Embed Size (px)
Citation preview

CHAPTER
18Review of the Circulatory System
Cardiac Compromise
Basic Life Support
Automated External Defibrillation
Vascular Emergencies
A cardiovascular event is a true medicalemergency for a patient. The recognition andtreatment of a cardiovascular event can meanthe difference between life and death. Thischapter reviews the circulatory system, dis-cusses the anatomy and physiology of thecardiovascular system, and discusses the as-sessment and treatment of a patient experi-encing a cardiac event. The chapter also cov-ers the link between early recognition andtreatment of a cardiovascular event and pa-tient outcome. ■
346
Ch18-E4000_346-377 7/10/06 11:12 M Page 346

After completing this chapter, the EMT student will be able to do the following:
1 List the parts of the cardiovascular system and how they work.2 Describe the emergency medical care of the patient experiencing chest
pain/discomfort.3 List the indications and contraindications for automated external
defibrillation.4 Define the role of the emergency medical technician in the emergency
cardiac care system.5 Explain the impact of age and weight on defibrillation.6 Discuss the position of comfort for patients with various cardiac
emergencies.7 Explain the importance of airway management in the patient with
cardiovascular compromise.8 Predict the relationship between the patient experiencing cardiovascular
compromise and basic life support.9 Discuss the fundamentals of and reasons for early defibrillation.
10 Explain the importance of prehospital advanced cardiac life support (ACLS).11 Explain the importance of urgent transport to a facility with ACLS.12 Discuss the various types of automated external defibrillators and the
difference between the fully automated and the semiautomated externaldefibrillator.
18
347
CardiovascularEmergencies
Continued
Ch18-E4000_346-377 7/10/06 11:12 M Page 347

13 State the reasons for ensuring that the patient is pulseless and apneicbefore using the automated external defibrillator.
14 Discuss what might cause inappropriate shocks.15 Explain when you would stop cardiopulmonary resuscitation to use the
automated external defibrillator.16 Discuss rhythm monitoring.17 List the steps in the operation of the automated external defibrillator for one
emergency medical technician and two emergency medical technicians.18 Discuss the standard of care to use when treating a patient with constant
ventricular fibrillation when ACLS is not available.19 Discuss the standard of care to use when treating a patient with recurrent
ventricular fibrillation when ACLS is not available.20 Explain the reason for not checking a pulse between shocks with an
automated external defibrillator.21 Discuss the importance of and components for postresuscitation care.22 Explain the role medical direction plays in the use of automated external
defibrillation.23 State the reasons for reviewing each call following the use of the automated
external defibrillator.24 Discuss the components that should be included in a case review.25 Explain the role of medical direction and protocols in the emergency
medical care of the patient with chest pain.26 List the indications for the use of nitroglycerin.27 State the contraindications for and side effects of the use of nitroglycerin.28 Describe the controls on an automated external defibrillator and how they work.29 Describe event documentation.30 Explain why the maintenance of automated external defibrillators is important.31 Explain the reasons for giving nitroglycerin to a patient with chest pain or
discomfort.32 Demonstrate the assessment and emergency medical care of a patient
experiencing chest pain/discomfort.33 Demonstrate the application and operation of the automated external
defibrillator.34 Demonstrate the maintenance of an automated external defibrillator.35 Demonstrate the assessment and documentation of the patient’s response to
the automated external defibrillator.36 Perform the steps in assisting the patient to use nitroglycerin for chest pain
or discomfort.37 Demonstrate the assessment and documentation of patient response to
nitroglycerin.38 Practice completing a prehospital care report for patients with cardiac
emergencies.
Chapter Objectives—cont’d
348
Ch18-E4000_346-377 7/10/06 11:12 M Page 348

CHAPTER 18 ■ Cardiovascular Emergencies 349
More than 600,000 persons die each yearfrom various types of cardiovascular dis-ease. Approximately half of those deaths re-
sult from sudden cardiac death. Sudden cardiacdeath is often the first warning sign a patient displaysof cardiac disease. Up to 50% of sudden cardiacdeaths occur before the patient reaches a hospital.
Cardiac events are true medical emergencies. Inthe prehospital setting, emergency medical care canmake a significant difference in the patient’s survivaland outcome. This chapter discusses the assessmentand treatment of cardiac emergencies and the man-agement of cardiac arrest.
■ REVIEW OF THECIRCULATORY SYSTEM
The circulatory system can be thought of as a trans-port system for the body, with various one-way streetsand highways along the way. As discussed in Chapter4, the circulatory system includes not only the heartbut also an integrated arterial and venous system thatserves specific functions to keep the body working.
The circulatory system transports oxygen and nutri-ents to the body and removes carbon dioxide andother wastes from the tissues.
AnatomyHeartThe heart is more than a muscle. The heart is the “en-gine” of the circulatory system. The heart is com-posed of two sides, the right side and the left side. Awall called the septum divides the two sides. Eachside of the heart has an atrium and a ventricle, sepa-rated by a one-way valve, meaning the valve only al-lows blood to flow in one direction.
The right atrium receives oxygen-depleted bloodfrom the veins of the body and the heart and pumpsit to the right ventricle. From the right ventricle theoxygen-poor blood is pumped to the lungs to be “re-fueled.” Picking up oxygen in the lungs, the blood re-turns to the left atrium of the heart via the pul-monary veins. The left atrium pumps the nowoxygen-rich blood to the left ventricle which thenpumps the blood out to the body so that the bloodcan deliver oxygen and nutrients.
Dinner is almost done. Jack is cleaning up the re-mainder of the dishes while Elizabeth wipes downthe table. Jane is using the broom, sweepingaround the table. The ride-along, Jack, is alreadyoff to the common area, looking again at his emer-gency medical technology book, hoping that thetones go off soon. They already have had two runsearlier in the shift, causing dinner to run late. Butit was so exciting to see the crew in action; theyseemed to work so well together.
Jack’s prayers are answered: The county tonesbegin to warble, and the house lights came on.“Rescue Six Thirty-six, Seventy-three TalbertRoad, cross of Main, report of respiratory dis-tress.” Jack wipes his hands and heads to thegarage to start up the ambulance.
They pull up to a single-story tract home in oneof the older sections of town. An older womangreets them at the door, looking anxious. “My hus-band is in the back room. I think he fainted.Please hurry!”
“What is his name, ma’am?” asks Elizabeth,while walking down the narrow hallway toward theback bedroom.
“Jim Markham,” replies the woman.In the bedroom, Elizabeth leans over to the
man, who is lying on the bed. “Mr. Markham, howare you doing?”
“I am . . . okay,” the patient replied slowly, as ifhe were trying to convince himself that in fact hewas. Although awake, Mr. Markham looked a bitconfused as to where he was. He was pale, andsweating profusely. Following instructions he re-ceived from Elizabeth earlier in the shift, Jackopened the first-in bag to retrieve the penlight,stethoscope, and blood pressure cuff. Jane is busyopening the airway kit and cracking open the oxy-gen tank.
Question: What are some of the procedures theemergency medical services crew should do im-mediately to help manage this patient?
Ch18-E4000_346-377 7/10/06 11:12 M Page 349

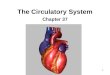
The one-way valve that separates the atria and ven-tricles prevents the backflow of blood and enables aone-way flow of blood through the heart (Fig. 18-1).
Blood VesselsIn addition to the heart, the circulatory system iscomposed of various vessels called arteries and veinsin a network that is connected to the heart. Each ofthese arteries and veins has a specific route and afunction to provide for the body.
Arteries carry blood away from the heart to the restof the body. They carry oxygen-rich blood and delivernutrients to the various organs of the body. Witheach contraction of the heart, you can feel it pump-ing blood through the body wherever you are able to
palpate a pulse. You can feel a pulse through an ar-tery that lies close to the surface of your skin and liesover a bony prominence. Fig. 18-2 shows peripheraland central pulse sites. Arteries become smaller andsmaller until they connect to arterioles. Arteriolesbecome smaller and smaller until they connect withcapillaries. Capillaries are intertwined with all of thetissues in the body, allowing the exchange of oxygenfor carbon dioxide. The capillaries then join with tinyvessels called venules. The venules join with veins,which become larger and larger in diameter returningto the right atrium. In the right atrium, the processbegins all over again.
The largest artery (in diameter) of the body is theaorta. The aorta is a major artery that originates from
350 ■ EMERGENCY MEDICAL TECHNICIAN
Rightpulmonary
artery toright lung
Left pulmonaryartery to left lung
Pulmonaryartery
Leftpulmonaryveins
Myocardium
LEFTVENTRICLE
RIGHTVENTRICLE
Rightpulmonary
veins
Inferior venacava
Superior vena cava
Aorta
LEFT ATRIUM
RIGHT ATRIUM
Interventricularseptum
Aorta
Fig. 18-1 Anatomy of the heart.
Ch18-E4000_346-377 7/10/06 11:12 M Page 350

