Embed Size (px)
Citation preview

1
Chapter 25Chapter 25Spinal TraumaSpinal Trauma
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ObjectivesObjectivesDescribe incidence, morbidity, mortality related to spinal Describe incidence, morbidity, mortality related to spinal injuryinjury
Predict mechanisms of injury likely to cause spinal injuryPredict mechanisms of injury likely to cause spinal injury
Describe anatomy and physiology of spine and spinal Describe anatomy and physiology of spine and spinal cordcord
Outline assessment of a patient with suspected spine Outline assessment of a patient with suspected spine injuryinjury
Distinguish between types of spine injuryDistinguish between types of spine injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
ObjectivesObjectivesDescribe prehospital assessment of spinal cord injuryDescribe prehospital assessment of spinal cord injury
Identify prehospital management of the patient with Identify prehospital management of the patient with spinal injuriesspinal injuries
Distinguish between spinal shock, neurogenic shock, Distinguish between spinal shock, neurogenic shock, and autonomic hyperreflexia syndromeand autonomic hyperreflexia syndrome
Describe selected nontraumatic spinal conditions and Describe selected nontraumatic spinal conditions and the prehospital assessment and treatment of themthe prehospital assessment and treatment of them
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
Sanders: Mosby's Paramedic Textbook, Revised 3rd Edition PowerPoint Lecture Notes
Chapter 25: Spinal Trauma

2
ScenarioScenarioIt is 0300 and pouring rain when you reach the It is 0300 and pouring rain when you reach the crumpled car in the ditch. It appears to have rolled crumpled car in the ditch. It appears to have rolled several times. It is uprightseveral times. It is upright——and empty. Your flashlight and empty. Your flashlight beam glances over your patient, a 20beam glances over your patient, a 20--yearyear--old man old man who is lying in the nearby brush moaning. He is prone, who is lying in the nearby brush moaning. He is prone, smells strongly of sour beer, and repeats, smells strongly of sour beer, and repeats, ““My neck, My neck, my neck.my neck.”” There is severe tenderness over his lower There is severe tenderness over his lower CC--spine area. You quickly determine that he has rapid, spine area. You quickly determine that he has rapid, shallow respirations; a weak, slow radial pulse; and no shallow respirations; a weak, slow radial pulse; and no movement of his arms or legs.movement of his arms or legs.
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
DiscussionDiscussionWhat is your first challenge in the management of this What is your first challenge in the management of this patient?patient?
What concerns do you have about his respiratory status?What concerns do you have about his respiratory status?
Why is his pulse slow and weak?Why is his pulse slow and weak?
What drugs would be indicated on this call?What drugs would be indicated on this call?
How will you answer when he asks, How will you answer when he asks, ““Why canWhy can’’t I move my t I move my legs?legs?””
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal TraumaSpinal TraumaCausesCauses
MVC (48%)MVC (48%)Falls (21%)Falls (21%)Penetrating injuries (15%)Penetrating injuries (15%)Sports injury (14%)Sports injury (14%)
40% of victims with neurological deficit will 40% of victims with neurological deficit will have permanent injuryhave permanent injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

3
Spinal Assessment CriteriaSpinal Assessment CriteriaAltered level of consciousnessAltered level of consciousness
Spinal pain or tendernessSpinal pain or tenderness
Neurological deficit or complaintNeurological deficit or complaint
Anatomical deformity of the spineAnatomical deformity of the spine
Alcohol or drugsAlcohol or drugs
Distracting injuryDistracting injury
Inability to communicateInability to communicate
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mechanism of InjuryMechanism of Injury
Classify mechanism of injury as:Classify mechanism of injury as:PositivePositiveNegativeNegativeUncertain Uncertain
Combine with clinical criteria for spinal injury Combine with clinical criteria for spinal injury to help identify situations in which spinal to help identify situations in which spinal immobilization is appropriateimmobilization is appropriate
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Positive MOIPositive MOIForces highly suggestive of spinal cord injuryForces highly suggestive of spinal cord injury
Requires full spinal immobilizationRequires full spinal immobilization
ExamplesExamplesHighHigh--speed motor vehicle crashesspeed motor vehicle crashesFalls >3x patientFalls >3x patient’’s heights heightViolent injuries occurring near patientViolent injuries occurring near patient’’s spine s spine Sports injuriesSports injuriesOther highOther high--impact situationsimpact situations
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

