Embed Size (px)
Citation preview

CHAPTER 115
Tarlov CystsFrank Feigenbaum | Jean-Marc VoyadzisFraser C. Henderson
A Tarlov cyst is a bulbous enlargement of a spinal nerve rootcerebrospmal fluid (CSF) space that is distinct from othermeninge?! cysts, such as dural ectasia or meningeal diver-ticula. Tarlov cysts most often are found in the sacral spinalcanal, where they can produce bone erosion and compres-sion of adjacent spinal nerve roots, resulting in a debilitatingsacral radiculopathy syndrome.
Tarlov iirst described these cysts in 1938 during his autopsystudies of the filum terminale at the Montreal NeurologicalInstitute,' Since his seminal report, numerous cases of symp-tomatic Tarlov cysts have been published in the literature.2'7With the advent of MRI, our ability to diagnose meningealcysts, such as Tarlov cysts, has been enhanced.
The treatment of symptomatic Tarlov cysts has evolved,along with our understanding of their pathophysiology.Various therapeutic strategies have been described overthe years, with more recent literature trending towarddefinitive surgical treatment. In this chapter the patho-logic, radiographic, and clinical characteristics of Tarlovcysts are presented, and the current treatment options arediscussed.
Epidemiology and Histology
tarlov, or perineurial, cysts are one of the most common formsor meningeal cyst. Estimates of the prevalence of meningeal^ysts, including Tarlov cysts, in the general population vary,h"t generally are in the 5% range.8 In a study of 500 consecu--o/e Patlents with back pain undergoing lumbosacral MRI,
-OLlnd to have one or more meningeal cysts. Amonger group, the cyst was thought to be the source of the
s in 1% Of the cases. Tarlov cysts, particularly thosere are symPtomatic, are more common among women. The
°P or this is unclear, and we have postulated that there^f A 8eilc^er'related differences in the fundamental make-, • i Ura mater or spinal nerve roots that produce this epi-
c disparity.Distinguished perineurial cysts from other menin-"as^ on several histologic criteria.1'9'10 He defined
neur: as Penri-eurial dilations that develop between the endo-just n anO Perineuriuru> typically of the S2 or 3 nerve roots,nerve Xlm to the junction of the dorsal root ganglion andsPirial Ot ' H^-l). Simply stated, each cyst is a dilated
6iv'e root sheath, and the individual nerve fibers of
-o/, °
s
that root are found running within the cyst cavity or its innerlining. Other meningeal cyst subtypes, such as meningealdiverticula and arachnoid cysts, typically are devoid of nerveroot fiber elements.
Tarlov cysts can be single or multiple, and can developanywhere along the spine where nerve roots are present.Progressive cyst enlargement can cause significant bony ero-sion and impingement of adjacent spinal nerve roots, pro-ducing corresponding radiculopathies. For example, a Tarlovcyst in the sacral spinal canal arising from the S3 nerve rootcan cause symptomatic impingement of the ipsilateral S2nerve root beside it, and of the S4 or S5 nerve root below(Fig. 115-2). A Tarlov cyst can also produce contralateralsymptoms if it is large enough to extend across the midlineand compress contralateral nerve roots. Additionally, thenerve root fibers running inside a Tarlov cyst often are atten-uated and splayed out over the inner wall of the cyst. Thisneural fiber alteration and stretching also are suspected ofcausing symptoms.
Tarlov cysts occasionally can be found in combinationwith other meningeal cysts. For example, patients with con-nective tissue disorders, such as Marfan syndrome, can haveTarlov cysts and large ectatic dural cysts so extensive that thedistal spinal sac extends out into the pelvis (Fig. 1 15-3).
