Embed Size (px)
Citation preview

CHAPTER II
BASIC CONSEPT
A. Growing and Development
1. Definition
a. Growing
Growing is increasing of physical size ( anatomy ) and body
structur in the sense part or all of body beause of multiplication ( many
increase ) body cells and because of cell enlarge ( Nursalam, 2005:32 ).
Growing is a natural process that happen on individu there is step
by step child will be more heaviness and tall (Supartini, 2002 : 49).
b. Characterístic of Growth
According to Hidayat (2008), characteristic of child growth are:
1) During growth will be cahnge in physical, suhc as body weight, tall,
head circle, arm circle, chest circle, and another.
2) Dueing growth will be change proportion that can seen on physical or
human organ that occur Stara from conception until adult.
3) In growing and development past of characteristic that appear during
growth, likes thymus glan, the loss of milk teeth or the loss of certain
reflexes
4) In growth there is a new feature is slowly following the maturation
process as the hair on the axilla area, pubic, or chest.

c. Detection of Growth and normal standard
Detection and normal Standard of growth according to Nursalam
(2005:47), are:
1) Antropometry Size
Meassuring of antropometry to know physical size a children with use
certain of size equipment like scales and measuring tape.
Anthropometry measurement can be grouped into two depending on
age and not dependent age. And anthropometric measurements were
used to measure, weight, height, head scale, upper arm scale, and skin
fold.
2) All of physical
With physical examination, can get that child where being sick or
health. Related with growth, things that can be observe from physical
examination is all of body, muscle tissue, hair, and tooth.
3) Laboratory and Radiology Examination
Laboratory and radiology examination can be done in clinic if any
sign or symptoms of disease, for example anemia or abnormality of
physical growth. Laboratory examination which often is the
examination of blood for Hb, serum proteins (albumin and globulin),
and growth hormone. Radiological examinations performed primarily
to assess the biological age, is the bone age.
4) Detection of development
Detection of development to give toddler nursing care.
d. The growth of the baby (10 month year old)
According Hidayat (2005:23), at the age of 10 months of growth
in body weight can occur twice body weight at born and average 500-600
gram per month if get well nutrition. Where as tall no increasing on
growth and occur stabilization based on age add.
Development
According to Hidayat (2005:15-16), events on the child's
development can occur on a change of form and function of organ
maturation begins from social, emotional, and intellectual aspect.
Development of physical can happen in size change large and small of the
organ function start from cell stage until organ change of body.
Development of intellectual can seen from ability symbols or abstract
such as speak, play, account, read, and another, whereas emotional
development of children can seen from social behavior in children around.
Development is a process that happen stimulant with growing that
produce individual quality to function matured and learning process from
environment (Supartini, 2002: 49).
Development is ability and structure or body function which more
complex in stable pattern, can be predicted for result from cell
differentiation process, body tissue, organs, and organized system
(Pusponegoro, 2004: 369).
2. Growth and Development Phase

Growth and Development Phase according to Soetjiningsih (2002) is:
Growth and development phase (2002) are:
a. Prenatal period ( born concept ), divided into:
1) Fetus embryo : conception period until 8 weeks
2) Fetus period : 9 weeks until birth
b. Postnatal period, divided into:
1) Neonatal period 0 – 28 days
a) Early neonatal ( prenatal ) : 0 – 7 days
b) Advance neonatal : 8 – 28 days
2) Baby period
a) Early baby period : 1 – 12 months
b) Last baby period : 1 – 2 years
c. Preschool period (3 – 6 years)
d. School age period ( 6 – 12 years )
e. Teenager period ( 13 – 18 years )
3. Theory of Growth and Development
a. According to Freud
Frued said if child psychosocial development consists of oral phase, falik
phase, and genital phase.
1) Oral Phase (0 – 11 months)

