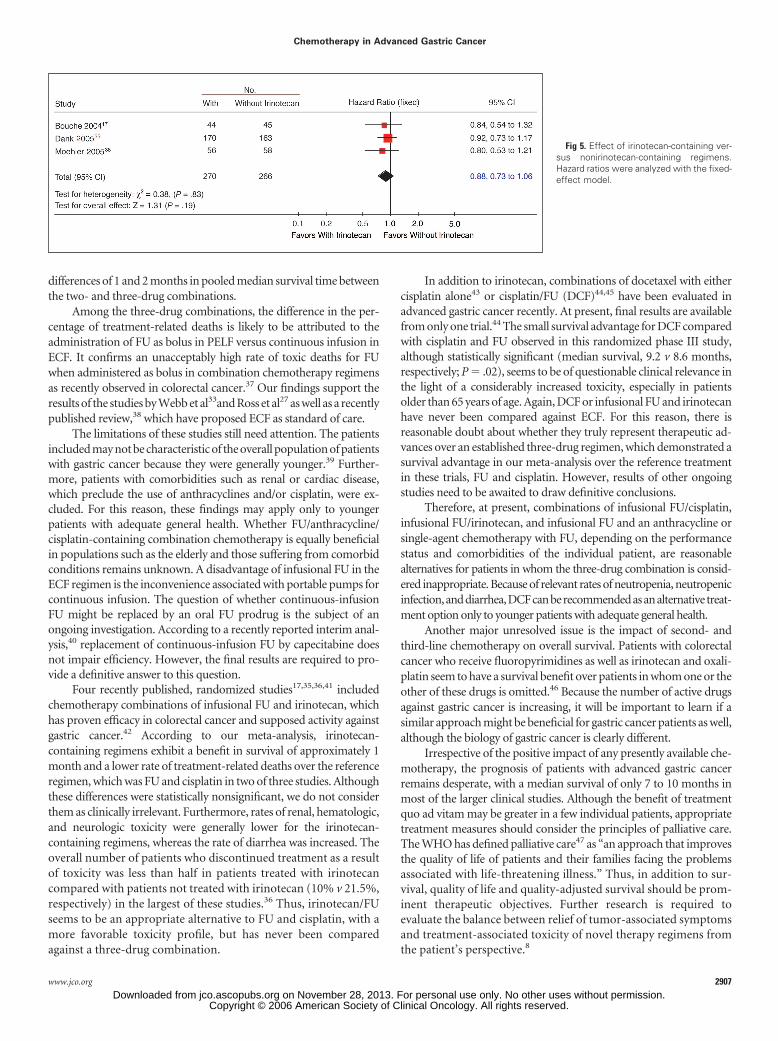
Irinotecan-Containing Versus Nonirinotecan-
Containing Combinations
Three trials including 536 patients17,35,36 were summarized inthis meta-analysis. Only the combination chemotherapy arms of thestudy by Bouché et al17 were eligible and, therefore, included for thisanalysis. The resulting HR for overall survival of 0.88 (95% CI, 0.73 to1.06; Fig 5) in favor of the irinotecan-containing regimens translatesinto a benefit in pooled median survival time of approximately 1month for the irinotecan-containing regimens. Heterogeneity wasnonsignificant (P � .83). Rates of treatment-related deaths were 0.7%in the irinotecan-containing arm versus 2.6% in the nonirinotecan-containing arm (exact Mantel-Haenszel OR � 0.275; P � .16624). Intwo of three studies included in this comparison, irinotecan/FU com-binations were compared against cisplatin/FU. The analysis was per-formed on ITT in all three studies.
Funnel plots have been drawn for all comparisons. They couldnot identify relevant publication bias, although the number of in-cluded studies was relatively small. In comparisons 3 to 5, most rele-vant studies included either all randomly assigned or all treatedpatients in the analysis of survival. Therefore, bias introduced byselective exclusion of patients from the analysis is unlikely to affect theresults of these comparisons.