The pathogenesis of Tarlov cysts remains unclear. Tarlovproposed that cyst formation could be the result of trauma,ischemic degeneration, inflammation, or hemorrhagic infil-tration from the subarachnoid space.1'9'10 Some patients withsymptomatic Tarlov cysts report a history of sacral trauma,and evidence of old hemorrhage in the form of hemosid-erin deposits and dystrophic calcification within Tarlov cystwalls supports prior trauma as an etiologic factor.7-11"13 Otherreports have suggested that Tarlov cysts result from arach-noidal proliferation or blockage of perineurial fluid flow.14'15
Nabors et al. support a developmental origin, although anassociation between Tarlov cysts and spinal dysraphism is notas strong as that with other types of meningeal cysts.16 Onlytwo patients with symptomatic Tarlov cysts and spina bifidahave been reported, and the relationship could have beencoincidental.7'17
Strully et al.18'19 and Smith20 proposed that Tarlov cystsform as a result of increased CSF hydrostatic pressure. Theypoint out that spinal nerve roots are in communication withthe thecal sac, and that there is myelographic evidence thatspinal fluid flows within the nerve roots and could produce
1135

1136 SECTION 4 I Surgical Procedures
Pia materArachnoidDura mater
Normal spinal nerveEpineurium
PerineuriumEndoneurium
Perineurial cyst
Extraduralmeningealcyst
Leptomeningealcyst
Prolongedsubarachnoidspace over root
Meningealdiverticulum
Extraduralmeningeal(false) cyst
^=7
Meningeal diverticulum
FIGURE 115-1. This diagram illustrates some of the different typesof dural meningeal cysts, including the perineurial (Tarlov) cyst.
FIGURE 115-2. Axial (A) and sagittal (B) T2-weighted sacral MRIsreveal a large Tarlov cyst in the S2 region,central and rightwardwithin the spinal canal. Its contents have imaging qualities similarto those of cerebrospinal fluid (CSF), and there is widening of thespinal canal around it due to bone erosion. A compressed nerveroot is seen adjacent to the cyst (arrow). C, Intraoperatively, thecompressed nerve root (upper Penfield dissector) was visualizedafter retracting the cyst (lower Penfield dissector). The cyst wasfound to arise from the S3 nerve root, and the compressed nerveroot was S2. D, View inside a Tarlov cyst. The nerve root fibersenter the cyst through the ostium and then splay out over thecyst wall.
dilatation due to either higher hydrostatic pressure or inher-ent, traumatic, or iatrogenic weakness in the nerve rootsheath. They also point out that the frequency and size ofTarlov cysts along the spine can be correlated with the ros-tral-caudal hydrostatic pressure gradient.17'18 Several reportson patients with Tarlov cysts have documented either a his-tory of straining or coughing or an exacerbation of symptomsby these maneuvers.7'10'11'18 We also are aware of two cases ofTarlov cysts in patients with pseudotumor cerebri. However,no criteria have been established to determine who mightbenefit from CSF shunting for Tarlov cysts, and investigationsare ongoing.
FIGURE 115-3. This coronal T2-weighted MRI of the sacrum from apatient with Marfan syndrome reveals multiple meningeal cysts.The distal spinal sac continues on as a large ectatic dural cyst erod-ing rightward into the sacrum. Also, multiple separate Tarlov cystsare seen adjacent to the spinal sac, particularly on the left (arrow).
Diagnosis
The treatment of a symptomatic Tarlov cyst first requires acorrect diagnosis. Unfortunately, many patients languishwith undiagnosed or untreated symptomatic cysts due to dieincorrect "rule" that Tarlov cysts always are asymptomatic,regardless of the presence of blatant compression of adjacentnerves or extensive bone erosion. Such patients often are rel-egated to an escalation of narcotics, injection procedures, andneuromodulatory medications as they become progressivelymore symptomatic. It is not uncommon to encounter patientswho have developed narcotic dependency after managementwith extended-release morphine, transdermal fentanyl, orimplanted pain pumps before they are finally referred formeningeal cyst evaluation.