the heart and lies in front of the spine in the thoracicand abdominal cavity. At the level of the navel, the aortadivides to form the iliac arteries. These arteries supplythe lower extremities with oxygen and nutrients.
The pulmonary artery originates in the right ven-tricle of the heart. It carries oxygen-poor blood anddelivers it to the lungs to be replenished. The pul-monary artery is the only artery in the body that car-ries oxygen-poor blood instead of oxygen-rich blood.
The carotid arteries are the major arteries in theneck. They supply the head with oxygenated blood.The carotid pulse can be felt on either side of theneck next to the trachea.
The femoral artery is the major artery of the thighand supplies the groin and lower extremities withoxygenated blood. Femoral pulses can be felt on ei-ther side of the groin area at the crease between theabdomen and thigh.
The radial artery supplies the lower arm and handwith oxygenated blood. Radial pulses can be felt inthe distal anterior area of the wrist (near the base ofthe thumb on the palm side of the wrist).
The brachial artery can be felt in the upper armand can be palpated on the inside of the arm be-
tween the elbow and the shoulder. The brachial ar-tery most commonly is used to determine a bloodpressure with a sphygmomanometer (blood pres-sure cuff) and a stethoscope. The sphygmomanome-ter is placed over the brachial artery and the bloodpressure is auscultated at the distal end of thebrachial artery in the antecubital fossa at the elbow.
Arteries that can be palpated in the lower extremi-ties are the posterior tibial artery and the dorsalispedis artery. The posterior tibial artery is located onthe medial side of the malleolus (near the inside ofthe ankle). The dorsalis pedis artery is located on theanterior surface of the foot.
The primary function of the venous system(veins) is to carry blood back to the heart after the ar-terial system has delivered oxygen and nutrients. Thepulmonary vein carries blood to the left atrium ofthe heart from the lungs after being replenished withoxygen. From there, the blood once again is pumpedout into the body. Consequently, the pulmonary veinis the only vein in the body that carries oxygen-richblood.
The venae cavae are major veins that consist of twobranches: the superior vena cava and the inferiorvena cava. The superior vena cava carries oxygen-poorblood from the head and arms. The inferior vena cavacarries oxygen-poor blood from the lower extremitiesand torso. This oxygen-poor blood in both of thesemajor veins is transported to the right atrium of theheart. As mentioned previously, the blood then is car-ried to the lungs from the right atrium via the rightventricle and pulmonary artery to be reoxygenated.
Blood CompositionWhat is blood? Blood is composed of numerouscomponents including red blood cells (erythro-cytes), white blood cells (leukocytes), plasma, andplatelets. Red blood cells give blood its red color.They also carry oxygen to the organs of the body andcarry carbon dioxide away from the organs. Whiteblood cells help defend the body against infections.Plasma is the fluid that moves the red and whiteblood cells and nutrients throughout the body. Itcontains a variety of proteins, hormones and infec-tion-fighting chemicals called antibodies. Plateletsare special cells that make the blood form clots andhelp the body to stop bleeding.
PhysiologyThe left ventricle of the heart contracts, sending theoxygen-rich blood through the arteries of the body.As this occurs, you can simultaneously feel that push
CHAPTER 18 ■ Cardiovascular Emergencies 351
Temporal artery
Facial artery
Brachial artery
Popliteal artery(behind knee)
Posteriortibial artery
Dorsalis pedisartery
Femoral artery
Common carotidartery
Radial artery
Fig. 18-2 Peripheral and central pulse sites.
Ch18-E4000_346-377 7/10/06 11:12 M Page 351

of blood by palpating any of the major arteries thatare located over a bone near the surface of the skin.This is called a pulse.
To review, peripheral pulses are the following:
• Radial• Brachial• Posterior tibial• Dorsalis pedis
Central pulses are the following:
• Carotid• Femoral
Blood pressure is the pressure exerted against thewalls of an artery when the left ventricle contracts. Whenone is using a sphygmomanometer, this reading is calledthe systolic blood pressure. This pressure is recorded asthe top number of the blood pressure reading.
The pressure against the arteries when the left ven-tricle completes its contraction and is at rest is calledthe diastolic blood pressure. This pressure is recordedas the bottom number of the blood pressure reading,when assessed with a sphygmomanometer.
Inadequate circulation can cause a state of pro-found depression to the vital processes of the bodycalled shock (hypoperfusion). A lack of blood vol-ume or a lack of blood circulating in the body cancause shock. Shock can be recognized by specificsigns and symptoms as the body reacts and attemptsto compensate for its loss of perfusion. Signs andsymptoms of shock include the following:
• Pale, cyanotic, cool, clammy skin• Weak but rapid pulse• Rapid and shallow breathing• Restlessness, anxiety, or mental dullness• Nausea and/or vomiting• Low or decreased blood pressure• Subnormal temperature
Chapter 25 further discusses the effects shock (hy-poperfusion) has on the body.
■ CARDIAC COMPROMISE
As you perform your patient assessment, look forsigns and symptoms that may indicate cardiac com-promise. Chest pain that the patient describes as adull pressure, a dull ache, or a squeezing or tightnesscan be a symptom of myocardial (cardiac muscle)
compromise. The chest discomfort also may radiateinto the jaw or down the arms or into the upper back.A sudden onset of sweating, even as a primary symp-tom, can be a significant finding and can indicate car-diac compromise. Difficulty breathing (dyspnea),anxiety, irritability, and a feeling of impending doomalso can be symptoms that the emergency medicaltechnician (EMT) should consider to be cardiac re-lated. Abnormal pulse rate, which also may have anirregular rhythm, and an abnormal blood pressurealso are common. The patient may complain of epi-gastric pain or nausea and vomiting.
Similar symptoms can result from angina, is-chemia, or myocardial infarct. Angina is a conditionthat usually presents as chest discomfort upon physicalexertion. It usually goes away when the patient rests orwhen the patient takes nitroglycerin. Ischemia resultswhen an area of the heart muscle is not receivingenough oxygen. Myocardial infarction is the result of ablockage to one of the vessels in the heart resulting indeath (infarction) of heart muscle (myocardium).
AssessmentWell-developed assessment skills are essential informing a field impression to determine an appropri-ate treatment plan for a patient with possible cardiaccompromise. The initial assessment for any patientwith suspected cardiac disease is the same as it is forany other type of patient. Once your scene is secureand you have your necessary personal protective gearin place, assessment can begin. Assessment shouldinclude forming a general impression and continuingwith your evaluation of airway, breathing, and circu-lation and determining the priority status or critical-ity of your patient. Apply high-flow oxygen as soon aspossible to any patient showing signs and symptomsof cardiac compromise.
If the patient is able to interact with you and has aknown history of cardiac problems, move on to yourfocused assessment and physical examination afteryour initial assessment. Patients tend to place them-selves in a position that provides the most comfort tothem. Be sure to allow the patient to continue to as-sume his or her position of comfort as you are as-sessing, treating, and transporting him or her. Pa-tients with hypotension (low blood pressure) or whocomplain of being light-headed or dizzy may feelbest when lying down. Patients who are complainingof difficulty breathing may feel best when sitting up.Be sensitive to what feels the most comfortable to thepatient. Patients with cardiac symptoms should notexert themselves. Any patient who is suspected of
352 ■ EMERGENCY MEDICAL TECHNICIAN
Ch18-E4000_346-377 7/10/06 11:12 M Page 352

