Embed Size (px)
Citation preview

8/7/2018
1/33
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e >
Chapter 185: AlcoholsJennifer P. Cohen; Dan Quan
INTRODUCTION
All alcohols cause clinical inebriation, with the strength of the inebriating e�ects directly proportional to thealcohol's molecular weight; hence, at the same concentration, isopropanol is more intoxicating than ethanol(Figure 185–1).
FIGURE 185–1.
Chemical structures of the common alcohols.
Primary toxicity can be due to the parent compound (ethanol and isopropanol) or to toxic metabolites(ethylene glycol and methanol). Ethanol and isopropanol are the most common alcohols ingested; theirprincipal e�ects are GI irritation and intoxication; and they do not in themselves produce metabolic acidosis.Methanol and ethylene glycol are toxic alcohols because they cause serious physiologic morbidity.
ETHANOL
INTRODUCTION
Ethanol (CH3CH2OH, molecular weight 46.07) is a colorless, volatile liquid that is the most frequently used
and abused drug in the world. Morbidity from acute ethanol intoxication is usually related to secondaryinjuries rather than direct toxic e�ects. Toxicity most commonly occurs from ingestion, but ethanol may alsobe absorbed via inhalation or percutaneous exposure.
Ethanol is readily available in many di�erent forms. A standard alcoholic beverage, such as 12 oz (355 mL) ofbeer (2% to 6% ethanol by volume), 5 oz (148 mL) of wine (10% to 20% ethanol by volume), or 1.5 oz (44 mL)

8/7/2018
2/33
of 80-proof spirits (40% ethanol by volume), contains about 15 grams of ethanol. Ethanol may be found inhigh concentrations in many other common household products such as mouthwash (may contain up to 75%ethanol by volume), colognes and perfumes (up to 40% to 60%), and as a diluent or solvent for medications(concentration varies widely between 0.4% and 65%). Such products are o�en flavored or brightly coloredand may be attractive to children.
PATHOPHYSIOLOGY
Ethanol is rapidly absorbed a�er oral administration, and blood levels peak about 30 to 60 minutes a�eringestion. The presence of food in the stomach prolongs absorption and delays the peak blood level. Highconcentrations of ethanol in the stomach may cause pylorospasm delaying gastric emptying. Some ethanolis broken down in the stomach by gastric alcohol dehydrogenase, which lowers the amount available forabsorption. This enzyme is present at higher levels in men than in women, which may account for the factthat women usually develop a higher blood ethanol level than men a�er consuming the same dose perkilogram of body weight. The volume of distribution of ethanol is also gender dependent due to di�erence inbody fat percentages: 0.6 L/kg in men and 0.7 L/kg in women.
Ethanol is a CNS depressant1 that enhances the inhibitory neurotransmitter γ-aminobutyric acid receptorsand blockade of excitatory N-methyl-d-aspartic acid receptors. Modulation of these systems leads to thedevelopment of tolerance, dependence, and a withdrawal syndrome when ethanol intake ceases independent individuals.
Because of the phenomenon of tolerance, blood ethanol levels correlate poorly with degree of intoxication.Although death from respiratory depression may occur in nonhabituated individuals at concentrations of 400to 500 milligrams/dL (87 to 109 mmol/L), some alcoholic individuals can appear minimally intoxicated at
blood concentrations as high as 400 milligrams/dL (87 mmol/L).2 Although Canada, Mexico, and the UnitedStates have adopted 80 milligrams/dL (17 mmol/L) as the legal definition of intoxication for the purposes ofdriving a motor vehicle, impairment may occur with levels as low as 50 milligrams/dL (11 mmol/L), especially
in nonhabituated individuals.3
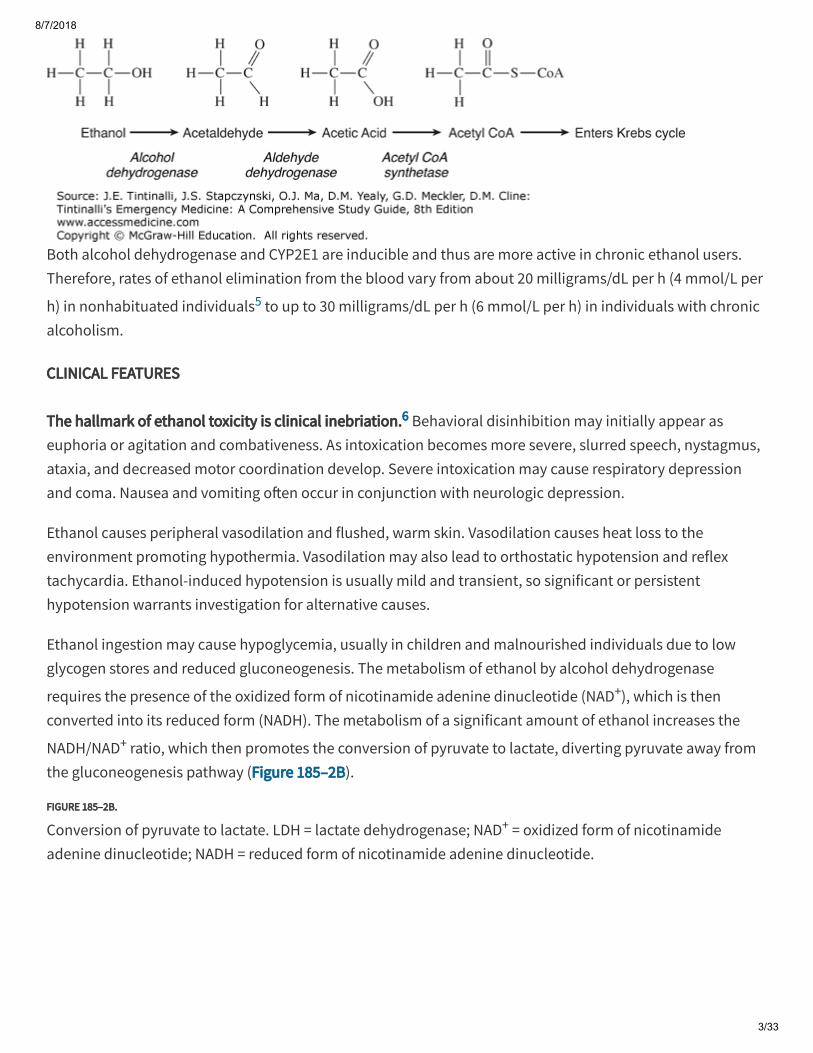
Ethanol is predominantly eliminated by hepatic metabolism, with about 10% excreted in the urine, exhaledbreath, and sweat. Alcohol dehydrogenase (Figure 185–2A) is the major enzyme involved in the metabolism
of ethanol, producing acetaldehyde. At low ethanol concentrations, this process follows first-order kinetics,4
but as concentrations rise, alcohol dehydrogenase becomes saturated and metabolism switches to zero-order kinetics—a fixed amount is metabolized per unit of time. Also, as ethanol concentrations rise, thehepatic microsomal oxidizing system (specifically, cytochrome P-450 2E1 [CYP2E1]) plays a more importantrole in metabolism.
FIGURE 185–2A.
Metabolism of ethanol. CoA = coenzyme A.
8/7/2018
3/33
Both alcohol dehydrogenase and CYP2E1 are inducible and thus are more active in chronic ethanol users.Therefore, rates of ethanol elimination from the blood vary from about 20 milligrams/dL per h (4 mmol/L per
h) in nonhabituated individuals5 to up to 30 milligrams/dL per h (6 mmol/L per h) in individuals with chronicalcoholism.
CLINICAL FEATURES
The hallmark of ethanol toxicity is clinical inebriation.6 Behavioral disinhibition may initially appear aseuphoria or agitation and combativeness. As intoxication becomes more severe, slurred speech, nystagmus,ataxia, and decreased motor coordination develop. Severe intoxication may cause respiratory depressionand coma. Nausea and vomiting o�en occur in conjunction with neurologic depression.
Ethanol causes peripheral vasodilation and flushed, warm skin. Vasodilation causes heat loss to theenvironment promoting hypothermia. Vasodilation may also lead to orthostatic hypotension and reflextachycardia. Ethanol-induced hypotension is usually mild and transient, so significant or persistenthypotension warrants investigation for alternative causes.
Ethanol ingestion may cause hypoglycemia, usually in children and malnourished individuals due to lowglycogen stores and reduced gluconeogenesis. The metabolism of ethanol by alcohol dehydrogenase
requires the presence of the oxidized form of nicotinamide adenine dinucleotide (NAD+), which is thenconverted into its reduced form (NADH). The metabolism of a significant amount of ethanol increases the
NADH/NAD+ ratio, which then promotes the conversion of pyruvate to lactate, diverting pyruvate away fromthe gluconeogenesis pathway (Figure 185–2B).
FIGURE 185–2B.
Conversion of pyruvate to lactate. LDH = lactate dehydrogenase; NAD+ = oxidized form of nicotinamideadenine dinucleotide; NADH = reduced form of nicotinamide adenine dinucleotide.

