Upload
luiperdvrou
View
218
Download
2
Tags:
Embed Size (px)
DESCRIPTION
Equine Medicine surgery and reprodution Secon edition 2012 Capitulo 1
Citation preview
1 2013 Elsevier LtdDOI: 10.1016/B978-0-7020-2801-4.00004-3
CONTENTS
1.1 Normalupperalimentarytractfunction:deglutition 2
Oral, pharyngeal and oesophageal phases of deglutition 2Prehension 2Mastication 2Lingual function 2Elevation of palate 2Pharyngeal constriction 2Laryngeal protection 2Crico-pharyngeal relaxation 2Primary and secondary oesophageal peristalsis 2
1.2 Diagnosticapproachtocasesofdysphagia 2History signs of dysphagia 2Physical examination, external and oral inspection 3Endoscopy per nasum 3Radiography and fluoroscopy 4Oral examination under general anaesthesia 4
1.3 Aetiologyofdysphagia:oralphaseabnormalities 4Facial palsy and lip lesions 4Temporo-mandibular joint and hyoid disorders 4Lingual abnormalities 5Dental disorders 5Congenital and acquired palatal defects 5Other oral conditions: foreign bodies, neoplasia 5
1.4 Aetiologyofdysphagia:pharyngealphaseabnormalities 5
Pharyngeal paralysis 5Pharyngeal compression: strangles abscessation 5Pharyngeal cysts, palatal cysts 5Epiglottal lesions, including sub-epiglottic cysts 5Laryngeal abnormalities 6Fourth branchial arch defects (4-BAD) 6
1.5 Aetiologyofdysphagia:oesophagealphaseabnormalities 6
Megaoesophagus 6Oesophageal obstruction (choke) 6Oesophageal strictures/stenosis 6Intra-mural oesophageal cysts 6Oesophageal rupture 6Neoplasia 6Wind-sucking 6Grass sickness 7
1.6 Oraltrauma,mandibularfracturesetc. 71.7 Oesophagealobstruction 71.8 Anatomyoftheoralcavity 8
Oral cavity 8Normal dental anatomy 8Triadan system 9Eruption of teeth 10
1.9 Abnormalitiesofwearabrasionandattrition 101.10 Periodontaldisease 121.11Dentalcaries 131.12 Endodonticdiseaseincludingdentalabscessation 141.13 Tumoursoftheupperalimentarytract 15
Odontogenic tumours 15Other tumours of the jaw 15
1.14Diagnosticapproachtodentaldisorders 15Ageing of horses by dentition 15Clinical signs of dental disease 15Oral examination 16Radiography of teeth 16Other ancillary diagnostic techniques 17Indications for dental extraction 17Options for the extraction of incisors, canines and wolf teeth 18Options for the extraction of cheek teeth 18
Furtherreading 20
Upper alimentary systemJ. Geoffrey Lane, Robert Pascoe
Chapter 1
2Equine Medicine, Surgery and Reproduction
Elevation of palateThe action of the levator palatini muscles draws the soft palate dorsally to close off the naso-pharynx and prevents the nasal reflux of ingesta; this marks the onset of the involuntary stages of deglutition.The horse has an intra-narial larynx at all times other than during
the momentary disengagement for deglutition. (See 5.18 and 5.21.)The levator palatini muscles lie parallel with the drainage ostia of
the auditory tube diverticula (ATDs) so that when they contract the ostia open to allow exchanges of air for pressure equilibration across the ear drum.
Pharyngeal constrictionThe constrictor action of the circular muscles of the pharyngeal walls embraces both oro-pharynx and naso-pharynx the latter can be appreciated during endoscopic examinations of the naso-pharynx. A wave of constriction follows the contraction of the tongue base and passes from rostral to caudal efficiently to empty the oro-pharynx the pharyngeal stripping wave leaving minimal quantities of ingesta at the base of the tongue.
Laryngeal protectionAspiration of food and fluid through the rima glottidis is prevented primarily by the tight adduction of the vocal folds and arytenoid cartilages and to a lesser extent by the retroversion of the apex of the epiglottis.
Crico-pharyngeal relaxationThe upper oesophageal sphincter is formed by the thyro- and crico-pharyngeus muscles, and these are maintained in a state of contrac-tion to prevent involuntary aerophagia, especially during forced exercise. Relaxation of the crico-pharynx simultaneous with the pha-ryngeal stripping wave permits the food and fluid boluses to pass caudally into the proximal oesophagus.
Primary and secondary oesophageal peristalsisAfter each bolus has passed through into the proximal oesophagus, primary peristaltic waves are initiated by active closure of the cricopharynx.Primary oesophageal peristalsis carries individual boluses to the
cardia, but the process is not completely efficient and small quantities of ingesta are left at variable levels in both the cervical and thoracic oesophagus, even in normal horses. These ingesta are either picked up in the bolus of a subsequent primary wave or by locally generated secondary peristalsis.
1.2 DIAGNOSTIC APPROACH TO CASES OF DYSPHAGIA
History signs of dysphagiaThe signs of dysphagia include: an unwillingness to eat. slow, messy feeding. halitosis. rejection of semi-masticated food onto the ground (quidding).
1.1 NORMAL UPPER ALIMENTARY TRACT FUNCTION: DEGLUTITION
Normal deglutition comprises the prehension and mastication of ingesta followed by its transfer from the oro-pharynx to the stomach.
Oral, pharyngeal and oesophageal phases of deglutitionDeglutition is divided into three stages:
1. The oral phase which includes the gathering of food, movements within the oral cavity, mastication and the formation of boluses of ingesta at the base of the tongue is under voluntary control.
2. The presence of a bolus gathered at the tongue base triggers the sequence of reflexes, collectively known as swallowing, which propels the ingesta from the pharynx the pharyngeal phase into the oesophagus. The glosso-pharyngeal nerve (IX) and the pharyngeal branches of the vagus (X) innervate the pharynx and larynx, and their afferent and efferent pathways are co-ordinated in the swallowing centre in the brainstem.
3. Waves of peristalsis convey the ingesta along the oesophagus to the stomach the oesophageal phase of deglutition.
PrehensionPrehension in the horse relies on the incisor teeth to grasp and section herbage and on the lips to pick up smaller pieces of ingesta as well as to contain it within the mouth and to manipulate food towards the cheek teeth.
MasticationThe molar and premolar teeth are responsible for the mechanical crushing of the fibrous diet.The tongue and buccal musculature assist in manipulating the
ingesta between the maxillary and mandibular dental arcades.Mastication requires free opening and closure of the temporo-
mandibular joints (TMJs) through the action of the masticatory muscles the masseter, pterygoid and temporal muscles close the jaws, and gravity, assisted by the digastric muscles, opens them. The masticatory muscles receive their innervation through the mandibular branch of the trigeminal nerve (V).The shape of the articular surfaces of the TMJs together with the
presence of menisci permit lateral movements by the mandibular teeth across the wearing surfaces of the upper cheek teeth.
Lingual functionThe tip of the tongue assists in prehension and moves the ingesta between the cheek teeth.Contraction of the tongue base helps in the formation of boluses
and, once collected, each bolus is driven caudally; this triggers the involuntary phases of deglutition by driving food and fluid caudally from the oro-pharynx.The tongue is attached to the hyoid apparatus, and free move-
ment at the tympano-hyoid articulation is required for the craniocaudal tongue motion which facilitates bolus formation in the oro-pharynx.The glossal musculature receives its motor supply via the hypoglos-
sal nerve (XII).
3ChapterUpper alimentary system | 1 |
Local lymphadenopathies and firm distension of the oesophagus to the left side of the trachea are changes which might be found during palpation of the throat area.Useful information can be obtained by attempting to pass a
nasogastric tube. This should determine whether pharyngeal swallow-ing reflexes are still present or whether the upper alimentary tract is physically obstructed.Under sedation and with a Hausmann gag in place, a detailed
inspection of the oral cavity with the aid of a dental mirror should look for evidence of dental malalignment, enamel pointing of the cheek teeth, fractures of the dental crowns, periodontitis, soft-tissue lesions of the buccal cleft and palate, oral foreign bodies and lesions of the tongue. The structures involved may require digital manipula-tion to complete the examination, and a tell-tale foul smell points to the presence of stale entrapped ingesta.Defects of the palate cannot always be appreciated from a conscious
examination of the mouth because they are often restricted to the caudal section of the soft palate.
Endoscopy per nasumThe presence of ingesta in the nasal meati, nasopharynx, larynx or trachea is never normal and confirms the broad diagnosis of pharyn-geal or oesophageal phase dysphagia. Such contamination may range from clods of green grass to tiny flecks of chewed ingesta. The latter may be appreciated only on examination of tracheal aspirate samples.Endoscopy per nasum is necessary to confirm whether pharyngeal
paralysis is present (Figure 1.2). The usual findings consist of:
a mixture of saliva and ingesta on the walls of the nasopharynx. persistent dorsal displacement of the palatal arch. poor constrictor activity during deglutition. failure of dilation of one or both ATD ostia during swallowing.Where functional pharyngeal paralysis is diagnosed, many horses are afflicted with pharyngeal hemiplegia, i.e. the pharyngeal neuropathy is unilateral, for example in cases of guttural pouch mycosis (see Aetiopathogenesis in 5.6).True pharyngeal paralysis may be seen in cases of botulism.Conchal necrosis may accompany prolonged dental suppuration
and may be seen on endoscopy of the nasal chambers (see Conchal necrosis and metaplasia in 5.16).
productive coughing. nasal reflux of saliva, ingesta and fluids.Obviously, horses that are unable to eat and swallow food are likely to lose weight rapidly, but this process is accelerated if the horse develops secondary inhalation pneumonia, which is a common sequel to dysphagia. A moist cough is typical of animals aspirating food or saliva into the rima glottidis. In addition to a clear case history, careful observation of the patients attempts to eat and drink should be made.If the horse shows return of ingesta from its mouth, the site of the
lesion causing the dysfunction must lie in the oral cavity or oropharynx.Nasal reflux of ingesta points to an abnormality of the pharyngeal
or oesophageal phase of deglutition (Figure 1.1).
