Embed Size (px)
Citation preview

687
Chapter 83 Pulmonary Thromboendarterectomy: Patient Selection and Clinical Outcomes from a Single Centre Experience DEVIPRASAD SHETTY • VARUN SHETTY • ABHIJIT JOSHI
is choice of treatment for CTEPH, about 10%–50% patients are not eligible to undergo the surgery 14 and they need to remain on medical management. An international registry reported 36.3% (247 out of 679) of newly diagnosed CTEPH cases were not operable 15 .
However, following surgery there is a demon-strable improvement in PH and functional class 16 . Centre experience plays an important role in the outcome following surgery 17 . Thus, the selection of CTEPH patients is as crucial as the surgery itself.
OUR EXPERIENCE WITH PTE
We began our endarterectomy programme in 2004. We have performed more than 400 cases of PTE across 14 years. Our annual caseload is over 30 cases. To the best of our knowledge, this is the fi rst and largest series to report on the outcomes of PTE from India. The mean age at the time of surgery is 39.67 � 11.74 years (mean � SD), with males being more common (71%). About 85% of the patients survived after the surgery. The overall in-hospital mortality rate was 14.4%.
PREOPERATIVE AND POSTOPERATIVE CHARACTERISTICS
Prior to PTE, 74.4% of patients had a history of deep vein thrombosis (DVT) and 60.4% of patients were diagnosed with prothrombotic syndromes. One-third of the patients had a history of congestive cardiac failure (CCF) before the surgery. The mean pulmonary artery systolic pressure (PASP) by echo-cardiography and right heart catheterization were 83.52 � 25.29 and 94.85 � 20.53 mm Hg, respec-tively. The mean postoperative PASP and pulmonary vascular resistance were 38.5 � 12.04 mm Hg and
INTRODUCTION
Chronic thromboembolic pulmonary hyperten-sion (CTEPH) is a subset of pulmonary hyperten-sion. CTEPH develops when the pulmonary artery (PA) branches are obstructed from the accumula-tion of thromboembolic material which raises mean pulmonary arterial pressure (mPAP) 1 .
CTEPH, defi ned as precapillary pulmonary hy-pertension (PH) by invasive right heart catheteriza-tion (mPAP � 25 mm Hg, mean pulmonary arterial wedge pressure � 15 mm Hg) in the presence of chronic/organized fl ow-limiting thrombi/emboli in the elastic pulmonary arteries (main, lobar, segmen-tal, subsegmental) after at least 3 months of effec-tive anticoagulation 2 . One study reported that mPAP more than 30 mm Hg is associated with a poor prognosis 3 . Another study reported that 3-year mortality rate is approximately 90% in patients with mPAP � 50 mm Hg 4 .
The actual incidence of CTEPH is unknown, but the reported literature shows the occurrence is be-tween 0.57% and 3.8% of survivors following acute pulmonary embolism (PE) and over 10% in patients with recurrent PE 5–8 . The prevalence of PE in Indian patients presenting with symptomatic lower limb DVT is very high (48%; both lower limbs 24.6% and proximal 70%) 9 . The rate of progression from PE to CTEPH is higher in Indian subcontinent, from our centre, Dutt et al., reported about 20% of patients will progress to CTEPH after acute PE 10 .
Anticoagulation therapy can only prevent recur-rent venous thromboembolism and PA thrombo-sis 11 . Pulmonary thromboendarterectomy (PTE) is the potential and curative treatment option for PH with CTEPH in eligible patients 4 , 12 . Untreated CTEPH can lead to progressive right heart failure with an increased risk of mortality 13 . Although PTE

688 SECTION IX — Right Heart and Pulmonary Circulation
135.77 � 52.50 dyn·s·cm−5, respectively. The median length of the hospital stay was 12 days (IQR, 9–16).
