Embed Size (px)
Citation preview

Changes in Healthcare: It’s a good thingDr. Sean G. Boynes
Director of Interprofessional Practice

Disclosure: Dental Benefits for 23M People in 28 States

“Integrated” Has Many Meanings1. “Integrated” is frequently used to refer to a package of preventive and curative
health interventions for a particular population group – often (but not always) this group is distinguished by its stage in the life cycle.
2. “Integrated health service” can refer to multi-purpose service delivery points – a range of services for a catchment population is provided at one location and under one overall manager.
3. “Integrated services” to some means achieving continuity of care over time.
4. Integration can also refer to the vertical integration of different levels of service – for example a regional hospital, health centers and private practice
5. Integration can also refer to integrated policy-making and management which is organized to bring together decisions and support functions across different parts of the health service
6. Integration can mean working across sectors.
• In countries dominated by health insurance, integration can mean that the insurance function and health care provision are provided by the same organization.
Source: World Health Organization, Technical Brief No. 1, 2008. Integrated Health Services – What and Why?

Dental
Behavioral
PharmacySocial
Services
LabSurgical
& Specialty
Care
Imaging
Physical Therapy
Primary Care
Key Attributes of Integrated Care
• Centered in primary care - PCMH
• Informed & involved patient
• Comprehensive treatment plan for total health
• Sharing data
• Coordination of care
• Effective communications

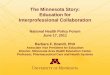
Background Information: Driving Change

Health Care Cost Crisis
H1965
H1967
H1969
H1971
H1973
H1975
H1977
H1979
H1981
H1983
H1985
H1987
H1989
H1991
H1993
H1995
H1997
H1999
H2001
H2003
H2005
H2007
H2009
H2011
P2013
P2015
P2017
P2019
P2021$0
$250
$500
$750
$1,000
$1,250
$1,500
$1,750
$2,000
$2,250
$2,500
$2,750
0.0%
2.5%
5.0%
7.5%
10.0%
12.5%
15.0%
17.5%
20.0%
22.5%
25.0%
27.5%
H1970; 7.0%H1980; 8.9%
H1990; 12.1%H2000; 13.4%
H2011; 16.8%
P2022; 24.9%
Government Entitlements Other Benefit Programs Out-of- PocketHealthcare as Percent of GDP
Expe
ndit
ures
(Mill
ions
)
Perc
ent
of G
DP
H = HistoricalP = Projected
National Health Expenditure Survey Historical and Projection Data
Government 104%Private Payers 81%Consumers 49%

Consumer Price Index of Goods & Services

Top 5 Most Expensive Conditions
Source: Medical Expenditure Panel Survey (MEPS)
Dental CPI growing faster than others!

Declining Dental Care Use
Marko Vujicic, VP ADA
WHY?

Integrating Oral Health into Primary Care“It focuses on frontline primary care health professionals, specifically nurse practitioners, nurse midwives, physicians and physician assistants. These primary care practitioners are members of the existing delivery system who could incorporate oral health core clinical competencies into their existing scope of practice.”
“HRSA synthesized the following recommendations:
1. Apply oral health core clinical competencies within primary care practices to increase oral health care access for safety net populations in the United States. 2. Develop infrastructure that is interoperable, accessible across clinical settings, and enhances adoption of the oral health core clinical competencies. The defined, essential elements of the oral health core clinical competencies should be used to inform decision-making and measure health outcomes. 3. Modify payment policies to efficiently address costs of implementing oral health competencies and provide incentives to health care systems and practitioners. 4. Execute programs to develop and evaluate implementation strategies of the oral health core clinical competencies into primary care practice. “

NNOHA / IPOHCCC: Implementation of HRSA Competencies
http://www.nnoha.org/nnoha-content/uploads/2015/01/IPOHCCC-Users-Guide-Final_01-23-2015.pdf
NNOHA (2015)

NNOHA / IPOHCCC: Users Guide
• READINESS ASSESSMENT• Planning
– Establish Integration Team– Profit/Loss– Population Focus– Timeline
• Training• Health Information Systems• Clinical Care Systems
– Workflow– Methodology/Techniques– Referrals
NNOHA (2015)

