Embed Size (px)
Citation preview

183
Chapter
9 Urinary System ♦ Components of the Urinary System -The urinary system consists of 2 kidneys, 2 ureters, 1 urinary bladder, and 1 urethra (Figure 26.1, Tortora). 1. kidneys - The kidneys are involved in several functions: a. The kidneys filter blood of wastes and any excess substances. -The cells of the body continuously release waste products into the blood as a result of normal metabolic reactions. -Some of these waste products include urea, ammonia, creatinine, uric acid, and urobilin. -Urea and ammonia (NH3) are formed in hepatocytes as a result of the deamination of amino acids. -Recall that the deamination of an amino acid causes the production of ammonia and a keto acid. -Most of the ammonia is converted to urea, which is released into the blood as a waste product. -The rest of the ammonia, however, remains unconverted and is also released into the blood as a waste product. -Creatinine is formed in skeletal muscle fibers (cells) as creatine phosphate is catabolized. -Uric acid is formed in body cells from the breakdown of nucleic acids. -Urobilin is a yellowish pigment that is responsible for the color of urine; it is derived from the breakdown of hemoglobin via a complex pathway that involves macrophages, the liver, and the intestines (Figure 19.5, Tortora). -Note that urea, uric acid, creatinine, ammonia, and urobilin are called nitrogenous wastes because they are waste products that contain nitrogen atoms. -All of these waste products must be excreted from the body because they are toxic to cells. -The kidneys are the body’s main excretory organ; they filter the blood of these waste products and then concentrate them in a fluid called urine. -In addition, the kidneys channel any substances in excess of the body’s needs into the urine as well. -These excess substances include H2O and electrolytes (ions) like Na+, K+, Ca+2, H+, and HCO3
- (bicarbonate).

184
-Hence, urine is the fluid produced by the kidneys, consisting of waste products and any excess substances not needed by the body. b. The kidneys maintain body fluid volume and solute composition. -The kidneys regulate the amount of water and electrolytes that are present in the body. c. The kidneys regulate the blood pH. -The kidneys along with the lungs are involved in maintaining the blood pH at 7.4. 2. ureters -tubes that transport urine from the kidneys to the urinary bladder 3. urinary bladder -a hollow organ that stores urine 4. urethra -a duct that tranports urine from the urinary bladder to the exterior of the body -Pathway of Urine Flow: A Summary The kidneys produce urine. From each kidney, the urine passes into the ureter and then into the urinary bladder. Urine is stored in the urinary bladder until it is released out of the body through the urethra, a process called micturition. ♦Characteristics of Urine -Figure 9.1 (Derrickson) lists various characteristics of normal urine.
185
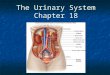
♦Kidneys -Location -The kidneys are located towards the back near the lumbar vertebrae (Figure 26.2, Tortora). -The lower part of the rib cage partially covers the kidneys, thereby providing these organs with some protection. -The kidneys are said to be retroperitoneal because of their location behind the peritoneum. -In other words, the kidneys are located behind the digestive organs. -Size -A typical adult kidney has the following dimensions: • length: 4 inches • width: 3 inches -Structure -External Anatomy -There are 3 layers of connective tissue that surround each kidney, holding it firmly in place (Figure 26.2, Tortora): 1. renal fascia -outer layer 2. adipose capsule -middle layer 3. renal capsule -inner layer -fuses directly to the wall of the kidney -renal hilum -a depression located near the center of each kidney (Figure 26.3, Tortora) -the area where blood vessels, lymphatic vessels, nerves, and the ureter enter or leave the kidney -Internal Structure -There are 4 major internal regions of the kidney (Figure 26.3, Tortora): 1. renal cortex -outer layer of the kidney -extends from the renal capsule to the medulla -also dips down in between sections of the medulla as the renal columns.

186
2. renal medulla -inner layer of the kidney -consists of cone-shaped masses called the renal pyramids renal pyramids -consist of parts of the renal tubules -Each renal pyramid has a base and an apex. -The base of the renal pyramid faces the renal cortex. -The apex of the renal pyramid is called the renal papilla and it drains into the minor calyx. 3. calyces -The minor and major calyces (singular is calyx) are cup-like structures located beyond the renal papillae. -Several minor calyces collect urine from the renal papillae. Urine then flows into a major calyx. From the major calyx, the urine flows into the renal pelvis. 4. renal pelvis -a large cavity that is continuous with the ureter -allows urine to pass from the major calyx into the ureter -Histology -Each kidney consists of about 1 million microscopic units called nephrons (Figures 9.2 and 9.3, Derrickson). nephron -the functional unit of the kidney -2 components 1. glomerulus -a knot of capillaries 2. renal tubule -a single layer of epithelial cells that line a lumen -The renal tubule is divided into the following regions: a. Bowman’s capsule -also called the glomerular capsule -the beginning part of the renal tubule -surrounds the glomerulus b. proximal tubule -Most of the proximal tubule is convoluted (bent). -Hence, the term proximal convoluted tubule is often used.

