Embed Size (px)
Citation preview

CHAPTER 7
DEPRESSIVE AND BIPOLARDISORDERS
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

WE ALL HAVE OUR DAYS WHEN WE ARE SAD, WHEN IS IT DEPRESSION?
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

DEPRESSIVE DISORDERS
• A disorder that involves periods of symptoms in which an individual experiences an unusually intense sad mood.
• Dysphoria
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

MAJOR DEPRESSIVE DISORDER
• Acute, but time-limited, periods of depressive symptoms that are called major depressive episodes
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

SIGECAPS
S leep changes: increase during day or decreased sleep at night
I nterest (loss): of interest in activities that used to interest them
G uilt (worthless): depressed elderly tend to devalue themselves
E nergy (lack): common presenting symptom (fatigue)
C ognition/C oncentration: reduced cognition &/or difficulty concentrating
A ppetite (wt. loss); usually declined, occasionally increased
P sychomotor: agitation (anxiety) or retardations (lethargic)
S uicide/death preocp.
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

TABLE 7.1 - CRITERIA FOR A MAJOR DEPRESSIVE EPISODE
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

MAJOR DEPRESSIVE DISORDER
• Two major categories of major depressive disorder:• Single episode• Recurrent
• The lifetime prevalence of major depressive disorder in the United States is 16.6 percent of the adult population. • Each year, 6.7 percent of the adult population receives a
diagnosis of major depressive disorder, with clinicians classifying 30.4 percent of these cases (2.0 percent of the adult population) as severe.
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

FIGURE 7.1 - PREVALENCE OF MAJOR DEPRESSIVE DISORDER IN THE UNITED
STATES
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

POSTPARTUM DEPRESSION
• https://www.youtube.com/watch?v=yH3WMQO-ooU
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

PERSISTENT DEPRESSIVE DISORDER (DYSTHYMIA)
• A depressive disorder involving chronic depression of less intensity than major depressive disorder.
• Symptoms present for at least 2 years.
• The 12-month prevalence is 1.5 percent of the U.S. population, • Almost half of these (.8 percent of the adult population)
classified as severe
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.
"Jack is an 18 year old college student who was seeking psychotherapy because, after reading about depression in his "Introduction to Psychology" textbook, decided that the description fit him. Despite doing quite well in his classes he complained of feeling a constant tiredness. However, along with feeling tiredness, he also felt blue, down and hopeless. He described himself as being a loner, with a few friends but no girls, no dates and no sexual experiences. He also had no goals and no aspirations for himself. His parents remained married but unhappily so and that was one of those open secrets. His father was a teacher but always felt unfilled and openly stated how much he hated his job. His mother, a housewife, also seemed to never have any enthusiasm for life. It soon became clear that Jack never really felt loved by his parents, whose lives seemed colorless and bland. The boredom of home was broken by episodes of loud arguing between his mother and father. The issues usually centered around money and how much his mother spent for food and clothing. The fights would suddenly erupt for no apparent reason and would fill him with enormous dread. Jack always experienced and ill defined sense of guilt, as though the lives of his parents would have been better had he never been born. A good student since elementary school, neither parent seemed to take any joy in his achievements and never expressed any goals they wished or hoped he would achieve. Jack's therapist was the first adult male he ever remembered taking an interest in him. Jack became a long term psychotherapy patient who had a wonderful outcome in his therapy five years later."Jack's story is not unusual. His symptoms fit the profile of someone coping with Dysthymia.

