Embed Size (px)
Citation preview
GITT Implementation Manual 2012
Implementation Chapter 2 - 1
Chapter 2: Developing an Action Plan for GITT
A. Purpose To help you bring together the human, financial, and material resources needed to replicate GITT. B. Objectives After reviewing this chapter, you will be able to:
• Clarify your vision for improved geriatric interdisciplinary team training at your institution • Build support among key personnel (administration, faculty) for replicating GITT • Create a core team to replicate GITT
C. GITT Materials
• Sample GITT Budget • Sample Scripted GITT Presentation for Faculty Meetings • Worksheet Defining Your Vision for Improved Geriatric Care through • Interdisciplinary Teams • Worksheet Support for GITT • Worksheet Creating the GITT Team
Introduction
The purpose of this chapter is to help sites develop an action plan for implementing GITT. We start by describing some of the lessons learned from the GITT programs and the requisite steps that were discovered to implement team training effectively in the academic environment.
Factors Critical to Develop a Successful GITT Program While academic institutions often create excellent curricula, a variety of other factors are also important when trying to develop a program that produces change in didactic curricula and clinical practice. While the major points are identified using a variety of models, we use the model developed by the Education Development Center, Inc.,1 to point out factors that implementing sites should consider when moving toward a program such as GITT. A Clear Vision
Institutions should have a strong and identifiable interest in trying to replicate the GITT program and agreement among the affected faculty as to how the goals will take place.
GITT Implementation Manual 2012
Implementation Chapter 2 - 2
National Program/Movement Institutions should recognize that they are part of a national movement and that there are national experts who can assist them as they replicate GITT.
Leadership Skills
Strong leadership must be ensured across all of the disciplines involved and faculty should have a strong background and expertise in geriatric teaming.
Data-Driven Decision Making
Institutions should consider, at the outset, how they would evaluate the program and how to use data to inform future program corrections and enhancements.
Critical Mass
Institutions must consider how they will generate a critical mass of physicians, nurses, and social workers (as a minimum) to promote and publicize the GITT program.
Clinically Based Team Education and Ongoing Mentoring
Sites should consider ways to make their team education clinically based in order to reflect the realities of clinical care and develop ongoing coaching in the academic environment to ensure that the other aspects of academic culture do not override the lessons learned in GITT.
Adaptation to Local Concerns
Institutions should consider adapting the approach and materials, including the models of team training and curricula, to make them their own and continually improve the materials to meet their local needs.
Administrative and Management Support
Early, ongoing, and visible administrative support is key to an effective GITT program replication. Sites should consider the availability of this support as soon as implementation is considered.
Attention to External Forces
Sites should consider how to mesh GITT program activities with what is happening politically, economically, and socially at the national and local levels in order to leverage external forces as supports rather than barriers to program implementation.
Dedicated Time and Resources
Sites should be clear on the amount of time and resources that will be necessary to replicate GITT.
As future GITT sites think about how the program fits with the goals of their institution(s), faculty will need to assess the extent to which their departments possess these factors and are poised for GITT implementation. The first step in developing a GITT program is defining the vision for improved geriatrics and interdisciplinary team training.
Defining Your Vision Having recognized the changing values in academic curricula and recognizing the need to change in response to these forces, a site considering implementing an interdisciplinary team training program must identify which specific skills are needed by students to meet the new needs. Teams teach providers, especially physicians, that they do not have to be all things to all people. Interdisciplinary team training provides participants with the opportunity to learn the skills and knowledge other disciplines bring to the clinical team, as well as to reaffirm their roles on the clinical team. In this way, clinicians learn the scope of practice for other professionals and that these professionals are also responsible for patients.

GITT Implementation Manual 2012
Implementation Chapter 2 - 3
Dr. Steven Rothschild, a residency director from the Rush GITT in Chicago, says that teams help physicians learn what they do best and allow others to do what they do better. Interdisciplinary learning should be targeted toward this goal. But, a variety of additional skills and can be taught in interdisciplinary teams:
• Coordination of complex clinical care • Communication • Leadership • Geriatric knowledge • Cultural competency • Patient-centered Care
A GITT curriculum could enhance these areas and more. One caveat is important, however. If the university has little in the way of geriatric curriculum, a site will need to address this deficit first. The GITT program and materials assume that faculty who want to add teaming to their skill bank are already prepared to teach the geriatric content as it relates to their own profession. Without this base of clinical knowledge, students are unlikely to integrate team learning into their professional activities. The worksheet “Defining Your Vision for Improved Geriatric Care through Interdisciplinary Teams” at the end of this chapter may help you to define and clarify your vision.
Building Support Across the University To develop GITT, a site must have an idea of how to enhance interdisciplinary interaction across the university and a structure to operationalize relations among different schools or departments such as medicine, social work, nursing, and others. Since few universities have a commitment to interdisciplinary collaboration, it is likely that in developing a GITT program, you will be forging a new model for clerkship or clinical rotation. As such, it is essential to involve academic, clinic, and system administrators in the early planning of a GITT program and obtain their support and interest. Organizational support at the highest levels, including support of deans across schools prior to program development, is essential to program success. Furthermore, planning should also include consideration of sustainability of the program over time. GITT sites found that a lack of consideration of sustainability as the program was being developed hindered both the development of the program and the ability of the program to recruit interested students.