187
c. loop of Henle -also called the nephron loop -consists of 1. descending thin limb (DTL) 2. ascending thin limb (ATL) 3. thick ascending limb (TAL) d. distal tubule -The distal tubule is also convoluted. -Hence, the term distal convoluted tubule is often used. e. collecting duct -the terminal part of the renal tubule -Renal Vasculature -Figures 26.4 and 26.5c (Tortora) illustrate the blood supply of the kidneys. -Of all of the blood vessels pictured, just know the ones that are listed below: 1. renal artery -brings oxygenated blood to the kidney 2. afferent arteriole -gives rise to the glomerulus 3. glomerulus -a knot of capillaries -surrounded by Bowman’s capsule 4. efferent arteriole -forms from the glomerulus 5. peritubular capillaries -branch off of the efferent arteriole -surround the upper parts of the renal tubule (i.e. the proximal tubule, distal tubule, and cortical collecting duct) 6. vasa recta -extensions of the peritubular capillaries -surround the lower parts of the renal tubule (i.e. the loop of Henle and medullary collecting duct) 7. renal vein -drains the kidney of deoxygenated blood -Note that the nephron is associated with several capillary beds: the glomerulus, peritubular capillaries, and the vasa recta. -Renal Blood Flow -The renal blood flow (RBF) is the rate of blood flow through both kidneys per minute. -Under normal resting conditions, RBF = 1200 mL/min. -Renal Fraction -The renal fraction (RF) is the amount of the cardiac output (CO) that passes through both kidneys per minute. RBF RF = CO

188
-Under normal resting conditions, the RF is about 20%: 1200 mL/min RF = ≈ 0.20 5250 mL/min -Hence, every minute about 20% (one-fifth) of your cardiac output passes through the kidneys for processing. -Mechanism of Urine Formation -In order to form urine, blood in the glomerulus is filtered into the renal tubule, a process called glomerular filtration, and the resulting glomerular filtrate moves through the nephron where it is further modified. -Hence, the formation of urine requires 2 major processes: (1) glomerular filtration and (2) modification of the filtrate through the renal tubule (Figure 9.2, Derrickson). 1. glomerular filtration -the process by which blood in the glomerulus is filtered into the lumen of Bowman’s Capsule -occurs at the renal corpuscle renal corpuscle -consists of a. glomerulus -a knot of capillaries b. Bowman’s capsule -also called the glomerular capsule -the beginning of the renal tubule -surrounds the glomerulus -consists of 2 layers (Figure 26.6, Tortora): 1. parietal layer -outer layer of epithelial cells that are continuous with the epithelial cells of the rest of the renal tubule 2. visceral layer -consists of specialized epithelial cells called podocytes that are fused to the glomerulus Bowman’s space -also called the capsular space -the space between the parietal and visceral layers of Bowman’s capsule -continuous with the lumen of the rest of the renal tubule
189
-During glomerular filtration, fluid enters from the blood into Bowman’s space, where it is called glomerular filtrate or just filtrate. -This fluid is not called urine until it flows out of the nephron and into the renal calyces. -Note that the fluid that becomes the filtrate must pass through a subcomponent of the renal corpuscle called the filtration membrane. filtration membrane -includes the glomerulus and the visceral layer (podocytes) of Bowman’s capsule -consists of the following layers in the order in which substances in the blood of the glomerulus must pass to reach Bowman’s space (Figure 26.8, Tortora): a. endothelium of the glomerulus -single layer of epithelial cells -The endothelium contains pores (holes) called fenestrations. b. basal lamina of the glomerulus -consists of connective tissue -surrounds the endothelium -also contains pores c. visceral layer of Bowman’s capsule (podocytes) -The podocytes contain foot-like processes called pedicels. -Between the pedicels are porous spaces called filtration slits (slit pores). -Glomerular Filtrate -also called filtrate -the fluid produced in Bowman’s space upon filtration of blood at the filtration membrane of the renal corpuscle -Composition a. H2O -main component b. nutrients -glucose, amino acids, etc. c. ions -Na+, K+, Ca+2, HCO3
-, H+, etc. d. wastes -urea, ammonia, uric acid, creatinine, urobilin, etc. -Blood cells and most proteins in the blood (albumin, fibrinogen, hemoglobin, etc.) are too large to fit through the pores of the filtration membrane.
190
–The only proteins that are small enough to be filtered are protein hormones (LH, HCG, etc.) and their concentrations are extremely low. –Hence, the glomerular filtrate is similar to blood in composition except for the fact that it is cell-free and contains almost no protein. -Glomerular Filtration Rate -The glomerular filtration rate (GFR) is the amount of glomerular filtrate formed each minute in all nephrons of both kidneys. -Under normal resting conditions, the GFR = 125 mL/min. ⇒ Hence, the total quantity of glomerular filtrate formed each day is typically 180 L ! 2. modification of filtrate through the renal tubule -As the filtrate moves through each nephron, it is further modified by the processes of reabsorption and secretion (Figure 9.2, Derrickson). • Needed substances (nutrients, H2O, ions, etc.) in the filtrate are reabsorbed, while wastes and excess substances that are already in the filtrate are not reabsorbed and eventually become part of the urine. reabsorption -In this context, reabsorption refers to the transport of a substance from the lumen of the renal tubule into the blood. -Substances reabsorbed in the proximal tubule, distal tubule, and cortical collecting duct move from the lumen of these regions of the renal tubule into the blood of the peritubular capillaries. -Substances reabsorbed in the loop of Henle and the medullary collecting duct move from the lumen of these regions of the renal tubule into the blood of the vasa recta -Under normal conditions, about 99% of the filtrate contains needed substances, while the remaining 1% consists of wastes and excess substances. –Hence, as filtrate moves through all of the renal tubules of both kidneys, about 99% of it is reabsorbed, while the remaining 1% (about 1.5 L/day) moves into the renal calyces and is then called urine. • Additional wastes and excess substances in the blood are secreted into the filtrate to eventually become part of the urine. secretion -In this context, secretion refers to the transport of a substance from the blood into the lumen of the renal tubule.
191
-Reabsorptive and Secretionary Activities of Different Regions of the Renal Tubule a. proximal tubule -Structure -The cells of the proximal tubule contain microvilli (Figure 9.4, Derrickson). microvilli -finger-like projections of the cell membranes of absorptive cells -increase the surface area for absorption -also called the brush border because the microvilli resemble the bristles of a brush -The microvilli of the proximal tubule cells are loaded with protein transporters that are involved in the processes of reabsorption and secretion. -The plasma membranes of the cells of the remaining parts of the renal tubule (i.e. loop of Henle, distal tubule, and collecting duct) lack microvilli. –This indicates that these cells do not reabsorb as much solute as the cells of the proximal tubule. –Only a small amount of solute reabsorption occurs in the rest of the renal tubule. –Hence, the presence of microvilli correlates with high solute reabsorption. -Functions -The proximal tubule has 5 major functions (Figures 9.4 and 9.5, Derrickson): 1. The proximal tubule reabsorbs 100% of filtered glucose and amino acids. -Under normal dietary conditions, transporters within the plasma membrane of each proximal tubule cell continuously reabsorb all of the glucose and amino acids in the filtrate. -Therefore, no glucose or amino acids should be present in the urine. -Note, however, that the transporters for glucose do have a limit to the amount of glucose that can be reabsorbed just as an elevator has a limit to the amount of people that it can transport at one time; this limit is called the transport maximum (Tm). -Suppose that the glucose concentration in the blood is higher than normal (as in diabetes or a diet high in junk food).