DISCUSSION
This systematic review revealed major findings for two questions ofongoing debate. First, is combination therapy better than single-agent
chemotherapy? Although the use of combination chemotherapy isaccepted as standard of care in Europe and the United States, this issueis a matter of discussion in Japan. In this controversy, the findings ofour review provide important information. Nine of 11 individualstudies relevant for this comparison did not demonstrate a significantbenefit in overall survival for the combination chemotherapy arms.However, our meta-analysis demonstrates a small but statisticallysignificant and consistent advantage of approximately 1 month inpooled median survival time for combination chemotherapy, which,in view of the short overall survival of these patients, we consider asclinically relevant. Nevertheless, because this survival benefit isachieved at the expense of increased toxicity and has to be balancedagainst it, this might be regarded as controversial. The impact ofchemotherapy-related toxicity on the patients’ quality of life has beeninsufficiently studied. However, the combination chemotherapy reg-imens in this comparison probably have not achieved optimal survivalresults because most of them included only FU/anthracycline but notFU/anthracycline/platinum combinations.
Thus, the second question should ask which of the combinationchemotherapy regimens is best. The survival advantage of the three-drug combination of FU/anthracyclines and cisplatin compared withregimens containing either FU and cisplatin without anthracyclines orFU and anthracyclines without cisplatin is comparable to the differ-ence in survival between combination and single-agent chemother-apy. Again, only a few of the individual studies for these comparisonsgenerated conclusive results, and the power of the meta-analysis wasnecessary to demonstrate statistically significant and clinically relevant
Fig 3. Effect of fluorouracil (FU)/cisplatin(P)/anthracycline combinations versus FU/cisplatin combinations (without anthracy-clines). Hazard ratios were analyzed with thefixed-effect model (reproduced with permis-sion8). KRGCGC, Kyoto Research Group forChemotherapy of Gastric Cancer.
Fig 4. Effect of fluorouracil (FU)/cisplatin(P)/anthracycline combinations versus FU/anthracycline combinations (without cis-platin). Hazard ratios were analyzed withthe fixed-effect model (reproduced withpermission8). GITSG, Gastrointestinal Tu-mor Study Group.
Wagner et al
2906 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.Copyright © 2006 American Society of Clinical Oncology. All rights reserved.
differences of 1 and 2 months in pooled median survival time betweenthe two- and three-drug combinations.
Among the three-drug combinations, the difference in the per-centage of treatment-related deaths is likely to be attributed to theadministration of FU as bolus in PELF versus continuous infusion inECF. It confirms an unacceptably high rate of toxic deaths for FUwhen administered as bolus in combination chemotherapy regimensas recently observed in colorectal cancer.37 Our findings support theresults of the studies by Webb et al33and Ross et al27 as well as a recentlypublished review,38 which have proposed ECF as standard of care.
The limitations of these studies still need attention. The patientsincluded may not be characteristic of the overall population of patientswith gastric cancer because they were generally younger.39 Further-more, patients with comorbidities such as renal or cardiac disease,which preclude the use of anthracyclines and/or cisplatin, were ex-cluded. For this reason, these findings may apply only to youngerpatients with adequate general health. Whether FU/anthracycline/cisplatin-containing combination chemotherapy is equally beneficialin populations such as the elderly and those suffering from comorbidconditions remains unknown. A disadvantage of infusional FU in theECF regimen is the inconvenience associated with portable pumps forcontinuous infusion. The question of whether continuous-infusionFU might be replaced by an oral FU prodrug is the subject of anongoing investigation. According to a recently reported interim anal-ysis,40 replacement of continuous-infusion FU by capecitabine doesnot impair efficiency. However, the final results are required to pro-vide a definitive answer to this question.
Four recently published, randomized studies17,35,36,41 includedchemotherapy combinations of infusional FU and irinotecan, whichhas proven efficacy in colorectal cancer and supposed activity againstgastric cancer.42 According to our meta-analysis, irinotecan-containing regimens exhibit a benefit in survival of approximately 1month and a lower rate of treatment-related deaths over the referenceregimen, which was FU and cisplatin in two of three studies. Althoughthese differences were statistically nonsignificant, we do not considerthem as clinically irrelevant. Furthermore, rates of renal, hematologic,and neurologic toxicity were generally lower for the irinotecan-containing regimens, whereas the rate of diarrhea was increased. Theoverall number of patients who discontinued treatment as a resultof toxicity was less than half in patients treated with irinotecancompared with patients not treated with irinotecan (10% v 21.5%,respectively) in the largest of these studies.36 Thus, irinotecan/FUseems to be an appropriate alternative to FU and cisplatin, with amore favorable toxicity profile, but has never been comparedagainst a three-drug combination.