Planning/Implementation: Levels of Integration



MORE CARE - DQICare Pathway Coordination of Care
• “Cross-Referral” or “Hand-off Process”• Responsibilities and Accountability
– Who is responsible for what?• Organize delivery of care options and determine pathways to
success• Primary, Secondary, and Tertiary Prevention methodology

Levels of Oral Health Care
Levels of Oral Health Care:
Levels of PreventionPrimary Secondary Tertiary
Examples of Care: Health Promotion• Dietary
counseling• Behavior
modification
Specific Protection• Fluoride varnish• Dental sealant• Medication
optimization
Arrest & Reverse• Remineralization• Periodontal
maintenance
Dental Intervention• Stabilize disease• Restore form and
function

Pathway PlacementEducation/Knowledge Protocol Development
CRA/PAAPathway Designation
DQI: MORE Care Initiative
Intervention DeterminationEDUCATIONAL
Anticipatory GuidanceBehavior Modification
Shared Patient OutcomesCLINICAL
PreventionRemineralization
Stabilization“Prescription Power”
Dental Team ActivationCooperative Care
Referral System ActivationDental Professional Role Assignment

MORE Care Pathway (Pediatric)
Oral Health at Well Child Visit
1) Review medical/dental histories2) Oral Health Risk Assessment3) Perform HEENOT (w/ intraoral examination)4) Fluoride varnish / silver diamine fluoride5) Prescriptions (PRN)
Risk based instruction6) Counseling to decrease or maintain low oral
health risk (Risk Factor based)7) Anticipatory guidance8) Delivery of patient education documents (PRN)9) Follow up and referral plan
Medical DentalLow risk and < 3 yr.
High risk and > 3 yr.
Care Coordination1) 15 and 30 day follow up of referral to gauge
completion from patient2) Repeat process at next well child visit
Dental Care Referral
Dental Care Appointment
1) Review medical/dental histories2) Complete Caries Risk Assessment and
assign status (Low, Mod, High)3) Preventive Dental Care Appointment4) Treatment Plan Creation
Disease Management6) Reinforcement of counseling to decrease
or maintain low oral health risk7) Provide direct support for risk
management / maintenance8) Complete disease management
communication
Care Coordination1) Complete consultation letter to referring medical
provider that patient completed referral visit2) Complete consultation letter that patient has
completed all necessary treatment, provide recall schedule
3) Provide communication of incomplete treatment plan completion if patient has not returned for dental care visit after initial referral visit (3 mos)

Population Health

Population Health• Population health
– Identifies target (at risk) populations• Includes outcomes, patterns of determinants, and policies and
procedures that involve the aforementioned • Opportunity for health care delivery systems, public health agencies,
community-based organizations, and many other entities to work together • Pediatric
– Majority of innovation focused on children– Dental financial system in U.S. leans toward pediatric care
• Adult– Usually organized according to systemic illness
• Primary diagnosis• Limited intervention models being evaluated• Research on systemic / oral health linkage has not resulted in
consensus

Pediatric Care

Pediatric Primary Care – Caries Disease• CDC: One in five children have untreated decay
• Pew: 29 million children enrolled in Medicaid: only 12.9 million received dental care
• Cavities are the 4th most expensive disease in the U.S.• Poor children had one half the number of dental visits
compared with higher income children– Limited access to dental: higher encounter rates with
medical• “Despite acknowledgement of this problem by dental health
providers little has changed to improve these statistics.”• Pediatricians/Family Practitioners may be able to improve
oral health outcomes.
Mattheus and Mattheus (2014); CDC (2010); Truman et al. (2002); USDHHS (2000); PEW (2011)

Restorative Costs - Typical Medicaid Program
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20$0.0
$500,000.0
$1,000,000.0
$1,500,000.0
$2,000,000.0
$2,500,000.0
$3,000,000.0
$3,500,000.0
$4,000,000.0
$4,500,000.0
$5,000,000.0
Restorative Costs by Age and Tooth Type
D 2nd MolarD 1st MolarD CanineD Lateral IncisorD Central Incisor2nd Molars1st Molars2nd Premolars1st PremolarsCaninesLateral IncisorsCentral Incisors
Age of Beneficiaries
ECC
Sealants