having cardiac-related signs and symptoms shouldnot be allowed to get up and move about and shouldnot be allowed to walk. For the patient to remain atrest during assessment and transport is crucial toavoid increasing cardiac workload.
Obtain baseline vital signs including skin assess-ment and mental status.
Important questions to ask your patient in assess-ing any chest pain are the OPQRST questions:
• O—Onset• P—Provocation• Q—Quality• R—Radiation• S—Severity• T—Time
Box 18-1 gives further details of the OPQRST as-sessment for evaluating a patient with chest pain.
Any prior cardiac-related history is pertinent infor-mation. Included in your SAMPLE history (Signs andsymptoms, Allergies, Medications, Past medical his-tory, Last oral intake, Events preceding), you shouldask the patient about any prescribed cardiac medica- tion. You also should ask whether he or she has been
prescribed nitroglycerin.
NitroglycerinNitroglycerin (generic name) most commonly isfound in the form of sublingual (under the tongue)tablets or in sublingual spray (Fig. 18-3). Commontrade names for nitroglycerin are Nitrostat or Ni-trolingual (nitroglycerin translingual) Spray.
ActionNitroglycerin dilates blood vessels, decreasing theworkload of the heart, which in turn alleviates car-diac-related signs and symptoms. With dilation ofthe blood vessels, however, comes a risk that the pa-tient’s blood pressure may decrease. If the patient’ssystolic blood pressure decreases to less than 100 mmHg, place the patient in the Trendelenburg position(supine with his or her feet elevated) and withholdfurther administration of nitroglycerin.
If the patient has a current prescription of nitro-glycerin that has been issued to him or her, askwhether the patient has taken any before your ar-rival. For the conscious and alert patient showingsigns and symptoms of a cardiac emergency, con-sider administration of nitroglycerin. The EMTshould examine the patient’s prescription of nitro-glycerin to ensure that it is prescribed for the patient,is not expired, is the correct dosage, and is to be ad-
CHAPTER 18 ■ Cardiovascular Emergencies 353
BOX 18-1OPQRST Assessment for Chest Pain
Onset: When did the symptoms first occur?What were you doing when they first started?
P rovocation: Does anything make the pain worseor better? Does it hurt when inhaling or exhaling?
Quality: Describe the pain. Is it sharp or dull?Is it constant, or does it subside and get worse?
Radiation: Does the pain go to anywhere elsebesides the chest? Is there pain in the jaw, arm,or back?
Severity: How bad is the pain? A tool that isuseful for assessing the pain of a patient with car-diac disease is the 1-to-10 pain scale. Ask thepatient to rate his or her chest pain or discomfort,with 1 being the least pain and 10 being theworst pain he or she can imagine. This initial rat-ing makes it easier to evaluate the level of painduring your ongoing assessment of the patient. Italso helps you to determine whether the interven-tions performed are benefiting the patient andeasing his or her symptoms.
T ime: How long have you had the pain? Whendid it start and has it come and gone?
Jack’s first set of measured vital signs were:
Pulse Respirations Blood Pressure110 20 86/64
From Elizabeth’s SAMPLE history andOPQRST of the complaint, Jack suspected thatMr. Markham was experiencing a cardiac emer-gency. His history indicated that he had highrisk: he was taking medications for high bloodpressure and high cholesterol. Elizabeth held upone of the medications. “Jack, should we helphim with his nitroglycerin?”
Question: Given Jack’s findings, should Mr.Markham receive nitroglycerin? Why or why not?
continued
Ch18-E4000_346-377 7/10/06 11:12 M Page 353

ministered sublingually. The patient may take up tothree consecutive doses of nitroglycerin, either bysublingual pill or spray. If the patient has not metthe maximum dosage, the EMT should obtain orders(online or off-line) for authorization to assist the pa-tient with nitroglycerin administration. Once ordersare obtained from medical direction for the admin-istration of nitroglycerin, the EMT must be sure thepatient meets the following criteria:
• Signs and symptoms of cardiac-related chest pain• Systolic blood pressure greater than 100 mm Hg• Physician-prescribed nitroglycerin tablets or spray
in the patient’s name• Specific authorization from medical direction
The EMT also must be certain that none of the fol-lowing contraindications are present before admin-istering nitroglycerin:
• Systolic blood pressure less than 100 mm Hg• Head injury
• Use of sildenafil (Viagra), vardenafil (Levitra),tadalafil (Cialis), or similar types of drugs forerectile dysfunction within the previous 48 hours
• Infants and children• Patient has met maximum dosage before arrival
of emergency medical services (EMS)• Patient does not have his or her own prescribed
medication• Medical direction has not authorized administra-
tion of nitroglycerin for this patient
The EMT should be knowledgeable about anydrug for which he or she is responsible for adminis-tering or with which he or she can assist.
DosageThe dosage for nitroglycerin is one tablet or one meteredspray under the tongue (0.3 to 0.4 mg). This dosage maybe repeated in 3 to 5 minutes if there is not sufficient re-lief of the patient’s symptoms. A maximum of threedoses may be given with approval from medical direc-tion. The EMT should reassess the patient after each doseof nitroglycerin before assisting the patient with moredoses. Be especially alert for blood pressure that dropsless than 100 mm Hg after giving nitroglycerin.
AdministrationOnce medical direction has issued orders to administernitroglycerin and the EMT has found no contraindica-tions, the EMT should assist the patient with adminis-tering nitroglycerin. Be sure to follow the four R’s of med-ication administration: the right medication, the rightpatient, the right dose, and the right route. The patientmust be alert as well. Check the expiration date of the ni-troglycerin. Ask the patient to lift his or her tongue andplace or have the patient place the nitroglycerin tablet orone pump of spray under his or her tongue (Skill 18-1).Instruct the patient to keep his or her mouth closed andnot to swallow until the tablet completely dissolves andis absorbed. Reassess the patient’s blood pressure within2 minutes of administration of the nitroglycerin. For apatient to complain of a headache or a burning sensa-tion under the tongue is normal. Record administrationof the nitroglycerin along with accurate times of the ad-ministration and any effects it has had in relieving thepatient’s signs and symptoms.
ReassessmentOngoing assessment of the patient with cardiacdisease is important. Vital signs, pain assessment,and assessment of the effects of interventionsshould be recurrent.
354 ■ EMERGENCY MEDICAL TECHNICIAN
Fig. 18-3 Nitroglycerin. A, Spray. B, Tablet form.
A
B
Ch18-E4000_346-377 7/10/06 11:12 M Page 354

SKILL 18-1Administration of Nitroglycerin
355
1. Follow appropriate body substance isolation pre-cautions and assess the patient’s vital signs. Con-sult medical direction regarding nitroglycerin ad-ministration.
2. Instruct the patient to lift his or her tongue. Placeone tablet under the tongue and ask the patientto close his or her mouth. Instruct the patient toleave the tablet under the tongue until it is com-pletely dissolved and to not chew the tablet.
4. Take the patient’s blood pressure within 2 min-utes of administration. Record the patient’s name,the name of the medication, the dosage of themedication (listed on bottle), the time of admin-istration, and the name of the ordering physicianproviding medical direction.
5. Reassess and record all vital signs. Also assess anddocument any effects the medication has had onthe patient. Notify medical direction of anychanges in the patient’s condition or for requestsfor additional doses.
3. If the patient uses nitroglycerin spray, spray onceunder the tongue. Instruct the patient to close hisor her mouth quickly.
Ch18-E4000_346-377 7/10/06 11:12 M Page 355

TransportDo not allow the patient to move himself or her-self, as exertion only serves to increase the work-load of the heart. Moreover, transport the patientin a position that is most comfortable for him orher. Consider any patient with signs and symptomsof cardiac compromise as critical. If available, re-quest a tier rendezvous with advanced life support.Consider methods of transportation that are bestfor the patient. For example, although a patient’ssituation may be urgent and critical and rapidtransport may be necessary, lights and sirens maycause added fear and anxiety for the patient. Assesswhat is necessary and explain to the patient whatwill occur. If it is determined that lights and sirensare needed to help control traffic, explain this tothe patient. Assure the patient that safety is the pri-mary concern. A calm and careful transport for thepatient is best, and safety is the most importantconsideration.
■ BASIC LIFE SUPPORT
Not all patients who experience cardiac compromiseexperience cardiac arrest. That possibility does exist,however, and the EMT must be prepared to managesuch an event by being proficient in cardiopul-monary resuscitation (CPR). Any patient who iscomplaining of breathing difficulty or chest pain ordiscomfort should be considered a candidate for po-tential cardiac arrest. Therefore the EMT should beprepared and have the necessary equipment nearbyin anticipation of such an event (Skill 18-2).
Good basic life support skills are essential. Emer-gency medical technicians rarely have a situation inthe field that calls for performing one-person CPR(Skill 18-3). However, some situations may require it.For example, your partner may need to prepare or re-trieve equipment. Similarly, he or she may be drivingen route to the hospital while you are the only otherEMS provider on the scene or in the back of the am-bulance.
You should practice these techniques and en-hance them during your EMT course. In addition,defibrillation should be integrated into your one-and two-rescuer CPR skills. The use of automatedexternal defibrillation devices is discussed later inthis chapter.
As a professional emergency medical provider,learning basic life support includes using bodysubstance isolation techniques, airway adjuncts,
and oxygenation and ventilation equipment suchas oral or nasal airways, bag-valve-mask, and flow-restricted oxygen-powered ventilation devices. Theuse of these devices is discussed in Chapters 7 and17. The EMT must practice and become proficientat using these devices along with the integrationof CPR. The EMT also must assume responsibilityfor keeping informed of current trends in treat-ment standards and the latest developments intechnology.
Obtaining a pertinent history by interviewingbystanders and/or family members is important.The history can aid in determining the nature ofcardiac arrest and what may have led to it. Docu-ment this information. Also share this informa-tion with other health care providers to assist indetermining further management of the patient’scondition.
When available, request advanced cardiac life sup-port (ACLS) to tier with any patient with cardiac ar-rest in order to continue the chain of survival. TheAmerican Heart Association defines the chain of sur-vival as a series of actions that include early access toEMS, early CPR, early defibrillation, and early ACLS1
(Box 18-2).
356 ■ EMERGENCY MEDICAL TECHNICIAN
BOX 18-2Chain of Survival
Early access: Early identification of a cardiacemergency and access to emergency medicalservices. Training the public to recognize signs ofcardiac arrest and when to contact emergencymedical services.
Early cardiopulmonary resuscitation: Lay pub-lic education and training in performing car-diopulmonary resuscitation until emergency med-ical personnel can arrive. Early cardiopulmonaryresuscitation is an essential element in the pa-tient’s chance of survival.
Early defibrillation: Defibrillation is the mostimportant element in reversing ventricular fibrilla-tion and aiding the heart to resume functioning.Public access defibrillation is becoming morewidespread.
Early advanced care: Access to advanced car-diac life support is needed to provide the neces-sary life support needed for a cardiac arrest victim.
Ch18-E4000_346-377 7/10/06 11:13 M Page 356