8/7/2018
4/33
When a chronic alcoholic suddenly stops consuming calories in the form of either ethanol or food, the bodyuses alternative fuel sources and begins to break down adipose tissue. This metabolism of fatty acids resultsin ketoacidosis (see chapter 226, Alcoholic Ketoacidosis).
DIAGNOSIS
Ethanol-intoxicated patients o�en have other disease processes, such as infections and traumatic injuries, soperform a detailed physical examination, looking especially for evidence of trauma, and obtain as muchhistory as possible. Uncomplicated ethanol intoxication improves over a few hours. If depressed mentalstatus fails to improve or deteriorates, consider other causes of altered mental status and evaluate
aggressively.7,8
The clinical assessment guides the selection of laboratory tests. For altered levels of consciousness, obtain apoint-of-care glucose level. Ethanol levels are not necessarily required in cases of mild or moderateintoxication when no other abnormality is suspected, but measure serum alcohol levels in patients withaltered mental status of unclear cause. Clinical judgment of ethanol intoxication is unreliable, and self-
reported drinking is also unreliable, particularly around levels of 100 milligrams/dL (22 mmol/L)9,10 or in
alcohol-tolerant patients.11 In isolated ethanol intoxication, the presence of horizontal gaze nystagmus has asensitivity of 70% to 80% for a blood ethanol level of 80 milligrams/dL (17 mmol/L) and a sensitivity of 80% to
90% for blood ethanol levels >100 milligrams/dL (22 mmol/L).12,13,14
Ask about concomitant drug use, especially cocaine. The attraction of abusing these drugs together mayrelate to the formation of the cocaine metabolite cocaethylene that, although less potent than the parent
compound, has a half-life that is three to five times longer.15 The risk of sudden death among users of bothdrugs simultaneously is higher than that among cocaine users alone.
Ethanol ingestion is the most common cause of an osmolar gap on serum electrolyte analysis (see chapter
17, Fluids and Electrolytes) and may be associated with a mild metabolic acidosis,16 but a significant aniongap metabolic acidosis suggests the presence of lactic acidosis, ketoacidosis, or methanol or ethylene glycoltoxicity.
TREATMENT
8/7/2018
5/33
Management is observation until sobriety.6 Activated charcoal is not useful since ethanol is rapidly absorbed;consider activated charcoal only if toxic adsorbable substances have been coingested.
Treat hypoglycemia with IV glucose 0.5 to 1 grams/kg. Although acute Wernicke's encephalopathy can beprecipitated by prolonged sustained administration of IV carbohydrate, there is no evidence that a single
dose of IV glucose can cause this syndrome.17,18 The prevalence of vitamin deficiencies in acutely intoxicated
ED patients is low and does not justify the routine use of IV vitamin-containing fluids.19 However, long-termdrinkers are sometimes treated with IV fluids containing magnesium, folate, thiamine, and multivitamins,termed a banana bag because of the yellow color imparted by the multivitamin mixture. Wernicke'sencephalopathy is characterized by abnormal mental status, ataxia, and nystagmus, and requires dailytreatment with thiamine, 100 milligrams, until normal diet is resumed. Fluid administration does not hastenalcohol elimination, so establishment of IV access for fluid administration alone is unnecessary in
uncomplicated mild to moderate intoxication.20,21
Metadoxine, which is not currently available in the United States but is available in Latin America, Mexico,
Asia, Africa, and Eastern Europe, enhances the metabolism of ethanol and accelerates recovery.6,22
Metadoxine is an ion pair between pyrrolidone carboxylate and pyridoxine. A dose of 900 milligrams IV isreported to double the rate at which ethanol blood levels decrease with time compared with the patient's
own metabolism.23,24
DISPOSITION AND FOLLOW-UP
Patients with acute ethanol intoxication as the only clinical problem require ED observation until sober. Priorto discharge, reassess for an underlying mental health disorder, such as suicidal or homicidal ideation, thatrequires further care or hospital admission. Clinical judgment, rather than a serum ethanol level, determinesthe appropriateness of discharge. Discharge the patient in the care of a responsible companion. Patientstreated for alcohol intoxication should not be responsible for their own transportation home.
ISOPROPANOL
INTRODUCTION
Isopropanol (CH3CHOCH3, molecular weight 60.10), also known as isopropyl alcohol and 2-propanol, is a
colorless, volatile liquid with a bitter, burning taste and an aromatic odor. It is found in many common,inexpensive household products, such as rubbing alcohol (usually 70% isopropanol). Isopropanol is widelyused in industry as a solvent and disinfectant and is a component of a variety of skin and hair products,jewelry cleaners, detergents, paint thinners, and deicers.
Poisoning usually results from ingestion25 but may also occur a�er inhalation or dermal exposure in poorlyventilated areas or during alcohol sponge bathing. Isopropanol is approximately twice as potent as ethanol