4
Positive MOIPositive MOI
In absence of signs and symptoms of SCI, some In absence of signs and symptoms of SCI, some medical direction agencies may recommend that medical direction agencies may recommend that a patient with a positive MOI not be immobilizeda patient with a positive MOI not be immobilized
Based on assessment when:Based on assessment when:Patient history is reliablePatient history is reliableThere are no distraction injuriesThere are no distraction injuries
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Negative MOINegative MOI
Force or impact suggests no potential for spinal Force or impact suggests no potential for spinal injuryinjury
If no SCI signs and symptoms, does not require If no SCI signs and symptoms, does not require spinal immobilizationspinal immobilization
Examples:Examples:Dropping an object on the footDropping an object on the footTwisting an ankle while runningTwisting an ankle while runningIsolated soft tissue injuryIsolated soft tissue injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Uncertain MOIUncertain MOIImpact or force involved in injury is unknown or Impact or force involved in injury is unknown or uncertainuncertain
Clinical criteria used to determine need for Clinical criteria used to determine need for spinal immobilizationspinal immobilization
ExamplesExamplesTripping or falling and hitting headTripping or falling and hitting headFalls 2Falls 2--4 ft4 ftLowLow--speed motor vehicle crashes (speed motor vehicle crashes (““fender bendersfender benders””))
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

5
Assessment of Uncertain MOIAssessment of Uncertain MOIEnsure patient is reliableEnsure patient is reliable
Calm, cooperative, sober, alert, and orientedCalm, cooperative, sober, alert, and oriented
Unreliable patientsUnreliable patientsAcute stress reactions Acute stress reactions Brain injuryBrain injuryIntoxicatedIntoxicatedAbnormal mental statusAbnormal mental statusDistracting injuriesDistracting injuriesProblems communicatingProblems communicating
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal ColumnSpinal Column
33 vertebrae33 vertebrae7 cervical7 cervical12 thoracic12 thoracic5 lumbar5 lumbar5 sacrum (fused)5 sacrum (fused)4 coccyx (fused)4 coccyx (fused)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal ColumnSpinal Column
Anterior spineAnterior spineVertebral bodiesVertebral bodiesIntervertebral disksIntervertebral disksAnterior and posterior Anterior and posterior longitudinal ligamentslongitudinal ligaments
•• Connect vertebral bodies Connect vertebral bodies anteriorly and inside canal anteriorly and inside canal
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

6
Spinal ColumnSpinal ColumnVertebraVertebra
Solid bodySolid body•• Bears weight of Bears weight of
vertebral columnvertebral columnPosterior and anterior Posterior and anterior archarchPosterior spinous Posterior spinous processprocessTransverse process (in Transverse process (in some vertebrae)some vertebrae)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal ColumnSpinal Column
Spinal cord lies in Spinal cord lies in spinal canalspinal canal
Spinal nerve roots Spinal nerve roots pass out through pass out through vertebral foramen vertebral foramen
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Adult SkullAdult Skull
Sits first cervical vertebra (C1) (atlas)Sits first cervical vertebra (C1) (atlas)
Second cervical vertebra (C2) (axis) and its Second cervical vertebra (C2) (axis) and its odontoid process allow head to move with odontoid process allow head to move with about 180about 180--degree range of motiondegree range of motion
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

7
Adult SkullAdult Skull
Cervical spine susceptible to injury due to:Cervical spine susceptible to injury due to:Weight and position of head in relation to Weight and position of head in relation to Thin neck and cervical vertebraeThin neck and cervical vertebrae
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cervical Spine InjuryCervical Spine Injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal InjurySpinal InjuryCausesCauses
Axial loadingAxial loadingFlexion, hyperextension, hyperrotationFlexion, hyperextension, hyperrotationExcessive lateral bendingExcessive lateral bendingDistractionDistraction
Stable and unstable injuries based on:Stable and unstable injuries based on:Extent of disruption to spinal structuresExtent of disruption to spinal structuresRelative strength of structures remaining intactRelative strength of structures remaining intact
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

8
Axial Loading Axial Loading
Direct forces transmitted along length of spinal Direct forces transmitted along length of spinal columncolumn
May produce compression fracture or a May produce compression fracture or a crushed vertebral body without SCIcrushed vertebral body without SCI
Commonly occur at T12 to L2Commonly occur at T12 to L2
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Flexion, Hyperextension, Flexion, Hyperextension, HyperrotationHyperrotation
Extremes may result in:Extremes may result in:FractureFractureLigamentous injuryLigamentous injuryMuscle injuryMuscle injury
Spinal cord injury when impingement into spinal Spinal cord injury when impingement into spinal canal by subluxation of one or more cervical canal by subluxation of one or more cervical vertebraevertebrae
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Lateral BendingLateral Bending
Excessive lateral bendingExcessive lateral bendingDislocations and bony fractures of cervical and Dislocations and bony fractures of cervical and thoracic spinethoracic spineSudden lateral impact moves torso sidewaysSudden lateral impact moves torso sideways
Head remains in place until pulled along by Head remains in place until pulled along by cervical attachmentscervical attachments
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

