Embed Size (px)
Citation preview

Chapter 50Disorders of
Motor Function


Spinal CordSomatosensory– Dorsal column-medial lemniscus tract• Touch/proprioception/vibration sensory pathway
– Anterolateral system• Pain/temperature sensory pathway
• Motor– Corticospinal tract• Motor pathway for upper motor neuronal signals
coming from cerebral cortex and brainstem motor nuclei


Brain StemMidbrain• associated with vision,
hearing, motor control, sleep/wake, arousal (alertness), and temperature regulation
Pons• nuclei that deal primarily
with sleep, respiration, swallowing, bladder control, hearing, equilibrium, taste, eye movement, facial expressions, facial sensation, and posture

Brain StemMedulla• Contains the cardiac,
respiratory, vomiting and vasomotor centers dealing with autonomic, involuntary functions– Breathing, heart rate
and blood pressure


• The cerebellum receives continuous information about the sequence of muscle contractions from the brain
• Receives sensory information from the peripheral parts of the body– Proprioception
• sequential changes in the status of each body part

The Cerebellum
• Coordination of motor movement– proprioception
• Cerebellum-associated movement disorders – Causes• Congenital defect, vascular accident, or growing tumor
– Types• Vestibulocerebellar ataxia– Not smooth movement
• Decomposition of movement• Cerebellar tremor– Rhythmic back-and-forth movement of a finger or toe– Cannot maintain a fix on the body part

Thalamus• It relays to the cerebral
cortex information received from other regions of the brain and spinal cord.
• Sends information down spinal cord to the body– a brain “switching
station”

Thalamus
• The cerebral cortex is interconnected with the Thalamus– Excitatory circuit• If unmodulated would cause
hyperactivity = stiffness and rigidity with a continuous tremor (tremor at rest)



Structural Components of the Basal Ganglia
• Caudate nucleus• Putamen• Globus pallidus in the forebrain– Substantia Nigra (midbrain)– Subthalamic nucleus

Basal Ganglia• A group of deep, interrelated subcortical nuclei
that play an essential role in control of movement• Receive indirect input from the cerebellum and
from all sensory systems, including vision, and direct input from the motor cortex– Function in the organization of inherited and
highly learned and rather automatic movement programs
– Also involved in cognitive and perception functions

Structural Components of the Basal Ganglia
• Caudate + Putamen = Striatum
• Putamen + Globus Pallidus = Lentiform nucleus

Basal Ganglia
• Basal Ganglia modulates the Thalamic excitability by inhibitory loop
• Basal Ganglia monitors sensory information coming into the brain– sends it to the right place to be stored as a
memory

Four Functional Pathways Involving Basal Ganglia
1. A dopamine pathway from the substantia nigra to the striatum
2. A γ-aminobutyric acid (GABA) pathway from the striatum to the globus pallidus and substantia nigra
3. Acetylcholine-secreting neurons, which are important in networks within the neostriatum
4. Multiple general pathways from the brain stem that secrete norepinephrine, serotonin, enkephalin, and several other neurotransmitters in the basal ganglia and the cerebral cortex

Characteristics of Disorders of the Basal Ganglia
• Involuntary movements• Alterations in muscle tone• Disturbances in body posture

Motor Cortex• Highest level of motor
function– Precise, skillful,
intentional movements• Speech, flexor muscles of
limbs, etc.
– Controlled by the primary, premotor and supplementary motor cortices in the frontal lobe• Receives information
from the Thalamus, cerebellum and basal ganglia

Motor Cortex
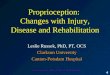
Primary motor cortex•Responsible for execution of a movement.•Adjacent to central sulcus
•Motor Humunculus
Premotor cortex (areas 6 and 8)•Generates intricate plan of movement.
•Throwing a ball or picking up a fork
Homunculus

Motor Cortex
Supplementary motor cortex• Involved in the performance
of complex, skillful movements– (areas 6 and 8)

Pyramidal motor system• Originates in the motor
cortex• Controls all of our
voluntary movements• Consists of upper motor
neurons in the Primary Motor Cortex and lower motor neurons in the anterior horn of the spinal cord– The Ventral Corticospinal
tract• Damage to LMN's causes
flaccid paralysis
Extrapyramidal motor system • Originates in the basal ganglia• Provides background for the
more crude, supportive movement patterns
• Includes the substantia nigra, caudate, putamen, globus pallidus, thalamus, and subthalamic nucleus.
• All of these nuclei are synaptically connected to one another, the brainstem, cerebellum and the pyramidal system.