Even more unfortunately, we have encountered patients withsymptomatic Tarlov cysts that were misdiagnosed with a vari-ety of other ailments and treated unsuccessfully with a varietyof procedures, such as hysterectomy, laparoscopic exploration,endometriosis surgery, oophorectomy, appendectomy, surgeryfor piriformis syndrome, sacroiliac joint fusion with implantedcages, fusion of degenerative discs in the adjacent spine, coc-cygectomy, and urinary bladder procedures (Fig. 115-4).
FIGURE 115-4. A, Preoperative axial T2-weighted MRI of the sacrJmfrom a patient with a large Tarlov cyst (white arrowhead). A com-pressed nerve root is just visible to the right of the cyst (blac*arrowhead). B, This axial CTscan reveals that the patient was mis"diagnosed with sacroiliac joint instability. The symptoms did notimprove following insertion of a threaded titanium cage to fuse
the joint. Symptoms improved only after later treatment of thTarlov cyst, which can be seen expanding and eroding the ieral spinal canal.

115 I Tarlov Cysts 1137
„, _ _ found anywhere spinal nerve roots arent and can produce corresponding radiculopathic symp-
Pre IP our experience, symptomatic Tarlov cysts are mostt0 rtionly encountered in the sacral region. The sacralc°,. u}opathy pattern produced can include a multitude of13 toffls> including sacral pain and numbness radiatingS? ,m the backs of the legs to the bottoms of the feet in thedownSI or
theS2 dermatomes; perineal pain; rectal pain; numbness
'
S2-5 dermatomes; neurogenic bladder findings suchurgency, frequency, nocturia, and urinary retention with
a, neec] TO perform a Valsalva or Crede maneuver to ini-• te voiding (S3-4); bowel dysfunction requiring the usef laxatives (S2-3); dyspareunia in women; and erectile/xual dysfunction in men. Symptoms often are positional,
t ino exacerbated by sitting or standing and improved byking down. This finding supports the notion that symptomsre relate J to variations in hydrostatic cyst pressures. Cyst
expansion also can produce adjacent bone erosion, resultingin painf ji insufficiency fractures.
Patients typically describe a crippling inability to sit,describing the feeling as being like "sitting on a rock," caus-ing them to constantly shift from hip to hip when seated ina fruitless quest to find a comfortable position. They oftenare unable to participate in sitting-related activities, such asdriving, working seated at a desk, dining out, or going to mov-ies, events, and religious services. Many patients are forcedto carry cushions or pillows to sit on wherever they go in anattempt tu ameliorate their seated discomfort.
The severe limitation on quality of life experienced bythese pati ;nts often costs them their employment, results indepression as they find themselves progressively houseboundand unable to participate in social activities, and contributesto marital dysfunction and divorce. Making matters worse,some patients may be told by medical professionals thatTarlov cysts are always asymptomatic, despite obvious evi-dence to the contrary.
Differe ^tial Diagnosis
he surgeon should be aware of a host of disease entities thatmay be comorbid or confused with symptomatic Tarlov cysts.
Hydrocephalus, Benign IntracranialHypertension, or Pseudotumor Cerebri
addition to producing symptoms such as headaches andual changes, increased intracranial pressure also may be a
ctor in dae causation of Tarlov cysts. Our evaluation withPnal flij^i taps reveaiec| tnat 1 in 10 patients with symp-
su a 1S 'arlov cysts has consistently elevated opening pres-pr ' ° rurther confound the matter, patients with ongoingPa' Ure Ssues can> like Tarlov patients, also experience back
|J> Paresthesias, and bowel and bladder changes.sPin up0?'8 °^ the subset of patients with comorbid increased
&o n r ] •m
Pressure and symptomatic Tarlov cysts should rely1UII1L ( > u t other causes of pain, and findings on a series oft0 ^ r. P"anctures that consistently reveal the CSF pressureof p ..^' ated. An ophthalmo logic examination for evidence
leuerna may be useful. However, there is no consensus
on the selection criteria for shunting of patients with Tarlovcysts and its contribution to the amelioration of Tarlov cyst-related symptoms is being investigated.
