Embed Size (px)
Citation preview

XA9847625
Chapter 28
LIVER AND GASTROINTESTINAL TRACT
Maqbool Ahmed Shahid
Introduction
Liver is often a site of a variety of diseases. A palpable liver during a routine clinical
examination is an important finding and requires further investigations. The availability of
non-invasive liver imaging procedures using nuclear, ultrasound, C.T. (and now MRI)
techniques have immensely enhanced diagnostic accuracy in liver diseases. In this Chapter,
a detailed description of routinely practised nuclear medicine procedures related to liver is
given. Brief reference is also made to other imaging techniques, particularly
ultrasonography, only for the purposes of comparison. Most of the information is based on
our own clinical experience of past 30 years.
While examining a radionuclide image of liver, it should be kept in mind that it is
basically a functional image and illustrates only those areas which have retained their function
in spite of disease. The unique advantage of this image is that at the same time it also shows
anatomical parameters i.e.size, shape, displacements, distortions, etc. The disease pattern
seen on the radionuclide liver image may be described as diffuse (as seen in hepatitis,
cirrhosis, fatty infiltration etc.) or focal (as in abscess, cyst, tumour etc.).
The visualization of spleen in a radiocolloid liver image provides additional valuable
information about the functional status of the liver. In addition to liver scintigraphy, other
useful nuclear medicine techniques applicable to liver include blood pool imaging,
hepatobiliary study, immunoscintigraphy, and radioimmunoassay for tumour markers.
A list of radiopharmaceuticals commonly employed for the diagnosis of liver diseases is
shown in Table I.
517

CHAPTER 28
TABLE I.
Radiocolloids
"Tc"
"Tc"
"Tcm
"Tc"1
Hepatobiliary
*Tcm
99Tca,
"Tc"
"Tcm
^ c "
RADIOPHARMACEUTICALS FORLIVER IMAGING
Sulphur Colloid
Tin Colloid
Antimony Colloid
Phytate
agents
Iminodiacetic acid (HIDA)
Paraisopropyl iminodiacetic acid (PIPIDA)
Parabutyl iminodiacetic acid (BIDA)
Diisopropyl iminodiacetic acid (DISIDA)
Diethyl iminodiacetic acid (DEIDA)
Tumour/abscess localization
67-Gallium (Tumour & abscess)
Ill-Indium labelled WBCs (Abscess).
Blood Pool agents
*TC»
"Tc"
"Tc"
'in vivo' labelled RBCs.
'in vitro' labelled RBCs.
labelled human serum albumin.
518

LIVER AND GASTROINTESTINAL TRACT
Anatomy
Liver is a bilobed, large solid organ which occupies almost the whole of the righthypochondrium. A part of its left lobe occupies the epigastrium and extends into the lefthypochondrium. The liver is divided into two parts by the falciform ligament. This divisionis also very often visible on the scintigram, but does not correspond to the actual anatomicaldivision of left and right lobes based on their blood supply and biliary drainage. The rightlobe also includes two other small lobes called caudate and quadrate lobes. The caudate lobeis situated on the posterior surface while the quadrate lobe lies on the inferior surface of theright lobe immediately medial to the gall bladder fossa. The quadrate lobe, if prominent,may be visible on the radionuclide image. The confluence of the portal vein, bile ducts andhepatic artery is called porta hepatis and this may show prominently as a focal defect at thejunction of the right and left lobes. Similarly the confluence of the hepatic veins at thecephalic attachment of falciform ligament sometimes appears as a wedge shaped defect alongthe upper border of the liver. The liver is surrounded from all sides by a large number ofother organs which may affect the shape of liver image in a radionuclide study. Theimportant organs include the diaphragm, right lung, heart, rib cage, gall bladder, rightkidney, intestines, biliary tract, stomach and pancreas.
The knowledge of the anatomy of biliary tract is necessary to interpret a hepatobiliarystudy. The two main hepatic ducts emerge from right and left lobes and join in the regionof porta hepatis to make common hepatic duct which travels inferiorly and is joined by thecystic duct from the gall bladder to make common bile duct. The common bile duct furtherdescends downwards up to 10-15 cm and enters the duodenum at ampulla of Vater where itis also joined by the pancreatic duct.
Gall bladder is a sac-like, pear-shaped structure which fills and empties through cysticduct. It is about 10 x 4 cm in size and is attached to the inferior surface of the right lobe,lateral to the quadrate lobe. It stores and concentrates bile and contracts to pour bile into thelumen of the duodenum. In acute cholecystitis, following a blocked cystic duct, the gallbladder is not visible in a hepatobiliary study. Intrahepatic gall bladder may produce a defectin the lower lateral part of the right lobe. In case of congenital biliary atresia, the obstructionat the level of hepatic duct is sometimes clearly visible in a hepatobiliary study. Similarlythe point of obstruction in the common bile duct due to a calculus or external pressure canbe detected.
In a radionuclide scan of liver, the spleen is also imaged due to its reticulo-endothelialsystem which normally phagocytoses the colloid particles. A normal spleen measures about12 x 7 cm in size and is situated posteriorly in the left hypochondrium. It can not be palpatedbelow the costal margin unless it is about three times enlarged. Very occasionally anaccessory spleen or a double spleen may be detected in the scintigram. In the developingcountries, the large spleens are seen in cirrhosis of liver and chronic myeloid leukaemia.Large malarial spleens are now not common in many of the South-East Asian countries.
519

CHAPTER 28
Physiology
The two main types of liver cells relevant to radionuclide imaging are the hepatocytes,which constitute the major bulk of the organ (80-90%) and the macrophages (Kupffer cells)which constitute only 2% of the total mass. The Kupffer cells are distributed in the liningof the vascular sinusoids and effectively remove colloid particles from the circulation. Theultimate clearance of the colloid from the circulation depends on the function of macrophages,perfusion of the hepatic lobules, and size of the colloid particles. Hepatocytes are capableof concentrating chemical substances like HID A, Rose Bengal and other dyes from thecirculation and excrete them with the bile. Diseases which affect the function of thehepatocytes e.g., inflammations, fatty infiltrations, toxic substances, malignancies, fibrosisetc. also affect the uptake and excretion of these substances.
RADIO-COLLOID LIVER-SPLEEN IMAGING
The function of phagocytosis is common to both liver and spleen due to the presence ofreticulo-endothelial cells (macrophages) in both the organs. Similar cells are also present inthe bone marrow and to a small extent in the lungs. The Kupffer cells make about 65% ofall macrophages in the body but would concentrate 80 to 90% of the total colloid particlesfrom the circulation. There is some correlation between the particle size and the extractionof the colloid by these organs. Smaller particles go the liver and smallest to the bonemarrow. Spleen takes up the larger particles. Thus the variation in the particle size mayalter the relative distribution of the radio-colloid injected.
Most commonly used radio-colloid for liver-spleen scintigraphy is "Tc" sulphur colloid.The usual dose is 2 to 5 mCi (75-185 MBq) and the estimated particle size is 0.3 to 1 micron.The uptake of radio-colloid in the liver depends on the overall perfusion of the organ and thefunctional integrity of Kupffer cells. In conditions affecting these factors, the uptake of "Tcm
colloid by the liver is diminished with corresponding increase in the uptake by spleen andbone marrow and infrequently by the lungs. This phenomenon is sometimes described as'spill over'.
Technical Procedure
The patient's abdomen is carefully palpated. Xiphisternum, costal margins, liver andspleen borders (if palpable) and outlines of any mass palpable in connection with the liver orin its vicinity are marked on the skin of the patient using an ordinary ink marker. These skinmarkings should be done in the same position in which the patient is going to be scanned onthe imaging device. The marking of mid-axillary line for the Right Lateral view may alsobe useful for aspiration or biopsy if required later.
It takes about 10 to 15 minutes for the maximum accumulation of radioactivity after aradiocolloid injection, and this is the optimum time to commence imaging in most of thecases. In patients with impaired liver function or portal hypertension, the optimal
520

