Embed Size (px)
Citation preview

Chapter 3
Applying LearningTheories toHealthcare Practice
Margaret M.BraungartRichard G.Braungart
KEY TERMS
❑ learning ❑ information processing ❑ learning theory ❑ cognitive development ❑ respondent conditioning ❑ social constructivism ❑ systematic desensitization ❑ social cognition❑ stimulus generalization ❑ cognitive-emotional perspective❑ discrimination learning ❑ role modeling❑ spontaneous recovery ❑ vicarious reinforcement❑ operant conditioning ❑ defense mechanisms❑ escape conditioning ❑ resistance❑ avoidance conditioning ❑ transference❑ metacognition ❑ hierarchy of needs❑ gestalt perspective ❑ therapeutic relationship
51
CHAPTER HIGHLIGHTS
Applying Learning TheoriesBehaviorist Learning TheoryCognitive Learning TheorySocial Learning TheoryPsychodynamic Learning TheoryHumanistic Learning Theory
Neuropsychology and LearningComparison of Learning Theories
Common Principles of LearningHow Does Learning Occur?What Kinds of Experiences Facilitate or
Hinder the Learning Process?What Helps Ensure That Learning Becomes
Relatively Permanent?State of the Evidence
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 51

52 Chapter 3: Applying Learning Theories to Healthcare Practice
OBJECTIVES
After completing this chapter, the reader will be able to
1. Differentiate among the basic approaches to learning for each of the five learning theories.2. Define the principal constructs of each learning theory.3. Give an example applying each theory to changing the attitudes and behaviors of learners in
a specific situation.4. Discuss how neuroscience research has contributed to a better understanding of learning and
learning theories.5. Outline alternative strategies for learning in a given situation using at least two different
learning theories.6. Identify the differences and similarities in the learning theories specific to (a) the basic pro-
cedures of learning, (b) the assumptions made about the learning, (c) the task of the educa-tor, (d) the sources of motivation, and (e) the way in which the transfer of learning isfacilitated.
Learning is defined in this chapter as a relativelypermanent change in mental processing, emo-tional functioning, and/or behavior as a result ofexperience. It is the lifelong, dynamic process bywhich individuals acquire new knowledge orskills and alter their thoughts, feelings, atti-tudes, and actions.
Learning enables individuals to adapt todemands and changing circumstances and iscrucial in health care—whether for patients andfamilies grappling with ways to improve theirhealth and adjust to their medical conditions,for students acquiring the information and skillsnecessary to become a nurse, or for nurses andother healthcare staff devising and learningmore effective approaches to educating andtreating patients and each other in partnership.Despite the significance of learning to each indi-vidual’s development, functioning, health andwell-being, debate continues about how learn-
ing occurs, what kinds of experiences facilitateor hinder the learning process, and what ensuresthat learning becomes relatively permanent.
Until the late 19th century, most of the dis-cussions and debates about learning weregrounded in philosophy, school administration,and conventional wisdom (Hilgard, 1996).Around the dawn of the 20th century, the newfield of educational psychology emerged andbecame a defining force for the scientific studyof learning, teaching, and assessment (Woolfolk,2001). As a science, educational psychology restson the systematic gathering of evidence or datato test theories and hypotheses about learning.
A learning theory is a coherent framework ofintegrated constructs and principles thatdescribe, explain, or predict how people learn.Rather than offering a single theory of learning,educational psychology provides alternative the-ories and perspectives on how learning occurs
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 52

Applying Learning Theories 53
and what motivates people to learn and change(Hilgard & Bower, 1966; Ormrod, 2004;Snowman & Biehler, 2006).
The construction and testing of learning the-ories over the past century have contributedmuch to our understanding of how individualsacquire knowledge and change their ways ofthinking, feeling, and behaving. Reflecting anevidence-based approach to learning, the accu-mulated body of research information can be usedto guide the educational process and has chal-lenged a number of popular notions and mythsabout learning (e.g., “Spare the rod and spoil thechild,” “Males are more intelligent than females,”“You can’t teach an old dog new tricks.”). In addi-tion, the major learning theories have wide appli-cability and form the foundation of not only thefield of education but also psychological counsel-ing, workplace organization and human resourcemanagement, and marketing and advertising.
Whether used singly or in combination,learning theories have much to offer the practiceof health care. Increasingly, health profession-als must demonstrate that they regularlyemploy sound methods and a clear rationale intheir education efforts, patient and client inter-actions, staff management and training, andcontinuing education and health promotionprograms (Ferguson & Day, 2005).
Given the current structure of health care inthe United States, nurses, in particular, are oftenresponsible for designing and implementingplans and procedures for improving health edu-cation and encouraging wellness. Beyond one’sprofession, however, knowledge of the learningprocess relates to nearly every aspect of daily life.Learning theories can be applied at the individ-ual, group, and community levels not only tocomprehend and teach new material, but also to
solve problems, change unhealthy habits, buildconstructive relationships, manage emotions,and develop effective behavior.
This chapter reviews the principal psycho-logical learning theories that are useful to healtheducation and clinical practice. Behaviorist, cog-nitive, and social learning theories are most oftenapplied to patient education as an aspect of pro-fessional nursing practice. It is argued in thischapter that emotions and feelings also needexplicit focus in relation to learning in general(Goleman, 1995) and to health care in particular(Halpern, 2001). Why? Emotional reactions areoften learned as a result of experience, they playa significant role in the learning process, andthey are a vital consideration when dealing withhealth, disease, prevention, wellness, medicaltreatment, recovery, healing, and relapse preven-tion. To address this concern, psychodynamicand humanistic perspectives are treated as learn-ing theories in this review because they encour-age a patient-centered approach to care and addmuch to our understanding of human motiva-tion and emotions in the learning process.
The chapter is organized as follows. First,the basic principles of learning advocated bybehaviorist, cognitive, social learning, psycho-dynamic, and humanistic theories are sum-marized and illustrated with examples frompsychology and nursing research. With thecurrent upsurge and interest in neuroscienceresearch, brief mention is made of the contri-butions of neuropsychology to understandingthe dynamics of learning and sorting out theclaims of learning theories. Next, the learningtheories are compared with regard to:
• Their fundamental procedures forchanging behavior
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 53

54 Chapter 3: Applying Learning Theories to Healthcare Practice
• The assumptions made about the learner• The role of the educator in encouraging
learning• The sources of motivation for learning• The ways in which learning is trans-
ferred to new situations and problems
Finally, the theories are compared and then syn-thesized by identifying their common features andaddressing three questions: (1) How does learningoccur? (2) What kinds of experiences facilitate orhinder the learning process? (3) What helps ensurethat learning becomes relatively permanent?While surveying this chapter, readers are encour-aged to think of ways to apply the learning theo-ries to both their professional and personal lives.
The goals of this chapter are to provide a con-ceptual framework for subsequent chapters inthis book and to offer a toolbox of approachesthat can be used to enhance learning and changein patients, students, staff, and oneself. Althoughthere is a trend toward integrating learning the-ories in education, it is argued that knowledge ofeach theory’s basic principles, advantages, andshortcomings allows nurses and other health pro-fessionals to select, combine, and apply the mostuseful components of learning theories to specificpatients and situations in health care. After com-pleting the chapter, readers should be able toidentify the essential principles of learning,describe various ways in which the learningprocess can be approached, and develop alterna-tive strategies to change attitudes and behaviorsin different settings.
Learning TheoriesThis section summarizes the basic principlesand related concepts of the behaviorist, cogni-tive, social learning, psychodynamic, and hu-manistic learning theories. While reviewing
each theory, readers are asked to consider the fol-lowing questions:
• How do the environment and the inter-nal dynamics of the individual influencelearning?
• Is the learner viewed as relatively pas-sive or more active?
• What is the educator’s task in the learn-ing process?
• What motivates individuals to learn?• What encourages the transfer of learn-
ing to new situations?• What are the contributions and criti-
cisms of each learning theory?
Behaviorist Learning TheoryFocusing mainly on what is directly observable,behaviorists view learning as the product of thestimulus conditions (S) and the responses (R)that follow—sometimes termed the S-R modelof learning. Whether dealing with animals orpeople, the learning process is relatively simple.Generally ignoring what goes on inside theindividual—which, of course, is always difficultto ascertain—behaviorists closely observeresponses and then manipulate the environmentto bring about the intended change. Currentlyin education and clinical psychology, behavior-ist theories are more likely to be used in com-bination with other learning theories, especiallycognitive theory (Bush, 2006; Dai & Sternberg,2004). Behaviorist theory continues to be con-sidered useful in nursing and health care.
To modify people’s attitudes and responses,behaviorists either alter the stimulus conditionsin the environment or change what happensafter a response occurs. Motivation is explainedas the desire to reduce some drive (drive reduc-tion); hence, satisfied, complacent, or satiated
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 54

Learning Theories 55
individuals have little motivation to learn andchange. Getting behavior to transfer from theinitial learning situation to other settings islargely a matter of practice (strengtheninghabits). Transfer is aided by a similarity in thestimuli and responses in the learning situationrelative to future situations where the responseis to be performed. Much of behaviorist learn-ing is based on respondent conditioning andoperant conditioning procedures.
Respondent conditioning (also termed classical orPavlovian conditioning) emphasizes the impor-tance of stimulus conditions and the associationsformed in the learning process (Ormrod, 2004).In this basic model of learning, a neutral stim-
ulus (NS)—a stimulus that has no particularvalue or meaning to the learner—is paired witha naturally occurring unconditioned or unlearnedstimulus (UCS) and unconditioned response(UCR) (Figure 3–1). After a few such pairings,the neutral stimulus alone, without the uncondi-tioned stimulus, elicits the same unconditionedresponse. Thus, learning takes place when thenewly conditioned stimulus (CS) becomes associ-ated with the conditioned response (CR)—aprocess that may well occur without consciousthought or awareness.
Consider an example from health care.Someone without much experience with hospi-tals (NS) may visit a sick relative. While in the
Figure 3–1 Respondent conditioning model of learning.
BASIC MODEL OF LEARNING
EXAMPLE
UCS
NS
CS
NS = Neutral stimulus UCS = Unconditioned stimulusUCR = Unconditioned response CS = Conditioned stimulus CR = Conditioned response
NS + UCS UCR
UCR
where:
CR
UCR
(Several pairings)
or
Offensive odors(UCS)
Queasy feeling(UCR)
Queasy feeling(UCR)
Hospital + Offensive odors(NS) (UCS)
(Several pairings of Hospitals + Offensive odors Queasy feeling)
Queasy feeling(CR)
Hospital(CS)
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 55

56 Chapter 3: Applying Learning Theories to Healthcare Practice
relative’s room, the visitor may smell offensiveodors (UCS) and feel queasy and light-headed(UCR). After this initial visit and later repeatedvisits, hospitals (now the CS) may become asso-ciated with feeling anxious and nauseated (CR),especially if the visitor smells odors similar tothose encountered during the first experience(see Figure 3–1). Respondent conditioning high-lights the importance of the atmosphere and itseffects on staff morale in health care. Often with-out thinking or reflection, patients and visitorsformulate these associations as a result of theirhospital experiences, providing the basis forlong-lasting attitudes toward medicine, health-care facilities, and health professionals.
Besides influencing the acquisition of newresponses to environmental stimuli, principlesof respondent conditioning may be used toextinguish a previously learned response. Re-sponses decrease if the presentation of the con-ditioned stimulus is not accompanied by theunconditioned stimulus over time. Thus, if thevisitor who became dizzy in one hospital sub-sequently goes to other hospitals to see relativesor friends without smelling offensive odors, thenher discomfort and anxiety about hospitals maylessen after several such experiences.
Systematic desensitization is a technique basedon respondent conditioning that is used by psy-chologists to reduce fear and anxiety in theirclients (Wolpe, 1982). The assumption is thatfear of a particular stimulus or situation islearned, so it can, therefore, be unlearned orextinguished. Fearful individuals are first taughtrelaxation techniques. While they are in a stateof relaxation, the fear-producing stimulus isgradually introduced at a nonthreatening levelso that anxiety and emotions are not aroused.After repeated pairings of the stimulus underrelaxed, nonfrightening conditions, the indi-
vidual learns that no harm will come to him orher from the once fear-inducing stimulus.Finally, the client is able to confront the stimu-lus without being anxious and afraid.
As examples from healthcare research, re-spondent conditioning has been used to extin-guish chemotherapy patients’ anticipatorynausea and vomiting (Stockhurst, Steingrueber,Enck, & Klosterhalfen, 2006), while systematicdesensitization has been used to treat drugaddiction (Piane, 2000), phobias (McCullough& Andrews, 2001), tension headaches (Deyl &Kaliappan, 1997), and to teach children withADHD or autism to swallow pills (Beck,Cataldo, Slifer, Pulbrook, & Guhman, 2005). Asanother illustration, prescription drug advertis-ers regularly employ conditioning principles toencourage consumers to associate a brand namemedication with happy and improved lifestyles;once conditioned, consumers will likely favorthe advertised drug over the competitors’ med-ications and the much less expensive genericform. As a third example, taking the time tohelp patients relax and reduce their stress whenapplying some medical intervention—even apainful procedure—lessens the likelihood thatpatients will build up negative and anxiousassociations about medicine and health care.
Certain respondent conditioning concepts areespecially useful in the healthcare setting.Stimulus generalization is the tendency of initiallearning experiences to be easily applied to othersimilar stimuli. For example, when listening tofriends and relatives describe a hospital experi-ence, it becomes apparent that a highly positiveor negative personal encounter may colorpatients’ evaluations of their hospital stays aswell as their subsequent feelings about havingto be hospitalized again. With more and variedexperiences, individuals learn to differentiate
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 56