During enjoyment baby limited in oral activity look likes suck, bit,
chew and say. Detention or unsatisfied in oral need compliance will
effect to the next phase of development.
2) Anal phase (1 – 3 years)
Life child with centrally in child enjoyment, there is during sphincter
muscle development. Child happy to hold up the feces, eventually
playing their feces as they want, so toilet training is the best time to do
in this period.
3) Falik phase (3 – 6 years)
During this phase, genital has been interesting area and sensitive body
area. Child start learns different sex stuff. In psychosocial this phase
start growing super ego, there is child with decreasing of their ego.
4) Pelitescent phase (6 – 12 years)
During this phase child use physical energy and psychological that
include media for explore knowledge and experience by physical
activity or their social.
5) Phase genital (12 – 18 years)
The last development phase according to freud is phase when child
entry pubertal phase, there is whit any mature process of sex organs
and sex hormone production.
b. Psychosocial development according to Erickson

Erikson's approach in discussing the process of child development is by
using the five stages of psychosocial development, there is:
1) Relieve and unbelieve (0 – 1 years)
Investment confidence is The most basic thing in this phase.
Establishment of trust got from relationships with other people and the
man who first connected are parents, especially his mother. Therefore
mothers need support especially from her husband to foster a close
relationship with the child.
2) Autonomy vs. shame and doubt
The development of autonomy based on the ability of children for
control the body and its environment. Children want to do the things
he wanted to do by their self with use ability that they have like
walking, tiptoe, climb, and choice toys or stuff that they wanted. In
this phase, children will imitate the behavior of others around them
and this is a learning process.
3) Initiative vs. guilt (3 – 6 years)
Initiative developing got by assets the environment by own sense
ability. Child developing they wanted with explore what around them.
Guilty will be occur to child if child cannot achiever so they
unsatisfied with them development that has not achieved.
4) Industry vs Inferiority (6 – 12 years)

Child can learn walking for cooperate and compete with another child
by activity that was done well in academic or association by game that
was done together. Autonomy start developing in this phase,
especially in early 6 years old with the closest family support. Child
ability to interact more with friend around can facilitate success feels
development (sense of industry).
5) Identity vs wrong role (12 – 19 years)
Adult will try to dapted as they role as child that were trantition phase
from child to adult. They show them role with dressy as adult wich
very close with them group, interact with adopted group value and
environment to take own decicion. Clarity identity was goten if any
decicion wich get from parent or environment they place wich help
them by searching self identity process as adult, where as unability to
solved conflict will occur wrong role that must be done (Supartini,
2004: 59 – 63)
B. Brhoncopneumoniae
1. Definition
Pneumoniae is lower acute respiratory infection, wich hit lungs
parenkim (Mansjoer, 2000 : 465)
Pneumoniae is infalamation that hit distal lungs parenkim from adalah
peradangan yang mengenai parenkim paru distal dari terminalist

broncheolous wich includes respiratory broncheolous and alveoli and occur
disturbance of gas exchange arround (Dahlan, 2007 : 964).
Pneumoniae is lungs inflamation that caused of many etiology such as
bacterial, virus, ang foreign body (Hassan, 2005 : 1228)
Brhoncopneumoniae also can called an inflamation on lungs parenkim
that caused of bacterial, virus, fungus or foreign body wich signed fever,
anxiety, dispnoe, tachipsnoe, fast and shallow breath, vomiting, diarrhea, dry
and productive cough (Hidayat, 2006 : 80).
Brhoncopneumoniae is obstruction on the las brhoncheolous that
obstruct by exudate, mukoprulent, to built consolidation plaques in lobus
(Wong, 2004 : 460)
From above definition can be concluded brhoncopneumoniae is
infalamtion on lungs parenkim that caused of bacterial, virus, fungus, or
foreign body agent that can be disturb gas exchange on the last brhonceolous
because of exudate so built consolidation plaques in lobus.
2. Etiology
According to Hidayat (2006 : 80) etiology from brhoncpneumoniae
are:
a. Bacterial
Strepcoccocus pneumoni, staphylococcus aureus.
b. Virus
The most often virus is parainfluenzae, influenzae, adenovirus and RSV.
c. Foreign Body