The Program Champions Critical to the success of a GITT program is the identification of a program champion. While it could be that only one program champion directs the GITT program across schools or departments within the university, the eight GITT sites found that the program was more effective when a program included one champion per discipline. In effect, a program aimed at developing interdisciplinary team knowledge required an interdisciplinary team to develop the program and make it work across the university. The role of the program champion is more than just acting as a figurehead or a cheerleader. Each participating academic discipline requires a champion with primary authority or the ability to significantly influence curriculum and practicum requirements. Champions need to be of a high enough level within their own school to get the buy-in needed at the faculty and dean level to ensure that necessary program changes will occur. The GITT programs that had non-tenured faculty as champions were generally not as successful because the faculty member did not have the authority to commit students to participate and was not secure enough in his/her position to command the needed respect from other departments. Generally, it is also easier if the champion is associated with geriatrics. Combining carefully developed resources on geriatric skills increases the likelihood that GITT will be included in crowded curricula especially for medicine. Moreover, the champion needs to know how to package geriatric resources in a user-friendly fashion so they can be adapted to varying learning situations.
GITT Implementation Manual 2012
Implementation Chapter 2 - 4
Ensuring Dean/Program Director Support
Administrative and management support is critical to a successful GITT program. Support from deans and program directors enable system changes and resources to be redirected to GITT activities. Program champions can convince deans and program directors to support GITT by demonstrating to them how GITT meets the changing needs of the students, the larger health care environment, and the move toward more effective academic programs. In effect, show the deans that by instituting GITT, their school is riding the wave of change. The scripted “GITT Presentation for Faculty Meetings” provides an outline of a sample presentation to help garner support. Support from deans and program directors, however, means nothing if that support is not demonstrated through action. Champions should encourage deans to show support by:
• Announcing the program at faculty meetings • Sending encouraging notes to faculty about participation in GITT • Attending and speaking at GITT presentations • Asking trustees for a public expression of endorsement for the program • Arranging for workload reductions to enable faculty to develop the program and recruit the
appropriate students
Creating the GITT Team: Partnering Across Disciplines in the University
Creating the GITT team requires more than regular meetings of the individual disciplinary champions. The GITT team needs to involve the champions as well as faculty and administrators throughout each school. Steering committees were valuable at every GITT site for encouraging the development of new ideas, increasing communication across disciplines, and simply organizing the program. However, like all teams, each GITT steering committee needed to create its own norms, standards, and operating rules. The closer the team modeled the values of interdisciplinary cooperation — for instance, by rotating meeting sites and leadership roles — the more the steering committee was able to accomplish institutional change. Additionally, routine, predictable discussion of the program was required during program development and initial implementation to ensure that all participants felt included in the group and up-to-date on the program’s progress. Some GITT sites created subcommittees with operational managers to work out course content, clinical practicum problems, and other logistical barriers. These subcommittees reported their recommendations back to the steering committee for approval. The team process of meeting to discuss and work out the details benefited the overall GITT program across the university. All of the GITT programs thought the process of meeting, as a GITT steering committee, was essential to implementing changes in both the institution and the community. The worksheet, “Creating the GITT Team,” may help you to identify appropriate members for the GITT team. Steering Committee Work The activities of the steering committee and subcommittees revolved mainly around curriculum content, scheduling, and other logistical aspects. For instance, the inability to schedule students to attend a common didactic across disciplines or the inability to get students from multiple disciplines into a common practicum site, posed major barriers to accomplishing the goals of GITT. Steering committees or subcommittees must also determine which members will attend the curriculum committees of each different school and how to demonstrate that common coursework will meet the curricular requirements of outside agencies. Sites often found that attendance at curriculum committee meetings of all three disciplinary champions was an asset to smooth committee acceptance.

GITT Implementation Manual 2012
Implementation Chapter 2 - 5
Different disciplines can also help each other obtain access to the various clinical practicum settings. For instance, one site may commonly work with one discipline. But with a team process, the initial discipline can help to leverage their relations with the site and expand the opportunities for other disciplines to participate at that site. New sites should recognize, however, that not all GITT programs were successful at getting medicine, nursing, and social work rotations at all team-training sites. For those programs, the didactic component then took on a heightened importance for ensuring that students learned to work with all three disciplines. Changes in the Steering Committee Mission over Time After program development and initial implementation, the steering committee’s mission changes. Astute managers, along with the committee, need to decide what the group wants to achieve -- if anything -- in the future. This time may be the opportunity to remind health science chancellors and clinical administrators of the successful model. Can the GITT experience parlay into a larger institutional commitment to inter-disciplinary education or just incremental changes in the program? The networking function of the group is another important benefit to the members. GITT programs found that steering committee membership helped to encourage additional cross-fertilization of ideas and projects beyond those contemplated by the GITT program. However, steering committees need to remember that maintaining members’ interest and involvement is essential for functional meetings. Membership for busy people is best maintained through short, well-structured meetings will a clear agenda and defined outcomes.