LIVER AND GASTROINTESTINAL TRACT
concentration may be reached as late as 30 minutes after injection. The scanning is usuallydone with patient in the lying position. If a rectilinear scanner is being used, this is the onlypossible posture. When using this machine, the markings already made on the skin of thepatient are easily transferred to scan paper or X-ray film before starting the scan. A lowenergy, medium focus, five inches focal length collimator is used. The information densityshould be at least 800 counts/cm2. Background subtraction of 5 to 10% may be used. The'hot spot' is taken over the highest count rate on the liver in the anterior, right lateral, andposterior views. If spleen is the organ of interest, 'hot spot' is taken over the spleen in theleft lateral and posterior views. Anterior, posterior and Rt. lateral views are obtainedroutinely. If spleen is the organ of interest left lateral view should always be taken. Scanis started from the level of the fourth intercostal space downwards to below all liver or spleenactivity.
While using a gamma camera both lying and standing positions can be utilized. Theadvantage of standing position is that the up and down movement of the liver due todiaphragmatic excursions is reduced. Such movements degrade the quality of the image andsmall focal lesions may be obscured. A low energy, high resolution, parallel hole collimatoris used for the gamma camera and 500 000 to 1000 000 counts are collected for each image.Counts below 300 000 would be unsatisfactory. The views to be taken are the same asdescribed for the rectilinear scanner. Skin markings can be transferred to the image by usingradioactive point sources or thin lead strip. 2 cm2 pieces of lead may also be used to serveas a reference marker for the size of focal lesions on the image.
In a gamma camera having a provision for taking counts over the region of interest(ROI), the square of the ROI can be adjusted to the minimum and marked on the image.With the help of a radioactive point source, skin markings can be transferred to the imagein the form of small mini-squares. If a discrete focal lesion is seen in the liver, its positioncan be marked over the skin of the patient to facilitate biopsy or aspiration. A storageoscilloscope (persistent scope), if available on the gamma camera, is very useful inpositioning the patient for different views.
Interpretation
The evaluation of a liver image should include:
(a) Size, shape and position of the liver. Upwards, downwards and lateraldisplacement should be noted if present. Any deformity in the outlinedue to external pressure caused by the pathology in the neighbouringorgans like lungs, heart, stomach, pancreas, kidneys, gall bladder,biliary tract, intestines and ascitic fluid should be described. Degree ofhypertrophy or atrophy of the liver should be noted.
(b) The homogeneity of activity in the liver is described as uniform,non-uniform, diffuse, mottled, decreased etc. referring to differentanatomical parts of the organ.
521

CHAPTER 28
(c) Presence of focal defects is noted and their number, size, and exactanatomical location in the liver is described.
(d) Splenic image is carefully studied for size, site, density, deformity, andpresence of focal lesions. The presence of visibility of bone marrow andrelative distribution of colloid among liver, spleen and bone marrow isnoted. Occasionally the radiocolloid may also be visible in the lungfields.
(e) Artifacts due to pendulous right breast or metallic articles on the bodyof the patient such as coins should also be kept in mind whileinterpreting a liver scintigram. Hot spots produced by slightextravasation of radioactivity at the site of injection at the ante-cubitusand contamination of bed or patient's clothes by radioactive drops orspirit swab may be another source of artifacts.
The International Atomic Energy Agency (IAEA) in 1984, sponsored a three yearregional coordinated research project on liver imaging in the South East Asian Countries, forwhich a standard liver scintigram report sheet was prescribed. This includes a comprehensiveand convenient list of important points for the interpretation and description of a liver-spleenscintigram. This sheet can be requested from the Agency.
Normal liver scintigram
Radiocolloid image gives the best assessment of the size of the liver. It is difficult togive measurements for a standard 'normal' adult liver. The correct assessment of size comeswith experience. Clinical examination of the patient improves this assessment but it shouldbe always kept in mind that a palpable liver is not always enlarged. Conditions like chronicobstructive pulmonary disease, pleural effusion, tumours, subphrenic abscess, ascites, andlaxity of the hepatic ligaments in the old age can make a normal liver palpable. On the otherhand, an enlarged liver may not be palpable in cases of upward movement of righthemidiaphragm due to atelectasis or phrenic nerve paralysis.
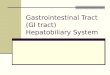
The distribution of the radioactivity in a normal liver image is homogenous, graduallythinning out towards the left lobe. (Fig. 28.1.) Regarding the shape of the liver, variousnormal configurations have been described. A triangular outline due to less prominent leftlobe; a prominent quadrate lobe; a tail-like projection extending downwards from the lowerend of the right lobe (Riedal's lobe), which may sometimes appear 'detached' from the rightlobe due to deep impression of the lower coastal margin; and so on. Impressions of portahepatis and falciform ligament may be seen at the junction of right and left lobes. Gallbladder may indent the inferior surface of the right lobe. Hepatic veins can notch the upperborder of the hepatic image. Similarly enlarged heart and pericardial effusion produce a deepconcavity along the upper border. In the posterior view, the right kidney often produces animpression on the right lobe and there is some masking of radioactivity in the liver tissuelying in front of the vertebral column. Spleen appears more prominent in this view as it is
522

LIVER AND GASTROINTESTINAL TRACT
nearer to the detector of the imaging instrument. In cases of biliary obstruction, the dilatedhepatic ducts may produce an appearance of focal defect at the junction of right and leftlobes.
A normal liver may appear abnormal in the image due to extrahepatic causes e.g.displacement and compression by the abdominal masses, supra and subphrenic pathology andbiliary disease.
Any deviation from the above description of a normal scan would indicate a strongpossibility of a diseased liver. There are two main types of abnormalities which can be seenin the liver. These are (a) Diffuse or (b) Focal.
The diffuse abnormalities may manifest as hepatomegaly or atrophy of the liver. Theimage may show overall diminution of the uptake of the radioisotope irrespective of the sizeof the liver. The distribution of the radiopharmaceutical may be non-uniform with or withoutdiminished uptake. A non-uniform uptake may be described, somewhat subjectively, invarious ways, such as diffuse, patchy, mottled; occasionally a non-uniform uptake may mimican appearance of multiple focal lesions, but such lesions do not show distinct boundaries.
The radiocolloid image is very sensitive for detecting the photon-deficient areas in theliver usually called focal defects. The smallest focal defect which can be detected in liver,using the modern gamma camera is about 1.0 cm in diameter. The detectibility also dependsupon the location of the lesion. Rarely, focal hot spots may be visualized on the scan. Thismay happen in cases of Budd-Chiari syndrome (hepatic vein obstruction), focal nodularhyperplasia, and occasionally in superior vena caval obstruction where a bolus of activityinjected into the basilic vein, can travel via collaterals and deliver a large amount of activityto the anterior mid-portion of liver.
Focal lesions can also be seen in the spleen, and one should not miss looking at thespleen critically in a radiocolloid liver image.
DIFFUSE DISEASES OF LIVER
Cirrhosis
Suspected cirrhosis of liver is a very important indication for radiocolloid liverscintigraphy. The typical picture in the advanced liver cirrhosis shows an atrophic, shrunkenliver having markedly diminished radionuclide uptake with patchy, mottled appearance. Thespleen is grossly enlarged and shows excessive radionuclide concentration. Thisphenomenon, where the normal liver-spleen ratio is reversed is called 'colloid shift' or'spill-over', as the diseased liver is unable to accommodate sufficient quantity of colloidwhich is then shifted to or spilled over to spleen. (Fig. 28.2.) Additional confirmation of thiscondition is obtained by the visibility of spine, sternum and the pelvis in the scan and
523