d. Fungus
Hystoplasm, capsulatum, cryptoccus neoformans.
e. Aspiration
Aspiration can be happen because drink a lot of kerosone or gasoline,
food. And foreign body.
According to Ngastiyah (2005 : 577), another factor that can influence
pneumoniae is decreasing of body imune, for example because malnutrition
of protein energy ( MEP ), chronic disease, traumatic lungs, anesthesia,
aspiration, and unperfect antibiotic medication .
3. Pathophysiology
If patogen germ reach terminalist broncheoly edema fluid entry to
alveoli inclusion leoucosite in large quantity, then macrofag will cleans debris
cell and bacterial. This process ussually spread more far enlargement or just
in the same lobus, or maybe to another part of lungs by brnchials fluid that
has been infected through lungs limph lines, bacterial can reach blood flow
because lungs tissue has been consolidation occur shunt from right to left
with perfution ventilation so can occur mismacth, on hypoxiae. Heart work
maybe increasing because of oxygen saturation has been decrease and
hyperchapneoa in severe condition, can be happen respiratory failure
(Nursalam, 2005: 114- 115)
According to Hasan (2005:1229-1230), Pneumococcus entry to lungs
through droplet.
Infalamtion process can be divided in four stage:

a. Hyperemia stadium : refer to inflamation early response that was
happening in lung which was infected. This is as sign as increasing of
blood flow and permeabillity capiler in infected area. This Hyperemia
because of mediators release from mast cell after imune cell activation
and traumatic tissue. Mediator icludes hystamine and prostaglandine .
Degranulation mast cell also activated complemen lungs line. Complemen
work with hystamine and prostaglandine to relax smooth lungs muscle
and increasing capiler permeabillity. This is can cause plasmae exudate
movement into interstitial so occur oedem and edema between capiler and
alveoli increasing distance that must be reach by oxygen and
carbondioxide to disfution, so decreasing of gas difution has been happen.
Because less of oxygen disolved better than carbondioxide, so gas
movement into blood most influence, that most cause decreasing of
oxygen haemoglobine saturation.
b. Red hepatization Stadium: lobes and lobules that have been hit become
tight and without air, clour become red and like hepar palpation. In
alveoli got fibrin, leoucosite neoutrofile, exudate and more erytocite and
microbe. This stadium last very short.
c. Gray Stadium hepatization: lobes still tight and red colors become pale
gray. Superficies pleura look pale because be around of. Alveolus
contains of fibrin and leukocyte, place of phagocytes pneumococcus.
Caviler not congestive any more.

d. Resolution Stadium: exudates are decrease into alveoli, macrophage and
leucosticte been necrosis and lipid degeneration, Fibrin have been
resorting and disappear.
Pathway
Inflammatory process
Entry in airway
Bacteria, viruses, fungi / foreign body
Germs growing in the bronchus
Increasing of body temperature
Body's immune compensation issue (Ig E) Bronchospasm
Pathogen Reach the bronchi
Increased capillary permeability
Cough, nausea, vomiting
Increased mucus production
Mast cell degranulation
Anorexia
Difficulty breathing
Airway constriction
Prostaglandin
Swelling between capillary and alveolus
Transfer the plasma into the space exudates interstitial
Histamine
Fever
Risk of infection
Ineffective breathing patternIncreased blood flow in the
bronchi and pulmonary vascular muscles Nutrition less
than body requirements