8/7/2018
6/33
in causing CNS depression, and its duration of action is two to four times that of ethanol. As a result, it iso�en used as a substitute intoxicant by alcoholics as well as in suicide attempts.
PATHOPHYSIOLOGY
Isopropanol is rapidly absorbed from the GI tract. Its peak blood levels occur 30 to 120 minutes a�eringestion, and its volume of distribution is similar to that of ethanol. The major pathway for the metabolismof isopropanol is in the liver by alcohol dehydrogenase (50% to 80%), with the remainder excretedunchanged in the urine. Isopropanol is metabolized to a ketone, not an acid (Figure 185–3).
FIGURE 185–3.
Metabolism of isopropanol. NAD+ = oxidized form of nicotinamide adenine dinucleotide; NADH = reducedform of nicotinamide adenine dinucleotide.
Ketosis and an osmolar gap without acidosis are the hallmarks of isopropanol toxicity.25,26 The principalmetabolite, acetone, does not cause eye, kidney, cardiac, or metabolic toxicity, although high levels ofacetone may contribute to CNS depression. Acetone is excreted primarily by the kidneys, with someexcretion through the lungs. It takes about 30 to 60 minutes a�er isopropanol ingestion for acetone to appear
in the serum and about 3 hours for it to be detectable in the urine.27
Isopropanol metabolism most closely follows concentration-dependent (first-order) kinetics. The eliminationhalf-life of isopropanol in the absence of ethanol is 6 to 7 hours, whereas the elimination half-life of acetone
is 17 to 27 hours.28 The long half-life of acetone may contribute to the prolonged mental status depressiono�en associated with isopropanol poisoning. The toxic dose of 70% isopropanol is approximately 1 mL/kg,although as little as 0.5 mL/kg may cause symptoms. The minimum lethal dose for an adult has beenreported as approximately 2 to 4 mL/kg, but survival has been reported following ingestions of up to 1 L.Children are especially susceptible to toxic e�ects and may develop symptoms a�er as little as three
swallows of 70% isopropanol.29
CLINICAL FEATURES
8/7/2018
7/33
The primary clinical toxicities of isopropanol are CNS depression caused by both the parent compound and
acetone, and gastric irritation from isopropanol itself.25,26 Onset of symptoms occurs within 30 to 60 minutesa�er ingestion, with peak e�ects in a few hours and duration of symptoms for many hours longer, possiblydue to the contribution of acetone. As with the metabolism of any alcohol by alcohol dehydrogenase, the
increased NADH/NAD+ ratio may produce hypoglycemia.
Gastric irritation appears early and is a striking feature of isopropanol ingestions. GI symptoms range fromnausea, vomiting, abdominal pain, and acute pancreatitis to hemorrhagic gastritis and upper GI bleeding.Severe poisoning is marked by early onset of coma, respiratory depression, and hypotension;rhabdomyolysis and renal failure have also been reported.
Massive ingestion may cause hypotension secondary to peripheral vasodilation. In infants and smallchildren, if isopropanol is used to clean the skin, chemical burns can result and systemic symptoms canoccur from dermal absorption.
DIAGNOSIS
Obtain point-of-care glucose testing and other testing as directed by the history and physical examination.Assess for upper and lower GI bleeding. Suspect isopropanol poisoning if the fruity odor of acetone or thesmell of rubbing alcohol is present on the breath. Other signs are elevated osmolar gap, ketonuria, andketonemia without acidosis. An increased anion gap or metabolic acidosis is not due to isopropanolintoxication, so if either is present, investigate for another cause.
A spurious increase in serum creatinine level as a result of acetone's interference with the colorimetric
creatinine assay is sometimes seen.30,31
Serum isopropanol and acetone levels may be assessed, although isopropanol levels may not be readilyavailable from hospital laboratories. Isopropanol levels of 50 milligrams/dL (8 mmol/L) are o�en associatedwith intoxication in individuals who are not habituated to ethanol, but alcoholic patients may beconsiderably more resistant to the CNS e�ects of isopropanol.
TREATMENT
Treatment is supportive. Do not administer activated charcoal or perform gastric lavage unless indicated bycoingestion of an additional toxic substance. Do not administer fomepizole or ethanol, because themetabolite (acetone) is no more toxic than isopropanol itself, and preventing isopropanol metabolism mayprolong CNS toxicity.
Monitor for respiratory depression, and intubate and ventilate as needed. Hypotension usually responds to IVfluids. Obtain blood for type and cross-match if needed to treat GI bleeding.
8/7/2018
8/33
Consider hemodialysis if hypotension is refractory to conventional therapy or when the isopropanol level is
>400 milligrams/dL (>66 mmol/L).25 However, there is no consensus regarding the need for hemodialysis
even in life-threatening situations.31 Hemodialysis eliminates both isopropanol and acetone.
DISPOSITION AND FOLLOW-UP
Patients with lethargy or prolonged CNS depression should be admitted to the hospital. Those who remainasymptomatic for 4 to 6 hours a�er ingestion may be discharged with referral for substance abuse counselingor mental health evaluation as indicated.
METHANOL AND ETHYLENE GLYCOL
INTRODUCTION
Methanol and ethylene glycol are similar in that the parent compounds possess minor toxicity (both causinginebriation and some direct gastric irritation) but the major toxicity occurs when the liver metabolizes these
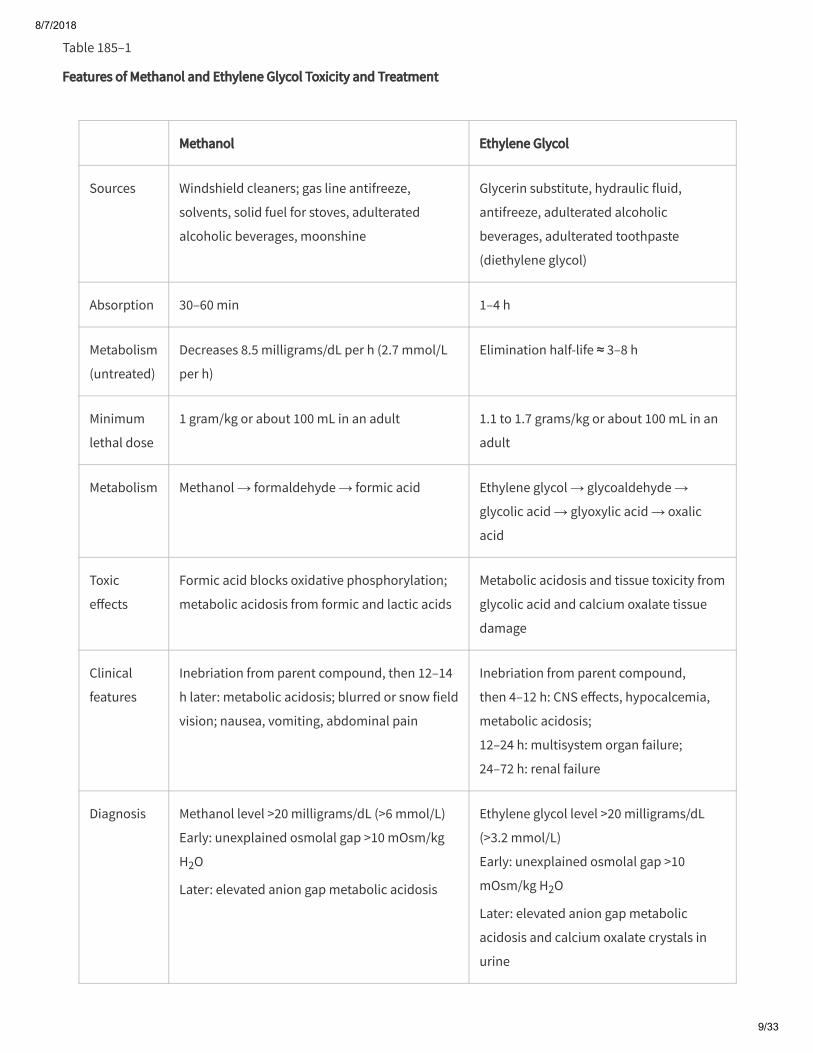
compounds to substances that cause metabolic acidosis and end-organ damage.25,32,33,34 Treatment isprimarily directed toward halting the formation of these toxic metabolites. Table 185–1 provides a summarycomparison of methanol and ethylene glycol metabolism, clinical features, and treatment.
8/7/2018
9/33
Table 185–1
Features of Methanol and Ethylene Glycol Toxicity and Treatment
Methanol Ethylene Glycol
Sources Windshield cleaners; gas line antifreeze,
solvents, solid fuel for stoves, adulterated
alcoholic beverages, moonshine
Glycerin substitute, hydraulic fluid,
antifreeze, adulterated alcoholic
beverages, adulterated toothpaste
(diethylene glycol)
Absorption 30–60 min 1–4 h
Metabolism
(untreated)
Decreases 8.5 milligrams/dL per h (2.7 mmol/L
per h)
Elimination half-life ≈ 3–8 h
Minimum
lethal dose
1 gram/kg or about 100 mL in an adult 1.1 to 1.7 grams/kg or about 100 mL in an
adult
Metabolism Methanol → formaldehyde → formic acid Ethylene glycol → glycoaldehyde →
glycolic acid → glyoxylic acid → oxalic
acid
Toxic
e�ects
Formic acid blocks oxidative phosphorylation;
metabolic acidosis from formic and lactic acids
Metabolic acidosis and tissue toxicity from
glycolic acid and calcium oxalate tissue
damage
Clinical
features
Inebriation from parent compound, then 12–14
h later: metabolic acidosis; blurred or snow field
vision; nausea, vomiting, abdominal pain
Inebriation from parent compound,
then 4–12 h: CNS e�ects, hypocalcemia,
metabolic acidosis;
12–24 h: multisystem organ failure;
24–72 h: renal failure
Diagnosis Methanol level >20 milligrams/dL (>6 mmol/L)
Early: unexplained osmolal gap >10 mOsm/kg
H2O
Later: elevated anion gap metabolic acidosis
Ethylene glycol level >20 milligrams/dL
(>3.2 mmol/L)
Early: unexplained osmolal gap >10
mOsm/kg H2O
Later: elevated anion gap metabolic
acidosis and calcium oxalate crystals in
urine
8/7/2018
10/33
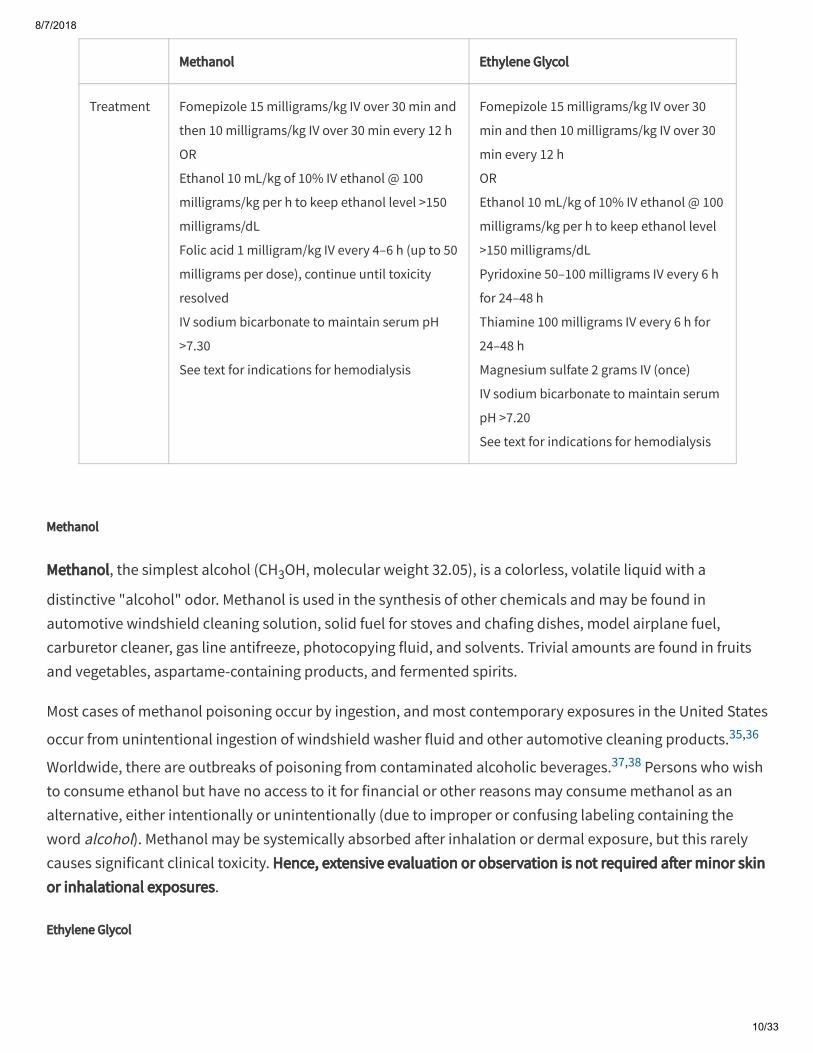
Methanol Ethylene Glycol
Treatment Fomepizole 15 milligrams/kg IV over 30 min and
then 10 milligrams/kg IV over 30 min every 12 h
OR
Ethanol 10 mL/kg of 10% IV ethanol @ 100
milligrams/kg per h to keep ethanol level >150
milligrams/dL
Folic acid 1 milligram/kg IV every 4–6 h (up to 50
milligrams per dose), continue until toxicity
resolved
IV sodium bicarbonate to maintain serum pH
>7.30
See text for indications for hemodialysis
Fomepizole 15 milligrams/kg IV over 30
min and then 10 milligrams/kg IV over 30
min every 12 h
OR
Ethanol 10 mL/kg of 10% IV ethanol @ 100
milligrams/kg per h to keep ethanol level
>150 milligrams/dL
Pyridoxine 50–100 milligrams IV every 6 h
for 24–48 h
Thiamine 100 milligrams IV every 6 h for
24–48 h
Magnesium sulfate 2 grams IV (once)
IV sodium bicarbonate to maintain serum
pH >7.20
See text for indications for hemodialysis
Methanol
Methanol, the simplest alcohol (CH3OH, molecular weight 32.05), is a colorless, volatile liquid with a
distinctive "alcohol" odor. Methanol is used in the synthesis of other chemicals and may be found inautomotive windshield cleaning solution, solid fuel for stoves and chafing dishes, model airplane fuel,carburetor cleaner, gas line antifreeze, photocopying fluid, and solvents. Trivial amounts are found in fruitsand vegetables, aspartame-containing products, and fermented spirits.
Most cases of methanol poisoning occur by ingestion, and most contemporary exposures in the United States
occur from unintentional ingestion of windshield washer fluid and other automotive cleaning products.35,36
Worldwide, there are outbreaks of poisoning from contaminated alcoholic beverages.37,38 Persons who wishto consume ethanol but have no access to it for financial or other reasons may consume methanol as analternative, either intentionally or unintentionally (due to improper or confusing labeling containing theword alcohol). Methanol may be systemically absorbed a�er inhalation or dermal exposure, but this rarelycauses significant clinical toxicity. Hence, extensive evaluation or observation is not required a�er minor skinor inhalational exposures.
Ethylene Glycol

8/7/2018
11/33
Ethylene glycol [CH2CH2(OH)2, molecular weight 62.07] is a colorless, odorless, sweet-tasting liquid. It was
considered nontoxic in the early 1900s until the first case of toxicity was reported in 1930.39 Ethylene glycolhas many contemporary uses as a glycerin substitute, preservative, component of hydraulic brake fluid, foamstabilizer, component for chemical synthesis, and most commonly an automotive coolant (antifreeze).
Virtually all ethylene glycol toxicity results from ingestion, because the chemical has a low vapor pressure
and does not penetrate skin well.40 Its sweet taste renders ethylene glycol an attractive ingestant for childrenand pets. Other common exposure scenarios include ingestion as an ethanol substitute when ethanol is
unavailable, and intentional suicidal ingestions.36
PATHOPHYSIOLOGY
Methanol
A�er ingestion, methanol is rapidly absorbed, with peak blood levels achieved within 30 to 60 minutes,
although there has been a case report of delayed peak at 8 hours a�er a large ingestion.41 Methanol is rapidlydistributed among body water with a volume of distribution of 0.6 to 0.77 L/kg. Without treatment, theminimum lethal dose in humans is thought to be approximately 1 gram/kg or 1.25 mL/kg. With treatment,survival has been reported a�er much larger ingestions. The dose required to cause permanent visualimpairment in an adult is estimated to be about a mouthful (24 grams or 30 mL).
Methanol is metabolized in the liver by alcohol dehydrogenase to formaldehyde, and then by aldehydedehydrogenase to formic acid (Figure 185–4). First-order kinetics is present at very low methanol
concentrations, with an elimination half-life of 1.8 to 3.0 hours.42 At higher methanol concentrations,metabolism switches to zero-order kinetics, and blood methanol level decreases at a fixed rate, roughly 8.5
milligrams/dL per h (2.7 mmol/L per h).43 Very small amounts of the unchanged parent compound may alsobe exhaled in vapor form.
FIGURE 185–4.
Metabolism of methanol. NAD+ = oxidized form of nicotinamide adenine dinucleotide; NADH = reduced formof nicotinamide adenine dinucleotide.