Tethered Cord Syndrome
The presence of a tethered spinal cord sometimes may beoverlooked in the setting of a radiographically impressivesacral Tarlov cyst. Such patients typically present with verysimilar symptoms, including pain and numbness in the lowback or sacral region that radiates down the backs of the legs.They also can have overlapping bowel, bladder, and sexualdysfunction. As with Tarlov cysts, the onset of tethered cordsymptoms may occur at any time in life, particularly followingtrauma, childbirth, or hyperflexion of the spine. Patients withconnective tissue disorders such as Marfan or Ehlers-Danlossyndrome can have meningeal cysts, including Tarlov cysts,and occult tethered spinal cord even though the conus is atlevel LI-2 or above.
Unlike Tarlov cysts, however, tethered cord syndrome isassociated with toe walking, flat feet or pes cavus, enuresis,and scoliosis. A spinal neurocutaneous marker sometimesmay be present. The pain associated with tethered cord syn-drome usually is more moderate, exacerbated by straight legraising or other maneuvers that stretch the cauda equina, andis not affected by upright posture, as with Tarlov cysts. Muscleatrophy is prominent, and especially in the L5- and SI-relatedmuscles. Imaging studies may reveal syringomyelia, descent ofthe conus to the L2 level or below, and a thickened fatty filumor a lipomeningocoele.
Spinal Stenosis and OccultSpondylolisthesis
Stenosis of the central canal or neural foramina can mimicTarlov cyst—related symptoms and should be carefully ruledout with appropriate high-resolution imaging and dynamicradiographs. Overlapping symptoms common to both includeradicular pain and numbness and urinary symptoms.
Cervical and thoracic stenosis symptoms not typical ofTarlov cysts include long-tract findings, such as spasticity andpathologic reflexes like the Babinski and Hoffman signs, andabsence of the abdominal reflex. In cases of lumbar steno-sis, patients usually describe pain in the lumbar area, whereaspatients with symptomatic sacral Tarlov cysts complain morespecifically about pain well below in the sacral region.
Other Masses
Schwannomas and neurofibromas can produce a radicu-lopathic pattern of symptoms similar to those of Tarlovcysts. They also can share imaging characteristics, such asa cystic appearance, lateral location in the spinal canal,and production of bone erosion and foraminal expansion(Fig. 115-5). However, Tarlov cysts do not enhance onMRI following the administration of gadolinium contrast,which is a characteristic typical of schwannomas and neu-rofibromas. Instead, they have signal characteristics similarto spinal fluid on all sequences, with the possible excep-tion of differing signal when there has been hemorrhage oraccumulation of stagnant, more proteinaceous, spinal fluidwithin a cyst.

1138 SECTION 4 i Surgical Procedures
FIGURE 115-5. A, This left S1 foramen mass appears hyperintenseon T2-weighted imaging. B, Unlike a Tarlov cyst, however, itenhances on T1-weighted imaging following gadolinium admin-istration. At surgery, the lesion was found to be a schwannoma.
FIGURE 115-6. A, The cystic lesion seen centrally and to the left inthe spinal canal has imaging characteristics similar to those of aTarlov cyst on T2-weighted imaging. B, However, on T1-weightedimaging, the lesion is hyperintense to cerebrospinal fluid andhas some areas of internal heterogeneity. Further workup withCT myelography, needle biopsy, and angiography revealed thelesion to be a large venous angioma.
We also have encountered other lesions with imaging char-acteristics similar to those of Tarlov cysts. For example, in onecase, a large cystic lesion filling the left SI foramen had theTZ-weighted imaging appearance of a Tarlov cyst, but differedon other sequences (Fig. 115-6). Further workup revealed thelesion to be a large venous angioma within the spinal canal.