Physical examination, external and oral inspectionEvidence of systemic and/or toxic disease, including Streptococcus equi infection, botulism, grass sickness, rabies, upper motor neuron disease, lead poisoning and tick paralysis should be sought.The external assessment should check for evidence of concurrent
neuropathies such as facial palsy, Horners syndrome or head tilt.Thoracic auscultation should check for signs of inhalation
pneumonia.
Figure1.1 Nasal reflux of saliva and ingesta in a case of acute oesophageal obstruction.
Figure1.2 Pharyngeal paralysis in a case of guttural pouch mycosis. Note the asymmetric larynx the GPM is right-sided; the dorsally displaced soft palate; and the saliva and ingesta on the pharyngeal walls.
4Equine Medicine, Surgery and Reproduction
structures. Fluoroscopic studies again, using contrast media are required for the dynamic investigation of deglutition.Lateral radiographs of the chest are a useful aid to monitor the
progress of aspiration pneumonia which shows a characteristic pattern of consolidation in the dependent lung lobes.
Otherimagingtechniques
Ultrasonography always has a potential role in the investigation of the soft tissues of the throat but also has a specific value in the assessment of the temporo-mandibular joint, which is a difficult structure for radiography.Scintigraphy has a specific role in the investigation of early cases of
dental apical infections and can also confirm bony activity in the area of the TMJ.The role of advanced techniques of MRI and CT in the investigation
of dysphagia, and the advantages over traditional methods such as palpation and endoscopy, is not yet established.
Oral examination under general anaesthesiaGeneral anaesthesia is necessary to complete the inspection of the oral cavity. The tendency for soft tissues to obscure the view, particularly towards the base of the tongue, can be overcome by the use of an endoscope passed through a polypropylene mare gynaecological speculum. Again, general anaesthesia is required for a more detailed manual or endoscopic examination of the caudal oral cavity, espe-cially in the region of the epiglottis and ary-epiglottic folds.
1.3 AETIOLOGY OF DYSPHAGIA: ORAL PHASE ABNORMALITIES
Facial palsy and lip lesionsFacial paralysis inhibits the ability of a horse to prehend and retain ingesta in the oral cavity (see Chapter 11).A laceration at the commissures of the lips can arise when a horse
becomes hooked at the corner of the mouth and a major avulsion injury follows. Careful anatomical reconstruction of the lip margins is required.Sarcoids may develop at the lip margins, especially the commis-
sures, and the method of therapy (excision, cryosurgery or chemical cautery) which is used to ablate the lesions must also take regard of the acceptance of a bit after healing.
Temporo-mandibular joint and hyoid disordersThe temporo-mandibular joints (TMJs) lie very superficially imme-diately ventral to the zygomatic arch and are vulnerable to direct trauma, including penetrating wounds. However, TMJ disorders are rare in the horse but when they do occur they cause marked pain and a rapid loss of bodily condition. Disuse leads to obvious atrophy of the masticatory muscles, most obviously the masseters. Clinical exam-ination shows resentment of attempts to open the mouth and even under general anaesthesia the range of opening may be severely reduced. A diagnosis of TMJ disease is difficult to confirm by radiog-raphy and other techniques such as ultra-sonography, scintigraphy, MRI or CT scanning, depending on availability, will provide superior images.
Provided that an endoscope with a diameter of 8.0 mm or less is available, the diagnosis of a palatal defect by inspection of the floor of the nasopharynx per nasum presents no difficulties, even in quite young foals (Figure 1.3).Other abnormalities which may cause dysphagia and which can be
confirmed by endoscopy of the pharynx and larynx include:
epiglottal entrapment, with or without a sub-epiglottic cyst (see 5.22 and 5.23).
epiglottal hypoplasia. iatrogenic palatal defects after over-enthusiastic staphylectomy. fourth branchial arch defects (4-BAD syndrome) (see 5.25). evidence of sub-epiglottic foreign bodies, usually in the form of
unilateral oedema in the region of the ary-epiglottic folds. intra-palatal cysts (see Palatal defects in 5.28). nasopharyngeal cicatrix. iatrogenic hyper-abduction of the arytenoid cartilage from
prosthetic laryngoplasty or other evidence that tie-back surgery has triggered dysphagia.
arytenoid chondropathy (see 5.24). pharyngeal neoplasia (see Pharyngeal and laryngeal neoplasia
in 5.28). pharyngeal distortion by external compressive lesions such as
neoplasia or abscesses.
The extent of tracheal aspiration of ingesta which accompanies the dysphagia can be deduced by advancing the endoscope into the trachea to the level of the thoracic inlet. This is particularly helpful to assess compromised swallowing after tie-back surgery.Oesophagoscopy is often unrewarding in the investigation of
equine dysphagia simply because physical or functional obstructions of the oesophagus invariably lead to a build-up of ingesta and saliva in the lumen which, in turn, inhibits a satisfactory field of view. However, when the patient has been starved prior to endoscopy, evi-dence of conditions such as oesophagitis, megaoesophagus, stricture, rupture, tracheo-oesophageal fistula, diverticulum, intra-mural cyst, dysautonomia and neoplasia may be found.
Radiography and fluoroscopyPlain lateral radiographs of the pharynx, larynx and cervical oesopha-gus are used to investigate the relationships between normal anatomi-cal structures and to identify intra-luminal, mural and extra-mural soft-tissue swellings. Contrast media can be helpful to outline these
Figure1.3 Midline cleft of the soft palate in a foal exhibiting the nasal reflux of milk. Most clefts are confined to the soft palate in horses, and the hard palate is rarely involved. Diagnosis is best confirmed by endoscopy per nasum.
5ChapterUpper alimentary system | 1 |
Squamous cell carcinomas, lymphosarcoma and connective tissue tumours arise sporadically in horses, and they tend to cause dysphagia simply by virtue of space occupation.
1.4 AETIOLOGY OF DYSPHAGIA: PHARYNGEAL PHASE ABNORMALITIES
Pharyngeal paralysisParalysis or paresis of the pharyngeal constrictor muscles arises when the function of glosso-pharyngeal nerve (IX) is compromised. When food and fluids are not propelled into the upper oesophagus they may be returned via the nostrils, aspirated into the laryngeal airway, or spilled out of the mouth. The most common causes of pharyngeal paralysis are:
guttural pouch mycosis (see 5.6) (Figure 1.2). ATD diverticulitis (see 5.5). botulism (see Chapter 11). heavy-metal poisoning (see Chapter 22).It is always correct to investigate the possibility of ATD disease in cases of pharyngeal dysfunction. When there is marked inhalation of ingesta leading to broncho-pneumonia or evidence of dehydration, the condition of the patient demands euthanasia on humane grounds. However, some horses with partial pharyngeal dysfunction may survive without distress and simply show an occasional cough and nasal discharge without progress to aspiration pneumonia. Restora-tion of pharyngeal function may occur, but this takes many months.Nasopharyngeal cicatrization inhibits the efficiency of pharyngeal
constrictor function, but horses with this disorder are more likely to present for the investigation of respiratory noises and/or exercise intolerance.
Pharyngeal compression: strangles abscessationThe presence of extra-mural soft-tissue swellings adjacent to the pharynx may cause dysphagia because of external compression of the pharynx and also, in the case of an abscess because of the pain associated with the movement of food boluses past the lesions (see Chapter 19).
Pharyngeal cysts, palatal cystsThe origin of pharyngeal wall cysts is not known, but intra-palatal cysts may well develop from salivary tissue which is normally distrib-uted widely in the palatal mucosa. Diagnosis of both conditions is by a combination of endoscopy and radiography. While cysts on the pharyngeal walls can be excised or ablated by trans-endoscopic laser application, lesions within the substance of the soft palate are not as easily treated because fistulation of the palate is a likely sequel to surgery.
Epiglottal lesions, including sub-epiglottic cystsPeracute epiglottitis, with oedema and cellulitis may occur as a com-plication of upper respiratory tract viral infections and can be so severe that a potentially fatal airway obstruction occurs. Emergency trache-otomy intubation may be necessary to prevent asphyxiation.A less severe form of epiglottitis with swelling and distortion of the
epiglottis may have a similar aetiology and causes dysphagia and
Ankylosis of the joint between the stylo-hyoid and petrous temporal bones is often a feature of temporo-hyoid osteoarthritis (THO) in horses and may limit a horses ability to move the tongue (see Temporohyoid osteoarthropathy, THO in 5.2)
Lingual abnormalitiesThe well protected location of the hypoglossal nerve in horses is such that injuries to the nerve with lingual paralysis are rare.Trauma, either in the form of lacerated wounds or tongue-strap
strictures, accounts for the majority of tongue lesions of the horse. A horse with a severely injured tongue may be unable to manoeuvre ingesta around the mouth and is inclined to drop food or to collect it in the buccal cleft.Horses which lose the rostral portion of the tongue through incisive
wounds can maintain normal bodily condition, albeit showing messy feeding patterns.Foreign bodies may become buried in the lingual tissues, and the
painful suppurative response can reduce a horses inclination to eat.