Acquiring Administrative Support Successful GITT programs were those programs in which administrative commitment to the program was early, ongoing, and publicly visible. Successful sites had champion/leaders publicizing the program and getting people involved. However, integrating academic and clinical training across multiple disciplines also requires substantial administrative coordination that will not occur unless it is explicitly someone’s responsibility. The operational and programmatic activities required of an interdisciplinary team training program include:
• Faculty, preceptor, and trainee recruiting • Curriculum development • Classroom and clinical scheduling • Keeping in contact with training sites • Evaluating program effectiveness
A sample worksheet, “Building Support for GITT,” may help you identify what administrative activities your site will need. While some of these activities can be directed by the steering committee, many of these activities necessitate having a program coordinator. Acquiring the administrative support of a program coordinator helps to further demonstrate the importance of the GITT program within and outside of the school. Moreover, it makes one individual directly responsible for key activities. GITT sites found that having an identified program coordinator:
• Committed the institution and its resources to carrying out the changes in planning, scheduling, and monitoring
• Clarified the faculty involvement and role • Made someone responsible for noting progress and conveying that progress to senior
administrators and to other stakeholders and surrounding programs • Clearly defined roles, responsibilities, and communication channels amongst the schools
GITT Implementation Manual 2012
Implementation Chapter 2 - 6
• Demonstrated a commitment of staff and fiscal resource support
The GITT Program Coordinator The GITT program coordinator is probably the person most critical to the success and adaptation of GITT. In the role of coordinator, he/she should be a champion for the program: the coordinator introduces the new program, ushers it through implementation, and sees that GITT becomes a part of ongoing curricula in the different departments. Moreover, the coordinator provides a structure for leadership and the coordination necessary to address logistical barriers. The coordinator can interface with the administrators who set up clinical practica and create the practica agreements with the settings. Without a program coordinator interfacing with these individuals to ensure their support, a program is unlikely to successfully place its students in interdisciplinary settings and, thus, will not meet its objectives. In essence, the program coordinator is the hub of the GITT project and makes possible the changes that lead to improvements in geriatric care. Ideally, this person should be a full-time, technically competent, respected, and committed geriatric leader who can galvanize the interest and involvement of others in his/her institution. We have found that GITT coordinators must possess certain characteristics to ensure that GITT is implemented successfully. Some of the following characteristics are not exclusive to GITT but are qualities any program leader should possess:
• Must have organizational/leadership support during implementation • Must have key administrative direction and coordination with good access to organizational
leadership • An effective coordinator is a positive risk-taker. He/she possesses the confidence to act • An effective coordinator is a good manager as well as a leader -- he/she is able and willing to
delegate tasks and responsibilities • An effective coordinator is intelligent and respected by faculty and staff -- he/she is well educated
(master’s prepared at a minimum) and has excellent clinical knowledge and skills in geriatric care • An effective coordinator is a good communicator -- he/she can write and speak well, possessing
the ability to persuade as needed • An effective coordinator is a good teacher -- he/he is willing to share knowledge to empower
others • An effective coordinator is trustworthy -- he/she is the kind of person who requires little direct
supervision, demonstrates initiative, and is accountable
Allocating Human and Material Resources The clinical practical model used in the GITT program has a high teacher/student ratio that is hard to sustain without external support. Small groups are most effective for teaching the content, but that requires the commitment of staff and resources. An infrastructure is required to ensure that faculty makes time in their schedules to teach in the didactic portion and to ensure that preceptors are available to take on students and are prepared to teach teaming skills in addition to other clinical information. The GITT Budget In most cases, you don’t need to hire additional staff to implement GITT. Current faculty/staff will have the educational skills necessary to implement the program. On the other hand, GITT does require careful allocation of staff time and material resources. The original GITT sites found that if they secured these resources up front, they were less likely to encounter problems when implementing GITT activities. A sample GITT budget is included in the appendix of this chapter. A GITT coordinator will need time from current responsibilities to get the program going. For the first year, it may take a 50%-75% coordinator effort, until the program is in place. GITT leaders should not underestimate the amount of time it takes to supervise and advocate for GITT. Other members of the GITT team will also require support for the time they spend on the project. It is likely, however, that the
GITT Implementation Manual 2012
Implementation Chapter 2 - 7
GITT responsibilities blend into existing roles. For example, a social worker on a clinical unit may join a GITT team and act as a student preceptor. This may, in fact, streamline communication with other disciplines and create time savings. A faculty member who teaches the clinical portion of a nursing course may find the GITT experience serves as a perfect experience to meet other course requirements and/or objectives. All disciplines involved need to consider the amount of time that must be made available for participation in GITT. Are there funds available to support GITT? From what source? Will trainees be able to attend GITT classes during their regular day or will they need to participate on their own time? How do departments share costs to pay preceptors as appropriate? If faculty from outside the institution must be hired, that may also be an additional cost. Schools and departments will also need to consider revenue. In some universities, individual schools receive a portion of operating funds for each course that is taught or for each enrolled graduate. But if students attend a course in another school, does the revenue follow the student or do the schools share the revenue? Although the mechanisms may differ, such revenue aspects may have a substantial influence on overall program costs. Sample GITT Budget In creating a GITT budget, program champions and coordinators should consider costs in the following areas:
• Personnel (including time for the program coordinator) • Faculty time buyout • Preceptor payment • Training materials for faculty/preceptors (photocopies, etc.) • Food for meetings, etc.
A sample budget is included in the appendix of this chapter.
Promoting and Publicizing GITT Even before the GITT program formally begins, you will need to promote awareness of the program as a whole to make it more likely that faculty and students will want to participate. You can use the following methods to get people talking about the program. A sample scripted faculty presentation is included in the appendix of this chapter.
• Brief announcements at faculty meetings • E-mail announcements that inform others of the program progress with contact numbers for
further information • Posters displaying relevant information about GITT posted in appropriate places • Memos or flyers inserted in mailboxes or at regular staff mailings • Distribution of articles on GITT models of training and care • Announcement of stipends for GITT trainees
In the early support-building phase, it is best to operate by a principle of inclusion. Anyone and everyone who can promote or impede the goals of the program should know about it and be invited to participate, as early as possible. The best way to do this is to make presentations to key audiences about the importance of participating in the GITT program. The original GITT implementation sites found these key people included the following individuals:
• Deans and program directors • Heads/chiefs of services • Key geriatric faculty

GITT Implementation Manual 2012
Implementation Chapter 2 - 8
• Directors of continuing education • Student leadership groups
Converting the Skeptics
In the early support-building phase, you will also need to consider the potential sources of opposition to the program. You may be able to identify some of these on your own; others will emerge as you begin the program development process. In either case, it is important to be willing to listen and be responsive to these people's concerns. Curricula are very full and faculty perceives new courses as a threat to existing courses. It is important to try to identify, in advance, who might be impacted by the new program and determine ways to work with them. Visible support from deans and program administrators can be helpful to encourage involvement or at least to neutralize the negative influence of skeptics.
