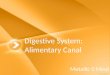
Chapter 14. Organs of the Alimentary canal Alimentary canal a.k.a. Gastrointestinal tract Mouth...
39
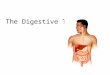
Digestive System Chapter 14
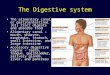
Chapter 14. Organs of the Alimentary canal Alimentary canal a.k.a. Gastrointestinal tract Mouth Pharynx Esophagus Stomach Small intestine Large intestine
Organs of the Alimentary canal Alimentary canal a.k.a.
Gastrointestinal tract Mouth Pharynx Esophagus Stomach Small
intestine Large intestine Rectum All food passing through the AI
canal is technically outside the body
Slide 3
Tunics of the AI Canal (Esophagus to Lg. Intestines) 1. Mucosa
innermost layer that lines the lumen. Mostly surface epithelium and
small amounts of CT (lamina propria) and a scanty smooth muscle
layer The esophagus epithelium is stratified squamous. The rest of
the AI canal is mostly simple columnar 2. Submucosa just below the
mucosa. Soft CT layer with blood vessels, nerve endings, GALT
(gut-associated lymphoid tissue), and lymphatic vessels 3.
Muscularis externa dual smooth muscle layers. The inner circular
layer and outer longitudinal layer 4. Serosa outermost layer of the
wall. Single layer of serous fluid-producing visceral peritoneum
which is continuous with the parietal peritoneum and mesentery
Slide 4
Innervation of the AI Canal The canal wall has two intrinsic
nerve plexuses Submucosal nerve plexus Myenteric (intestinal
muscle) nerve plexus These are part of the autonomic nervous system
Help regulate mobility and secretory activity of the AI canal
organs
Slide 5
Sphincters in the AI Canal Sphincters are circular arrangements
of muscle fascicles and are found in four places in the GI tract 1.
Cardioesophageal sphincter (aka: Cardiac sphincter or esophageal
sphincter) found at the entrance to the stomach 2. Pyloric
sphincter (aka: pyloric valve) found at the entrance to the small
intestines 3. Ileocecal valve found at the entrance to the large
intestines 4. Internal and External anal sphincters found in the
anus These are controlled by a variety of neural, chemical and
mechanical mechanisms to ensure that food is allowed proper time to
be digested and/or absorbed in different locations of the GI
tract
Slide 6
Sphincters of the AI Canal
Slide 7
Functions of the Digestive System 1. Ingestion active and
voluntary process of putting food into the mouth 2. Propulsion-
moving food from one digestive organ to the next Ex: Peristalsis in
the esophagus and segmentation in the small intestines (which is
used more for mixing food with digestive enzymes) 3. Food
breakdown: Mechanical digestion 4. Food breakdown: Chemical
digestion 5. Absorption 6. Defecation
Slide 8
Food breakdown: Chemical digestion The process of breaking
organic food molecules down into building blocks Carbs
monosaccharides Proteins amino acids Lipids glycerols and fatty
acids All hydrolysis reactions because water is added to each bond
to be broken Water is also necessary as a solvent and softening
agent for food Each food molecule is broken down by a different
enzyme There are many molecules in food that we do not have enzymes
for, thus these food pass out of the body either undigested or
partially digested by gut bacteria
Slide 9
The Mouth Mechanical digestion begins: mastication of food with
teeth. Chemical digestion follows: saliva produced by the salivary
glands secretes enzymes in an alkaline solution along with
antibodies (IgA) and lysozymes Main enzyme: amylase breaks starch
into disaccharides and oligosaccharides Saliva is produced in
copious amounts due to presence of food and stimulation of
mechanoreceptors Thoughts, smells and sight of food can also
stimulate production via cranial nerves VII and IX Sensory papillae
on taste buds send taste info to the brain
Slide 10
Food Propulsion Mouth to Stomach Deglutition (a.k.a.