Learning Theories 57
among similar stimuli, and we say that discrim-ination learning has occurred. As an illustration,patients who have been hospitalized a numberof times often have learned a lot about hospital-ization. As a result of their experiences, theymake sophisticated distinctions and can dis-criminate among stimuli (e.g., what the variousnoises mean and what the various health profes-sionals do) that novice patients cannot. Much ofprofessional education and clinical practiceinvolves moving from being able to make gen-eralizations to discrimination learning.
Spontaneous recovery is a useful respondent con-ditioning concept that needs to be given carefulconsideration in relapse prevention programs.The principle of the concept operates as follows:Although a response may appear to be extin-guished, it may recover and reappear at any time(even years later), especially when stimulus con-ditions are similar to those in the initial learn-ing experience. Spontaneous recovery helps usunderstand why it is so difficult to completelyeliminate unhealthy habits and addictive behav-iors such as smoking, alcoholism, or drug abuse.
Another widely recognized approach tolearning is operant conditioning, which was devel-oped largely by B. F. Skinner (1974, 1989).Operant conditioning focuses on the behavior ofthe organism and the reinforcement that occursafter the response. A reinforcer is a stimulus orevent applied after a response that strengthensthe probability that the response will be per-formed again. When specific responses are rein-forced on the proper schedule, behaviors can beeither increased or decreased.
Table 3–1 summarizes the principal ways to increase and decrease responses by applyingthe contingencies of operant conditioning.Understanding the dynamics of learning pre-sented in this table can prove useful in assessing
and identifying ways to change individuals’behaviors in the healthcare setting. The key is tocarefully observe individuals’ responses to spe-cific stimuli and then decide the best reinforce-ment procedures to use to change a behavior.
Two methods to increase the probability of aresponse are to apply positive or negative rein-forcement after a response occurs. According toSkinner (1974), giving positive reinforcement(i.e., reward) greatly enhances the likelihoodthat a response will be repeated in similar cir-cumstances. As an illustration, although apatient moans and groans as he attempts to getup and walk for the first time after an operation,praise and encouragement (reward) for hisefforts at walking (response) will improve thechances that he will continue struggling towardindependence.
A second way to increase a behavior is byapplying negative reinforcement after a responseis made. This form of reinforcement involves theremoval of an unpleasant stimulus througheither escape conditioning or avoidance condi-tioning. The difference between the two typesof negative reinforcement relates to timing.
In escape conditioning, as an unpleasant stimulusis being applied, the individual responds in someway that causes the uncomfortable stimulation tocease. Suppose, for example, that when a memberof the healthcare team is being chastised in frontof the group for being late and missing meetings,she says something humorous. The head of theteam stops criticizing her and laughs. Because theuse of humor has allowed the team member toescape an unpleasant situation, chances are thatshe will employ humor again to alleviate a stress-ful encounter and thereby deflect attention fromher problem behavior.
In avoidance conditioning, the unpleasant stim-ulus is anticipated rather than being applied
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 57

58 Chapter 3: Applying Learning Theories to Healthcare Practice
directly. Avoidance conditioning has been usedto explain some people’s tendency to become illso as to avoid doing something they do not wantto do. For example, a child fearing a teacher ortest may tell his mother that he has a stom-achache. If allowed to stay home from school,the child increasingly may complain of sicknessto avoid unpleasant situations. Thus, when fear-ful events are anticipated, sickness, in this case,is the behavior that has been increased throughnegative reinforcement.
According to operant conditioning princi-ples, behaviors also may be decreased througheither nonreinforcement or punishment. Skinner(1974) maintained that the simplest way toextinguish a response is not to provide any kindof reinforcement for some action. For example,offensive jokes in the workplace may be handledby showing no reaction; after several such expe-
riences, the joke teller, who more than likelywants attention—and negative attention is pre-ferable to no attention—may curtail his or heruse of offensive humor. Keep in mind, too, thatdesirable behavior that is ignored may lessen aswell.
If nonreinforcement proves ineffective, thenpunishment may be employed as a way todecrease responses, although there are risks inusing this approach. Under punishment condi-tions, the individual cannot escape or avoid anunpleasant stimulus. Suppose, for example, thehealthcare team member’s attempt at humor ismet by the leader’s curt remark, “You are con-tinually a source of difficulty in this group, andif this continues, your job is in jeopardy,”embarrassing her in front of her peers. The prob-lem with using punishment as a technique forteaching is that the learner may become highly
Table 3–1 Operant Conditioning Model: Contingencies to Increaseand Decrease the Probability of an Organism’s Response
I. To increase the probability of a response:
A. Positive reinforcement: application of apleasant stimulus
Reward conditioning: a pleasant stimulus isapplied following an organism’s response
B. Negative reinforcement: removal of an aver-sive or unpleasant stimulus
Escape conditioning: as an aversive stimu-lus is applied, the organism makes aresponse that causes the unpleasantstimulus to cease
Avoidance conditioning: an aversive stimu-lus is anticipated by the organism, whichmakes a response to avoid the unpleasantevent
II. To decrease or extinguish the probability of aresponse:
A. Nonreinforcement: an organism’s con-ditioned response is not followed byany kind of reinforcement (positive,negative, or punishment)
B. Punishment: following a response, anaversive stimulus that the organismcannot escape or avoid is applied
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 58

Learning Theories 59
emotional and may well divert attention awayfrom the behavior that needs to be changed.Some people who are being punished become soemotional (sad or angry) that they do notremember the behavior for which they are beingpunished. One of the cardinal rules of operantconditioning is to “punish the behavior, not theperson.”
If punishment is employed, it should beadministered immediately after the responsewith no distractions or means of escape. Pun-ishment must also be consistent and at the high-est reasonable level (e.g., health professionalswho apologize and smile as they admonish thebehavior of a staff member or client are sendingout mixed messages and are not likely to betaken seriously or to decrease the behavior theyintend). Moreover, punishment should not beprolonged (bringing up old grievances or com-plaining about a misbehavior at every opportu-nity), but there should be a time-out followingpunishment to eliminate the opportunity forpositive reinforcement. The purpose of punish-ment is not to do harm or to serve as a release foranger; rather, the goal is to decrease a specificbehavior and to instill self-discipline.
The use of reinforcement is central to the suc-cess of operant conditioning procedures. Foroperant conditioning to be effective, it is nec-essary to assess what kinds of reinforcement arelikely to increase or decrease behaviors for eachindividual. Not every client, for example, findshealth practitioners’ terms of endearmentrewarding. Comments such as “Very nice job,dear,” may be presumptuous or offensive tosome clients. A second issue involves the timingof reinforcement. Through experimentationwith animals and humans, it has been demon-strated that the success of operant conditioningprocedures partially depends on the schedule of
reinforcement. Initial learning requires a con-tinuous schedule, reinforcing the behaviorquickly every time it occurs. If the desiredbehavior does not occur, then responses thatapproximate or resemble it can be reinforced,gradually shaping behavior in the direction ofthe goal for learning. As an illustration, for geri-atric patients who appear lethargic and unre-sponsive, nurses or physicians might begin byrewarding small gestures such as eye contact ora hand that reaches out, then build on thesefriendly behaviors toward greater human con-tact and connection with reality. Once aresponse is well established, however, it becomesineffective and inefficient to continually rein-force the behavior; reinforcement then can beadministered on a fixed (predictable) or variable(unpredictable) schedule after a given numberof responses have been emitted or after the pas-sage of time.
Operant conditioning techniques provide rel-atively quick and effective ways to changebehavior. Carefully planned programs usingbehavior modification procedures can readily beapplied to health care. For example, computer-ized instruction and tutorials for patients andstaff rely heavily on operant conditioning prin-ciples in structuring learning programs. In theclinical setting, the families of chronic back painpatients have been taught to minimize theirattention to the patients whenever they com-plain and behave in dependent, helpless ways,but to pay a lot of attention when the patientsattempt to function independently, express apositive attitude, and try to live as normal a lifeas possible. Some patients respond so well tooperant conditioning that they report experi-encing less pain as they become more active andinvolved. Operant conditioning and behaviormodification techniques also have been found to
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 59

60 Chapter 3: Applying Learning Theories to Healthcare Practice
work well with some nursing home and long-term care residents, especially those who are los-ing their cognitive skills (Proctor, Burns,Powell, & Tarrier, 1999).
The behaviorist theory is simple and easy touse, and it encourages clear, objective analysis ofobservable environmental stimulus conditions,learner responses, and the effects of reinforce-ments on people’s actions. There are, however,some criticisms and cautions to consider. First,this is a teacher-centered model in which learn-ers are assumed to be relatively passive and eas-ily manipulated, which raises a crucial ethicalquestion: who is to decide what the desirablebehavior should be? Too often the desiredresponse is conformity and cooperation to makesomeone’s job easier or more profitable. Second,the theory’s emphasis on extrinsic rewards andexternal incentives reinforces and promotesmaterialism rather than self-initiative, a love oflearning, and intrinsic satisfaction. Third,research evidence supporting behaviorist theoryis often based on animal studies, the results ofwhich may not be applicable to human behav-ior. A fourth shortcoming of behavior modifica-tion programs is that clients’ changed behaviormay deteriorate over time, especially once theyare back in their former environment—an envi-ronment with a system of rewards and punish-ments that may have fostered their problems inthe first place.
We now move from focusing on responsesand behavior to the role of mental processes inlearning.
Cognitive Learning TheoryWhile behaviorists generally ignore the internaldynamics of learning, cognitive learning theo-rists stress the importance of what goes oninside the learner. Cognitive theory is assumed
to be comprised of a number of subtheories andis widely used in education and counseling. Thekey to learning and changing is the individual’scognition (perception, thought, memory, andways of processing and structuring information).Cognitive learning, a highly active processlargely directed by the individual, involves per-ceiving the information, interpreting it based onwhat is already known, and then reorganizingthe information into new insights or under-standing (Bandura, 2001; Hunt, Ellis, & Ellis,2004).
Cognitive theorists, unlike behaviorists,maintain that reward is not necessary for learn-ing. More important are learners’ goals andexpectations, which create disequilibrium,imbalance, and tension that motivate them toact. Educators trying to influence the learningprocess must recognize the variety of past expe-riences, perceptions, ways of incorporating andthinking about information, and diverse aspira-tions, expectations, and social influences thataffect any learning situation. A learner’s metacog-nition, or understanding of her way of learning,influences the process as well. To promote trans-fer of learning, the learner must mediate or acton the information in some way. Similar pat-terns in the initial learning situation and subse-quent situations facilitate this transfer.
Cognitive learning theory includes severalwell-known perspectives, such as gestalt, infor-mation processing, human development, socialconstructivism, and social cognition theory.More recently, attempts have been made toincorporate considerations related to emotionswithin cognitive theory. Each of these perspec-tives emphasizes a particular feature of cognition,which, when pieced together, indicates muchabout what goes on inside the learner. As the var-ious cognitive perspectives are briefly summa-
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 60

Learning Theories 61
rized here, readers are encouraged to think oftheir potential applications in the healthcare set-ting. In keeping with cognitive principles oflearning, being mentally active with informationencourages memory and retention.
One of the oldest psychological theories isthe gestalt perspective, which emphasizes theimportance of perception in learning and laidthe groundwork for the various other cognitiveperspectives that followed (Kohler, 1947, 1969;Murray, 1995). Rather than focusing on discretestimuli, gestalt refers to the configuration orpatterned organization of cognitive elements,reflecting the maxim that the whole is greaterthan the sum of the parts. A principal assump-tion is that each person perceives, interprets, andresponds to any situation in his or her own way.While there are many gestalt principles worthknowing (Hilgard & Bower, 1966), several willbe discussed here as they relate to health care.
A basic gestalt principle is that psychologi-cal organization is directed toward simplicity,equilibrium, and regularity. For example, studythe bewildered faces of some patients listeningto a complex, detailed explanation about theirdisease, when what they desire most is a simple,clear explanation that settles their uncertaintyand relates directly to them and their familiarexperiences.
Another central gestalt principle is that per-ception is selective, which has several ramifica-tions. First, because no one can attend to all thesurrounding stimuli at any given time, individ-uals orient themselves to certain features of anexperience while screening out or ignoring otherfeatures. Patients in severe pain or worried abouttheir hospital bills may not attend to well-intentioned patient education information.Second, what individuals pay attention to andwhat they ignore are influenced by a host of fac-
tors: past experiences, needs, personal motivesand attitudes, reference groups, and the partic-ular structure of the stimulus or situation (Sherif& Sherif, 1969). Assessing these internal andexternal dynamics has a direct bearing on how ahealth educator approaches any learning situa-tion with an individual or group. Moreover,because individuals vary widely with regard tothese and other characteristics, they will per-ceive, interpret, and respond to the same eventin different ways, perhaps distorting reality tofit their goals and expectations. This tendencyhelps explain why an approach that is effectivewith one client may not work with anotherclient. People with chronic illnesses—even dif-ferent people with the same illness—are notalike, and helping any patient with disease ordisability includes recognizing each person’sunique perceptions and subjective experience(Imes, Clance, Gailis, & Atkeson, 2002).
Information processing is a cognitive perspectivethat emphasizes thinking processes: thought,reasoning, the way information is encounteredand stored, and memory functioning (Gagné,1985; Sternberg, 2006). How information isincorporated and retrieved is useful for healthprofessionals to know, especially in relation toolder people’s learning (Hooyman & Kiyak,2005; Kessels, 2003).
An information-processing model of memoryfunctioning is illustrated in Figure 3–2. Track-ing learning through the various stages is help-ful in assessing what happens to information asit is perceived, interpreted, and remembered byeach learner, which, in turn, may suggest waysof improving the structure of the learning situ-ation as well as how to correct misconceptions,distortions, and errors in learning.
The first stage in the memory processinvolves paying attention to environmental
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 61