Dedicating Time to Implementation The time it takes to implement GITT in will vary for each site. Sites found certain factors were most responsible for lengthening the time needed for full program implementation. Curriculum Development
The largest time factor is the time needed to design the curriculum and organize didactic content. Time needed for this activity may vary depending on the ability of program coordinator and faculty of each discipline to commit their own time and resources.
Curriculum Committees
Each school has a different curriculum committee and timing for work of the committee. If the program champions or steering committee were unable to make the curriculum committee’s timeframe for introducing new courses in one school, the timeframe for the whole program could be backed up.
Dean and Program Administrator Support
If Deans are not involved in the early stages, getting them to support the program and commit resources can be a significant barrier to program implementation or significantly lengthen the time needed for implementation.
Preceptors
Each discipline has different rules for preceptors. Programmatically, while one structure may make the most sense, if the suggested preceptors are not certified appropriately or if student involvement there will not count toward broader graduation requirements, implementation may be slowed.
Contracts with Clinical Settings
Program development must take into account time frames needed to create new contracts with clinical sites and for different disciplines to identify whether new clinical sites must be found.
Academic Credit
Some programs found that a substantial barrier to program implementation was clarifying how to obtain academic credit for students participating in the program. Often, to do so requires novel ways of manipulating current curricular requirements or the didactic and clinical content to match these broader needs. Making such modifications can take time and should be done before students enter into a GITT experience.
Hints from the Field
Sites considering replication of the GITT program should consider issues in program design that have previously created barriers to successful program implementation.
GITT Implementation Manual 2012
Implementation Chapter 2 - 9
Logistics
The logistics (e.g., differences in length of learner rotations, discipline training requirements, discipline philosophies, existing structures both in the clinics and internal to the university, etc.) make mounting an interdisciplinary team training program extremely difficult. This kind of training cannot be done without a strong infrastructure. Negotiating scheduling nightmares. Scheduling the didactic classes was a major frustration due to the varying schedules of the trainees. Sites had to be flexible to meet the schedules of the trainees and implemented a combination didactic class and self-study program in the third year. Though sometimes difficult to achieve because of scheduling conflicts, having team members’ work with the same patients throughout their training rotation is the optimum way to teach about interdisciplinary care in the clinical setting.
Elective vs. Mandatory
Trainees recruited to GITT are often more open to learning, however, mandating GITT experiences insure balanced participation across disciplines. In the beginning, participation in GITT was part of the required internship for the various disciplines. Sites learned that each discipline had strict supervision guidelines that limited placement options. To deal with this issue, sites recruited trainees to participate in GITT as an elective or extra credit, thereby not restricting the supervision as much. Recruitment was a challenging aspect of GITT. Sites learned that the interest in aging was not as high as had been anticipated among students. Presentations about GITT and aging were done in classes to increase interest in geriatrics. As an incentive, some trainees were offered extra credit or stipends from the academic institution or the clinical setting to participate.
Administrative Support
Involvement of clinic and system administrators and early consideration of sustainability issues are key. A steering committee process is essential to implementing changes in both the institution and the community. Sites must have organizational support at the highest level prior to program development. Sites must have organizational/leadership support during implementation. Sites must have key administrative direction and coordination with good access to organizational leadership.
Coordination
Integrating academic and clinical training across multiple disciplines requires substantial administrative coordination that will not occur unless it is explicitly someone’s responsibility. Leadership and coordination can address logistics barriers. The operational and programmatic activities required of an interdisciplinary team training program -- including faculty, preceptor and trainee recruiting, curriculum development, classroom and clinical scheduling, maintaining contact with training sites, evaluation, and other activities -- necessitate having a program coordinator.
GITT Implementation Manual 2012
Implementation Chapter 2 - 10
GITT Steering Committee. The committee is necessary and very useful during program development, resulting in benefits to overall GITT Program. After program development and revision, faculty must consider if there is a role for the Steering Committee other than networking.
Each participating academic discipline requires a Program Champion with primary authority or significant influence around curriculum and practicum requirements.
Cost
The used has a high teacher/student ratio. It may be hard to sustain without external support. Small groups are effective for teaching this material. Interdisciplinary training has a strong positive effect on learners but is expensive and requires substantial coordination, an infrastructure item that is often not considered in academic budgets.
Curricular Flexibility
The current educational system trains disciplines in isolation. Interdisciplinary team training provides learners with the opportunity to learn which skills and knowledge other disciplines bring to the clinical team, as well as reaffirm their role on the clinical team. Facilitation is an essential support at start up but can be reduced or internalized as teams become more skilled. Packaging carefully developed resources on geriatric skills increases the likelihood that GITT will be included in crowded curricula. Resources need to be user friendly so they can be adapted to varying learning situations.
Team Focus
For faculty trying to keep the focus on teams, resisting the urge to teach geriatric concepts is difficult. Tools, such as a checklist to review team concepts including roles on teams, conflict styles, etc., help focus team learning. Team care is not appropriate for every case but does work for targeted patients. Not every case needs the resources implied by teams. Better tools are needed to help identify which patients need a team approach. An inherent difficulty exists for learners trying to combine learning of geriatrics and teams.
Teaching Teamwork
Teaching teamwork is challenging and difficult; however, results are rewarding. Teaching teamwork is time and labor intensive. Sometimes it is difficult to make teamwork explicit at clinical sites. Educational tools emphasizing meeting etiquette are only one tool and not necessarily the most important exercise to use in teaching about interdisciplinary teams. The economic and clinical practice realities of captivated delivery systems are essential elements in teaching about the efficacy and necessity of teams in an interdisciplinary team program.