Radiography
MRI currently is the gold standard for imaging meningealcysts.21'22 Not only is it useful for differentiating them fromother lesions, but it also can help distinguish among the dif-ferent types of meningeal cysts, including Tarlov cysts. Forexample, Tarlov cysts typically are lateral in the spinal canaland arise from an individual spinal nerve root. Nerve rootfibers often are identifiable inside the cyst on T2-weightedimages (Fig. 115-7). In contrast, meningeal diverticula arefound centrally in the spinal canal, and arise from the tip of
the spinal sac, not from an individual nerve root. When theyare large, Tarlov cysts can be seen to erode and expand thespinal canal or neural foramina and extend into the retroperi-toneal pelvis (Fig. 115-8).
MRI also is superior for defining anatomic relationshipswith surrounding structures. For example, a careful reviewof imaging studies often reveals symptomatic cysts to be bla-tantly compressing adjacent nerve roots and displacing thespinal sac. Understanding these relationships preoperativelyis critical for surgical planning.
CT myelography previously was used preoperatively todistinguish Tarlov cysts from other forms of meningeal cvstsbased on the premise that Tarlov cysts filled poorly and in adelayed fashion.1'2'16-19 Other meningeal cysts, such as menin-geal diverticula, were believed to fill more rapidly. However,these criteria are not reliable, because the extent of dye pen-etration into a cyst depends on the degree of its communica-tion with the spinal sac, not on the cyst type. For example,we have encountered Tarlov cysts that communicate quitefreely with the spinal sac, and filled readily on CT myelog-raphy (Fig. 115-9). Such cysts would have been erroneouslycategorized as non-Tarlov cysts using the more antiquatedradiographic criteria.
Despite the fact that meningeal cysts, particularly Tarlovcysts, can be radiographically impressive, a careful searchshould be conducted to rule out other pathology that mightexplain the patient's symptoms. For example, a completeworkup of a sacral Tarlov cyst should include not only a sacral
FIGURE 115-8. A, Two large intrapelvic Tarlov cysts are seen on thisaxial T2-weighted MRI (blackarrows). Also seen is a separate 1 ar-lov cyst within the sacral spinal canal abutting a nerve root to theright of midline (white arrow). B, On this sagittal image from 'hesame patient, the left intrapelvic cyst can be seen extending outthrough the S1 neural foramen ventrally into the retroperitoneurn.
FIGURE 115-7. The nerve root fiber bundle inside this sacral Tarlovcyst is clearly seen on an axial T2-weighted MRI.
FIGURE 115-9. A, Side-by-side Tarlov cysts are present on thisaxial CT myelogram image (arrowheads). One fills with dye t>ut
the other does not, demonstrating that CT myelography is urtrelj'able as a diagnostic tool for this pathology. B, Unlike CT, botnTarlov cysts are clearly seen on T2-weighted MRI, the preferredimaging modality.
115 | Tarlov Cysts 1139
/oT but also an MRI and flexion-extension radiographs of, lumbar spine to evaluate for disc herniations, stenosis,
1 nrh'lolisthesis, metastases, hemorrhages, and other pos-cpOIl"'Jble pathologies.
ia ostic Cyst Aspiration
vv/e usually avoid percutaneous procedures involving menin-al cvsts due to the risks involved. However, needle aspi-tion occasionally is used as a diagnostic tool to determinehether a Tarlov cyst is symptomatic. When conducted with_ropriate imaging to confirm correct needle placement,
spiration may temporarily decompress a cyst long enoughbefore it refills for a patient to notice a transient improve-ment in symptoms. This would imply that the aspirated cyst isat least partially responsible for the patient's symptoms. Sucha cyst could then be a target for treatment.
jreatmentNeedle Aspiration
Unfortunately, a significant number of patients with symp-tomatic Tarlov cysts undergo percutaneous needle aspirationprocedures as an attempt at treatment, not for diagnosis. Suchprocedures are ineffective, because aspirated fluid within aTarlov cyst typically is replaced rapidly with spinal fluid throughthe proximal nerve root in communication with the spinalsac.2'7'16 One study that assessed the effectiveness of percutane-ous drainage of Tarlov cysts found that four of the five patientsin that :eries suffered a recurrence of symptoms.8 A separatereport in 2001 described patients who underwent percutaneousaspiration of their cysts preoperatively.7 None of those patientsimproved, and, in fact, some experienced marked worsening oftheir symptoms. This deterioration may have been the result ofhemorrhage in the cyst wall, or nerve root injury.