(Modification: Nelson, 2000: 885; Nursalam, 2005: 114-115; Hasan,
2005: 1229-1230)
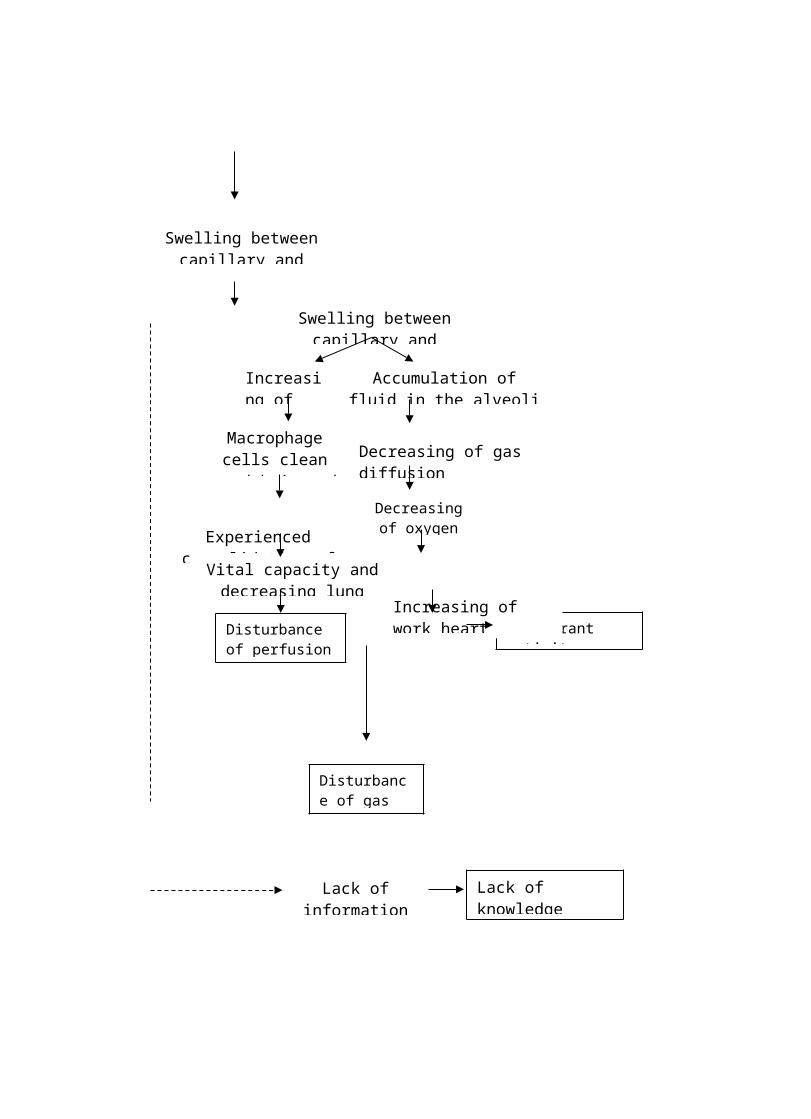
Swelling between capillary and alveolus
Macrophage cells clean up debris and
bacterial
Decreasing of gas diffusion
Decreasing of oxygen saturation
Experienced consolidation of lung tissue
Vital capacity and decreasing lung complains
Accumulation of fluid in the alveoli
Increasing of leukocyte
Intolerant activityFatigue
Increasing of work heart
Disturbance of perfusion tissue
Disturbance of gas exchanges
Lack of information
Lack of knowledge

4. Clinical Manifestation
According to Corwin (2000:413), shymthomps of pneoumoniae like
to all kind of pneoumoniae. This shymthomps includes:
a. Fever and shake because of inflamation process
b. Productive and purulent cough
c. Red Sputum (for streptococcus pneumoniae) pink (for stapilococcus
aureus) or greeny with khas smell (for pseudomonas aeruginosa)
d. Krekel (additional lung sounds)
e. Pleura pain because of inflamation and oedema
f. Maybe occur cyanosis shymptomps
5. Supporting Examination
According to Marry (2005 : 230), supporting examination on
brhoncopeoumonia are :
a. Radiologyst Examination
This examination as description brhoncogram fluid (airspace disease)
b. Chest X-Ray
Chest X-Ray will show plaques infiltrate
c. Blood culture, gram colouration, culture sputum can get caused organism.
d. Pulmonary Fungciont Examination
Volume maybe will be decrease (congestive, and alveoli colaps), airway
pressure can increase and decrease. Maybe will be seeped.
Cemas pada ortu dan anak