62 Chapter 3: Applying Learning Theories to Healthcare Practice
stimuli; attention, then, is the key to learning.Thus, if a client is not attending to what a nurseeducator is saying, perhaps because the client isweary or distracted, it would be prudent to trythe explanation at another time when he is morereceptive and attentive.
In the second stage, the information isprocessed by the senses. Here it becomes impor-tant to consider the client’s preferred mode ofsensory processing (visual, auditory, or motormanipulation) and to ascertain whether there aresensory deficits.
In the third stage, the information is trans-formed and incorporated (encoded) briefly intoshort-term memory, after which it is either disre-garded and forgotten or stored in long-term mem-ory. Long-term memory involves the organizationof information by using a preferred strategy forstorage (e.g., imagery, association, rehearsal, orbreaking the information into units). While long-term memories are enduring, a central problem isretrieving the stored information at a later time.
The last stage involves the action or responsethat the individual makes on the basis of howinformation was processed and stored. Educationinvolves assessing how a learner attends to,processes, and stores the information that is pre-sented as well as finding ways to encourage theretention and retrieval processes. Errors are cor-rected by helping learners reprocess what needsto be learned (Kessels, 2003).
In general, cognitive psychologists note thatmemory processing and the retrieval of informa-tion are enhanced by organizing information andmaking it meaningful. A widely used descriptivemodel has been provided by Robert Gagné(1985). Subsequently, Gagné and his colleaguesoutlined nine events and their correspondingcognitive processes that activate effective learn-ing (Gagné, Briggs, & Wagner, 1992):
• Gain the learner’s attention (reception)• Inform the learner of the objectives and
expectations (expectancy)
Stage 1Attention
Stage 2Processing
Stage 4Action
Stage 3Memory Storage
EXTERNALPROCESSES
EXTERNALPROCESSES
INTERNALPROCESSES
SensoryMemory
Short-TermMemory
Long-TermMemory
Responseencoding storage
strategy
(Briefless than30 seconds)
(Fleetingless than1 second)
(Enduring:butretrievalproblems)
Orientingstimuli
Physical andemotionalpropertiesarouseinterest.
Figure 3–2 Information-processing model of memory.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 62

Learning Theories 63
• Stimulate the learner’s recall of priorlearning (retrieval)
• Present information (selective percep-tion)
• Provide guidance to facilitate thelearner’s understanding (semanticencoding)
• Have the learner demonstrate the infor-mation or skill (responding)
• Give feedback to the learner (reinforce-ment)
• Assess the learner’s performance(retrieval)
• Work to enhance retention and transferthrough application and varied practice(generalization)
In employing this model, instructors must care-fully analyze the requirements of the activity,design and sequence the instructional events, andselect appropriate media to achieve the outcomes.
Within the information-processing perspec-tive, Sternberg (1996) reminds us to considerstyles of thinking, which he defined as “a prefer-ence for using abilities in certain ways” (p. 347).Thinking styles concern differences, he noted,and not judgments of better or worse. In educa-tion, the instructor’s task is to get in touch withthe learner’s way of processing information andthinking. Some implications for health care arethe need to carefully match jobs with styles ofthinking, to recognize that people may shift frompreferring one style of thinking to another, and,most important, to appreciate and respect the dif-ferent styles of thinking reflected among themany players in the healthcare setting (seeChapter 4 on learning styles). Yet striving for amatch in styles is not always necessary or desir-able. Tennant (2006) notes that adult learnersmay actually benefit from grappling with views
and styles of learning unlike their own, whichmay promote maturity, creativity, and a greatertolerance for differences. Since nurses are expectedto instruct a variety of people with diverse stylesof learning, Tennant’s suggestion has interestingimplications for nursing education programs.
The information-processing perspective isparticularly helpful for assessing problems inacquiring, remembering, and recalling infor-mation. Some strategies include the following:(1) have learners indicate how they believe theylearn (metacognition); (2) ask them to describewhat they are thinking as they are learning; (3) evaluate learners’ mistakes; and (4) give closeattention to their inability to remember ordemonstrate information. For example, forget-ting or having difficulty in retrieving informa-tion from long-term memory is a majorstumbling block in learning. This problem mayoccur because the information has faded fromlack of use, other information interferes with itsretrieval (what comes before or after a learningsession may well confound storage and re-trieval), or individuals are motivated to forgetfor a variety of conscious and unconscious rea-sons. This material on memory processing andfunctioning is highly pertinent to healthcarepractice—whether in developing health educa-tion brochures, engaging in one-to-one patienteducation, delivering a staff development work-shop, preparing community health lectures, orstudying for one’s courses and examinations.Focusing on attention, storage, and memory isessential in the patient education of older adults,including the identification of fatigue, medica-tions, and anxieties that may interfere withlearning and remembering (Kessels, 2003).
Heavily influenced by gestalt psychology, cog-nitive development is a third perspective on learningthat focuses on qualitative changes in perceiving,
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 63

64 Chapter 3: Applying Learning Theories to Healthcare Practice
thinking, and reasoning as individuals grow andmature (Santrock, 2006; Vander Zanden, Crandell,& Crandell, 2007). Cognitions are based on howexternal events are conceptualized, organized, andrepresented within each person’s mental frame-work or schema, which is partially dependent onthe individual’s stage of development in percep-tion, reasoning, and readiness to learn.
Much of the theory and research in this areahas been concerned with identifying the charac-teristics and advances in the thought processesof children and adolescents. A principal assump-tion is that learning is a developmental, sequen-tial, and active process that transpires as thechild interacts with the environment, makesdiscoveries about how the world operates, andinterprets these discoveries in keeping withwhat s/he knows (schema).
Jean Piaget is the best-known of the cogni-tive developmental theorists. His observationsof children’s perceptions and thought processesat different ages have contributed much to ourrecognition of the unique, changing abilities ofyoungsters to reason, conceptualize, communi-cate, and perform (Piaget & Inhelder, 1969). Bywatching, asking questions, and listening tochildren, Piaget identified and described foursequential stages of cognitive development (sen-sorimotor, preoperational, concrete operations,and formal operations). These stages becomeevident over the course of infancy, early child-hood, middle childhood, and adolescence,respectively (see Chapter 5 on developmentalstages). According to Piaget’s theory of cogni-tive learning, children take in information asthey interact with people and the environment.They either make their experiences fit withwhat they already know (assimilation) or changetheir perceptions and interpretations in keepingwith the new information (accommodation).
Health professionals and family members needto determine what children are perceiving andthinking in a given situation. As an illustration,young children usually do not comprehend fullythat death is final. They respond to the death ofa loved one in their own way, perhaps askingGod to give back the dead person or believingthat if they act like a good person, the deceasedloved one will return to them (Gardner, 1978).
Within the cognitive development perspectiveare some differences worth considering. For exam-ple, while Piaget stressed the importance of per-ception in learning and viewed children as littlescientists exploring, interacting, and discoveringthe world in a relative solitary manner, Russianpsychologist Lev Vygotsky (1986) emphasized thesignificance of language, social interaction, andadult guidance in the learning process. Whenteaching children, Vygotsky says the job of adultsis to interpret, respond, and give meaning to chil-dren’s actions. Rather than the discovery methodfavored by Piaget, Vygotsky advocated clear, well-designed instruction that is carefully structured toadvance each person’s thinking and learning.
In practice, some children may learn moreeffectively by discovering and putting piecestogether on their own, whereas other childrenbenefit from a more social and directiveapproach. It is the health educator’s responsi-bility to identify the child’s or teenager’s stageof thinking, to provide experiences at an appro-priate level for children to actively discover andparticipate in the learning process, and to deter-mine whether a child learns best through lan-guage and social interaction or throughperceiving and experimenting in his or her ownway. Research suggests that young children’slearning is often more solitary, whereas olderchildren may learn more readily through socialinteraction (Palincsar, 1998).
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 64

Learning Theories 65
What do cognitive developmental theoristssay about adult learning? First, although thecognitive stages develop sequentially, someadults never reach the formal operations stage.These adults may learn better from explicitlyconcrete approaches to health education. Second,adult developmental psychologists and geron-tologists have proposed advanced stages of rea-soning in adulthood beyond formal operations.For example, it is not until the adult years thatpeople become better able to deal with con-tradictions, synthesize information, and moreeffectively integrate what they have learned—characteristics that differentiate adult thoughtfrom adolescent thinking (Kramer, 1983). Third,older adults may demonstrate an advanced levelof reasoning derived from their wisdom and lifeexperiences, or they may reflect lower stages ofthinking due to lack of education, disease,depression, extraordinary stress, or medications(Hooyman & Kiyak, 2005).
Research indicates that adults generally dobetter with self-directed learning (emphasiz-ing learner control, autonomy, and initiative),an explicit rationale for learning, a problem-oriented rather than subject-oriented approach,and the opportunity to use their experiences andskills to help others (Tennant, 2006). Also, keepin mind that anxiety, the demands of adult life,and childhood experiences may interfere withlearning in adulthood.
Because cognitive theory was criticized forneglecting the social context, the effects of socialfactors on perception, thought, and motivationare receiving increased attention. Social construc-tivism and social cognition are two increasinglypopular perspectives within cognitive theory.Drawing heavily from gestalt psychology anddevelopmental psychology, social constructiviststake issue with some of the highly rational
assumptions of the information-processing viewand build on the works of John Dewey, JeanPiaget, and Lev Vygotsky (Palincsar, 1998).Social constructivists posit that individuals for-mulate or construct their own versions of realityand that learning and human development arerichly colored by the social and cultural contextin which people find themselves. A central tenetof this approach is that ethnicity, social class,gender, family life, past history, self-concept,and the learning situation itself all influence anindividual’s perceptions, thoughts, emotions,interpretations, and responses to informationand experiences. A second principle is that effec-tive learning occurs through social interaction,collaboration, and negotiation (Shapiro, 2002).
According to this view, the players in anyhealthcare setting may have differing percep-tions of external reality, including distorted per-ceptions and interpretations. Every personoperates on the basis of her or his unique repre-sentations and interpretations of a situation, allof which have been heavily influenced by thatindividual’s social and cultural experiences. Theimpact of culture cannot be ignored, and learn-ing is facilitated by sharing beliefs, by acknowl-edging and challenging differing conceptions,and by negotiating new levels of conceptualunderstanding (Marshall, 1998). Cooperativelearning and self-help groups are examples ofsocial constructivism in action. With America’srapidly changing age and ethnic composition,the social constructivist perspective has much tocontribute to health education and health pro-motion efforts.
Rooted in social psychology, the social cog-nition perspective reflects a constructivist ori-entation and highlights the influence of socialfactors on perception, thought, and motivation.A host of scattered explanations can be found
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 65

66 Chapter 3: Applying Learning Theories to Healthcare Practice
under the rubric of social cognition (Fiske &Taylor, 1991; Moskowitz, 2005), which, whenapplied to learning, emphasize the need forinstructors to consider the dynamics of the socialenvironment and groups on both interpersonaland intrapersonal behavior. As an illustration,attribution theory concerns the cause-and-effectrelationships and explanations that individualsformulate to account for their own and others’behavior and the way in which the world operates.Many of these explanations are unique to the indi-vidual and tend to be strongly colored by culturalvalues and beliefs. For example, patients with cer-tain religious views or a particular parentalupbringing may believe that their disease is apunishment for their sins (internalizing blame);other patients may attribute their disease to theactions of others (externalizing blame). From thisperspective, patients’ attributions may or may notpromote wellness and well-being. The route tochanging health behaviors is to change distortedattributions. The medical staff’s prejudices, biases(positive and negative), and attributions need tobe considered as well in the healing process.
Cognitive theory has been criticized forneglecting emotions, and recent efforts havebeen made to incorporate considerations relatedto emotions within a cognitive framework,known as the cognitive-emotional perspective. AsEccles and Wigfield (2002) commented, “ ‘cold’cognitive models cannot adequately captureconceptual change; there is a need to consideraffect as well” (p. 127).
Several slightly different cognitive orienta-tions to emotions have been proposed and arebriefly summarized in the following list:
• Empathy and the moral emotions (e.g.,guilt, shame, distress, moral outrage)play a significant role in influencing
children’s moral development and inmotivating people’s prosocial behaviorand ethical responses (Hoffman, 2000).
• Memory storage and retrieval, as well asmoral decision making, involve bothcognitive and emotional brain process-ing, especially in response to situationsthat directly involve the self and arestressful (Greene, Sommerville,Nystrom, Darley, & Cohen, 2001).
• Emotional intelligence (EI) entails man-aging one’s emotions, self-motivation,reading the emotions of others, andworking effectively in interpersonalrelationships, which some argue is moreimportant to leadership, social judg-ment, and moral behavior than cogni-tive intelligence (Goleman, 1995).
• Self-regulation includes monitoringcognitive processes, emotions, and one’ssurroundings to achieve goals, which isconsidered a key factor to successful liv-ing and effective social behavior (Eccles& Wigfield, 2002).
The implications are that nursing and otherhealth professional education programs would dowell to exhibit and encourage empathy and emo-tional intelligence in working with patients,family, and staff and to attend to the dynamics ofself-regulation as a way to promote positive per-sonal growth and effective leadership. Researchindicates that the development of these attri-butes in self and patients is associated with agreater likelihood of healthy behavior, psycho-logical well-being, optimism, and meaningfulsocial interactions (Brackett, Lopes, Ivcevic,Mayer, & Salovey, 2004).
A significant benefit of the cognitive theory tohealth care is its encouragement of recognizing
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 66