In general, the use of aspiration for treatment of a Tarlovcyst is inconsistent with an understanding of the fundamen-tal underlying pathology involved and exposes the patient tothe risk >f spinal fluid leakage, meningitis, hemorrhage, andnerve root injury. We therefore restrict the use of needle aspi-ration, i is ing it only as a diagnostic tool in rare situations, asdescribed in the preceding section.
Needle Aspiration and Fibrin Glue Injection
treatment with percutaneous aspiration followed by fibringlue injection also has been described. Authors of one reportof tour patients with symptomatic Tarlov cysts found thatPercutaneous fibrin glue therapy was effective in alleviatingyntptorns, although three patients developed postprocedural
eptic meningitis.23 Blind percutaneous introduction of mul-Ple needles into a Tarlov cyst also increases the probability
ot causing nerve injury.to our experience, fibrin glue treatment fails in a largetuber of patients, and those patients require subsequent
K D> Unfortunately, the introduction of fibrin glue or otherrates into a Tarlov cyst makes subsequent surgical treat-
-j-1 aiore difficult because it produces scarring or coating.to neural elements within the cyst are then much harder
entify and protect during surgery. We have encountered
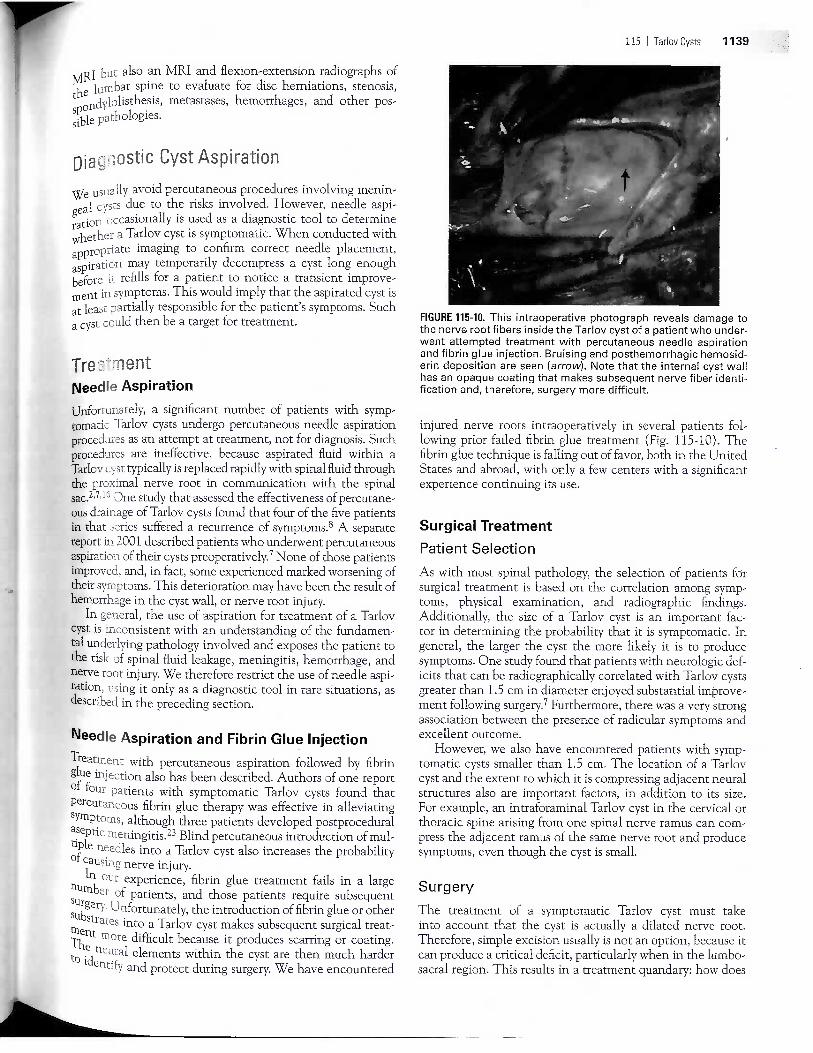
FIGURE 115-10. This intraoperative photograph reveals damage tothe nerve root fibers inside the Tarlov cyst of a patient who under-went attempted treatment with percutaneous needle aspirationand fibrin glue injection. Bruising and posthemorrhagic hemosid-erin deposition are seen (arrow). Note that the internal cyst wallhas an opaque coating that makes subsequent nerve fiber identi-fication and, therefore, surgery more difficult.