GITT Implementation Manual 2012
Implementation Chapter 2 - 11
Since learner teams are always in the forming and norming stages, creating conflict situations and teaching conflict resolution are difficult. Students are adept at role-playing. It is generally not worth it to them to deal with interpersonal problems that arise if they will be moving on shortly. Videos of poor team performance give the students some material around which to discuss how to handle conflict. Regular team meetings are not always essential to the success of interdisciplinary teams. Communicating effectively, sharing information in a timely manner, understanding and respecting the roles and contributions of multiple disciplines involved in the care of the patient are more important skills to emphasize than how to function in a team meeting. The classic team is not necessarily a realistic model of health care today.
Real time experiences (e.g., home care visits) are successful.
Team Maturity
Learners enter with varying levels of awareness about their own and other disciplines, and most expand their appreciation of other disciplines and the value of interdisciplinary collaboration. Learning in the team setting stimulates clinicians to make changes to improve care. Day-to-day interaction as a team and supporting each other levels the playing field in terms of clinical hierarchy. There are different levels of team collaboration and teams go through a developmental process.
Didactic Sessions
Shortening and bringing more focus to training workshops improved outcomes. The choice of teaching tools and didactic resources must fit the learning environment. Trainees in clinical rotations are less likely to read a manual or work on a written case than trainees convened in a classroom or workshop. Flexibility in scheduling, class teaching experientials and methodologies, and utilizing a variety of teaching methodologies are essential. A successful interdisciplinary program requires didactic and clinical experiences that complement and support the principles and necessity of interdisciplinary care. Trainees must experience how teams work in actual practice.
Sites must orient each discipline to the others — lack of information, myths, etc., are prevalent. Case-based teaching works best — trainees should participate in presentations. Students prefer to learn from their own cases rather than from hypothetical material. Distance learning and the integration of computer technology are important for sustainability of the model in the future. Students from different disciplines need a fun way to work together productively. Interactive workshops are focused, positive learning experiences.

GITT Implementation Manual 2012
Implementation Chapter 2 - 12
Clinical Maturity
It is difficult to teach learners about teams when they have not yet established clarity about their roles in their training program. There is a marked difference in students between fall semester vs. spring semester learners, and first- vs. third-year residents. Learners do better in teams when they can contribute clinically. This level of performance requires clinical maturity. Students without a lot of clinical geriatric experience (e.g., in the fall) needs some sort of structured material to discuss.
Value of the GITT Experience
While learners completing the training now have a conceptual framework on team development, process, evaluation, and enhancement, the true value of the experience and content will not be appreciated until they have been practicing for 2 or more years. Because practicum experiences or rotations are often seen as a limited experience --something that is part of the learners’ required education -- the impact of interdisciplinary team training will become clearer to learners once they are in what they perceive to be real jobs. The didactic class was a success and sites learned from the trainees that aside from the geriatrics and team training information, learning the roles of each of the disciplines was extremely valuable information. Regardless of their future careers or interest in teams, they believed this information was very beneficial.
Quality of Clinical Sites
Teaching interdisciplinary teams to learners in clinical settings is complicated by the clinic’s own level of development or functioning as an interdisciplinary team. Establish specific clinic-readiness criteria to identify sites best able to function as interdisciplinary training sites. Practitioners like the case study approach to interdisciplinary care. The geriatric syndrome modules were well received for this reason. Sites should recognize that due to differing philosophies and basic economics, many clinical settings are not truly active; functioning interdisciplinary teams, but rather are hybrids (a combination of multidisciplinary and interdisciplinary teams). Sharing learning across clinical sites helps teams move their own learning process forward. Turnover in personnel can easily derail carefully defined arrangements. Redundancy of involved faculty and preceptors for each participating discipline is optimal but not always possible. Clinical settings must perceive some current or future benefit from the involvement of significant numbers of trainees in the clinical environment (i.e., potential for employee recruitment, trainee contributions to ongoing work of the organization, affiliation with academic programs which lend other resources such as continuing education or staff development).
Having pre-existing models of care in the institutional and community setting facilitates development of successful clinical experiential.
GITT Implementation Manual 2012
Implementation Chapter 2 - 13
The issues for the GITT project sites are very different in some respects, depending upon whether the clinical sites and preceptors are experienced and well functioning or if they are brand new sites with people new to the preceptor role. The use of interdisciplinary teams works better at some sites than it does at others for reasons having to do with logistics, types of patients served, availability of training resources such as preceptors, and changes in the organizational structure of sites. When there is conflict and pressure from the system, teams can bring a measure of strength and push back with input and new ideas. The process of implementing GITT in a managed care setting was successful and improved care to older adults. The staff, trainees, and patients benefited from the team process and interdisciplinary assessment.
Preceptors
Discipline-specific preceptors need to be trained to become able to function in an interdisciplinary team setting and to precept as a team. Preceptors and faculty need training to develop confidence in their own GITT skills and also need ongoing reinforcement about how to help trainees. Clinical experiential were well received by students; need preceptors to buy-in and have a clear understanding of expectations. Teamwork in the management structure is important for setting a positive tone. It is very important to orient all (e.g., trainees, preceptors/faculty) to GITT. Sites must have formal preceptor training. The presence of an interdisciplinary team - training program in a large, academic institution has created as much of an interdisciplinary learning and practice experience for academic faculty as it has for trainees.
Documentation/Evaluation
Process tools and documented care plans are necessary to provide a structure for efficient and effective team meetings. Evaluation must be understood and reinforced as an important and integral part of interdisciplinary team training (for both trainees and preceptors).