Disorders of Motor Function
Upper motoneuron (UMN’s)• Originate in the motor region of the cerebral
cortex or brain stem– Carries motor information down spinal cord to
stimulate target muscle• Lesions can involve the motor cortex, the internal
capsule, or other brain structures through which the corticospinal or corticobulbar tracts descend, or the spinal cord

1. Paralysis or weakness of movements of the affected side but gross movements may be produced. – No muscle atrophy is seen initially
2. Babinski sign is present: 3. Loss of performance of fine-skilled voluntary
movements especially at the distal end of the limbs4. Superficial abdominal reflexes and cremasteric reflex
are absent.5. Spasticity or hypertonicity of the muscles.6. Clasp-knife reaction: initial higher resistance to
movement is followed by a lesser resistance7. Exaggerated deep tendon reflexes and clonus may be

Disorders of Motor FunctionLower motoneurons (LMN’s)• Connects the brainstem and spinal cord to muscle
cells– Brings nerve impulses from upper motor
neuron to the muscles• Lesions disrupt communication between the
muscle and all neural input from spinal cord reflexes, including the stretch reflex, which maintains muscle tone

Signs of Lower Motor Neuron Lesions (LMNL)
1. Flaccid paralysis of muscles supplied.2. Atrophy of muscles supplied.3. Loss of reflexes of muscles supplied.4. Muscles fasciculation (contraction of a group
of fibers) due to irritation of the motor neurons – seen with nakedeye

Disorders of Skeletal Muscle Groups• Muscular atrophy – If a normally innervated muscle is
not used for long periods, the muscle cells shrink in diameter, lose much of their contractile protein, and weaken.
• Muscular dystrophy– Genetic disorders that produce
progressive deterioration of skeletal muscles because of mixed muscle cell hypertrophy, atrophy, and necrosis

Muscular Dystrophy
• Involves the motor neuron– Probably do not involve the nervous system
• Slow progressive onset of muscle weakness
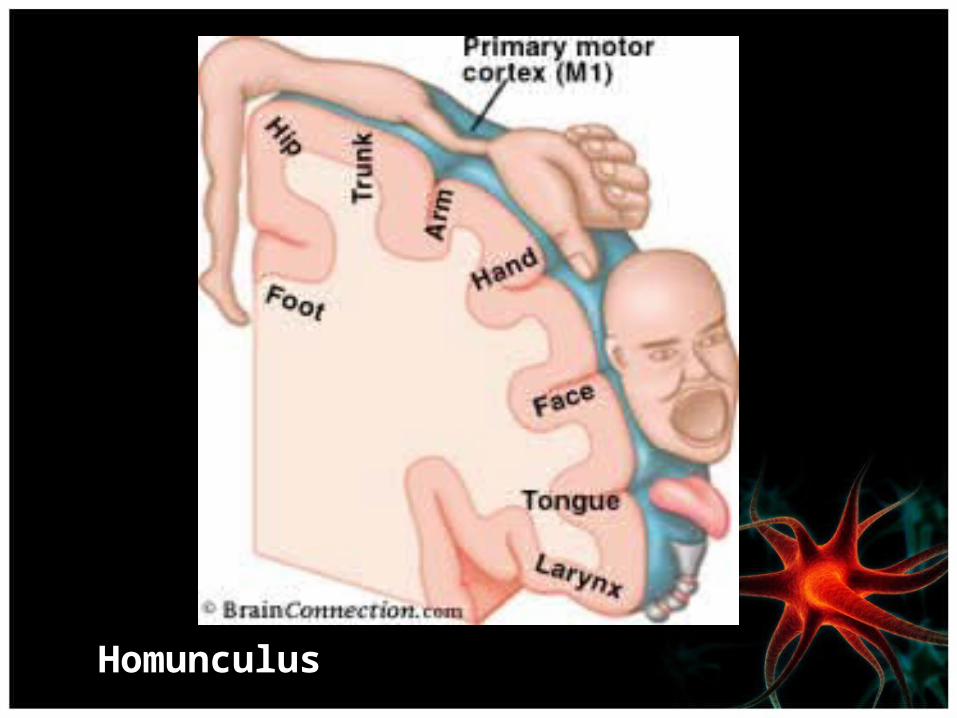
Duchenne Muscular Dystrophy• 1:3500 male births– Inherited recessive single-
gene defect• On short arm of X
chromosome
– Gene codes for dystrophin• Connects Z-lines to
connective tissue surrounding muscle
– Break down of sarcolemma = necrosis of muscle fibers