swallowing) is a two phase event 1. Buccal phase (voluntary) food
is chewed, mixed with saliva, and forms a bolus (food mass). The
tongue forces the bolus into the pharynx 2. Pharyngeal-esophageal
phase (reflex) food moves down the esophagus. Mostly controlled by
vagus nerve activity. All exits are blocked off and food is
propelled down the esophagus via peristaltic contractions food
pressing on the cardioesophageal sphincter causes it to open and
allows food into the stomach The sphincter closes behind to
food
Slide 11
The Stomach Three parts: The fundus, body, and pyloric antrum
Has large folds called rugae that allow the stomach to stretch and
hold up to ~4L of food The muscularis externa has a third oblique
(inner) layer of muscle which helps mechanical digestion and mixing
Once food is thoroughly mixed with gastric juice, it is known as
chyme
Slide 12
The Stomach The lining has gastric glands that produce various
secretions (collectively: gastric juice) by different cells: Mucous
neck cells (top) make acidic mucous Parietal cells (middle) secrete
HCl Chief cells (base) produce pepsinogen (activated by HCl)
Enteroendocrine cells (scattered) produce local hormones, ex:
Gastrin Intrinsic factor also produced by gastric glands (needed
for B 12 absorption) Rennin, also a protease, works mostly on milk
proteins in infants, may not be produced in adults
Slide 13
More on the Stomach Before swallowing, cephalic input causes
the stomach to produce copious gastric juice Food in the stomach,
and a rising pH stimulates release of more gastrin Gastrin in turn
causes an increase in pepsinogen, mucus, and HCl production
Different nutrients in food can change the rate of gastric
emptying. A balanced meal takes 2-4 hrs to pass through, high fat
meal may take up to 6: Water, acidic and salty foods increase
gastric emptying Simple and some complex carbs increase the rate of
gastric emptying Proteins empty less quickly than carbs Fats slow
gastric emptying and take the longest to leave the stomach No food
is absorbed in the stomach Aspirin, caffeine and alcohol are*
Slide 14
Homeostatic Imbalance Heartburn typically occurs when the
cardioesophageal sphincter fails to close completely and
inflammation of the esophagus results Sometimes due to Hiatal
hernia. This occurs when the fundus protrudes above the diaphragm
The sphincter is typically weak and this condition prevents it from
working properly Ulcers often result from infection with H. pylori
bacteria Emesis vomiting. Occurs when the emetic center of the
brain in the medulla is stimulated. Retropulsion of food coupled
with a strong abdominal muscle and diaphragm contraction force food
back through the sphincter Triggered by many factors
Slide 15
From the stomach to the intestines Once chyme is mixed
thoroughly, the stomach begins peristalsis to push food towards the
pyloric antrum (pylorus) which holds ~30 mL chyme Each wave of
contraction pushes a small squirt of chyme into the intestines, ~3
mL The rest is pushed back into the body for more mixing
(retropulsion) As the duodenum of the small intestines is stretched
and the acidic food enters, the enterogastric reflex occurs,
putting the breaks on gastric emptying Inhibits vagus nerve
Slide 16
The Small Intestines 2-4 m longs, hangs in sausage-like coils,
suspended from the posterior abdominal wall by the fan-shaped
mesentary Three subdivision: Duodenum (literally twelve fingers
widths long) 5% of length Jejunum (empty) 40% of length Ileum
(twisted intestine) 55% of length Main site of chemical digestion
and absorption Can only handle a small amount of chyme at a time
Flow into the intestine is controlled by the pyloric sphincter Up
to this point, only carbs and some proteins have been partially
digestion. No fats have been digested yet.