Dental disordersDental disorders are discussed at length later in this chapter, but the reason why dental diseases cause dysphagia is through oral pain. There is little evidence that horses are afflicted with tooth-ache per se, but soft-tissue pain through ulceration of the oral mucosa, particu-larly at the gingival margins in the form of periodontitis, is a major contributor to an inability to masticate food adequately and to reject partly masticated food to the ground quidding.
Congenital and acquired palatal defectsThe presence of a defect in the soft palate prevents an effective seal between the oral cavity and the naso-pharynx during the lingual pro-pulsion of ingesta towards the tongue base and during pharyngeal contraction. The result is that food and fluids are refluxed via the nasal chambers to the nares.Simple midline linear defects of the soft palate are the most
common cause of the nasal reflux of milk by foals in early life (Figure 1.3). Rarely, the midline cleft extends rostrally into the hard palate.Other forms of palatal defect include unilateral hypoplasia and
pseudo-uvula formation which can escape confirmation until the patient is considerably older. They often occur in association with epiglottal entrapment.Palatal reconstructive surgery using mandibular symphysectomy
has been described, but the results are invariably disappointing.Excessive palatal resection (staphylectomy) (see 5.21) in the treat-
ment of dorsal displacement of the soft palate (DDSP) is irreparable.Inadvertent splits in the palate have been reported after the relief of
epiglottal entrapment by section with a hooked bistoury passed per nasum in the standing horse (see 5.22).
Other oral conditions: foreign bodies, neoplasiaThe most common foreign bodies in the oro-pharynx are brambles/thorned plant material which become lodged in the sub-epiglottal area or in the lateral food channels causing acute-onset dysphagia. Endoscopy per nasum will show oedema in the ary-epiglottic folds, even when the foreign body itself cannot be seen. Such an endoscopic finding is an indication for an oral examination, either by palpation or with a guarded endoscope, under general anaesthesia. Other foreign bodies such as wire fragments may become wedged between teeth.
6Equine Medicine, Surgery and Reproduction
1.5 AETIOLOGY OF DYSPHAGIA: OESOPHAGEAL PHASE ABNORMALITIES
MegaoesophagusMegaoesophagus has been reported sporadically in the horse, some-times as a primary congenital disorder and sometimes secondary to other conditions causing restriction of oesophageal function such as vascular ring strictures. Coughing, nasal reflux of ingesta and disten-sion of the cervical oesophagus may all be features. Confirmation of the diagnosis is easily achieved by contrast radiography.
Oesophageal obstruction (choke)Obstruction of the oesophagus is discussed in greater detail at the end of this chapter (see 1.7). Impaction of dry fibrous material to occlude the lumen of the oesophagus, typically in the cervical segment, is the commonest cause of acute dysphagia in the horse. Older horses seem to be more susceptible but this may relate to the diets offered to horses which are not being fed for competitive exercise. In contrast, foals which are beginning to take herbage occasionally plug the oesophagus with a bolus of dry grass.
Oesophageal strictures/stenosisOesophageal strictures are thought to be the sequel of episodes of acute obstruction, and horses with this condition are presented with recurring choke. Confirmation of the diagnosis is best achieved by contrast radiography. The most common site for stricture develop-ment is at the thoracic inlet. Resection of the stenosed segment of oesophagus may be attempted, but a guarded prognosis is indicated because recurrence of the stricture at the site of anastomosis is a fre-quent complication.
Intra-mural oesophageal cystsCongenital intra-mural cysts may be encountered in young horses and cause dysphagia through restricting peristalsis and obstruction to the passage of oesophageal boluses. The lesions may be seen as swellings in the oesophageal wall at endoscopy or by ultrasonography or con-trast radiography.
Oesophageal ruptureRuptures of the oesophagus may arise through external trauma by kicks or stake wounds or by misuse of a nasogastric tube. Regardless of the cause, the condition carries a poor prognosis unless affected horses are presented for treatment soon after the injury has occurred because of the rapid advance of contamination and cellulitis into the surrounding tissues.
NeoplasiaTumours of the oesophagus are very rare in the horse, but squamous cell carcinoma at this site has been reported.
Wind-suckingHorses performing this stereotypy do not swallow air, and deglutition is not part of the sequence of events. The muscles of the upper neck contract to create a pressure gradient across the soft tissues of the throat so that the walls of the pharynx and upper oesophagus are
coughing presumably through discomfort during deglutition. Afflicted horses also produce untoward respiratory sounds at exercise. The diagnosis is established by endoscopy, but it can be difficult to differentiate this form of epiglottitis, which is likely to be responsive to vigorous antibiotic therapy, from a para-epiglottic foreign body.The increased mass of the epiglottis arising in entrapment by the
glosso-epiglottal mucosa (see 5.22) or by a sub-epiglottic cyst (Figure 1.4) (see 5.23) causes dysphagia because of space-occupation and a restriction of the freedom for epiglottal retroversion. Secondary per-sistent dorsal displacement of the palatal arch may occur. Persistent DDSP is an indication for oral endoscopy and lateral radiography possibly using contrast medium. Both conditions are amenable to successful excisional surgery.
Laryngeal abnormalitiesCompromised glottic protection leading to the aspiration of ingesta into the lower airways may arise spontaneously in cases of arytenoid chondropathy, or through iatrogenic causes such as complications of prosthetic laryngoplasty or partial arytenoidectomy (see 5.20). The precise cause of post-laryngoplasty dysphagia is not known, but over-abduction of the arytenoid cartilage, the physical presence of the implants themselves and nerve injuries are amongst the suggestions which have been proposed. Removal of the prosthesis is often, but not always, effective in control of the dysphagia, but, of course, the respiratory obstruction for which the surgery was originally performed can be expected to return as the arytenoid cartilage reverts to its col-lapsed state.
Fourth branchial arch defects (4-BAD)Approximately two thoroughbreds per thousand born are afflicted with defects of the structures which derive from the fourth branchial arch, specifically the wings of the thyroid cartilage, the crico-thyroid articulation, the crico-thyroideus muscle and the crico- and thyro-pharyngeus muscles (see 5.25). The fourth branchial arch defect (4-BAD) syndrome may arise unilaterally or bilaterally, and any or all of the structures may show partial or complete aplasia. When the 4-BAD syndrome includes aplasia or hypoplasia of the crico- and thyro-pharyngeal muscles the proximal oesophageal sphincter remains permanently open. Horses afflicted with 4-BAD usually present with abnormal respiratory noises at exercise, and it is most unusual for them to show dysphagia unless they are badly afflicted or there is another concurrent defect. Horses with 4-BAD may show bizarre eructation-like noises at rest and may be confused with wind-suckers.
Figure1.4 Sub-epiglottal cyst in a foal. Note that in this case there is no associated entrapment of the epiglottis by the glosso-epiglottal mucosa.
7ChapterUpper alimentary system | 1 |
antibiotic cover during the immediate post-traumatic period should be routine.Most palpable bone fragments, or those seen on radiographs, retain
periosteal or endosteal attachments and heal uneventfully, but occa-sionally devitalization leads to sequestration with a discharge to the nose or skin surface. These should be dealt with by surgical removal as they arise.Grossly deforming depression fractures should be treated by eleva-
tion as soon as possible after the trauma otherwise a fibrous union will form in a matter of days.Molar and premolar involvement in upper or lower jaw fractures is
best managed on a wait-and-see basis because generally it will not be possible to determine whether or not a tooth is devitalized in the acute phase, and, in any event, the procedure of dental extraction will simply exacerbate the original trauma.Fractures of the incisor quadrants can be repaired effectively by
in-and-out wire fixation of the loosened teeth to secure neighbours and/or to the mandible or premaxilla. Alternatively, the canine teeth can be used to anchor the fixation wires.
PrognosisIn general terms the outlook for horses which sustain traumatic inju-ries to the jaws is favourable because there is often little displacement of bone in cases of fracture, and the devitalization of soft tissue and teeth is limited.
1.7 OESOPHAGEAL OBSTRUCTION
AetiologyAcute obstruction of the oesophagus by impacted, dry ingesta (choke) is typically associated with the ingestion of inadequately soaked sugar beet pulp in the United Kingdom. Equivalent offending possibilities occur in other parts of the world. The dry fibrous mate-rial swells with the absorption of saliva and an expanding bolus occludes the oesophageal lumen. Subsequent boluses compound the obstruction.
Clinical signsHorses with choke present in an acutely distressed state with copious reflux, particularly of saliva, to the nostrils and mouth (Figure 1.1).
DiagnosisThe initial diagnostic challenge in cases of oesophageal obstruction is to differentiate this condition from other causes of acute dysphagia most notably pharyngeal paralysis.The cervical oesophagus may be palpably distended with firm
ingesta, and the passage of a nasogastric tube beyond the pharynx is generally not possible.Inhalation tracheitis is invariably present, and inhalation pneumo-
nia may follow if treatment is not promptly instituted.Endoscopy of the pharynx and ATDs may be helpful when the
case history convincingly rules out access to the common causes of obstruction.