Duchenne Muscular Dystrophy
Symptoms usually appear before age 6 and may appear as early as infancy. They may include:Fatigue, mental retardtion, muscle weakness (begins in legs and pelvis), difficulty with motor skills (running, jumping hopping), frequent falls
May be confined to wheelchair by age of 12

Signs and Tests
• A complete nervous system (neurological), heart, lung, and muscle exam may show:
• Abnormal heart muscle• Congestive heart failure• Arrhythmia• Scoliosis• Respiratory disorders• Muscle wasting

Tests
• Electromyography (EMG)• Genetic tests• Muscle biopsy• Serum CPK

Treatments
• There is no known cure for Duchenne muscular dystrophy.
• Treatment aims to control symptoms to maximize quality of life. – Gene
therapy may become available in the future.
Becker Muscular Dystrophy
• Very similar to Duchenne muscular dystrophy– Becker muscular dystrophy gets worse much more
slowly• 3 - 6 out of every 100,000 males• X-linked– Manifests later in childhood of adolescence

Question
• Which motor system is responsible for crude muscle movements?
a. Pyramidal motor systemb. Extrapyramidal motor system

Answer
b. Extrapyramidal motor system: This system originates in the basal ganglia and provides background for the more crude, supportive movement patterns.

Neuromuscular Junction• Serves as a synapse between a motor
neuron and a skeletal muscle fiber• Consists of the axon terminals of a
motor neuron and a specialized region of the muscle membrane called the endplate
• The transmission of impulses is mediated by the release of the neurotransmitter acetylcholine from the axon terminals.
• Acetylcholine binds to receptors in the endplate region of the muscle fiber surface to cause muscle contraction.
Alterations of Neuromuscular Function• Drugs and Toxins can alter neuromuscular function
by changing the release, inactivation, or receptor binding of acetylcholine.– Curare acts on the post-junctional membrane of
the motor endplate to prevent the depolarizing effect of the neurotransmitter.• Used during many types of surgical procedures
– Clostridium botulinum blocks acetylcholine release and results in paralysis• Botox
– Organophosphates block acetylcholinesterase• Nerve gases and pesticides

Myasthenia Gravis
• Definition– Disorder of transmission at the neuromuscular
junction that affects communication between the motoneuron and the innervated muscle cell
• Cause– Autoimmune disease caused by antibody-
mediated loss of acetylcholine receptors in the neuromuscular junction• Sensitized Helper T Cells
– Antibody directed attack on receptors
Myasthenia Gravis• Muscle weakness and fatigability with sustained effort– Ptosis due to eyelid weakness– Diplopia– Progresses to generalized weakness
• Myasthenic crisis– Compromised ventilation– Usually during a period of stress


Diagnosis
• Tensilon or Edrophonium test– Acetylcholinesterase inhibitor• Patient feels little to no weakness for a short period of
time
• MUSK antibodies• http://www.youtube.com/watch?v
=k7YX9kuWrxA
Treatment• Pyridostigmine and neostigmine are the drugs of choice– Drug used to inhibit acetylcholinesterase
• Plasmapheresis– Removes antibodies from circulation– http://www.youtube.com/watch?v=AwAs7uUZJVE
• Intravenous immunoglobulin– Unknown how it works

Components of the Peripheral Nervous System
• Motor and sensory branches of the cranial and spinal nerves
• The peripheral parts of the autonomic nervous system
• Peripheral ganglia

Peripheral Nerve Regeneration
• Damage to a peripheral nerve axon due to injury or neuropathy– Results in degenerative changes, followed by
breakdown of the myelin sheath and Schwann cells • Regeneration factors– Proximity to soma– Crushing vs. cutting

Peripheral Neuropathy
• Definition– Any primary disorder of the peripheral nerves
• Results– Muscle weakness, with or without atrophy and
sensory changes• Involvement– Can involve a single nerve (mononeuropathy) or
multiple nerves (polyneuropathy)

Mononeuropathies
• Caused by localized conditions such as trauma, compression, or infections that affect a single spinal nerve, plexus, or peripheral nerve trunk– Fractured bones may lacerate or compress
nerves.– Excessively tight tourniquets may injure nerves
directly or produce ischemic injury.– Infections such as herpes zoster may affect a
single segmental afferent nerve distribution.

Mononeuropathies
• Carpal Tunnel Syndrome– Compression-type mononeuropathy
• Median nerve compression
– Tinsel Sign• Development of a tingling sensation in palm by light
percussion on median nerve at the wrist

Polyneuropathy
• Involves demyelination or axonal degeneration of multiple peripheral nerves that leads to symmetric sensory, motor, or mixed sensorimotor deficits
• Typically, the longest axons are involved first, with symptoms beginning in the distal part of the extremities.