Continuous Quality Improvement in GITT
Soliciting feedback from all constituencies is crucial to improving training for trainees, academic faculty, and preceptors. Solicit feedback from multiple sources to continuously improve the program. Must have ongoing relationships between academic partners and community/clinical sites. While strengthened by GITT, many of these relationships are still tentative and true collaboration is also tentative, in many cases. Must review clinical and didactic content and structure of training and revise, revise, revise, as needed.
GITT Implementation Manual 2012
Implementation Chapter 2 - 14
Continuation and long-term integration of the geriatric interdisciplinary model is the most critical issue and challenge to address. Developing and maintaining a continuous, coordinated didactic and clinical curriculum that meets the training requirements and scheduled rotations of all participating disciplines is one of the biggest challenges to creating and sustaining a meaningful training program. An interdisciplinary curriculum, once developed, cannot remain static. Its content must change continually to reflect the economic, political, and programmatic realities of the system in which it is situated and the availability of appropriate, dedicated faculty to participate in the curriculum.
Modifying our curriculum from student feedback enhanced the program (e.g., dropped a group paper and replaced exercises with website case studies done by student teams with faculty preceptors).
Medical Residents
Consider using medical students or 1st year residents rather than 2nd or 3rd year residents; this change would have created less disparity between disciplines. Residents liked the inclusion of health systems information (i.e., managed care) in their clinical rotation, because they had not received the content previously. It is difficult to recruit medical students due to a crowded and demanding curriculum. It is difficult to integrate medical residents into GITT
GITT Implementation Manual 2012
Implementation Chapter 2 - 15
GITTMaterials
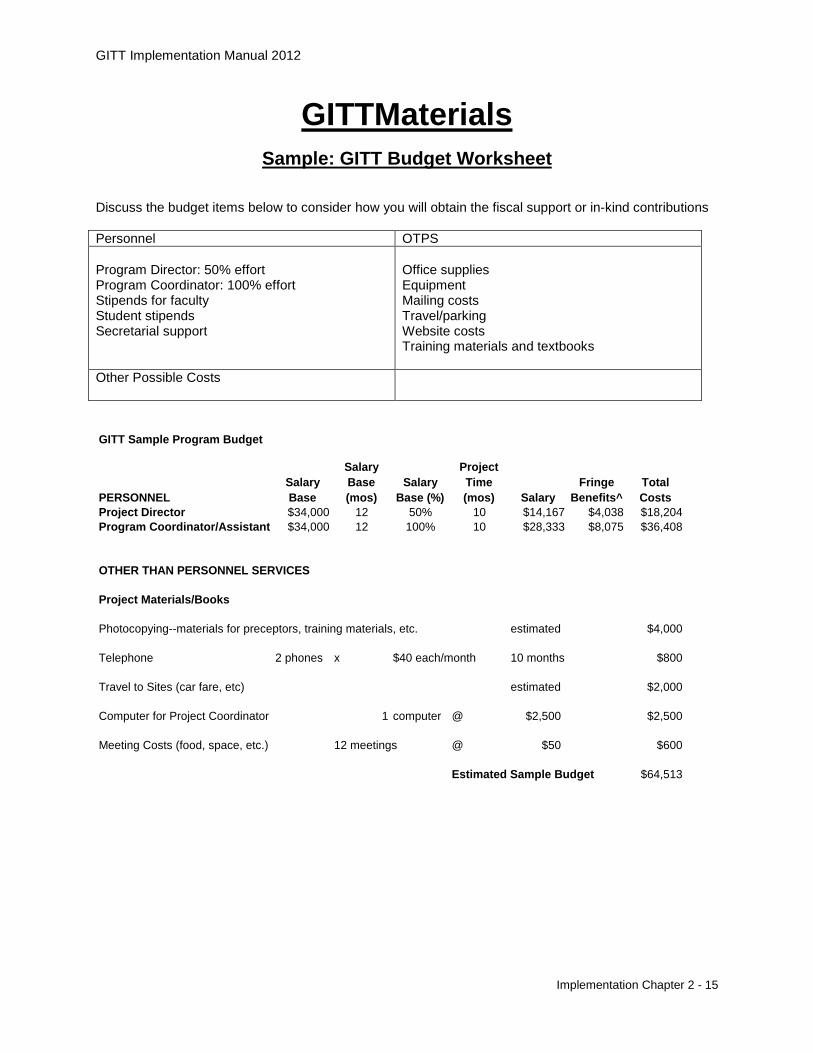
Sample: GITT Budget Worksheet Discuss the budget items below to consider how you will obtain the fiscal support or in-kind contributions Personnel OTPS Program Director: 50% effort Program Coordinator: 100% effort Stipends for faculty Student stipends Secretarial support
Office supplies Equipment Mailing costs Travel/parking Website costs Training materials and textbooks
Other Possible Costs
GITT Sample Program Budget
PERSONNELSalary Base
Salary Base (mos)
Salary Base (%)
Project Time (mos) Salary
Fringe Benefits^
Total Costs
Project Director $34,000 12 50% 10 $14,167 $4,038 $18,204Program Coordinator/Assistant $34,000 12 100% 10 $28,333 $8,075 $36,408
OTHER THAN PERSONNEL SERVICES
Project Materials/Books
Photocopying--materials for preceptors, training materials, etc. estimated $4,000
Telephone 2 phones x $40 each/month 10 months $800
Travel to Sites (car fare, etc) estimated $2,000
Computer for Project Coordinator 1 computer @ $2,500 $2,500
Meeting Costs (food, space, etc.) 12 meetings @ $50 $600
Estimated Sample Budget $64,513
GITT Implementation Manual 2012
Implementation Chapter 2 - 16
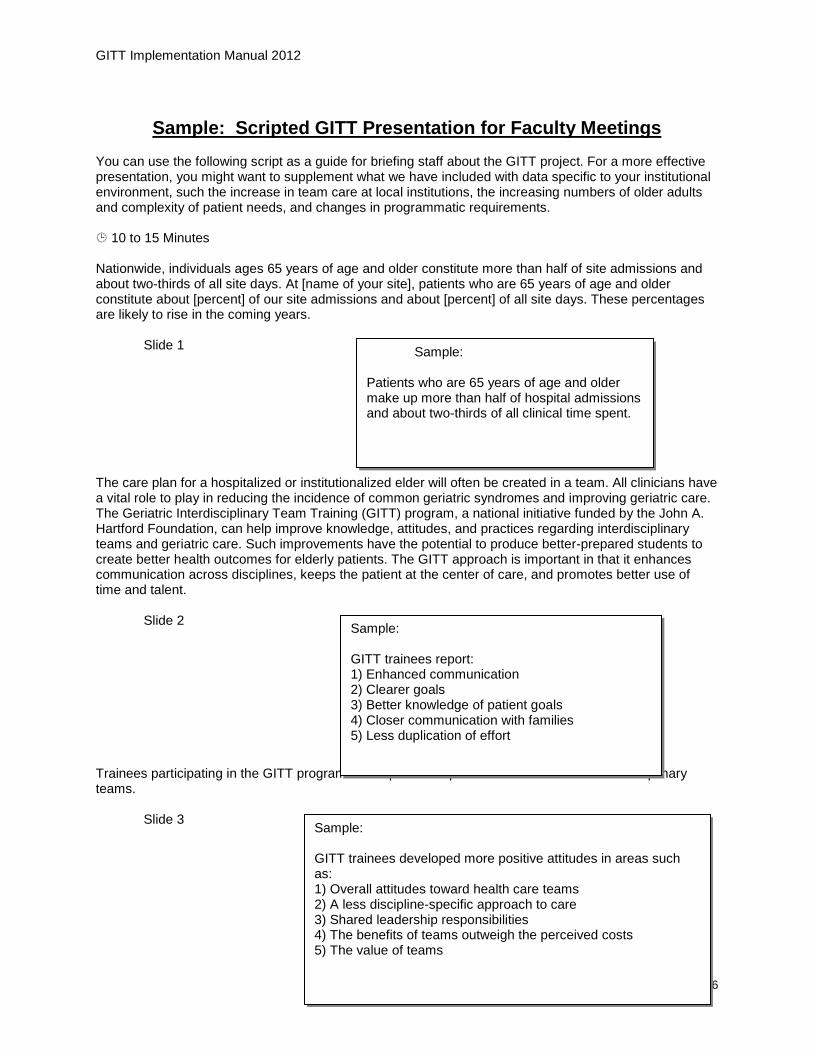
Sample: Scripted GITT Presentation for Faculty Meetings
