Embed Size (px)
Citation preview

Changing Lives Changing Times,The Development of the Social Model:The Thinking that made the Difference
Richard RieserCoordinator UK Disability History
Month [email protected]

UNITED NATIONS CONVENTION ON THE RIGHTS OF PEOPLE WITH DISABILITIES DEC. 2006:A NEW PARADIGM CENTERED ON THE PERSON WITH
DISABILITY
To
From Medical Model of Disability Problem in the Person.Cure, Fix or Separate
To Social Model of Disability based on Human Rights approach- Problem with Society that needs to be changed.AttitudesOrganisationEnvironment
155 signatories to the Convention115 ratifications of the ConventionOptional Protocol90 signatories65 ratifications
Shifting the Focus in UNCRPD
• “Recognizing that disability is an evolving concept and that disability results from the interaction of persons with impairments and attitudinal and environmental barriers that hinders their full and effective participation in society on an equal basis with others.”
• Move from a dominant medical model to a social model approach- European Disability Strategy 2010
• http://www.un.org/disabilities/

Traditional views• Disabled people were evil or the
‘spawn of the devil’• Disabled people were not human• Disabled people were sinners• Disabled people were the way they
were because they, or their parents, had done something wrong
• Disabled people needed pity or charity• Disabled people were objects of fun or
the butt of jokes• Disabled people were unworthy of life• Disabled people were asexual and
incapable of relationships or perpetual children
• Disabled people were mendicants or liars to get ‘our’ sympathy and money
For thousands of years, in different cultures, all around the world, people believed that disabled people’s impairments -loss of bodily or mental function -was due to a wide range of inferred causes. These views were backed up by beliefs in myth, magic and religion that a powerful and negative impact on our lives.

Beginnings of the Medical Model
• To distinguish between the worthy poor and unworthy poor in the workhouse.
• Distinguish those with genuine loss of bodily or mental function and those who did not
• Went on to the view that disabled people could rehabilitate and make normal
• Incurables-Eugenics view keep in institutions• Linked with growth of Charity


Medical model 1900s
Bodies and minds to be fixed/cured
Roots: professionalism
Problem: individual and lack of function/ways we are not viewed as ‘normal’
Solution: rehabilitation, drugs, therapy by professionals who ‘know what’s best’, hospitalised, locked away.

Paul Hunt writes to Guardian September 20th 1972
From this the Union of the Physically Impaired Against Segregation is Formed UPIAS -The Social Model is invented.
“I am proposing the formation of a consumer group to put forward, nationally, the views of actual and potential residents of these successors of the workhouse. We hope in particular, to formulate and publicise plans for alternative kinds of care.
I should be glad to hear from anyone who is interested to join or support this project-yours faithfully
Yours faithfully Paul Hunt”
Changing Lives Changing TimesThe Thinking that made the Difference
Edits ‘ Stigma’ 1966

“Disability is something imposed on top of our impairment by the way we are unnecessarily isolated and excluded from full participation in society.
Disabled people are therefore an oppressed group in society”
Union of Physically Impaired against Segregation
“It is of course a fact that we sometimes require skilled medical help to treat our physical impairments - operations, drugs andnursing care. We may also need therapists to help restore or maintain physical function, and to advise us on aids to independence and mobility. But the imposition of medical authority, and of a medical definition of our problems of living in society, have to be resisted strongly.”
UPIAS Principles 1974/76

“Impairment is the functional limitation within the individual caused by physical, mental or sensory impairment.
Disability is the loss or limitation of opportunities to take part in the normal life of the community on an equal level with others due to physical and social barriers” .
By 1981 The British Council of Disabled People is formed and Adopts distinction between impairments and disability

Social Model 1970s/1980s
Those with impairments disabled by society’s attitudes and barriers
roots: disabled activists and academics
Problem: social and attitudinal barriers, capitalism/corporatism
Solution: activism, policy change, independent user-led organisations active in leading challenges