In addition to irinotecan, combinations of docetaxel with eithercisplatin alone43 or cisplatin/FU (DCF)44,45 have been evaluated inadvanced gastric cancer recently. At present, final results are availablefrom only one trial.44 The small survival advantage for DCF comparedwith cisplatin and FU observed in this randomized phase III study,although statistically significant (median survival, 9.2 v 8.6 months,respectively; P � .02), seems to be of questionable clinical relevance inthe light of a considerably increased toxicity, especially in patientsolder than 65 years of age. Again, DCF or infusional FU and irinotecanhave never been compared against ECF. For this reason, there isreasonable doubt about whether they truly represent therapeutic ad-vances over an established three-drug regimen, which demonstrated asurvival advantage in our meta-analysis over the reference treatmentin these trials, FU and cisplatin. However, results of other ongoingstudies need to be awaited to draw definitive conclusions.
Therefore, at present, combinations of infusional FU/cisplatin,infusional FU/irinotecan, and infusional FU and an anthracycline orsingle-agent chemotherapy with FU, depending on the performancestatus and comorbidities of the individual patient, are reasonablealternatives for patients in whom the three-drug combination is consid-ered inappropriate. Because of relevant rates of neutropenia, neutropenicinfection,anddiarrhea,DCFcanberecommendedasanalternative treat-ment option only to younger patients with adequate general health.
Another major unresolved issue is the impact of second- andthird-line chemotherapy on overall survival. Patients with colorectalcancer who receive fluoropyrimidines as well as irinotecan and oxali-platin seem to have a survival benefit over patients in whom one or theother of these drugs is omitted.46 Because the number of active drugsagainst gastric cancer is increasing, it will be important to learn if asimilar approach might be beneficial for gastric cancer patients as well,although the biology of gastric cancer is clearly different.
Irrespective of the positive impact of any presently available che-motherapy, the prognosis of patients with advanced gastric cancerremains desperate, with a median survival of only 7 to 10 months inmost of the larger clinical studies. Although the benefit of treatmentquo ad vitam may be greater in a few individual patients, appropriatetreatment measures should consider the principles of palliative care.The WHO has defined palliative care47 as “an approach that improvesthe quality of life of patients and their families facing the problemsassociated with life-threatening illness.” Thus, in addition to sur-vival, quality of life and quality-adjusted survival should be prom-inent therapeutic objectives. Further research is required toevaluate the balance between relief of tumor-associated symptomsand treatment-associated toxicity of novel therapy regimens fromthe patient’s perspective.8
Fig 5. Effect of irinotecan-containing ver-sus nonirinotecan-containing regimens.Hazard ratios were analyzed with the fixed-effect model.
Chemotherapy in Advanced Gastric Cancer
www.jco.org 2907Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.
Copyright © 2006 American Society of Clinical Oncology. All rights reserved.

REFERENCES
1. Kelley JR, Duggan JM: Gastric cancer epide-miology and risk factors. J Clin Epidemiol 56:1-9,2003
2. Correa P: Helicobacter pylori and gastric can-cer: State of the art. Cancer Epidemiol BiomarkersPrev 5:477-481, 1996
3. Montgomery E, Goldblum JR, Greenson JK,et al: Dysplasia as a predictive marker for invasivecarcinoma in barrett esophagus: A follow-up studybased on 138 cases from a diagnostic variabilitystudy. Hum Pathol 32:379-388, 2001