9
DistractionDistraction
Cervical spine suddenly stops while weight Cervical spine suddenly stops while weight and momentum of body pull away from itand momentum of body pull away from it
May result in tearing and laceration of spinal cordMay result in tearing and laceration of spinal cord
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Less Common Mechanisms Less Common Mechanisms
Other mechanisms of spine injuryOther mechanisms of spine injuryBlunt traumaBlunt traumaElectrical injuryElectrical injuryPenetrating traumaPenetrating trauma
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Classifications of Spinal InjuryClassifications of Spinal Injury
SprainsSprainsStrainsStrainsFracturesFracturesDislocationsDislocationsSacral fracturesSacral fracturesCoccygeal fracturesCoccygeal fracturesCord injuriesCord injuries
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

10
Spinal Injuries Spinal Injuries
Immobilize patients with:Immobilize patients with:Suspected spinal traumaSuspected spinal trauma
OROR
Signs and symptoms of SCISigns and symptoms of SCI•• Avoid unnecessary movement Avoid unnecessary movement
Unstable spine can be ruled out only by Unstable spine can be ruled out only by radiography or lack of any mechanism for radiography or lack of any mechanism for injury injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Assume Spinal InjuryAssume Spinal Injury
Significant trauma and Significant trauma and use of intoxicating use of intoxicating substancessubstancesSeizure activitySeizure activityPain or paresthesia in Pain or paresthesia in neck or armsneck or armsNeck tendernessNeck tendernessUnconsciousness Unconsciousness because of head injurybecause of head injury
Significant injury above Significant injury above clavicleclavicleFall more than three times Fall more than three times patient's heightpatient's heightFall and fracture of both Fall and fracture of both heels heels Injury from a highInjury from a high--speed speed motor vehicle crashmotor vehicle crash
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal InjurySpinal Injury
Damage further complicated by:Damage further complicated by:Patient's agePatient's agePreexisting bone diseasesPreexisting bone diseasesCongenital spinal cord anomalies Congenital spinal cord anomalies
Spinal cord neurons do not regenerate to any Spinal cord neurons do not regenerate to any great extentgreat extent
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

11
Hyperflexion Sprains and StrainsHyperflexion Sprains and Strains
Hyperflexion sprainsHyperflexion sprainsPosterior ligamentous complex tears Posterior ligamentous complex tears
Hyperextension strains (whiplash)Hyperextension strains (whiplash)LowLow--velocity, rearvelocity, rear--end automobile collisionsend automobile collisions
Local painLocal painSpasms of neck musclesSpasms of neck musclesNonradiating, aching soreness of neck or backNonradiating, aching soreness of neck or backTreat as cord injury until cleared by xTreat as cord injury until cleared by x--rayray
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Fractures and DislocationsFractures and Dislocations
Most frequently injured spinal regionsMost frequently injured spinal regionsC5C5--C7C7C1C1--C2C2T12T12--L2L2
WedgeWedge--shaped compression fractures and shaped compression fractures and "teardrop" fractures or dislocations common"teardrop" fractures or dislocations common
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
WedgeWedge--Shaped FracturesShaped FracturesHyperflexion injuryHyperflexion injury
Compressive force to Compressive force to anterior vertebral body anterior vertebral body stretches posterior ligament stretches posterior ligament complex complex
Industrial accidents, fallsIndustrial accidents, fallsMiddle or lower cervical Middle or lower cervical segments or at T12 and L1segments or at T12 and L1
Generally stable Generally stable
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

12
Teardrop Fractures and DislocationsTeardrop Fractures and Dislocations
Extremely unstable Extremely unstable
Severe hyperflexion and Severe hyperflexion and compression forcescompression forces
Motor vehicle crashesMotor vehicle crashes
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Sacral and Coccygeal FracturesSacral and Coccygeal Fractures
Most serious spinal injuries in cervical, Most serious spinal injuries in cervical, thoracic, and lumbar regionsthoracic, and lumbar regions
Patient may say, Patient may say, ““I broke my tailboneI broke my tailbone””Moderate pain from mobile coccyxModerate pain from mobile coccyx
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Sacral and Coccygeal FracturesSacral and Coccygeal Fractures
Fractures of S1 and S2 fairly commonFractures of S1 and S2 fairly commonMay compromise sacral nerves May compromise sacral nerves May result in loss of perianal sensory motor May result in loss of perianal sensory motor function and in bladder and sphincter disturbancesfunction and in bladder and sphincter disturbances
Sacrococcygeal joint may be injured from Sacrococcygeal joint may be injured from direct blows and fallsdirect blows and falls
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

