Embed Size (px)
Citation preview

Preclinical Development
Characterization of an Oxaliplatin Sensitivity Predictorin a Preclinical Murine Model of Colorectal Cancer
Mickey K. Kim2, Takuya Osada3, William T. Barry2,5, Xiao Yi Yang3, Jennifer A. Freedman2,Katherine A. Tsamis2, Michael Datto4, Bryan M. Clary3, Timothy Clay6, Michael A. Morse1,Philip G. Febbo7, H. Kim Lyerly3, and David S. Hsu1,2
AbstractDespite advances in contemporary chemotherapeutic strategies, long-term survival still remains elusive for
patients withmetastatic colorectal cancer. A better understanding of themolecularmarkers of drug sensitivity
to match therapy with patient is needed to improve clinical outcomes. In this study, we used in vitro drug
sensitivity data from the NCI-60 cell lines together with their Affymetrix microarray data to develop a gene
expression signature to predict sensitivity to oxaliplatin. To validate our oxaliplatin sensitivity signature,
patient-derived colorectal cancer explants (PDCCE) were developed in nonobese diabetic/severe combined
immunodeficient (NOD/SCID) mice from resected human colorectal tumors. Analysis of gene expression
profiles found similarities between the PDCCEs and their parental human tumors, suggesting their utility to
study drug sensitivity in vivo. The oxaliplatin sensitivity signature was then validated in vivo with response
data from14PDCCEs treatedwith oxaliplatin andwas found to have an accuracy of 92.9% (sensitivity¼ 87.5%;
specificity ¼ 100%). Our findings suggest that PDCCEs can be a novel source to study drug sensitivity
in colorectal cancer. Furthermore, genomic-based analysis has the potential to be incorporated into future
strategies to optimize individual therapy for patients with metastatic colorectal cancer.Mol Cancer Ther; 11(7);
1500–9. �2012 AACR.
IntroductionColorectal cancer is the third most common cancer in
the world with approximately 150,000 new cases in theUnited States each year and ranks second only behindlung cancer as the leading cause of cancer-related deaths(1). At initial diagnosis approximately 20%of patientswillhave distant metastasis, and another 25% to 30% ofpatients with early stage disease will develop metastasis(2, 3). Currently, the use of chemotherapy in themetastaticsetting is predominantly for disease control and palliationof symptoms. If left untreated, patients with metastaticcolorectal cancer have an overall survival of 6 to 9months,but with combination therapy, survival can be improved
to greater than 20 months (4–6). Although the prolongedsurvival with current combination therapy represents asignificant achievement, metastatic colorectal cancer stillremains an incurable disease, and new therapeuticapproaches are required to improve clinical outcomes.
Therapy based upon the biology of an individual’stumor rather than established histopathologic and ana-tomic classification is an approach that promises to opti-mize the use of existing therapies and identify noveltargets for future therapies. Currently, either a single geneor a small collection of genes is used to determineresponse to therapeutic agents. Gene expression analysisoffers the potential to measure genome-wide gene activ-ity, which can be used to complement currently availableclinical and biochemical markers to identify discrete clin-ically and biologically relevant phenotypes to better char-acterize a disease (7, 8). As a result, clinical medicinebecomes a data-intensive, quantitative genomic science,and such data can be used to uncover patterns and trendsthat can distinguish between biologic phenotypes to helpguide existing therapies and discover new therapeutictargets (9–11).
The ability to create a predictive model that can deter-mine which patient may derive the most benefit from aparticular agent is the first step in guiding therapy.Previous studies have shown that the NCI-60 cell linepanel can be used to create predictive therapeutic models(12–14); however, it remains unclear whether or not
Authors' Affiliations: 1Division ofMedical Oncology, 2Institute for GenomeSciences and Policy, Departments of 3Surgery, 4Pathology, and 5Biosta-tistics and Bioinformatics, Duke University, Durham, North Carolina; 6GSKBiologicals, Rixensart, Belgium; and 7Division of Medical Oncology,University of California, San Francisco, San Francisco, California
Note: Supplementary material for this article is available at MolecularCancer Therapeutics Online (http://mct.aacrjournals.org/).
M.K. Kim and T. Osada contributed equally to this work.
Corresponding Author: David S. Hsu, Institute for Genome Sciences &Policy, Duke University Medical Center, DUMC 3382, 2167 CIEMAS Build-ing,Durham,NC27710.Phone: 919-684-1379; Fax: 919-668-4777;E-mail:[email protected]
doi: 10.1158/1535-7163.MCT-11-0937
�2012 American Association for Cancer Research.
MolecularCancer
Therapeutics
Mol Cancer Ther; 11(7) July 20121500
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937

responses to therapeutic agents in vitro are predictive ofclinical response. Therefore, similarly to the incorporationof new therapeutic agents in the clinical setting, predictivebiomarkers must be assessed for their therapeutic poten-tial in preclinical models.In the past, mouse xenografts have been developed
to screen new cancer drugs (15). Initially, athymic mice(nu/nu) and SCID mice were used to establish xenograftsfrom human tumor cell lines to test their response tocancer drugs (16). More recently, the direct transplanta-tion of resected human tumors into mice to study sensi-tivities to therapeutic agents in gastrointestinal cancershas been carried out (17, 18). However, it remains unclearwhether or not responses to therapeutic agents in vivoare predictive of clinical responses; thus, the need for aclinically relevant preclinical model arises.In this study, we have developed a predictor of sensi-
tivity to oxaliplatin to identify patients who would derivethe most benefit from oxaliplatin-based therapy alongwith a preclinical murine model of patient-derived colo-rectal cancer explants (PDCCEs) to validate our predictivesignature. Together, these approaches describe a widelyapplicable system that facilitates the preclinical develop-ment and characterization of therapeutic agents alone andin combination to maximize response to chemotherapeu-tic drugs and change the current paradigm of clinicalcancer therapy evaluation in colorectal cancers.
Materials and MethodsDevelopment of in vitro oxaliplatin sensitivitypredictorAn oxaliplatin sensitivity signature was generated as
follows. Briefly, the concentration needed to reduce thegrowth of treated cells to half that of untreated cells (GI50),tumor growth inhibition (TGI), and concentration of drugresulting in a 50% reduction in themeasuredprotein at theend of the drug treatment as compared with that at thebeginning (LC50) data for oxaliplatin on the NCI-60 cellline panel obtained from the NCI Developmental Thera-peutics Program (19) were compared to determine rela-tive oxaliplatin sensitivity. We subsequently chose celllines within the NCI-60 panel that would represent theextremes of sensitivity to develop an in vitro gene expres-sion–based predictor of oxaliplatin sensitivity from thepharmacologic data used in the NCI-60 drug screen stud-ies. RMA-normalized expression data from the NCI-60cell lineswere estimated fromCELfiles downloaded fromCellMiner (20, 21) and were used in a supervised analysisusing Bayesian regression methodologies to develop asignature for sensitivity to oxaliplatin. Specifically, aBayesian probit regression model was fit to the mostdifferentially expressed genes, as summarized by the topcomponents of singular value decomposition. The pre-dictive probability of chemosensitivity was computed asthe average of the posterior distribution of the Bayesianmodel. Complete details are in the Supplementary Mate-rial and Methods.