Learning Theories 67
and appreciating individuality and diversity inhow people learn and process experiences.Whenapplied to health care, cognitive theory has beenuseful in formulating exercise programs for breastcancer patients (Rogers, Matevey, Hopkins-Price,Shah, Dunnington, & Courneya, 2004), under-standing individual differences in bereavement(Stroebe, Folkman, Hansson, & Schut, 2006), anddealing with adolescent depression in girls(Papadakis, Prince, Jones, & Strauman, 2006).Cognitive theory highlights the wide variation inhow learners actively structure their perceptions;confront a learning situation; encode, process,store, and retrieve information; and manage theiremotions, all of which are affected by social andcultural influences. The challenge to educators isto identify each learner’s level of cognitive de-velopment and the social influences that affectlearning, and then find ways to foster insight, cre-ativity, and problem solving. Difficulties lie inascertaining exactly what is transpiring inside themind of each individual and in designing learn-ing activities that encourage people to restructuretheir perceptions, reorganize their thinking, reg-ulate their emotions, change their attributionsand behavior, and create solutions.
The next learning theory to be discussedcombines principles from both the behavioristand cognitive theories.
Social Learning TheorySocial learning theory is largely the work ofAlbert Bandura (1977; 2001), who mapped outa perspective on learning that includes consid-eration of the personal characteristics of thelearner, behavior patterns, and the environment.The theory has gone through several “paradigmshifts” (2001, p. 2). In early formulations, heemphasized behaviorist features and the imita-tion of role models; next the focus was on cog-
nitive considerations, such as the attributes ofthe self and the internal processing of thelearner. More recently, his attention turned tothe impact of social factors and the social con-text within which learning and behavior occur.As the model has evolved, the learner hasbecome viewed as central (what Bandura calls a“human agency”), which suggests the need toidentify what learners are perceiving and howthey are interpreting and responding to socialsituations. As such, careful consideration needsto be given to the healthcare environment as asocial situation.
One of Bandura’s early observations was thatindividuals need not have direct experiences tolearn; considerable learning occurs by takingnote of other people’s behavior and what hap-pens to them. Thus, learning is often a socialprocess, and other individuals, especially signif-icant others, provide compelling examples orrole models for how to think, feel, and act. Rolemodeling is a central concept of the theory. As anexample, a more experienced nurse who demon-strates desirable professional attitudes and be-haviors sometimes is used as a mentor for a lessexperienced nurse. Research indicates that nursemanagers’ attitudes and actions—ensuringsafety, integrating knowledge with practice,sharing feelings, challenging staff nurses andstudents, and their competence and willingnessto provide guidance to others—influence theoutcomes of the clinical supervision process(Berggren & Severinsson, 2006). How nursementors perceive their role is an important con-sideration in the leadership selection process(Neary, 2000).
Vicarious reinforcement is another concept fromthe social learning theory and involves deter-mining whether role models are perceived asrewarded or punished for their behavior. Reward
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 67

68 Chapter 3: Applying Learning Theories to Healthcare Practice
is not always necessary, however, and the behav-ior of a role model may be imitated even whenno reward is involved for either the role model orthe learner. In many cases, however, whether themodel is viewed by the observer as rewarded orpunished may have a direct influence on learn-ing. This relationship may be one reason why itis difficult to attract health professionals to geri-atric care. Although some highly impressive rolemodels work in the field, geriatric health care isoften accorded lower status with less pay in com-parison to other specialty areas.
While social learning theory is based partiallyon behaviorist principles, the self-regulation andcontrol that the individual exerts in the processof acquiring knowledge and changing behaviorare considered more critical and are more reflec-tive of cognitive principles. Bandura (1977) out-
lined a four-step, largely internal process thatdirects social learning, as can be seen in Figure3–3. Although some components are similar tothe information processing model described pre-viously, a principal difference is the inclusion ofa motivational component in the social learningtheory model.
First is the attentional phase, a necessary con-dition for any learning to occur. Research indi-cates that role models with high status andcompetence are more likely to be observed,although the learner’s own characteristics (needs,self-esteem, competence) may be the more sig-nificant determiner of attention. Second is theretention phase, which involves the storage andretrieval of what was observed. Third is thereproduction phase, where the learner copies theobserved behavior. Mental rehearsal, immediate
MotivationalPhase
ReproductionPhase
RetentionPhase
AttentionalPhase
Performance
INTERNAL PROCESSES EXTERNALPROCESSES
EXTERNALPROCESSES
Observationof rolemodel
Processingand repre-sentationin memory
Memoryguidesperformanceof model'sactions
Influenced byvicarious rein-forcement andpunishment
Covert cogni-tive activity,consequencesof behavior,and self-reinforcementandpunishment
Self-Regulation and Control
Role modeldemonstratesbehavior,which isperceivedby the learnerto bereinforced(vicariousreinforcement);modelmay facilitateor inhibitlearninga behavior.
Figure 3–3 Social learning theory.
Source: Based on Bandura (1977).
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 68

Learning Theories 69
enactment, and corrective feedback strengthenthe reproduction of behavior. Fourth is the moti-vational phase, which focuses on whether thelearner is motivated to perform a certain type ofbehavior. Reinforcement or punishment for arole model’s behavior, the learning situation, andthe appropriateness of subsequent situationswhere the behavior is to be displayed all affect alearner’s performance (Bandura, 1977; Gage &Berliner, 1998). Well suited to conductinghealth education and staff development training,this organized approach to learning requiresattention to the social environment, the behav-ior to be performed, and the individual learner(Bahn, 2001).
Reflecting a constructivist orientation,Bandura (2001) shifted his focus to socioculturalinfluences, viewing the learner as the agentthrough which learning experiences are filtered.As he argues, the human mind is not just re-active; it is generative, creative, and reflective.Essentially, the individual engages in a transac-tional relationship between the social environ-ment and the self, where sociocultural factors aremediated by “psychological mechanisms of theself-system to produce behavioral effects” (p. 4).In his model, Bandura stressed the internaldynamics of personal selection, intentionality,self-regulation, self-efficacy, and self-evaluationin the learning process. Culture and self-efficacyplay a key role, with Bandura noting that indi-vidualistic cultures interpret self-efficacy differ-ently than group-oriented cultures. Howeverdefined, a low sense of self-efficacy in eitherkind of culture produces stress. This perspectiveapplies particularly well to the acquisition ofhealth behaviors and partially explains whysome people select positive role models andeffectively regulate their attitudes, emotions,and actions, whereas other people choose nega-
tive role models and engage in unhealthy anddestructive behaviors. Healthcare professionalsneed to find ways to encourage patients’ feelingsof competency and to promote wellness ratherthan fostering dependency, helplessness, andfeelings of low self-worth.
The social learning theory extends the learn-ing process beyond the educator–learner rela-tionship to the larger social world. The theoryhelps explain the socialization process as well asthe breakdown of behavior in society. Respon-sibility is placed on the educator or leader to actas an exemplary role model and to choose sociallyhealthy experiences for individuals to observeand repeat (requiring the careful evaluation oflearning materials for stereotypes, mixed or hid-den messages, and negative effects). Yet simpleexposure to role models correctly performing abehavior that is rewarded (or performing someundesirable behavior that is punished) does notensure learning. Attention to the learner’s self-system and the dynamics of self-regulation mayhelp sort out the varying effects of the sociallearning experience.
In health care, social learning theory has beenapplied to nursing education, to addressing psy-chosocial problems, and to maximizing the useof support groups. For example, research indi-cates that those managers who are aware of theirroles and responsibilities in promoting a positivework environment enhance learning, compe-tence, and satisfaction; dissatisfaction, of course,has a detrimental effect and is a significant causeof staff turnover (Kane-Urrabazo, 2006). Nurseshave applied social learning principles success-fully when working with teenage mothers(Stiles, 2005) and in addressing alcoholismamong older adults (Akers, 1989). A major dif-ficulty is that this theory is complex and not eas-ily operationalized, measured, and assessed.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 69

70 Chapter 3: Applying Learning Theories to Healthcare Practice
The final two theories to be reviewed in thischapter focus on the importance of emotions andfeelings in the learning process.
Psychodynamic LearningTheoryAlthough not typically treated as a learningtheory, some of the constructs from the psy-chodynamic theory (based on the work ofSigmund Freud and his followers) have signif-icant implications for learning and changingbehavior (Hilgard & Bower, 1966; Slipp,2000). Largely a theory of motivation stressingemotions rather than cognition or responses,the psychodynamic perspective emphasizes theimportance of conscious and unconscious forcesin guiding behavior, personality conflicts, andthe enduring effects of childhood experiences.As Pullen (2002) pointed out, negative emo-tions are important to recognize and assess innurse–patient–doctor–family interactions, andthe psychodynamic theory can be helpful in thisregard.
A central principle of the theory is thatbehavior may be conscious or unconscious—thatis, individuals may or may not be aware of theirmotivations and why they feel, think, and act asthey do. According to the psychodynamic view,the most primitive source of motivation comesfrom the id and is based on libidinal energy (thebasic instincts, impulses, and desires we areborn with), which includes eros (the desire forpleasure and sex, sometimes called the “lifeforce”) and thanatos (aggressive and destructiveimpulses, or death wish). Patients who surviveor die despite all predictions to the contrary pro-vide illustrations of such primitive motivations.The id, according to Freud, operates on the basisof the pleasure principle—to seek pleasure and
avoid pain. For example, dry, dull lectures givenby nurse educators who go through the motionsof the presentation without much enthusiasm oremotion inspire few people (patients, staff, orstudents) to listen to the information or heedthe advice being given. This does not mean,however, that only pleasurable presentationswill be acceptable.
The id (primitive drives) and superego (inter-nalized societal values and standards, or the con-science) are mediated by the ego, which operateson the basis of the reality principle—rather thaninsisting on immediate gratification, people learnto take the long road to pleasure and to weigh thechoices or dilemmas in the conflict between the idand superego. Healthy ego (self) development, asemphasized by Freud’s followers, is an importantconsideration in the health fields. For example,patients with ego strength can cope with painfulmedical treatments because they recognize thelong-term value of enduring discomfort and painto achieve a positive outcome. Patients with weakego development, in contrast, may miss theirappointments and treatments or engage in short-term pleasurable activities that work against theirhealing and recovery. Helping patients developego strength and adjust realistically to a changedbody image or lifestyle brought about by diseaseand medical interventions is a significant aspectof the learning and healing process. Nurses andother health professionals, too, require personalego strength to cope with the numerous predica-ments in the everyday practice of delivering careas they face conflicting values, ethics, and de-mands. Professional burnout, for example, isrooted in an overly idealized concept of thehealthcare role and unrealistic expectations forthe self in performing the role. Malach-Pines(2000) notes that burnout may stem from nurses’childhood experiences with lack of control.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 70

Learning Theories 71
When the ego is threatened, as can easilyoccur in the healthcare setting, defense mechanismsmay be employed to protect the self. The short-term use of defense mechanisms is a way of com-ing to grips with reality. The danger comes inthe overuse or long-term reliance on defensemechanisms, which allows individuals to avoidreality and may act as a barrier to learning andtransfer. Table 3–2 describes some of the morecommonly used defense mechanisms. Because ofthe stresses involved in health care, knowledgeof defense mechanisms is useful, whether nurs-ing students are grappling with the challengesof nursing education, staff nurses are dealingwith the strains of working in hospitals andlong-term care facilities, or patients and theirfamilies are learning to cope with illness.
As an example of defense mechanisms inhealth care, Kübler-Ross (1969) pointed outthat many terminally ill patients’ initial reaction
to being told they have a serious threat to theirhealth and well-being is to employ the defensemechanism of denial. It is too overwhelming forpatients to process the information that they arelikely to die. While most patients graduallyaccept the reality of their illness, the dangers arethat if they remain in a state of denial, they maynot seek treatment and care, and if their illnessis contagious, they may not protect othersagainst infection. In turn, a common defensemechanism employed by healthcare staff is tointellectualize rather than deal realistically at anemotional level with the significance of diseaseand death. For example, one study reported thatnurses may strive too quickly to classify termi-nally ill patients within a denial-acceptanceframework and, as a result, may not listen topatients attempting to tell their stories andinterpret their illness experiences (Telford,Kralik, & Koch, 2006). Protecting the self (ego)
Table 3–2 Ego Defense Mechanisms: Ways of Protecting the Selffrom Perceived Threat
Denial: ignoring or refusing to acknowledgethe reality of a threat
Rationalization: excusing or explaining away athreat
Displacement: taking out hostility and aggres-sion on other individuals rather than directinganger at the source of the threat
Depression: keeping unacceptable thoughts,feelings, or actions from conscious awareness
Regression: returning to an earlier (less mature,more primitive) stage of behavior as a way ofcoping with a threat
Intellectualization: minimizing anxiety byresponding to a threat in a detached, abstractmanner without feeling or emotion
Projection: seeing one’s own unacceptablecharacteristics or desires in other people
Reaction formation: expressing or behaving theopposite of what is really felt
Sublimation: converting repressed feelings intosocially acceptable action
Compensation: making up for weaknesses byexcelling in other areas
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 71