You can use the following script as a guide for briefing staff about the GITT project. For a more effective presentation, you might want to supplement what we have included with data specific to your institutional environment, such the increase in team care at local institutions, the increasing numbers of older adults and complexity of patient needs, and changes in programmatic requirements. 10 to 15 Minutes Nationwide, individuals ages 65 years of age and older constitute more than half of site admissions and about two-thirds of all site days. At [name of your site], patients who are 65 years of age and older constitute about [percent] of our site admissions and about [percent] of all site days. These percentages are likely to rise in the coming years. Slide 1 The care plan for a hospitalized or institutionalized elder will often be created in a team. All clinicians have a vital role to play in reducing the incidence of common geriatric syndromes and improving geriatric care. The Geriatric Interdisciplinary Team Training (GITT) program, a national initiative funded by the John A. Hartford Foundation, can help improve knowledge, attitudes, and practices regarding interdisciplinary teams and geriatric care. Such improvements have the potential to produce better-prepared students to create better health outcomes for elderly patients. The GITT approach is important in that it enhances communication across disciplines, keeps the patient at the center of care, and promotes better use of time and talent. Slide 2 Trainees participating in the GITT program developed more positive attitudes toward interdisciplinary teams. Slide 3
Sample:
Patients who are 65 years of age and older make up more than half of hospital admissions and about two-thirds of all clinical time spent.
Sample: GITT trainees report: 1) Enhanced communication 2) Clearer goals 3) Better knowledge of patient goals 4) Closer communication with families 5) Less duplication of effort
Sample: GITT trainees developed more positive attitudes in areas such as: 1) Overall attitudes toward health care teams 2) A less discipline-specific approach to care 3) Shared leadership responsibilities 4) The benefits of teams outweigh the perceived costs 5) The value of teams
GITT Implementation Manual 2012
Implementation Chapter 2 - 17
In addition, GITT trainees cultivated more positive self-perceptions regarding their team skills and their ability to function effectively on a team. Slide 4 With the application of an effective model of geriatric care, GITT can lead to outcomes that extend well beyond the individual trainee. Slide 5 GITT is a practical, evidenced-based approach to improving geriatric interdisciplinary teams. The GITT program does not prescribe how institutions should go about training students to work in interdisciplinary teams. Rather, it provides the materials and models necessary to stimulate and support a site's planning and implementation process. Slide 6 GITT includes practical materials to facilitate improvements in geriatric care. Slide 7
Sample:
GITT trainees' self-perceived team skills improved in areas such as:
1) Identifying contributions to patient care that different disciplines can offer. 2) Ensuring that patient/family goals are considered when developing a care plan. 3) Handling disagreements effectively. 4) Raising appropriate issues at team meetings. 5) Recognizing when the team is not functioning well. 6) Intervening effectively to improve team functioning.