Development of PDCCEsColon tumor tissue specimens were obtained from
patients (n ¼ 14) with histologically confirmed colorectalcancer who had undergone complete surgical resectionsat the Duke University Medical Center (Durham, NC)between November 15, 2007, and August 27, 2009. Thisinvestigation was approved by the Institutional ReviewBoard of the Duke University Medical Center, and allpatients provided informed consent. All specimens weresectioned, stained with hematoxylin and eosin (H&E),and examined by microscopy by a board certified pathol-ogist. Colorectal tumors resected at the time of surgerywere washed with PBS and then minced into 2- to 3-mmcubes. The samples were then placed in an enzymemedi-um [RPMI media containing collagenase IV (6 mg/mL),hyaluronidase (1 mg/mL), and deoxyribonuclease (0.25mg/mL; Sigma)] and agitated at room temperature for 18to 24 hours. After agitation, the cells were centrifuged at2,000 rpm for 15 minutes at room temperature, washedwith PBS, and passed through a 70 mmol/L cell strainer(BD Biosciences). After washing with PBS, the cells wereagain centrifuged at 2,000 rpm for 15 minutes at roomtemperature, resuspended in serum-free RPMI/Matrigelmixture (1:1 volume), and then injected into the flanks of4-week-old female JAX NOD.CB17-PrkdcSCID-J mice.
All mouse experiments were carried out in accordancewith the animal guidelines and with the approval of theInstitutional Animal Care andUseCommittee (IACUC) atthe Duke University Medical Center.
In vivo oxaliplatin sensitivity assay of PDCCEsTo test the sensitivity of oxaliplatin in the PDCCEs,
colorectal cancer cells extracted from previously generat-ed, earlier passaged explants (passages 4–8) were injectedsubcutaneously into the flanks of 5 JAX NOD.CB17-PrkdcSCID-J mice (four-week-old female) and measuredevery 2 to 3 dayswith a vernier caliper until the volume ofthe tumor (V ¼ L�W2 � 0.5 where L¼ longest diameter,W ¼ shortest diameter) reached approximately 500 mm3.The mice were then randomized and treated either withoxaliplatin at a standard dose of 10 mg/kg weekly viaintraperitoneal injection or with saline for 2.5 weeks witheach group containing 5 mice each. Tumors were thenmeasured at least 2�/wkwith a vernier caliper, and bothtumor volume and TGI ratio [TGI%¼ 1� (average tumorvolume of oxaliplatin group)/(average volume tumor ofcontrol group)� 100%]were calculated at each timepoint.At the end of 3 weeks, the tumors from both groups wereharvested and placed immediately in optimal cuttingtemperature (OCT) compound (Sakura Finetek) and fro-zenondry ice or placed in formalin overnight andparaffinembedded the next day.
Sample processing: fresh-frozen samplesFrozen PDCCE samples were sectioned at 8 mm and
placed onto histologic slides. An initial section wasstained with H&E (Sigma) for histologic characterizationof the tissue, and the sample was subsequently
Development of an Oxaliplatin Sensitivity Predictor
www.aacrjournals.org Mol Cancer Ther; 11(7) July 2012 1501
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937

macrodissected to ensure more than 80% tumor. Approx-imately 100 mg of tissue was macrodissected, and totalRNA was isolated from the homogenized tissue by theRNAase Isolation Kit (Qiagen). RNA were quantifiedusing a Nanodrop ND-1000 spectrophotometer (Nano-drop Technologies), and quality was assessed by spectro-photomeric analysis on an Agilent 2100 Bioanalyzer con-ductor by the RNA 6000 Nano Assay Kit (AgilentTechnologies).
Four mg of total RNAwas used to generate gene expres-sion data. Briefly, first strand cDNA synthesis was gen-erated using a T7-linked oligo-dT primer followed bysecond strand synthesis. An in vitro transcription reactionwas carried out to generate the cRNA-containing bioti-nylated UTP and CTP, which is subsequently chemicallyfragmented at 95�C for 35 minutes. The fragmented,biotinylated cRNAwashybridized inMESbuffer contain-ing 0.5 mg/mL acetylated bovine serum albumin to Affy-metrix GeneChip Human U133A 2.0 arrays at 45�C for 16hours, according to the Affymetrix protocol (Affymetrix).Generated CEL files are available at GEO (GSE28691).
Formalin-fixed, paraffin-embedded samplesTumors from the PDCCEs were fixed in formalin over-
night and paraffin embedded the following day. Forma-lin-fixed, paraffin-embedded (FFPE) PDCCE sampleswere sectioned at 10 mmand placed onto histologic slides.An initial section was stained with H&E for histologiccharacterization of the tissue to ensure more than 80%tumor. RNA was then isolated from 8- to 10-mm FFPEsections by the RecoverAll-MagMAX Custom Kit andprotocol (Applied Biosystems) with the following mod-ifications: RNA isolation digestions were incubated at50�C for 15 minutes and then at 80�C for 15 minutes;lysis-binding solution was reconstituted with 22 mL of100% isopropanol (Mallinckrodt Chemicals); wash solu-tion 1H was reconstituted with 12 mL of 100% isopropa-nol; and wash solution 2 was reconstituted with 44 mL of100% ethanol (Pharmco-AAper).
RNA was amplified according to the MessageAmpPremier protocol (Ambion). Affymetrix DNAmicroarrayanalysis was prepared according to the manufacturer’sinstructions, and targets were hybridized to the HumanU133A 2.0 GeneChip (Affymetrix). Generated CEL filesare available at GEO (GSE28691).
Validation of oxaliplatin sensitivity signatureTo validate the accuracy of the Bayesian probit regres-
sion model, first, the RMA-normalized gene expressiondata of the training data set (NCI-60 oxaliplatin sensi-tivity signature) and validation data set (PDCCE fresh-frozen or PDCCE FFPE samples) were merged togetherusing an in-house program, File Merger (22). Next, themodel was used to estimate the relative probabilitiesand associated measures of uncertainty for each samplein the validation set as described previously (23). Sam-ples scoring below 0.5 were considered belonging to theoxaliplatin-resistant class, whereas samples scoring
above 0.5 were considered belonging to the oxalipla-tin-sensitive class. The associations between the oxali-platin sensitivity predictor and PDCCE TGIs wereevaluated using Pearson correlation coefficients and2-sided P values. Complete details are in the Supple-mentary Material and Methods.