Ecological Plaque Hypothesis
• Microflora adapted to low-sugar diet• Infrequent low-pH episodes• Non-aciduric/non-acidogenic flora
• Selection against non-aciduric bacteria• Aciduric bacteria gain competitive
advantage• Growth of aciduric-acidogenic bacteria
• Low-pH episodes deeper and more involved
• Microflora adapted to efficient use of sugar• Frequent, prolonged low-pH episodes• Acidogenic, aciduric flora
SugarAcidic drinks
Caries Management – Science and Clinical Practice. Hendrik Meyer-Lueckel, Sebastian Paris, Kim R. Ekstrand. Thieme Medical Publishers. NY 2013
Non-Cariogenic Plaque
Cariogenic Plaque
Mom

Accountability – Who’s Accountable
Strep mutans is acquired at an average age of approximately 2 yearsCaufield PW, Cutter GR, Dasanayake AP. Initial acquisition of Mutans streptococci by infants: evidence for a discrete window of infectivity. J Dent Res. 1993;72:37–45

Fluoride application in Primary Care• Holve’s Well Visit Study: Children with 4 or more treatments
had 15.5 dmfs (95%CI 10.8–20.4) versus children with no fluoride varnish treatments who had 23.6 dmfs (95%CI 19.5–25.8) for a 35% decrease in overall caries.
• COCHRANE LIBRARY REVIEW: – The 13 trials that looked at children and adolescents with
permanent teeth the review found that the young people treated with fluoride varnish experienced on average a 43% reduction in decayed, missing and filled tooth surfaces.
– In the 10 trials looking at the effect of fluoride varnish on first or baby teeth the evidence suggests a 37% reduction in decayed, missing and filled tooth surfaces.
Holve, S. (2008); Marinho [Cochrane Library] (2014)

Proposed Mechanisms of Oral Health’s Systemic Impact• Inflammation
– Chronic oral infection contributes to systemic inflammation and increases in the plasma concentration of acute-phase proteins, inflammatory cytokines and coagulation factors which increase the potential for cardiovascular disease (persists long after tooth extraction)
• Infection– Bacterial end products enter the blood stream and result in
transient bacteremia • Diet and Nutrition
– Based on the dysfunctional masticatory system and on the ability to obtain proper nutrition from the diet

Oral Health Systemic Connection

Oral Health Systemic Connection

Aetna’s Data Warehouse Analysis - 2006
• Periodontitis treatment groups had a lower retrospective risk for their chronic condition than patients without periodontitis treatment.
• Recommend examination of the oral cavity for patients with diabetes, coronary artery disease, and cerebrovascular disease.
• Found a need for periodic dental visits for patients with diabetes and cardiovascular disease
• Patients with periodontitis had a higher cost per member per month than patients with gingivitis, other dental diagnosis or no dental diagnosis
Albert et al. (2006)

United Healthcare: Medical Dental Integration Study - 2013
• Study compares the medical and pharmacy costs of individuals with six chronic medical conditions with the dental treatment they receive to determine if there is a difference in total health care costs associated with dental treatments.– Diabetes– Asthma– Congestive Heart Failure– Coronary Artery Disease– Chronic Obstructive Pulmonary Disease– Chronic Kidney/Renal Failure
United Healthcare (2013)

United Healthcare: Medical Dental Integration Study - 2013
• Utilized 3 years of dental claims experience with 2 years of United Healthcare Evidence Based Medicine and episode treatment group claims analysis.
• Summary– Net medical costs (including pharmacy costs) for members who
received dental care was on average $1,037 lower per individual than medical costs for members not receiving care, after adjusting for extra expense of dental care.
– The largest medical savings ($1,849) were for members who were not medically compliant with their disease management program.
– Biggest impact related to members who received frequent cleanings and/or periodontal maintenance.
United Healthcare (2013)

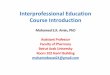
United Healthcare: [Non-Med Compliant] Medical Dental Integration Study - 2013
United Healthcare (2013)
Dia-betes
Asthma CAD CHF COPD Renal Dx
0
10000
20000
30000
40000
50000
60000
No Dental CareReceiving Dental Care

Integrated Model (Cost Effective)
Jeffcoat et al. (2012); United Concordia Wellness Oral Health Study (2012)