13
Classification of Cord InjuriesClassification of Cord Injuries
Primary injuriesPrimary injuriesOccur at time of impactOccur at time of impact
Secondary injuriesSecondary injuriesOccur later due to:Occur later due to:
•• SwellingSwelling•• IschemiaIschemia•• Movement of bony fragmentsMovement of bony fragments
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cord InjuriesCord InjuriesConcussedConcussed
ContusedContused
CompressedCompressed
LaceratedLacerated
Severity of injuries depends on:Severity of injuries depends on:Amount and type of force Amount and type of force Duration of injuryDuration of injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cord LesionsCord Lesions
Lesions (transections) of spinal cord are Lesions (transections) of spinal cord are classified as:classified as:
CompleteCompleteIncompleteIncomplete
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

14
Complete Cord LesionsComplete Cord LesionsUsually spinal fracture or dislocationUsually spinal fracture or dislocation
Absence of pain, pressure, and joint sensationAbsence of pain, pressure, and joint sensation
Complete motor paralysis below injury Complete motor paralysis below injury
QuadriplegiaQuadriplegia•• Injury at cervical levelInjury at cervical level•• Loss of all function below injury site Loss of all function below injury site
Paraplegia Paraplegia •• Thoracic or lumbar level injuryThoracic or lumbar level injury•• Loss of lower trunk functionLoss of lower trunk function
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Complete Cord LesionsComplete Cord Lesions
Autonomic dysfunction may occur with Autonomic dysfunction may occur with complete cord lesions complete cord lesions
Manifestations of autonomic dysfunctionManifestations of autonomic dysfunctionBradycardia Bradycardia HypotensionHypotensionPriapismPriapismLoss of sweating and shiveringLoss of sweating and shiveringPoikilothermy Poikilothermy Loss of bowel and bladder controlLoss of bowel and bladder control
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Incomplete LesionsIncomplete LesionsCentral cord syndromeCentral cord syndrome
Seen with hyperextension or flexion cervical Seen with hyperextension or flexion cervical injuriesinjuriesGreater motor impairment of upper than lower Greater motor impairment of upper than lower extremitiesextremities
Signs and symptomsSigns and symptomsParalysis of armsParalysis of armsSacral sparingSacral sparing
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

15
Incomplete LesionsIncomplete LesionsAnterior cord syndromeAnterior cord syndrome
Usually flexion injuriesUsually flexion injuriesPressure on anterior spinal cord by ruptured Pressure on anterior spinal cord by ruptured intervertebral diskintervertebral disk
•• Fragments of vertebral body extruded into spinal canalFragments of vertebral body extruded into spinal canal
Signs and symptomsSigns and symptomsDecreased sensation of pain and temperature Decreased sensation of pain and temperature below lesionbelow lesionIntact light touch and position sensationIntact light touch and position sensationParalysisParalysis
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Incomplete LesionsIncomplete LesionsBrownBrown--SSééquard syndromequard syndrome
Hemitransection of spinal cordHemitransection of spinal cord•• Ruptured intervertebral diskRuptured intervertebral disk•• Encroachment on spinal cord by a fragment of vertebral Encroachment on spinal cord by a fragment of vertebral
bodybody
Pressure on half spinal cord results in:Pressure on half spinal cord results in:•• Weakness of upper and lower extremities on ipsilateral Weakness of upper and lower extremities on ipsilateral
sideside•• Loss of pain and temperature on contralateral sideLoss of pain and temperature on contralateral side
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Pharmacological TherapyPharmacological Therapy
Use in incomplete cord injury is very Use in incomplete cord injury is very controversialcontroversial
GlucocorticoidsGlucocorticoidsNaloxoneNaloxoneCalcium channel blockersCalcium channel blockersMethylprednisolone (SoluMethylprednisolone (Solu--Medrol)Medrol)
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