Slide 17
Chemical Digestion in the Duodenum Intestine fluid is
relatively enzyme poor, though brush border enzymes in the
microvilli have important roles ie: break down disaccharides into
monosaccharides Intestinal juice itself is enzyme-poor but rich
with protective mucus Most digestive enzymes come from the pancreas
in enzyme-rich pancreatic juice Some enzymes are made by the
intestinal cells, others by the pancreas and liver The acidity of
chyme, molecules in the chyme (ie: fat), and stretch receptors
trigger the release of hormones from intestinal cells: Secretin
causes the pancreas to release pancreatic juice in conjunction with
the vagus nerve Cholecyctokinin (CCK) triggers release of bile from
gall bladder Gastric inhibitory peptide (GIP) inhibits gastric
juice secretion and stimulates insulin secretion
Slide 18
Duodenum The pancreas releases a mixture of enzymes in alkaline
solution (pancreatic juice) straight into the duodenum via the
pancreatic ducts Bile, formed by the liver and stored in the gall
bladder is released into the intestine in the same location. Both
accessory organs share the common bile duct, a.k.a.:
hepatopancreatic ampulla From there, both bile and pancreatic juice
enter the duodenum through the duodenal papilla
Slide 19
Pancreatic Juice Carb digestion enzymes: Pancreatic amylase:
Along with the brush border enzymes, this completes digestion of
starch Protein digestion enzymes: Trypsin, chymotrypsin,
carboxypeptidase and others Lipid digestion enzymes: Lipases
(different types) Nucleic acid digestion enzymes: Nucleases Lots
and lots of bicarbonate (alkaline buffer) which makes the juice
have a pH ~8 Used to neutralize stomach acid and prevent damage to
intestinal walls
Slide 20
Small Intestine propulsion and digestion continued Water and
nutrients are absorbed along the length of the intestine Most
nutrients are absorbed via active transport From the blood,
nutrients are shunted to the liver via hepatic portal vein Fats and
lipids diffuse into mucosa cells, then form micelles which are
taken up by lymph vessels that subsequently dump the lipids into
the blood in the jugular vein Peristalsis propels chyme forward,
segmentation mixes the chyme further with digestive secretions
Slide 21
Small Intestine Microstructure Three features increase
absorptive surface area: 1.Microvilli tiny projections on the
plasma membrane of mucosa cells. Also collectively called the brush
border 2.Villi finger-like projections of the mucosa that give a
velvety appearance and feel Inside each villi is a capillary bed
and a lacteal (modified lymph capillary) 3.Plicae circularis deep
circular folds of the mucosa and submucosa. These do not disappear
when the intestines are stretched with chyme (unlike rugae in the
stomach)
Slide 22
Small Intestines Continued Peyers patches lymphatic tissue
found in the submucosa toward the end of the small intestine. Since
undigested food reaching the large intestine is riddled with
bacteria, these lymph patches aide in prevention of bacteria
reaching the blood stream
Slide 23
Large Intestine About 1.5 m long, extends from ileocecal valve
to anus Food spends 12-24 hrs in here Major function: Remove excess
water from indigestible food No digestion enzymes or villi Parts:
cecum, appendix, colon, rectum, anal canal Colon: Ascending up on
right Transverse Descending down on left Sigmoid s-shaped curve
Anus: guarded by purse strings voluntary external sphincter
Involuntary internal sphincter
Slide 24
Large Intestine Fauna The large intestine is a complex
ecosystem Many bacteria here aide in digestion of some remaining
nutrients The gases released by bacterial metabolism (methane and
hydrogen sulfide) contribute to feces odor and flatus (500 mL
flatus produced/daymore when certain carb-rich foods are consumed)
Bacteria also produce some vitamins. Ex: Vit. K, and B vitamins
Absorption in the large intestine is limited to most of the
remaining water, these vitamins, and some ions Feces = the
undigested food residues, mucus, bacteria and some water
Slide 25
Large Intestine Continued The longitudinal layer of the
muscularis externa is a three-band cord of muscle called the teniae