TreatmentMany chokes can be relieved by heavy sedation, the repeated admin-istration of spasmolytics and prophylactic use of broad spectrum anti-microbials. This treatment can be continued for several hours or even days, but the distressed state of the patient and the likelihood of serious respiratory complications demand that conservative manage-ment should not be prolonged.
pulled apart. The sudden in-rush of air through the open crico-pharynx coincides with the gulping sound which is typically heard during attacks of wind-sucking, but the air is returned from the oesophagus to the pharynx immediately.
Grass sickness (See Chapter 3)Grass sickness produces dysphagia in its acute form but colic in the sub-acute and chronic forms. The condition is seen in horses of all ages throughout the United Kingdom and northern Europe. Afflicted horses are generally severely depressed with patchy sweating, elevated pulse and ileus. The dysphagia arises as a part of total gastro-intestinal stasis, and nasal reflux of ingesta adds to the pitiful appearance of the patients. There is currently no reliable in vitro diagnostic test, but the radiographic demonstration of oesophageal stasis and the endoscopic identification of ulceration of the oesophageal mucosa are helpful pointers to the likely diagnosis.
1.6 ORAL TRAUMA, MANDIBULAR FRACTURES ETC.
PathogenesisFractures of the teeth and jaws are not unusual and arise from falls, kicks by other horses and by bitting injuries and stick-and-ball trauma in polo. Fractures of the teeth themselves often lead to pulp exposure and devitalization and periapical suppuration. Restoration may be considered with early diagnosis but extraction becomes the preferred course for chronic cases.
Clinical signsIn many instances, particularly with horses at pasture, the traumatic incident is unwitnessed. Occasionally compound fractures of the mandible or maxilla are sustained with an obvious external wound. Horses with these injuries may present with sudden onset swellings of the facial and mandibular areas or inability to close the mouth with failure of effective prehension of ingesta and drooling of saliva. Neglected cases of oro-facial trauma may show external evidence of suppuration from devitalized tissue and weight loss from an inability to prehend and masticate food.
DiagnosisFractures of the mandibular rami should always be considered in cases of acute onset swelling of the jaw. External palpation, a judicious intra-oral examination and a careful radiographic investigation are used for damage assessment.
TreatmentFortunately, many fractures of the mandible and maxilla show little displacement of the bone fragments, and surgical fixation is often not necessary. However, teeth may be devitalized either by infection through the fracture line or by disruption of their vascular supply. The decision whether or not to extract depends on radiographic findings, but such surgery should be delayed at least until a firm fibrous union of the fracture site is present. At this time sequestra may also be located and removed.Open wounds over the sinuses may necessitate removal of
loose bone fragments and debridement of gross contamination. An implanted irrigation catheter can be a useful measure to flush away blood and debris and should always be used when the sinus wall has sustained a full thickness penetration. The provision of broad-spectrum
8Equine Medicine, Surgery and Reproduction
than the surrounding primary dentine and as it is exposed at the occlusal surface it becomes stained by oxidized plant material creating the dental star which lies labially to the infundibulum. Continued attrition at the occlusal surface reaches the base of the infundibulum made solely of enamel and is termed the enamel mark. Eventually the enamel is worn away completely and the dental star takes a more central position within the occlusal surface which now has a more triangular appearance.The adult incisors are all preceded by deciduous dentition, which
is lost at approximately 2.5 years for the central incisors, 3.5 years for the middle incisors and 4.5 years for the corner incisors. The decidu-ous incisors are smaller in appearance to their permanent counterparts and viewed from rostrally have a semicircular shape in contrast to the more rhomboid or oblong shape of the permanent dentition. At birth the central incisors are erupting, and usually present within the first week of life. The deciduous middle incisors erupt at approxi-mately 6 weeks of age, with the corner incisors appearing around 6 months of age.The canine teeth, sometimes referred to as tushes, are most com-
monly seen in stallions or geldings. The upper and lower canine teeth erupt from the premaxilla and mandible respectively. They may be present in mares as well, although are often vestigial, unerupted and/or variable in number. The canine teeth are said to erupt around five to six years of age, although this can be extremely variable.The incisors and canines are separated from the remaining dental
arcades by the interdental space. This is often misnamed as the diastema a term which refers to a pathological condition often responsible for periodontal disease. In some horses, wolf teeth are found within the interdental space. These vestigial first premolar teeth are found most commonly in the maxillary arcades, lying rostral to the first cheek teeth. These teeth are commonly blamed for riding or bitting problems; however, in many cases it is hard to attribute the clinical signs shown to their presence. More commonly other patho-logical conditions of the oral cavity can explain the clinical signs shown and, therefore, removal of the wolf teeth, which lie just lateral to the palatine artery, is not always indicated.The cheek teeth lie within the caudal oral cavity, comprising two
upper and two lower batteries of teeth. The cheek teeth can be subdi-vided into premolars, the first three teeth in each battery, and molars, the last three teeth in each battery. The premolars of the horse are unique in that they are molarized and as such are morphologically identical to the molar teeth. The teeth have a hypsodont confor-mation, divided into three regions, the visible clinical crown, a sub-gingival reserve crown and an apical region. As these teeth erupt they are angled in such a way as to move towards each other creating a tight junction between adjacent teeth, in a process known as mesial drift. The premolar teeth each have a deciduous precursor which erupt in the first 7 days of life and are shed at approximately 212 years, 3 years and 4 years for the 2nd, 3rd and 4th premolars respectively. The molar teeth have no deciduous precursors, and erupt at 1 year, 2 years and 312 years for the 1st, 2nd and 3rd molars. The eruption of the molars corresponds with lengthening of the head as the horse grows.The cheek teeth are continually wearing down due the presence of
abrasive silicates within the diet. The relative hardness of the different dental tissues results in a naturally roughened surface which is impor-tant in mastication. The enamel, though brittle, is slightly harder than the surrounding cementum and dentine resulting in small ridges over the surface of the tooth. The mandibular teeth are oblong in shape and have a single enamel ridge with marked folding creating a millstone-like surface. The maxillary are square in shape and have two infundibulae creating an enamel ridge around the periphery of the tooth and two small enamel rings in the centre of the tooth. The centre of these two smaller enamel rings contains cementum which is often hypoplastic, and may predispose to caries (see dental caries later).
If conservative therapy fails to relieve the obstruction after 24 hours, most clinicians advocate lavage under sedation or general anaesthesia.The authors preference is to institute vigorous lavage, under anaes-
thesia, by stirrup pump through a nasogastric tube. Obviously the patients trachea should be intubated, and the head is positioned over a supporting bag with the nose inclined downwards. In this way the impacted ingesta is progressively washed back out at the nostrils.Other clinicians prefer to attempt relief using a similar lavage tech-
nique with the patient standing but sedated. It is important that the horses head and neck are maintained in a lowered position during the procedure to prevent aspiration of food and lavage fluid. Excessive pressure on the oesophageal lavage must be avoided.
PrognosisThe prognosis for a complete recovery after the relief of an oesopha-geal obstruction is good. The possibility of recurrence of the choke or of long-term stricture development can be reduced by withholding dry fibrous foods for at least 72 hours as oesophageal motility is likely to remain weak for several days. Instead, wet sloppy foods, mashes and fresh grass should be fed. Oesophageal motility is likely to remain weak for several days. The inhalational tracheitis or bronchitis is usually self-limiting, but broad-spectrum antibiotic cover should be maintained for 710 days.
1.8 ANATOMY OF THE ORAL CAVITY
Oral cavityThe oral cavity of the horse forms the first part of the alimentary tract. The horse is an obligate nasal breather so the oral cavity takes no part in respiration in contrast to many other species. The role of the oral cavity is to prehend food, particularly forage, and processes this into a form that allows for efficient digestion in the hind gut. This is dif-ferent to the digestive process in ruminants, which allows for repeated cycles of mastication and digestion via regurgitation of partially digested boluses of food in a process known as rumination. In horses, the processing of food occurs in one attempt and has resulted in development of a specialized hypsodont dental anatomy. This feature of equine dental anatomy and function should always be borne in mind when carrying out corrective dental procedures that may adversely affect the masticatory function of the oral cavity as they may, indirectly, have a significant effect on the function of the entire diges-tive tract. The teeth are comprised of three main types of hard dental tissue, cementum, enamel and dentine (divided into primary and secondary type) which are exposed at the occlusal surface with wear (Figure 1.5a, b & c).