16
Assessment of Spinal Cord Injury Assessment of Spinal Cord Injury
After lifeAfter life--threatening injuries have been threatening injuries have been assessed and treatedassessed and treated
Priorities:Priorities:Scene surveyScene surveyAssess airway, breathing, and circulationAssess airway, breathing, and circulationPreserve spinal cord functionPreserve spinal cord functionAvoid secondary injury to spinal cordAvoid secondary injury to spinal cord
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Assessment of Spinal Cord InjuryAssessment of Spinal Cord Injury
Prevent secondary injury from:Prevent secondary injury from:Unnecessary movementUnnecessary movementHypoxemiaHypoxemiaEdemaEdemaShock Shock
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Prehospital GoalsPrehospital GoalsSuspect spinal injury:Suspect spinal injury:
Scene surveyScene surveyKinematicsKinematicsHistory of eventHistory of event
Early spinal immobilizationEarly spinal immobilization
Oxygen Oxygen
Correct volume deficitsCorrect volume deficits
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

17
Neurological ExaminationNeurological Examination
Neurological examNeurological examAt scene or en routeAt scene or en routeDocument findingsDocument findingsMotor and sensory findingsMotor and sensory findingsReflex responsesReflex responses
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
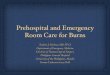
DermatomesDermatomesSpinal nerves (except Spinal nerves (except C1) have specific C1) have specific cutaneous sensory cutaneous sensory distributiondistribution
DermatomeDermatome is skin is skin surface area supplied surface area supplied by a single spinal nerveby a single spinal nerve
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
DermatomesDermatomesLandmarks for sensory Landmarks for sensory evaluationevaluation
C2 to C4: Around the C2 to C4: Around the neck and over anterior neck and over anterior chest to below clavicleschest to below claviclesT4: Nipple lineT4: Nipple lineT10: UmbilicusT10: UmbilicusS1: Soles of feetS1: Soles of feet
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

18
Reflex ResponsesReflex ResponsesSeldom evaluated Seldom evaluated prehospitalprehospital
Some indicate autonomic Some indicate autonomic injuryinjury
Babinski's signBabinski's signPlantar reflexPlantar reflexDorsiflexion of great toe Dorsiflexion of great toe with or without fanning of with or without fanning of toestoes
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Methods of EvaluationOther Methods of Evaluation
Visual inspectionVisual inspectionCord transection above C3 often results in Cord transection above C3 often results in respiratory arrestrespiratory arrestC4 lesions may cause paralysis of diaphragmC4 lesions may cause paralysis of diaphragmTransections at C5Transections at C5--C6 spare diaphragmC6 spare diaphragm
•• Permit diaphragmatic breathingPermit diaphragmatic breathing
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal InjurySpinal Injury
Absence of neurological deficits Absence of neurological deficits does notdoes not rule rule out spinal injuryout spinal injury
Ability to walk should Ability to walk should notnot be a factor in be a factor in determining need for spinal precautionsdetermining need for spinal precautions
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

19
Spinal ImmobilizationSpinal ImmobilizationPrimary goalPrimary goal
Prevent further injuryPrevent further injury
Treat spine as a long bone with a joint at either end Treat spine as a long bone with a joint at either end (the head and pelvis)(the head and pelvis)
Use complete spinal immobilizationUse complete spinal immobilization
Begins at initial assessmentBegins at initial assessment
Maintain until spine is immobilized on a long Maintain until spine is immobilized on a long backboardbackboard
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal Immobilization TechniquesSpinal Immobilization Techniques
When a possible or When a possible or potential spine injury potential spine injury recognized, manually recognized, manually protect head and neckprotect head and neck
Maintain in line with long Maintain in line with long axis of bodyaxis of body
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Manual InManual In--Line Immobilization from the FrontLine Immobilization from the Front
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

20
Log RollLog Roll——Prone PatientProne PatientIn one move, patient is rotated away from prone position.
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Manual InManual In--Line Immobilization from the FrontLine Immobilization from the Front
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Log RollLog Roll——Supine PatientSupine PatientRescuer 1 at head, rescuers 2 and 3 at midthorax and knees
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

21
Log RollLog Roll——Supine PatientSupine PatientRescuer 4 manages spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Log RollLog Roll——Supine PatientSupine PatientMaintain immobilization and roll in one move
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Log RollLog Roll——Supine PatientSupine PatientIn one move, rescuers log-roll and center patient on spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

22
Log RollLog Roll——Prone PatientProne PatientRescuer 1 provides in-line stabilization; prepares for rotation
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Log RollLog Roll——Prone PatientProne PatientIn one move, rescuers log-roll and center patient on spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Rigid Cervical CollarRigid Cervical Collar
Protects cervical spine from compressionProtects cervical spine from compressionReduces movement and some range of motion of Reduces movement and some range of motion of headheadDoes not provide adequate spinal immobilizationDoes not provide adequate spinal immobilization
Use with manual inUse with manual in--line stabilization or line stabilization or immobilization by a suitable deviceimmobilization by a suitable device
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