SKILL 18-2Two-Rescuer Cardiopulmonary Resuscitation
357
1. Establish responsiveness. 2. If patient is unresponsive, one rescuer should callfor help or retrieve the AED if available, while theother opens the patient’s airway with a headtilt–chin lift or jaw thrust.
3. Look, listen, and feel for breathing. 4. If there are no signs of breathing, provide two res-cue breaths or retrieve the AED if available.
Continued
Ch18-E4000_346-377 7/10/06 11:13 M Page 357

SKILL 18-2Two-Rescuer Cardiopulmonary Resuscitation—cont’d
358
5. Check for signs of circulation, including carotidpulse, signs of normal breathing, coughing, ormovement.
6. If no signs of circulation, one rescuer performs 30chest compressions, followed by two ventilationsgiven by the second rescuer.
7. After five cycles of 30 compressions and two ven-tilations, the rescuer at the head should check forsigns of circulation. If no signs of circulation, re-sume cardiopulmonary resuscitation. Check forsigns of circulation after every five cycles (about 2minutes). Rescuers should switch between pro-viding compressions and ventilations as they tireand as convenient.
Ch18-E4000_346-377 7/10/06 11:13 M Page 358

SKILL 18-3One-Rescuer Cardiopulmonary Resuscitation
359
1. If the rescuer witnesses the patient suddenlycollapse, the rescuer should establish unrespon-siveness, then phone 911 or get the AED if avail-able. If the lone rescuer is called to an asphyxialcause such as a drowning, the rescuer shouldperform five cycles of CPR (30 compressions totwo ventilations each).
2. Open the airway with a head tilt–chin lift or jawthrust.
3. Look, listen, and feel for breathing. 4. If no signs of breathing, provide two rescuebreaths.
5. Check for signs of circulation including carotidpulse, signs of normal breathing, coughing, ormovement.
Continued
Ch18-E4000_346-377 7/10/06 11:13 M Page 359

SKILL 18-3One-Rescuer Cardiopulmonary Resuscitation—cont’d
360
7. Place the heel of one hand in the appropriatespot and place your other hand on top. Use theforce from the heels of your hands only.
8. Position yourself directly over the patient’s ster-num and lock your elbows to deliver 30 com-pressions.
9. Provide two rescue breaths.
10. After approximately five cycles of 30 compres-sions and two ventilations, check again for signsof circulation. If no signs, resume cardiopul-monary resuscitation, checking for signs of cir-culation every five cycles. If there are signs ofcirculation but no signs of breathing, continuerescue breathing at a rate of one breath every 5 seconds.
6. If no signs of circulation, locate landmark forcompressions on the lower portion of the sternum.
Ch18-E4000_346-377 7/10/06 11:13 M Page 360

■ AUTOMATED EXTERNALDEFIBRILLATION
Cardiac arrest, sometimes referred to as suddendeath, can be a sudden loss of heart function. Mostsudden deaths from cardiac arrest occur when theelectrical impulses in the heart become rapid andchaotic. Impulses in the heart that are rapid andchaotic do not allow the heart to pump blood out tothe body as it is designed to do. This electrical activ-ity is called ventricular fibrillation (Fig. 18-4) andsometimes can be reversed with the use of a cardiacdefibrillator.
Early defibrillation, a continued link in the chainof survival, includes recognizing and treating ventric-ular fibrillation. The automated external defibrilla-tor (AED; Fig. 18-5) is a machine designed to evalu-ate and recognize a patient’s cardiac rhythm anddeliver a shock if the patient displays a cardiacrhythm such as ventricular fibrillation.
Many EMS systems have demonstrated increasedsurvival rates of patients with cardiac arrest when us-ing AEDs as opposed to CPR alone. Early defibrilla-tion programs are gaining popularity in the publicand in traditional health care arenas. Automated ex-ternal defibrillators are functional and simple to use.As public access defibrillation programs are gainingpopularity, and access to AEDs is becoming more
common, response time in the chain of survival is de-creasing, and survival rates for victims of sudden car-diac arrest is increasing.
Overview of the AutomatedExternal DefibrillatorHealth care providers have been using defibrillationfor cardiac arrest for many years. With the advance-ment of computer technology, defibrillation hasevolved into an easy-to-access, easy-to-learn, andeasy-to-perform treatment.
Defibrillators deliver a shock to the patient’s chest.The intent is to reverse the rapid, chaotic electric ac-tivity the heart experiences during ventricular fibrilla-tion. Ventricular fibrillation sometimes is describedas the heart “quivering” and not producing the or-ganized impulses necessary to cause the heart to con-tract in an effective manner. Defibrillation can inter-rupt that chaotic electrical impulse and cause theheart to start contractions in a more orderly fashion.The more orderly fashion enables the heart to pumpblood out to the body as designed.
Most commonly, AEDs come fully automated orsemiautomated. Fully automated external defibrilla-tors require the EMT simply to apply two electrodepatches to the patient’s chest, attach the electrodes tothe AED, and turn on the machine. The AED then an-
CHAPTER 18 ■ Cardiovascular Emergencies 361
Fig. 18-4 Ventricular fibrillation.
Fig. 18-5 Example of an automated external defibrillator.
Ch18-E4000_346-377 7/10/06 2:38 PM Page 361

alyzes the cardiac rhythm and delivers shocks to thepatient when appropriate.
A semiautomated external defibrillator operatesin much the same way. The EMT turns on the powerto the AED, applies the electrodes (adhesive patches)to the patient’s chest, and attaches the electrodewires to the AED. The EMT then must press a buttontelling the machine to analyze the cardiac rhythm.Once the cardiac rhythm is analyzed, the machine,through a computer-synthesized voice, will instructthe EMT on subsequent needed actions. If it is deter-mined that a shock is needed, the voice on the AEDwill instruct the EMT to deliver a shock by pushingthe shock button.
The AED is designed to deliver a shock only if thepatient has a “shockable” rhythm. The AED has amicroprocessor installed that evaluates the cardiacrhythm and determines whether it is a rhythm forwhich a shock is indicated. Ventricular fibrillationand ventricular tachycardia are rhythms that theAED will shock. Ventricular tachycardia is a rapidcardiac rhythm in which the heart beats so rapidlythat it is not producing output to the rest of thebody (Fig. 18-6). When the cardiac rhythm is ven-tricular tachycardia, the patient may or may nothave a discernable pulse. The AED will advise toshock for ventricular tachycardia once the rate ex-
ceeds 180 beats per minute. The AED cannot deter-mine whether the patient has a pulse. It can deter-mine only what electrical rhythm the heart has. Toavoid delivering a shock to a patient who has apulse, attach the AED only to patients who are un-responsive, breathless, and pulseless. Patients with apulse still have electrical impulses in the heart thatare functioning. Shocking a patient with a pulse cancause the heart to convert into ventricular fibrilla-tion or into asystole. Asystole (Fig. 18-7) also isknown as flatline or cardiac standstill. Asystole in-dicates that the heart has stopped all function, in-cluding any electrical activity.
In very few instances has an AED delivered an in-appropriate shock. These machines are accurate at in-terpreting cardiac activity and which rhythms requirea shock and which rhythms do not. Often failure ofthe machine is due to human error. A priority at everyshift check is making sure that batteries are workingand that extra batteries are available. The AED shouldnot be placed on patients who have a pulse. Moreover,it should never be operated when in a moving vehicleor while moving the patient. Stop CPR while the ma-chine is analyzing the patient’s heart rhythm andwhile shocks are being delivered. The person operat-ing the device should ensure that no one is touchingthe patient while the AED is analyzing the cardiac
362 ■ EMERGENCY MEDICAL TECHNICIAN
Fig. 18-6 Ventricular tachycardia.
Fig. 18-7 P-wave asystole.
Ch18-E4000_346-377 7/10/06 2:38 PM Page 362