72 Chapter 3: Applying Learning Theories to Healthcare Practice
by dehumanizing patients and treating them asdiseases and body parts rather than as wholeindividuals (with spiritual, emotional, andphysical needs) are occupational hazards fornurses and other health professionals.
Another central assumption of the psychody-namic theory is that personality developmentoccurs in stages, with much of adult behaviorderived from earlier childhood experiences andconflicts. One of the most widely used models ofpersonality development is Erikson’s (1968) eightstages of life, organized around a psychosocial cri-sis to be resolved at each stage (see Chapter 5).Treatment regimens, communication, and healtheducation need to include considerations of thepatient’s stage of personality development. Forexample, in working with 4- and 5-year-oldpatients, where the crisis is initiative versus guilt,health professionals should encourage the chil-dren to offer their ideas and to make and dothings themselves. Staff also must be careful notto make these children feel guilty for their illnessor misfortune. As a second example, the adoles-cent’s psychosocial developmental needs to havefriends and to find an identity require specialattention in health care. Adolescent patients maybenefit from help and support in adjusting to achanged body image and in addressing their fearsof weakness, lack of activity, and social isolation.One danger is that young people may treat theirillness or impairment as a significant dimensionof their identity and self-concept—well describedin poet Lucy Grealy’s personal account in Anatomyof a Face (1994).
According to the psychodynamic view, per-sonal difficulties arise and learning is limitedwhen individuals become fixated or stuck at anearlier stage of personality development. Theythen must work through their previously unre-solved crises to develop and mature emotionally.
For example, some staff members and patients feelan inordinate need to control the self, other peo-ple, and certain social situations. This behaviormay be rooted in their inability to resolve the cri-sis of trust versus mistrust at the earliest stage oflife. In working with these individuals, it is essen-tial to build a trusting relationship and to encour-age them gradually to relinquish some control.
Past conflicts, especially during childhood,may interfere with the ability to learn or totransfer learning. What people resist talkingabout or learning, termed resistance, is an indi-cator of underlying emotional difficulties, whichmust be dealt with for them to move aheademotionally and behaviorally. For instance, ayoung, pregnant teenager who refuses to engagein a serious conversation about sexuality (e.g.,changes the subject, giggles, looks out intospace, expresses anger) indicates underlyingemotional conflicts that need to be addressed.One study explored psychodynamic sources ofresistance among nursing students and how theyengaged with or resisted the learning process. Anumber of factors requiring consideration sur-faced, including childhood struggles, a historyof overadaptation, self-image, and learning cli-mate (Gilmartin, 2000).
Serious problems in miscommunication canoccur in health care as a result of childhoodlearning experiences. For example, some physi-cians and nurses may have had the childhoodexperience of standing helplessly by watchingsomeone they loved and once depended onendure disease, suffering, and death. Althoughthey could do little as children to improve thesituation, they may be compensating for theirchildhood feelings of helplessness and depen-dency as adults by devoting their careers to fend-ing off and fighting disease and death. Thesemotivations, however, may not serve them well
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 72

Learning Theories 73
as they attempt to cope, communicate, and edu-cate dying patients and their families.
Emotional conflicts are not always due to inter-nal forces; society exerts pressures on individualsthat promote emotional difficulties as well. Thereluctance of health professionals to be open andhonest with a terminally ill patient partially maybe derived from American culture, which encour-ages medical personnel to fix their patients andextend life. Staff members may or may not be con-scious of these pressures, but either way they arelikely to feel guilty and that they are failures whendealing with a dying patient.
The concept of transfer has special meaningto psychodynamic theorists. Transference occurswhen individuals project their feelings, con-flicts, and reactions—especially those developedduring childhood with significant others suchas parents—onto authority figures and otherindividuals in their lives. The danger is that therelationship between the health professional andthe patient may become distorted and unrealis-tic because of the biases inherent in the trans-ference reaction. For example, because patientsare sick, they may feel helpless and dependentand then regress to an earlier stage in life whenthey relied on their parents for help and support.Their childhood feelings and relationship witha parent—for better or worse—may be trans-ferred to a nurse or physician taking care ofthem. While sometimes flattering, the love anddependency that patients feel may operateagainst the autonomy and independence neededto get back on their feet. A particular patientmay also remind a staff member of someonefrom her or his past, creating a situation ofcountertransference.
The psychodynamic approach reminds healthprofessionals to pay attention to emotions,unconscious motivations, and the psychological
growth and development of all those involved inhealth care and learning. Health care rests onboth interpersonal and intrapersonal processesinvolved in the therapeutic use of the self in car-rying out patient care (Gallop & O’Brien,2003). Psychodynamic theory is well suited tounderstanding patient and family noncompli-ance (Menahern & Halasz, 2000), trauma andloss (Duberstein & Masling, 2000), palliativecare and the deeply emotional issues of terminalillness (Chochinov & Breitbart, 2000), and theanxieties of working with long-term psychiatricresidents (Goodwin & Gore, 2000). From a pro-fessional perspective, when examining the prob-lems of bullying nurse managers or the failureof nurses to formally report incidents of violenceand aggression, results indicated the need toconsider childhood and adult experiences withabuse and violence, as well as guilt, low self-image, and cultural expectations about nurses(Ferns, 2006).
The psychodynamic approach has been criti-cized because much of the analysis is speculativeand subjective, and the theory is difficult tooperationalize and measure. Psychodynamictheory also can be used inappropriately; it is notthe job of health professionals with little clini-cal psychology or psychiatric training to probeinto the private lives and feelings of patients soas to uncover deep, unconscious conflicts.Another danger is that health professionals maydepend on the many psychodynamic constructsas a way of intellectualizing or explaining away,rather than dealing with, people as individualswho need emotional care.
Humanistic Learning TheoryUnderlying the humanistic perspective onlearning is the assumption that each individualis unique and that all individuals have a desire
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 73

74 Chapter 3: Applying Learning Theories to Healthcare Practice
to grow in a positive way. Unfortunately, posi-tive psychological growth may be damaged bysome of society’s values and expectations (e.g.,males are less emotional than females, some eth-nic groups are inferior to others, making moneyis more important than caring for people) andby adults’ mistreatment of their children andeach other (e.g., inconsistent or harsh discipline,humiliation and belittling, abuse and neglect).Spontaneity, the importance of emotions andfeelings, the right of individuals to make theirown choices, and human creativity are the cor-nerstones of a humanistic approach to learning(Rogers, 1994; Snowman & Biehler, 2006).Humanistic theory is especially compatible withnursing’s focus on caring and patient centered-ness—an orientation that is increasingly chal-lenged by the emphasis in medicine and healthcare on science, technology, cost efficiency, for-profit medicine, bureaucratic organization, andtime pressures.
Like the psychodynamic theory, the human-istic perspective is largely a motivational theory.From a humanistic perspective, motivation isderived from each person’s needs, subjectivefeelings about the self, and the desire to grow.The transfer of learning is facilitated by curios-ity, a positive self-concept, and open situationsin which people respect individuality and pro-mote freedom of choice. Under such conditions,transfer is likely to be widespread, enhancingflexibility and creativity.
Maslow (1954, 1987), a major contributor tohumanistic theory, is perhaps best known foridentifying the hierarchy of needs (Figure 3–4),which he says plays an important role in humanmotivation. At the bottom of the hierarchy arephysiological needs (food, warmth, sleep); thencome safety needs; then the need for belongingand love; followed by self-esteem. At the top of
the hierarchy are self-actualization needs (max-imizing one’s potential). Additional considera-tions include cognitive needs (to know andunderstand) and, for some individuals, aestheticneeds (the desire for beauty). An assumption isthat basic-level needs must be met before indi-viduals can be concerned with learning and self-actualizing. Thus, clients who are hungry, tired,and in pain will be motivated to get these bio-logical needs met before being interested inlearning about their medications, rules for self-care, and health education. While intuitivelyappealing, research has not been able to supportMaslow’s hierarchy of needs with much consis-tency. For example, although some people’sbasic needs may not be met, they may nonethe-less engage in creative activities, extend them-selves to other people, and enjoy learning(Pfeffer, 1985).
Besides personal needs, humanists contendthat self-concept and self-esteem are necessaryconsiderations in any learning situation. Thetherapist Carl Rogers (1961, 1994) argued thatwhat people want is unconditional positive self-regard (the feeling of being loved withoutstrings attached). Experiences that are threaten-ing, coercive, and judgmental undermine theability and enthusiasm of individuals to learn.It is essential that those in positions of author-ity convey a fundamental respect for the peoplewith whom they work. If a health professionalis prejudiced against AIDS patients, then littlewill be healing or therapeutic in her relationshipwith them until she is genuinely able to feelrespect for the patient as an individual.
Rather than acting as an authority, sayhumanists, the role of any educator or leader isto be a facilitator (Rogers, 1994). Listening—rather than talking—is the skill needed.Because the uniqueness of the individual is fun-
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 74

Learning Theories 75
damental to the humanistic perspective, muchof the learning experience requires a direct rela-tionship between the educator and the learner,with instruction tailored to the needs, self-esteem, and positive growth of each learner.Learners, not educators, choose what is to belearned, and within this framework educatorsserve as resource persons whose job is to encour-age learners to make wise choices. Because thecentral focus is on learners’ perceptions, desires,and decision making, the humanistic orienta-
tion is referred to as a learner-directed approach(Snowman & Biehler, 2006).
Mastering information and facts is not the cen-tral purpose of the humanistic model of learning.Instead, fostering curiosity, enthusiasm, initia-tive, and responsibility is much more importantand enduring and should be the primary goal ofany educator. Rather than inserting health edu-cation videos into television sets for hospitalpatients to view or routinely distributing lots ofpamphlets and pages of small-print instructions,
Self-Actualizationneed to fulfill one’s potential
Esteemneed to be perceived as competent,have confidence and independence,
and have status, recognition, and appreciation
Safetyneed for security, stability, structure, and protection
as well as freedom from fear
Belonging and Loveneed to give and receive affection
Physiologicalto have basic survival needs met
(food, water, warmth, sleep)
Figure 3–4 Maslow’s hierarchy of needs.
Source: Adapted from Maslow (1987).
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 75

76 Chapter 3: Applying Learning Theories to Healthcare Practice
the humanist perspective would suggest estab-lishing rapport and becoming emotionally at-tuned to patients and their family members. Inprofessional education, the goal is to providepsychologically safe classrooms and clinicalenvironments, where humanistic principles canbe taught through caring, role modeling, small-group discussion, case discussions, attention toself-awareness and feelings, role playing, andvideotaping students in the clinical setting fol-lowed by feedback and reflection (Biderman,2003). Providing time for student reflection isessential, and instructor feedback must be givensensitively and thoughtfully (Fryer-Edwards,Arnold, Baile, Tulsky, Petracca, & Back, 2006).
Humanistic psychology contends that feel-ings and emotions are the keys to learning, com-munication, and understanding. Humanistsworry that in today’s stressful society, people caneasily lose touch with their feelings, which setsthe stage for emotional problems and difficultiesin learning (Rogers, 1961). To humanists, “tellme how you feel” is a much more importantinstruction than “tell me what you think,” asthoughts and admonitions (the latter of whichRogers calls “the shoulds”) may be at odds withtrue feelings. Consider the implications of thefollowing statements: (1) a young person whosays, “I know I should go to medical school andbecome a doctor because I am smart and that iswhat my parents want, but I don’t feel comfort-able with sick people—I don’t even like them!”or (2) the dying patient who says, “I realize thatI am going to die and should be brave, but I feelso sad that I am losing my family, my friends,and my self; frankly, I am afraid of dying—allthe pain and suffering, being a burden—I’mscared!” In both cases, humanists would argue,the overriding factor that will affect the behav-ior of the young person and the dying patient istheir feelings, not their cognitions.
The humanistic learning theory has modifiedthe approach to education and changing behav-ior by giving primary focus to the subjectiveneeds and feelings of the learner and by redefiningthe role of the educator. Humanistic principles havebeen a cornerstone of self-help groups, wellness pro-grams, and palliative care. Humanistic theory hasalso been found to be well suited to working withchildren and young patients undergoing separationanxiety due to illness, surgery, and recovery (Holy-oake, 1998) and for working in the areas of mentalhealth and palliative care (Barnard, Hollingum, &Hartfiel, 2006). Similar to psychodynamic theory,a principal emphasis is on the healing nature of thetherapeutic relationship (Pearson, 2006) and the needfor nursing students and health professionals togrow emotionally from their healthcare experiences(Block & Billings, 1998).
The humanistic theory has its weaknesses aswell. Research has not been able to substanti-ate some of its strongest claims, and the theoryhas been criticized for promoting self-centeredlearners who cannot take criticism or compro-mise their deeply felt positions. Charged withbeing more of a philosophy—or a cult—than ascience, the touchy-feely approach of humanistsmakes some learners and educators feel trulyuncomfortable. Moreover, information, facts,memorization, drill, practice, and the tediouswork sometimes required to master knowledge,which humanists minimize and sometimes dis-dain, have been found to contribute to signifi-cant learning, knowledge building, and skilldevelopment (Gage & Berliner, 1992).
Neuropsychology andLearning One of the newest and most rapidly growingareas of psychology research involves investiga-tions into the physiological and neurological
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 76