4. Powell J, McConkey CC: The rising trend inoesophageal adenocarcinoma and gastric cardia. EurJ Cancer Prev 1:265-269, 1992
5. Lord RV, Law MG, Ward RL, et al: Risingincidence of esophageal adenocarcinoma in men inAustralia. J Gastroenterol Hepatol 13:356-362, 1998
6. Deeks JJ, Higgins JPT, Altman DG (eds):Cochrane Reviewers’ Handbook. http://www.co-chrane.org/resources/handbook/hbook.htm
7. Altman DG: Systematic reviews of evalua-tions of prognostic variables, in Egger M, Smith GD,Altman D (eds): Systematic Reviews in Health Care(ed 2). London, United Kingdom, BMJ PublishingGroup, 2001, pp 228-248
8. Wagner AD, Grothe W, Behl S, et al: Chemo-therapy for advanced gastric cancer. Oxford, En-gland, Cochrane Library, issue 2, 2005
9. Murad AM, Santiago FF, Petroianu A, et al:Modified therapy with 5-fluorouracil, doxorubicin,and methotrexate in advanced gastric cancer. Can-cer 72:37-41, 1993
10. Pyrhönen S, Kuitunen T, Nyandoto P, et al:Randomised comparison of fluorouracil, epidoxoru-bicin and methotrexate (FEMTX) plus supportivecare with supportive care alone in patients withnon-resectable gastric cancer. Br J Cancer 71:587-591, 1995
11. Scheithauer W, Kornek G, Hejna M, et al:Palliative chemotherapy versus best supportive carein patients with metastatic gastric cancer: A ran-domized trial. Ann Hematol 73:A181, 1994 (suppl 2,abstr)
12. Glimelius B, Ekstrom K, Hoffman K, et al:Randomized comparison between chemotherapyplus best supportive care with best supportive carein advanced gastric cancer. Ann Oncol 8:1-6, 1997
13. Loehrer PJ Sr, Harry D, Chlebowski RT:5-Fluorouracil vs. epirubicin vs. 5-fluorouracil plusepirubicin in advanced gastric carcinoma. InvestNew Drugs 12:57-63, 1994
14. Cullinan SA, Moertel CG, Fleming TR, et al: Acomparison of three chemotherapeutic regimens inthe treatment of advanced pancreatic and gastriccarcinoma: Fluorouracil vs fluorouracil and doxorubi-cin vs fluorouracil, doxorubicin, and mitomycin.JAMA 253:2061-2067, 1985
15. Cullinan SA, Moertel CG, Wieand HS, etal: Controlled evaluation of three drug combina-tion regimens versus fluorouracil alone for thetherapy of advanced gastric cancer: North CentralCancer Treatment Group. J Clin Oncol 12:412-416, 1994
16. Ohtsu A, Shimada Y, Shirao K, et al: Ran-domized phase III trial of fluorouracil alone versusfluorouracil plus cisplatin versus uracil and tegafurplus mitomycin in patients with unresectable,advanced gastric cancer: The Japan Clinical On-cology Group Study (JCOG9205). J Clin Oncol21:54-59, 2003
17. Bouché O, Raoul JL, Bonnetain F, et al: Ran-domized multicenter phase II trial of a biweeklyregimen of fluorouracil and leucovorin (LV5FU2),LV5FU2 plus cisplatin, or LV5FU2 plus irinotecan inpatients with previously untreated metastatic gas-tric cancer: A Fédération Francophone de Cancérolo-gie Digestive Group study-FFCD 9803. J Clin Oncol22:4319-4328, 2004
18. Barone C, Corsi DC, Pozzo C, et al: Treatmentof patients with advanced gastric carcinoma with a5-fluorouracil-based or a cisplatin-based regimen:Two parallel randomized phase II studies. Cancer82:1460-1467, 1998
19. Colucci G, Giotta F, Maiello E, et al: Efficacy ofthe association of folinic acid and 5-fluorouracil aloneversus folinic acid and 5-fluorouracil plus4-epidoxorubicin in the treatment of advanced gas-tric carcinoma. Am J Clin Oncol 18:519-524, 1995
20. De Lisi V, Cocconi G, Tonato M, et al: Ran-domized comparison of 5-FU alone or combinedwith carmustine, doxorubicin, and mitomycin(BAFMi) in the treatment of advanced gastric can-cer: A phase III trial of the Italian Clinical ResearchOncology Group (GOIRC). Cancer Treat Rep 70:481-485, 1986
21. Popov I, Svetislav BJ, Jezdic SD: Bi-weekly24-hour infusion of high dose 5-fluorouracil versusEAP regimen in advanced gastric cancer: A random-ised phase II study. Ann Oncol 13:188, 2002 (suppl5)