CHAPTER 28
occasionally the lungs as some colloid also spills over to the reticuloendothelial cells presentin these organs.
In cases where the excessive intake of alcohol plays an etiological role, frequently theright lobe may be more damaged and appear smaller on the scan than the left lobe. Thepossible explanation for this being that the main stream of portal blood flow passes throughthe right lobe, and therefore more alcoholic damage to this lobe. In early cases of cirrhosis,the liver may appear enlarged or normal in size, although with diminished uptake, and spleenmay be only moderately enlarged with positive 'spill-over' phenomenon. In long standingcases definite focal defects may appear indicating development of hepatocellular carcinomafor which cirrhosis is a predisposing condition.
The mechanism involved in producing diminished uptake of liver and spill-over to otherorgans seen on a radiocolloid scan involves:
(a) impairment of macrophage function
(b) diminished hepatic perfusion,
(c) replacement of liver parenchyma by fibrous tissue,
(d) shunting of blood from the liver to spleen and bone marrow,
(e) intrahepatic alteration in blood flow so that the blood is shunted away from thesinusoids which are lined by the macrophages.
In cirrhosis, widespread death of liver cells from many causes is accompanied andfollowed by progressive fibrosis, regenerative hyperplasia of surviving hepatocytes anddistortion of liver architecture resulting in portal-systemic vascular shunts. Splenicenlargement is caused mainly by portal hypertension. The extreme degree of splenicenlargement is observed in advanced cirrhosis. The other important condition withcomparable gross splenic enlargement is chronic myeloid leukaemia (CML). But in thisdisease, the most important finding on radiocolloid scan is normal relative uptake ofradioactivity by liver and spleen and the 'spill-over' is therefore, not seen.
Using a gamma camera, we have done a short study of comparing the counts of smallregions of interest (ROIs) of the same dimensions on the right lobe of liver and spleen. Innormal individuals the average liver/spleen ratio was 4:1. Advanced cirrhotic cases showedexactly a reverse ratio. In cases of chronic hepatitis the liver/spleen ratio was 1:1.5. Thistechnique can be applied in assessing the degree of impairment of liver function inquantitative terms to confirm the visual impression of diminished liver uptake.
524

LIVER AND GASTROINTESTINAL TRACT
Other Diffuse Liver disorders
Other diffuse liver disorders leading to liver enlargement with or without non-uniformdistribution of radioactivity in the liver include:
(a)(b)(c)(d)(e)(0(g)(h)(00)
Congestive cardiac failure,Lymphomas,Leukaemia,Amyloidosis,Sarcoidosis,Kala Azar,Malaria,Schistosomiasis,Acute and Chronic Hepatitis,fatty degeneration in diabetes.
Lymphomas may show as diffuse disease or as definite focal lesions.
FOCAL DISEASES OF LIVER
Amoebic abscess
In the developing countries, the amoebic liver abscess is still one of the common causesresulting in the appearance of a focal defect in a radiocolloid liver scan. However, in myexperience of about 30 years in nuclear medicine in a developing country, I feel that therehas been a gradual decline in the number of liver abscess cases during this long period. Thereason for this is probably the gradual improvement in the living conditions and standards ofpersonal and community hygiene in some of the developing countries. It is also likely thatless number of patients are referred to nuclear medicine department, as many of them arereferred for ultrasound examinations.
Amoebic liver abscess usually appears as a solitary, well-defined rounded focal defectmostly situated in the right lobe (Fig. 28.3). Less commonly the left lobe may be involved.Multiple abscesses of different sizes may occasionally be seen. Sometimes the location of theabscess is such that it produces obstructive jaundice through pressure on the main hepaticducts. The exact site of the abscess can be ascertained by taking multiple views. It must beremembered that a focal defect on radiocolloid image is a non-specific finding. Moreinformation would be required to confirm that the lesion is an abscess. Ultrasonography isa convenient procedure to differentiate between solid and cystic lesions. Cystic lesion in adeveloping country could be an abscess or an hydatid cyst, although the latter is not ascommon as an abscess. The abscess is characterized by the presence of abdominal pain,pyrexia, nocturnal sweating, malaise and liver tenderness. This clinical picture is not seenin the hydatid cyst where the main complaint is enlargement of liver which may feel hard inthe area of cyst. Amoebic abscess is often so insidious in its progress that clinical history is
525

CHAPTER 28
not very helpful in all the cases.It may also be remembered that in an early amoebic lesionwhere the disease is still in cellulitis phase and frank pus has not appeared theultrasonography may give misleading information. The central area of the abscess (and cyst)is usually avascular. It is therefore, a routine at some centres to inject the radiocolloid whenthe patient is lying under the gamma camera and take sequential pictures after every 2-4seconds for a dynamic blood flow study. A malignant lesion is usually hypovascular, but notcompletely devoid of perfusion as compared to the abscess or cyst.
Treatment with proper anti-amoebic drugs alleviates the patient's clinical symptomswithin one or two weeks. However, the cold area on the scan persists for a long time, evenfor several months. There is no point in doing follow-up scans every week or so. In anycase, ultrasound scans are better for follow-up evaluation.
Pyogenic Abscess
Pyogenic abscess is seen less commonly in the developing countries. A pyogenic abscessis accompanied by acute symptoms of fever, malaise, sweating and pain in the righthypochondrium and higher mortality. There may be a large single abscess or multiple smallabscesses. Timely treatment with antibiotics and aspiration, if required, often cures thedisease.
Subdiaphragmatic Abscess
This is an uncommon condition where there is an abscess in the potential space betweenright hemidiaphragm and right lobe of the liver. Clinically, the patient shows all signs andsymptoms of pyogenic infection but it is difficult to find the location of the abscess. Thepatient may complain of pain in the lower part of the chest on the right side. Theradiocolloid liver scan may appear normal or there may be slight flattening of the upperborder of the right lobe. The condition can be diagnosed by doing a liver and lungradiocolloid scan simultaneously. Patient is injected with "Td* sulphur colloid and "Tc™Albumin macroaggregates and liver-lung area imaged in anterior, right lateral and posteriorviews. In case of subphrenic abscess, the cold gap between liver and lung is clearly outlined.
Hydatid cyst
Hydatid cyst is an helminthic infestation caused by a tiny tapeworm called Echinococcusgranulosum for which dog and certain wild canines act as definitive hosts. The worm residesin the gut of these hosts. Animals like sheep, camel and other cattle are infested by ingestingthe eggs from the pastures or water contaminated by the faeces of dogs. Men who live inclose contact with dogs have a risk of getting infested. The embryo is liberated from the eggin the small intestine and gains access to the liver through portal circulation. The resultantcyst which is the larval stage of the worm, grows very slowly for years. It may ultimatelycalcify or rupture giving rise to multiple cysts. When the cyst has grown to a large size, itmay produce pressure symptoms where it is located.
526

LIVER AND GASTROINTESTINAL TRACT
In nearly 75 % of patients with hydatid disease, the right lobe of liver contains a singlecyst. Multiple cysts are not very common. Hydatid cyst may also be found in lungs, brainor elsewhere. The treatment is essentially surgical. Cases of recurrence may be seen if somelarvae escape to other parts of the liver. On clinical examination, the cyst feels hard and maybe mistaken for a malignant growth. Calcification if present can be seen on radiologicalexamination.
On a radiocolloid scan, the hydatid cyst appears as a 'cold' area (Fig. 28.4). Themargins of the defect may be sharp and the shape more rounded as compared to an abscessor a tumour. Ultrasonography is a simple procedure to illustrate the cystic nature of thehydatid disease. Further confirmation may be possible through identification of daughter fociin the main cyst in the ultrasonogram. A blood pool or a perfusion study will exhibit alargely avascular nature of the defect. Intradermal (Casoni's) test, complement fixation andimmunofluorescent tests give support to the diagnosis in the presence of a long history andabsence of signs and symptoms of an abscess. No attempt of confirming diagnosis withneedle biopsy should be made in suspected hydatid cyst because of the risk of disseminationwithin and outside the liver.
Primary liver tumours
Hepatocellular carcinoma is a fairly common finding in some of the developing countries.It is the first or second commonest malignancy in the male population.
Cirrhosis of liver, a predisposing condition, increases the risk of primary liver cancermanifold. In a study done in Pakistan 12% of the cases of cirrhosis of Liver were found tobe positive for cancer on radiocolloid scan and histological examination (needle biopsy).Liver cancer can, however, occur in an otherwise normal liver at any age. Regular use oforal contraceptives, which may produce hepatic adenomas, may be another causative factor.HBsAg positive sera helps in detecting high risk groups. On a radiocolloid scan, the livercancer appears as a 'cold' area which is solitary in most of the cases but multiple primarylesions are also found. 67Ga study may produce a positive image of the cancerous area butit is not always outlined well and the appearance is non-specific. It is, therefore, not advisedas a routine test. The better alternative is to do ultrasonography and make sure that the lesionis solid and proceed with needle biopsy for the exact diagnosis. High blood level ofalpha-fetoprotein is a common finding but for diagnosis, it is still non-specific. Sequentialestimations at regular intervals are supposed to be of prognostic value.
The use of contraceptive pills on a regular basis, although uncommon in developingcountries, may be seen in young women in urban areas. This may give rise to asymptomatichepatic cell adenomas incidently detected on a radiocolloid image as a focal defect due to lackof Kupffer cells. The tumour tends to regress with the discontinuation of pills. The hepaticcell adenoma should be distinguished from focal nodular hyperplasia of liver which is alsocommon in women and appears as normal liver tissue in a radiocolloid image.
527