8/7/2018
12/33
Formic acid is the metabolite responsible for the toxicity and metabolic acidosis that occurs with methanolpoisoning. Acidosis correlates well with formic acid levels both in its magnitude and in the timing of itsdevelopment. Formic acid's main mechanism of toxicity is its binding to cytochrome oxidase and blockade of
oxidative phosphorylation. This leads to anaerobic metabolism and development of lactic acidosis.20 In
addition, metabolism of methanol increases the NADH/NAD+ ratio, which favors the conversion of pyruvateto lactate and thereby worsens lactic acidosis. Early in the course of methanol poisoning, more of theacidosis is due to formic acid itself, whereas later on, as cellular aerobic respiration is blocked and more
lactate builds up, the contribution of lactate becomes more significant.44
Formic acid's inhibition of cytochrome oxidase increases with decreasing pH, so acidemia worsens theblockade of aerobic metabolism. Falling pH also favors the undissociated form of formic acid (as opposed toformate ion), which moves more readily across tissue barriers. Therefore, at lower pH, more formic acid canenter the brain and ocular tissues, worsening CNS depression as well as retinal and optic nerve injury. Lower
pH may also prolong formic acid elimination by increasing tubular reabsorption.45
Ethylene Glycol
Ethylene glycol is rapidly absorbed from the GI tract, and blood levels generally peak 1 to 4 hours a�eringestion. Ethylene glycol distributes rapidly with a volume of distribution of 0.5 to 0.8 L/kg. Based on animalstudies and a limited number of case reports, the minimum lethal dose in humans is estimated to be 1.0 to
1.5 mL/kg or 1.1 to 1.7 grams/kg (approximately 100 mL in an adult).39
Like methanol, ethylene glycol itself has minor toxicity (it is a stronger inebriant than both methanol andethanol and causes gastric irritation), and it is the hepatic oxidation of ethylene glycol that creates the toxicmetabolites responsible for metabolic acidosis and end-organ damage. The liver metabolizes about 80% ofan ingested dose, whereas the other 20% is excreted unchanged in the urine. When metabolism is unblocked,ethylene glycol has first-order metabolic kinetics with an elimination half-life of roughly 3 to 8 hours.
8/7/2018
13/33
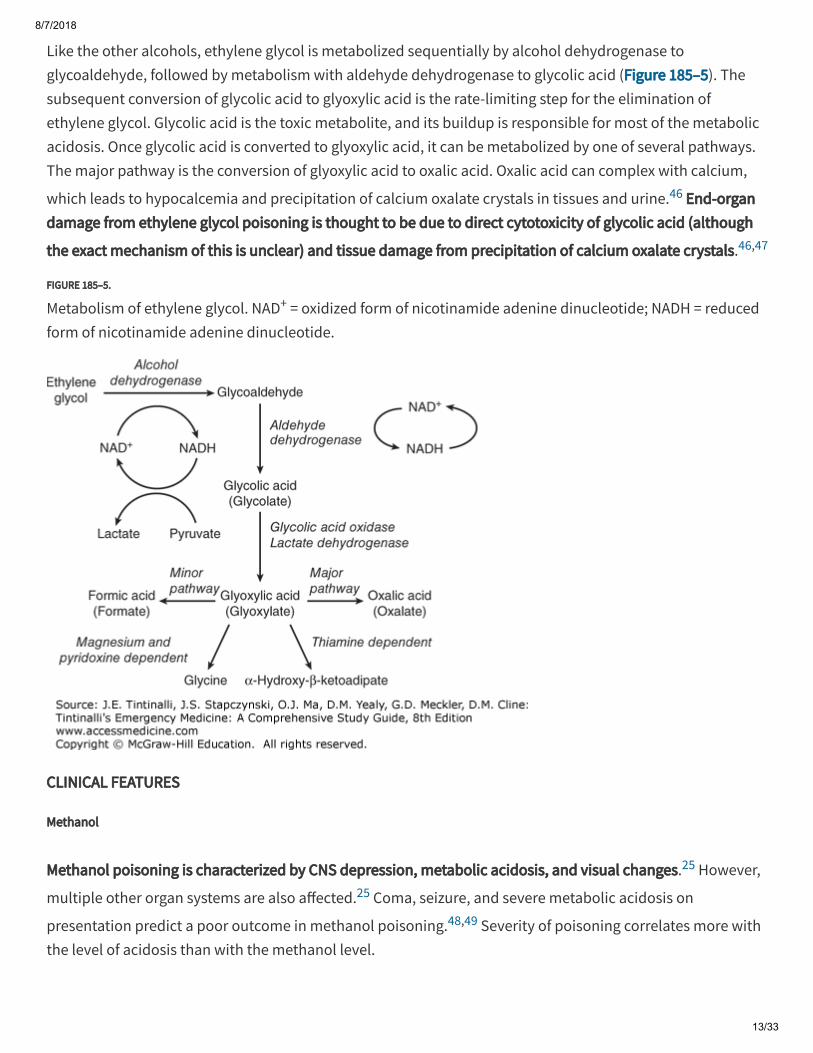
Like the other alcohols, ethylene glycol is metabolized sequentially by alcohol dehydrogenase toglycoaldehyde, followed by metabolism with aldehyde dehydrogenase to glycolic acid (Figure 185–5). Thesubsequent conversion of glycolic acid to glyoxylic acid is the rate-limiting step for the elimination ofethylene glycol. Glycolic acid is the toxic metabolite, and its buildup is responsible for most of the metabolicacidosis. Once glycolic acid is converted to glyoxylic acid, it can be metabolized by one of several pathways.The major pathway is the conversion of glyoxylic acid to oxalic acid. Oxalic acid can complex with calcium,
which leads to hypocalcemia and precipitation of calcium oxalate crystals in tissues and urine.46 End-organdamage from ethylene glycol poisoning is thought to be due to direct cytotoxicity of glycolic acid (although
the exact mechanism of this is unclear) and tissue damage from precipitation of calcium oxalate crystals.46,47
FIGURE 185–5.
Metabolism of ethylene glycol. NAD+ = oxidized form of nicotinamide adenine dinucleotide; NADH = reducedform of nicotinamide adenine dinucleotide.
CLINICAL FEATURES
Methanol
Methanol poisoning is characterized by CNS depression, metabolic acidosis, and visual changes.25 However,
multiple other organ systems are also a�ected.25 Coma, seizure, and severe metabolic acidosis on
presentation predict a poor outcome in methanol poisoning.48,49 Severity of poisoning correlates more withthe level of acidosis than with the methanol level.

8/7/2018
14/33
Because methanol itself is not toxic, but requires metabolism to formic acid before tissue damage occurs,clinical signs and symptoms may be significantly delayed a�er exposure, o�en by 12 to 24 hours. Becauseethanol competes for alcohol dehydrogenase, formation of the toxic metabolites from methanol will bedelayed if ethanol has also been ingested.
Methanol is only a mild inebriant, and patients with tolerance to ethanol also demonstrate tolerance tomethanol's intoxicating e�ects. Neurologic symptoms seen with methanol toxicity include headache, vertigo,dizziness, and seizures. Retinal and optic nerve tissue seem to be especially sensitive to the toxic e�ects offormic acid. Ocular toxicity may present as photophobia or blurred or "snow field" vision, with clinicalfindings including papilledema, nystagmus (rare), and nonreactive mydriasis once permanent damage has
occurred.50
Head CT may demonstrate bilateral putamen necrosis, subcortical white matter damage, and other patterns
of brain injury from methanol poisoning.51,52 Intracranial hemorrhages may occur in rare cases, so obtain a
noncontrast head CT first when considering heparin for hemodialysis or for other reasons.53 Delayed
parkinsonism and polyneuropathies can occur.54
Cardiovascular toxicity includes tachycardia and hypotension, which may progress to shock. Initially,patients o�en demonstrate tachypnea and shortness of breath while attempting to compensate for themetabolic acidosis, but over time, this may progress to respiratory failure.
Methanol is irritating to the GI tract and may cause abdominal pain, anorexia, nausea, vomiting, pancreatitis
or gastritis. Transaminitis is usually mild and transient.44 Rhabdomyolysis, renal failure, coma, and shock can
occur in severe cases.55
Ethylene Glycol
Ethylene glycol poisoning is characterized by CNS depression, metabolic acidosis, and renal failure.25,56
However, multiple other organ systems may be a�ected.25,56 Clinical poisoning has historically been dividedinto three stages, although timing may vary and stages may overlap.
The first or "neurologic" stage typically begins 30 minutes to 12 hours a�er ingestion due to the intoxicatinge�ects of the ethylene glycol parent compound, and may range from mild depression to seizure and coma.Patients with tolerance to the depressant e�ects of ethanol may also exhibit relative tolerance to theinebriating e�ects of ethylene glycol. Patients are o�en described as appearing intoxicated (with ataxia,confusion, and slurred speech) but without an ethanol odor on the breath. Ethylene glycol is directlyirritating to the GI tract, so abdominal pain, nausea, and vomiting may be present.
The generation of toxic metabolites generally takes 4 to 12 hours, or more if ethanol was coingested. CNStissue e�ects of glycolic acid and calcium oxalate crystals include cerebral edema, basal ganglia hemorrhagic