e. Laboratory
Description of pheriperal blood showed leoucocyte can reach 15.000 –
40.000 / mm3
f. Spirometric statistic
Used to assest air volume that have been inspirated.
6. Treatment
a. Medical
According to Ngastiyah (2000:58-59) medical threatment that must
done are:
1) Penicillin 50.000 u/kg bodyweight perdays,
added with cloronifenikol /50-70 mg bodyweight perday or give
antibiotic that have large spectrum such as amphycillin. This medication
give continuesly until no fevevr in 4-5 days .
2) Oxygenation and intravenous therapy fluid,
usually needs 5 % glucose and NaCl 0,9 % combination for comparison
3 : 1 added KCL 10 mg/500ml/bottle.
3) Because majority patient suffer acidose into
metabolic acidose because lack of nutrition and hypolena, so can give
correct whereas with the result of artery blood gas analysis.
4) Patient with light brhoncopneumoniae not need
to hozpitalisation.

b. Nursing
According to Ngastiyah (2000:58-59) nursing threatment that must
be done are:
1) Keep breathing continuity
Patient pneoumoniae where in dyspnoe and cyanosis condition because
of any pulmonary inflamation and amount of mucus in bronchous or
lungs. So patient can take a breath continuesly, that mucus must be
through out for reach oxygenation needed help with oxygen therapy 2
literperminutes.
2) Resting Needed
Pneoumoniae patient is weak patient, high body temperature, often
hyperexia so patient need more resting, all of patient needed must been
helped on the bed. Taking assesment contain or injection donot give when
patient still take a rest, try to make patient happy and comfort so patient can
take a rest well.
3) Observation Body Temperature
Pneoumoniae patient sometimes can got hyperexiae. For this, so body
temperature must be observe every hours beside try to decrease body
temperature with cold compress.
4) Lack of parent knowledge about the disease

Education especially shown to prevent pneoumoniae is with give about
definition. If chil suffer common cold with fever on 2 days not getting
better to bring to medical health service.
5) Prevent complication or disturbance of save and
comfortable feeling that canot been through out so atelektasis and
brhonchietaksis happen.
7. Nursing Diagnosis
a. Ineffective breathing pattern related to inflamation on lungs or lungs
parenkim.
b. Ineffective airways related to mecanical obstruction, inflamation, increasing
of secretion, pain
c. High risk of infection related to ineffective organism
d. Intoleran activity related to inflamation process, Intoleran aktivitas
berhubungan dengan proses inflamasi, imbalance beetwen suplay and
oxygen needed
e. Disturbance of gas exchange related to secret acumulation
f. Lack of nutrition from body needed related to anorexia
g. Hypertermia related to increasing of heat production
h. Lack of knowledge related to less of information
8. Focus Intervention
a. Ineffective breathing pattern related to airways constriction.
Purpose : reaten normaly breathing function.
Intervention :
1) Give semi fowler position or head elevation more than 30 degrees.
2) Avoid tigh wearing
3) Give support pillow so airway still open.
4) Give oxygenation as child needed.
5) Give lotion to contuinity breathing airway
b. Clear ineffectife airway related to mecanical obstruction, inflamation,
increasing of secretion.
Inflammation : airways still clear and child can take a breath easly,
respiratory in normaly limits
Intervension :
1) Prepare child in right body equal so can be lungs expantion well and
repair gas exchange, and prevent secretion aspiration (facedown, slape)
2) Suck the secretion airways as needed
3) Give supine position with head on snuff, neck more extend and nois
through to upper
4) Help child to through out the secretion
5) Give backslap
6) Give expectorant as rule
c. High risk infection related to ineffective organism
Purpose : Infection shymptomp decrease and infection not to spread
Intervention :
1) Keep aseptic enviroinment with use steril suction catheter and well
hand washing thecnique