injured nerve roots intraoperatively in several patients fol-lowing prior failed fibrin glue treatment (Fig. 115-10). Thefibrin glue technique is falling out of favor, both in the UnitedStates and abroad, with only a few centers with a significantexperience continuing its use.
Surgical Treatment
Patient Selection
As with most spinal pathology, the selection of patients forsurgical treatment is based on the correlation among symp-toms, physical examination, and radiographic findings.Additionally, the size of a Tarlov cyst is an important fac-tor in determining the probability that it is symptomatic. Ingeneral, the larger the cyst the more likely it is to producesymptoms. One study found that patients with neurologic def-icits that can be radiographically correlated with Tarlov cystsgreater than 1.5 cm in diameter enjoyed substantial improve-ment following surgery.7 Furthermore, there was a very strongassociation between the presence of radicular symptoms andexcellent outcome.
However, we also have encountered patients with symp-tomatic cysts smaller than 1.5 cm. The location of a Tarlovcyst and the extent to which it is compressing adjacent neuralstructures also are important factors, in addition to its size.For example, an intraforaminal Tarlov cyst in the cervical orthoracic spine arising from one spinal nerve ramus can com-press the adjacent ramus of the same nerve root and producesymptoms, even though the cyst is small.
Surgery
The treatment of a symptomatic Tarlov cyst must takeinto account that the cyst is actually a dilated nerve root.Therefore, simple excision usually is not an option, because itcan produce a critical deficit, particularly when in the lumbo-sacral region. This results in a treatment quandary: how does

1140 SECTION 4 I Surgical Procedures
one eliminate a symptomatic Tarlov cyst without injuring thenerve root fibers inside and producing a neurologic deficit?
In the past, surgical treatments such as decompressive lam-inectomy, cyst fenestration, and complete cyst excision havefallen from favor due to a lack of success and unacceptablecomplication rates.2'3'6'24 More recent surgical techniqueshave targeted the underlying pathology causing nerve rootdilation, that is, the process that allows spinal fluid to accu-mulate within an affected nerve root.
An initial step in this direction was the description offenestration and imbrication techniques that involve open-ing a Tarlov cyst.6 The cyst is then reduced in size, either byimbrication or partial wall excision, thereby reconstituting amore normal caliber nerve root, which no longer compressesadjacent structures. However, such techniques do not preventthe continued flow of spinal fluid into the affected nerve rootcyst, so they do not eliminate the risk of cyst reexpansion andspinal fluid leakage. Additionally, nerve fascicles in a Tarlovcyst often are found within the cyst wall itself, or so exten-sively splayed out over the internal surface of the cyst wallthat they are not easily seen, even with the aid of an oper-ating microscope. Cyst wall excision to decrease the overallsize of a Tarlov cyst therefore increases the risk of producingdeficits due to inadvertent nerve root fiber sectioning.