192
Then the glucose concentration in the filtrate will also become higher than normal as the blood is filtered at the glomerulus. If the glucose concentration in the filtrate exceeds the Tm of the glucose transporters, then the glucose transporters become saturated . Consequently, some of the glucose is not reabsorbed and eventually becomes part of the urine --a condition called glucosuria. -There is also a transport maximum for the amino acid transporter. -Higher than normal concentrations of amino acids in the blood (and subsequently the filtrate) lead to saturation of these transporters and some of the amino acids will eventually become part of the urine, a condition called aminoaciduria. 2. The proximal tubule reabsorbs 65% of the filtered ions (Na+, K+, Ca+2 , etc.) and H2O. -The reabsorption of these ions is continuous and involves membrane transporters. -The reabsorption of H2O is also continuous and it occurs as H2O follows reabsorbed solutes (glucose, amino acids, ions, etc.) via osmosis. 3. The proximal tubule secretes H+ ions and reabsorbs HCO3
- ions. -In the proximal tubule, the secretion of H+ ions is coupled with the reabsorption of HCO3- ions. -This function of the proximal tubule depends on the pH of blood: -If the pH of blood becomes too acidic (ex: respiratory acidosis), the proximal tubule cells respond by increasing H+ ion secretion and by increasing HCO3
- reabsorption. -If the pH of the blood becomes too alkaline (ex: respiratory alkalosis), the proximal tubules respond by decreasing H+ ion secretion and by decreasing HCO3
- reabsorption.