Normal dental anatomyThe dentition of the adult horse comprises six upper and lower inci-sors set within the premaxilla and mandible respectively. The teeth have a hypsodont conformation, divided into three regions, the visible clinical crown, a sub-gingival reserve crown and an apical region. These teeth function as a unit whose primary role is prehension of food. The anatomy of the incisors, and its change with age, has histori-cally been used as a guide to ageing the horses. The enamel infolds on the erupting crown creating an infundibulum which is filled with cementum. As the teeth come into wear this becomes isolated, forming the dental cup. The teeth at this stage are said to have an oval shape to the occlusal surface. As wear continues the pulp cavity lays down a protective tissue known as secondary dentine. This is more porous
9ChapterUpper alimentary system | 1 |
Figure1.5 (a) Occlusal surface of the equine incisor showing the presence of the central infundibulum filled with cementum and, just rostral, the dark stained dental star. (b) Occlusal surface of the equine mandibular cheek tooth note the lack of infundibulae. (c) Occlusal surface of the equine maxillary cheek tooth showing the two central infundibulae filled with cementum. C = cementum, E = enamel, P = primary dentine, S = secondary dentine.
a b
c
The overall contour of the occlusal surface of each tooth is not flat but contains a pair of transverse ridges which interdigitate with the opposing arcade to increase the surface area of the arcades. The height of these ridges varies between individual horses. Individually enlarged ridges, more appropriately termed transverse overgrowths, may arise opposing diastema (see 1.10) and should be reduced to prevent further food impaction between the opposing teeth.The pulp is the central vascular tissue surrounded by the hard tissues
of the tooth. The pulp is responsible for the innervation of the tooth as well as for the production of dentine. The odontoblast cells form the outermost layer of the pulp and are intrinsically linked to the dentine by means of odontoblast processes. It is believed that wear on the occlusal surface stimulates the odontoblasts via their processes which are responsible for the production of secondary dentine. The pulp anatomy of the incisors and canines are relatively similar with a single common pulp chamber. The pulp chamber is more complex in the cheek teeth with a common pulp chamber at the apex of the tooth in the young horse and five pulp horns separated by primary dentine extending towards the occlusal surface. In the most rostral
cheek tooth in each arcade an extra pulp horn is present on the rostral margin, and in the most caudal cheek tooth in each arcade an extra one or two pulp horns are present at the caudal aspect. Awareness of the location of these is essential when performing reductions of over-growths and also in identifying pathology affecting the pulp canal. The occlusal extremity of each pulp horn can be recognized as a dark stained area due to the porous nature of secondary dentine which uptakes food particles. These subsequently oxidize, creating a brown stain on the tooth surface.
Triadan systemIn equine dentistry it is essential that all practitioners use the same terminology when discussing diseases affecting the teeth. The length of name required to identify an individual tooth, as well as the confu-sion that arises from the cheek teeth being made up of both premolars and molars, has led to the establishment of a system of nomenclature adapted from human and small-animal dentistry. This is termed the
10
Equine Medicine, Surgery and Reproduction
eruption of the cheek teeth results in formation of an overgrowth. The reasons for overgrowth should always be ascertained. The overgrown tooth is seldom abnormal and is merely a normal erupting tooth that isnt being worn down. Evaluation of the arcade opposing the over-growth will often reveal the underlying pathology. Common causes include: missing teeth, malerupted teeth, fractured teeth, overall dis-parity in the apposition of the arcades, e.g. parrot mouth and diastem-ata. The shape and size of the overgrowth will be dictated by the nature of the abnormal wear. Large overgrowths if left untreated can result in soft-tissue trauma, tooth displacements and diastemata.Wear disorders may also arise due to lack of normal lateral move-
ment of the mandible during mastication. The most common causes are painful conditions of the oral cavity, such as diastemata, which result in a reduction in the lateral excursion of the opening phase of mastication. This, in turn, results in a lack of wear on the buccal aspect of the maxillary arcades and lingual aspect of the mandibular arcades. In time, the occlusal angle of the entire upper and lower arcades of teeth on the affected side steepens, a condition known as shear mouth.
Clinical signsClinical signs vary considerably between cases. Many cases are clini-cally silent. Eating problems, such as spilling hard feed, are often unnoticed by the owner. Large overgrowths resulting in significant soft-tissue trauma may cause quidding of forage. Riding problems may also be noticed, particularly in horses expected to work in an outline.In cases with shear mouth, the problems of mastication giving rise
to the wear disorder may be apparent in the form of quidding. In cases where quidding is not seen, careful observation may reveal mastica-tion occurring only on the unaffected side.
DiagnosisDiagnosis relies on a thorough clinical examination. Examination of the oral cavity by palpation and visual inspection and a good awareness of normal anatomy should quickly identify overgrowths. Care should be taken to avoid misinterpreting normal anatomical features such as transverse ridging and ventral curvature of the mandible (curve of spee) as overgrowths requiring correction. Iden-tification of shear mouth relies on awareness of the normal angle of occlusion, which varies between individuals and throughout each arcade. Recognition of the primary pathology which has resulted in the overgrowth or shear mouth should also be completed.
Treatment and preventionTreatment of sharp points consists of rounding the buccal aspect of the maxillary arcades and lingual aspect of the mandibular arcades. This can be accomplished using a range of hand rasps or motorized instruments. Care should be taken not to remove excessive width from the teeth being rasped by ensuring that the instruments are kept between 45 and 60 degrees and only the sharp points are removed and rounded.Overgrowths of the occlusal surface require careful assessment.
Reduction is often most easily accomplished using motorized instru-ments. These allow precise reduction of overgrowths on the tooth surface that would be impossible with hand instruments. It should be remembered that teeth are living anatomical structures. A large pro-portion of the occlusal surface is made of dentine (both primary and secondary) which is intimately connected to the pulp and, therefore, should be considered as a living tissue. Motorized instruments, if used, should feature continuous water cooling to prevent thermal trauma to the pulpal tissues. Reduction should be performed visually using a headlight to illuminate the mouth, with particular attention paid to the dark stained secondary dentine on the occlusal surface.
modified Triadan system and has become the standard used by prac-titioners working in the field of equine dentistry. The numbering system assigns a three-digit code which can be used to identify any normal tooth found in the equine mouth, and comprises two parts. The first digit denotes the arcade number, and the next two digits the tooth number.When viewed from rostrally, each quadrant in the adult horse is
assigned a number, starting at 1 for the upper right moving clockwise assigning the next number to each arcade in turn. Thus, quadrant 2 is the upper left, quadrant 3 the lower left and quadrant 4 the lower right. This is used for adult permanent dentition. For the deciduous dentition, the quadrant numbering starts at 5 for the upper right and moves round sequentially as for the permanent dentition so that quadrant 8 would be the lower right deciduous quadrant.The teeth are then numbered sequentially starting from the central
incisor, which is assigned 01, moving distally assigning a new number for each tooth that might be present. Thus, the incisors are 01 to 03; the canines are 04; the wolf teeth 05; the premolars 06 to 08 and the molars 09 to 11. This can be seen on the dental chart (Figure 1.6). It should be noted that extra numbers are not assigned for supernumary teeth, the extra tooth is merely noted as a supernumary and assigned the number of the adjacent normal tooth, e.g. a supernumary tooth at the caudal aspect of the upper right maxillary arcade would be a supernumary 111, not a 112. Likewise, numbers are not removed for absent teeth, e.g. a mare with no canines or wolf teeth will not start its cheek teeth arcades with 04s.
Eruption of teethThe teeth of equidae are unique in their hypsodont from, which has arisen due to their diet. The abrasive nature of their diet results in wear on the occlusal surface. In order to compensate for this wear the teeth continually erupt. The rate of eruption varies with age; in younger individuals it is more rapid it may be up to 10 mm per year. As the horse gets older the eruption rate slows down; a horse over 20 may erupt their teeth at only 1 mm per year. The eruption rate, in balance with the rate of wear, ultimately determines how quickly wear disor-ders will arise when mouths are left untreated, and also how quickly occlusion will be re-established following corrective procedures.
1.9 ABNOMALITIES OF WEAR ABRASION AND ATTRITION
Abnormalities of wear are the most common dental pathology encountered by the equine veterinary surgeon. They include minor sharp points through to large unopposed overgrowths.
PathogenesisWear disorders include problems of both insufficient and excessive attrition of the teeth. The most simple wear disorders are the produc-tion of sharp buccal points on the maxillary cheek teeth and sharp lingual points on the mandibular cheek teeth. They arise due to lack of attrition on these edges when horses feed on diets which are more easily masticated. The maxillary arcades are set wider apart than the mandibular arcades, and the reduced lateral movement associated with most domestic horses diets results in a lack of wear on the afore-mentioned edges. These sharp points can lead to abrasion and ulcera-tion of the cheeks and tongue. This causes discomfort during eating which results in further reduction of the lateral movement of the jaw.Most wear disorders of concern arise from a lack of attrition of the
occlusal surface. The lack of wear combined with the continued
11
ChapterUpper alimentary system | 1 |
Figure1.6 Dental chart using the Triadan system, with kind permission of the Bell Equine Clinic.
12
Equine Medicine, Surgery and Reproduction
cases quidding forage is incorrectly attributed to sharp enamel points, a rare cause of dysphagia of forage. The relationship of diastemata to dental overgrowths and displacements should not be overlooked when examining the oral cavity. Caudal overgrowths on the last man-dibular cheek teeth are commonly associated with diastemata due to caudal displacement of the overgrown teeth, widening of the inter-proximal space and impaction of food compounded by development of opposing transverse overgrowths. As such, the primary pathology, as well as the secondary, needs to be addressed.