22. Yamamura Y, Miyazaki I, Ogawa M, et al: Arandomized controlled trial with methotrexate(MTX), 5-fluorouracil (5-FU) and pirarubicin (THP) vs5-FU alone in advanced or recurrent gastric carci-noma: Tokai Hokuriku THP Study Group. Gan ToKagaku Ryoho 25:1543-1548, 1998
23. Levi JA, Fox RM, Tattersall MH, et al: Analysisof a prospectively randomized comparison of doxo-rubicin versus 5-fluorouracil, doxorubicin, and BCNUin advanced gastric cancer: Implications for futurestudies. J Clin Oncol 4:1348-1355, 1986
24. Agresti A: A survey of exact inference forcontingency tables (with discussion). Stat Sci 7:131-177, 1992
25. Kyoto Research Group for Chemotherapy ofGastric Cancer: A randomized, comparative study ofcombination chemotherapies in advanced gastriccancer: 5-fluorouracil and cisplatin (FP) versus5-fluorouracil, cisplatin, and 4�-epirubicin (FPEPIR).Anticancer Res 12:1983-1988, 1992
26. Kim TW, Choi SJ, Ahn JH, et al: A prospectiverandomized phase III trial of 5-fluorouracil and cis-platin (FP) versus epirubicin, cisplatin, and 5-FU(ECF) in the treatment of patients with previouslyuntreated advanced gastric cancer (AGC). Eur JCancer 37:S314, 2001 (suppl 6)
27. Ross P, Nicolson M, Cunningham D, et al:Prospective randomized trial comparing mitomycin,cisplatin, and protracted venous-infusion fluorouracil(PVI 5-FU) with epirubicin, cisplatin, and PVI 5-FU inadvanced esophagogastric cancer. J Clin Oncol 20:1996-2004, 2002
28. Gastrointestinal Tumor Study Group: Triazi-nate and platinum efficacy in combination with5-fluorouracil and doxorubicin: Results of a three-arm randomized trial in metastatic gastric cancer.J Natl Cancer Inst 80:1011-1015, 1988
29. Coccioni G, Bella M, Zironi S, et al: Fluoroura-cil, doxorubicin, and mitomycin combination versusPELF chemotherapy in advanced gastric cancer: Aprospective randomized trial of the Italian OncologyGroup for Clinical Research. J Clin Oncol 12:2687-2693, 1994
30. Coccioni G, Carlini P, Gamboni A, et al: Cis-platin, epirubicin, leucovorin and 5-fluorouracil(PELF) is more active than 5-fluorouracil, doxorubicinand methotrexate (FAMTX) in advanced gastric car-cinoma. Ann Oncol 14:1258-1263, 2003
31. Kikuchi K, Wakui A, Shimizu H, et al: Random-ized controlled study on chemotherapy with 5-FD,ADM plus CDDP in advanced gastric carcinoma.Gan To Kagaku Ryoho17:655-662, 1990
32. Roth A, Kolaric K, Zupanc D, et al: High dosesof 5-fluorouracil and epirubicin with or without cis-platin in advanced gastric cancer: A randomizedstudy. Tumori 85:234-238, 1999
33. Webb A, Cunningham D, Scarffe JH, et al:Randomized trial comparing epirubicin, cisplatin, andfluorouracil versus fluorouracil, doxorubicin, andmethotrexate in advanced esophagogastric cancer.J Clin Oncol 15:261-267, 1997
34. Altman DG: Practical Statistics for MedicalResearch. London, United Kingdom, Chapman &Hall, 1991, pp 253-257
35. Moehler M, Eimermacher A, Siebler J, et al:Randomized phase II evaluation of irinotecan plushigh-dose 5-fluorouracil and leucovorin (ILF) versus5-fluorouracil, leucovorin, and etoposide (ELF) inuntreated metastatic gastric cancer. Br J Cancer92:2122-2128, 2005
36. Dank M, Zaluski J, Valvere V, et al: Random-ized phase III trial of irinotecan (CPT 11) � 5-FU/folinic acid (FA) vs CDDP � 5-FU in first lineadvanced gastric cancer patients. J Clin Oncol 23:308s, 2005 (suppl 16, abstr 4003)
37. Delaunoit T, Goldberg RM, Sargent DJ, et al:Mortality associated with daily bolus 5-fluorouracil/leucovorin administered in combination with eitheririnotecan or oxaliplatin. Cancer 101:2170-2176,2004
38. Wöhrer SS, Raderer M, Hejna M: Palliativechemotherapy for advanced gastric cancer. AnnOncol 15:1585-1595, 2004
39. Peye JK, Crumplin MK, Charles J, et al: One-year survey of carcinoma of the esophagus andstomach in Wales. Br J Surg 88:278-285, 2001