193
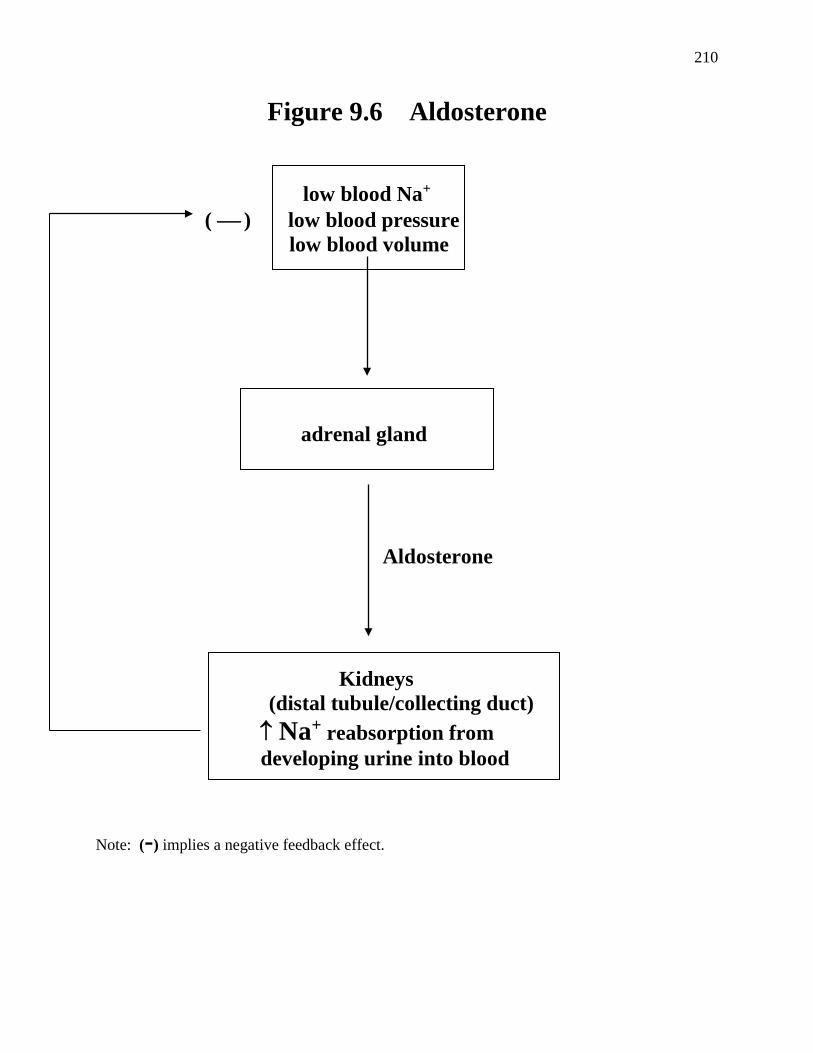
4. The proximal tubule secretes drugs. -The proximal tubule continuously removes drugs like penicillin and aspirin from the blood and then secretes them into the filtrate. 5. The proximal tubule secretes wastes. -The proximal tubule continuously secretes more wastes (like creatinine) from the blood into the filtrate. b. Loop of Henle -Functions -The loop of Henle has 2 major functions (Figure 9.5, Derrickson): 1. The loop of Henle reabsorbs about 20% of the filtered ions (Na+, K+,Ca+2, etc.). -The reabsorption of these ions is continuous. 2. The loop of Henle reabsorbs about 15% of the filtered H2O. -The reabsorption of this H2O is continuous. c. distal tubule -Functions -The distal tubule has 3 major functions (Figures 9.5, Derrickson): 1. The distal tubule reabsorbs variable amounts of filtered ions (especially Na+ and Ca+2 ). -The reabsorption of these ions in the distal tubule is not continuous, but rather is subject to hormonal regulation depending on the body’s nutritional needs. ♣ The reabsorption of Na+ ions in the distal tubule (and the collecting duct) is dependent on the hormone aldosterone . -Aldosterone is secreted by the adrenal gland in response to the following stimuli (Figure 9.6, Derrickson): • low blood Na+ -The importance of blood Na+ regulation is described in Figure 9.7 (Derrickson). • low blood volume • low blood pressure