Neuropsychology and Learning 77
bases of thinking, learning, and behavior. Neu-roscience research has implications for learningin several ways: (1) by documenting the dynam-ics of brain and central nervous system process-ing of information; (2) by understanding andworking with children and adults who have neu-rological conditions, face mental health issues, orhave learning disabilities; (3) by answering ques-tions about the relationship between stress andlearning; and (4) by providing evidence to sup-port the assumptions of various learning theoriesor the integration of these theories.
Much of the information in these areas hasbeen gained through advances in neuroimagingtechniques such as functional magnetic reso-nance imaging (fMRI) and positron emissiontomography (PET). Other methodologies in-clude animal studies based on surgery, electricalrecordings (EEG and ERP), and case studies ofchildren and adults with head trauma, brainlesions, and neurological abnormalities (Byrnes,2001). While the research findings highlightsome of the underlying biological mechanismsof learning and provide evidence to support someof the principal constructs and dynamics of exist-ing learning theories, there is as yet no coherentphysiological or neuropsychological theory oflearning.
In synthesizing neuropsychology research,some generalizations about learning can be made(Anderson, 1997; Gazzaniga, 2000; Page, 2006;Phelps, 2006; Shors, 2006; Silverstein & Uhlhaas,2004). Each generalization, listed below, hasimplications for health education in the clinicalsetting, and readers are encouraged to formulateapplications to nursing and health care.
• Emotions have been found to play a keyrole in Pavlovian conditioning, informa-tion processing, memory, and motiva-tion. Emotions are considered to
interact with cognitive factors in anylearning situation, suggesting that theycannot be ignored when teaching, learn-ing, reasoning, or making decisions.
• Neuropsychology studies of learninghave confirmed a number of learningtheories and constructs, including gestaltprinciples, constructivism, Piaget’snotions of assimilation and accommoda-tion, and Freud’s conceptualization ofconscious and unconscious processes.Neurological studies also have docu-mented physiological arousal and trackedattention, perception, and the organiza-tion of experience while learning.
• Learning is a function of physiologicaland neurological developmental changesthat are ongoing and dynamic; the brainis less fixed than once thought, and itchanges with learning and experience(called “plasticity”).
• Brain processing is different for eachlearner; thus, gaining the learner’sattention, controlling the pace of learn-ing, and identifying the specific mecha-nisms for enhancing learning are uniquefor each person.
• Learning is an active, multifaceted,complex process that involves preferredand interacting sensory modes, is col-ored by the past and present social con-text, and is regulated largely by thelearner on the basis of his or her devel-opment, experiences, and sense of self.
• Meaningful practice strengthens learn-ing connections, which may fade fromlack of use; thus, one-shot patient edu-cation efforts are not likely to be effec-tive in changing behavior.
• Stress can interfere with or stimulatelearning, although the responses to
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 77

78 Chapter 3: Applying Learning Theories to Healthcare Practice
stress may change with age and differfor males and females, or for those whohave experienced traumatic events.
Neurophysiological aspects of learningbecome all the more germane for children andadults with physiological disorders; for thosewith mental, emotional, and behavioral prob-lems; and for those facing the stresses of trauma,disease, disability, and socioeconomic hardship.Despite numerous neuroscientific studies re-lated to learning, the research is in its earlystages and remains fragmented, scattered, andlacking in integration. In addition, neuropsy-chological studies are often based on animalresearch or on highly specialized and restrictedhuman samples, so few generalizations can bemade about most people. Although addressingthe various biological connections to learning iscurrently a popular and relatively well-fundedarea of research, there is a risk of reducinghuman behavior to mere biology while ignoringthe individual as a person as well as the signifi-cance and complexity of psychological and socialprocesses in any learning situation.
Comparison of Learning TheoriesTable 3–3 provides a comparative summary ofthe five learning theories outlined in this chap-ter. Generalizations can be made about boththe differences and the similarities in what thetheories say about acquiring knowledge andchanging feelings, attitudes, and behavior.With regard to some of the differences amongthe theories, each theory has its own assump-tions, vocabulary, and way of conceptualizingthe learning process. The theories differ intheir emphasis on the relative influence of ex-ternal or internal factors in learning, the view
of the learner as more passive or active, the taskof the educator, the explanation of motivation,and the way in which the transfer of learningis accomplished.
A logical question is which of these five the-ories best describes or explains learning—whichtheory, in other words, would be the most help-ful to health professionals interested in increas-ing knowledge or changing the behavior ofpatients, staff, or themselves? The answer to thisquestion is that each theory contributes tounderstanding various aspects of the learningprocess and can be used singly or in combina-tion to help practitioners acquire new informa-tion and alter existing thoughts, feelings, andbehavior.
Each theory gives focus to important consid-erations in any learning situation, involving theconsideration of external social factors and inter-nal psychological processing. For example,behaviorists urge us to pay attention to andchange stimulus conditions and to provide rein-forcement to alter behavior. While criticized forbeing reductionistic, behaviorists’ emphasis onmanipulating the environment and reinforce-ments is admittedly simpler and easier than try-ing to undertake a massive overhaul of anindividual’s internal dynamics (perceptions, cog-nition, memory, feelings, and personality historyand conflicts). Moreover, getting someone firstto behave in a more appropriate way (abstainingfrom bad habits and engaging in healthy behav-ior) may not be as threatening or daunting to thelearner as it would be to suggest the need forinternal personality changes. Desired responsesare modified and strengthened through practice;the new learned responses, in turn, may lead tomore fundamental changes in attitudes and emo-tions. The social learning perspective is anotherrelatively simple theory to use, stressing theimportance of effective role models, who, by
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 78

Comparison of Learning Theories 79
Tabl
e 3–
3Su
mm
ary
of
Lea
rnin
g T
heo
ries
Lea
rnin
g A
ssu
mp
tion
s A
bou
t E
du
cato
r’s
Sou
rces
of
Tra
nsf
er o
f P
roce
du
res
the
Lea
rner
Tas
kM
otiv
atio
nL
earn
ing
Env
iron
men
tal s
tim
ulus
co
ndit
ions
and
rei
nfor
ce-
men
t pr
omot
e ch
ange
s in
res
pons
es.
To c
hang
e be
havi
or,
chan
ge t
he e
nvir
onm
ent.
Inte
rnal
per
cept
ion
and
thou
ght
proc
essi
ng w
ithi
n co
ntex
t of
hum
an d
evel
-op
men
t pr
omot
e le
arni
ng
and
chan
ge.
To c
hang
e be
havi
or, c
hang
eco
gnit
ions
.
Ext
erna
l rol
e m
odel
s an
dth
eir
perc
eive
d re
info
rce-
men
t al
ong
wit
h le
arne
r’sin
tern
al in
flue
nces
.
To c
hang
e be
havi
or, c
hang
ero
le m
odel
s, p
erce
ived
rein
forc
emen
t, a
nd t
hele
arne
r’s s
elf-
regu
lati
ngm
echa
nism
s.
Pas
sive
, rea
ctiv
e le
arne
r re
spon
ds
to e
nvir
onm
enta
l co
ndit
ions
(sti
mul
i an
d re
info
rcem
ent)
.
Act
ive
lear
ner
dete
r-m
ines
pat
tern
ing
of e
xper
ienc
es; i
sst
rong
ly in
flue
nced
by
att
ribu
tion
s.
Act
ive
lear
ner
obse
rves
oth
ers
and
regu
late
s de
cisi
on t
ore
prod
uce
beha
vior
.
Beh
avio
rist
Act
ive
educ
ator
man
ipu-
late
s st
imul
i and
rei
n-fo
rcem
ent
to d
irec
tle
arni
ng a
nd c
hang
e.
Cog
nit
ive
Act
ive
educ
ator
str
uc-
ture
s ex
peri
ence
s(t
hrou
gh o
rgan
izat
ion
and
mea
ning
fuln
ess)
to
enco
urag
e th
e re
orga
ni-
zati
on o
f cog
niti
ons.
Soci
al L
earn
ing
Act
ive
educ
ator
mod
els
beha
vior
, enc
oura
ges
perc
epti
on o
f rei
nfor
ce-
men
t, c
aref
ully
eva
luat
esle
arni
ng m
ater
ials
for
soci
al m
essa
ges,
and
atte
mpt
s to
infl
uenc
ele
arne
r’s s
elf-
regu
lati
on.
Dri
ve r
educ
tion
.
Goa
ls.
Exp
ecta
tion
s.
Dis
equi
libr
ium
.
Soci
aliz
atio
n ex
peri
ence
s,ro
le m
odel
s, a
nd s
elf-
reac
tive
infl
uenc
es(o
bser
ve s
elf,
set
goal
s,an
d re
info
rce
perf
orm
ance
).
Pra
ctic
e; s
imil
arit
y in
st
imul
us c
ondi
tion
s an
d re
spon
ses
betw
een
lear
ning
and
new
si
tuat
ions
.
Men
tal a
nd p
hysi
cal
acti
vity
.
Com
mon
pat
tern
s.
Und
erst
andi
ng.
Lear
ning
to
lear
n.
Sim
ilar
ity
of s
etti
ng
and
role
mod
els’
be
havi
or. co
ntin
ues
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 79

80 Chapter 3: Applying Learning Theories to Healthcare Practice
Tabl
e 3–
3Su
mm
ary
of
Lea
rnin
g T
heo
ries
(co
nti
nu
ed)
Lea
rnin
g A
ssu
mp
tion
s A
bou
t E
du
cato
r’s
Sou
rces
of
Tra
nsf
er o
f P
roce
du
res
the
Lea
rner
Tas
kM
otiv
atio
nL
earn
ing
Inte
rnal
forc
es s
uch
asde
velo
pmen
tal s
tage
,ch
ildh
ood
expe
rien
ces,
emot
iona
l con
flic
ts, a
ndeg
o st
reng
th in
flue
nce
lear
ning
and
cha
nge.
To c
hang
e be
havi
or,
chan
ge in
terp
reta
tion
san
d m
ake
unco
nsci
ous
mot
ivat
ions
con
scio
us.
Inte
rnal
feel
ings
abo
utse
lf, a
bili
ty t
o m
ake
wis
ech
oice
s, a
nd n
eeds
aff
ect
lear
ning
and
cha
nge.
To c
hang
e be
havi
or, c
hang
efe
elin
gs, s
elf-
conc
ept,
and
need
s.
Act
ive
lear
ner’s
life
styl
e,pa
st e
xper
ienc
es, a
ndcu
rren
t em
otio
nal c
on-
flic
ts in
flue
nce
wha
t is
lear
ned
and
how
it is
rem
embe
red
and
perf
orm
ed.
Act
ive
lear
ner
atte
mpt
s to
actu
aliz
e po
tent
ial f
orpo
siti
ve s
elf-
grow
th a
ndco
nfir
m s
elf-
conc
ept;
issp
onta
neou
s, c
reat
ive,
and
play
ful.
Psy
chod
ynam
icE
duca
tor
as a
ref
lect
ive
inte
rpre
ter
mak
es s
ense
of
lear
ner’s
per
sona
lity
an
d m
otiv
atio
n by
list
en-
ing
and
posi
ng q
uest
ions
to s
tim
ulat
e co
nsci
ous
awar
enes
s, in
sigh
t, a
ndeg
o st
reng
th.
Hu
man
isti
cFa
cili
tati
ve e
duca
tor
enco
urag
es p
osit
ive
self
-gr
owth
, lis
tens
em
path
-et
ical
ly, a
llow
s fr
eedo
m
of c
hoic
e, a
nd r
espe
cts
lear
ner.
Ple
asur
e pr
inci
ple
and
real
ity
prin
cipl
e.
Imba
lanc
e.
Con
scio
us a
nd u
ncon
-sc
ious
infl
uenc
e of
con
-fl
ict,
dev
elop
men
t, a
ndde
fens
e m
echa
nism
s.
Nee
ds, d
esir
e fo
r po
siti
vese
lf-g
row
th, a
nd c
onfi
r-m
atio
n of
sel
f-co
ncep
t.
Per
sona
lity
con
flic
t,re
sist
ance
, and
tra
nsfe
r-en
ce a
ssoc
iate
d w
ith
lear
ning
sit
uati
ons
may
act
as b
arri
er.
Pos
itiv
e or
neg
ativ
e fe
el-
ings
abo
ut s
elf a
ndfr
eedo
m t
o le
arn
pro-
mot
e or
inhi
bit
tran
sfer
.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 80