coli Usually have tone and cause intestine to pucker into saclike
pockets called haustra The contractions are called haustral
contractions Slow segmenting movements that last ~1 min, every 30
min Mass movements are long, slow, and powerful These flatten large
sections of colon and force contents toward the rectum 3 4x daily,
usually after a meal Fiber increases the strength of the
cotnractions and softens stool
Slide 26
Defecation The rectum is usually empty until a mass movement
forces feces into it and the walls are stretched Mechanoreceptors
in the rectum walls initial the defecation reflex which is
controlled by the sacral region of the spine The walls of the
sigmoid colon and the rectum contract and the anal sphincters relax
When the feces is forced into the rectum, the brain has enough time
to process the input and a conscious decision is made to whether
the external voluntary anal sphincter should remain open or be
constricted Defecation can be temporarily delayed to a more
convenient time If delayed, the reflex contractions end within
seconds and the rectal walls relax until the next mass
movement
Slide 27
Homeostatic Imbalances Gallstones crystallization of
cholesterol in gall baldder Jaundice failure of bile to enter the
small intestines, too much bile in the blood Hepatitis and
cirrhosis Pancreatitis Vitamin K deficiency from lack of bile or
pancreatic juice secretion Diverticulitis Diarrhea and
constipation
Slide 28
Nutrition and Digestion Major nutrients: carbs, lipids,
proteins, water Minor nutrients: vitamins, minerals All used for
growth, maintenance, and repair Some foods are nutrient rich, or
dense. Others are nutrient poor Typical Absorption per day: 100 g
Carbs, 60+ g fat, 50-100 g a.a.s, 3-5 g mins/vits, 7-8 L water
Capability for absorption per day: 1000s g Carbs, 500 g fat,
500-700 g a.a., 20+ L water Mypyramid.gov 2005 US Govt came up with
the new food pyramid to display the proper amount of nutrients one
should consume based on physical activity, age, and sex. The
website also gives customizable tools for determining your personal
nutrient needs
Slide 29
Carbohydrates Sugars, fiber and starches All derived from
plants except milk sugars Simple sugars (glucose, fructose,
galactose) give a sweet taste Starches (amylose, amylopectin,
glycogen) do not Some starches can be broken down completely or
partially by our enzymes, others cannot (ex: amylopectin) and are
called resistant starch These are broken down by bacteria in the
gut Fibers are nondigestible carbs that resemble starches (ex:
cellulose, pectins, gums, chitin, etc). These are NOT found in
animal foods Provide bulk and soften stool for easier passage Fiber
in the diet is essential for maintaining motility and intestinal
health Dietary Sources of Carbs: fruits, veggies, grain products,
milk products
Slide 30
Carbohydrate Metabolism Glucose (aka: Blood sugar) is the main
source of energy for ATP generation Galactose is converted to
glucose before metabolism in the traditional energy pathway
(oxidative cellular respiration) Glycolysis (cytosol) Krebs Cycle
(TCA/Citric acid cycle) (mitochondria) electron transport chain
(inner membrane mitochondria) ATP produced by F 0 F 1 enzyme C 6 H
12 O 6 + 6O 2 6CO 2 + 6H 2 O + 36 ATP Fructose is shunted into the
pentose pathway for energy generation before ultimately being
broken down for ATP generation Brain tissue and RBCs can ONLY use
glucose as fuel where as most other tissue may use either glucose
or fats Skeletal muscle tissue prefers fat as fuel during oxidative
respiration Glucose metabolism is much faster than fat metabolism
Homeo Imbalance: Hyperglycemia and hypoglycemia
Slide 31
Lipids Dietary lipids are mostly Triglycerides We can produce
enough of our own cholesterol and phospholipids Come in saturated,
monounsaturated, polyunsaturated, and trans-fatty acid form Some
are short-chain (
Slide 32
Lipid Metabolism Lipids must be broken down into two-carbon
units called acetic acid Acetic acid enters the TCA cycle for
oxidation The process is fast but incomplete and side-products;
acetoacetic acid and acetone, build up and form ketones which
change blood pH to acidic May result in acidosis, or ketoacidosis.