23
Rigid Cervical CollarsRigid Cervical CollarsMany sizes (or are adjustable)Many sizes (or are adjustable)
Appropriate size reduces flexion or hyperextension Appropriate size reduces flexion or hyperextension
Must not:Must not:Inhibit ability to open mouth or clear airway Inhibit ability to open mouth or clear airway Obstruct airway or ventilationsObstruct airway or ventilations
Apply after head is in neutral inApply after head is in neutral in--line positionline position
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Cervical Collar ApplicationCervical Collar Application
Rescuer 1 maintains inRescuer 1 maintains in--line stabilizationline stabilization
Rescuer 2 positions and Rescuer 2 positions and secures collarsecures collar
Rescuer 1 maintains Rescuer 1 maintains support until patient has support until patient has been secured to boardbeen secured to board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Short Spine BoardsShort Spine BoardsSplint cervical and thoracic spineSplint cervical and thoracic spine
Vary in designVary in design
Spinal immobilization for patient in a sitting Spinal immobilization for patient in a sitting position or a confined spaceposition or a confined space
After short spine board has been applied, After short spine board has been applied, patient is transferred to a long spine boardpatient is transferred to a long spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

24
KED ApplicationKED Application
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Rapid ExtricationRapid Extrication
Steps vary depending on:Steps vary depending on:Size and make of vehicleSize and make of vehiclePatientPatient’’s location inside vehicles location inside vehicle
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Rapid ExtricationRapid ExtricationRescuer 1 maintains inRescuer 1 maintains in--line stabilizationline stabilization
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

25
Rapid ExtricationRapid ExtricationRescuer 2 supports Rescuer 2 supports midthorax as rescuer 3 midthorax as rescuer 3 frees lower extremitiesfrees lower extremities
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Rapid ExtricationRapid ExtricationPatient lowered onto Patient lowered onto long spine boardlong spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Rapid ExtricationRapid Extrication
Patient centered and Patient centered and secured on spine boardsecured on spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

26
Rapid ExtricationRapid Extrication——2 Rescuers2 Rescuers
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Rapid ExtricationRapid Extrication——2 Rescuers2 Rescuers
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Long Spine BoardLong Spine Board
Available in a variety of types:Available in a variety of types:Plastic and synthetic spine boardsPlastic and synthetic spine boardsMetal alloy spine boardsMetal alloy spine boardsVacuum mattress splintsVacuum mattress splintsSplit litters (scoop stretchers) that must be used Split litters (scoop stretchers) that must be used with a long spine boardwith a long spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

27
Long Spine BoardLong Spine Board——Supine PatientSupine Patient
Immobilize torso to a long spine board before Immobilize torso to a long spine board before immobilization of head immobilization of head
Torso must not be allowed to move up, down, Torso must not be allowed to move up, down, or to either sideor to either side
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Long Spine BoardLong Spine Board——Supine PatientSupine Patient
Place straps at:Place straps at:Shoulders or chest Shoulders or chest Around midtorsoAround midtorsoAcross iliac crests to prevent movement of lower Across iliac crests to prevent movement of lower torsotorso
After immobilization of torso, immobilize After immobilization of torso, immobilize head and neckhead and neck
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Long Spine BoardLong Spine Board——Supine PatientSupine Patient
Padding added as Padding added as needed before securing needed before securing headhead
Padding (if needed) Padding (if needed) should be firm and should be firm and extend full length and extend full length and width of the torso from width of the torso from the buttocks to the top the buttocks to the top of the shouldersof the shoulders
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

28
Long Spine BoardLong Spine Board——Supine PatientSupine Patient
Children have Children have proportionally larger proportionally larger headsheads
May require padding May require padding under the torso to allow under the torso to allow head to lie in a neutral head to lie in a neutral positionposition
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Long Spine BoardLong Spine Board——Supine PatientSupine PatientSecure head to device
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Long Spine BoardLong Spine Board——Supine PatientSupine Patient
Secure forehead across Secure forehead across supraorbital ridgesupraorbital ridge
Secure lower head Secure lower head across front of cervical across front of cervical collarcollar
Secure legs with two or Secure legs with two or more straps above and more straps above and below kneesbelow knees
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