Statistical analysisExpression estimates were obtained from the Affyme-
trix CEL files using MAS5 and RMA (24). To check forsample outliers and batch effects, 3-dimensional (3D)principal components analysis of the global gene expres-sion was conducted. Batch effects were normalized usingthe ComBat algorithm (25). Unsupervised hierarchicalclustering of the human tumors and matching PDCCEswas carried out on the 20% of genes with the greatestcoefficient of variation (CV). Agglomerative clusters weregenerated using the Pearson correlation coefficient andcomplete linkage. To determine whether clusters werestatistically robust, the AU (approximate unbiased) andBP (bootstrap probability) values were calculated by10,000 resamples using the R package pvclust. The asso-ciations between cell line phenotypes and genomic pre-dictors are evaluated using Spearman correlation coeffi-cients and 2-sided P values.
ResultsDevelopment of oxaliplatin sensitivity signature
Forpatientswithmetastatic colorectal cancer, standard-of-care first-line treatment options are either oxaliplatin oririnotecan-based therapies. However, response rates foreither drug regimen range between 40% and 45% (26). Asa first step in the goal to optimize therapy for colon cancerand to determine which patients would benefit fromoxaliplatin-based therapy, we used expression data fromNCI-60 cell lines (20) with known sensitivities to oxali-platin to develop a binary Bayesian model to predictoxaliplatin response. Genes whose expression was mosthighly correlated with sensitivity to oxaliplatin wereidentified, and these genes were then used to develop apredictive model that could differentiate between oxali-platin sensitivity and resistance.
First, we identified NCI-60 cell lines that were mostresistant or sensitive to oxaliplatin as defined by theiroxaliplatin GI50 (growth inhibition of 50%) values whilealso taking into consideration their TGI and LC50 values.Cell lines with a GI50 less than 0.5 mmol/L were consid-ered sensitive, and cell lines with a GI50 more than 20mmol/L were considered resistant (Supplementary TableS1). From these cell lines, corresponding RMA-estimatedgene expression array data were used for subsequentanalysis. However, one sensitive cell line, MCF-7, wasobserved to be a single outlier by 3D principal compo-nents analysis of global expressionvalues of all of theNCI-60 cell lines (Supplementary Fig. S1). Because of this,MCF-7 was omitted from the training set before develop-ing the predictor (Table 1).
Kim et al.
Mol Cancer Ther; 11(7) July 2012 Molecular Cancer Therapeutics1502
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937
To tune parameters in the model to give the largestseparation between binary phenotypes, a data-drivenempirical approach was taken to select the optimalnumber of genes to include in the predictor. The dis-criminatory power was evaluated using the misclassi-fication rate under leave-one-out performance (LOOP)with an a priori defined threshold of Pr � 0.5. Gene setsizes of 50 to 200 were considered. Note: because theLOOP is used to optimize the multigene models, nostatistical inferences are drawn from the cross-valida-
tion, and an independent validation is required to fullyassess their predictive value. After consideration, thefinal developed model consisted of 120 probes (Supple-mentary Table S2) based on prediction of oxaliplatinsensitivity and LOOP (Fig. 1).
Development of PDCCEsThe true value of a predictor lies in its ability to predict
sensitivity in an independent in vivo setting. To generate avalidation set to test our oxaliplatin sensitivity signature, a
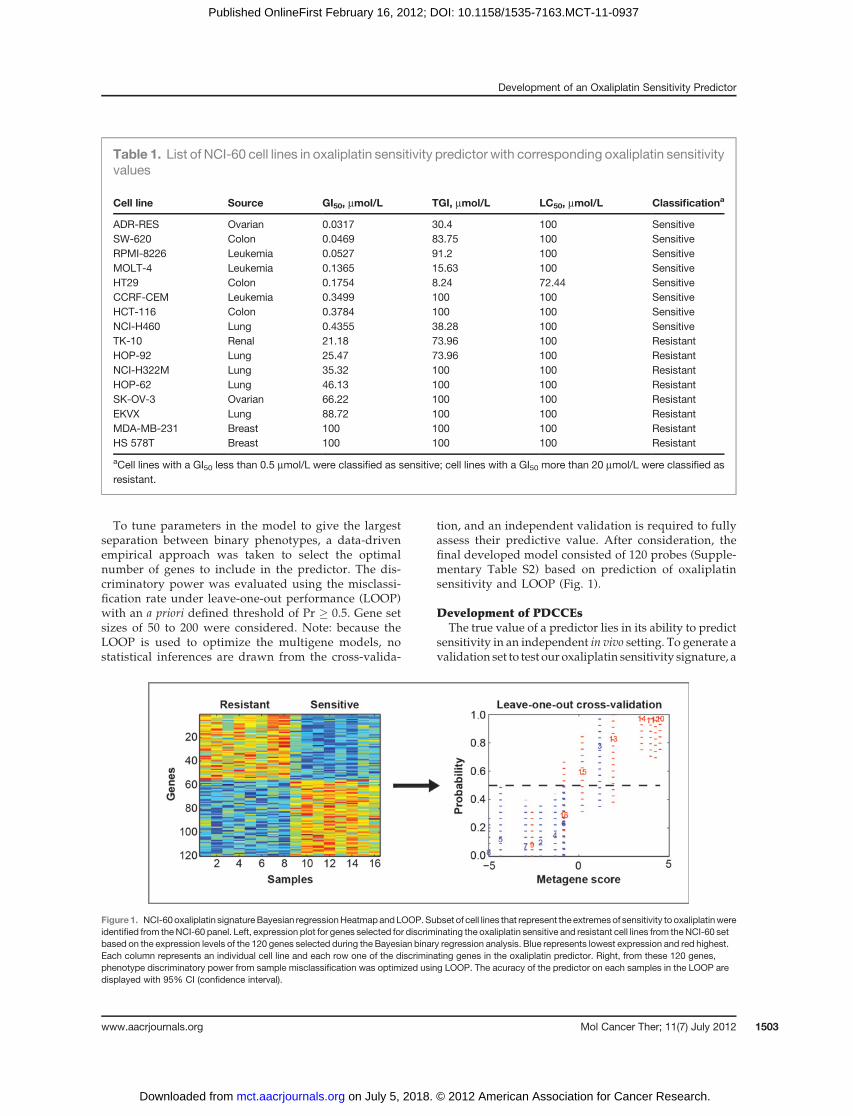
Table 1. List of NCI-60 cell lines in oxaliplatin sensitivity predictor with corresponding oxaliplatin sensitivityvalues
Cell line Source GI50, mmol/L TGI, mmol/L LC50, mmol/L Classificationa
ADR-RES Ovarian 0.0317 30.4 100 SensitiveSW-620 Colon 0.0469 83.75 100 SensitiveRPMI-8226 Leukemia 0.0527 91.2 100 SensitiveMOLT-4 Leukemia 0.1365 15.63 100 SensitiveHT29 Colon 0.1754 8.24 72.44 SensitiveCCRF-CEM Leukemia 0.3499 100 100 SensitiveHCT-116 Colon 0.3784 100 100 SensitiveNCI-H460 Lung 0.4355 38.28 100 SensitiveTK-10 Renal 21.18 73.96 100 ResistantHOP-92 Lung 25.47 73.96 100 ResistantNCI-H322M Lung 35.32 100 100 ResistantHOP-62 Lung 46.13 100 100 ResistantSK-OV-3 Ovarian 66.22 100 100 ResistantEKVX Lung 88.72 100 100 ResistantMDA-MB-231 Breast 100 100 100 ResistantHS 578T Breast 100 100 100 Resistant
aCell lines with a GI50 less than 0.5 mmol/L were classified as sensitive; cell lines with a GI50 more than 20 mmol/L were classified asresistant.