194
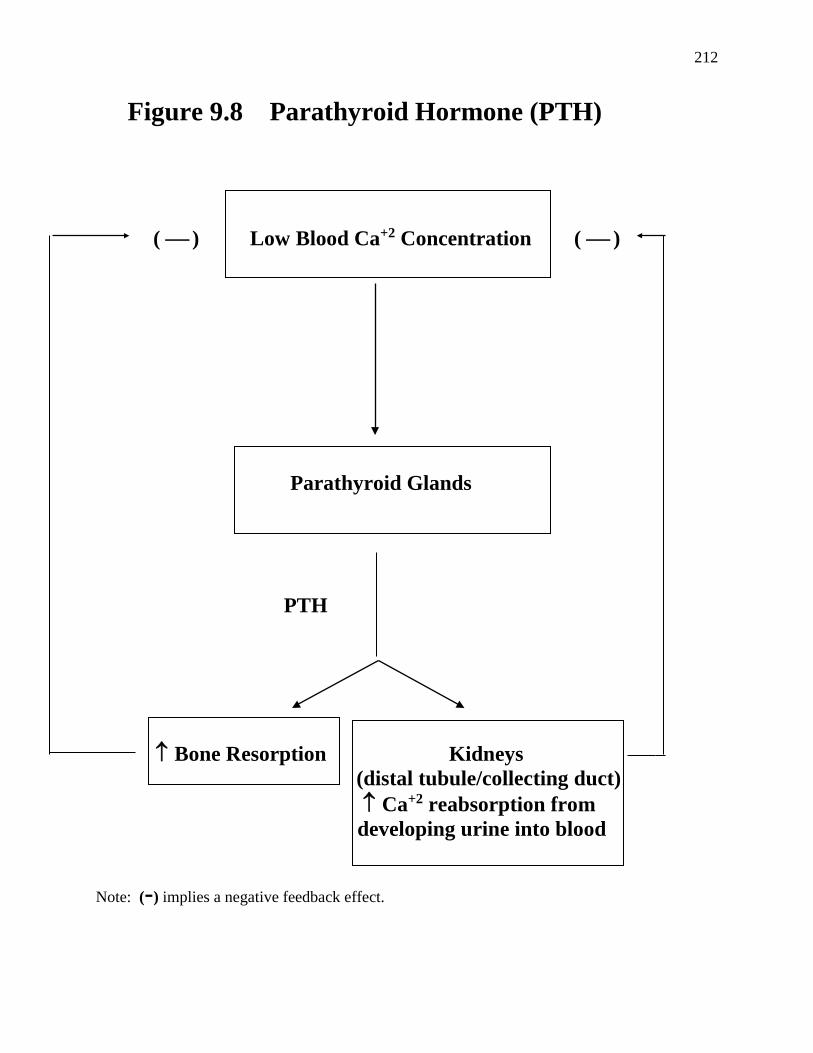
-Aldosterone functions to increase the blood volume and blood pressure back to normal. -The way that aldosterone achieves this goal is by stimulating the cells of the distal tubule and the collecting duct to reabsorb Na+ ions. This Na+ ion reabsorption then causes H2O reabsorption via osmosis (as long as the hormone ADH is present). Consequently, blood volume and blood pressure increase back to normal. -In the absence of aldosterone, Na+ ions are not reabsorbed by the cells of the distal tubule and the collecting duct; they remain in the filtrate and eventually become part of the urine. ♣ The reabsorption of Ca+2 ions in the distal tubule (and the collecting duct) is dependent on parathyroid hormone (PTH). - PTH is released by the parathyroid glands in response to a low blood Ca+2 concentration (Figure 9.8, Derrickson). -The importance of blood Ca+2 regulation is described in Figure 9.9 (Derrickson). -The main function of PTH is to increase the blood Ca+2 concentration back to normal. -One way that PTH accomplishes this function is by stimulating the cells of the distal tubule and the collecting duct to reabsorb Ca+2 ions. -In the absence of PTH, Ca+2 ions are not reabsorbed by the cells of the distal tubule and the collecting duct; they remain in the filtrate and eventually become part of the urine.

195
2. The distal tubule reabsorbs about 10% of the filtered H2O. -The reabsorption of this H2O is not continuous, but rather is subject to hormonal regulation depending on the body’s nutritional needs. -The reabsorption of H2O in the distal tubule is dependent on antidiuretic hormone (ADH). -ADH is a hormone released by the posterior pituitary gland in response to the following stimuli (Figure 9.10, Derrickson): • dehydration • low blood volume • low blood pressure -ADH functions to increase blood volume and blood pressure back to normal. - One way that ADH achieves this goal is by stimulating H2O reabsorption in the distal tubule and the collecting duct. -The distal tubule can reabsorb about 10% of the filtered H2O as long as ADH is present. -Note that in the absence of ADH, H2O is not reabsorbed in the distal tubule nor in the collecting duct. 3. The distal tubule secretes H+ ions and reabsorbs HCO3
- ions. -In the distal tubule (as in the proximal tubules), the secretion of H+ ions is coupled with the reabsorption of HCO3- ions. -This function of the distal tubule depends on the pH of blood: -If the pH of blood becomes too acidic (ex: respiratory acidosis), the distal tubule cells respond by increasing H+ ion secretion and by increasing HCO3
- reabsorption. -If the pH of the blood becomes too alkaline (ex: respiratory alkalosis), the distal tubule cells respond by decreasing H+ ion secretion and by decreasing HCO3
- reabsorption.