8/7/2018
15/33
infarction, and meningoencephalitis.57 Hypocalcemia, which occurs when calcium combines with oxalate,may contribute to seizures. Metabolic acidosis appears as toxic metabolites are generated.
The second or "cardiopulmonary" stage begins 12 to 24 hours a�er ingestion and is characterized bytachycardia and possibly hypertension. Tachypnea compensates for metabolic acidosis. Glycolate andoxalate crystal deposition in tissues leads to multiorgan system failure, including heart failure, acute lunginjury, and myositis. Hypocalcemia, if present during any stage, may cause prolongation of the QT interval,myocardial depression, and arrhythmias. Most deaths occur during this stage.
The third or "renal" stage is o�en delayed 24 to 72 hours a�er ingestion and is characterized by renal failuredue to calcium oxalate crystal deposition in the proximal tubules, the most common major complication ofserious ethylene glycol poisoning. Short-term hemodialysis is o�en required, and it may take weeks tomonths for the kidneys to recover. Delayed neuropathies may occur 5 to 20 days a�er ethylene glycol
poisoning.54,58,59
DIAGNOSIS OF METHANOL OR ETHYLENE GLYCOL POISONING
Laboratory tests for a patient with suspected methanol or ethylene glycol poisoning should include bloodethanol levels, arterial blood gas analysis, chemistry panel, calculation of anion and osmolar gaps, serumosmolarity, and creatine kinase level. Serum ketone, β-hydroxybutyrate (if available), and lactate levels arehelpful if a metabolic acidosis or an osmolar gap is present. Falsely elevated lactate results have been seen
with some point-of-care analyzers in patients with severe ethylene glycol poisoning.60,61 Check point-of-careglucose level. Measure serum acetaminophen and salicylate levels in patients with an intentional overdose.Consider methanol or ethylene glycol poisoning in a patient with an unexplained acidosis (see chapter 15,Acid-Base Disorders).
Acidosis will not be present immediately a�er exposure. The parent compounds must be converted to toxicmetabolites before the acidosis develops; this may be delayed by hours to over a day, especially if ethanol iscoingested.
Methanol and Ethylene Glycol Levels
The best laboratory test for diagnosing methanol or ethylene glycol poisoning is measurement of the specific
serum level of the alcohol.34
Asymptomatic individuals following methanol ingestion usually have levels of <20 milligrams/dL (<6mmol/L), and CNS symptoms may appear as levels rise above that. Ocular problems are associated withmethanol levels of >50 milligrams/dL (>16 mmol/L), and the risk of fatality rises with levels >150 to 200milligrams/dL (>47 to 62 mmol/L). However, toxicity associated with a given level depends greatly on howlong a�er ingestion the level was measured. A level of 50 milligrams/dL (16 mmol/L) obtained 3 hours a�eringestion implies a much smaller ingestion and less toxicity than if the same value was obtained 12 hours
a�er ingestion.62

8/7/2018
16/33
Notes: Calculated serum osmolarity = 2 × sodium + (blood urea nitrogen/2.8) + (glucose/18) + (ethanol/4.6) +
(isopropanol/6.0) + (methanol/3.2) + (ethylene glycol/6.2)
Osmolar gap = measured serum osmolarity – calculated serum osmolarity
Asymptomatic individuals following ethylene glycol ingestion usually have peak levels <20 milligrams/dL(<3.2 mmol/L). As with methanol, toxicity associated with a given level depends greatly on how long a�eringestion the level was measured. More useful are factors indicating metabolic dysfunction such as acidosis.
Osmolar Gap
In many hospital and clinical laboratories, methanol and ethylene glycol levels are not available in a timelymanner to assist with initial medical decision making. In such circumstances, the osmolar gap may be used
as a surrogate marker for toxic alcohol levels (Table 185–2).63 This calculation determines the di�erencebetween the measured serum osmoles and the calculated osmoles. Methanol and ethylene glycol, but nottheir metabolites, are osmotically active and will contribute to the measured serum osmolarity.
Table 185–2
Substances That Contribute to the Osmolar Gap
SubstanceMolecular
Weight
mOsm/kg H2O with a Serum Concentration of 100
milligrams/dL
Conversion
Factor
Ethanol 46 22 4.6
Isopropanol 60 17 6.0
Methanol 32 31 3.2
Ethylene
glycol
62 16 6.2
For accurate calculation of the osmolar gap, obtain blood samples for a basic serum chemistry panel(including blood urea nitrogen, glucose, and sodium levels), measurement of ethanol level, andmeasurement of serum osmolarity simultaneously. Using a previously obtained specimen to measure serumosmolarity ("add-on" tests) is not acceptable, because any toxic alcohols present may have volatilized sincethe sample was obtained. In addition, the freezing point depression method must be used to measure serumosmolarity, rather than the vapor pressure method, which can miss volatile substances such as toxicalcohols. There is considerable variation in baseline osmolar gap in healthy subjects depending on the
formula used for calculation,64 so the range of "normal" values is –14 to +10 mOsm/kg H2O, and ranges may

8/7/2018
17/33
di�er among clinical laboratories. In general, an osmolar gap of more than 10 to 15 mOsm/kg H2O raises
concern for toxicity. An osmolar gap of >50 mOsm/kg H2O is highly suggestive of either methanol or ethylene
glycol poisoning and is associated with increased mortality.65
The osmolar gap is highest when the parent toxic alcohol level is at its peak (roughly 30 to 60 minutes a�eringestion), before significant metabolism has occurred (Figure 185–6). As the time since ingestion increasesand the parent compound is metabolized, the osmolar gap will decrease. Hence, later-presenting patientsmay not have significant osmolar gaps. As metabolism occurs, acid metabolites build up and an anion gapmetabolic acidosis develops as the osmolar gap narrows. There may be a time period in the middle range
when the patient has both an osmolar gap and an anion gap.66
FIGURE 185–6.
Relative changes in anion and osmolar gaps over time from ingestion of a toxic alcohol.
Although the osmolar gap may be helpful in conjunction with the rest of the clinical picture, it has many
shortcomings and cannot be relied on to definitively diagnose or exclude a toxic alcohol poisoning.63,67,68
Other conditions such as ketoacidosis, shock, and sepsis may cause an elevated osmolar gap.69 Also,forgetting to account for ethanol is a common error when calculating the osmolar gap.
As noted, the range of normal variation in osmolar gap is wide and dependent on the formula used forcalculation, so a toxic concentration of methanol or ethylene glycol may be present with an osmolar gap in
the normal range.67,68,69 For example, 1 milligram/dL (0.3 mmol/L) of methanol will raise serum osmolarity
by 0.34 mOsm/kg H2O.20 Therefore, a methanol concentration of 50 milligrams/dL (15 mmol/L)—generally
accepted to be toxic—will raise serum osmolarity 17 mOsm/kg H2O. If a given patient's baseline was low to
begin with, this methanol concentration would not create an abnormal osmolar gap.

8/7/2018
18/33
Anion Gap
The positively charged cations in the serum are electrically balanced by the negatively charged anions. In theclinical laboratory, not all cations and anions are routinely measured, and the level of measured cations isusually greater than that of measured anions; the di�erence is termed unmeasured anions. The predominantserum cation measured is sodium, which is almost completely balanced by the measured charged chlorideand bicarbonate anions; the di�erence is termed the anion gap, consisting mostly of serum proteins,phosphate, sulfate, organic acids, and conjugate bases of ketoacids (see chapter 15, Acid-Base Disorders).
The normal anion gap varies according to the methodology used, and the physician should use the valuesestablished by the clinical laboratory. In most clinical settings, an anion gap >15 mEq/L should be consideredabnormal. As noted, it takes time for the acidotic metabolites to become present, as much as 12 to 16 hoursfollowing methanol ingestion, so a normal anion gap does not exclude the diagnosis.
Urinary Fluorescence
Urinary fluorescence under an ultraviolet or Wood's lamp has been anecdotally taught to be a helpful sign ofethylene glycol poisoning because most antifreeze products contain sodium fluorescein as an additive to aidin the detection of radiator leaks. Not all ethylene glycol products contain fluorescein; the fluorescence maybe short-lived (lasting about 4 hours a�er ingestion); and the ability of the physician to detect fluorescence is
a�ected by many technical factors.70 Thus, the absence of urinary fluorescence cannot exclude an ethyleneglycol ingestion. In addition, false-positive results occur, because many types of glass or plastic containersfluoresce on their own, and numerous foods, medications, toxins, and endogenous substances may cause
urinary fluorescence.71,72
Calcium Oxalate Crystals for Ethylene Glycol
Approximately half of patients poisoned with ethylene glycol demonstrate either monohydrate or dihydrate
calcium oxalate crystals on urinalysis.73 These are o�en misread as hippurate crystals. If present, they startto appear 4 to 6 hours a�er ingestion and may persist for days, especially in patients with renal failure. Themonohydrate form is more common, and the dihydrate form is more specific for ethylene glycol poisoning.
TREATMENT
Because toxic alcohols are absorbed so rapidly, gastric decontamination is unlikely to be of benefit, and
there is no evidence to support its routine use.39,44,74 Activated charcoal may be used if there is a coingestantknown to adsorb to charcoal.
The basic principles of treatment for both methanol and ethylene glycol poisoning are performing initialresuscitation, providing cardiopulmonary support, correcting acidosis, preventing formation of toxic

8/7/2018
19/33
metabolites, and enhancing the clearance of the parent compound and toxic metabolites.
Correct Acidosis
Correcting acidosis may improve the outcome in patients poisoned with methanol because acidosis worsensthe toxicity of formate; rapid improvement in visual and other systemic symptoms has been reported withcorrection of acidosis. In addition, alkalinization may help increase formic acid clearance by decreasing
reabsorption in the proximal renal tubules.45 However, the benefits of alkalinization may be equivocal if thepatient is treated with metabolic blockade and hemodialysis. When used in methanol poisoning, give IV
sodium bicarbonate infusions to maintain a serum pH of >7.30.44 There is no evidence that alkalinization isspecifically beneficial in ethylene glycol poisoning, but it seems reasonable to use sodium bicarbonate IV ifthere is a severe metabolic acidosis with pH <7.20.
Metabolic Blockade
Because laboratory confirmation may take time and because prompt treatment is important to prevent theformation of toxic metabolites, the decision to block metabolism o�en must be made before the diagnosis is
secure (Table 185–3).75 Start treatment while sorting out the clinical picture to protect the patient fromserious toxicity, such as blindness or renal failure. Treatment with either ethanol or fomepizole greatly slowsthe elimination of methanol and ethylene glycol. Because hepatic oxidation is inhibited, elimination isdetermined by first-order renal excretion, and the elimination half-life averages 52 hours (range 22 to 87hours) for methanol (compared to an elimination half-life without metabolic blockade of 1.8 to 3 hours) and13 to 20 hours for ethylene glycol (compared to an elimination half-life without metabolic blockade of 3 to 8
hours).39,45,76,77