Figure 1. NCI-60oxaliplatin signatureBayesian regressionHeatmapandLOOP.Subset of cell lines that represent the extremesof sensitivity to oxaliplatinwereidentified from theNCI-60 panel. Left, expression plot for genes selected for discriminating the oxaliplatin sensitive and resistant cell lines from theNCI-60 setbased on the expression levels of the 120 genes selected during the Bayesian binary regression analysis. Blue represents lowest expression and red highest.Each column represents an individual cell line and each row one of the discriminating genes in the oxaliplatin predictor. Right, from these 120 genes,phenotype discriminatory power from sample misclassification was optimized using LOOP. The acuracy of the predictor on each samples in the LOOP aredisplayed with 95% CI (confidence interval).
Development of an Oxaliplatin Sensitivity Predictor
www.aacrjournals.org Mol Cancer Ther; 11(7) July 2012 1503
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937

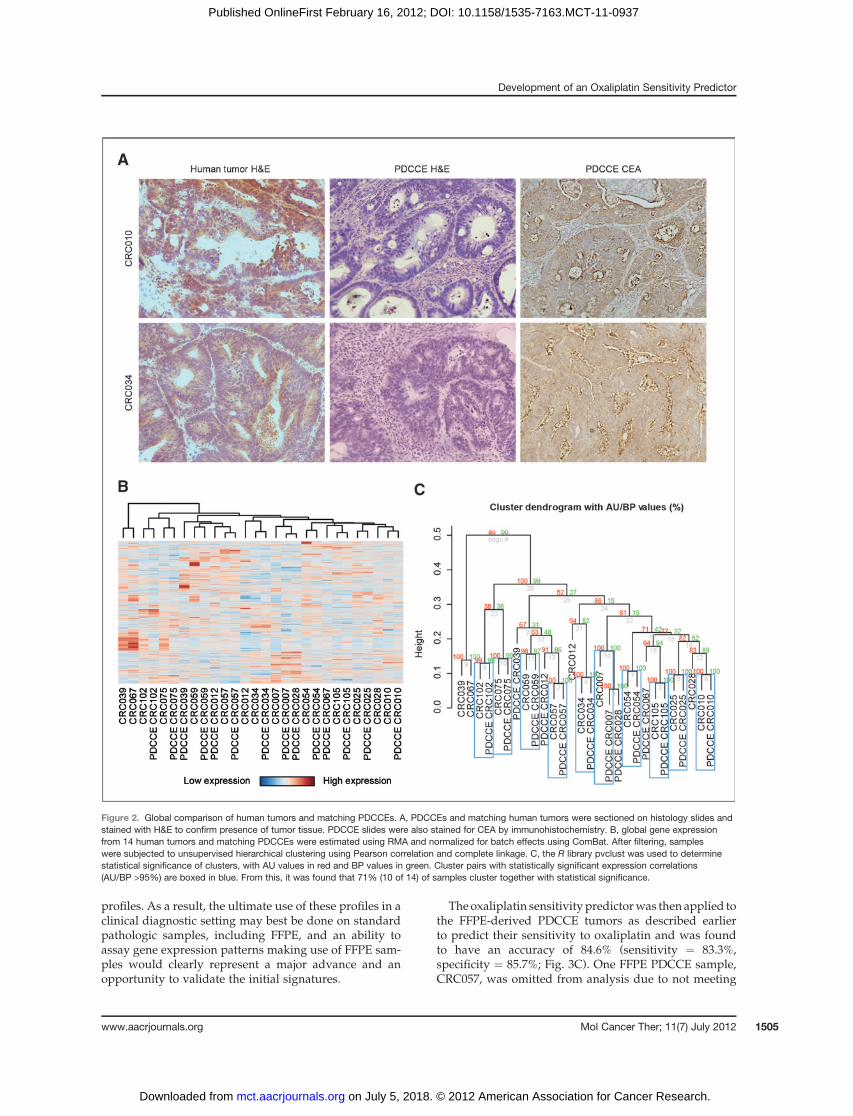
murine model was developed by generating humanmetastasis-derived colorectal cancer explants (PDCCE)in nonobese diabetic/severe combined immunodeficient(NOD/SCID) mice. Following surgical resection andpathologic assessment, excess tissue to be discarded wasimmediately processed to generate PDCCEs as describedearlier. A total of 20 resected tumors were injected intoSCID mice, and 14 PDCCEs (Table 2) have been estab-lished for an uptake rate of 70% (14 of 20). Of thesepatients, 9 of 14 did not receive any chemotherapy beforesurgical resection (neoadjuvant) and 9 of 14 receivedchemotherapy after surgical resection (adjuvant). Figure2A revealed that sections stained with H&E were consis-tent with adenocarcinoma and that immunohistochemis-try stains with carcinoembryonic antigen (CEA) wereconsistent with a colorectal cancer.
To determine the extent to which the underlying biol-ogy of a resected colorectal cancer metastatic tumor ismaintained when explanted into a murine model, globalgene expression analysis between the matched resectedpatient colorectal tumor and PDCCE was conducted.Initial 3D principal components analysis between thepatient tumors and the corresponding explants revealedbatch effects; therefore, tominimize these effects, the 2 setswere subsequently normalized using ComBat. An unsu-pervised hierarchical clustering was then carried out onCV-filtered expression data to generate a Heatmap ofclustered gene expression (Fig. 2B), which revealed that10 of 14 (71%) of the matched patient tumor samples andcorresponding PDCCEs clustered together with greaterthan 95%probability under resampling (Fig. 2C), suggest-ing that the global biology between the matched samplesare similar.
In vivo validation of the oxaliplatin predictorTo identify oxaliplatin-sensitive tumors, the 14PDCCEs
were treatedwith oxaliplatin as described earlier, andTGIwas monitored and recorded for each PDCCE duringtreatment (Supplementary Table S3). Figure 3A showsphotographs taken at time of PDCCE extraction to illus-trate the difference between oxaliplatin-sensitive (e.g.,CRC025) and oxaliplatin-resistant (e.g., CRC039)PDCCEs. The cutoff point for sensitivity was defined asthe arithmetic mean of the TGI values (mean ¼ 0.665).From these studies, 7 PDCCEswere identified as sensitive(TGI% <mean) and 7 PDCCEswere identified as resistant(TGI% > mean).
The accuracy of the oxaliplatin sensitivity predictorwasthen determined using drug sensitivity data derived fromthe PDCCEs treated with oxaliplatin. Using the definedcutoff point for sensitivity as described earlier, the oxali-platin sensitivity predictor was then applied to eachPDCCE (Table 3) and was found to have an accuracy of92.9% (sensitivity ¼ 87.5%, specificity ¼ 100%; Fig.3B). Figure 3B shows that there is a statistically significantcorrelation between predicted probability of oxaliplatinsensitivity and TGI% to oxaliplatin treatment (P ¼ 0.002).