TreatmentFollowing detailed examination and accurate diagnosis, the food impacted around the interproximal space needs to be removed. This is usually accomplished by careful use of a combination of fine dental picks and lavage using low pressure water picks, or three-way syringes found on some dental machines. Care should be taken to avoid causing more damage to the periodontium. High-pressure, air abra-sion units, in particular, must be used with great care to avoid forcing food material deeper into the periodontal tissues.Once the impacted food has been removed, further assessment of
the interproximal space is required. The depth of periodontal pockets should be assessed using fine periodontal probes, again ensuring care is taken not to cause further damage to the periodontium. The degree of gingival recession should also be noted which will reduce the measured depth of periodontal pockets. Radiography, using either intraoral or open-mouth oblique views, should be used to assess the loss of interproximal bone and also to assess the interproximal con-formation. The periodontal pocket should be cleaned to remove any necrotic tissue and the interproximal tooth surfaces debrided using hand scalers and/or high-speed burrs where necessary.In some cases, removal of the impacted feed and necrotic tissue
from the periodontal pocket and correction of the related dental malocclusions are sufficient alone to resolve the clinical condition.If the interproximal conformation, assessed using clinical examina-
tion and radiography, is such that the space between adjacent teeth is narrower at the occlusal surface than at the gingival margin a diagnosis of valve diastema can be made. In these cases widening of the inter-proximal space at the occlusal surface using a fine right-angled burr may be indicated. The aim is to prevent food trapping between the
This thin layer of porous dentine lies over the pulp horns of the tooth, and as the overgrowth is reduced the protection of the pulp is removed. Monitoring the change in colour of the secondary dentine, as the superficial stained layer is removed, gives a guide to the location of the pulp horns, and once the stained layer is completely removed, further reduction should be avoided. When reducing an overgrowth it should be done in a manner to maintain the normal lateromedial angulation of the occlusal arcades.In cases with shear mouth, correction can present a significant chal-
lenge. Initially, treatment of the underlying pathology is indicated. In mild cases this may be sufficient for normal mastication to resume which, in turn, will result in more normal wear forces. In more severe cases it should be remembered that the pathology has taken many months, and in most cases years, to arise. As such the chewing motion and musculature is adapted to the abnormal masticatory action, so corrections should be done gradually. Correction should begin by addressing the normal sharp buccal and lingual points, followed by reduction of the highest side of the arcade being treated. Attempts to re-establish normal occlusal angle starting from the lower side of the tooth should be avoided as this area is excessively worn, and would result in excessive removal of clinical crown.
PrognosisThe prognosis for most overgrowth corrections is good. Excessive removal of occlusal surface or heating of the tooth structure using uncooled instruments can result in post-procedure quidding, either through dentine sensitivity, lack of differential wear or lack of occlu-sion between opposing arcades. These can take many months or years to resolve, and in geriatric patients may never fully recover so care should be taken to identify these risks and ensure procedures are done in an appropriate manner.
1.10 PERIODONTAL DISEASE
PathogenesisPeriodontal disease is defined as pathology affecting the periodontal ligament and associated structures. In comparison to man, plaque retention is not believed to be as important an initiating factor as food stasis. Most periodontal disease arises as the result of food stasis in the region of the interproximal spaces between cheek teeth or inci-sors, and is often associated with pathological spaces occurring between the teeth, known as diastema. Food accumulation in the spaces results in a localized periodontal disease (Figure 1.7). Localized periodontal disease may arise with lower canine teeth in association with tartar accumulation.
Clinical signsIn many instances mild periodontal disease appears clinically silent, with localized diastemata not being immediately apparent without detailed oral examination under sedation, aided by use of a dental mirror and/or dental endoscope. In more severe cases, the predomi-nant sign is oral phase dysphagia, particularly when masticating long-stem forage (quidding). This can be quite dramatic with large piles of partially masticated forage building up on the floor of the stable.
DiagnosisClinical cases presenting with signs of quidding forage should be sedated and receive a detailed oral examination using a bright head-light and dental mirror or an oral endoscope to establish a correct diagnosis. Diastemata between the caudal mandibular cheek teeth are easily missed on a cursory dental examination, and frequently in these
Figure1.7 Diastemata with localized periodontal disease between mandibular cheek teeth.
13
ChapterUpper alimentary system | 1 |
occurs at the alveolar crest and providing the ongoing disease process can be stopped it may be possible for the diseased peripheral cemen-tum to be replaced as the tooth erupts. Peripheral cemental caries may also be linked to periodontal disease, although at present it is unclear which disease is the initiating problem.
Clinical signsClinical signs vary between cases but often cases of dental caries are clinically silent. In some cases extensive peripheral caries on the caudal mandibular arcades can result in lingual ulceration which can cause hypersalivation or dysphagia although this is rare. Infundibular caries is almost always clinically silent until the point of fracture at which point sudden onset dysphagia can occur.
DiagnosisAccurate diagnosis relies upon a detailed oral examination. Food must be washed from the mouth using copious water or disinfectant solu-tion as a clear view of the tooth surfaces is required. The use of a dental mirror and bright headlamp is essential to recognize lesions within the caudal oral cavity, and in some instances an oral endoscope may be preferable. The diagnosis of dental caries is not solely made on the appearance of discoloration, although this is a helpful guide. The use of a dental explorer to assess the relative hardness of the tooth surfaces also aids diagnosis with active caries lesions being softened by the disease process. The extent of caries lesions should also be assessed. This is not always immediately apparent, especially in cases with infundibular disease. Radiographs, and, if available, computed tom-ography, may help in ascertaining the extent of involvement and depth of lesions. In cases where there is extension into the pulp canal the lesion is likely to result in apical infection and, as such, extraction of the tooth is likely to be required. Care should be taken to avoid confusion in young horses with recently erupted permanent dentition where the infundibulum has a very open shape, frequently confused as dental caries. Also, it is imperative that the practitioner understands the occlusal surface anatomy in detail to avoid confusion between infundibular caries (which initially involves cementum only) and secondary dentinal defects which can be the consequence of endo-dontic disease.
TreatmentA number of practitioners have tried to treat dental caries using restor-ative dentistry techniques adapted from human dentistry. It is essen-tial in cases where this treatment is being considered that the extent of the caries process is accurately known. The nature of many infundib-ular lesions is such that the disease process may not be completely apparent from the occlusal surface. This, in combination with the curved anatomy of the infundibulae and the depth from the occlusal surface of the active lesion in many cases, makes complete restoration of the lesion impossible.In those cases where restoration is considered suitable it is impor-
tant that owners are made aware that cases will require careful moni-toring. The initial process consists of debridement of the carious dental tissue using a combination of high- and low-speed dental handpieces and, in some cases, high-pressure air abrasion using alu-minium oxide powder. It should be remembered that the infundibu-lum is a central structure within the tooth and is surrounded by multiple pulp horns; therefore, debridement should be done carefully to avoid excessive removal of dental tissue and inadvertent pulp expo-sure. Following debridement, the cavity is lavaged and dried using a three-way syringe and then etched using phosphoric acid gel for 1020 seconds. This dissolves the inorganic calcium salts from the superficial layers of the cavity. The acid gel is removed by lavage and then air-dried briefly to remove the majority of the moisture. A bonding agent is then applied to the walls of the cavity and thinned using air
teeth; however, care should be taken to prevent inadvertent pulp exposure by excessive removal of dental tissue and thermal trauma by using a continuously irrigated instrument. In some cases, especially in the caudal oral cavity, it can be very difficult to ensure that the burr is accurately located within the interproximal space; the use of instru-ments with an adjustable head angle and assessment of the instru-ment placement with a dental mirror or endoscope are indicated.Once the periodontal pocket has been cleaned and any interproxi-
mal widening required has been completed, then periodontal pocket can be protected using polyvinylsiloxane impression material dis-pensed using an automix syringe over the top of the pocket. Some practitioners advocate the use of calcium sulphate (Plaster of Paris) within the base of the pocket to act as an osteoconductive material to promote regeneration of interproximal bone and/or antibiotic gel preparations as an aid to treat the bacterial infection associated with periodontal disease.
PrognosisThe prognosis for treatment of periodontal disease varies depending on the extent of the disease at time of treatment. Localized low-grade periodontal disease can often be effectively treated with conservative management and routine rasping and carries a good prognosis. Exten-sive periodontal disease with concurrent loss of bone in multiple locations can prove very frustrating to treat and carries a guarded to poor prognosis.
1.11 DENTAL CARIES
PathogenesisDental caries occurs as a result of acid erosion of the calcified dental tissues of the teeth. In the horse, this most commonly involves the cementum, either on the periphery of the tooth, so called peripheral caries, or within the infundibulae of the maxillary cheek teeth, termed infundibular caries. The exact pathogenesis is at present undetermined; however, it is believed to be similar to that found in other species, where oral bacteria metabolize simple carbohydrates in food to form acid which dissolves the inorganic salts from the cementum.It has been suggested that hypoplasia of the cementum found
within the infundibulae of maxillary cheek teeth, a common finding in anatomical studies, may predispose to food accumulation within the cavity and thereby allow the disease process to begin. The reasons for cemental hypoplasia are not clear. It has been proposed that early removal of deciduous caps may prematurely disrupt the blood supply to the infundibular cementum thereby causing cessation of cementum production, this doesnt explain why the most commonly affected teeth are the first maxillary molars, which have no deciduous precursors.The pathogenesis of peripheral caries is also poorly understood.
Low-grade pitting is commonly found; however, more extensive disease resulting in almost complete loss of peripheral cementum, predominantly affecting the mandibular molars, in some individuals often has no clear cause. Undoubtedly the make up of an individuals own dentition will have some bearing, but factors such as dietary carbohydrates and acids may also play an important role. The authors have observed cases where the excessive feeding of sugary sweets to horses on box rest or feeding a haylage has resulting in rapid onset of peripheral caries which has responded to removal of treats or altera-tion of the forage diet and resulting in cessation of the disease process; however in many cases there is no clear cause that can be identified. The peripheral cementum in the horse is a dynamic tissue integral to the periodontium. A dramatic increase in the thickness of cementum
14
Equine Medicine, Surgery and Reproduction
and in these cases, anaechoresis associated with dental eruption is a possible pathogenesis.