rhythm or while shocks are being delivered. Stop CPRand artificial ventilations while the machine is ana-lyzing and while it is delivering shocks to the patient.Anyone touching the patient can be shocked as well.Although CPR is part of the chain of survival for pa-tients with cardiac arrest, early defibrillation is moreeffective in terminating ventricular fibrillation. Be-cause most patients with shockable rhythms are inventricular fibrillation, stopping CPR to defibrillate ismore beneficial to the patient. Cardiopulmonary re-suscitation may be resumed after the initial shocks aredelivered.
Advantages of the AutomatedExternal DefibrillatorThe AED has many advantages. Operation is simpleand quick. Learning to use a defibrillator is easierthan learning the techniques of CPR. However, onemust memorize the appropriate sequence for usingthe AED. After the initial training is completed,continuing education should be in place. Moreover,regular practice sessions using an AED trainer andvarious cardiac arrest scenarios should be in place.Skills should be evaluated periodically. Medical di-rection should be involved in ensuring a system ofquality assurance and evaluation of cardiac arrestevents.
The machine can be attached to the patient andthe first shock delivered within 1 minute of arrival atthe patient’s side. Adhesive pads make using the AEDa hands-off operation. Automated external defibrilla-tion is safer than traditional ACLS defibrillation,which requires placing and holding paddles directlyonto the patient’s chest. Electrodes are large and easyto place on the patient. Some AEDs have an optionalrhythm-monitoring system that can be beneficialwhen tiering with ACLS services.
Automated External DefibrillatorOperationApproaching a patient with cardiac arrest requires thesame initial actions as any other call requires. Practicebody substance isolation using personal protectivegear. If possible, don your gear while en route to thescene. Once you arrive on scene, survey the scene andensure safety. If additional resources have not beencalled for already, you should request resources suchas ACLS.
Perform your initial assessment of patient respon-siveness, airway, breathing, and circulation. If CPR is
in progress by bystanders, ask them to stop while youverify pulselessness and apnea. Once it is verified thepatient is pulseless and breathless, have your partnerresume CPR for 5 cycles (about 2 minutes) while youprepare the AED.
Skill 18-4 outlines the steps for using an AED asdescribed in this section. Turn on the defibrillatorpower. Attach the adhesive pads to the patient’s chest,and ensure the electrodes are attached to the AED. Ifthe AED is a machine that has an event voicerecorder, begin your narrative. Stop CPR and ask allbystanders to “clear” (stand away from and do nottouch) the patient. Rescuers who are managing thepatient’s airway also must be clear of the patient. Ini-tiate the analysis of the cardiac rhythm by pushingthe analyze button.
Fig. 18-8 depicts a universal algorithm protocolfor operation of an AED.
Shock AdvisedIf the AED advises to deliver a shock, again clear thepatient by ensuring that no one is touching the pa-tient. Once the machine charges and advises to de-liver the shock, press the shock button. Allow the
CHAPTER 18 ■ Cardiovascular Emergencies 363
Apply the AED to people at least 1 year old who areunresponsive and without normal breathing,
coughing, or movement.
Do 5 cycles (about 2 min) of CPR.
Resume CPR for 5 cycles. Check rhythm.
NO BREATHING, COUGHING, OR MOVEMENT
1. POWER ON the AED first.2. ATTACH the pads to the patient’s bare chest.3. ANALYZEAlways “clear” before analysis and shock!
• Analyze.• Repeat shock as indicated.
COUGHING OR MOVEMENT PRESENT• Check breathing.• Rescue breathe, if
breathing is inadequate.• Recovery position if
breathing adequate.
NO SHOCKADVISED
SHOCK ADVISED• Analyze and shock.
Fig. 18-8 Automated external defibrillator protocol.
Ch18-E4000_346-377 7/27/06 2:56 PM Page 363

SKILL 18-4Use of the Automated External Defibrillator
364
1. Place the automated external defibrillator (AED)next to the patient’s left ear if possible. Turn theAED on.
2. Attach the AED pads to the patient’s chest as di-rected on the pads.
3. Allow the AED to analyze the patient’s rhythm.Do not touch the patient.
4. If the AED states that a shock is advised, ensurethat everyone is clear of the patient.
5. Press the shock button. Once the shock is deliv-ered, immediately begin 5 cycles (about 2 min-utes) of CPR beginning with chest compressions.
Ch18-E4000_346-377 7/27/06 2:56 PM Page 364

machine to shock the patient. Immediately resumeCPR for 5 cycles. Check rhythm.
If the patient is not breathing, provide mechanicalventilations with supplemental oxygen and initiatetransport.
If after any rhythm analysis, the machine advises noshock, check the patient’s pulse. If the patient has apulse, check the patient’s breathing. If the patient isbreathing adequately, apply high-flow oxygen by non-rebreather mask and initiate transport. If the patient isnot breathing adequately, provide mechanical ventila-tion with supplemental oxygen and initiate transport.
Standard Operational ProceduresThe EMT must be familiar with the operation of thedevice that is used in his or her EMS system. No AEDcan work without properly functioning batteries.Thus the EMT should check to see that the batteriesare in working order at the beginning of each shift.Extra batteries also should be carried and should beaccessible at all times.
Although rapid defibrillation is of utmost impor-tance, airway and ventilation are prime concerns forthe patient also. As emphasized in previous learning,the body and the brain cannot survive without oxy-gen. Therefore, manage airway and breathing concur-rently while carrying out the AED protocol. Stay clearof patients when the AED is analyzing and deliveringshocks, but provide airway support and ventilationswhen performing CPR.
If the patient has persistent ventricular fibrilla-tion (the machine repeatedly advises to deliver ashock) and there is no ACLS available, transport assoon as possible. Additional shocks may be deliv-ered to the patient in persistent ventricular fibrilla-tion en route. Automated external defibrillatorscannot analyze a rhythm accurately when an emer-gency vehicle is in motion. Thus you first must havethe driver stop the vehicle before you have the AEDanalyze the patient’s cardiac rhythm. Defibrillationin a moving vehicle is never safe because of the po-tential for the rescuer to be shocked.
If en route with an unconscious patient who has apulse or a patient who has been resuscitated but isunresponsive, monitor the patient’s pulse frequently(every 30 seconds). If you subsequently determinethat a pulse is not present, do the following:
• Stop the vehicle.• Start CPR if the defibrillator is not immediately
available.
• Once the AED is attached, analyze the rhythm.• Deliver one shock if indicated.• Resume CPR for 5 cycles.• Continue transport.
Single Rescuer with AutomatedExternal DefibrillatorAs a professional provider, you likely will not findyourself in a position of being a lone rescuer on acall. However, in the event this should occur, followthis sequence for using the AED:
• Perform the initial assessment (airway, breathing,and circulation).
• Ensure the patient is pulseless and apneic.• Turn on AED power.• Attach the device to the patient.• Initiate rhythm analysis.• Deliver the shock if directed.• Follow AED protocol.
Your protocols should have criteria in place for us-ing ACLS tiers within your EMS system. Advancedcardiac life support is not required in order to use anAED; however, ACLS is a link in the chain of survival.Advanced cardiac life support can provide ongoingadditional care for the patient in cardiac arrest. Im-plement ACLS as soon as possible. Protocols estab-lished by medical direction should explain what ac-
CHAPTER 18 ■ Cardiovascular Emergencies 365
The automated external defibrillator gener-ally is not used for patients under the age of1 year old. Most children experience car-diac arrest following respiratory arrest. Au-tomated external defibrillators designed foradults may deliver a shock that has toomuch energy for a child less than 55 lb.This can cause additional damage to themyocardium. Many AED manufacturers nowoffer child pads that deliver less energy.Use these pads for children if available. Ifchild pads are not available, use adult pads.Consult medical direction and become fa-miliar with your local protocols and equip-ment for recommendations on using the au-tomated external defibrillator for pediatricpatients.
Ch18-E4000_346-377 7/27/06 2:57 PM Page 365