In vivo validation of the oxaliplatin predictor in FFPEsamples
Finally, although microarray analyses are best con-ducted using minimally degraded RNA from freshlycollected cell lines or tumor tissue, the challenge of incor-porating a genomic signature into the clinical setting isthat fresh tissue samples can be limited and thereforeconstrains our ability to take these studies forward tobroad validations of the initially identified predictive
Table 2. PDCCEs with human origin and chemotherapy history
Tumor IDa Primary site Metastatic siteb Neoadjuvant chemotherapy Adjuvant chemotherapy
CRC007 Colon Liver None FOLFIRICRC010 Colon Liver None NoneCRC012 Colon Liver None N/ACRC025 Rectal Lung None XELOXCRC028 Colon Liver None FOLFOX þ bevacizumabCRC034 Colon Colon N/A XELOXCRC039 Colon Liver FOLFOX þ bevacizumab NoneCRC054 Colon Lung Xeloda FOLFOX þ bevacizumabCRC057 Colon Liver None FOLFIRI þ bevacizumabCRC059 Colon Colon N/A NoneCRC067 Colon Liver FOLFOX þ bevacizumab Xeloda þ bevacizumabCRC075 Colon Liver None FOLFOX þ bevacizumabCRC102 Colon Liver XELOX þ bevacizumab XELIRI þ bevacizumabCRC105 Colon Liver FOLFOX None
NOTE: FOLFOX ¼ oxaliplatin þ 5-fluorouracil (5-FU)/leucovorin; XELOX ¼ oxaliplatin þ xeloda; FOLFIRI ¼ irinotecan þ 5-FU/leucovorin; XELIRI ¼ irinotecan þ xeloda.aHuman tumors were extracted from their respective metastatic sites and implanted into NOD/SCID mice.bTumors labeled as colon in the metastatic site column are primary colon tumors.
Kim et al.
Mol Cancer Ther; 11(7) July 2012 Molecular Cancer Therapeutics1504
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937
profiles. As a result, the ultimate use of these profiles in aclinical diagnostic setting may best be done on standardpathologic samples, including FFPE, and an ability toassay gene expression patterns making use of FFPE sam-ples would clearly represent a major advance and anopportunity to validate the initial signatures.
The oxaliplatin sensitivitypredictorwas then applied tothe FFPE-derived PDCCE tumors as described earlierto predict their sensitivity to oxaliplatin and was foundto have an accuracy of 84.6% (sensitivity ¼ 83.3%,specificity ¼ 85.7%; Fig. 3C). One FFPE PDCCE sample,CRC057, was omitted from analysis due to not meeting
Figure 2. Global comparison of human tumors and matching PDCCEs. A, PDCCEs and matching human tumors were sectioned on histology slides andstained with H&E to confirm presence of tumor tissue. PDCCE slides were also stained for CEA by immunohistochemistry. B, global gene expressionfrom 14 human tumors and matching PDCCEs were estimated using RMA and normalized for batch effects using ComBat. After filtering, sampleswere subjected to unsupervised hierarchical clustering using Pearson correlation and complete linkage. C, the R library pvclust was used to determinestatistical significance of clusters, with AU values in red and BP values in green. Cluster pairs with statistically significant expression correlations(AU/BP >95%) are boxed in blue. From this, it was found that 71% (10 of 14) of samples cluster together with statistical significance.
Development of an Oxaliplatin Sensitivity Predictor
www.aacrjournals.org Mol Cancer Ther; 11(7) July 2012 1505
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937
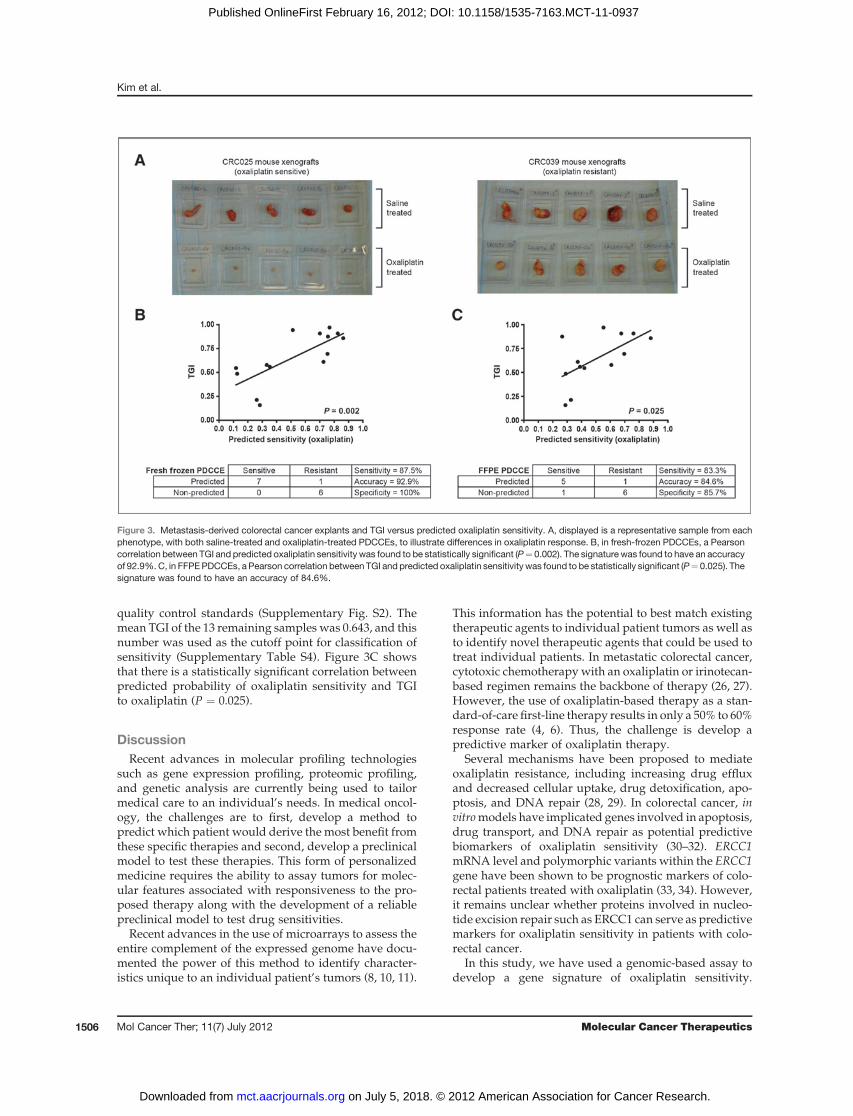
quality control standards (Supplementary Fig. S2). Themean TGI of the 13 remaining samples was 0.643, and thisnumber was used as the cutoff point for classification ofsensitivity (Supplementary Table S4). Figure 3C showsthat there is a statistically significant correlation betweenpredicted probability of oxaliplatin sensitivity and TGIto oxaliplatin (P ¼ 0.025).