8/7/2018
20/33
*If serum ethanol level is >100 milligrams/dL (>22 mmol/L), patient will be protected from the formation of toxic
metabolites by coingestion of ethanol, and specific metabolic blockade treatment can be delayed until toxic alcohol
level is available. If the ethanol level is likely to fall to <100 milligrams/dL before the toxic alcohol results are back, then
initiate metabolic blockade.
Table 185–3
Indications for Metabolic Blockade with Fomepizole or Ethanol
1. Elevated plasma levels: methanol >20 milligrams/dL (>6 mmol/L) or ethylene glycol >20 milligrams/dL (>3
mmol/L)
2. If methanol or ethylene glycol level not available:
A. Documented or suspected significant methanol or ethylene glycol ingestion with ethanol level lower
than approximately 100 milligrams/dL (22 mmol/L)*
B. Coma or altered mental status in patient with unclear history and:
(1) Unexplained serum osmolar gap of >10 mOsm/L
or
(2) Unexplained metabolic acidosis and ethanol level of <100 milligrams/dL (<22 mmol/L)*
Metabolic Blockade with Fomepizole
The initial step in the metabolism of methanol (see Figure 185–4) or ethylene glycol (see Figure 185–5) isperformed by alcohol dehydrogenase. This enzyme is competitively inhibited by either ethanol or fomepizole
(4-methyl-1H-pyrazole).76 Both ethanol and fomepizole have a much higher a�inity for alcoholdehydrogenase than does methanol or ethylene glycol. Although ethanol was traditionally administered formetabolic blockade in methanol and ethylene glycol poisonings, fomepizole has supplanted ethanol for thispurpose in many institutions. The primary advantage of fomepizole is the lack of side e�ects such as CNS
depression, GI irritation, and hypoglycemia caused by ethanol therapy.78,79,80 Fomepizole is less susceptible
to dosing errors than ethanol.81 The primary limiting factor to fomepizole use is the increased cost of thedrug relative to ethanol, which may reduce availability in resource-poor locations.
Fomepizole is dosed with an initial loading dose of 15 milligrams/kg IV administered over 30 minutes,followed by additional doses of 10 milligrams/kg IV (also infused over 30 minutes) every 12 hours.Fomepizole is continued until the toxic alcohol level is <20 milligrams/dL (methanol <6 mmol/L or ethyleneglycol <3 mmol/L) and the metabolic acidosis has resolved. Fomepizole is believed to induce its ownmetabolism, so it is recommended that the dose be increased to 15 milligrams/kg every 12 hours if treatment
lasts >48 hours.44,82 More frequent dosing (every 4 hours) is required during hemodialysis because

8/7/2018
21/33
fomepizole is removed during this procedure. Fomepizole does not require frequent monitoring of serumlevels or dosage adjustments necessary with ethanol treatment.
Adverse e�ects from fomepizole are rare; mild and transient nausea, headache, dizziness, and injection site
irritation are most commonly reported.76 The safety of fomepizole in pregnancy is unknown, so the risks andbenefits to fetus and mother of fomepizole therapy should be weighed against those of the alternative
treatments. Reports show good e�icacy of fomepizole therapy in children.83
Metabolic Blockade with Ethanol
If fomepizole is not available or its use is contraindicated (i.e., the patient has a known allergy), ethanol may
be used to inhibit toxic alcohol metabolism. Ethanol may be administered PO or IV.84 Although ethanol mayprevent toxic alcohol metabolism at blood levels as low as 30 milligrams/dL (7 mmol/L), the general
recommendation is to maintain a target ethanol level of 100 to 150 milligrams/dL (22 to 33 mmol/L).44
Extremely elevated toxic alcohol levels may reduce the e�ectiveness of alcohol dehydrogenase inhibition byethanol, and ethanol levels of >150 milligrams/dL (>33 mmol/L) may be required to e�ectively blockproduction of the toxic metabolites. Achieving the desired ethanol level may be di�icult because individualresponse to ethanol administration varies considerably depending on baseline ethanol consumption.
The loading dose of IV ethanol is 800 milligrams/kg (10 mL/kg of 10% IV solution). Maintenance dosing variesdepending on the patient's baseline ethanol use but generally averages 100 milligrams/kg per h (1.2 mL/kgper h of 10% IV solution) with ranges between 70 and 150 milligrams/kg per h (0.8 to 2 mL/kg per h of 10% IVsolution). The oral loading dose (PO or via nasogastric tube) using 80-proof liquor is 1.5 to 2 mL/kg followedby maintenance dosing of 0.2 to 0.5 mL/kg per h. Do not use oral ethanol preparations IV. Serum ethanolconcentrations should be monitored every 1 to 2 hours. All maintenance doses need to be doubled forpatients undergoing hemodialysis.
With severe adult poisoning and when fomepizole therapy may be delayed or transport time to the hospitalmay be long, administration of three or four 1-oz (30-mL) "shots" of 80-proof liquor should raise blood
ethanol concentrations su�iciently to block toxic alcohol metabolism in a 70-kg adult.20 Maintenancedosages are approximately one to two shots per hour.
Ethanol treatment is continued until the toxic alcohol level is <20 milligrams/dL (methanol <6 mmol/L orethylene glycol <3 mmol/L) and the metabolic acidosis has resolved. The disadvantage of using ethanol is theinduction of a state of inebriation, so patients require close monitoring for neurologic and respiratorydepression. Individual metabolic variations make dosing complicated, and frequent serum level monitoringand dosage adjustments are required. Children and malnourished individuals are particularly at risk for the
development of hypoglycemia, although with careful monitoring, this complication is rare.79 Administrationof the 10% IV ethanol solution requires central venous access, because it is hyperosmolar and irritating toperipheral veins. Use of less concentrated solutions, such as 5% IV ethanol solutions, may requireadministration of large fluid volumes.

8/7/2018
22/33
*Applies only to methanol; visual abnormalities may not resolve immediately, so their persistence in the absence of
other indications once hemodialysis is started is not an indication for continued hemodialysis.
†Although previously considered an indication for hemodialysis, there are reports of patients with levels of ≥50
milligrams/dL (methanol ≥15 mmol/L or ethylene glycol ≥7.5 mmol/L) being successfully treated with fomepizole with
or without bicarbonate and no hemodialysis.
Hemodialysis
Hemodialysis can rapidly clear the toxic alcohols and metabolites, as well as correct acid-base disorders,
thereby shortening the duration of metabolic blockade treatment.39,44,85,86,87 Conversely, with fomepizole,patients can receive prolonged treatment with few side e�ects and without the need for hemodialysis and
attendant risks.88
Hemodialysis may be required emergently for patients with severe acidosis, visual changes, hemodynamic
instability, or renal failure (Table 185–4).39,44,89,90 A serum level of ≥50 milligrams/dL (methanol ≥15 mmol/Lor ethylene glycol ≥7.5 mmol/L) is considered an indication for hemodialysis, but this criterion has beenquestioned because many patients with high methanol or ethylene glycol levels have been e�ectively treated
without hemodialysis.56,88,91,92 Consider the entire clinical picture, rather than making a decision based onlyon a serum level. Some rebound in toxic alcohol levels may occur a�er hemodialysis is stopped, so it isrecommended that metabolic blockade therapy be continued for several hours a�er cessation of dialysis,
with blood level rechecked to ensure that the toxic alcohol level remains low.39,44
Table 185–4
Indications for Hemodialysis a�er Methanol or Ethylene Glycol Ingestion
Refractory metabolic acidosis: pH <7.25 with anion gap >30 mEq/L and/or base deficit less than –15
Visual abnormalities*
Renal insu�iciency
Deteriorating vital signs despite aggressive supportive care
Electrolyte abnormalities refractory to conventional therapy
Serum methanol or ethylene glycol level of >50 milligrams/dL†
Vitamin Therapy
Adjunctive treatment with B vitamins (including folate) is recommended to help clear the toxic metabolites ofmethanol and ethylene glycol more quickly, although no solid evidence exists to indicate that this treatment
is necessary or even helpful.93
8/7/2018
23/33
1.
2.
In methanol poisoning, high doses of folate or folinic acid may facilitate breakdown of formic acid intocarbon dioxide and water (see Figure 185–4). Experimental animals with very large folate stores do notdevelop acidosis and toxicity from methanol poisoning unless they are artificially depleted of folate.Theoretically, increasing folate stores should hasten the detoxification of formate and prevent it fromaccumulating and causing end-organ damage. Folinic acid, the activated form of folic acid, is preferred, butfolic acid may be used if the former is not available. Recommended dosing is 1 milligram/kg (up to 50
milligrams) IV every 4 to 6 hours.44
In ethylene glycol poisoning, adjunctive therapy with pyridoxine, thiamine, and magnesium may be used tofacilitate metabolism of glyoxylate to nontoxic glycine and α-hydroxy-β-ketoadipoic acid (see Figure 185–5).Magnesium can be given as a one-time dose of magnesium sulfate 2 grams IV. The two B vitamins are given inlarge doses: thiamine, 100 milligrams IV, and pyridoxine, 50 to 100 milligrams IV, both every 6 hours for 2
days.94
Visual impairment can be a permanent complication of methanol poisoning.95,96 Although treatment withfomepizole or ethanol and bicarbonate can prevent ocular toxicity, there is no other proven therapy to
prevent or restore established visual damage.95
DISPOSITION AND FOLLOW-UP
Because of the complex management decisions required with methanol or ethylene glycol poisoning,consultation with a medical toxicologist or a regional poison control center is strongly recommended.Symptoms of methanol or ethylene glycol intoxication may be delayed, particularly if ethanol has beencoingested. A patient with suspected ethylene glycol ingestion should be observed and monitored for 6hours. If no ethanol is present, the patient remains completely asymptomatic, there is no osmolar gap, andno metabolic acidosis develops, the patient can be discharged. Methanol toxicity may be delayed longer, so apatient with suspected methanol ingestion should be observed for 12 hours using the same criteria. A patientwith significant signs and symptoms should be admitted to an intensive care setting. Patients seen atfacilities unable to provide hemodialysis or intensive care should be transferred as soon as possible, if insu�iciently stable condition, to institutions capable of providing such care. Suicidal patients should receive apsychiatric evaluation when their condition improves and prior to discharge.
REFERENCES
Goforth HW, Fernandez F: Acute neurologic e�ects of alcohol and drugs. Neurol Clin . 2012; 30: 277. [PubMed: 22284063]
Sullivan JB, Hauptman M, Bronstein AC: Lack of observable intoxication in humans with high bloodalcohol concentrations. J Forensic Sci . 1987; 32: 1660.
[PubMed: 3430134]
8/7/2018
24/33
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Fell JC, Voas RB: The e�ectiveness of reducing illegal blood alcohol concentration (BAC) limits for driving:evidence for lowering the limit to .05 BAC. J Safety Res . 2006; 37: 233.
[PubMed: 16824545]
Lamminpää A, Hoppu K: First-order alcohol elimination in severe alcohol intoxication in an adolescent: acase report. Am J Emerg Med . 2009; 27: 128.
[PubMed: 19041554]
Gershman H, Steeper J: Rate of clearance of ethanol from the blood of intoxicated patients in theemergency department. J Emerg Med . 1991; 9: 307.
[PubMed: 1940231]
Vonghia L, Leggio L, Ferrulli A, et al. : Alcoholism Treatment Study Group: acute alcohol intoxication. Eur JIntern Med . 2008; 19: 561.
[PubMed: 19046719]
Hall D, Riley J, Swann I: Can alcohol intoxication be excluded as the cause of confusion following headinjury? Scott Med J . 2005; 50: 24.
[PubMed: 15792385]
Sperry JL, Gentilello LM, Minei JP, Diaz-Arrastia RR, Friese RS, Shafi S: Waiting for the patient to “soberup”: e�ect of alcohol intoxication on Glasgow coma scale score of brain injured patients. J Trauma . 2006; 61:1305.
[PubMed: 17159670]
Rubenzer S: Judging intoxication. Behav Sci Law . 2011; 29: 116. [PubMed: 20623796]
Bond J, Ye Y, Cherpitel CJ, et al. : The relationship between self-reported drinking and BAC level inemergency room injury cases: is it a straight line? Alcohol Clin Exp Res . 2010; 34: 1118.
[PubMed: 20374201]
Roberts JR, Dollard D: Alcohol levels do not accurately predict physical or mental impairment in ethanol-tolerant subjects: relevance to emergency medicine and dram shop laws. J Med Toxicol . 2010; 6: 438.
[PubMed: 20358415]
Goding GS, Dobie RA: Gaze nystagmus and blood alcohol. Laryngoscope . 1986; 96: 713. [PubMed: 3724319]
Citek K, Ball B, Rutledge DA: Nystagmus testing in intoxicated individuals. Optometry . 2003; 74: 695. [PubMed: 14653658]