DISRUPTIVE MOOD DYSREGULATION DISORDER
• A depressive disorder in children who exhibit chronic and severe irritability and have frequent temper outbursts.
• Outbursts must be developmentally inappropriate and occur three or more times per week.
• Between outbursts, children with this disorder are extremely irritable or angry.• Research suggests that they are at risk of developing
depressive and/or anxiety disorders when they reach adulthood.• https://www.youtube.com/watch?v=Qg-BBKB1nJc
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

PREMENSTRUAL DYSPHORIC DISORDER (PMDD)
• Women who experience depressed mood or changes in mood, irritability, dysphoria, and anxiety during the premenstrual phase that subside after the menstrual period begins for most of the cycles of the preceding year.
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

DISORDERS INVOLVING ALTERATIONS IN MOOD
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIPOLAR DISORDER
• Manic episodes and very disruptive experiences of heightened mood, possibly alternating with major depressive episodes
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIPOLAR DISORDER
• Manic episode: A period of euphoric mood with symptoms involving:• Abnormally heightened levels of thinking, behavior, and
emotionality• https://www.youtube.com/watch?v=Y4GYwymtbUU
• Children and teens having a manic episode may:• Feel very happy or act silly in a way that's unusual• Have a very short temper• Talk really fast about a lot of different things• Have trouble sleeping but not feel tired• Have trouble staying focused• Talk and think about sex more often• Do risky things.
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

CRITERIA FOR A MANIC EPISODE
• Inflated self-esteem or grandiosity• Decreased need for sleep• Pressure to keep talking• Flight of ideas• Distractibility• Increase in goal-directed activity• Excessive involvement in activities that have a
high potential for painful consequences
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIPOLAR DISORDER
• Types• Bipolar I disorder - One or more manic episodes, and
possibility of major depressive episodes
• Bipolar II disorder - One or more major depressive episodes and at least one hypomanic episode
• https://www.youtube.com/watch?v=8Ki9dgG3P5M
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

FIGURE 7.2 - RANGE OF MOODS PRESENT IN PEOPLE WITH BIPOLAR DISORDER
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIPOLAR DISORDER, RAPID CYCLING
• Bipolar disorder with rapid cycling can be diagnosed if they have four or more episodes within the previous year that meet the criteria for manic, hypomanic, or major depressive disorder.
• In some individuals, the cycling may occur within 1 week or even 1 day.
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIPOLAR DISORDER
• Factors that predict rapid cycling:
• Earlier onset• Higher depression scores• Higher mania scores • Lower global assessment of functioning• Hypothyroidism• Disturbances in sleep-wake cycles• Antidepressant medications
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

CYCLOTHYMIC DISORDER
• Not as intense as bipolar• Met the criteria for a hypomanic episode• Chronic condition
• Lasts at least 2 years
• Numerous periods of depressive symptoms• Never meet the criteria for a major depressive
episode
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

THEORIES AND TREATMENT OF MOOD DISORDERS
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIOLOGICAL PERSPECTIVES
• First-degree relatives of those with major depression are two to four times the rates of nonrelatives
• Twin studies• Altered serotonin functioning• Brain-derived neurotrophic factor (BDNF)• Heritability estimated at 60%• PCLO gene
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIOLOGICAL PERSPECTIVES
• Antidepressant medication • Treatment for bipolar disorder is lithium
carbonate• Pharmacogenetics• Circadian rhythms• Light therapy
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

PSYCHOLOGICAL PERSPECTIVES
• Psychodynamic• Insecure attachment style• Defensive responses
• Behavioral & cognitive• Behavioral activation• Role of dysfunctional thoughts as causes• Behavioral contracting combined with self-reinforcement• Pharmacological and psychological interventions• Psychoeducation
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

COGNITIVE PERSPECTIVES
• Cognitive triad• A negative view of:
• Self• World • Future
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

EXAMPLES OF COGNITIVE DISTORTIONS
• Overgeneralizing• Selective abstraction• Excessive responsibility• Assuming temporal causality• Making excessive self-references• Catastrophizing• Dichotomous thinking
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

PSYCHOLOGICAL PERSPECTIVES
• Interpersonal approaches• Assessing the magnitude and nature of the individual’s
depression• Formulating a treatment plan• Implementation of treatment plan
• Treatment• Interpersonal and social rhythm therapy
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