FOLLOW-UP AND CLINICAL OUTCOME
After discharge from the hospital, patients are fol-lowed up in the outpatient clinic. We were able to follow up about 55% of the total patients under-went PTE; follow-up is limited because most of the patients who undergo PTE at our centre are from other states. The median follow-up time was 16 months. During the follow-up, the patients’ PASP, TAPSE and 6-min walk test were recorded. The mean PASP and TAPSE were 37.11 � 17.59 mm Hg (range, 12–140) and 16.83 � 5.86 cm (range, 10–86), respectively. The mean 6-min walk distance was 452 m (IQR, 360, 549).
EVALUATION OF THE PATIENT WITH CTEPH FOR PTE
It is important to determine whether PTE is feasible, and after careful assessment of comorbidities, risks and anticipated benefi ts, whether surgical treat-ment should be pursued. Despite of advanced diag-nostics techniques and an expanding surgical expe-rience, the assessment and case selection remain subjective. A report of 42 patients with symptom-atic chronic thromboembolic disease and a baseline mPAP � 25 mm Hg concluded that there was sig-nifi cant improvement in functional status and quality of life after PTE 18 .
PATIENT SELECTION CRITERIA FOR PTE
Selection of cases plays an important role in endarter-ectomy. All patients may not be fi t for surgery, and need to be managed medically. Generally patients are selected for PTE, if they meet the following crite-ria 19 : (i) presence of surgically resectable chronic
thromboembolic disease, (ii) symptomatic chronic thromboembolic disease, with or without PH and right-sided heart dysfunction at rest, (iii) absence of concurrent illnesses representing an immediate threat to life, (iv) patient’s desire for surgical treatment based on dissatisfaction with poor cardiorespiratory func-tion or prognosis and (v) patient’s willingness to ac-cept the mortality risk of the PTE surgical procedure.
PATIENT WORKUP
At our centre, CTEPH patients are diagnosed with ventilation–perfusion scan, those scans suggestive of ventilation–perfusion defects are subjected to computerized tomography pulmonary angiogra-phy (CTPA). CTPA is used to study the extent of the disease, parenchymal changes and the pres-ence of systemic to pulmonary collaterals. Addi-tionally right heart catheterization and pulmonary angiography are done.
OPERATIVE TECHNIQUE
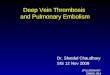
We operate under cardiopulmonary bypass (CPB) and the patient is cooled to 18°C. The endarterec-tomy plane is identifi ed through the opening of PA while the patient is on CPB. Systemic to pulmonary collaterals are common in CTEPH; hence, the blood circulation is stopped (18°C) to prevent fl ooding of the fi eld. Total circulatory arrest is restricted to 20 min intervals to prevent neurological injury. End-arterectomy is always bilateral, and once complete, the PA is closed and the patient is re-warmed. After this, the patient is weaned off CPB, if the endarterec-tomy is complete the PA pressure usually normalizes and the right ventricular dysfunction reverses imme-diately. A complete endarterectomy specimen always tapers off and never cuts off abruptly, if so, it means there is some residual disease. Fig. 83-1 shows the specimen of thrombus after PTE.
A B C
Figure 83-1. Specimen of thrombus showing (A) occlusion at the subsegmental level, (B) occlusion at the segmental level and (C) occlusion at the lobar level.

689Chapter 83 — PTE: Patient Selection and Clinical Outcomes from a Single Centre Experience
POSTOPERATIVE CARE
Right ventricular dysfunction usually resolves after PTE and there is an increased urine output. Furose-mide infusion is used postsurgery to keep the patient overall fl uid negative. The patients are extu-bated the next day if they are haemodynamically stable and there is no reperfusion oedema and right ventricular dysfunction. Residual pulmonary artery hypertension (PAH) is managed with intravenous milrinone, inhaled nitric oxide and pulmonary vasodilators.
CHALLENGES IN STARTING PTE PROGRAMME
MULTIDISCIPLINARY TEAM
CTEPH is a multidisciplinary disorder which re-quires multidisciplinary intervention. All PTE pro-grammes need a dedicated multidisciplinary team, which should include a cardiothoracic surgeon, cardiac anaesthetist, intensivist, cardiologist and pulmonologist.