Clinical signsDental pain is rarely seen in cases of endodontic disease in horses. Occasionally the owner may notice a brief period of dysphagia associ-ated with initial onset of the disease, but in the absence of other clini-cal signs, this is rarely investigated if it resolves in a couple of days.Cheek teeth are most commonly affected by endodontic disease.
Clinical signs noted are mandibular swelling with the lower cheek teeth, maxillary swelling with the rostral upper cheek teeth, and uni-lateral purulent nasal discharge with caudal upper cheek teeth.
DiagnosisEarly diagnosis of endodontic disease is rare in the horse.Detailed oral examination using a bright headlamp, dental mirror
and dental explorer may find defects in the secondary dentine of the affected tooth. These arise due to the continual eruption of the teeth and attrition of the occlusal surface. In normal teeth the secondary dentine is laid down continuously by the odontoblasts within the pulp; however, with pulpitis the odontoblasts are impaired, so that production of secondary dentine is insufficient to compensate for occlusal surface wear.Radiography is the most commonly used diagnostic imaging
modality in equine dentistry. Changes associated with endodontic disease include disruption of the lamina dura denta, periapical scle-rosis and blunting of the dental apices. Where a draining tract is present it may be possible to gain further information by placing a probe within the tract during radiography. In many cases though, dental radiographs are hard to interpret, making early diagnosis dif-ficult. It may be necessary to repeat radiographs over several weeks to assess changes around teeth and avoid misdiagnosis.Computed tomography allows more detailed imaging of the teeth
and associated structures, without the problems associated with super-imposition. Until recently this required general anaesthesia of the patient; recently developed techniques now allow CT to to be used to image the head of horses with the horse sedated and standing.
TreatmentTreatment of teeth with endodontic disease primarily consists of extraction of the affected tooth. The complex nature of the pulp canals of equine cheek teeth make endodontic therapy difficult, if not impos-sible. There have been many studies looking into the success rates of total root canal therapy in the horse, using a variety of different materi-als and techniques. Short-term success is often good, around 70%; however, the outcome in the medium to long term is usually poor, requiring extraction of the affected tooth. Recent advances in our understanding of the unique anatomy and physiology of equine cheek teeth have revealed why failure is so common. The apical and coronal seal is a common source of technique failure in brachydont teeth and with the continual wear and complex anatomy of the pulp canals in equine cheek teeth breaching of this seal is likely to occur in most cases.Early diagnosis of tooth fracture or recognition of iatrogenic pulp
exposure, may allow the use of pulp capping techniques, with or without partial pulpotomy to preserve the tooth; however, these techniques have yet to be evaluated with research to be scientifically evaluated.
PrognosisThe prognosis for individually affected teeth is poor as most will require extraction. The likelihood of complications occurring after extractions is very technique-dependent; however, the long-term outlook is good following tooth extraction.
followed by curing using a high-intensity blue light from a specially designed curing light. It should be remembered that infundibular lesions primarily involve cementum, which is different to human dentition, where caries involves enamel and dentine, which means that the bonding of dental materials is unproven in the horse. For this reason the use of combined etch and bonding materials has not been recommended. Following bonding, the cavity is then filled using restorative materials in thin layers applied to the individual walls of the cavity to build up the restoration. Following restoration, cases require careful monitoring. Once a restoration is in place, it can be difficult to assess whether caries is ongoing underneath the restora-tion. For this reason, follow-up examinations and radiography every 6 months are essential to prevent subsequent endodontic involvement.In those cases where the caries process has progressed to the point
of fracture (Figure 1.8) the only viable treatment option is extraction of the affected tooth.
PrognosisThe prognosis for horses with extensive caries lesions involving both infundibulae is guarded, with many cases resulting in sagittal fracture of the tooth. These cases require extraction of the affected tooth. The prognosis for horses with peripheral caries, for horses with mild to moderate infundibular caries, and for horses with caries where restora-tion has been attempted remains undetermined.
1.12 ENDODONTIC DISEASE INCLUDING DENTAL ABSCESSATION
PathogenesisEndodontic disease is defined as disease affecting the pulp and peri-apical tissues of the tooth. Once within the pulpal tissues, bacteria cause infection and ultimately necrosis of pulp. The pathogenesis varies between cases but includes extension of periodontal disease around the tooth to allow bacteria to affect the apical region, exten-sion of dental caries from the cementum, through the enamel and dentine into the pulp canal, dental fracture and, less commonly, max-illary or mandibular fracture. In many cases the exact cause is unclear,
Figure1.8 An extracted maxillary cheek tooth showing a sagittal fracture due to coalescing infundibular caries.
15
ChapterUpper alimentary system | 1 |
fibroma) occur predominantly in foals. In addition bone cysts may arise in the upper or lower jaws.
Clinical signsApart from swelling of the affected jaw, horses with non-dental tumours or cysts may show dysphagia with quidding if there is mechanical interference with mastication, or they may not accept the bit if the interdental space is involved. Expansive lesions of the maxilla may obstruct the flow through the nasolacrimal duct leading to an overflow of tears at the medial canthus.
DiagnosisIn the differential diagnosis of swellings of the mandible and maxilla, suppuration at the roots of the cheek teeth predominates, but bone cysts and non-dental neoplasms should be considered. An extensive firm swelling of either jaw of a foal represents an indication for further evaluation particularly by radiography. A definitive diagnosis requires histological confirmation.
TreatmentLocalized lesions may lend themselves to excision on similar lines to those described for odontogenic tumours (see 1.13). Bone cysts should be opened and drained before curettage of the lining. Small cysts may be packed with cancellous bone but larger defects are better packed with medicated gauze which is steadily withdrawn in the postoperative period.
PrognosisSimilar prognostic guidelines apply to these lesions as to odontogenic tumours.
1.14 DIAGNOSTIC APPROACH TO DENTAL DISORDERS
Ageing of horses by dentitionThe patterns of eruption and attritional wear of the incisor teeth can be used to estimate the age of horses. The age of horses up to 6 years of age can be determined with some confidence based on the sequence of eruption of the incisors, which is approximately 2.5 years for central incisors (01s), 3.5 years for the middle incisors (02s) and 4.5 years for the corner incisors (03s). Thereafter, the presence or absence of cups, marks and stars, the shape of the occlusal surfaces and the angle of occlusion, and the existence of Galvaynes groove can be used to provide clues upon which to base a guestimate. The variation in individual anatomy, wear rates, diet and the presence of cribbing may lead to a result which is in error by many years.The permanent cheek teeth also erupt in a constant sequence, 09s (~1
year), 10s (~2 years), 06s (~2.5 years), 07s (~3 years), 11s (~3.5 years) and 08s (~4 years). Thus, the 09s are the oldest teeth in each arcade, and on radiographs, have the shortest crown; the 08s are the last to erupt into the middle of the arcade and have the longest reserve crown.
Clinical signs of dental diseaseMany cases with findings of dental disease on oral examination have no clinically discernible signs of the disease from the outside. Spilling of hard feed can often be associated with sharp enamel points causing soft-tissue trauma; however, equally, it may simply be a habit in a particular horse. Riding abnormalities are commonly attributed to dental disease, and in many cases improvement seen following treat-ment can justify such assumptions; however, the significance of dental
1.13 TUMOURS OF THE UPPER ALIMENTARY TRACT
Odontogenic tumours
PathogenesisNeoplasia may arise from any of the dental tissues, including the cementum and periodontium, although odontomas and ameloblasto-mas, derived from dentine and enamel respectively, are more common. In general terms the greater the level of differentiation of the tumour tissues the more identifiable mineralized dental material will be present and the better the prospects of successful surgical extirpation. In contrast, poorly differentiated odontogenic tumours have no min-eralized elements and are extremely aggressive.
Clinical signsAlthough these tumours are rare in horses, the possibility of an odon-togenic tumour should be considered whenever an animal develops a localized swelling of either jaw, and particular suspicion should be raised when the patient is young, coinciding with the time of greatest activity by the primordial dental tissues. However, ameloblastomas are more prevalent in older horses.
DiagnosisA definitive diagnosis of odontogenic neoplasia can be made only after biopsy of the lesion, but histological interpretation is both dif-ficult and confusing. In addition, the result of the biopsy investigation may not be known until long after extirpation surgery has been per-formed because samples must undergo demineralization before they can be fixed. Thus, the major diagnostic challenge in the case of a horse presented with a swelling of either jaw is to differentiate between dental periapical infection, post-traumatic reaction including seques-tration, dental impaction, cysts and tumours not related to dental tissues (see 1.8) and odontogenic neoplasia.
TreatmentSome benign, well-differentiated lesions are amenable to surgical removal, but this may necessitate the use of an osteoplastic flap through the mandibular cortex or maxilla to expose and withdraw the tumour piecemeal. Postoperative radiographs are advisable to establish that all aberrant dental tissue has been removed. It may be necessary to close defects into the mouth with a sealant such as dental impression compound while closure by granulation takes place.