CHAPTER 28
Metastatic liver disease
Primary malignancies of the gastro-intestinal tract are likely to give rise to earlysecondary deposits in the liver via portal circulation. Direct local extension from the gallbladder is also a common finding. Other more common primary malignancies Likely toproduce metastatic liver disease are those of breast and lungs (Fig. 28.5). Lymphomas alsoinvolve liver at an advanced stage. The hepatic metastases in most of the cases appear asmultiple lesions which may be discrete or infiltrative in type. However, a solitary lesion inthe presence of a known primary malignancy indicates a strong possibility of a secondarydeposit. Ultrasound examination may be done to ascertain the solid nature of the lesion.
Massive infiltration of liver by metastatic tissue may produce impairedreticulo-endothelial function causing colloid shift from liver to spleen. The sensitivity ofradio-colloid scan to detect metastatic disease in the liver has been mentioned to be in therange of 75-80% as the small deep seated lesions are likely to be missed. The sensitivity willprobably improve with the use of single photon emission tomography (SPECT) but its use inthe developing countries is still limited.
Spleen Image
Reference to enlargement of spleen in cases of portal hypertension has already been madewhile discussing cirrhosis of the liver. In the tropical countries, repeated malarial infestationmay be an important cause of splenomegaly but is not as frequently seen as before. Anumber of haematological disorders also produce splenic enlargement. A grossly enlargedspleen with moderate liver enlargement is quite a frequent finding in cases of chronic myeloidleukaemia. Hepatosplenomegaly may also be seen in patients suffering from Tymphoma. Itmay be emphasized that the normal liver/spleen ratio of radiocolloid accumulation is notaltered in splenomegaly due to reasons other than portal hypertension unless the liver is alsodamaged.
Focal defects in spleen is a rare finding which may be seen in cases of lymphoma.Haematoma as a result of injury to an enlarged spleen also appears as a cold area on aradiocolloid scan. We have not seen any case of cyst or abscess in the spleen.
Like liver, the spleen can also be displaced by mass lesions and other abnormalities inthe neighbouring structures like stomach, pancreas, left lung, pleura, left kidney and massesin the abdomen.
528

LIVER AND GASTROINTESTINAL TRACT
PATTERN OF LIVER DISEASE IN PATIENTS IMAGED WITH RADIOCOLLOIDS
The information given below was presented in a meeting of Experts Group for theIAEA-RCA Regional Cooperative project on "Imaging procedures for the diagnosis of liverdiseases" held at Seoul on 22 - 24 August, 1984. It is derived by analyzing the results of1000 consecutive patients in whom radiocolloid liver imaging was done during July toOctober, 1983 at the Mayo Hospital, Lahore, Pakistan. Out of these 1000 patients 514 wereimaged with a gamma camera and 486 with a rectilinear scanner.
Table II shows the age and sex distribution of these 1000 cases. About half of thepatients (45%) are between the age 41 and 60, and the male to female ratio is almost same.Table III shows the disease-spectrum in these patients. Definite focal defects were found in11.3% cases. A majority of the patients (46.9%) were those with Hepatomegaly of diverseorigin. 18.6% cases had no abnormality. In the patients with definite focal defectsmalignancy was the most common (6.8%). Abscess was found in 3% and the cyst in only1.4%. Spleen was enlarged in 31.3% of the images. Cirrhosis of liver is still fairlycommon. In 3.8% cases, it was not possible to say whether the abnormality seen is a truefocal defect or is a diffuse low activity area.
This information describes a pattern of hepatic diseases in patients referred for imagingto a nuclear medicine department in one of the developing countries. It may not representthe pattern in all the developing countries of South East Asia but it still gives an overallpicture of the types of liver diseases with their relative frequencies as seen in one of them.
TABLE II. AGE AND SEX DISTRIBUTION OF 1000 PATIENTSREFERRED FOR LIVER IMAGING.
AEMC, LAHORE, PAKISTAN.
AGE
0 - 10
11 - 2 0
21 - 3 0
31 - 4 0
41 - 5 0
51 - 6 0
61 - 7 0
> 70
TOTAL
MALE
20
45
63
75
100
102
50
28
482
FEMALE
9
33
67
111
142
120
27
8
518
TOTAL
29
78
130
186
242
222
77
36
1000
%
2.9
7.8
13.0
18.6
24.2
22.2
7.7
3.6
100
529

CHAPTER 28
TABLE i n . DISEASE SPECTRUM OF PATIENTS FOR LIVER IMAGING.
DISEASE
Cirrhosis
Abscess
Cyst
SubphrenicAbscess
Malignancy
Hepatomegaly;unif. upt.
Diffuse low upt.areas
Uncertain
Normal
TOTAL
Spleen enlargem.
MALE
51
19
08
01
34
212
44
18
95
482
156
FEMALE
51
11
06
0
34
257
48
20
91
518
156
TOTAL
102
30
14
01
68
469
92
38
186
1000
312
%
10.2
3.0
1.4
0.1
6.8
46.9
9.2
3.8
18.6
100
31.2
COMPARISON OF NUCLEAR HEPATIC IMAGINGWITH ULTRASONOGRAPHY
In most of the developing countries, the nuclear medicine facilities are scarce and workload immense. A considerable number of routine referral is for radiocolloid liver imaging.At the same time, there is a feeling that the information obtained by a nuclear liver image canalso be obtained from ultrasound examination which is less expensive and also time-saving.In the developing countries therefore, if most of the load of liver imaging is shifted fromnuclear to sonography, the nuclear facility can be spared for tests like detection of skeletalmetastases, cardiac studies etc. which can not be done by non-nuclear techniques. Thequestion to be answered is, how far an ultrasonographic examination can replace the nuclearradiocolloid liver imaging? The following Table IV summarizes the differences betweenthese two imaging modalities:
530

LIVER AND GASTROINTESTINAL TRACT
TABLE IV. COMPARISON OF NUCLEAR WITH ULTRASOUNDIMAGING OF THE LIVER.
Cost
Spatial resolution
Differentiation between cystic vs solid
Skills and training required
Liver size estimation
Radiation exposure
Imaging in the presence of dressings,drains, plasters, open wounds etc.
Nuclear
more expensive
2 cm or larger
not possible
modest
excellent
within permissiblelimits
possible
Ultrasound
less expensive
can detect smallerlesions
possible
highly skilled andexperienced doctor
required
less satisfactory
nil
Impossible
Previously the ultrasound examination of the liver suffered from the presence of'rib-shadowing' rendering a part of the liver 'invisible' to the transducer, but now with theadvances in the design of transducers and availability of sector scanners the entire liver cannow be 'seen'. One can even scan through the intercostal spaces.
The International Atomic Energy Agency under its Regional Cooperation Agreement(RCA) program for Asia Pacific Region has started a regional cooperative research projectin 1989 comparing the efficacy of ultrasonography with nuclear imaging for the detection offocal and diffuse liver disease. Our institute (INMOL Lahore) is also one of the participantsin this study.
Although it will take another two or more years for the final results of the IAEA'sproject to come but in the meantime, we have been collecting information on patients whohave undergone both radiocolloid and ultrasound imaging and have analyzed results in 196patients up to now which is as follows.
531