Causes of Polyneuropathies• Immune mechanisms (Guillain-Barré syndrome,
rheumatoid arthitis, lupus, hypothyroid)• Toxic agents (arsenic polyneuropathy, lead
polyneuropathy, alcoholic polyneuropathy)• Metabolic diseases (diabetes mellitus, uremia,
chronic kidney disease)• Low levels of vitamin B12 or other problems
with your diet• Poor blood flow to the area

Segmental Demyelination• Disorder of the Schwann cells– Guillain-Barré Syndrome• Autoimmune disorder
– Linked to CMV, Campylobacter jejuni, and Epstein-Barr Virus
• Common in people of both sexes between ages 30 and 50• Can replace the Schwann cells• New myelin sheath is thin and subject to injury
• A serious disorder that occurs when the body's defense (immune) system mistakenly attacks part of the nervous system. This leads to nerve inflammation that causes muscle weakness.

Guillain-Barré Syndrome
• Symptoms– Rapidly progressing limb weakness and loss of
tendon reflexes– Flaccid paralysis– Pain– May lead to death due to ventilatory failure and
autonomic disturbances• Treatment– Plasmapheresis– Intravenous Immunoglobulin therapy– 80-90% achieve a gull and spontaneous recover in
6 to 12 months

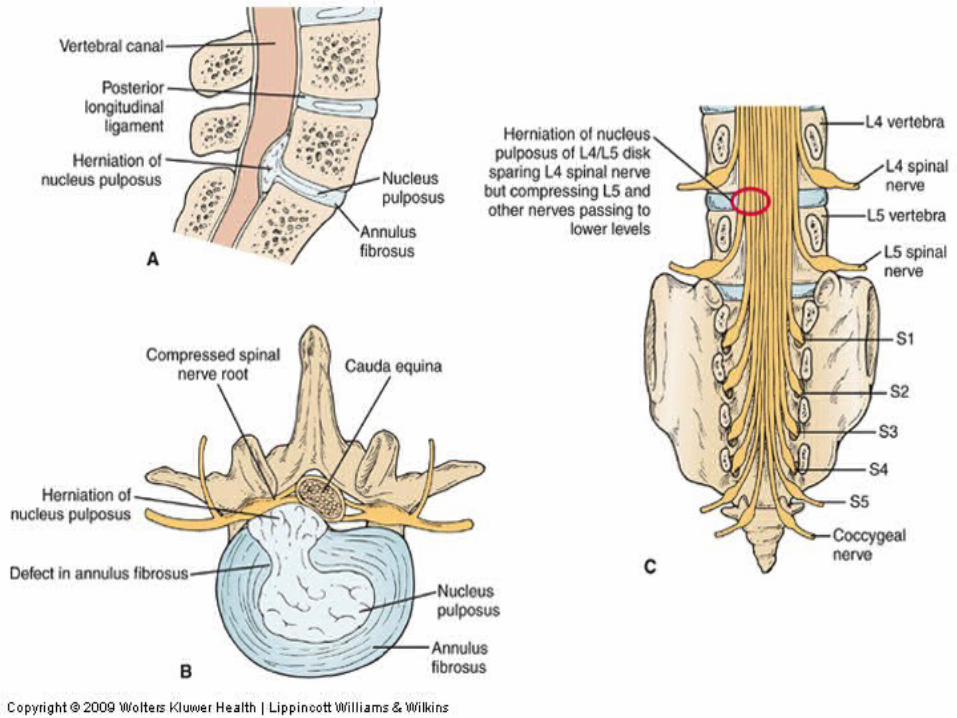
Nerve Root Injuries
• Herniated or Ruptured intervertebral disk – Sensory deficits • Spinal nerve root compression• Paresthesias and numbness
– Particularly of the leg and foot– Knee and ankle reflexes also may be diminished or absent
– Motor weakness and Pain


Question
• Lead toxicity would result in which of the following conditions?
a. Mononeuropathiesb. Polyneuropathiesc. Upper motor lesiond. Myasthenia gravis

Answer
a. Mononeuropathiesb. Polyneuropathies: Polyneuropathies would
result from systemic exposure to lead.c. Upper motor lesiond. Myasthenia gravis