40. Sumpter KA, Harper-Wynne C, CunninghamD, et al: Report of two planned interim analyses in arandomised multicentre phase III study comparingcapecitabine with fluorouracil and oxaliplatin withcisplatin in patients with advanced oesophagogas-tric cancer receiving ECF. Br J Cancer 92:1976-1983, 2005
41. Pozzo C, Barone C, Szanto J, et al: Irinotecanin combination with 5-fluorouracil and folinic acid orcisplatin in patients with advanced gastric oresophageal-gastric junction adenocarcinoma: Re-sults of a randomized phase II study. Ann Oncol15:1773-1781, 2004
42. Kohne CH, Catane R, Klein B, et al: Irinotecanis active in chemonaive patients with metastaticgastric cancer: A phase II multicentric trial. Br JCancer 89:997-1001, 2003
43. Fahlke J, Ridwelski K, Schmidt C, et al:Docetaxel-cisplatin (DC) versus 5-fluouracil-leucovorin-cisplatin (FLC) as first-line treatment forlocally advanced or metastatic gastric cancer: Pre-liminary results of a phase III study. J Clin Oncol23:319s, 2005 (suppl 16, abstr 4045)
44. Moiseyenko VM, Ajani J, Tjulandin SA, et al:Final results of a randomized controlled phase III trial(TAX 325) comparing docetaxel (T) combined withcisplatin (C) and 5-fluorouracil (F) to CF in patients(pts) with metastatic gastric adenocarcinoma(MGC). J Clin Oncol 23:308s, 2005 (suppl 16, abstr4002)
Wagner et al
2908 JOURNAL OF CLINICAL ONCOLOGY
Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.Copyright © 2006 American Society of Clinical Oncology. All rights reserved.

45. Roth AD, Falk S, Stupp R, et al: Docetaxel-cisplatin-5-FU (TCF) versus docetaxel-cisplatin (TC)versus epirubicin-cisplatin-5-FU (ECF) as systemictreatment for advanced gastric carcinoma (AGC): Arandomized phase II trial of the Swiss Group for
Clinical Cancer Res (SAKK). J Clin Oncol 22:312s,2004 (suppl 16, abstr 4020)
46. Grothey A, Sargent D, Goldberg RM, et al:Survival of patients with advanced colorectal can-cer improves with the availability of fluorouracil-
leucovorin, irinotecan and oxaliplatin in the course oftreatment. J Clin Oncol 22:1209-1214, 2004
47. Sepulveda C, Marlin A, Yoshida T, et al: Pallia-tive care: The World Health Organization’s global per-spective. J Pain Symptom Manage 24:91-96, 2002
■ ■ ■
Acknowledgment
We thank Shino Yuo for translations of Japanese studies, Y. Shimada for providing important insights on the Japanese view of the subject, allauthors who provided unpublished data, and J. Abbruzzese, D. Cunningham, and B. Glimelius for helpful comments.
Authors’ Disclosures of Potential Conflicts of InterestThe authors indicated no potential conflicts of interest.
Author Contributions
Conception and design: Anna D. Wagner, Wilfried Grothe, Johannes Haerting, Gerhard Kleber, Axel Grothey, Wolfgang E. FleigCollection and assembly of data: Anna D. Wagner, Wilfried GrotheData analysis and interpretation: Anna D. Wagner, Johannes Haerting, Gerhard Kleber, Axel Grothey, Wolfgang E. FleigManuscript writing: Anna D. Wagner, Johannes Haerting, Gerhard Kleber, Axel Grothey, Wolfgang E. FleigFinal approval of manuscript: Anna D. Wagner, Wilfried Grothe, Johannes Haerting, Gerhard Kleber, Axel Grothey, Wolfgang E. Fleig
Chemotherapy in Advanced Gastric Cancer
www.jco.org 2909Downloaded from jco.ascopubs.org on November 28, 2013. For personal use only. No other uses without permission.
Copyright © 2006 American Society of Clinical Oncology. All rights reserved.




















![Sarcina ventriculi-associated with chemotherapy-induced ... of...emphysematous gastritis and gastric perforation with mortality have been reported [7]. In our case, the patient has](https://img.dokumen.tips/doc/110x75/607b6c04a2e1a47b706c7adc/sarcina-ventriculi-associated-with-chemotherapy-induced-of-emphysematous.jpg)