196
d. collecting duct -Functions -The collecting duct has 3 major functions (Figure 9.5, Derrickson): 1. The collecting duct reabsorbs variable amounts of filtered ions (especially Na+ and Ca+2 ). -The reabsorption of these ions in the collecting duct is not continuous, but rather is subject to hormonal regulation depending on the body’s nutritional needs. ♣ The reabsorption of Na+ ions in the collecting duct is dependent on the hormone aldosterone (Figure 9.6, Derrickson) . ♣ The reabsorption of Ca+2 ions in the collecting duct is dependent on the hormone PTH (Figure 9.8, Derrickson). 2. The collecting duct secretes H+ ions and reabsorbs HCO3
- ions. -In the collecting duct (as in the proximal tubules and distal tubule), the secretion of H+ ions is coupled with the reabsorption of HCO3- ions. -This function of the collecting duct depends on the pH of blood: -If the pH of blood becomes too acidic (ex: respiratory acidosis), the collecting duct cells respond by increasing H+ ion secretion and by increasing HCO3
- reabsorption. -If the pH of the blood becomes too alkaline (ex: respiratory alkalosis), the collecting duct cells respond by decreasing H+ ion secretion and by decreasing HCO3
- reabsorption. 3. The collecting duct reabsorbs about 9% of the filtered H2O. -The collecting duct can reabsorb about 9 % of the filtered H2O as long as ADH is present (Figure 9.10, Derrickson). -Under normal conditions, there is a small amount of ADH present in the blood. -This normal amount of ADH in the blood results in the production of about 1.5 L/day of urine

197
that is slightly hyperosmotic (i.e. slightly concentrated). -If the body becomes dehydrated (examples: decreased water intake, sweating, or hemorrhage) the blood level of ADH increases above the normal level. -As a result, even more water is reabsorbed from the filtrate in the distal tubule and collecting duct, which causes the urine to become even more hyperosmotic (i.e. very concentrated). -The urine flow rate under these conditions is about 300 ml/day. -In the absence of ADH, a large volume (about 35 L/day) of hypoosmotic (dilute) urine is produced by the kidneys. -This is due to the fact that about 20% of the filtered water is not reabsorbed in the absence of ADH (10% in the distal tubule and 10% in the collecting duct). -Figure 9.11 (Derrickson) summarizes the effects of ADH. ♦Acid-Base Balance -Overview -The normal blood pH = 7.4 (i.e. blood is slightly alkaline). pH = - log [H+ ion] acidosis -a condition in which the pH of blood is below 7.35 alkalosis -a condition in which the pH of blood is above 7.45 -Acidic Products of Metabolism (Sources of H+ ions) -Various metabolic reactions generate acidic products that can lower the pH of blood. 1. CO2 -a waste product generated from aerobic respiration in body cells glucose + O2 CO2 + H2O + 32 ATP (energy)

198
-CO2 can lead to the release of H+ ions into the blood as illustrated in the following reaction: carbonic CO2 + H2O H2CO3 H+ + HCO3
- anhydrase carbonic acid ♠ When the CO2 concentration is high, CO2 combines with H2O to form H2CO3. -Recall that an acid is defined as a compound that releases a H+ ion into solution. -Accordingly, H2CO3 dissociates into a H+ ion and a HCO3
- (bicarbonate) ion. -This reaction is catalyzed by the enzyme carbonic anhydrase and occurs in red blood cells (Figure 9.12, Derrickson). -However, the products (H+ and HCO3
- ) are eventually released into the surrounding plasma. –Note that the release of H+ ions from H2CO3 causes the blood pH to decrease (become acidic). 2. lactic acid -an acidic waste product generated from anaerobic respiration in skeletal muscle glucose lactic acid + 2 ATP (energy) 3. fatty acids - acidic products generated from lipid catabolism in adipose tissue 4. ketones -acidic products generated from fatty acids in the liver -Acidosis occurs when these acidic products of metabolism are not removed from the blood. -Alkalosis occurs when these acidic products of metabolism are removed from the blood too quickly. -Effect of Acidosis -The major effect of acidosis is depression of the CNS, which can lead to disorientation, coma, and even death. -Effects of Alkalosis • CNS hyperexcitability • muscle hyperexcitability -Death can occur if the respiratory muscles contract too much and out of sequence.

199
-Types of Acidosis and Alkalosis -Acidosis and alkalosis are categorized by the cause of the condition. -Respiratory acidosis and respiratory alkalosis are caused by the inability of the respiratory system to regulate the concentration of the gas CO2 in the blood. -Compensation occurs by the kidneys (i.e. renal compensation). -Metabolic acidosis and metabolic alkalosis are caused by the inability of the kidneys to regulate the concentration of dissolved acids in the blood. -Dissolved acids are defined as any type of acid except for the one generated from CO2; examples of dissolved acids include lactic acid, fatty acids, and ketones. -Compensation occurs by the respiratory system (i.e. respiratory compensation). ♣ Respiratory Acidosis -Definition -Respiratory acidosis is a condition in which the pH of blood is below 7.35 due to an abnormally high concentration of CO2 in the blood. -Cause hypoventilation -reduced breathing -may be due to asphyxia (airway obstruction), emphysema, narcotic or barbiturate overdose (results in depression of respiratory centers), etc. -Hypoventilation causes an increase in the blood concentration of CO2 : -When the CO2 concentration is high, the carbonic anhydrase reaction shifts to the right in effort to get rid of some of the CO2 (Figure 9.12, Derrickson). carbonic CO2 + H2O H2CO3 H+ + HCO3
- anhydrase carbonic acid -This reaction results in the formation of H+ ions, which causes the pH of blood to become acidic. -Treatment: Renal Compensation -The cells of the proximal tubule, distal tubule, and collecting duct eliminate the respiratory acidosis by increasing their secretion of H+ ions into the urine and by increasing their reabsorption of HCO3
- ions into the blood (Figure 9.4, Derrickson).