Current surgical techniques are focused on resolving thequandary of how to prevent spinal fluid flow into a symptom-atic Tarlov cyst without injuring its nerve root fibers. To thisend, we have focused on treatment of the ostium, where spi-nal fluid and nerve root fibers enter the cyst. We also havemade efforts to confine cysts to prevent further compressionof adjacent structures (Fig. 115-11).
Intraoperative electrophysiologic monitoring is an inte-gral component of Tarlov cyst surgery. During the process ofexposure and cyst dissection, it aids the surgeon in identifyingspecific nerve roots and gives feedback on the tolerance ofnerves to manipulation. Thus, intraoperative monitoring canbe used to assess the status of a Tarlov cyst—involved nerveroot throughout the process of cyst treatment, and gives thesurgeon a baseline to assess nerve function before and aftercyst treatment. For example, the nerve root sleeve proximal
FIGURE 115-11. A, Two Tarlov cysts abutting nerve roots in thesacral spinal canal are seen on this preoperative axial T2-weightedMRI (arrows). B, Postoperatively, the treated cysts are identified(arrows), as are the decompressed nerve roots just ventral andlateral to each treated cyst.
to a treated cyst can be stimulated following cyst explorationand treatment to determine whether it is still in continuityand conducting as it was before treatment.
Summary
Tarlov cysts are an important clinical entity in the differentialdiagnosis of spinal radiculopathy, sacral pain syndromes, andsacral spinal insufficiency fractures, particularly in women.The symptoms they produce can be crippling. Althoughthe relationship remains unclear, elevated CSF pressureand trauma may play a role in their pathogenesis. MRI hasenhanced our ability to diagnose symptomatic Tarlov cvstsand preoperatively assess their anatomic relationships.
The management of symptomatic Tarlov cysts has pro-gressed significantly in the last decade. Trends in the litera-ture have favored surgical treatment in experienced hands toreduce the risk of nerve root injury and spinal fluid leakage.Treatments with percutaneous needle techniques such asaspiration or fibrin glue injection are falling out of favor dueto lack of symptomatic improvement and high cyst refillingrates. In our experience, patients with large cysts and corre-sponding radicular symptoms are more likely to experiencesubstantial relief from surgery. However, patients with smallercysts also can benefit if focal nerve root compression is identi-fied on preoperative imaging.
KEY REFERENCES
Acosta F, Quinones-Hinojosa A, Schmidt MH, et al: Diagnosis and manage-ment of sacral Tarlov cysts. AJNR Am ] Neurosurg Focus 15:1—10, 2003.
Feigenbaum F, Henderson F: Surgical management of meningeal cysts,including perineural (Tarlov) cysts and meningeal diverticula. Semin SpineSurg 18:154-160, 2006.
Nabors NW, Fait TG, Byrd EB, et al: Updated assessment and current clas-sification of spinal meningeal cysts. ] Neurosurg 68:366-377, 1988.
North RB, Kidd DH, Wang H: Occult, bilateral anterior sacral and intrasa-cral meningeal and perineural cysts: case report and review of the litera-ture. Neurosurgery 27:981-986, 1990.
Patel MR, Louie W, Rachlin J: Percutaneous fibrin glue therapy of meningealcysts of the sacral spine. AJR Am ] Roentgenol 168:367-370, 1997.
Paulsen RD, Call GA, Murtagh FR: Prevalencce and percutaneous drainageof cysts of the sacral nerve root sheath (Tarlov cysts). AJNR Am J Neuro-rodiol 15:293-297, 1994.
Strully K, Heiser S: Lumbar and sacral cysts of meningeal origin. Radiology62:544-549, 1954.
Tarlov IM: Perineurial cysts of the spinal nerve roots. Arch Neural Psychaay(Chic) 40:1067-1074, 1938.
Voyadzis JM, Bhargava P, Henderson F: Tarlov cysts: a study of 10 cases withreview of the literature. J Neurosurg Spine 95:25-32, 2001.
REFERENCES
The complete reference list is available online atexpertconsult.com.





