DiscussionRecent advances in molecular profiling technologies
such as gene expression profiling, proteomic profiling,and genetic analysis are currently being used to tailormedical care to an individual’s needs. In medical oncol-ogy, the challenges are to first, develop a method topredict which patient would derive the most benefit fromthese specific therapies and second, develop a preclinicalmodel to test these therapies. This form of personalizedmedicine requires the ability to assay tumors for molec-ular features associated with responsiveness to the pro-posed therapy along with the development of a reliablepreclinical model to test drug sensitivities.
Recent advances in the use of microarrays to assess theentire complement of the expressed genome have docu-mented the power of this method to identify character-istics unique to an individual patient’s tumors (8, 10, 11).
This information has the potential to best match existingtherapeutic agents to individual patient tumors as well asto identify novel therapeutic agents that could be used totreat individual patients. In metastatic colorectal cancer,cytotoxic chemotherapywith an oxaliplatin or irinotecan-based regimen remains the backbone of therapy (26, 27).However, the use of oxaliplatin-based therapy as a stan-dard-of-care first-line therapy results in only a 50% to 60%response rate (4, 6). Thus, the challenge is develop apredictive marker of oxaliplatin therapy.
Several mechanisms have been proposed to mediateoxaliplatin resistance, including increasing drug effluxand decreased cellular uptake, drug detoxification, apo-ptosis, and DNA repair (28, 29). In colorectal cancer, invitromodels have implicated genes involved in apoptosis,drug transport, and DNA repair as potential predictivebiomarkers of oxaliplatin sensitivity (30–32). ERCC1mRNA level and polymorphic variants within the ERCC1gene have been shown to be prognostic markers of colo-rectal patients treated with oxaliplatin (33, 34). However,it remains unclear whether proteins involved in nucleo-tide excision repair such as ERCC1 can serve as predictivemarkers for oxaliplatin sensitivity in patients with colo-rectal cancer.
In this study, we have used a genomic-based assay todevelop a gene signature of oxaliplatin sensitivity.
Figure 3. Metastasis-derived colorectal cancer explants and TGI versus predicted oxaliplatin sensitivity. A, displayed is a representative sample from eachphenotype, with both saline-treated and oxaliplatin-treated PDCCEs, to illustrate differences in oxaliplatin response. B, in fresh-frozen PDCCEs, a Pearsoncorrelation between TGI and predicted oxaliplatin sensitivity was found to be statistically significant (P¼ 0.002). The signature was found to have an accuracyof 92.9%. C, in FFPEPDCCEs, a Pearson correlation between TGI and predicted oxaliplatin sensitivitywas found to be statistically significant (P¼ 0.025). Thesignature was found to have an accuracy of 84.6%.
Kim et al.
Mol Cancer Ther; 11(7) July 2012 Molecular Cancer Therapeutics1506
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937

However, genes identified in the predictor didnot includepreviously identified genes known to be involved inoxaliplatin resistance such as ERCC1 and other repairproteins, but instead consisted of genes known to beinvolved in oncogenesis [epidermal growth factor recep-tor (EGFR), insulin-like growth factor–binding protein(IGFBP7), VEGF-C, platelet-derived growth factor C(PDGFC), and CD44]. These genes were found to havelower expression in oxaliplatin sensitive cell lines and areconsistent with studies that show low levels of VEGF-Aand VEGF-C in oxaliplatin-sensitive cell lines (35), andthat cetuximab, which targets the EGFR pathway, canovercome oxaliplatin resistance (36).A frequently used strategy for identifying and testing
potentially effective drugs is to administer them to immu-nodeficient mice that have been implanted with well-characterized cancer cell lines that mimic human malig-nancies. However, these cell lines, having been derivedand repeatedly cultured over many years, may have littleresemblance to tumors growing in patients. Thus, a morereliable model is needed. Recently, the direct transplan-tation of resected gastrointestinal human tumors in micehas been developed as amore comparable model to studydrug sensitivities (17, 18), but it remains unclear whetheror not responses seen in these models are predictive ofclinical response. In our current study, we rapidlyengrafted metastatic colorectal cancers into NOD/SCIDmice and observed that the biology of the metastasis-derived colorectal cancer explants were similar to theircorresponding patient tumors based on gene expressionprofiling. It was, however, observed that 2 of the PDCCEs(CRC067 and CRC039) did not cluster with the rest of thesamples, suggesting that these tumorsmay have differentbiology, but this may be a result of these 2 patientsreceiving more chemotherapy [FOLFOX (oxaliplatin/
5-FU) þ bevacizumab] than the other 12 patients beforeresection of their cancer (Table 2). As a whole, we feel thatthese findings provide greater reassurance that theobserved antitumor effects in our murine model wouldbe similar to those observed in patients and thus provide apreclinical model to study drug sensitivities andmechanisms.
Our study has now shown both the ability to develop agenomic based predictor for oxaliplatin sensitivity andalso the capability to validate the accuracy of the predictorin a preclinical model. Furthermore, we have also shownthat our genomic based predictors can also be applied toFFPE samples, which are much more prevalent in theclinical setting. However, we do realize the limitations ofour study. First, in using the NCI-60 cell lines as ourtraining set, there were only 2 colon cancer cell lines thatwere classified as sensitive to oxaliplatin and no coloncancer cell lines that were classified as resistant to oxali-platin. This raises the question as towhether or not amorerobust colorectal cancer oxaliplatin sensitivity predictorcould be generated if only colorectal cancer cell lines areused. To attempt this, we treated 25 colorectal cancer celllines with oxaliplatin but found that there was only a 10-fold difference in oxaliplatin IC50 values between themostsensitive and most resistant cell lines (data not shown),which is consistent with another published report (31).Furthermore, when attempting to develop an oxaliplatinsensitivity signature from these colorectal cancer celllines, this signature was not able to predict response tooxaliplatin in the PDCCEs (data not shown). The discrep-ancy between the performance of the NCI-60 oxaliplatinsignature and the colorectal cancer cell line signature inpredicting oxaliplatin response in the PDCCE model ismost likely due to the greater than 100-fold difference inoxaliplatin IC50 values in the NCI-60 cell lines as opposed
Table 3. List of fresh-frozen PDCCEs with corresponding class and predicted response
Mouseexplant TGI
Identifiedclassificationa
Oxaliplatin-predictedprobability
Predictedresponseb
CRC007 0.907 Sensitive 0.826 RespondCRC010 0.875 Sensitive 0.757 RespondCRC012 0.486 Resistant 0.127 NonrespondCRC025 0.969 Sensitive 0.768 RespondCRC028 0.907 Sensitive 0.701 RespondCRC034 0.559 Resistant 0.353 NonrespondCRC039 0.159 Resistant 0.284 NonrespondCRC054 0.546 Resistant 0.118 NonrespondCRC057 0.943 Sensitive 0.512 RespondCRC059 0.214 Resistant 0.262 NonrespondCRC067 0.578 Resistant 0.332 NonrespondCRC075 0.694 Sensitive 0.754 RespondCRC102 0.858 Sensitive 0.863 RespondCRC105 0.611 Resistant 0.726 Respond
aEach sample was identified as either resistant or sensitive to oxaliplatin based on the TGI cutoff value of 0.665.bPredicted response to oxaliplatin was determined by the oxaliplatin predicted probability cutoff value of 0.5.