Impacts • BCODP formed 1980• Disabled People International
adopt 1981• Disability Living Allowance• Motability• Independent Living Fund• Disability Discrimination Act 1995 (
passed on 17th attempt)• Section M Building Regulations• SEN and Disability Act 2001• Disability Amendment Act 2005• Life Chances Report Equality 2025• Equalities Act 2010 • UN CRPD

CHILD DEVELOPMENT TEAM SPECIALISTS
GPs
OCCUPATIONAL THERAPISTS
SPEECH THERAPISTS
BENEFITS AGENCY
DISABLED PEOPLE AS PASSIVE RECEIVERS OF SERVICES AIMED AT CURE OR MANAGEMENT
SHELTERED WORKSHOPS
DOCTORS
TRAINING CENTRES
SPECIAL SCHOOLS
EDUCATIONAL PSYCHOLOGISTS
SPECIAL TRANSPORT
SURGEONS
SOCIAL WORKERS
The dominant view is the Medical Model.

The Social Model of disablement focuses on the barriers
DISABLED PEOPLE AS ACTIVE FIGHTERS FOR EQUALITY WORKING IN PARTNERSHIP WITH ALLIES.
LACK OF USEFUL EDUCATION
INACCESSIBLE ENVIRONMENT
DE-VALUING
PREJUDICE
INACCESSIBLE INFORMATION
INACCESIBLE TRANSPORT
‘BELIEF’ IN THE MEDICAL MODEL
POVERTY
SEGREGATED SERVICES
DISCRIMINATION IN EMPLOYMENT

MEDICAL MODEL THINKING SOCIAL MODEL THINKING
Person is faulty Person is valued
Diagnosis Strengths and needs defined by self and others
Labelling/Deficit Identify barriers and develop solutions
Impairment becomes focus of attention
Outcome based programme designed
Assessment, monitoring, programmes of therapy
imposed
Resources are made available to ordinary services
Segregation and alternative services
Training for disabled people, parents and professionals
Ordinary needs put on hold Relationships nurtured
Re-entry if normal enough OR permanent exclusion
Diversity welcomed and person is included
Society remains unchanged Society evolves
Medical /Social Model thinking[1]
[1] Adapted from M. Mason 1994, R. Rieser 2000 http://www.worldofinclusion.com/res/altogether/AltogetherBetter.pdf

Thinking/Model
Characteristics Form of Education
1 Traditional DP a shame on family, guilt, ignorance. DP seen as of no value.
Excluded from education altogether.
2 Medical 1 Focus on what DP cannot do. Attempt to normalize or if cannot make to fit into things as they are keep them separate.
Segregation
Institutions/ hospitals
Special schools (with ‘expert’ special educators)3 Medical 2 Person can be supported by minor
adjustment and support, to function normally and minimize their impairment. Continuum of provision based on severity and type of impairment.
Integration in mainstream:-
a)At same location-in separate class/units
b)Socially in some activities e.g. meals, assembly or art.
c)In the class with support, but teaching & learning remain the same.
What you cannot do determines which form of education you receive.
Social Model Barriers Identified-solutions found to minimize them. Barriers of attitude, environment and organization are seen as what disables and are removed to maximize potential of all. DP welcomed . Relations are intentionally built. DP achieve their potential. Person centred approach.
Inclusive education- schools where all are welcomed and staff, parents and pupils value diversity and support is provided so all can be successful academically and socially. This requires reorganizing teaching, learning and assessment. Peer support is encouraged.
Focus on what you can do.
Types of thinking about disabled people and forms of education.