8/7/2018
25/33
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Karlovsek MZ, Balazic J: Evaluation of the post-rotational nystagmus test (PRN) in determining alcoholintoxication. J Anal Toxicol . 2005; 29: 390.
[PubMed: 16105267]
Jang GR, Harris RZ: Drug interactions involving ethanol and alcoholic beverages. Expert Opin Drug MetabToxicol . 2007; 3: 719.
[PubMed: 17916057]
Zehtabchi S, Sinert R, Baron BJ, Paladino L, Yadav K: Does ethanol explain the acidosis commonly seenin ethanol-intoxicated patients? Clin Toxicol (Phila) . 2005; 43: 161.
[PubMed: 15902789]
Donnino MW, Vega J, Miller J, Walsh M: Myths and misconceptions of Wernicke’s encephalopathy: whatevery emergency physician should know. Ann Emerg Med . 2007; 50: 715.
[PubMed: 17681641]
Schabelman E, Kuo D: Glucose before thiamine for Wernicke encephalopathy: a literature review. JEmerg Med . 2012; 42: 488.
[PubMed: 22104258]
Li SF, Jacob J, Feng J, Kulkarni M: Vitamin deficiencies in acutely intoxicated patients in the ED. Am JEmerg Med . 2008; 26: 792.
[PubMed: 18774045]
Li J, Mills T, Erato R: Intravenous saline has no e�ect on blood ethanol clearance. J Emerg Med . 1999; 17:1.
[PubMed: 9950378]
Hindmarch PN, Land S, Wright J: Emergency physicians’ opinions on the use of intravenous fluids totreat patients intoxicated with ethanol (alcohol): attitudes of emergency medicine physicians in the NorthEast of England toward the use of intravenous fluids to treat individuals intoxicated with ethanol (alcohol)attending the emergency department compared with the scientific evidence. Eur J Emerg Med . 2012; 19:379.
[PubMed: 22134421]
Addolorato G, Ancona C, Capristo E, Gasbarrini G: Metadoxine in the treatment of acute and chronicalcoholism: a review. Int J Immunopathol Pharmacol . 2003; 16: 207.
[PubMed: 14611722]
Díaz Martínez MC, Díaz Martínez A, Villamil Salcedo V, Cruz Fuentes C: E�icacy of metadoxine in themanagement of acute alcohol intoxication. J Int Med Res . 2002; 30: 44.

8/7/2018
26/33
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
[PubMed: 11921498]
Shpilenya LS, Muzychenko AP, Gasbarrini G, Addolorato G: Metadoxine in acute alcohol intoxication: adouble-blind, randomized, placebo-controlled study. Alcohol Clin Exp Res . 2002; 26: 340.
[PubMed: 11923586]
Jammalamadaka D, Raissi S: Ethylene glycol, methanol and isopropyl alcohol intoxication. Am J MedSci . 2010; 339: 276.
[PubMed: 20090509]
Zaman F, Pervez A, Abreo K: Isopropyl alcohol intoxication: a diagnostic challenge. Am J Kidney Dis .2002; 40: E12.
[PubMed: 12200829]
Lacouture PG, Heldreth DD, Shannon M, Lovejoy FH Jr: The generation of acetonemia/acetonuriafollowing ingestion of a subtoxic dose of isopropyl alcohol. Am J Emerg Med . 1989; 7: 38.
[PubMed: 2914047]
Jones AW: Elimination half-life of acetone in humans: case reports and review of the literature. J AnalToxicol . 2000; 24: 8.
[PubMed: 10654562]
Stremski E, Hennes H: Accidental isopropanol ingestion in children. Pediatr Emerg Care . 2000; 16: 238. [PubMed: 10966340]
Adla MR, Gonzalez-Paoli JA, Rifkin SI: Isopropyl alcohol ingestion presenting as pseudorenal failure dueto acetone interference. South Med J . 2009; 102: 867.
[PubMed: 19593296]
Trullas JC, Aguilo S, Castro P, Nogue S: Life-threatening isopropyl alcohol intoxication: is hemodialysisreally necessary? Vet Hum Toxicol . 2004; 46: 282.
[PubMed: 15487656]
Kraut JA, Kurtz I: Toxic alcohol ingestions: clinical features, diagnosis, and management. Clin J Am SocNephrol . 2008; 3: 208.
[PubMed: 18045860]
Kruse JA: Methanol and ethylene glycol intoxication. Crit Care Clin . 2012; 28: 661. [PubMed: 22998995]
Porter WH: Ethylene glycol poisoning: quintessential clinical toxicology; analytical conundrum. Clin ChimActa . 2012; 413: 365.