Development of an Oxaliplatin Sensitivity Predictor
www.aacrjournals.org Mol Cancer Ther; 11(7) July 2012 1507
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937

to the 10-fold difference in the purely colorectal cancer celllines, suggesting that to develop a reliable and accuratechemotherapy sensitivity predictor, the difference in sen-sitivity to a drug must be greater than 2 logs.
Second, we must also be very careful in extrapolatingresults from a preclinical model to potential patient out-come. In our preclinical model, the PDCCEs were onlytreated for 2.5 weeks, and outcome was measured byresponse to drug. Although, there are studies in colorectalcancer suggesting that response rate can be a surrogate forsurvival (37), response rate is still not an accepted endpoint in clinical trials. In addition, although single-agentoxaliplatin is not typically used in the initial treatment ofcolorectal cancer due to poor response rates (2%–10%), itmust be noted that these trials were mainly small phase IItrials (38–40). However, given these limitations, we mustbe careful with interpreting these results within a clinicalsetting.
Nevertheless, while this only serves as a proof-of-concept study, it is still a crucial first step in bringing apredictive biomarker to the clinic. However, before apredictive biomarker can become clinically relevant, itmust undergo rigorous preclinical testing to gauge itsaccuracy, reliability, and reproducibility. The next cru-cial step is the retrospective validation of our oxaliplatinsensitivity predictor in patient samples, and this mustbe carried out on multiple patient samples to furthervalidate the signature’s predictive capabilities before itcan finally be prospectively tested in a clinical trial.Thus, the strength of our study lies in the power of ourpreclinical murine model coupled with gene expressiontechnology to identify and test novel combinations oftherapeutic agents and also to develop both predictive
and prognostic biomarkers that can then be systemat-ically brought forth into the clinical setting. Moreimportantly, this now lays down the foundation for thedevelopment and validation of future genomic basedbiomarkers in a preclinical model before clinicalassessment.
Finally, the capacity of a genomic based signature topredict response in preclinical models begins to define astrategy for personalized medicine and also presentsthe ability to identify cytotoxic agents that best matchindividual patients with advanced colorectal cancer.Although these strategies will need to be eventuallyvalidated in clinical trials, this model is the first step inevaluating the performance of genomic signature–basedselection in the individualized treatment strategy forpatients with metastatic colorectal cancer.
Disclosure of Potential Conflicts of InterestM.Datto is a consultant/on advisory board of Affymetrix. No potential
conflicts of interest were disclosed by the other authors.
AcknowledgmentsThe authors thank the Duke microarray core facility for collecting the
microarray data.
Grant SupportThis work was supported by grants from the Charles Scott Research
Fund and the Mentored Research Scholars Grant (119824-MRSG-10-195-01-TBG) from the American Cancer Society.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedNovember 16, 2011; revised January 13, 2012; accepted January16, 2012; published OnlineFirst February 16, 2012.
References1. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J
Clin 2010;60:277–300.2. Andre T, Bensmaine MA, Louvet C, Francois E, Lucas V, Desseigne F,
et al. Multicenter phase II study of bimonthly high-dose leucovorin,fluorouracil infusion, and oxaliplatin for metastatic colorectal cancerresistant to the same leucovorin and fluorouracil regimen. J Clin Oncol1999;17:3560–8.
3. August DA, Sugarbaker PH, Ottow RT, Gianola FJ, Schneider PD.Hepatic resection of colorectalmetastases. Influenceof clinical factorsand adjuvant intraperitoneal 5-fluorouracil via Tenckhoff catheter onsurvival. Ann Surg 1985;201:210–8.
4. Saltz LB,ClarkeS,Diaz-Rubio E, ScheithauerW, Figer A,WongR, et al.Bevacizumab in combination with oxaliplatin-based chemotherapy asfirst-line therapy in metastatic colorectal cancer: a randomized phaseIII study. J Clin Oncol 2008;26:2013–9.
5. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J,Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, andleucovorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335–42.
6. Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M,et al. Randomized, phase III trial of panitumumab with infusionalfluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4alone as first-line treatment in patients with previously untreatedmetastatic colorectal cancer: the PRIME study. J Clin Oncol 2010;28:4697–705.
7. Golub TR. Genome-wide views of cancer. N Engl J Med 2001;344:601–2.
8. Golub TR, Slonim DK, Tamayo P, Huard C, Gaasenbeek M, MesirovJP, et al. Molecular classification of cancer: class discovery and classprediction by gene expression monitoring. Science 1999;286:531–7.
9. PerouCM,Sorlie T, EisenMB, vandeRijnM, JeffreySS, ReesCA, et al.Molecular portraits of human breast tumours. Nature 2000;406:747–52.
10. Rosenwald A, Wright G, Chan WC, Connors JM, Campo E, Fisher RI,et al. The use of molecular profiling to predict survival after chemo-therapy for diffuse large-B-cell lymphoma. N Engl J Med 2002;346:1937–47.
11. Shipp MA, Ross KN, Tamayo P, Weng AP, Kutok JL, Aguiar RC, et al.Diffuse large B-cell lymphoma outcome prediction by gene-expres-sion profiling and supervised machine learning. Nat Med 2002;8:68–74.
12. Lee JK, Havaleshko DM, Cho H, Weinstein JN, Kaldjian EP, KarpovichJ, et al. A strategy for predicting the chemosensitivity of humancancers and its application to drug discovery. Proc Natl Acad SciU S A 2007;104:13086–91.
13. Riddick G, Song H, Ahn S, Walling J, Borges-Rivera D, Zhang W, et al.Predicting in vitro drug sensitivity using Random Forests. Bioinfor-matics 2011;27:220–4.
14. Staunton JE, Slonim DK, Coller HA, Tamayo P, Angelo MJ, Park J, ,et al. Chemosensitivity prediction by transcriptional profiling. ProcNatlAcad Sci U S A 2001;98:10787–92.
15. SuggittM,BibbyMC.50 yearsof preclinical anticancer drug screening:empirical to target-driven approaches. Clin Cancer Res 2005;11:971–81.
Kim et al.
Mol Cancer Ther; 11(7) July 2012 Molecular Cancer Therapeutics1508
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937

16. Alley M, Hollingshead MG, Dykes DJ, Waud WR. Human tumorxenograft models in NCI drug development. In:Teicher BA, AndrewsPA, editors. Anticancer drug development guide. Totowa, NJ: HumanaPress; 2004. p. 125–52.