tions to carry out if you are waiting for ACLS to arriveon scene.
The AED is an electrical device and should behandled appropriately. Never operate the AED in ornear water or in the rain. Water can transport anelectric current from the device not only to the pa-tient but also to the rescuer and bystanders if usedin or near water. If necessary, move the patient tothe ambulance and remove any wet clothing he or
she may be wearing. When operating the AED, besure the patient is not touching anything metal.Metal also has the ability to transmit the electriccurrent. The possibility of electric current beingtransmitted when delivering a shock to the patientis an important consideration when clearing by-standers.
Postresuscitation CareIf the patient remains pulseless once the AED proto-col has been completed, follow local protocol re-garding transport with CPR, ACLS tier activation andrendezvous, and continued use of the AED. If the pa-tient does regain a pulse after AED protocol has beenfollowed, ensure a patent airway and maintain basiclife support. Keep the AED attached to the patientwhile transporting to the receiving facility. Continuewith a focused assessment and ongoing assessmenten route. Be sure to reassess frequently any interven-tions you have initiated.
DocumentationDocumentation is an important part of ongoingmedical care for the patient. Document the initialand ongoing assessments and interventions per-formed. Also document any response or lack of re-sponse to interventions you have performed. Docu-mentation should include shocks that have beendelivered and analysis of no shocks advised. Also doc-ument the patient’s vital signs and airway, breathing,and circulatory status during the AED protocol. Somesystems use a standard documentation form for pa-tients with cardiac arrest with AED use. This may behelpful in documenting the event.
Defibrillator MaintenanceDefibrillators require regular maintenance. The EMTshould complete a maintenance checklist every shift(Fig. 18-9). Each unit the system has should bechecked. Defibrillator failure is usually due to im-proper maintenance, most commonly battery failure.
366 ■ EMERGENCY MEDICAL TECHNICIAN
An occasion may arise when you are calledto the scene of a cardiac arrest and familymembers or bystanders inform you the pa-tient does not wish to have resuscitativemeasures taken. It is important that yoube informed of your local laws in this typeof situation and follow the appropriateprotocol.
You may encounter a patient who has an im-planted device such as a pacemaker or animplanted defibrillator. Treatment for thesepatients remains the same as for any otherpatient exhibiting signs and symptoms of acardiac emergency. If cardiac arrest occursin these situations, continue with protocolsfor cardiopulmonary resuscitation and use ofthe automated external defibrillator just asyou would with any other patient. The onlyadjustments you need to make are to be sureto place the automated external defibrillatoradhesive patches a few inches away from theimplanted device and to inform medical con-trol of the patient’s history.
Ch18-E4000_346-377 7/27/06 2:57 PM Page 366

A schedule for regular replacement of batteriesshould be established. The American Heart Associa-tion has published information regarding guidelinesand additional information for the use of automatedexternal defibrillation.
Skills MaintenanceMost systems require a 90-day rotation of skills veri-fication for operation of the AED. To be well pre-pared during a cardiac event, you should practiceyour skills frequently, incorporating various cardiacarrest scenarios.
Training to use an AED as an EMT does not au-tomatically allow you to use it legally. State lawsand rules and local medical direction will deter-mine whether your EMS system is allowed to usedefibrillation during a cardiac arrest event. Everycardiac arrest call with an AED used should be re-viewed by the medical director or his designee. Reviews can be written reports or, if used, voicerecording or solid state or magnetic tape recordingsthat are stored in the AED. Reviewing AED callshelps to aid in quality improvement and assurance.The review process should involve review of opera-tor performance and review of the EMS system as a whole. This will help to ensure that every link in the chain of survival has been established and is used.
■ VASCULAR EMERGENCIES
All chest pain is not cardiac. The great vessels sharethe chest cavity with the heart, and disorders of or in-jury to these structures can cause pain and dysfunc-tion that may mimic cardiac problems.
AneurysmsThis is a weakening and dilation of the artery wall.The layers that make up the artery separate, and a
hematoma or bulge develops. This bulge can impaircirculation beyond the aneurysm and it can leak orrupture, creating complications in the chest cavity orshock and death.
Aortic DissectionOver 85% of aortic dissections present as acute chestpain. Patients most frequently will describe abruptsevere chest pain. Often patients describe the pain asgoing to the back between the scapulas. Many pa-tients describe a “ripping or tearing” sensation intheir chest.
The condition is caused by a tear that causes the layers in the aorta to separate, and blood canthen enter between the layers, further separatingthem. This can happen spontaneously, often in patients with hypertension, or it can be brought on by trauma or possibly medical procedures likecatheterizations.
During assessment, vital signs may indicate exten-sion of the developing dissection. As blood flow intothe arteries branching off the aorta is compromised,the pulse in one or more extremity may be dimin-ished or obliterated. This condition can cause furthercardiac complications by involving the coronary ar-teries, and rupture of the dissection can cause bleed-ing into the pericardial space.
These patients require urgent medical or surgicalintervention depending on the location of theaneurysm. Field care will include IV access and infu-sions, at least 95% oxygen by mask, and expeditioustransport to an appropriate facility.
Vascular OcclusionsVascular occlusions occur particularly in patients be-tween the ages of 50 and 70. Narrowing of the vesselsdue to chronic atherosclerotic disease further compli-cated by emboli can narrow and obstruct arteries.Sudden occlusion of a vessel will cause hypoxia tothe tissues counting on the vessel for its blood sup-
CHAPTER 18 ■ Cardiovascular Emergencies 367
Ch18-E4000_346-377 7/27/06 2:57 PM Page 367

368 ■ EMERGENCY MEDICAL TECHNICIAN
Fig
.18-9
Au
tom
ated
ext
ern
al d
efib
rill
ato
r o
per
ato
r ch
eckl
ist.
Ch18-E4000_346-377 7/10/06 11:14 M Page 368

CHAPTER 18 ■ Cardiovascular Emergencies 369
Fig
.18-9
,cont’d
Au
tom
ated
ext
ern
al d
efib
rill
ato
r o
per
ato
r ch
eckl
ist.
Ch18-E4000_346-377 7/10/06 11:14 M Page 369

ply. These patients present with sudden onset pain,paresthesia, paralysis, and pulselessness to the ex-tremity deprived of circulation.
These patients require definitive care at the hospi-tal, and management focuses on IVs, oxygen, and car-diac monitoring (possible movement of clots andcardiac complications).
Deep Vein ThrombosisTrauma, prolonged immobility, advanced age, birthcontrol pills, cancer, obesity, pregnancy, and otherconditions can promote development of clots. Mostcommonly, older women are affected, and calves andthighs are most often the sites.
When red blood cells and platelets for thrombi at-tach to vessel walls, blood flow is occluded. Thesethrombi can break off and move, creating pulmonaryemboli. Inflammation of venous walls where thrombihave attached is called thrombophlebitis.
Pain and swelling are common in patients withdeep vein thrombosis due to partial or complete ob-struction of blood flow. Redness and warmth andhardness to the extremity are common. The involvedextremity should be immobilized, and the patientshould be monitored for possible progression ofclots into the lungs.
Emergency medical technicians can offer three ofthe links in the chain of survival: early EMS, earlyCPR, and early defibrillation. Once these are accom-
370 ■ EMERGENCY MEDICAL TECHNICIAN
You and your emergency medical technician part-ner have just finished your shift checks, restockingand checking your ambulance equipment, whenyou are dispatched to a local public eating estab-lishment for an adult patient who is complainingof chest pain.
• While en route to the scene, what can you doto prepare for this call?
• What essential equipment should you takewith you to the patient’s side?
The scene is safe, and as you approach the pa-tient, you see an adult man, approximately 70years of age who is sitting upright on a chair. Thepatient appears alert but pale and diaphoretic.
• What information is important to gather aboutthis patient’s history?
• What essential links in the chain of survivalhave been established up to this point?
• As an emergency medical technician, whatcan you do to continue the chain of survivalfor this patient?
The patient states he has a history of cardiacproblems. He also explains that his chest painstarted about an hour ago and has become increas-ingly worse.
• What questions should you ask this patientabout his chest pain?
• What tool can you use to help gauge the sever-ity of this patient’s pain?
• What intervention can you provide to this pa-tient at this time?
The patient states he takes nitroglycerin andhas it with him.
• What factors are important in determiningwhether nitroglycerin should be given to this pa-tient?
You have determined the patient has no con-traindications for nitroglycerin use and have con-tacted medical control. Medical control directsyou to proceed with assisting this patient in ad-ministering nitroglycerin.
• What things should you confirm before givingthe nitroglycerin?
• What questions can you ask this patient to de-termine whether the nitroglycerin is helping?
• What is the maximum dose of nitroglycerinthis patient can take?
With your assistance and instruction, your pa-tient has taken one dose of nitroglycerin. He stateshe is afraid he is dying and suddenly slumps over.You and your partner lower him to the floor. Yourpartner confirms the patient is unresponsive,breathless, and pulseless.
What is the most important intervention youcan provide for this patient at this time?
Ch18-E4000_346-377 7/10/06 11:14 M Page 370