ECMO REQUIREMENT
Every PTE programme must be equipped with ex-tracorporeal membrane oxygenation (ECMO). Veno-venous ECMO is useful in patients with reper-fusion oedema and not responding to conventional methods. Persistent right or biventricular dysfunc-tion leading to low cardiac output is supported with central veno-arterial ECMO. Residual PAH requiring pulmonary vasodilators are very rare. In our experi-ence, we observed that 50 (12.2%) patients required ECMO during PTE; survival with ECMO was 24%. The major indication for ECMO was reperfusion oedema, seen in 56% of cases.
HIGH MORTALITY RATE AND SURGEON DEPENDENT
PTE is a technically demanding operation requiring proper case selection, a dedicated surgical team to operate and manage the complications. The out-come rate is highly dependent on the surgeon. PTE has a long learning curve; the San Diego group pio-neered surgery for CTEPH and has done over 1500 cases. In the beginning, their mortality rate was 17% for the fi rst 200 cases, which improved to 4.4% for the last 500 cases 20 .
In general, mortality rate is high in PTE. In our centre, the overall in-hospital mortality rate was
14.4% across 14 years. Mortality between 2004 and 2010 was 18.5% which has reduced to 11.9% be-tween 2011 and 2016. The reduction in mortality rate was 35.6%. Since then our team has improved on the case selection, surgical technique, identifi ca-tion and prevention of complications. A centre can be considered to have suffi cient expertise if it has an annual caseload of 20 with a mortality rate under 10% 17 .
CONCLUSION
PTE is a complex operation requiring expertise at every stage. A dedicated multidisciplinary team to CTEPH is crucial for good outcomes. Our data have shown a signifi cant reduction in PASP, in-hospital mortality and improved quality of life after PTE. This is attributed to an improved experience in case selection and handling of surgical complications.
REFERENCES
1. Galiè, N., Humbert, M., Vachiery, J-L., Gibbs, S., Lang, I., Torbicki, A., et al. ( 2016 ). 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hyperten-sion The Joint Task Force for the Diagnosis and Treat-ment of Pulmonary Hypertension of the European So-ciety of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), Interna-tional Society for Heart and Lung Transplantation (ISHLT). European Heart Journal , 37 , 67 – 119 .
2. Lang, I. M., Pesavento, R., Bonderman, D., & Yuan, JX-J. ( 2013 ). Risk factors and basic mechanisms of chronic thromboembolic pulmonary hypertension: A current understanding. European Respiratory Journal , 41 , 462 – 468 .
3. Lewczuk, J., Piszko, P., Jagas, J., Porada, A., Wójciak, S., Sobkowicz, B., et al. ( 2001 ). Prognostic factors in medi-cally treated patients with chronic pulmonary embo-lism. Chest , 119 , 818 – 823 .
4. Dalen, J. E., & Alpert, J. S. ( 1975 ). Natural history of pulmonary embolism. Progress in Cardiovascular Dis-eases , 17 , 259 – 270 .
5. Miniati, M., Monti, S., Bottai, M., Scoscia, E., Bauleo, C., Tonelli, L., et al. ( 2006 ). Survival and restoration of pul-monary perfusion in a long-term follow-up of patients after acute pulmonary embolism. Medicine (Baltimore) , 85 , 253 – 262 .
6. Klok, F. A., van Kralingen, K. W., van Dijk, A. P. J., Heyning, F. H., Vliegen, H. W., & Huisman, M. V. ( 2010 ). Prospec-tive cardiopulmonary screening program to detect chronic thromboembolic pulmonary hypertension in patients after acute pulmonary embolism. Haemato-logica , 95 , 970 – 975 .
7. Konstantinides, S. V., Vicaut, E., Danays, T., Becattini, C., Bertoletti, L., Beyer-Westendorf, J., et al. ( 2017 ). Impact of thrombolytic therapy on the long-term outcome of

690 SECTION IX — Right Heart and Pulmonary Circulation
8. Pengo V, Lensing AWA, Prins MH, Marchiori A, Davidson BL, Tiozzo F, et al. ( 2004 ). Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. New England Journal of Medicine , 350 , 2257 – 2264 .