2) Isolating child as indication to prevent nasocomial infection spread.
3) Give antibiotic as indication to prevent or solved the infection
4) Give nutrition diit as child favorite and desire to consumption
nutrition to support natural body
5) Give chest therapy.
d. Intolerant activity related to inflamation process, imbalance beetwen supply
and oxygen needed
Purpose : child can rest well and optimally
Intervention :
1) Assest child physical.
2) give distraction activity as old age, condition, and interest.
3) Rest period and sleep as old age and condition
4) Help chilg in daily activity wich more tolerate
5) Balancing rest and sleep if patient ambulation
(Wong, 2002 : 353)
e. Change nutrition lack of body needed related to anorexia (Carpenito, 2001 :
450).
Purpose : patient got optimally nutrition
Intervention :
1) Give food and drink that child wanted.
2) Give little but often food
3) Antisipation sadness reaction to child losing perfectlly. Because this is
ussually happen in adapted process

4) Avoid oversupport to consumption for eat and drink
5) Avoid food with strengh smell because can make nausea.
6) Give fun enviroinment to eat
(Wong, 2002 : 368)
f. Disturbance of gas exchange related to accumulation of secret.
Purpose : Increasing adequate gas exchange.
Intervention :
1) Asset respiratory status every 2 hours, regular respiratory sound or
irregular and vital sign .
2) Elevating head more high than sleeping bed.
3) Change position every 2 hours as well as condition.
4) If child can tolerate give free to choice comfortable position.
(Suriadi, 2001 : 276)
g. Hypertermia related to increasing of heat production.
Purpose : Keep patient temperature in normally limite.
Intervenstion :
1) Give cold compress during 20 – 30 minutes.
2) Give cold towel, wet, or washlap, chnge as needed, continues
approximately 30 minutes.
3) Don’t ever use isopropil alcohol swap when take a bath to compress
because can occur neurotocsic effect.
4) Observe body temperature to prevent over body colder.
(Wong, 2002 : 377)

h. Lack of knowledge related to lack of information.
Purpose : Patient and family can make life change and participate in
medication programe.
Intervention :
1) Discuss inability aspec from the disease, healing time, and whises to
geting better.
2) Give information by notes and verbal.
3) Choise method, vocabulary , and content as education level patient
family to optimally learning process .
4) Choese condusive enviroinment to studyed.
(Wong, 2002 : 534)
B. Hospitalization
1. Definition
According to Supartini (2004: 133), hospitalizes is process that cause
reason which planned or emergency, require process to hospitalize, going to
therapy and caring until get back home.
Many feeling that often occur there is: anxiety, madness, sad, afraid,
and guilty. That feels can occur because of face a new something and never
experience yet. If child stress during hospitalization, parent will stress too,
and parental stress can increasing child stress.
2. Stressor on child when hospitalize
a. Anxiety because of separation
More stress happen in todller until preschool child, especially
child in 6 years old until 30 months old are anxiety because of separation.
Todller canot comunicate with language well yet and have limited
knowledge about reality. Relationship child with mother is close, so
separate with mother can occur loss feeling on child.
Child response attitude with effec separation divided into three
phase, there:
1) Phase of protest (phase of protest)
This phase sign with strong crying, yelling, and calling mother or use
aggressive behavior such as kick, bit, hit, pitch, and rejecting parental
attention.
2) Phase of despair (phase of despair)
In this phase child looks strained, reducing them cry, passive, not
interest to playing, anorexia, withdrawal, silence, sad, aphasia, and
aggression ( for example bedwetting, sucking tumb ). In this phase
condition of child is worrying because of child reject to eat, drink, or
moved .
3) Phase of denial (phase of denial)
In subtly child accepting the separation, start interesting with
something around, and built a little relation with other people. Child
starts happy. This phase usually happen after a long time with parent.
b. Lost Control