SOCIOCULTURAL PERSPECTIVE
• Individuals develop depressive disorders in response to stressful life circumstances• Exposure to an acute stress• Exposure to chronic strains
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.
SUICIDE
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

SUICIDE
• Fatal self-inflicted destructive act with explicit or inferred intent to die
• Suicidal behavior runs from a continuum of thinking about:• Ending one’s life • To developing a plan• To nonfatal suicidal behavior • To the actual ending of one’s life
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

SUICIDE
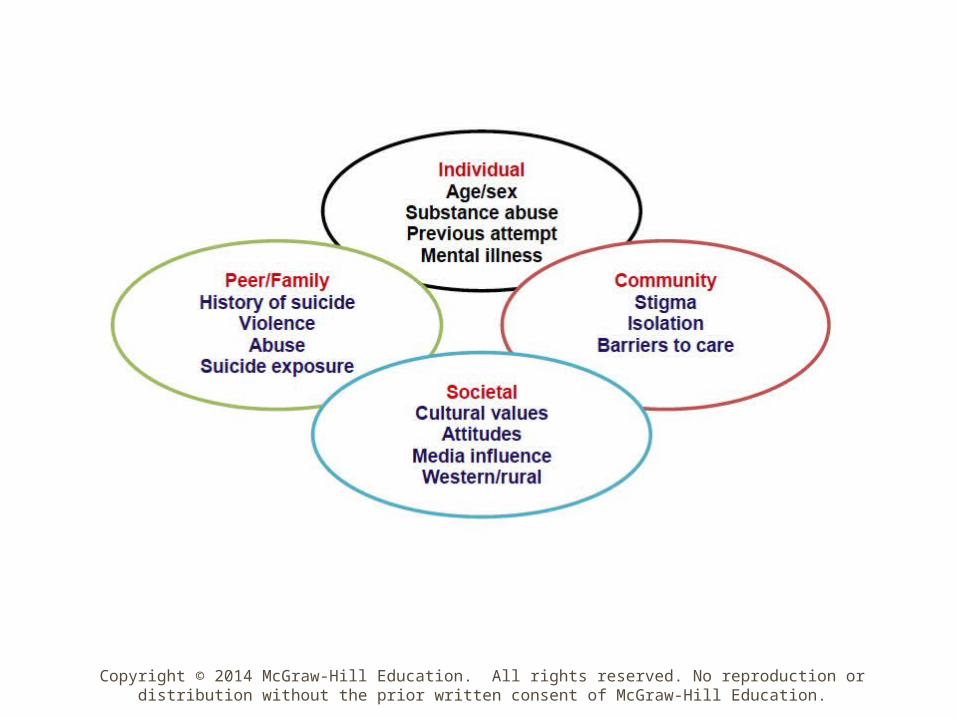
• Biopsychosocial perspective• Biological theories• Psychological theories
• Sociocultural perspective• Perspective of positive psychology
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

SUICIDE
• Buffering hypothesis of suicidality• Resilience as separate dimension from risk• Risk and resilience as bipolar dimensions• Resilience as a psychological construct
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

SUICIDE
• Factors that buffer suicide risk• Ability to solve problems• High levels of self-esteem• Confidence in one’s problem-solving ability• General feelings of social support and support from
family• Secure attachment• Suicide beliefs (not regarding suicide as a personal
option)
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

BIOPSYCHOSOCIAL PERSPECTIVE
• Disorders involve: • Disturbances in neurotransmitter functioning• Cognitive processes• Sociocultural factors
• Development of evidence-based approaches allows individuals to:• Obtain treatment that regulates their moods and lead
more fulfilling lives
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.

• For more information on material covered in this chapter, visit our Web site:
• http://www.mhhe.com/whitbourne7eupdate
Copyright © 2014 McGraw-Hill Education. All rights reserved. No reproduction or distribution without the prior written consent of McGraw-Hill Education.





