200
♣ Respiratory Alkalosis -Definition -Respiratory alkalosis is a condition in which the pH of blood is above 7.45 due to an abnormally low CO2 concentration in the blood. -Cause hyperventilation -excessive breathing -may be due to anxiety/emotions or being at a high altitude -Hyperventilation causes a decrease in the blood concentration of CO2 : -When the CO2 concentration is low, the carbonic anhydrase reaction shifts to the left in effort to generate more CO2
(Figure 9.13, Derrickson). carbonic CO2 + H2O H2CO3 H+ + HCO3
- anhydrase carbonic acid -The HCO3
- ion acts as a base by removing a H+ ion from the blood to form H2CO3. -Recall that a base is defined as a compound that removes a H+ ion from solution. -The H2CO3 is then converted into CO2 and H2O. -Since H+ ions have been removed from the blood by HCO3
-, the pH becomes more alkaline. -Treatment: Renal Compensation -The cells of the proximal tubule, distal tubule, and collecting duct eliminate the respiratory alkalosis by decreasing their secretion of H+ ions into the urine and by decreasing their reabsorption of HCO3
- ions into the blood (Figure 9.4, Derrickson). ♣ Metabolic Acidosis -Definition -Metabolic acidosis is a condition in which the pH of blood is below 7.35 due to an abnormally high concentration of dissolved acids in the blood. -Possible Causes 1. rapid loss of large amounts of HCO3
- -This occurs during severe diarrhea. 2. ketoacidosis -high concentration of ketones in the blood -This occurs due to starvation or untreated diabetes mellitus

201
3. lactic acidosis -high concentration of lactic acid in the blood -This can occur after very strenuous exercise. 4. alcoholism -At a high concentration, alcohol is converted into various types of acids. -Treatment: Respiratory Compensation hyperventilation -This response of the respiratory system eliminates the metabolic acidosis by removing CO2 (and hence H+ ions) from the blood. -In other words, the carbonic anhydrase reaction shifts to the left (Figure 9.13, Derrickson). carbonic CO2 + H2O H2CO3 H+ + HCO3
- anhydrase carbonic acid ♣ Metabolic Alkalosis -Definition -Metabolic alkalosis is a condition in which the pH of blood is above 7.45 due to an abnormally low concentration of dissolved acids in the blood. -Cause rapid loss of H+ ions from the body -This occurs during vomiting. -Treatment: Respiratory Compensation hypoventilation -This response of the respiratory system eliminates the metabolic alkalosis by retaining CO2 (and hence H+ ions) in the blood. -In other words, the carbonic anhydrase reaction shifts to the right (Figure 9.12, Derrickson). carbonic CO2 + H2O H2CO3 H+ + HCO3
- anhydrase carbonic acid

202
♦Clinical Applications and Disorders -Look up the following clinical applications and disorders in Tortora: 1. nephroptosis p. 997 2. diuretics p. 1022 3. abnormal constituents in urine p. 1023 (Table 26.6) 4. dialysis p. 1024 5. urinary incontinence p. 1027 6. renal calculi p. 1030 7. urinary tract infections p. 1030 8. glomerular diseases p. 1032 9. renal failure p. 1032 10. polycystic kidney disease p. 1032 11. urinary bladder cancer p. 1032 12. kidney transplant p. 1033 13. cystoscopy p. 1033 14. azotemia p. 1033

203
15. cystocele p. 1033 16. enuresis and nocturnal enuresis p. 1033 17. intravenous pyelogram p. 1033 18. polyuria p. 1033 19. stricture p. 1033 20. urinary retention p. 1033