PrognosisSome odontogenic tumours are not amenable to surgical removal by virtue of their size or invasive nature, and euthanasia may be neces-sary. The surgical removal of a benign odontogenic lesion may neces-sitate the loss of a permanent tooth. Although the original lesion may cause considerable swelling, bony remodelling should improve the cosmetic result in the months which follow surgery.
Other tumours of the jaw
PathogenesisThe non-dental tumours of the mandible or maxilla include osteoma, osteosarcoma, ossifying fibroma, fibrous dysplasia and juvenile man-dibular ossifying fibroma. Horses in any age group may be afflicted by osteomas, and mature animals are more likely to be the subject of malignant bone tumours, but the other three tumours listed: (ossify-ing fibroma, fibrous dysplasia, and juvenile mandibular ossifying
16
Equine Medicine, Surgery and Reproduction
Placement of an oral speculum should be done with care. They are large heavy, usually metal, objects, and there is significant potential for injury to the practitioner and other personnel in close proximity. Care should be taken to maintain control of both the horse and the speculum during its placement and use. A handler who can aid restraint is often useful, but in many cases sedation will be required. The use of a twitch is contraindicated due to the proximity of this to the practitioner performing an examination. The incisor plates of the speculum need to be securely located on the incisor teeth. In cases with incisor malocclusions, such as parrot mouth, the use of specially designed plates which can rest on the bars of the mouth may be neces-sary. These can cause severe injury to the bars if the horse chews so sedation is usually required. It is important to ensure that once in place the poll strap is done up securely, centred, and the speculum is opened gradually ensuring that each side is opened equally to prevent excessive stresses on either the horses temporomandibular joint or the speculum itself.Once the speculum is placed and open, a brief manual examination
will reveal major pathology and location of food within the mouth. It is sensible for protection of the practitioners hands and prevention of disease transmission that thin nitrile examination gloves are worn for examination. Following initial examination the mouth should be rinsed using a large flushing syringe to remove all loose food from the mouth.Palpation of the mouth should be done in a methodical manner,
paying attention to the occlusal, buccal and lingual/palatal aspects of each arcade in turn. The soft tissues adjacent to each of these areas should also be palpated. Palpation should be followed up with a visual examination using a bright head light (Figure 1.9). The use of a rigid dental mirror can aid clear visualization of the anatomy of the caudal oral cavity, and is essential for accurate assessment of lesions of the occlusal surface such as caries or secondary dentinal defects and periodontal lesions within the interproximal spaces (Figure 1.10). Dental endoscopy can be useful for recognition and documentation of subtle lesions of the caudal aspect of the oral cavity as well as for documentation of cases, but the equipment can be expensive.
Radiography of teethRadiography is the most useful diagnostic tool for imaging teeth. The high contrast afforded by the teeth, bones and surrounding air spaces
disease in riding problems should not be overestimated or used to justify excessive or unnecessary treatments. In many cases the prob-lems are just as likely to be behavioural, rider performance or related to another non-dental disease.More significant signs that are likely to represent severe dental
disease include halitosis, oral phase dysphagia (particularly involving forage quidding), unilateral nasal discharge, facial or mandibular swelling and very occasionally, oesophageal obstruction.
Oral examinationA good oral examination is the key to accurate diagnosis of equine dental disease, and it should be done in an ordered manner. An oral examination is indicated as part of a routine health check at least every year, and in younger horses may be required every six months. It can often be included alongside vaccinations as part of a wider routine health check.The first part of any examination is taking an accurate history. This
will include details such as previous dental care history, reasons for examination (e.g. routine check-up, dysphagia, facial swelling), and age and breed of the horse. Much of this history will be taken over the phone so it is essential that individuals within a practice taking phone calls are briefed on the information required.Clinical examination is best performed in a systematic manner in
every case. This may vary between individual practitioners, but a routine of work should be established, which can then be applied in each case to achieve an accurate diagnosis and treatment plan. Initial examination of the horse should be done at a distance, noting demeanour and eating behaviour, as well as using this time to obtain further clinical details from the client.Once close examination of the horse begins, the horse should be
restrained with a headcollar and lead rope. Headcollars which feature adjustable nose bands are particularly useful as they can be adjusted during the course of the examination once a speculum is placed. A basic clinical examination to assess heart, lungs and body tempera-ture, as well as examining other systems for signs of disease, should be undertaken initially to avoid misdiagnosis of non-dental condi-tions. Examination of the head should start with examination of the external surfaces, looking for any swellings, facial symmetry, signs of nasal or ocular discharge, or lymph node enlargement. Nasal and oral malodour should be noted. Done carefully, this early examination can often calm a nervous horse and/or owner.After initial examination, the decision to use sedation can be made
depending on the response of the patient. It may be that the previous history from the owner has already indicated that this is required, due to the horses temperament or severity of clinical signs. The use of an alpha 2 agonist, such as detomidine or romifidine, in combination with an opioid, such as butorphanol, is most commonly used and will usually be sufficient. For prolonged examinations or procedures, then infusions of detomidine or romifidine can be administered using an intravenous catheter.Examination of the teeth begins with assessment of the incisors.
Their number, relative location to each other and any overgrowths should be noted. Teeth with extensive periodontal disease or fracture should be assessed carefully. Placement of a conventional speculum for examination of the cheek teeth may be contraindicated in cases where severe incisor disease is present and the speculum is likely to result in further tooth damage.Careful palpation of the interdental space prior to placing an oral
speculum can reveal information regarding the presence of canines and wolf teeth as well as bitting injuries. However, care should be taken as it can place the practitioners digits at risk of serious injury from being bitten. For this reason it is often preferable to undertake examination of this area using an oral speculum.
Figure1.9 Visual oral examination using a Millenium oral speculum and bright headlight.
17
ChapterUpper alimentary system | 1 |
rostro-caudally on the rostral aspect of the facial crest and collimated to include all the cheek teeth in the arcade. Care should be taken to avoid excessive dorsal or ventral angulation as well as ensuring that the beam is directed in a truly lateral plane. The use of higher kV and lower mAs will improve the contrast and aid in assessing the teeth and surrounding boney structures.Open-mouth oblique and intraoral radiography can be useful in
assessing the clinical crown in cases with caries or periodontal disease. In open-mouth obliques, the mouth is held open using a Butler gag, and the beam directed lateroventral-10-lateral for the maxillary arcades and laterodorsal-15-lateral for the mandibular arcades, and centred rostro-caudally on the rostral aspect of the facial crest and between the cheek teeth arcades. Intraoral radiography avoids the complications of superimposition; however, the need for specialist cassettes and, in the case of computed radiography, specific equip-ment, has prevented its widespread use.
Other ancillary diagnostic techniquesUltrasonography, due to the poor sound transmission of bone, is of limited direct use in equine dentistry. In some cases it may be useful to identify anatomical features, such as blood vessels, prior to surgery.Endoscopy of the nasal cavities, pharynx and sinuses (through a
small sinusotomy) can allow visual inspection of the associated struc-tures of the head and can prove useful in identifying pathology related to dental disease or in ruling out non-dental diagnoses.Computed tomography can generate extremely useful diagnostic
images of the equine head. By producing a series of cross sectional images of the head, the superimposition problems associated with conventional radiography are eliminated. Recently, it has become pos-sible to undertake computed tomography of the head in the standing horse, and this has the potential to revolutionize our understanding of dental disease.
Indications for dental extractionIndications for dental extraction depend upon the type of tooth to be extracted.Wolf teeth are the most commonly extracted teeth, and are often
removed in young horses to prevent problems associated with bitting.
makes imaging easy to accomplish using portable X-ray generators. The use of computed or direct digital radiography has greatly enhanced the quality of image possible in practice and have reduced the need for repeat exposures; however, it is important that the practitioner is experienced in taking the views that are required to assess the teeth and surrounding structures. Due to the hidden nature of the dentition when viewing the skull externally, orientation can be difficult, result-ing in poor quality or non-diagnostic images. Due to the relatively long exposures taken in radiography it is essential that movement of the subject is prevented. The use of sedatives, rope halters and, in some instances, head supports can greatly aid in steadying the head to achieve high-quality images.Radiography of the incisors is best done using an intraoral view.
The horse will need to be sedated heavily to prevent chewing whilst the cassette, protected in a plastic bag, is inserted diagonally between the incisor arcades and pushed caudally into the interdental space. Care should be taken not to allow the cassette to come between the cheek teeth. The angle of the X-ray beam will depend on the age of the horse, but rostral angulation of approximately 45 degrees to the cassette will achieve satisfactory images in most cases. The beam should be centred on the tooth of interest, although in cases where this is not clear, initial views centred on midline should be taken. These views, if the cassette is placed far enough caudally, can also be used to assess the canine teeth.Latero-lateral radiography is useful for imaging the sinuses but
seldom useful for imaging the teeth where superimposition obscures the apices and crowns. To image the sinuses, using a low kV and higher mAs provides reduced contrast necessary to assess pathology of soft-tissue dens
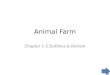

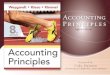

![Chapter 1: Getting Started with Alteryx · Chapter 1 [ 42 ] Chapter 4: Writing Fast and Accurate. Chapter 1 [ 43 ] Chapter 1 [ 44 ]](https://img.dokumen.tips/doc/110x75/5e903c60f316447eb43c0e7a/chapter-1-getting-started-with-alteryx-chapter-1-42-chapter-4-writing-fast.jpg)
