Common Principles of Learning 81
their example, demonstrate exactly what behav-ior is expected.
Cognitive, social learning, psychodynamic,and humanistic theories remind us to considerinternal factors—perceptions, thoughts, ways ofprocessing information, feelings, and emotions.These factors cannot be ignored because, ulti-mately, it is the learner who controls and regu-lates learning: how information is perceived,interpreted, and remembered, and whether thenew knowledge is expressed or performed.
In practice, learning theories should not beconsidered to be mutually exclusive but ratherto operate together to change attitudes andbehavior. For example, patients undergoingpainful procedures are first taught systematicdesensitization (behaviorist) and while experi-encing pain or discomfort are encouraged toemploy imagery, such as thinking about afavorite, beautiful place or imagining thehealthy cells gobbling up the unhealthy cells(cognitive). Staff members are highly respectful,upbeat, and emotionally supportive of eachpatient (humanistic) and create the time andopportunity to listen to patients discuss some oftheir deepest fears and concerns (psychody-namic). Waiting rooms and lounge areas forpatients and their families are designed to becomfortable, friendly, and pleasant to facilitateconversation and interaction, while supportgroups may help patients and family memberslearn from each other about how to cope withillness or disability and how to regulate theiremotions so that their health is not further com-promised (social learning).
Another generalization from this discussionis that some learning theories are better suitedto certain kinds of individuals than to others.While theoretical assumptions about the learnerrange from passive to highly active, passive indi-viduals may learn more effectively from behav-
iorist techniques, whereas curious, highly active,and self-directed persons may do better withcognitive and humanistic approaches. Also,keep in mind that some learners require exter-nal reinforcement and incentives, whereas otherlearners do not seem to need—and may evenresent—attempts to manipulate and reinforcethem.
Individuals who are well educated, verbal,and reflective may be better candidates for cog-nitive and psychodynamic approaches, whereasbehaviorist approaches may be more suitable forpersons whose cognitive processes are impairedor who are uncomfortable dealing with abstrac-tions or scrutinizing and communicating theirthoughts and emotions.
In addition, each individual’s preferred modesof learning and processing may help determinethe selection of suitable theoretical approaches.That is, while some individuals learn by actingand responding (behaviorist), the route to learn-ing for others may be through perceptions andthoughts (cognitive) or through feelings andemotions (humanistic and psychodynamic).Most people appear to benefit from demonstra-tion and example (social learning).
Common Principles ofLearningTaken together, the theories discussed in thischapter indicate that learning is a more compli-cated process than any one theory implies.Besides the distinct considerations for learningsuggested by each theory, the similarities amongthe perspectives point to some core features oflearning. The issues raised at the beginning ofthe chapter can be addressed by synthesizing thelearning theories and identifying their commonprinciples.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 81

82 Chapter 3: Applying Learning Theories to Healthcare Practice
1. How Does Learning Occur?Learning is an active process that takes place asindividuals interact with their environment andincorporate new information or experiences withwhat they already know or have learned. Factorsin the environment that affect learning includethe society and culture, the structure or patternof stimuli, the effectiveness of role models andreinforcements, feedback for correct and incor-rect responses, and opportunities to process andapply learning to new situations.
Furthermore, the individual exerts significantcontrol over learning, often involving consider-ations of his or her developmental stage, past his-tory (habits, cultural conditioning, socialization,childhood experiences, and conflicts), cognitivestyle, dynamics of self-regulation, conscious andunconscious motivations, personality (stage, con-flicts, and self-concept), and emotions. Also,learners often have a preferred mode for takingin information (visual, motor, auditory, or sym-bolic), and, while some individuals may learnbest on their own, others will benefit from ex-pert guidance, social interaction, and cooperativelearning.
Learning is an individual matter. Neuro-psychology research is beginning to documentthe uniqueness of each person’s way of activelyperceiving and processing information, his orher flexibility and reactions to stress, and theimpact of culture and emotions on how andwhat is learned.
A critical influence on whether learningoccurs is motivation (see Chapter 6 on motiva-tion). The learning theories reviewed here sug-gest that to learn, the individual must want togain something (receive rewards and pleasure,meet goals and needs, confirm expectations,grow in positive ways, or resolve conflicts),
which, in turn, arouses the learner by creatingtension (drives to be reduced, disequilibrium,and imbalance) and the propensity to act orchange behavior.
The relative success or failure of the learner’sperformance may affect subsequent learningexperiences. In some cases, an inappropriate,maladaptive, or harmful previously learnedbehavior may need to be extinguished and thenreplaced with a more positive response. It is, ofcourse, easier to instill new learning than to cor-rect faulty learning.
2. What Kinds of ExperiencesFacilitate or Hinder theLearning Process?The educator exerts a critical influence on learn-ing through role modeling, the selection oflearning theories, and how the learning experi-ence is structured for each learner. To be effec-tive, educators must have knowledge (of thematerial to be learned, the learner, the socialcontext, and educational psychology), and theymust be competent (be imaginative, flexible,and able to employ teaching methods; displaysolid communication skills; and have the abil-ity to motivate others).
All the learning theories discussed in thischapter acknowledge the need to recognize andrelate the new information to the learner’s pastexperiences (old habits, culture, familiar pat-terns, childhood memories, feelings about theself, and what is valued, normative, and per-ceived as successful or rewarded in society). Theultimate control over learning rests with thelearner, but effective educators influence andguide the process so that learners advance intheir knowledge, perceptions, thoughts, emo-tional maturity, and behavior.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 82

State of the Evidence 83
Ignoring these considerations, of course, mayhinder learning. Other impediments to learningmay involve a lack of clarity and meaningfulnessin what is to be learned, neglect or harsh pun-ishment, fear, or negative or ineffective rolemodels. Providing inappropriate materials forthe individual’s ability, readiness to learn, orstage of life-cycle development is another obsta-cle to learning. Moreover, individuals areunlikely to want to learn if they have had detri-mental socialization experiences, are deprived ofstimulating environments, and are withoutgoals and realistic expectations for themselves.
3. What Helps Ensure ThatLearning Becomes RelativelyPermanent?Four considerations assist learning in becomingpermanent. First, the likelihood of learning isenhanced by organizing the learning experience,making it meaningful and pleasurable, recogniz-ing the role of emotions in learning, and by pac-ing the presentation in keeping with the learner’sability to process information. Second, practicing(mentally and physically) new knowledge orskills under varied conditions strengthens learn-ing. The third issue concerns reinforcement.Although reinforcement may or may not be nec-essary, some theorists have argued that it may behelpful because it serves as a signal to the indi-vidual that learning has occurred.
A fourth consideration involves whetherlearning transfers beyond the initial educationalsetting. Learning cannot be assumed to be rela-tively lasting or permanent; it must be assessedand evaluated by the educator soon after thelearning experience has occurred as well as byfollow-up measurements at later times. Researchskills, knowledge of evaluation procedures, and
the willingness and resources to engage in edu-cational assessment are now considered essentialresponsibilities of the educator in carrying outthe teaching/learning process. Evaluation feed-back can then be used by the nurse educator torevamp and revitalize learning experiences.
State of the EvidenceThe study of learning in educational psychologyis based on evidence from research similar tothat advocated in nursing, medicine, and healthcare. Rather than assuming the instructorknows best, we gather evidence and test learn-ing theories, teaching methods, and what isbelieved to be true about learners, teachers, andthe environment. The research results are thenevaluated for the purpose of modifying the the-ories, methods, and assumptions about learning.
Ideally in health education, existing researchin psychology, nursing, and medicine is used todesign learning experiences for patients, families,and communities. The same is true for develop-ing, implementing and evaluating teaching andlearning experiences for nursing students andstaff. On the basis of the research findings, whatdoes not work is eliminated, modifications aremade grounded in additional research, and newprograms are attempted and assessed. Educa-tional accountability is stressed, and decisionsabout how to educate must be justified on thebasis of data and research.
The applications of the learning theories andprinciples discussed in this chapter are illus-trated by a number of research studies in nurs-ing, psychology, education, and health care. It isthe research that has allowed us to gain someconfidence about choosing the most appropriatetheories and principles for each educational expe-rience, and it is the research that has helped us
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 83

84 Chapter 3: Applying Learning Theories to Healthcare Practice
hone our approach to teaching and learning inthe healthcare setting. Educational research hasconfirmed many of the constructs and principlesfrom the various learning perspectives. It also hasprovided evidence to dispute some of the con-ventional wisdom and myths about learning—helping us realize that punishment is notgenerally effective and may inhibit learning;males are not necessarily more intelligent thanfemales; and when teaching people, there are anumber of strongly held realities that may ormay not be rational, which strongly influenceeach learner’s processing of the educational expe-rience. The research on learning in general andhealth care in particular clearly demonstratesthere is no one-size-fits-all approach to educat-ing patients, nursing students, or nursing staff.To be effective, educational experiences need tobe refined and tailored to each individual learner.
Though many advancements have been madein understanding the learning process over thepast century, much remains unknown and re-quires careful research, such as why some pa-tients and nursing students are so much moreeager to learn than others, what can be done toencourage reluctant learners to change theirattitudes or behavior, how the various learningtheories and principles can work together forevery learner, and how the healthcare settingchanges the teaching/learning situation. In thefuture, more interdisciplinary efforts betweenpsychologists and nurses are needed to move ustoward a more sophisticated level of researchand understanding that can be applied to thehealthcare setting.
Research is not a panacea, however. Criticscharge that the widely promoted research-based evidence approach to education andhealth care is jargonistic, places the emphasison outcomes rather than on the process oflearning, and oversimplifies the complexity of
learning in any attempt to measure and evalu-ate it. The challenges of measurement areimmense and require a highly sophisticatedknowledge of research methods and theirweaknesses. Another problem is the lack ofresources, support, and well-trained personnelneeded to truly implement and sustain aresearch-based approach to teaching and learn-ing (Ferguson & Day, 2005).
SummaryThis chapter demonstrates that learning is com-plex. Readers may feel overwhelmed by thediverse theories, sets of learning principles, andcautions associated with employing the variousapproaches. Yet, like the blind men exploringthe elephant, each theory highlights an impor-tant dimension that affects the overall learningprocess, and together the theories provide awealth of complementary strategies and alter-native options. There is, of course, no single bestway to approach learning, although all the the-ories indicate the need to be sensitive to theunique characteristics and motivations of eachlearner. For additional sources of informationabout psychological theories of learning andhealth care, see Table 3–4.
Educators in the health professions cannot beexpected to know everything about the teachingand learning process. More importantly, perhaps,is that they can determine what needs to beknown, where to find the necessary information,and how to help individuals, groups, and them-selves benefit directly from a learning situation.Psychology and nursing work well together.Psychology has much to contribute to health-care practice, and nursing is in a strategic posi-tion to apply and test psychological principles,constructs, and theories in both the educationaland clinical settings.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 84

Summary 85
Table 3–4 Psychological Theories of Learning and Healthcare:Links
Internet Educational Psychology resources (ERIC):http://www.lib.muohio.edu/edpsych/internetresources.html
McMaster University: Evidence-based medicine links:http://www.mlanet.org/education/telecon/ebhc/resource.html
U.S. Department of Education: Evidence-Based Education help desk:http://www.whatworkshelpdesk.ed.gov
American Psychological Association (search for learning topics): http://www.apa.org
National Institutes of Health (search for patient education topics):http://www.nih.gov
Learning Theory Resources (Nova Southeastern University):http://www.nova.edu/~burmeist/learning_theory.html
Learning Theory links (emTech.net): http://www.emtech.net/learning_theories.htm
Nursing Patient Education resources (about.com):http://nursing.about.com/od/patienteducation/Patient_Education_Tools_and_Information_for_Nurses.htm
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 85

86 Chapter 3: Applying Learning Theories to Healthcare Practice
REVIEW QUESTIONS
1. What are the five major learning theories discussed in this chapter? 2. What are the principal constructs and contributions of each of the five learning theories?3. According to the concept of operant conditioning, what are three techniques to increase
the probability of a response, and what are two techniques to decrease or extinguish theprobability of a response?
4. What are some ways the behaviorist theory (which focuses on the environment andresponses to it) and the cognitive perspective (which emphasizes the individual’s inter-nal processing) could be combined to facilitate knowledge acquisition or change a healthbehavior?
5. What is meant by the term gestalt, and to which major learning theory is it associated?6. Which learning theory is a combination of the principles from both the behaviorist and
cognitive perspectives?7. Which perspective is based primarily on the theory of motivation and stresses emotions
rather than cognition and stimulus-response connections?8. How do the major learning theories compare to one another with regard to their sim-
ilarities and differences? 9. How does motivation serve as the critical influence on whether learning occurs or not?
10. What types of experiences may facilitate or hinder the learning process?11. What factors help ensure that learning becomes relatively permanent? 12. What are some ways that emotions might be given more explicit consideration in
nurses’ education and in patient education?13. How has neuroscience research contributed to our understanding of learning and learn-
ing theories?
Akers, R. L. (1989). Social learning theory and alcoholbehavior among the elderly. Sociological Quarterly,30, 625–638.
Anderson, O. R. (1997). A neurocognitive perspective oncurrent learning theory and science instructionalstrategies. Science Education, 81, 67–89.
Bahn, D. (2001). Social learning theory: Its applicationto the context of nurse education. Nurse EducationToday, 21, 110–117.
Bandura, A. (1977). Social learning theory. EnglewoodCliffs, NJ: Prentice-Hall.
Bandura, A. (2001). Social cognitive theory: An agenticperspective. Annual Review of Psychology, 52, 1–26.
Barnard, A., Hollingum, C., & Hartfiel, B. (2006).Going on a journey: Understanding palliative carenursing. International Journal of Palliative Nursing,12, 6–12.
Beck, M. H., Cataldo, M., Slifer, K. J., Pulbrook, V., &Guhman, J. K. (2005). Teaching children withattention deficit hyperactivity disorder (ADHD)and autistic disorder (AD) how to swallow pills.Clinical Pediatrics, 44, 515–526.
References
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 86