Sample: GITT can lead to the following outcomes: 1) A shared vocabulary for caring. 2) An appreciation for team member roles 3) Improved team skills 4) Enhanced use of time and services
Sample: GITT Evidence: 1) Trainee evaluations 2) Pre-post changes 3) Preceptor evaluations
Sample: GITT Materials: 1) Models for program development 2) Curricula for geriatric care 3) Curricula for effective teaming 4) Evaluation materials
GITT Implementation Manual 2012
Implementation Chapter 2 - 18
GITT is designed for use in different site environments. Indeed, eight very different institutions around the country have already implemented GITT with some success. Slide 8 GITT requires a commitment from administration in terms of resource allocation. We do not need to hire additional staff to implement GITT. In most situations, current personnel can implement the program. Slide 9 The program coordinator should have the knowledge and skills to move forward and promote the GITT plan as well as oversee the implementation of that plan and day-to-day activities. A current master’s-prepared staff member is probably qualified to undertake this responsibility. Also critical to the adoption and success of the intervention are faculty who are willing to act as program champions. In this role, faculty may introduce the program to other faculty and staff, support it through implementation, and see that it becomes a regular part of services. Like any innovation, the program may encounter obstacles. The program champions can help secure resources, identify and address potential problems, answer questions, and generally serve as an advocate for improved geriatric training. Moreover, when we join the GITT program, we become part of a national movement to improve geriatric interdisciplinary teams. As such, we acquire the materials and services we will need to help us improve the care we provide to our older patients. Among those services is ongoing technical assistance from staff at the John A. Hartford Foundation’s Geriatric Nursing Institute at NYU and connection to other sites that have implemented GITT. The benefits of adopting and implementing the GITT approach and materials outweigh the costs. The GITT program requires some time commitments from staff, as well as a few changes in site procedures and a few expenditures for materials. However, the potential benefits are great: enhanced capacity to provide geriatric care, improved staff skills, and increased confidence in assessing and managing older patients
Sample:
GITT Models: 1) The Academic Model: Faculty from different disciplines "teach" geriatric teaming. 2) The Clinical Agency Model: Clinical agencies institute geriatric training at their sites and recruit from within 3) The Mixed Model: Faculty works in the role of educator/clinician typically at a clinical agency.
Sample: Key to the success of GITT is a team composed of: 1) Program Champions 2) Steering Committee 3) Program Coordinator All of who are committed to improving geriatric interdisciplinary teams
GITT Implementation Manual 2012
Implementation Chapter 2 - 19
Worksheet: Defining Your Vision for Improved Geriatric Care through Interdisciplinary Teams
SECTION 1: Identifying the Disciplines: Does your school have a medical school with a likely program champion? Does your school have a nursing school/department with a likely program champion? Does your school have a social work school/department with a likely program champion? Are there other disciplines within your academic environment that might be likely to partner in developing a GITT Program? Are there faculties across the different disciplines who have the knowledge and skills to teach geriatrics and/or team training? What are your institution’s current and future goals related to geriatric interdisciplinary team care? How will GITT relate to existing programs — geriatric and others — already in place?
GITT Implementation Manual 2012
Implementation Chapter 2 - 20
Worksheet: Building Support for GITT How would you introduce the program to key faculty and staff? Whom would you approach about implementing GITT? From whom do you need support for institutional commitment to conduct GITT? Have you secured the necessary support? If not, with whom do you need to speak? What do you plan to do to promote and publicize the GITT program at your institution and in clinical sites? Which of the following methods do you plan to employ?
• brief announcements at regular meetings (e.g., grand rounds, unit meetings, specialty meetings) • announcements via e-mail, etc. • distribution of articles on geriatric models of care and geriatric protocols at the clinical sites • T-shirts, coffee mugs, and buttons with your own GITT logo
Whom do you expect to be skeptical about GITT implementation? How do you plan to convince skeptics of the importance of offering GITT? What external forces or trends in health care practice and policy might affect the implementation of GITT? Will these forces positively or negatively affect GITT? How do you plan to deal with some of the forces you have identified?
GITT Implementation Manual 2012
Implementation Chapter 2 - 21
Worksheet: Creating the GITT Team Is there a program coordinator at your site who is willing to provide senior -level support, including securing resources and advocating for the GITT program from assessment to institutionalization? YES NO If so, who? If not, who at the site could assume this role? What will the program champions’ responsibilities be? Is there a program coordinator at your site who is willing to provide hands-on leadership and guidance for the GITT program from assessment to institutionalization? YES NO If so, who? If not, who at the site could assume this role? What will the program coordinator’s responsibilities be? Are there faculty at your site who possesses the characteristics that would make them effective program champions in their individual disciplines? YES NO If so, who? If not, whom would you nominate? What will the program champions’ responsibilities be? Are there faculties with an interest in geriatrics or teaming who should be brought into the GITT program development process to help guide the work of the steering committee or subcommittees? YES NO If so, who? If not, whom would you nominate?
GITT Implementation Manual 2012
Implementation Chapter 2 - 22
What will their responsibilities be? 5. Are the roles of each member of the team defined clearly? In general, who will be responsible for what? (Denote these roles on the following page.) 6. Have you set up a meeting schedule for the GITT steering committee to exchange ideas, review progress, and plan next steps? YES NO If so, when does the group meet?
GITT Implementation Manual 2012
Implementation Chapter 2 - 23
Creating the Steering Committee: Member Responsibilities
ROLES
RESPONSIBILITIES
Champion:
Coordinator:
Core team members:
Evaluator:
Faculty/Educators:





