Segregation

Integration

Inclusion

EnvironmentOrganisation,
Teaching &Curriculum
School
Find Barriers and thenAfter film Solutions
Medical, Personal & Equipment Needs
Attitudes & Culture
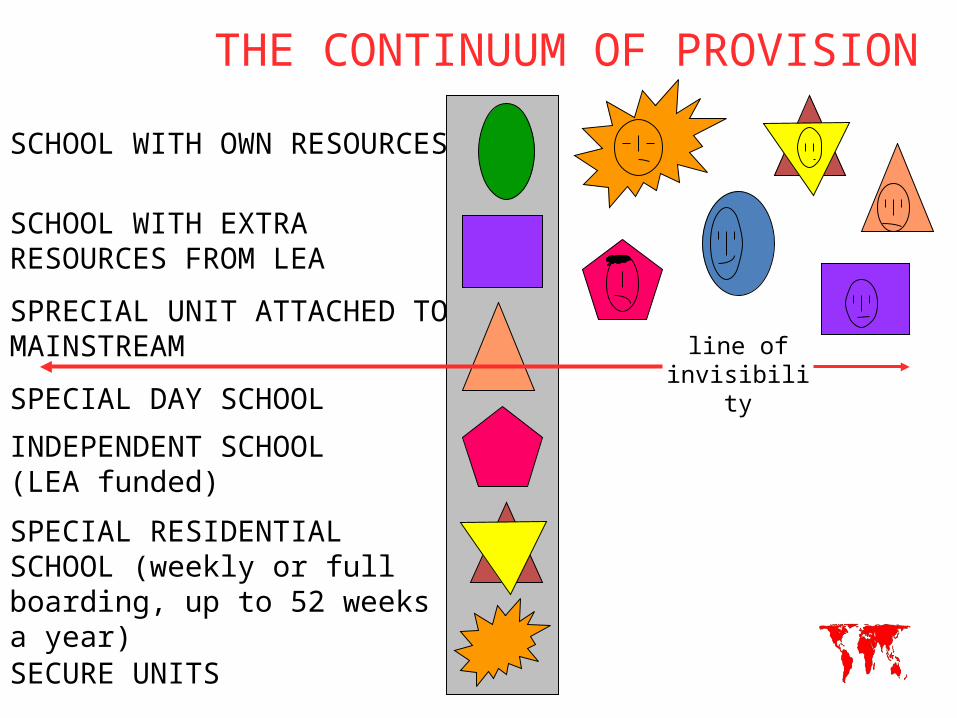
THE CONTINUUM OF PROVISION
SCHOOL WITH OWN RESOURCES
SCHOOL WITH EXTRA RESOURCES FROM LEA
SPRECIAL UNIT ATTACHED TO MAINSTREAM
SPECIAL DAY SCHOOL
INDEPENDENT SCHOOL (LEA funded)
SPECIAL RESIDENTIAL SCHOOL (weekly or full boarding, up to 52 weeks a year)
SECURE UNITS
line of invisibility

The Constellation of Services
CHILD
TEACHER
Transport Department
LearningSupport Assistant
Friends
Brothers and Sisters
Visually Impaired
service
Individual Support Teacher
SENCO Aids AdvisorVoluntary
Sector Specialists
Parents
Head teacher
Educational Psychologist
LEA Inclusion Officers
Physiotherapist
VolunteersSpeech
TherapistBehaviour
Support Team
Hearing Impaired
Service

Inclusive Education -UNESCO
Inclusive Education -UNESCO sees inclusive education as a process of addressing and responding to diversity of needs of all learners through increasing participation in learning, cultures and communities, and reducing exclusion within and from education. It involves changes and modifications in content, approaches, structures and strategies, with a common vision which covers all children of appropriate age range and a conviction that it is the responsibility of the regular system to educate all children.

Bio-psychosocial model 1990sDeveloping a ‘can do’
attitude, ‘work can set you free’
Roots: private insurance, corporatism, welfare reform/cuts
Problem: individual, welfare ‘dependency’, adopting a ‘sick role’
Solution: remove social/financial support, promote ‘work as therapy’ and bizarre ‘think yourself well’ mantras

Bio-psychosocial model 1990sDeveloping a ‘can do’
attitude, ‘work can set you free’
Roots: private insurance, corporatism, welfare reform/cuts
Problem: individual, welfare ‘dependency’, adopting a ‘sick role’
Solution: remove social/financial support, promote ‘work as therapy’ and bizarre ‘think yourself well’ mantras


The Struggle The Struggle for Equality for Equality ContinuesContinues





