References 87
Berggren, I., & Severinsson, E. (2006). The significanceof nurse supervisors’ different ethical decision-making styles. Journal of Nursing Management, 14,637–643.
Biderman, A. (2003). Family medicine as a frame forhumanized medicine in education and clinicalpractice. Public Health Review, 31, 23–26.
Block, S., & Billings, J. A. (1998). Nurturing humanismthrough teaching palliative care. AcademicMedicine, 73, 763–765.
Brackett, M. A., Lopes, P. N., Ivcevic, Z., Mayer, J. D.,& Salovey, P. (2004). Integrating emotion andcognition: The role of emotional intelligence. InD. Y. Dai & R. J. Sternberg (Eds.), Motivation,emotion, and cognition: Integrative perspectives on intel-lectual functioning and development (pp. 175–194).Mahwah, NJ: Lawrence Erlbaum.
Bush, G. (2006). Learning about learning: From theoriesto trends. Teacher Librarian, 34, 14–18.
Byrnes, J. P. (2001). Minds, brains, and learning:Understanding the psychological and educational rele-vance of neuroscientific research. New York: Guilford.
Chochinov, H. M., & Breitbart, W. (Eds.). (2000).Handbook of psychiatry in palliative medicine. NewYork: Oxford University Press.
Dai, D. Y., & Sternberg, R. J. (Eds.). (2004). Motivation,emotion, and cognition: Integrative perspectives on intel-lectual functioning and development. Mahwah, NJ:Lawrence Erlbaum.
Deyl, S. G., & Kaliappan, K. V. (1997). Improvement ofpsychosomatic disorders among tension headachesubjects using behaviour therapy and somaticinkblot series. Journal of Projective Psychology andMental Health, 4, 113–120.
Duberstein, P. R., & Masling, J. M. (Eds.). (2000).Psychodynamic perspectives on sickness and health.Washington, DC: American PsychologicalAssociation.
Eccles, J. S., & Wigfield, A. (2002). Motivational beliefs,values, and goals. Annual Review of Psychology, 53,109–132.
Erikson, E. (1968). Identity: Youth and crisis. New York:Norton.
Ferguson, L., & Day, R. A. (2005). Evidence-based nurs-ing education: Myth or reality? Journal of NursingEducation, 44, 107–115.
Ferns, T. (2006). Under-reporting of violent incidentsagainst nursing staff. Nursing Standard, 20, 41–45.
Fiske, S. T., & Taylor, S. E. (1991). Social cognition. New York: McGraw-Hill.
Fryer-Edwards, K., Arnold, R. M., Baile, W., Tulsky, J. A., Petracca, F., & Back, A. (2006). Reflectiveteaching practices: An approach to teaching communication skills in a small-group setting.Academic Medicine, 81, 638–644.
Gage, N. L., & Berliner, D. C. (1992). Educational psychology (5th ed.). Boston: Houghton Mifflin.
Gage, N. L., & Berliner, D. C. (1998). Educational psychology (6th ed.). Boston: Houghton Mifflin.
Gagné, R. M. (1985). The conditions of learning (4th ed.).New York: Holt, Rinehart & Winston.
Gagné, R. M., Briggs, L. J., & Wagner, W. W. (1992).Principles of instructional design (4th ed.). FortWorth, TX: HBJ College Publishers.
Gallop, R., & O’Brien, L. (2003). Re-establishing psy-chodynamic theory as foundational knowledge forpsychiatric/mental health nursing. Issues in MentalHealth Nursing, 24, 213–227.
Gardner, H. (1978). Developmental psychology: An introduc-tion. Boston: Little, Brown.
Gazzaniga, M. S. (Ed.). (2000). The new cognitive neuro-sciences (2nd ed.). Cambridge, MA: MIT Press.
Gilmartin, J. (2000). Psychodynamic sources of resis-tance among student nurses: Some observations ina human relations context. Journal of AdvancedNursing, 32, 1533–1541.
Goleman, D. (1995). Emotional intelligence. New York:Bantam Books.
Goodwin, A. M., & Gore, V. (2000). Managing thestresses of nursing people with severe and endur-ing mental illness: A psychodynamic observationstudy of a long-stay psychiatric ward. BritishJournal of Medical Psychology, 73, 311–325.
Grealy, L. (1994). Anatomy of a face. Boston: HoughtonMifflin.
Greene, J. D., Sommerville, R. B., Nystrom, L. E.,Darley, J. M., & Cohen, J. D. (2001). An fMRIinvestigation of emotional engagement in moraljudgment. Science, 293, 2105–2108.
Halpern, J. (2001). From detached concern to empathy:Humanizing medical practice. New York: OxfordUniversity Press.
Hilgard, E. R. (1996). History of educational psychol-ogy. In D. C. Berliner & R. C. Calfee (Eds.),Handbook of educational psychology (pp. 990–1004).New York: Simon & Schuster Macmillan.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 87

88 Chapter 3: Applying Learning Theories to Healthcare Practice
Hilgard, E. R., & Bower, G. H. (1966). Theories of learning(3rd ed.). New York: Appleton-Century-Crofts.
Hoffman, M. L. (2000). Empathy and moral development:Implications for caring and justice. New York:Cambridge University Press.
Holyoake, D. D. (1998). A little lady called Pandora: Anexploration of philosophical traditions of human-ism and existentialism in nursing ill children.Child Care, Health and Development, 24, 325–336.
Hooyman, N., & Kiyak, H. A. (2005). Social gerontology(7th ed.). Boston: Allyn & Bacon.
Hunt, R. R., Ellis, H. C., & Ellis, H. (2004).Fundamentals of cognitive psychology (7th ed.). NewYork: McGraw-Hill.
Imes, S. A., Clance, P. R., Gailis, A. T., & Atkeson, E.(2002). Mind’s response to the body’s betrayal:Gestalt/existential therapy for clients with chronicor life-threatening illnesses. Journal of ClinicalPsychology, 58, 1361–1373.
Kane-Urrabazo, C. (2006). Management’s role in shapingorganizational culture. Journal of NursingManagement, 14, 188–194.
Kessels, R. P. C. (2003). Patients’ memory of medicalinformation. Journal of the Royal Society of Medicine,96, 219–222.
Kohler, W. (1947). Gestalt psychology. New York: MentorBooks.
Kohler, W. (1969). The task of gestalt psychology.Princeton, NJ: Princeton University Press.
Kramer, D. A. (1983). Post-formal operations? A needfor further conceptualization. Human Development,26, 91–105.
Kübler-Ross, E. (1969). On death and dying. New York:Macmillan.
Malach-Pines, A. (2000). Nurses’ burnout: An existentialpsychodynamic perspective. Journal of PsychosocialNursing and Mental Health Services, 38, 23–31.
Marshall, H. H. (1998). Teaching educational psychol-ogy: Learner-centered constructivist perspectives.In N. M. Lambert & B. L. McCombs (Eds.), Howstudents learn: Reforming schools through learner-centered education (pp. 449–473). Washington, DC:American Psychological Association.
Maslow, A. (1954). Motivation and personality. New York:Harper & Row.
Maslow, A. (1987). Motivation and personality (3rd ed.).New York: Harper & Row.
McCullough, L., & Andrews, S. (2001). Assimilativeintegration: Short-term dynamic psychotherapy
for treating affect phobias. Clinical PsychologyScience and Practice, 8, 82–97.
Menahern, S., & Halasz, G. (2000). Parental noncompli-ance—a paediatric dilemma: A medical and psychodynamic perspective. Child Care, Healthand Development, 26, 61–72.
Moskowitz, G. B. (2005). Social cognition: Understandingself and others. New York: Guilford.
Murray, D. J. (1995). Gestalt psychology and the cognitiverevolution. New York: Harvester Wheatsheaf.
Neary, M. (2000). Supporting students’ learning andprofessional development through the process ofcontinuous assessment and mentorship. NurseEducation Today, 20, 463–474.
Ormrod, J. E. (2004). Human learning (4th ed.). UpperSaddle River, NJ: Prentice-Hall.
Page, M. P. A. (2006). What can’t functional neuroimag-ing tell the cognitive psychologist? Cortex, 42,428–443.
Palincsar, A. S. (1998). Social constructivist perspectiveson teaching and learning. Annual Review ofPsychology, 49, 345–375.
Papadakis, A. A., Prince, R. P. O., Jones, N. P., &Strauman, T. J. (2006). Self-regulation, rumina-tion, and vulnerability to depression in adolescentgirls. Developmental Psychopathology, 18, 815–829.
Pearson, A. (2006). Powerful caring. Nursing Standard,20(48), 20–22.
Pfeffer, J. (1985). Organizations and organizational theory. In G. Lindzey & E. Aronson (Eds.), Hand-book of social psychology: Vol. 1. Theory and method (3rded., pp. 379–440). New York: Random House.
Phelps, E. Z. (2006). Emotion and cognition: Insightsfrom studies of the human amygdala. AnnualReview of Psychology, 57, 27–53.
Piaget, J., & Inhelder, B. (1969). The psychology of the child(H. Weaver, Trans.). New York: Basic Books.
Piane, G. (2000). Contingency contracting and system-atic desensitization for heroin addicts inmethadone maintenance programs. Journal ofPsychoactive Drugs, 32, 311–319.
Proctor, R., Burns, A., Powell, H. S., & Tarrier, N.(1999). Behavioural management in nursing andresidential homes: A randomized controlled trial.Lancet, 354, 26–29.
Pullen, M. L. (2002). Joe’s story: Reflection on a difficultinteraction between a nurse and a patient’s wife.International Journal of Palliative Nursing, 8,481–488.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 88

References 89
Rogers, C. (1961). On becoming a person. Boston:Houghton Mifflin.
Rogers, C. (1994). Freedom to learn (3rd ed.). New York:Merrill.
Rogers, L. Q., Matevey, C., Hopkins-Price, P., Shah, P.,Dunnington, G., & Courneya, K. S. (2004).Exploring social cognitive theory constructs forpromoting exercise among breast cancer patients.Cancer Nursing, 27, 462–473.
Santrock, J. W. (2006). Life-span development (10th ed.).Boston: McGraw-Hill.
Shapiro, A. (2002). The latest dope on research (aboutconstructivism): Part I: Different approaches toconstructivism—What it’s all about. InternationalJournal of Education Reform, 12, 62–77.
Sherif, M., & Sherif, C. W. (1969). Social psychology. New York: Harper & Row.
Shors, T. J. (2006). Stressful experience and learningacross the lifespan. Annual Review of Psychology, 57,55–85.
Silverstein, S. M., & Uhlhaas, P. J. (2004). Gestalt psychology: The forgotten paradigm in abnormalpsychology. American Journal of Psychology, 117,259–277.
Skinner, B. F. (1974). About behaviorism. New York:Vintage Books.
Skinner, B. F. (1989). Recent issues in the analysis ofbehavior. Columbus, OH: Merrill.
Slipp, S. (2000). Subliminal stimulation research and its implications for psychoanalytic theory andtreatment. Journal of the American Academy ofPsychoanalysis, 28, 305–320.
Snowman, J., & Biehler, R. (2006). Psychology applied toteaching (11th ed.). Boston: Houghton Mifflin.
Sternberg, R. J. (1996). Styles of thinking. In P. B.Baltes & U. M. Staudinger (Eds.), Interactive minds:Life-span perspectives on the social foundation of cognition (pp. 347–365). New York: CambridgeUniversity Press.
Sternberg, R. J. (2006). Cognitive psychology (4th ed.).Belmont, CA: Thomson/Wadsworth.
Stiles, A. S. (2005). Parenting needs, goals, & strategiesof adolescent mothers. MCN American Journal ofMaternal/Child Nursing, 30, 327–333.
Stockhurst, U., Steingrueber, H. J., Enck, P., &Klosterhalfen, S. (2006). Pavlovian conditioningof nausea and vomiting. Autonomic Neuroscience,129, 50–57.
Stroebe, M. S., Folkman, S., Hansson, R. O., & Schut, H.(2006). The prediction of bereavement outcome:Development of an integrative risk factor frame-work. Social Science and Medicine, 63, 2440–2451.
Telford, K., Kralik, D., & Koch, T. (2006). Acceptanceand denial: Implications for people adapting tochronic illness. Literature review. Journal ofAdvanced Nursing, 55, 457–464.
Tennant, M. (2006). Psychology and adult learning (3rded.). New York: Routledge.
Vander Zanden, J. W., Crandell, T. L., & Crandell, C. H.(2007). Human development (8th ed.). Boston:McGraw-Hill.
Vygotsky, L. S. (1986). Thought and language. Cambridge,MA: MIT Press.
Wolpe, J. (1982). The practice of behavior therapy (3rd ed.).New York: Pergamon.
Woolfolk, A. E. (2001). Educational psychology. Boston:Allyn & Bacon.
46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 89

46436_CH03_051_090.qxd 11/19/07 9:37 AM Page 90

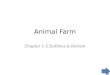


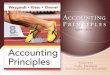












![Chapter 2 [Chapter 2]](https://img.dokumen.tips/doc/110x75/61f62040249b214bf02f4b97/chapter-2-chapter-2.jpg)