plished, the next link, early advanced care, needs tobe activated. Advanced cardiac life support offers thepatient further treatment in the fight against cardiacarrest. Specific advanced procedures and drug therapywork best for the patient when accessed as early aspossible. Emergency medical technicians should acti-vate and request ACLS services as soon as they areaware the patient is in a cardiac crisis.
Even with the recognized need for advanced lifesupport, the value of basic life support offered by
EMTs cannot be understated. Without excellent basiclife support techniques, advanced life support meas-ures are futile. From the layperson to the advancedcare provider, cardiac emergencies are conditions thattruly do take a team effort to create the best outcomepossible for the patient.
Reference1. American Heart Association: Circulation 112(24)(suppl),
December 13, 2005.
ResourcesAmerican Heart Association: Circulation 112(24)(suppl),
December 13, 2005.EMS Magazine: The Journal of Emergency Care, Rescue and
TransportationJEMS: A Journal of Emergency Medical Services
CHAPTER 18 ■ Cardiovascular Emergencies 371
Jack held onto Mr. Markham’s hand. He waslooking very sick; Jack had never seen someoneso ashen. The ambulance moved swiftly towardthe hospital, with Elizabeth providing an urgentreport over the radio to the receiving hospital.“The patient’s blood pressure has been decreas-ing over the past 20 minutes, but he remainsalert. We have him on high-flow oxygen, and ourETA is less than 5 minutes.” Hanging up the ra-dio, Elizabeth looked at Jack. “Not giving himthe nitro–does that make sense to you?”
Jack nodded. “His BP was too low to supporta drug that tends to lower blood pressure by itsmechanism of action.”
“Unfortunately, that is true in this case. Evenif it could help, it’s too dangerous. We can onlyhope that we get him to a coronary care unitwhere they might be able to help.” ■
conclusionEvery link in the chain of survival needs to be re-alized in order for the patient to have the bestchance of survival and the best outcome from acardiac event. Early access to emergency med-ical services involves the patient or bystandersrecognizing a cardiac emergency. Early car-diopulmonary resuscitation from bystanders andemergency medical services is crucial in thefight against time in saving these patients.
Ch18-E4000_346-377 7/27/06 2:57 PM Page 371

Critical Points
Cardiac events can be considered true emergen-cies for the patient and the prehospital provider.An essential part of caring for a patient with car-diac disease is acting quickly to assess your pa-tient and determine the nature of the chest pain.As an emergency medical technician, you mustknow your protocols and must be proficient atskills required in managing a cardiac emergency.Cardiac events are emergencies in which emer-gency medical services truly can make a differ-ence in the patient’s outcome.
Learning Checklist
❑ Sudden cardiac arrest accounts for morethan 300,000 deaths per year, with up tohalf of those deaths occurring in the prehos-pital setting. Sudden cardiac arrest is oftenthe first warning sign a person displays ofcardiac disease.
❑ Cardiac events are true medical emergencies.❑ The circulatory system is a transport system
for the body. This system includes the heartand arterial and venous systems.
❑ The circulatory system transports oxygen andnutrients to the body and removes wastefrom the tissues.
❑ The heart is made up of two sides: the rightside and the left side. Both sides have anatrium and a ventricle.
❑ The right atrium receives oxygen-poor bloodfrom the body.
❑ The right ventricle pumps the oxygen-poorblood to the lungs to replenish oxygen.
❑ The left atrium receives oxygenated bloodfrom the lungs. The left ventricle pumps theoxygenated blood out to the body.
❑ Arteries carry oxygenated blood away fromthe heart.
❑ Veins carry deoxygenated blood back to theheart.
❑ Capillaries are vessels in which the exchangeof oxygen for carbon dioxide occurs.
❑ The largest artery in the body is the aorta.❑ The aorta divides into the iliac arteries.❑ The pulmonary artery originates in the right
ventricle of the heart and delivers blood to
the lungs to be oxygenated. The pulmonaryartery is the only artery in the body thatcarries deoxygenated blood.
❑ Carotid arteries supply the head with blood.❑ Femoral arteries supply the lower body with
blood.❑ Radial arteries supply the lower arm and
hand with blood.❑ Brachial arteries most commonly are used to
obtain a patient’s blood pressure reading.❑ Tibial pulses are located near the inside of
the ankle.❑ Dorsalis pedis pulse can be felt on the top of
the foot.❑ Pulses are felt when an artery runs along a
bony prominence.❑ The primary function of the veins is to carry
deoxygenated blood back to the heart.❑ The pulmonary vein carries blood to the left
atrium of the heart from the lungs.❑ The pulmonary vein is the only vein in the
body that carries oxygenated blood.❑ The venae cavae are the major veins of the
body and consist of two branches: the supe-rior vena cava and the inferior vena cava.The superior vena cava carries oxygen-depleted blood from the head and arms. Theinferior vena cava carries oxygen-depletedblood from the lower extremities and thetorso.
❑ Blood consists of red blood cells, whiteblood cells, plasma, and platelets.
❑ Signs and symptoms of shock are pale, cyan-otic, cool, clammy skin; weak, rapid pulse;rapid, shallow breathing; restlessness,anxiety, or mental dullness; nausea or vom-iting; and decreased or low blood pressure.
❑ Cardiac chest pain may not be described aspain but as an ache, pressure, tightness, orsqueezing sensation. The pain also may radiateinto the jaw, arms, back, or epigastric region.
❑ Sudden onset of diaphoresis may be theonly significant symptom of cardiac compro-mise. Anxiety, restlessness, and dyspnea alsocan be associated with cardiac emergencies.
❑ Angina, ischemia, or myocardial infarct canproduce similar symptoms.
❑ Initial assessments for cardiac emergenciesare the same as they are for any other type ofemergency.
372
Ch18-E4000_346-377 7/10/06 11:14 M Page 372

❑ Apply high-flow oxygen to patients withcardiac disease as soon as possible.
❑ Obtaining a patient’s medical history isimportant in determining the nature of thechest pain.
❑ Allow the patient to remain in a position ofcomfort if at all possible.
❑ Never allow a patient with cardiac disease tomove about or to walk.
❑ Transport patients with cardiac disease withcaution, realizing that lights and sirens maycause additional anxiety to the patient andstress to the heart.
❑ Use the OPQRST acronym when assessingpatients with chest pain.
❑ Use nitroglycerin for cardiac chest pain if thepatient meets all of the criteria for it andshows no contraindications. Additionally,the patient must be alert.
❑ Up to three doses of nitroglycerin may be administered if approved by medicaldirection.
❑ Monitor patient vital signs before and afterthe administration of nitroglycerin.
❑ Do not give nitroglycerin to patients with asystolic blood pressure less than 100 mm Hg.
❑ Perform frequent reassessments for anypatient with chest pain.
❑ Ventricular fibrillation is a heart condition.With this condition the heart produces elec-trical signals in a rapid and chaotic mannerthat does not allow the heart to pump bloodto the body effectively. Defibrillation canreverse ventricular fibrillation of the heart.
❑ The emergency medical technician mustbecome proficient with using the automatedexternal defibrillator during a cardiac arrest.Time is crucial for the survival of victims ofcardiac arrest.
❑ The rescuer is responsible for clearingbystanders when the automated externaldefibrillator is analyzing and shocking thepatient.
❑ The emergency medical technician shouldnever analyze or shock the heart while in amoving vehicle or while moving the patient.
❑ Apply the automated external defibrillator onlyto patients who are breathless and pulseless.
❑ Advanced cardiac life support is an impor-tant part of the chain of survival. Request it(if available) for all patients with cardiacdisease.
❑ Most automated external defibrillator manu-facturers now offer child pads that deliverless energy than adult pads, and should beused for all pediatric patients when avail-able. If not available, use adult pads.
❑ The automated external defibrillator is anelectric device and should not be handled inwater. Remove wet clothing from the patientbefore applying the automated externaldefibrillator.
❑ Documentation of the events of any cardiaccall, including events while using the auto-mated external defibrillator, is important.Accurate documentation is needed for thecontinuum of patient care.
❑ Maintenance of the automated externaldefibrillator should be performed at everyshift. Batteries should be checked, and sparebatteries should be on hand and readilyaccessible. Mechanical failure of the auto-mated external defibrillator is most com-monly due to human error and batteries thatare not working.
❑ Emergency medical technicians are respon-sible for maintaining their skills. Automatedexternal defibrillator skills verificationshould be done at least every 90 days.
❑ Even though emergency medical techniciansare trained to use an automated externaldefibrillator, they need to be familiar withtheir local laws and rules regarding the useof automated external defibrillators by emer-gency personnel.
373
Ch18-E4000_346-377 7/27/06 2:57 PM Page 373