CHAPTER 28
Total number of Patients =
A) Focal lesion positive cases =(combining nuclear and ultrasound images)
Nuclear image detected =missed =Total =
Sensitivity =
Ultrasound detected =missed =Total
Sensitivity
196
142
12616
142
88%
1348
142
94%
This means that nuclear imaging missed 16 out of 142 cases of focal defects which weredetected by ultrasound imaging while ultrasound missed 8 out of 142 cases of focal defectswhich were detected by the nuclear image.
Diffuse liver disease positive = 44
Nuclear scan
Ultrasound
detected =missed =Total =
Sensitivity =
detected =missed =Total =
321244
72.7
404
44
Sensitivity = 90%
532

LIVER AND GASTROINTESTINAL TRACT
This means that 12 out of 44 cases missed by the nuclear imaging are detected by theultrasound and 4 out of 44 missed by the ultrasound were detected by the nuclear imaging.
(a) Cases normal both on nuclear and ultrasound imaging = 10
(b) Ultrasound examination revealed that 26 cases who werepositive for focal defect both on ultrasound and nuclearimaging were cystic in nature.
(c) In 12 cases, where nuclear scan showed only solitary lesion,the ultrasound revealed multiple lesions.
(d) The cases of diffuse disease which were missed by thenuclear image were mainly those with congestive cardiacfailure and biliary obstruction in which the ultrasound scanshowed congested vessels and dilated hepatic ducts.
From the above observations, it appears that ultrasonography is superior to nuclearimaging for the detection of focal defects and diffuse liver disease (Figs. 28.6 A and B and28.7 A and B). There is, however, a small percentage of cases missed by the ultrasound anddetected by nuclear imaging. It may, however, be prudent to see the final results andrecommendations of the above mentioned multicentric trial initiated by IAEA.
HEPATOBILIARY IMAGING.
The chemical substances which follow the route of bilirubin in liver and biliary passages,can be used with a suitable radioactive label to study the function of hepatbcyte and thebiliary system. In fact, the first compound recognized as a possible liver imagingradiopharmaceutical was a hepatobiliary agent, the I3II labelled Rose Bengal, a fluorescenthalogenated dye. The other dye used for this purpose was Bromosulphthalein (BSP). Ascompared to the colloids, these dyes had the disadvantage of rapid excretion and constantlychanging levels of activity in different parts of the liver even during the course ofexamination, especially with the rectilinear scanner, resulting in poor images. Later on, withthe development of gamma cameras m I labelled Rose Bengal and BSP were revived forstudying hepatobiliary function but by that time "Tcm labelled compounds had establishedtheir superiority for use with the gamma camera.
These new imaging agents are iminodiacetic acid (EDA) analogues which provide highquality images of the biliary system. The first IDA derivative used widely was the dimethylIDA also called hepatobiliary IDA or HIDA. Approximately 85% of this compound isexcreted by the liver and 15% by the kidneys. In cases of liver damage, a larger fraction isexcreted through the kidneys. However, acceptable biliary images can be obtained withserum bilirubin levels as high as 5-7 mg/dl. The other derivatives of IDA devised laterinclude paraisopropyl IDA (PIPIDA), parabutyl IDA (BIDA), diisopropyl IDA (DISIDA) and
533

CHAPTER 28
diethyl IDA (DEIDA). DISIDA is probably more suitable because of its high biliaryexcretion.
Procedure
About two hours fasting before the test is usually advised. Prolonged fasting renders thegall bladder akinetic and filled with viscous, static bile which inhibits the entry of HIDA inthe gall bladder and therefore poor visualization of gall bladder. Similar thing happens inpatients on total parenteral nutrition or patients of chronic alcoholism.
The patient is given 3 - 5 mCi (100 - 200 MBq) of "Tcm labelled IDA intravenously.Sequential images of anterior abdomen are taken with a gamma camera, at 10 minutesintervals for one hour. The first image taken five minutes after injection may be useful tooutline the liver as the radioactivity is passing through it.
As the study proceeds, the radioactivity passes from the liver towards porta hepatis andhepatic ducts may be (Fig. 28.8) visualized. Simultaneously the common bile duct and thecystic duct become visible. The gall bladder, normally, fills up within half an hour afterinjection. At about the same time, the loops of duodenum are also visualized. Clearance ofactivity from the liver starts within 10-15 minutes and at the end of the study the liver ishardly visible and the gall bladder still shows prominently. At this point, the patient may begiven a standard fatty meal as in cholecystography to demonstrate contraction and emptyingof the gall bladder.
In those cases, where the overall liver function is poor the study can be continued for alonger period as there may be a delayed visualization of various structures. If the liverfunction is grossly impaired the radiopharmaceutical is excreted mainly through the renalsystem and both kidneys and urinary bladder show up prominently. This also happens incases of biliary atresia. In such situations, the activity in the right kidney may be mistakenfor the gall bladder, but presence of the left kidney image in the scan picture should avoidsuch a confusion.
The IDA hepatobiliary study gives useful information in a number of clinical conditionslike acute cholecystitis, chronic cholecystitis, gall stones, biliary tract obstruction, jaundice,bile leak, congenital biliary atresia (Fig. 28.9) and choledochal cysts.
Acute cholecystitis
Acute cholecystitis is almost always associated with obstruction of the gall bladder neckor cystic duct by a gall stone or an intestinal parasite like a round worm. Occasionally,obstruction may be by mucus or rarely by a neoplasm. HIDA hepatobiliary study is ideal for(Fig. 28.10) investigating the patency of the cystic duct. If the gall bladder is outlined in thestudy, the patency of the cystic duct is proved beyond doubt. HIDA is so sensitive for thediagnosis of this condition that intravenous cholangiogram for this purpose is now consideredunnecessary.
534

LIVER AND GASTROINTESTINAL TRACT
Although the non-visualization of gall bladder in a HID A study in the presence of clinicalsigns and symptoms of acute cholecystitis establishes the diagnosis, some rare situationsshould be kept in mind where the non-visualization could also be due to few other reasons.As already mentioned a patient fasting for more than 12 hours has his gall bladder filled withbile and therefore the radioactive bile after HIDA injection cannot enter unless the gallbladder contracts and expels the stored bile. This can be achieved by giving an injection ofCholecystokinin (CCK) along with HIDA. However two other situations still remain in whichCCK fails to contract gall bladder. These include cases with chronic alcoholism and/orpancreatitis and those who are on total parenteral nutrition. In these situations theultrasonography can help in diagnosis by demonstrating a full gall bladder corresponding tothe clinically tender area in the right upper abdomen. Sonography is also capable of detectingcalculi, but the presence of calculi alone is not sufficient to prove the diagnosis of acutecholecystitis.
Although there are no specific findings in a HIDA study characteristic of chroniccholecystitis, a few important points can be briefly mentioned which are very often associatedwith chronic gall bladder disease:
(a) Delayed visualization of the gall bladder, i.e. one hour or moreafter injection of HIDA.
(b) Delayed biliary to bowel transit time.
(c) Filling defects within the gall bladder due to stones.
(d) Suboptimal contractile response of a filled gall bladder tocholecystokinin.
Biliary Atresia
In jaundiced neonates, it is important to differentiate between congenital biliary atresiaand neonatal hepatitis, so that biliary atresia could be corrected by timely surgicalintervention. If HIDA hepatobiliary study shows a patent biliary passage, biliary atresia isruled out. In cases of atresia, the exact site of obstruction can be seen sometimes at the levelof hepatic duct, as it emerges at the Porta hepatis. In such cases, the radioactivity isultimately excreted through the urinary system and both kidneys and the urinary bladder areoutlined in the scan.
The hepatobiliary study is the most convenient, sensitive, and non-invasive test fordetection of bile leakage after trauma or a surgical procedure. After an intravenous injectionof the radiopharmaceutical (5 mCi or 200 MBq), the abdomen is imaged for at least twohours. Delayed pictures may be taken at 12 hrs and 24 hrs. Presence of radioactivity outsideliver and biliary system would confirm pathological extravasation. Ultrasonography and CTimaging may reveal abnormal fluid collection in the area but cannot detect the exact natureof the fluid.
535