Child under 5 years old try more to defens them autonomy. This is
looks clearly in their attitude on motoric ability, play, making
interpersonal, activity daily living, and comonication. Cause of sick and
hospitalize child can lost they freedom and egocentries description on
their autonomy development. This is can occur regression.
c. Wound of body and pain (pain)
Consept about body image, especially definition about body
protection ( body bondaries ), very little ca developing on child under 5
years old. Accoerding to monitoring result, if doing ear, mouth, or anal
temperature examination can make child worriy. Child response related to
hurt examination, looklike reactiont when theiy get hurts .
3. Family reaction to child who was sick and hospitalized
According to Nursalam (2005 :18 – 21), family reaction to child who
was sick and hospitalized are :
a. Parental reaction
Parent reaction to them child influence of several factor, among:
1) Serious stage of child disease
2) Past experience to disease and hospitalization
3) Medication procedure
4) Available of support system
5) Intensity of individual ego
6) Ability on coping possession

7) Family support
8) Culture and trust
9) Communications on family
b. Reaction of sibling
Lonely, fear, worried, angry, jealousy, hate, and guilty
c. Decreasing of family member role
Effect from separation to family role is loss of parental role,
brother, son and grandson. Attention of parent just special to son who was
being sick, so their brother felt if that’s thing is not fair .
C. Stimulation and Role Play
1. Definition
Stimulation is something that activated on organ or part of bodies
(Hincliff, 2000: 417).
Activity of play is a happy activity for children although that is cannot
result of specific commodity, for example benefit of money. Childs free
expressing fear, worry, happy, or another feeling. So with giving freedom to
playing, parent can understand child feeling.
Playing is kind of infantile from adult ability to face model of
particular situation and try to capable through experiment and program .
2. Function of children play
a. Development of motoric sensor

Activity of motoric sensor is parth that most developing on babies.
Developing of motoric sensor supported by visual stimulation, auditory,
palpation, and kinetic. Stimulating of sensoric that was given by child
enviroinmen will be response with attention to motorics activity.
b. Developing of cognitive
Child learn with recognize the colour, form/meassure, texture
from many kinds of object, nimber, and object. Child start to string up
word, and thingking real and related to room like uo, down, under and
open.
c. Socialization
From early child, baby have showed interesting and happiness to
another, especially to the mother. With playing, recognize moral grade
and ethic, learn about what was wrong and right child will developing
and enlarge socialization, learn to solve the problem that has been occur.
d. Creativities
Children can make experimen and try to another idiea. Once child
feel satisfy to try samething new and different, they will moving their
creativities to another situation.
e. Self-awareness
With playing, children can awarenes that they are different with
other people and understan them self.

f. Grade of moral
Child learing a right and wrong attitude from enviroinmen, house,
or school. Interaction with group that have given meaning on their moral
practice.
g. Grade of therapeutic
Play can decreasing pressure or stress by enviroinmen. With
playing children can express emotion and unsatisfy of social situation and
their fear feeling that canot express in real.
3. Principe of playing activity
Several thing that need attention so playing can be effective
stimulation, following:
a. Need more energy
b. Need enough time
c. Toys must be adjust with old age and phase of child developmen
d. Place to play
e. Knowledge how to play
f. Playmate
4. Educative game equipment
Educative game equipment is equipment that can optimize child
development as age and developing stage and useful to physical development,
language, cognitive, and child social.
Parent can give educative equipment to children, requirement are:
a. Safety
Toys for children under 2 years is better not to small, not toxic coloration,
because in this age often entering something to the mouth.
b. Size and weight
The principe of game not dangerous and conform with children age.
c. Design
Equipment game is better having simple design in size, structure, and
colors, and clear of purpose.
d. Clear Function
e. Varies of game equipment
Equipment is better can be play variety (can be tide loading) but not too
difficult so children not frustrated.
f. Universal
Equipment game is better easily accepted and famous by all of culture and
nation.
g. Not easily to broken, easily obtained, and affordable to large community.
5. Type of Game
According to the content of playing can be different of game related to
another people (social effective play), game that related to fun (sense pleasure
play), game that just saw (unoccupied behavior) and skill play.
Game type according to social characteristic there are attention friends
playing (onlooker play), game that was playing by self (solitary play), game