Types of Involuntary Movement Disorders
• Tremor• Tics• Chorea = Irregular writhing movements• Athetosis = Wormlike twisting of limb• Ballismus = Violent flinging motion of limbs• Dystonia = Abnormal posture• Dyskinesias = Bizarre wriggling movements– Tardive Dyskinesia• Develops due to use of antipsychotic medications

Parkinson Disease• Definition
– A degenerative disorder of basal ganglia function that results in variable combinations of tremor, rigidity, and bradykinesia
• Characteristics– 0.3% of the general population has Parkinson Disease– Usually begins after 50 years of age– Progressive destruction of the nigrostriatal pathway, with subsequent
reduction in striatal concentrations of dopamine– Caused by environmental and genetic factors
• Clinical syndrome
– Parkinsonism• James Parkinson, 1817 = ‘shaky palsy’• Drug induced parkinsonism due to antipsychotics in high doses

Parkinson Disease
• Rigidity• Cogwheel-type motion– Ratchet-like movements
• Bradykinesia– Slowness initiating and performing
movements• Difficulty walking• Neuropsychiatric disorders

• http://www.youtube.com/watch?v=xuVY7wS25rc&feature=related

Amyotrophic Lateral Sclerosis (ALS)
• Definition– A devastating neurologic disorder that
selectively affects motor function– The disease typically follows a progressive
course, with a mean survival period of 2–5 years from the onset of symptoms.

Locations of Motoneurons Affected by ALS
• The anterior horn cells of the spinal cord
• The motor nuclei of the brain stem, particularly the hypoglossal nuclei
• The UMNS of the cerebral cortex
• Death of LMNs leads to denervation, with subsequent shrinkage of musculature and muscle fiber atrophy.

http://vimeo.com/27944955
http://www.youtube.com/watch?v
=-qFSMXEYC3c

Multiple Sclerosis (MS)
• A demyelinating disease of the CNS• Most common nontraumatic cause of neurologic
disability among young and middle-aged adults• Characterized by exacerbations and remissions over
many years in several different sites in the CNS– Initially, there is normal or near-normal
neurologic function between exacerbations.– As the disease progresses, there is less
improvement between exacerbations and increasing neurologic dysfunction.

http://www.youtube.com/watch?v=-BGBSsKBrbI&feature=related

http://www.youtube.com/watch?v=qgySDmRRzxY

Spinal Cord Injury (SCI)
• Definition– Damage to the neural elements of the spinal cord
• Causes– Motor vehicle crashes, falls, violence, and sporting
activities• Involvement
– Most SCIs involve damage to the vertebral column and/or supporting ligaments as well as the spinal cord.
– Commonly involve both sensory and motor function
Types of Injuries to the Vertebral Column
• Fractures• Dislocations• Subluxations

Types of Incomplete Spinal Cord Injuries
• Central cord syndrome• Anterior cord syndrome• Brown-Séquard syndrome• Conus medullaris syndrome

Areas Affected by SCI
• Spinal reflexes• Ventilation and communication• Autonomic nervous system• Temperature regulation• Edema and deep vein thrombosis• Sensorimotor function
Areas Affected by SCI (cont.)
• Skin integrity• Pain reception• Bladder and bowel function• Sexual function

Question
• Demyelination is the causative factor in which disease?
a. Parkinson diseaseb. ALSc. Multiple sclerosis

Answer
a. Parkinson’s diseaseb. ALSc. Multiple sclerosis: MS is caused by
an autoimmune attack on the oligodendrocytes of the CNS.

THE END

Classifications of Muscles
• Extensors– Muscles that increase the angle of a
joint• Flexors– Muscles that decrease the angle of
a joint

Components of the Neuromuscular System
• Neuromuscular unit containing motor neurons
• Myoneural junction• Muscle fibers– Actin and Myosin
• Spinal cord• Efferent pathways from the brain
stem circuits

Requirements of Motor Systems
• Upper motoneurons project from the motor cortex to the brain stem or spinal cord.– Directly or indirectly innervate the lower motoneurons or
contracting muscles– Motor unit is a motor neuron and all the muscle fibers it
innervates • Sensory feedback from the involved muscles – Continuously relayed to the cerebellum basal ganglia and
sensory cortex• Functioning neuromuscular junction that links nervous system
activity with muscle contraction

Mechanisms Controlling Coordinated Movement
• Agonists– Promote movement
• Antagonists– Oppose movement
• Synergists– Assist the agonist muscles by
stabilizing a joint or contributing additional force to the movement
Motor Unit
• The motor neuron and the muscle fibers it innervates– A single motor neuron may
innervate a few thousand muscle fibers
• Upper motor neurons• Lower motor neurons