8/7/2018
27/33
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
[PubMed: 22085425]
Davis LE, Hudson D, Benson BE, et al. : Methanol poisoning exposures in the United States: 1993–1998. JToxicol Clin Toxicol . 2002; 40: 499.
[PubMed: 12217003]
Montjoy CA, Rahman A, Teba L: Ethylene glycol and methanol poisonings: case series and review. W VMed J . 2010; 106: 17.
[PubMed: 21928557]
Shah S, Pandey V, Thakore N, Mehta I: Study of 63 cases of methyl alcohol poisoning (hooch tragedy inAhmedabad). J Assoc Physicians India . 2012; 60: 34.
[PubMed: 23029719]
Giovanetti F: Methanol poisoning among travellers to Indonesia. Travel Med Infect Dis . 2013; 11: 190. [PubMed: 23566856]
Barceloux DG, Krenzelok EP, Olson K, Watson W: American Academy of Clinical Toxicology practiceguidelines on the treatment of ethylene glycol poisoning. Ad Hoc Committee. J Toxicol Clin Toxicol . 1999; 37:537.
[PubMed: 10497633]
Patocka J, Hon Z: Ethylene glycol, hazardous substance in the household. Acta Medica (Hradec Kralove) .2010; 53: 19.
[PubMed: 20608228]
Elwell RJ, Darouian P, Bailie GR, et al. : Delayed absorption and postdialysis rebound in a case of acutemethanol poisoning. Am J Emerg Med . 2004; 22: 126.
[PubMed: 15011234]
Ha�ner HT, Wehner HD, Scheytt KD, Besserer K: The elimination kinetics of methanol and the influenceof ethanol. Int J Legal Med . 1992; 105: 111.
[PubMed: 1520634]
Jacobsen D, Webb R, Collins TD, McMartin KE: Methanol and formate kinetics in late diagnosedmethanol intoxication. Med Toxicol . 1988; 3: 418.
[PubMed: 3193890]
Barceloux DG, Bond GR, Krenzelok EP, et al. : American Academy of Clinical Toxicology Ad HocCommittee on the Treatment Guidelines for Methanol Poisoning: American Academy of Clinical Toxicologypractice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol . 2002; 40: 415.
[PubMed: 12216995]
8/7/2018
28/33
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
Hovda KE, Andersson KS, Urdal P, Jacobsen D: Methanol and formate kinetics during treatment withfomepizole. J Toxicol Clin Toxicol . 2005; 43: 221.
[PubMed: 16035197]
McMartin K: Are calcium oxalate crystals involved in the mechanism of acute renal failure in ethyleneglycol poisoning? Clin Toxicol (Phila) . 2009; 47: 859.
[PubMed: 19852621]
Hovda KE, Guo C, Austin R, McMartin KE: Renal toxicity of ethylene glycol results from internalization ofcalcium oxalate crystals by proximal tubule cells. Toxicol Lett . 2010; 192: 365.
[PubMed: 19931368]
Hassanian-Moghaddam H, Pajoumand A, Dadgar SM, Shadnia SH: Prognostic factors in methanolpoisoning. Hum Exp Toxicol . 2007; 26: 583.
[PubMed: 17884962]
Coulter CV, Farquhar SE, McSherry CM, Isbister GK, Du�ull SB: Methanol and ethylene glycol acutepoisonings: predictors of mortality. Clin Toxicol (Phila) . 2011; 49: 900.
[PubMed: 22091788]
Sharma R, Marasini S, Sharma AK, Shrestha JK, Nepal BP: Methanol poisoning: ocular and neurologicalmanifestations. Optom Vis Sci . 2012; 89: 178.
[PubMed: 22127151]
Sefidbakht S, Rasekhi AR, Kamali K, et al. : Methanol poisoning: acute MR and CT findings in ninepatients. Neuroradiology . 2007; 49: 427.
[PubMed: 17294234]
Jain N, Himanshu D, Verma SP, Parihar A: Methanol poisoning: characteristic MRI findings. Ann SaudiMed . 2013; 33: 68.
[PubMed: 22634487]
Sebe A, Satar S, Uzun B, et al. : Intracranial hemorrhage associated with methanol intoxication. Mt SinaiJ Med . 2006; 73: 1120.
[PubMed: 17285208]
Reddy NJ, Sudini M, Lewis LD: Delayed neurological sequelae from ethylene glycol, diethylene glycoland methanol poisonings. Clin Toxicol (Phila) . 2010; 48: 967.
[PubMed: 21192754]
8/7/2018
29/33
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
Gru�erman S, Morris D, Alvarez J: Methanol poisoning complicated by myoglobinuric renal failure. Am JEmerg Med . 1985; 3: 24.
[PubMed: 3970748]
Hovda KE, Julsrud J, Øvreb⊘ S, Br⊘rs O, Jacobsen D: Studies on ethylene glycol poisoning: onepatient - 154 admissions. Clin Toxicol (Phila) . 2011; 49: 478.
[PubMed: 21824058]
Corr P, Szólics M: Neuroimaging findings in acute ethylene glycol poisoning. J Med Imaging RadiatOncol . 2012; 56: 442.
[PubMed: 22883652]
Baldwin F, Sran H: Delayed ethylene glycol poisoning presenting with abdominal pain and multiplecranial and peripheral neuropathies: a case report. J Med Case Rep . 2010; 4: 220.
[PubMed: 20663174]
Rahman SS, Kadakia S, Balsam L, Rubinstein S: Autonomic dysfunction as a delayed sequelae of acuteethylene glycol ingestion: a case report and review of the literature. J Med Toxicol . 2012; 8: 124.
[PubMed: 22090149]
Pernet P, Bénéteau-Burnat B, Vaubourdolle M, Maury E, O�enstadt G: False elevation of blood lactatereveals ethylene glycol poisoning. Am J Emerg Med . 2009; 27: 132.e1.
[PubMed: 19041561]
Sandberg Y, Rood PP, Russcher H, Zwaans JJ, Weige JD, van Daele PL: Falsely elevated lactate in severeethylene glycol intoxication. Neth J Med . 2010; 68: 320
[PubMed: 20739730]
Kostic MA, Dart RC: Rethinking the toxic methanol level. J Toxicol Clin Toxicol . 2003; 41: 793. [PubMed: 14677789]
Ku E, Cheung EL, Khan A, Yu AS: Anion and osmolal gaps a�er alcohol intoxication. Am J Kidney Dis .2009; 54: 385.
[PubMed: 19560850]
Edijanto SP: Serum osmolal gap in healthy persons. Comparison of eleven formulas for calculatingosmolality. Folina Medica Indonesia . 2005; 41: 53.[no PMID]
Coulter CV, Farquhar SE, McSherry CM, Isbister GK, Du�ull SB: Methanol and ethylene glycol acutepoisonings: predictors of mortality. Clin Toxicol (Phila) . 2011; 49: 900.
[PubMed: 22091788]
8/7/2018
30/33
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
Mycyk MB, Aks SE: A visual schematic for clarifying the temporal relationship between the anion andosmol gaps in toxic alcohol poisoning. Am J Emerg Med . 2003; 21: 333.
[PubMed: 12898493]
Lynd LD, Richardson KJ, Purssell RA, et al. : An evaluation of the osmole gap as a screening test for toxicalcohol poisoning. BMC Emerg Med . 2008; 8: 5.
[PubMed: 18442409]
Krahn J, Khajuria A: Is osmol gap an e�ective screen in accurate prediction of toxic volatiles? Clin Lab .2011; 57: 297.
[PubMed: 21755818]
Hovda KE, Hunderi OH, Rudberg N, et al. : Anion and osmolal gaps in the diagnosis of methanolpoisoning: clinical study in 28 patients. Intensive Care Med . 2004; 30: 1842.
[PubMed: 15241587]
Wallace KL, Suchard JR, Curry SC, Reagan C: Diagnostic use of physicians’ detection of urinefluorescence in a simulated ingestion of sodium fluorescein-containing antifreeze. Ann Emerg Med . 2001; 38:49.
[PubMed: 11423812]
Casavant MJ, Shah MN, Battels R: Does fluorescent urine indicate antifreeze ingestion by children.Pediatrics . 2001; 107: 113.
[PubMed: 11134443]
Parsa T, Cunningham SJ, Wall SP, et al. : The usefulness of urine fluorescence for suspected antifreezeingestion in children. Am J Emerg Med . 2005; 23: 787. Erratum in: Am J Emerg Med . 2006; 24: 396.
[PubMed: 16182989]
Luqman A, Stanifer J, Asif Siddiqui OM, Naseer A, Wall BM: Calcium oxalate monohydrate crystals: aclue to ethylene glycol poisoning. Am J Med Sci . 2011; 341: 338.
[PubMed: 20571351]
Caravati EM, Erdman AR, Christianson G, et al. : American Association of Poison Control Centers:ethylene glycol exposure: an evidence-based consensus guideline for out-of-hospital management. ClinToxicol (Phila) . 2005; 43: 327.
[PubMed: 16235508]
Mangera Z, Isse S, Winnett G, Lal A, Ca�erkey M: Successful outcome of accidental ethylene glycolpoisoning despite delayed presentation. BMJ Case Rep 2010: July 21 , 2010.
[PubMed: 22767560]
8/7/2018
31/33
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
Brent J: Fomepizole for ethylene glycol and methanol poisoning. N Engl J Med . 2009; 360: 2216. [PubMed: 19458366]
Levine M, Curry SC, Ruha AM, et al. : Ethylene glycol elimination kinetics and outcomes in patientsmanaged without hemodialysis. Ann Emerg Med . 2012; 59: 527.
[PubMed: 22226175]
Hantson P, Wittebole X, Haufroid V: Ethanol therapy for methanol poisoning: duration and problems. EurJ Emerg Med . 2002; 9: 278.
[PubMed: 12394629]
Roy M, Bailey B, Chalut D, et al. : What are the adverse e�ects of ethanol used as an antidote in thetreatment of suspected methanol poisoning in children? J Toxicol Clin Toxicol . 2003; 41: 155.
[PubMed: 12733853]
Lepik KJ, Levy AR, Sobolev BG, et al. : Adverse drug events associated with the antidotes for methanoland ethylene glycol poisoning: a comparison of ethanol and fomepizole. Ann Emerg Med . 2009; 53: 439.
[PubMed: 18639955]
Lepik KJ, Sobolev BG, Levy AR, et al. : Medication errors associated with the use of ethanol andfomepizole as antidotes for methanol and ethylene glycol poisoning. Clin Toxicol (Phila) . 2011; 49: 391.
[PubMed: 21740138]
Bestic M, Blackford M, Reed M: Fomepizole: a critical assessment of current dosing recommendations. JClin Pharmacol . 2009; 49: 130.
[PubMed: 19004845]
De Brabander N, Wojciechowski M, De Decker K, et al. : Fomepizole as a therapeutic strategy inpaediatric methanol poisoning: a case report and review of the literature. Eur J Pediatr . 2005; 164: 158.
[PubMed: 15578220]
Holyoak AL, Fraser TA, Gelperowicz P: Cooling in the tropics: ethylene glycol overdose. Crit Care Resusc .2011; 13: 28.
[PubMed: 21355826]
Gilbert C, Baram M, Marik PE: Continuous venovenous hemodiafiltration in severe metabolic acidosissecondary to ethylene glycol ingestion. South Med J . 2010; 103: 846.
[PubMed: 20622722]
Minguela JI, Lanzagorta MJ, Hernando A, Audicana J: Methanol poisoning. Evolution of blood levelswith high-flux haemodialysis. Nefrologia . 2011; 31: 120.

8/7/2018
32/33
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
[PubMed: 21270930]
Kute VB, Godara SM, Shah PR, et al. : Hemodialysis for methyl alcohol poisoning: a single-centerexperience. Saudi J Kidney Dis Transpl . 2012; 23: 37.
[PubMed: 22237216]
Hovda KE, Jacobsen D: Expert opinion: fomepizole may ameliorate the need for hemodialysis inmethanol poisoning. Hum Exp Toxicol . 2008; 27: 539.
[PubMed: 18829729]
Mégarbane B, Borron SW, Baud FJ: Current recommendations for treatment of severe toxic alcoholpoisonings. Intensive Care Med . 2005; 31: 189.
[PubMed: 15627163]
Peces R, Fernández R, Peces C, et al. : [E�ectiveness of pre-emptive hemodialysis with high-fluxmembranes for the treatment of life-threatening alcohol poisoning.] Nefrologia . 2008; 28: 413.
[PubMed: 18662149]
Buchanan JA, Alhelail M, Cetaruk EW, et al. : Massive ethylene glycol ingestion treated with fomepizolealone-a viable therapeutic option. J Med Toxicol . 2010; 6: 131.
[PubMed: 20422336]
Buller GK, Moskowitz CB: When is it appropriate to treat ethylene glycol intoxication with fomepizolealone without hemodialysis? Semin Dial . 2011; 24: 441.
[PubMed: 21801226]
Ghosh A, Boyd R: Leucovorin (calcium folinate) in “antifreeze” poisoning. Emerg Med J . 2003; 20: 466. [PubMed: 12954693]
Davis DP, Bramwell KJ, Hamilton RS, Williams SR: Ethylene glycol poisoning: case report of record-highlevel and a review. Am J Emerg Med . 1997; 15: 653.
[PubMed: 9348055]
Paasma R, Hovda KE, Jacobsen D: Methanol poisoning and long term sequelae: a six years follow-upa�er a large methanol outbreak. BMC Clin Pharmacol . 2009; 9: 5.
[PubMed: 19327138]
Desai T, Sudhalkar A, Vyas U, Khamar B: Methanol poisoning: predictors of visual outcomes. JAMAOphthalmol . 2013; 131: 358.
[PubMed: 23303293]

8/7/2018
33/33
97.
98.
99.
100.
101.
USEFUL WEB RESOURCES
American Academy of Clinical Toxicology — http://www.clintox.org/index.cfm
Asia Pacific Association of Medical Toxicology — http://www.asiatox.org/
European Association of Poisons Centres and Clinical Toxicologists — http://www.eapcct.org/
South Asian Clinical Toxicology Research Collaboration — http://www.sactrc.org/
TOXBASE: The primary clinical toxicology database of the National Poisons Information Service (freeaccess for UK National Health Service hospital departments and general practices, and National HealthService departments of public health and health protection agency units; available to hospital EDs in Irelandby contract; available to European poison centers whose sta� are members of the European Association ofPoisons Centres and Clinical Toxicologists; overseas users may be allowed access on payment of a yearlysubscription, subject to the approval of the Health Protection Agency) — http://www.toxbase.org/
McGraw HillCopyright © McGraw-Hill Global Education Holdings, LLC.
All rights reserved. Your IP address is 50.26.48.115
Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair





