with friend without interaction (parallel play), game that playing without
group purpose (associative play), and game that playing with together
organized (cooperative play).
a. Babyhood (0 – 1 years)
Equipment sample that suggest is safe equipment to enter the mouth,
human/ animal soft doll, voice toy, handbell, ball, and other.
Characteristic of game on baby according to the content is possible
to interact child with social environment that can give fun to children.
b. Toddler (2 – 3 years)
Game equipment that suggest on this age are candle that can be
design, painting equipment, simple puzzle, chaplet, home equipment. In
this time children egocentrics very dominant and think that all toy is own
self.
According to game content, game in this time include in skill play
and parallel play.
c. Preschoolhood (3 - 6 years)
Following with growing and developmen, preschoolhood have hard
and soft motoric that more mature better than todlerhood. Children are
nore creative and imaginative. Kind of apprpiate gameare asosiative play,
dramatic play, and skill play.
Children playing together with their playmate, and comunicate as
them language ability. Child also have playing particular persons such as
father, mother, or them teacher. Game that use motoric ability more

choice on prescholhood. Kind of the right game are: bycicle, toy car, sport
equipment, swiming, and big box toy.
d. Schoolhood (6 - 12 years)
In schoolhood social ability is decrease, their more can cooperate
with them playmate. So game on schoolhood not onli advantage to their
physical skill and intellectual, but also can developing their sense to
involve into the group and cooperate with another .
Characteristic of schoolhood game different according to the
gender. Boy is right to playing kind of mecanic, that can stimulate their
creatifity on creation as a boy for exampel car toy. Girl is right to playing
game that can stimulate a feeling, thing, and attitude into role as a girl, for
exampel: cook toy and doll.
e. Adult (13 - 18 years)
Game charaterictic to adult are doing constructive activity, for exampel
with sport, hearing or playing a music. And doing positive organitation
activity of teenagers, such as bascetgroup, soccer, young group, and
another. Principe, play activity on adult not only look for fun and
increasing of emotion development. But also more to distribute interest,
talent, and aspiration also help teenagers to find self identity. For that the
right equipment can be divide to sport equipment, musical equipment, and
painting.
6. Playing in hospital

The purpose of playing in hospital principally is to continue developing
phase optimally, developing of children creativity, and can adapted more
effective with stress. Often happen when child on hospitalize, growth
development aspect has been ignored. Officer just focuses to how they will
recover.
After go home parent complain if they child be regression, although
before sick child can more independent and normally growth likes another.
In order to children can more effectively playing in hospital, intense with
this Principe is:
a. Children with not much use of energy, shorter play time, to avoid fatigue
and tools more simple game, for example: built a box, making Kraft (hand
basket), and watching TV.
b. Safe and been avoid from nasocomial infection.
c. Appropriate with same group age.
d. Not contra indication with therapy.
e. Need anticipation from parent and family.
Implementation of play activities in the hospital, need involvement from
medical officer, include nurse that on duty in pediatric. For that need effort
are:
a. Prepare of equipment game
b. Prepare of equipment game
c. In implementation, game activity in Hospital is health officer
responsibility help by parent.

d. In the first year children just inspecting around object. Beetwen 2 until 3
years old age, generally children with role play s mother, baby, docter,
child with customer. In school hood children more often join with in the
same age group and have a favorite friend.
(Nursalam 2005: 74 – 84)