204
Figure 9.1 Characteristics of Normal Urine Volume: ≈1.5 L / day Color: light yellow pH: acidic (usually around pH 6) Composition: Nitrogenous Wastes urea • the main waste product in urine • derived from the catabolism of amino acids in hepatocytes ammonia • also derived from the catabolism of amino acids in hepatocytes creatinine • derived from the breakdown of creatine phosphate in skeletal muscle fibers uric acid • derived from the breakdown of nucleic acids in body cells urobilin • a yellowish pigment that is responsible for the color of urine • derived from the breakdown of hemoglobin via a complex pathway that involves macrophages, the liver, and intestine Excess Substances H2O • the main component of urine electrolytes (Na+, K+, Ca+2, H+, and HCO3
-) ⇒ The concentrations of these substances vary depending on body needs. Other Substances hormones • present in minute quantities ketones (ketone bodies) • derived from lipid catabolism • normally present only in trace amounts • concentration increases during diabetes mellitus & starvation ⇒ A high ketone concentration in the urine causes the urine to have a fruity (sweet) odor. any drugs (legal or illegal) that a person has taken

205
Figure 9.2 Overview of the Nephron

206
Figure 9.3 Components of the Nephron

207
Figure 9.4 The Proximal Tubule

208
Figure 9.5 Reabsorption and Secretion in the Renal Tubule (Under Normal Conditions/Adequate Body Hydration) GFR = 125 mL/min or 180 L/day Proximal Tubule • continuous reabsorption of 100 % of filtered glucose and amino acids • continuous reabsorption of 65% of filtered H2O and ions (Na+, K+, Ca+2 , etc.) • pH-dependent secretion of H+ ions and reabsorption of filtered HCO3
- ions. • continuous secretion of drugs • continuous secretion of wastes Loop of Henle • continuous reabsorption of 20% of filtered ions (Na+, K+, Ca+2 , etc.) • continuous reabsorption of 15% of filtered H2O Distal Tubule • Aldosterone-dependent reabsorption of filtered Na+ ions. • ADH-dependent reabsorption of 10% of filtered H2O. • PTH-dependent reabsorption of filtered Ca+2 ions. • pH-dependent secretion of H+ ions and reabsorption of filtered HCO3
- ions. Collecting Duct • Aldosterone-dependent reabsorption of filtered Na+ ions. • PTH-dependent reabsorption of filtered Ca+2 ions. • pH-dependent secretion of H+ ions and reabsorption of filtered HCO3
- ions. • ADH-dependent reabsorption of 9 % of filtered H2O. The remaining 1% (1.5 L) of filtrate (H2O, wastes, any unreabsorbed ions, etc.) leaves the collecting duct and enters the calyces as slightly hyperosmotic urine.

209
Figure 9.5 (continued)
210
Figure 9.6 Aldosterone
low blood Na+ ( ) low blood pressure
low blood volume adrenal gland Aldosterone Kidneys (distal tubule/collecting duct) ↑ Na+ reabsorption from developing urine into blood
Note: (-) implies a negative feedback effect.

211
Figure 9.7 Blood Na+ Concentration Normal Blood Na+ Concentration 145 mEq/L Hyponatremia Hypernatremia • deficiency of Na+ ions • an excess of Na+ ions in the blood in the blood • may lead to hypotension, • may lead to excessive muscle weakness, mental thirst, hypertension, confusion, and coma and convulsions
212
Figure 9.8 Parathyroid Hormone (PTH) ( ) Low Blood Ca+2 Concentration ( ) Parathyroid Glands PTH ↑ Bone Resorption Kidneys (distal tubule/collecting duct) ↑ Ca+2 reabsorption from developing urine into blood
Note: (-) implies a negative feedback effect.

213
Figure 9.9 Blood Ca+2 Concentration Normal Blood Ca+2 Concentration 5 mEq/L Hypocalcemia Hypercalcemia • deficiency of Ca+2 ions • an excess of Ca+2 ions in the blood in the blood • may lead to muscle cramps, • may lead to cardiac arrest muscle tetany, hyperactive muscle weakness, mental reflexes, numbness confusion, and coma

214
Figure 9.10 ADH dehydration ( ) low blood pressure low blood volume posterior pituitary ADH Kidneys (distal tubule/collecting duct) ↓ urine output : movement of H20 from developing urine into blood Note: (-) implies a negative feedback effect.

215
Figure 9.11 Body Hydration, ADH, and Urine Dehydration Low [H2O] in blood High [ADH] in blood Urine • very hyperosmotic (dark yellow) • low volume (as low as 0.2% of filtrate ≈ 300 mL/day) More H2O is reabsorbed in the DT and CD than normal, allowing less than 0.2% of filtrate to enter pelvis as urine. Normal Hydration Adequate [H2O] in blood Low [ADH] in blood Urine • slightly hyperosmotic (light yellow) • normal volume (1% of filtrate ≈ 1.5 L/day) Overhydration High [H2O] in blood No ADH in blood Urine • hypoosmotic (clear) • high volume (as high as 20% of filtrate ≈ 35 L/day) 20 % of the filtered water remains unreabsorbed in the absence of ADH (10% in the DT + 9% in the CD + the 1% that normally leaves the kidney).

216
Figure 9.12 Hypoventilation

217
Figure 9.13 Hyperventilation