CHAPTER 28
Blood Pool Imaging of Liver
It may be useful to find out the state of perfusion of a focal defect seen on a radiocolloidliver scan. While cysts and abscesses are devoid of blood supply, the neoplastic focal defectsmay show varying degree of perfusion. However, the absence of perfusion does notnecessarily prove that the lesion is non-neoplastic because a neoplastic focal defects may alsoappear avascular in a blood pool scan due to central necrosis. Hemangiomas, on the otherhand, show as hypervascular areas in the blood pool scan.
If a computerized gamma camera is available for the study, information on perfusion ofdifferent parts of the liver can be obtained as a part of the routine radiocolloid imaging. Forthis purpose, the patient is positioned under the gamma camera before injecting theradiocolloid. The radioactivity over the liver is recorded continuously, immediately after theinjection as the blood carrying the bolus of radiocolloid appears in the liver. Later on, thestatic radiocolloid uptake images are taken as usual. Drawing the regions of interest (ROIs)over the focal defects in the perfusion phase and radiocolloid uptake phase it can be assessedwhether the focal defect appearing in the radiocolloid phase is vascular or avascular.Time-activity curve can also be generated on these ROIs to get better understanding of theperfusion of the lesion.
Alternatively, a blood pool agent can be used to study the vascularity of the areacorresponding to the focal defect in the radiocolloid image. For this purpose, the mostconvenient technique is the 'in vivo' of red blood cells using "Tc01 as a label.
A sterile solution of 1.2 mg stannous chloride and 1.8 mg of pyrophosphate stabilizedat a pH around six is injected intravenously. "Tc™, at least 10 mCi (400 MBq), is injectedi.v. half an hour later. This results in 'in vivo' of RBCs. We have used this techniquesuccessfully for investigating focal defects in the liver. The other possibilities are to use"Tc111 labelled human serum albumin or in vitro labelled red blood cells.
^Gallium imaging
Gallium localizes non-specifically in soft tissue tumours and inflammatory lesions. It isexpensive and difficult to obtain in the developing countries. Its physical characteristics arenot ideal for in vivo imaging; low energy photons (91 keV) not suitable for optimal intrinsicresolution and the high energy photons (394 keV) difficult to collimate. Its relatively slowexcretion through the intestine, often interferes with accurate Imaging of abdominal and pelviclesions.
67Ga scintigraphy is useful in detecting sites of acute infections as well as otherinflammatory and granulomatous processes. It is useful especially in detecting pulmonaryinflammatory diseases, abdominal and pelvic inflammations and in inflammatory diseases ofthe skeleton.
536

LIVER AND GASTROINTESTINAL TRACT
67Ga scintigraphy is also useful as a diagnostic procedure for tumour detection, stagingand monitoring the effect of therapy. The tumours usually detected with 67Ga arelymphomas, lung carcinoma, primary hepatic carcinoma and malignant melanoma. Galliumscintigraphy is neither very sensitive nor very specific but occasionally it might provide someuseful information. However, it has no significant role in routine diagnostic work up of apatient with a space occupying lesion in the liver.
A more specific and sensitive method for imaging inflammatory disease is byradiolabelled white blood cells, which is described extensively in Chapter 27.
SPECT vs conventional imaging of the liver
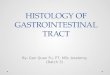
With the developments in ultrasonography and computerized axial tomography the valueof radionuclide liver imaging is significantly reduced as the sensitivity of the detection of liverlesions by isotopic methods has been reported to be 75% and 85% whereas these otherimaging modalities claim accuracies of 90% or better. Single photon emission tomographyhas been found to improve the detectability of liver lesions (Fig. 28.11).
Liver is a large solid organ with complex internal scatter patterns. Liver imaging withSPECT needs attenuation correction and a high resolution collimator. Sensitivity of SPECTfor liver focal defects is as high as 92% in some of the reported series.
Since the size of a liver lesion is a useful parameter to a clinical oncologist, the systemthat provides this information is advantageous. Lesion reduction is a volumetric phenomenon,not necessarily measured accurately in only two dimensions. It is possible to determine thevolume of liver lesions from SPECT data. This type of study is very helpful in monitoringestablished liver lesions in patients on chemotherapy. SPECT, not only providesimprovement in the detectability of liver lesions, but also gives exact measurement of thevolume of such lesions.
GASTROINTESTINAL TRACT
Gastro-oesophageal Function
Radionuclide techniques can be employed for studying the function of oesophagus,stomach and any abnormalities at the gastro-oesophageal junction. Using an appropriateradiopharmaceutical and a computerized gamma camera a number of useful tests can beperformed quite conveniently. The commonly performed tests include: gastric emptying rate,oesophageal transit time, and detection and quantification or gastro-oesophageal reflux. Inperforming these studies non-absorbable radiopharmaceuticals such as "Tc"1 sulphur colloidor "Tc^DTPA (diethylene triamine penta-acetic acid) are used.
537

CHAPTER 28
Gastrointestinal Bleeding
Since 1960, we have been using s 'Cr labelled red blood cells for measuring the amountof blood loss in the stools in suspected gastro-intestinal bleeding by a simple technique.Using an activity of 100 /id 51Cr, 5 to 10 ml of red cells of the patient are labelled in vitro,and re-injected immediately. The patient is asked to take two identical empty dry milk tinsof about half a litre capacity and collect 24 hours stools in one of these tins. Next day thetin containing the stools, closed with a tight lid, along with the empty tin is handed over bythe patient to the hospital staff.
Two ml of patient's blood is taken and added to the empty tin with some saponin tohaemolyze the blood. The tin containing stools is weighed on a small balance. The othertin, now containing two ml blood is placed on the same balance and water added to it slowlytill it weighs the same as the other tin containing the stools. The lid is tightly closed and tinis shaken few times to make a homogeneous solution of the haemolyzed blood. Theradioactivity of the two tins is measured by a scintillation counter in identical geometricalconditions. Counts of the stools compared with the blood counts. The exact volume of bloodpresent in the 24 hours stools can be calculated by a simple equation.
CPM of stools x 2Blood loss in mis. =
CPM of blood
Two ml blood sample is taken as this volume gives reasonable counts on the scintillationcounter. Thus simply by looking at the counts obtained from the 24 hours stools one can findout at a glance whether there is any excessive blood loss present. The exact volume is thencalculated.
This simple test, although quite useful for measuring total blood loss in stools in 24hours, does not give any information about the exact site of bleeding in the gut for which animaging technique is needed.
It is important to locate the site of gastrointestinal bleeding before a decision for an activeintervention. The radiopharmaceutical generally used for detecting lower G.I. bleeding is"Tc" sulphur colloid. It is routinely available in the nuclear medicine departments becauseof its use for radiocolloid liver imaging. The other important advantage which it has overthe intravascular blood pool agents (e.g. "Tcm labelled RBCs) is its rapid clearance fromcirculation by the reticuloendothelial system of liver and spleen resulting in very low tissuebackground activity providing excellent contrast between background and extravasatedradioisotope at the bleeding site.
The radioactivity in the liver makes it difficult to detect any bleeding sites in the upperabdomen, but even with the blood pool agents the liver activity is quite high because of thevascularity of liver. The procedure requires a dose of 10 mCi (400 MBq) of "Tc™ sulphurcolloid to be injected intravenously with the patient placed under the gamma camera. A large
538