Key Terms
Angina Chest discomfort felt upon exertion andusually relieved when resting.
Aorta The largest artery in the body. It originatesfrom the heart and lies in front of the spinein the thoracic and abdominal cavities.
Arteries Blood vessels that carry oxygenatedblood out to the body.
Arterioles Smallest arteries of the body.Asystole Event in which the heart has no
rhythm and has ceased all electrical activity.Atrium Upper chamber of the heart. The heart
has a right atrium that receives oxygen-depleted blood from the body, and a leftatrium that receives oxygen-enriched bloodfrom the lungs.
Automated external defibrillator Machine that isdesigned to deliver a shock for defibrillationof a cardiac rhythm known as ventricular fib-rillation.
Blood The fluid in the body that is made up ofred blood cells, white blood cells, platelets,and plasma.
Blood pressure The pressure the blood exertsagainst the walls of the blood vessels.
Brachial artery The major artery of the upper arm.Capillaries Tiny vessels that allow the exchange
of oxygen and carbon dioxide and nutrientsand waste to occur.
Cardiac arrest The halting of all functioningheart activity.
Cardiac compromise A term used for harmfulcardiac conditions.
Carotid arteries Arteries that supply the headand neck with blood.
Chain of survival A term used by the AmericanHeart Association to define a series ofactions that include early access to emer-gency medical services, early cardiopul-monary resuscitation, early defibrillation,and early advanced cardiac life support.
Clear the patient A phrase used to describe theaction an emergency medical technicianmust take to ensure that no bystander istouching the patient while the emergencymedical technician is analyzing or shockingwith an automated external defibrillator.
Contraindications Reasons or factors that pro-hibit administration of a drug.
Defibrillation Administering a shock to a patientin ventricular defibrillation in order to causethe heart to regain function.
Defibrillator Name for a machine that defibril-lates specific cardiac arrhythmias.
Diastolic blood pressure The pressure applied tothe blood vessels during the relaxation phaseof cardiac contractions. Represented as thebottom number of a blood pressure reading.
Dorsalis pedis artery Artery that supplies thefoot with blood.
Dosage Amount of a medication that should beadministered.
Femoral artery Artery that supplies the upperand lower leg with blood.
Iliac arteries Arteries that supply the lowerextremities with oxygen and nutrient-enriched blood.
Indications Conditions in which administeringa specific drug may benefit the patient.
Inferior vena cava Large vein that carriesoxygen-poor blood from the lower extremi-ties and torso.
Ischemia When an area of the heart muscle isnot receiving enough oxygen.
Myocardial Referring to cardiac muscle.Myocardial infarct Heart attack; caused when an
artery of the heart is blocked partially orcompletely, causing damage to the heart.
Nitroglycerin The generic name for a drug thatacts to dilate the blood vessels, decreasingthe workload of the heart.
Plasma Fluid in the blood that helps move theblood cells and platelets.
Platelets Cells that cause the blood to clot inorder to stop bleeding.
Public access defibrillation Laypersons trainedto use an automated external defibrillator inpublic areas.
Pulmonary artery Artery that carries deoxy-genated blood from the right ventricle of theheart to the lungs.
Pulmonary vein Vein that carries oxygenatedblood from the lungs to the left atrium ofthe heart.
Pulse Area where an artery can be felt over abony prominence in the body when theheart contracts.
Radial artery Artery located on the thumb sideof the wrist.
374
Ch18-E4000_346-377 7/10/06 11:15 M Page 374

Red blood cells Cells that carry oxygen and aretransported in the blood.
Semiautomated external defibrillator Type ofautomated external defibrillator that requiresoperator direction to analyze and shock.
Septum The wall that divides the right side ofthe heart and the left side of the heart.
Shock The inadequate delivery of oxygen andnutrients to cells, resulting in organ systemmalfunction. Eventually shock is detectablewith abnormal vital signs. It can lead todeath.
Sphygmomanometer The cuff and gauge used tomeasure the blood pressure.
Sublingual Under the tongue.Superior vena cava Large vein that carries
oxygen-poor blood from the head and arms.Systolic blood pressure The pressure applied to
the blood vessels during the contractionphase of the cardiac cycle. Represented as thetop number of a blood pressure reading.
Tibial artery Artery located in the lower extremi-ties.
Tier Action of continued care when a prehos-pital emergency medical services system con-tinues care with an advanced prehospitalemergency medical system.
Trendelenburg’s position A position in which thebody is supine with the feet elevated andhead down.
Veins Vessels that carry deoxygenated bloodback to the heart.
Venae cavae Major veins that carry blood backto the right atrium of the heart from thebody.
Venous system System of veins in the body.Ventricle Lower chamber of the heart. The heart
has a right ventricle that pumps deoxy-genated blood to the lungs and a left ventri-cleal that pumps oxygenated blood to thebody.
Ventricular fibrillation A rapid, chaotic cardiacrhythm in which the heart “quivers” withelectrical impulses but fails to contract.
Ventricular tachycardia Rapid heartbeat thatdoes not allow the heart time to fill andpump blood properly.
Venules Smallest size of vein.White blood cells Cells in the blood that help
the body fight infection.
National Standard Curriculum Objectives
Cognitive ObjectivesAfter completing this lesson, the EMT student will beable to do the following:
■ Describe the structure and function of thecardiovascular system.
■ Describe the emergency medical care of thepatient experiencing chest pain/discomfort.
■ List the indications for automated externaldefibrillation.
■ List the contraindications for automatedexternal defibrillation.
■ Define the role of emergency medical techni-cian in the emergency cardiac care system.
■ Explain the impact of age and weight ondefibrillation.
■ Discuss the position of comfort for patientswith various cardiac emergencies.
■ Establish the relationship between airwaymanagement and the patient with cardiovas-cular compromise.
■ Predict the relationship between the patientexperiencing cardiovascular compromise andbasic life support.
■ Explain that not all patients with chest painexperience cardiac arrest and do not need to beattached to an automated external defibrillator.
■ Explain the importance of prehospitaladvanced cardiac life support intervention ifit is available.
■ Explain the importance of urgent transportto a facility with advanced cardiac lifesupport if it is not available in the prehos-pital setting.
■ Discuss the various types of automatedexternal defibrillators.
■ Differentiate between the fully automatedand the semiautomated defibrillator.
■ Discuss the procedures to take into consider-ation for standard operations of the varioustypes of automated external defibrillators.
■ State the reasons for ensuring that thepatient is pulseless and apneic when usingthe automated external defibrillator.
■ Discuss the circumstances that may result ininappropriate shocks.
375
Ch18-E4000_346-377 7/27/06 2:57 PM Page 375

■ Explain the considerations for interruptionof cardiopulmonary resuscitation whenusing the automated external defibrillator.
■ Discuss the advantages and disadvantages ofautomated external defibrillators.
■ Summarize the speed of operation of auto-mated external defibrillation.
■ Discuss the use of remote defibrillationthrough adhesive pads.
■ Discuss the special considerations forrhythm monitoring.
■ List the steps in the operation of the auto-mated external defibrillator.
■ Discuss the standard of care to use toprovide care to a patient with persistent ven-tricular fibrillation and no availableadvanced cardiac life support.
■ Discuss the standard of care to use toprovide care to a patient with recurrent ven-tricular fibrillation and no availableadvanced cardiac life support.
■ Explain the reason for not checking pulsesbetween shocks with an automated externaldefibrillator.
■ Discuss the importance of coordinatingproviders trained in advanced cardiac lifesupport with personnel using automatedexternal defibrillators.
■ Discuss the importance of postresuscitationcare.
■ List the components of postresuscitationcare.
■ Explain the importance of frequent practicewith the automated external defibrillator.
■ Discuss the need to complete the AutomatedDefibrillator: Operator’s Shift Checklist.
■ Discuss the role of the American Heart Asso-ciation in the use of automated externaldefibrillation.
■ Explain the role medical direction plays inthe use of automated external defibrillation.
■ State the reasons why a case review shouldbe completed following the use of the auto-mated external defibrillator.
■ Discuss the components that should beincluded in a case review.
376
Ch18-E4000_346-377 7/27/06 2:57 PM Page 376

■ Discuss the goal of quality improvement inautomated external defibrillation.
■ Recognize the need for medical direction ofprotocols to assist in the emergency medicalcare of the patient with chest pain.
■ List the indications for the use of nitroglyc-erin.
■ State the contraindications and side effectsfor the use of nitroglycerin.
■ Define the function of all controls on anautomated external defibrillator, anddescribe event documentation and batterydefibrillator maintenance.
Affective ObjectivesAfter completing this lesson, the EMT student will beable to do the following:
■ Defend the reasons for obtaining initialtraining in automated external defibrillationand the importance of continuing education.
■ Defend the reason for maintenance of auto-mated external defibrillators.
■ Explain the rationale for administering nitro-glycerin to a patient with chest pain or dis-comfort.
Psychomotor ObjectivesAfter completing this lesson, the EMT student will beable to do the following:
■ Demonstrate the assessment and emergencymedical care of a patient experiencing chestpain/discomfort.
■ Demonstrate the application and operationof the automated external defibrillator.
■ Demonstrate the maintenance of an auto-mated external defibrillator.
■ Demonstrate the assessment and documen-tation of patient response to the automatedexternal defibrillator.
■ Demonstrate the skills necessary to completethe Automated Defibrillator: Operator’s ShiftChecklist.
■ Perform the steps in facilitating the use ofnitroglycerin for chest pain or discomfort.
■ Demonstrate the assessment and documen-tation of patient response to nitroglycerin.
■ Practice completing a prehospital care reportfor patients with cardiac emergencies.
377
Ch18-E4000_346-377 7/10/06 11:15 M Page 377