29
Long Spine BoardLong Spine Board——Standing PatientStanding PatientRescuer 1 maintains manual inRescuer 1 maintains manual in--line stabilization; rescuers 2 and 3 support patient;line stabilization; rescuers 2 and 3 support patient;
Patient is lowered onto long spine board for further immobilizatPatient is lowered onto long spine board for further immobilizationion
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Immobilizing Pediatric PatientsImmobilizing Pediatric Patients
Prehospital carePrehospital careManual inManual in--line line immobilizationimmobilizationRigid cervical collarRigid cervical collarSpinal immobilization Spinal immobilization device device
Adult long spine Adult long spine boards may be usedboards may be used
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Manual InManual In--Line ImmobilizationLine Immobilization
Apply without tractionApply without traction
Use only enough tension to relieve weight Use only enough tension to relieve weight of head from cervical spineof head from cervical spine
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

30
Manual InManual In--Line ImmobilizationLine ImmobilizationDo notDo not move head to inmove head to in--line position if:line position if:
Resistance to movementResistance to movementNeck muscle spasmNeck muscle spasmIncreased painIncreased painPresence or increase in neurological deficits Presence or increase in neurological deficits during movement during movement Compromise of airway or ventilationCompromise of airway or ventilationSevere misalignment of headSevere misalignment of head
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
HelmetsHelmets
Helmets protect head and brain, not neckHelmets protect head and brain, not neckLeaves cervical spine vulnerable to injuryLeaves cervical spine vulnerable to injury
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Types of HelmetsTypes of Helmets
FullFull--face or openface or open--face designsface designsMotorcycling, bicycling, rollerblading, and other Motorcycling, bicycling, rollerblading, and other activitiesactivities
Helmets designed for sports such as football Helmets designed for sports such as football and motocrossand motocross
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

31
Helmet RemovalHelmet Removal
If helmet removal is needed:If helmet removal is needed:Athletic trainers may have special equipment to Athletic trainers may have special equipment to remove faceremove face--pieces pieces Easier access to airwayEasier access to airwaySports gear (shoulder pads) could compromise Sports gear (shoulder pads) could compromise spine if helmet is spine if helmet is
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Helmet RemovalHelmet Removal
Helmet removal is controversial Helmet removal is controversial Guided by medical directionGuided by medical direction
FullFull--face helmets are removed in the fieldface helmets are removed in the fieldPermits access to airwayPermits access to airwayAllows assessment for hidden bleeding or injuriesAllows assessment for hidden bleeding or injuries
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Helmet RemovalHelmet Removal
Immobilize helmet and Immobilize helmet and head in inhead in in--line positionline position
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

32
Helmet RemovalHelmet Removal
Spread side of helmet Spread side of helmet away from head and away from head and earsears
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Helmet Removal Helmet Removal
Rotate helmet to clear Rotate helmet to clear nose and remove from nose and remove from head in straight linehead in straight line
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Helmet RemovalHelmet Removal
After removal of helmet, After removal of helmet, apply inapply in--line line immobilization and rigid immobilization and rigid cervical collarcervical collar
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

33
Spinal Immobilization in Diving AccidentsSpinal Immobilization in Diving Accidents
Most diving accidents cause injury to head, Most diving accidents cause injury to head, neck, and spineneck, and spine
Patient in water:Patient in water:Ensure scene and personal safetyEnsure scene and personal safetyRescuers trained in water rescue should enter Rescuers trained in water rescue should enter waterwater
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal Immobilization in Diving AccidentsSpinal Immobilization in Diving Accidents
Float supine patient to shallow area:Float supine patient to shallow area:No unnecessary movement of spineNo unnecessary movement of spine
Approach prone patient from top of head:Approach prone patient from top of head:Carefully turn supine and assess airway and Carefully turn supine and assess airway and breathingbreathingRescue breathing may be initiated in waterRescue breathing may be initiated in water
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal Immobilization in Diving AccidentsSpinal Immobilization in Diving Accidents
Rescuer 2 slides long spine board or rigid device under Rescuer 2 slides long spine board or rigid device under patientpatient
Rescuer 1 supports head and neck without flexion or extensionRescuer 1 supports head and neck without flexion or extensionRigid cervical collar is appliedRigid cervical collar is appliedMaintain manual inMaintain manual in--line immobilizationline immobilization
Float immobilization device to edge of water and lift outFloat immobilization device to edge of water and lift out
Immobilize patient on long spine boardImmobilize patient on long spine board
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

34
Extrication of a Diving Accident VictimExtrication of a Diving Accident Victim
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal ShockSpinal ShockTemporary loss of spinal cord function distal Temporary loss of spinal cord function distal to injuryto injury
Flaccid paralysisFlaccid paralysisLoss of autonomic functionLoss of autonomic function
Avoid secondary injury Avoid secondary injury OxygenOxygenTrendelenburgTrendelenburgIV crystalloidsIV crystalloids
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Neurogenic HypotensionNeurogenic HypotensionBlockade of vasoregulatory fibers, motor fibers, and Blockade of vasoregulatory fibers, motor fibers, and sensory fiberssensory fibers
RareRare
Hypotension Hypotension
BradycardiaBradycardia
Warm, dry skinWarm, dry skin
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