LIVER AND GASTROINTESTINAL TRACT
field-of-view camera which can cover the whole abdomen at a time and a low energycollimator are necessary. 300 000 to 500 000 count images are obtained every two minutesfor 15 minutes. A bleeding site is seen as a hot spot in the image. If the study is continued,the activity may be seen travelling distally along the intestine with peristaltic movements. Acarefully performed study has a high degree of sensitivity with a low false negative rate.Because the sulphur colloid is cleared from the circulation within 15 minutes, only thatbleeding can be detected which occurs within 15 minutes of injection.
For detecting intermittent bleeding, the intravascular blood pool agents should be usedand patient imaged intermittently for 24 hours after the injection. As the sensitivity of thisprocedure is low, larger amounts of blood should extravasate for detection as compared tothe radiocolloid technique.
Meckel's diverticulum
Meckel's diverticulum is a developmental anomaly which is in the form of a small saclike protrusion from anterior mesenteric border of the ileum about three feet proximal to theileocecal valve. This diverticulum is lined with ectopic gastric mucosa. This occurs in about2% of the population and in most of the cases remains symptomless. Occasionallyhaemorrhage, intussusception and volvulus may occur in this abnormal sac. Thesecomplications are accompanied by bleeding. The bleeding can be demonstrated by theradionuclide tests already described. The presence of ectopic gastric mucosa can bedemonstrated by the "Tc01 pertechnetate imaging. About 1-2 mCi (37- 54 MBq) of theradiopharmaceutical is injected intravenously and abdominal images are obtained sequentiallyevery five minutes. Any spot of radioactivity appearing in the intestinal area should beinterpreted with reference to gastric activity. A positive scan usually shows a focal area ofincreased activity in the right lower quadrant of the abdomen. Barret's disease (gastricmucosa at the distal end of the oesophagus) can also be demonstrated by this technique.
Gastric Emptying
Gastric emptying can be studied either with liquids or with solids. The liquids leave thestomach faster than the solids. For the study of liquid phase about 500 /xCi of "Tcm sulphurcolloid or "Tc™ DTPA is dissolved in half a glass of milk and given to the patient to drinkafter overnight fasting. For solid phase study, the same amount of radio-pharmaceutical ismixed with about 150 grams of solid diet like mashed potatoes and given to the patient to eat.Radioactivity is recorded over the stomach for one hour with the patient lying supine undera computerized gamma camera. A region of interest over the stomach is fixed and timeactivity curve generated. The results are usually expressed as "Tlh emptying" or the timetaken by the gastric radioactivity to reduce to half the original value.
The technique is frequently useful in finding out the state of gastric mobility in systemicdiseases like diabetes mellitus and scleroderma and following surgical procedures such asvagotomy.
539

CHAPTER 28
Gastro-oesophagea! reflux
The same dose of radiopharmaceutical is used in liquid form as prescribed for the gastricemptying procedure. The radioactivity is recorded with the help of a gamma camera overthe gastro-oesophageal junction, with the patient lying supine. The study may continue forhalf an hour. Continuous recording on a computerized gamma camera or repeat images atfixed intervals may be obtained. The simplest procedure would be to see the appearance ofradioactivity in the distal part of the oesophagus in the images taken. Pressure may beapplied over the stomach to provoke reflux. Using regions of interest over the loweroesophagus and stomach the amount of reflux can be expressed in quantitative terms aspercentage of the gastric contents observed in the oesophagus. (Fig. 28.12).
Oesophageal transit.
The oesophageal transit time may be prolonged in diseases like achalasia, scleroderma,diffuse idiopathic oesophageal spasm and other non- specific motor disorders of theoesophagus. This parameter can be measured by using "Tcm sulphur colloid or "Tc1" DTPAin liquid form in the same dose as for gastric reflux. The patient drinks, in one swallow, theradioactive liquid while lying supine under a computerized gamma camera. In normalsubjects the radioactivity rapidly traverses the oesophagus and is not visualized by 4-10seconds after deglutition. In patients with motor disorders the activity can be seen in theoesophagus for a long time In spite of repeated attempts to swallow ( successive dryswallows). In such cases, the study should be prolonged and actual transit time determined,which may be as long as 15-30 seconds.
Immunoscintigraphy for colorectal cancer
The presence of carcinoembryonic antigen (CEA) in the colorectal cancer makes itpossible to localize such tumours with immunoscintigraphic technique by using "Tc™ labelledanti-CEA antibodies. This procedure has been found useful in the following situations.
(a) In cases of apparently curative resection of the colorectal cancer, the risein the serum levels of CEA precedes clinically evident relapse by severalmonths. Scintigraphy using labelled anti CEA antibodies may detect therecurrent sites at an early stage.
(b) In cases of recurrence, the immunoscintigraphy may reveal an extensivedisease and save the patient from second laparotomy.
(c) Recurrence in the scar may be detected and removed.
(d) An apparently benign rectal polyp may give a positive image andresected extensively like a malignant lesion.
540

LIVER AND GASTROINTESTINAL TRACT
During the last few years, the anti-CEA colorectal scintigraphy has been fairlystandardized and kits are now commercially available.
RADIOEWMUNOASSAYS
Tumour markers
Tumour markers are chemical substances mostly proteins, which are associated with thepresence of certain specific tumours in the body. These substances are usually present in theserum of normal subjects in low quantities. With the appearance of specific tumours, andsecretion of these substances in large quantities by the tumour cells, the serum levels of thesetumour markers rise above the normal values. Regression of the tumours results in theirreturn to normal values. Any increase in the level of a particular tumour marker after thepatient has been successfully treated would indicate relapse. There are two important tumourmarkers related to gastro-intestinal tract and the liver malignancies which can be measuredby RIA technique. These include the carcinoembryonic antigen and Alpha-fetoprotein.
Carcinoembryonic antigen (CEA)
This antigen is a glycoprotein with a molecular weight of approximately 180 000, whichis produced in appreciable amounts by the fetal large intestine. In adults, the CEA may bepresent in serum in small quantities usually not exceeding 4 ng/ml, but in the presence ofcertain malignancies the serum concentration may rise to high levels. The malignant tumoursof gastro-intestinal tract and other sites such as pancreas, ovary, breast, lung and uterus maybe associated with excessive serum levels or CEA. Very high levels of CEA are often anindication of spread of tumour to the liver.
CEA levels in serum may be raised in a number of non-malignant conditions. Forinstance about 14% of chronic cigarette smokers have elevated serum levels of CEA.Patients with some non-malignant tumours may also have raised levels. 15 - 20% of subjectswith inflammatory disorders such as ulcerative colitis, Crohn's disease, pancreatitis, acute andchronic liver diseases and lung infections show elevated serum levels of CEA. In spite of thefact that raised serum CEA is not specific to malignant tumours, very high concentrations e.g.above 20 ng/ml are highly suggestive of malignancy.
The CEA test is not useful as a screening procedure to detect cancer in generalpopulation or in an otherwise asymptomatic person. However, the CEA test is nowwell-accepted as the best non-invasive test which may be used to assist in the managementof patients with colorectal, breast, lung and other cancers.
The CEA serum assays by radioimmunometric techniques are being widely used even inthe developing countries by using commercially available kits. Whenever possible thepatients must be given the benefit of this useful investigation. It is possible to reduce the costof these assays by using bulk reagents.
541