17. Pitts TM, Tan AC, Kulikowski GN, Tentler JJ, Brown AM, Flanigan SA,et al. Development of an integrated genomic classifier for a novel agentin colorectal cancer: approach to individualized therapy in early devel-opment. Clin Cancer Res 2010;16:3193–204.
18. Rubio-Viqueira B, Jimeno A, Cusatis G, Zhang X, Iacobuzio-Dona-hue C, Karikari C, et al. An in vivo platform for translational drugdevelopment in pancreatic cancer. Clin Cancer Res 2006;12:4652–61.
19. DTP Human Tumor Cell Line Screen [Internet]. Washington, DC:Developmental Therapeutics Program, National Cancer Institute;[updated 2011 Nov 2; cited 2012 Jan 13]. Available from: dtp.nci.nih.gov/docs/cancer/cancer_data.html.
20. ShankavaramUT, ReinholdWC, Nishizuka S,Major S, Morita D, CharyKK, et al. Transcript and protein expression profiles of the NCI-60cancer cell panel: an integromic microarray study. Mol Cancer Ther2007;6:820–32.
21. discover.nci.nih.gov [internet]. Washington, DC: Genomics and Bioin-formaticsGroup,NationalCancer Institute; [updated2012Jan12; cited2012 Jan 13]. Available from: http://discover.nci.nih.gov/cellminer/.
22. FileMerger [Internet]. Durham, NC: Duke University [updated July 1,2011; cited 2012 Jan 13]. Available from: filemerger.genome.duke.edu.
23. Bild AH, YaoG,Chang JT,WangQ, Potti A, ChasseD, et al. Oncogenicpathway signatures in human cancers as a guide to targeted therapies.Nature 2006;439:353–7.
24. Irizarry RA, Bolstad BM, Collin F, Cope LM, Hobbs B, Speed TP.Summaries of Affymetrix GeneChip probe level data. Nucleic AcidsRes 2003;31:e15.
25. Johnson WE, Li C, Rabinovic A. Adjusting batch effects in microarrayexpression data using empirical Bayes methods. Biostatistics 2007;8:118–27.
26. Tournigand C, Andre T, Achille E, Lledo G, Flesh M, Mery-Mignard D,et al. FOLFIRI followed by FOLFOX6 or the reverse sequence inadvanced colorectal cancer: a randomized GERCOR study. J ClinOncol 2004;22:229–37.
27. Grothey A, Sargent D, Goldberg RM, Schmoll HJ. Survival of patientswith advanced colorectal cancer improves with the availability offluorouracil-leucovorin, irinotecan, and oxaliplatin in the course oftreatment. J Clin Oncol 2004;22:1209–14.
28. WangD, Lippard SJ. Cellular processing of platinum anticancer drugs.Nat Rev Drug Dis 2005;4:307–20.
29. Siddik ZH. Cisplatin: mode of cytotoxic action and molecular basis ofresistance. Oncogene 2003;22:7265–79.
30. Plasencia C, Martinez-Balibrea E, Martinez-Cardus A, Quinn DI, AbadA, Neamati N. Expression analysis of genes involved in oxaliplatinresponse and development of oxaliplatin-resistant HT29 colon cancercells. Int J Oncol 2006;29:225–35.
31. Arango D, Wilson AJ, Shi Q, Corner GA, Aranes MJ, Nicholas C, et al.Molecular mechanisms of action and prediction of response to oxa-liplatin in colorectal cancer cells. Br J Cancer 2004;91:1931–46.
32. Arnould S, Hennebelle I, Canal P, Bugat R, Guichard S. Cellulardeterminants of oxaliplatin sensitivity in colon cancer cell lines. EurJ Cancer 2003;39:112–9.
33. Shirota Y, Stoehlmacher J, Brabender J, Xiong YP, Uetake H,Danenberg KD, et al. ERCC1 and thymidylate synthase mRNAlevels predict survival for colorectal cancer patients receiving com-bination oxaliplatin and fluorouracil chemotherapy. J Clin Oncol2001;19:4298–304.
34. ParkDJ, ZhangW,Stoehlmacher J, Tsao-Wei D,GroshenS,Gil J, et al.ERCC1 gene polymorphism as a predictor for clinical outcome inadvanced colorectal cancer patients treated with platinum-basedchemotherapy. Clin Adv Hematol Oncol 2003;1:162–6.
35. Dallas NA, Xia L, Fan F, LimSJ, GrayMJ, Samuel S, et al. Resistance ofcolon cancer cells to 5-FU or oxaliplatin enriches for tumor stem cells.Gastrointestinal Cancer Symposium 2008. Abstract nr 305.
36. Prewett M, Deevi DS, Bassi R, Fan F, Ellis LM, Hicklin DJ, et al. Tumorsestablishedwith cell lines selected for oxaliplatin resistance respond tooxaliplatin if combined with cetuximab. Clin Cancer Res 2007;13:7432–40.
37. Buyse M, Thirion P, Carlson RW, Burzykowski T, Molenberghs G,Piedbois P. Relation between tumour response to first-line chemo-therapy and survival in advanced colorectal cancer: a meta-analysis.Meta-Analysis Group in Cancer. Lancet 2000;356:373–8.
38. Becouarn Y, Ychou M, Ducreux M, Borel C, Bertheault-Cvitkovic F,Seitz JF, et al. Phase II trial of oxaliplatin as first-line chemotherapy inmetastatic colorectal cancer patients. Digestive Group of FrenchFederation of Cancer Centers. J Clin Oncol 1998;16:2739–44.
39. Diaz-Rubio E, Sastre J, Zaniboni A, Labianca R, Cortes-Funes H, deBraud F, et al. Oxaliplatin as single agent in previously untreatedcolorectal carcinoma patients: a phase II multicentric study. AnnOncol1998;9:105–8.
40. Machover D, Diaz-Rubio E, de Gramont A, Schilf A, Gastiaburu JJ,BrienzaS, et al. Twoconsecutive phase II studies of oxaliplatin (L-OHP)for treatment of patients with advanced colorectal carcinoma whowere resistant to previous treatment with fluoropyrimidines. AnnOncol1996;7:95–8.
Development of an Oxaliplatin Sensitivity Predictor
www.aacrjournals.org Mol Cancer Ther; 11(7) July 2012 1509
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937
2012;11:1500-1509. Published OnlineFirst February 16, 2012.Mol Cancer Ther Mickey K. Kim, Takuya Osada, William T. Barry, et al. Preclinical Murine Model of Colorectal CancerCharacterization of an Oxaliplatin Sensitivity Predictor in a
Updated version
10.1158/1535-7163.MCT-11-0937doi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2012/02/16/1535-7163.MCT-11-0937.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/11/7/1500.full#ref-list-1
This article cites 35 articles, 15 of which you can access for free at:
Citing articles
http://mct.aacrjournals.org/content/11/7/1500.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/11/7/1500To request permission to re-use all or part of this article, use this link
on July 5, 2018. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst February 16, 2012; DOI: 10.1158/1535-7163.MCT-11-0937