35
Autonomic Hyperreflexia SyndromeAutonomic Hyperreflexia Syndrome
Chronic SCI with injuries at T6 or aboveChronic SCI with injuries at T6 or above
Distended bladder or rectum initiatesDistended bladder or rectum initiatesHypertensionHypertensionHAHABlurred visionBlurred visionSweatingSweatingNauseaNauseaBradycardiaBradycardia
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Low Back Pain (LBP)Low Back Pain (LBP)
Affected areaAffected areaBetween lower rib cage and gluteal musclesBetween lower rib cage and gluteal musclesMay radiate to thighsMay radiate to thighs
Risk factorsRisk factorsRepetitive liftingRepetitive liftingVibrations from machineryVibrations from machineryOsteoporosisOsteoporosis
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Low Back PainLow Back Pain——CausesCauses
TumorsTumors
Disk prolapseDisk prolapse
BursitisBursitis
SynovitisSynovitis
Degenerative joint Degenerative joint diseasedisease
Abnormal joint diseaseAbnormal joint disease
Inflammation from Inflammation from infectioninfection
FracturesFractures
Ligament strainsLigament strains
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

36
Degenerative Disk DiseaseDegenerative Disk Disease
Common >50 y/oCommon >50 y/o
CausesCausesAlterations in tissue of intervertebral disks that Alterations in tissue of intervertebral disks that occur with agingoccur with agingNarrowing of disk results in variable segmental Narrowing of disk results in variable segmental instability and occasional low back paininstability and occasional low back pain
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
SpondylosisSpondylosis
Defect of lamina or vertebral archDefect of lamina or vertebral archUsually lumbar spine between superior and inferior Usually lumbar spine between superior and inferior articulating facetsarticulating facetsRotational stress fractures common at affected siteRotational stress fractures common at affected siteHeredity significant factor Heredity significant factor
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Herniated Intervertebral DiskHerniated Intervertebral DiskTear in posterior rim of capsule encloses gelatinous Tear in posterior rim of capsule encloses gelatinous center of diskcenter of disk
Rupture of disk by:Rupture of disk by:TraumaTraumaDegenerative disk diseaseDegenerative disk diseaseImproper lifting (most common)Improper lifting (most common)
Disks commonly affected:Disks commonly affected:L5L5--S1 and L4S1 and L4--L5L5Occasionally C5Occasionally C5--C6 and C6C6 and C6--C7C7
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

37
Spinal Cord TumorsSpinal Cord TumorsMay develop from:May develop from:
Cord compressionCord compressionDegenerative changes in bones and jointsDegenerative changes in bones and jointsInterruption in cordInterruption in cord’’s blood supplys blood supply
Classified by cell type, growth rate, and Classified by cell type, growth rate, and structure of originstructure of origin
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Spinal Cord TumorsSpinal Cord TumorsSigns and symptoms depend on tumor type and Signs and symptoms depend on tumor type and locationlocation
May include:May include:Temperature dysfunctionTemperature dysfunctionSensory changesSensory changesOther abnormalitiesOther abnormalitiesParesisParesisSpasticitySpasticityPainPainBilateral or asymmetric motor dysfunctionBilateral or asymmetric motor dysfunction
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Nontraumatic Spinal ConditionsNontraumatic Spinal Conditions
Assessment and management are based on:Assessment and management are based on:PatientPatient’’s chief complaints chief complaintPhysical examinationPhysical examinationEvaluation of associated risk factorsEvaluation of associated risk factors
Common signs and symptomsCommon signs and symptoms
Care must be taken to decrease pain and discomfortCare must be taken to decrease pain and discomfortFull spinal immobilization is not required unless condition is tFull spinal immobilization is not required unless condition is the he result of traumaresult of trauma
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.

38
ConclusionConclusionEducation in injury prevention, prehospital Education in injury prevention, prehospital
assessment, and proper handling and assessment, and proper handling and transportation of patients with spinal injury transportation of patients with spinal injury
can decrease mortality and morbidity.can decrease mortality and morbidity.
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Questions ?Questions ?
Copyright © 2007, 2006, 2001, 1994 by Mosby, Inc., an affiliate of Elsevier Inc.
Mosby, Inc. items and derived items © 2007, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.