CHAPTER 28
Alpha-fetoprotein (AFP)
Alpha-fetoprotein is a specific fetal serum alpha-globulin which consists of a singlepolypeptide chain and is composed of 96% protein and 4% carbohydrate. Initially during thefetal life the AFP is produced by the yolk sac and the fetal liver. By 13 weeks of gestation,the fetal plasma concentrations of AFP reach peak level of approximately 3000 /xg/ml whichis totally derived from the hepatic origin. Subsequently the AFP levels decline and reach alevel of approximately 80 /xg/ml at birth, and 0 - 2 0 ng/ml at the age of two years. Thislevel is maintained for the rest of the life.
Elevated levels of AFP are found in many patients of hepatocellular carcinoma andteratoma of the testis or the ovary. Measurement of the serum AFP levels can be useful inthe diagnosis and as a baseline information in these patients in following the response totreatment, which if successful results in decrease in AFP levels in serum. Similarly any riseof the AFP levels during follow-up would indicate a relapse or an uncontrolled disease.
AFP is not entirely specific to hepatocellular carcinoma and teratoma as elevated AFPlevels have been seen in liver cirrhosis and viral hepatitis probably associated with liverregeneration. However, persistently elevated level in excess of 1000 ng/ml are stronglysuggestive of presence of hepatocellular carcinoma or teratoma.
Hepatitis B surface antigen
Hepatitis B surface antigen (HBsAg) is a 22 nm particle, which can be produced by thevirus in the human body in large amounts. It is the outer coat of Hepatitis B virus (HBV)and is probably not infectious as such. Nevertheless, finding of HBsAg in the blood isregarded as an indicator of the presence HBV. All patients, who receive blood containingHBsAg, do not develop hepatitis, but the risk that they will develop hepatitis is very high.This close association between detection of HBsAg in the blood and the transmission ofhepatitis B led to the realization that all blood to be transfused should be screened for HBsAg.Thus a lot of work was done to develop the assay procedures for the detection of HBsAg.Since the use of screening procedures, the incidence or transfusion induced hepatitis hasdropped sharply. Moreover it has been established that a sensitive screening test likeRadioimmunoassay (RIA) can result in a very significant decrease of transfusion hepatitis.
There are several methods, which are employed for screening HBsAg from blood. Mostcommonly used are:
(1) Latex agglutination
(2) Red Cells agglutination
(3) Enzyme Immunoassay
(4) Radioimmunoassay
542

LIVER AND GASTROINTESTINAL TRACT
Radioimmunoassay is considered to be the most sensitive assay for the detection ofHBsAg, and is based on the principle that I25I conjugated to anti-HBs can act as a goodindicator for the presence of HBsAg in the antigen - antibody reaction. In this methodanti-HBs is coated on to a solid phase e.g. polystyrene beads. This is done by dipping thebeads overnight in anti-HBs solution buffered at pH 9.5. The specimen to be tested forHBsAg is poured on to the anti-HBs coated beads in a tube and incubated overnight at roomtemperature. After the incubation the beads are washed and I25I labelled anti-HBs is addedand incubated again for one to two hours depending upon the method used. At the end ofthis, the beads are washed again and binding of I25I is measured by a gamma counter. Thenumber of counts are directly proportional to the amount of HBsAg present in the sampletested. This is known as Sandwich method.
Routine screening of the patients with HBsAg resulted in the discovery that many peoplehave HBs in their blood. These people are healthy and are asymptomatic carriers of HBsAg.Test should be repeated to confirm the presence of HBsAg in their blood. If the antigenemialasts for more than six months and the persons are found positive for HBsAg in two serumsamples obtained six months or more apart, they should be considered as HBsAg chroniccarriers.
It has been found that the numbers of HBsAg chronic carriers are high among thefollowing groups:
(1) Drug Abusers
(2) Homosexuals
(3) Patients in renal dialysis and oncology units
(4) Recipients of blood transfusions
(5) Recipients of organ transplants
(6) Persons in lower socioeconomic areas.
Though the male population has been found to be positive for HBsAg twice as often asfemale population, it is essential that if the pregnant female is found positive for HBsAg, herneonate should be vaccinated within seven days after delivery so that the infant be protected.
In dialysis centres, separate machine should be used for HBsAg positive patients, so thatcross contamination be avoided.
HBsAg chronic carriers should be given the following instructions:
(1) The blood of the person should be checked every 6-12 months.
543

CHAPTER 28
(2) The person should be told NOT to donate blood.
(3) The person should not handle blood or blood products and his blood should beconsidered infectious and all precautions should be taken to prevent the spreadof the infection.
Although HBV (Dane Particles) has been shown to have other serological markers suchas anti-HBs, anti-HBc, HBeAg and anti-HBe, and the tests for these markers are alsoavailable, these markers are not used in the routine screening of the blood for hepatitis B.
It is worth mentioning here that an association exists between the presence of HBsAgcarrier state and cirrhosis of liver and to the eventual development of Primary HepatocellularCarcinoma. It has been found that the rate of development of Primary Hepatocellularcarcinoma is much higher among the people, who are HBsAg chronic carriers than those whoare negative for HBsAg.
544

LIVER AND GASTROINTESTINAL TRACT
ANTERIOR
RIGHTLATERAL
POSTERIOR
Fig. 28.1 Normal radiocolloid spleen / liver scan. Anterior, right lateraland posterior views.
545

CHAPTER 28
ANTERIOR
LATERAL
POSTERIOR
Fig. 28.2 Radiocolloid liver scan showing Cirrhosis of the liver. Notethe shrunken liver and marked 'spill-over' to the spleen andvisualization of the bone marrow.
546

LIVER AND GASTROINTESTINAL TRACT
ANTERIOR
RIGHTLATERAL
POSTERIOR
Fig. 28.3 RadiocoUoid liver scan of a patient with large liver abscess.
547

CHAPTER 28
ANTERIOR
RIGHTLATERAL
POSTERIOR
Fig. 28.4 Radiocolloid liver scan of a large hydatid cyst.
548

LIVER AND GASTROINTESTINAL TRACT
,:£i^MMl$^h
ANTERIOR
RIGHTLATERAL
POSTERIOR
Fig. 28.5 Radiocolloid liver scan showing multiple metastases fromprimary lung cancer.
549

CHAPTER 28
ANTERIOR
RIGHTLATERAL
•it
POSTERIOR
BFig. 28.6 A.
Fig. 28.6 B.
Radiocolloid liver scan shows no evidence of a focal defect.
Ultrasound examination of the same liver showing a focal lesion.
550

LIVER AND GASTROINTESTINAL TRACT
BFig. 28.7 A.
Fig. 28.7 B.
RadiocoUoid liver scan of a case of breast cancer showing a focaldefect in the upper medial part of the right lobe which wasconsidered to be a metastatic deposit.
Same patient. Ultrasound scan shows the lesion to be cystic.
551

CHAPTER 28
lit':.'
Fig. 28.8 A normal hepatobiliary study using "Tcm - HID A.
552

LIVER AND GASTROINTESTINAL TRACT
10 min 15 min
30 min
5 min
60 min
Fig. 28.9 Hepatobiliary study in an infant with biliary atresia. Notesatisfactory liver uptake and non-visualization of the gallbladder, bile ducts and duodenal loops. The entire activity isexcreted through the kidneys.
553

CHAPTER 28
ANTERIOR10 min
ANTERIOR30 min
ANTERIOR60 min iy«-•"'
Fig. 28.10 Hepatobiliary study showing a non-functioning gall bladder ina case of acute cholecystitis.
554

LIVER AND GASTROINTESTINAL TRACT
TRAMSAXIAL11- 83%
13
cTRANSAXIftL2O- 74X
COftONAL4 - Q7X
13 O- 88X1 O
5M 351229K
O
l oALEXANDER
3 - 87X1 O
5M 1751229K
0
5-loo:',l o
iM 31S1229K
1O 1
Fig. 28.11. SPECT imaging of liver The small lesion seen in the Coronal section wasnot detected in the planar images. Biopsy of lesion shows hepato cellularcarcinoma.
555

• * . , .
t-
CHAPTER 28
Fig. 28.12 Gastrooesophageal reflux study showing the filling of the lower half of theoesophagus with the regurgitant radioactive meal.
556