Symptoms include fruity, wine-smelling breath Often occurs from
no-carb diets (
Slide 33
Proteins Complete proteins provide all essential amino acids
(the ones we cant make in our bodies) Essential a.a.s: Tryptophan,
Methionine, Valine, Threonine, Phenylalanine, Leucine, Isoleucine,
Lysine Aminal sources are best, legumes, nuts, cereals also have
protein but are often incomplete Vegetarians must be careful to get
amino acid nutrition since non- meat products typically a
incomplete a.a profiles
Slide 34
Protein Metabolism After the liver has taken the amino acids it
needs, the rest are sent via blood to other tissues Some are used
within the cells for protein production (enzymes etc) others are
used for export products (hormones, mucus etc) Amino acids are
actively transported to ensure adequate supply of all 20+ types May
be used to make ATP if they are overabundant or carbs/fat are not
available The amino group is removed and forms ammonia while the
rest of the molecule enters the TCA cycle Ammonia (toxic) is sent
to the liver to join with CO 2 to form urea the major protein
component of urine
Slide 35
Liver and Metabolism Functions: Bile production, maintain blood
glucose levels, store glycogen, detoxify ammonia, drugs and
alcohol, degrade hormones, make vital substances available
(cholesterol, blood proteins, clotting proteins, lipoproteins etc),
synthesis of non-essential amino acids Second largest organ by
mass, we have much more tissue than we need and if damage, it can
regenerate easily All nutrients are shunted to the liver via
hepatic portal vein before they are circulated to the rest of the
tissues
Slide 36
Liver and Glucose Excess blood sugar is stored as glycogen
starch in the liver Process is called glycogenesis and is triggered
by insulin among other hormones and molecules levels When blood
glucose drops, the liver breaks down glycogen during glycogenolysis
Can also make new glucose from certain amino acids. Gluconeogenesis
is controlled by many hormones such as thyroxine, insulin,
glucagon, and cortisol
Slide 37
Cholesterol and Transport Cholesterol is the building blood for
many hormones, such as vitamin D, progesterones and androgens Also
a major component of cell membranes and prevents membranes from
becoming stiff We can make all the cholesterol we need and ~15%
comes from our diet Cholesterol is broken down into bile salts,
which eventually leave the body in feces Cholesterol must be
transported by lipoproteins to and from tissues since it is
hydrophobic LDL (bad cholesterol) carries cholesterol to tissues
HDL (good cholesterol) carries it to the liver for processing into
bile, then out (sort of) Both are necessary and good, but the ratio
between them is what may lead to atherosclerotic plaque
formation
Slide 38
Body Energy Balance Energy in (calories) = energy out (work,
storage, heat) When balanced, body weight remains stable, though
body composition may not Carbs: 4 C/g, Protein 4 C/g, Lipids 9 C/g,
Alcohol 7 C/g Hunger and satiety is controlled by a variety of
not-well- understood factors: Neural input from gut, chemicals in
blood, neurotransmitters in the brain, body temperature, and
psychological factors Brain receptors associated with hunger
include thermoreceptors, chemoreceptors, and receptors for leptin
and other peptides
Slide 39
Metabolic Rate Basal Metabolic Rate: the amount of heat
produced by the body per unit of time when it is under basal
condition (resting) Avg 70 kg male has BMR of ~60 to 72 C/hour
Influenced by age, sex, surface area, health status, activity level
and other factors including emotional status Thyroxine = major
determinant of BMR Hyperthyroidism and hypothyroidism both result
in homeostatic imbalance Total Metabolic Rate: the amount of
Calories the body must consume to fuel all ongoing activities
Muscular work is the major determinant of TMR. Slight increases in
activity may cause huge increases in TMR High-level athletes may
exercise vigorously for a few minutes and elevate their TMR 15-20
beyond normal. The TMR will remain elevated for several hours
afterwards (Build intensity, burn more fuel)