9. Parakh, R., Kapadia, S. R., Sen, I., Agarwal, S., Grover, T., & Yadav, A. ( 2006 ). Pulmonary embolism: a fre-quent occurrence in Indian patients with symptomatic lower limb venous thrombosis. Asian Journal of Surgery , 29 , 86 – 91 .
10. Dutt, T. S., Murali Mohan, B., Tousheed, S. Z., Raman-jenaya, R., & Shetty, D. P. ( 2013 ). Incidence of chronic thrombo-embolic pulmonary hypertension following acute pulmonary thrombo-embolism: An Indian per-spective. Indian Journal of Chest Diseases & Allied Sci-ences , 55 , 205 – 207 .
11. Piazza, G., & Goldhaber, S. Z. ( 2011 ). Chronic throm-boembolic pulmonary hypertension. New England Journal of Medicine , 364 , 351 – 360 .
12. Hoeper, M. M., Madani, M. M., Nakanishi, N., Meyer, B., Cebotari, S., & Rubin, L. J. ( 2014 ). Chronic thromboem-bolic pulmonary hypertension. Lancet Respiratory Medi-cine , 2 , 573 – 582 .
13. Hoeper, M. M., Mayer, E., Simonneau, G., & Rubin, L. J. ( 2006 ). Chronic thromboembolic pulmonary hyper-tension. Circulation , 113 , 2011 – 2020 .
14. Peacock, A., Simonneau, G., & Rubin, L. ( 2006 ). Con-troversies, uncertainties and future research on the treatment of chronic thromboembolic pulmonary
hypertension. Proceedings of the American Thoracic Society , 3 , 608 – 614 .
15. Pepke-Zaba, J., Delcroix, M., Lang, I., Mayer, E., Jansa, P., Ambroz, D., et al. ( 2011 ). Chronic thromboembolic pul-monary hypertension (CTEPH): Results from an interna-tional prospective registry. Circulation , 124 , 1973 – 1981 .
16. Mayer, E., Jenkins, D., Lindner, J., D’Armini, A., Kloek, J., Meyns, B., et al. ( 2011 ). Surgical management and outcome of patients with chronic thromboembolic pul-monary hypertension: Results from an international prospective registry. Journal of Thoracic and Cardiovascu-lar Surgery , 141 , 702 – 710 .
17. Galiè N, Hoeper, M. M., Humbert, M., Torbicki, A., Vachiery, J-L., Barbera, J. A., et al. ( 2009 ). Guidelines for the diagnosis and treatment of pulmonary hyper-tension. European Respiratory Journal , 34 , 1219 – 1263 .
18. D’Armini, A. M., Morsolini, M., Mattiucci, G., Grazioli, V., Pin, M., Valentini, A., et al . ( 2014 ). Pulmonary endarter-ectomy for distal chronic thromboembolic pulmonary hypertension . Journal of Thoracic and Cardiovascular Sur-gery , 148 , 1005 – 1011 , 1012.e1-2 , discussion 1011 – 1012 .
19. Banks, D. A., Auger, W. R., & Madani, M. M. ( 2017 ). Pulmonary thromboendarterectomy for chronic thromboembolic pulmonary hypertension . In: Ka-plan’s cardiac anesthesia [Internet] ( 7th ed ., pp. 994 – 1021 ). Philadelphia, PA : Elsevier .
20. Jamieson, S. W., Kapelanski, D. P., Sakakibara, N., Manecke, G. R., Thistlethwaite, P. A., Kerr, K. M., et al. ( 2003 ). Pulmonary endarterectomy: Experience and lessons learned in 1,500 cases. Annals of Thoracic Surgery , 76 ( 5 ), 1457 – 1462 , discussion 1462 – 1464 .
intermediate-risk pulmonary embolism. Journal of American College of Cardiology , 69 , 1536 – 1544 .