References• Albert et al. (2006); An examination of periodontal treatment and per member per month medical costs in an insured
population. BMC Health Services Research 6:103-113.• Bassett, KB et al. (2014). Local anesthesia for dental professionals. Prentice Hall, 2014.• Binkley CJ, Johnson KW. Application of the precede-proceed planning model in designing an oral health strategy. J Theory
Pract Dent Public Health. 2013; 1:2-6• Borrell LN, et al. (2007) Diabetes in the dental office: using NHANES III to estimate the probability of undiagnosed disease. J
Periodontal Res 22:559-565.• Boynes SG. Medical-dental integration: meaningful implementation. National Network for Oral Health Access Quarterly
Newsletter. Summer 2014: 5-6.• CDC (2010); National Center for Health Statistics, Oral and Dental Health. http://www.cdc.gov/nchs/fastats/dental.htm • Chan HH et al. (2012); Salivary proteins associated with periodontitis in patients with type 2 diabetes mellitus. International
Journal of Molecular Sciences 13:4652-4654.• Clark et al. (2014). Fluoride use in caries prevention in the primary care setting. Pediatrics, 134(3), 626-633.• Darre L et al. (2008) Efficacy of periodontal treatment on glycemic control in diabetic patients: a meta-analysis of
interventional studies. Diabetes Metab. 34:497-506.• DiMaria-Ghalili RA, Mutallo JM, Tobin BW, et al. Challenges for nutrition education and training in the health care
professions: intra-professional and interprofessional call to action. American Journal of Clinical Nutrition. 2014; 99:1184S-1193S.
• Elster AB, Levenberg P. Integrating comprehensive adolescent preventive services in routine medicine care: rationale and approaches. Ped Clin N Am 1997; 44:1365-1377.
• Engebretson et al. (2013) The effect of nonsurgical periodontal therapy on HA1C levels in persons with type 2 Diabetes and chronic periodontitis. JAMA 310:2523-2532.
• Engstrom et al. Efficacy of screening for high blood pressure in dental health care. BMC Public Health 2011; 11:194-201.• Glick M, Greenberg BL. The potential role of dentists in identifying patients’ risk of experiencing coronary heart disease
events. J Am Dent Assoc. 2005; 136:1541-1546.• Grossi SG. (1997) Treatment of Periodontal Disease in Diabetics Reduces Glycated Hemoglobin. J Periodontol 68:713–719.

References• Harris R, Bridgman C. Introducing care pathway commissioning to primary dental care: the concept. Br Dent J 2010; 209:233-239.• Holve, S. (2008). An observational study of the association of fluoride varnish applied during well child visits and the prevention of
early childhood caries in American Indian children. Maternal and child health journal, 12, 64-67.• Janket et al. (2005) Does periodontal treatment improve glycemic control in diabetic patients: a meta analysis. JDR 84:1154-1159.• Jeffcoat et al. (2012); Periodontal therapy reduces hospitalizations and medical costs in diabetics. Abstract: Am Assoc of Dental
Research; March 23, 2012.• Krol (2004); Educating pediatricians on children’s oral health: past, present, and future. Pediatrics 113:487-492.• Lalla et al. (2011). Identification of unrecognized diabetes and pre-diabetes in a dental setting. Journal of dental research, 90(7), 855-
860.• Lee JM et al. Salivary diagnositcs. Orthodontics and Craniofacial Research 2009; 12:206-211.• Lewis C et al. (2000); The role of the pediatrician in the oral health of children: a national survey. Pediatrics 106:1-7• Li S, et al. (2011) Development of clinical guideline to predict undiagnosed diabetes in dental patients. J Am Dent Assoc. 142:28-37.• Lockhart, P. B., Bolger, A. F., Papapanou, P. N., Osinbowale, O., Trevisan, M., Levison, M. E., ... & Baddour, L. M. (2012). Periodontal
disease and atherosclerotic vascular disease: does the evidence support an independent association? A scientific statement from the American Heart Association. Circulation, 125(20), 2520-2544.
• Malamed, S. F. (2004). Handbook of local anesthesia. Elsevier Health Sciences.• Malathi et al. Salivary diagnostics: a brief review. ISRN Dentistry 2014; OPEN ID# 158786.• Marinho VC. (2014). Cochrane fluoride reviews: an overview of the evidence on caries prevention with fluoride treatments. Faculty
Dental Journal, 5(2), 78-83.• Mattheus and Mattheus (2014); Saving one smile at a time: oral health promotion in pediatric primary care practice. Open Journal of
Nursing. 4:402-408.• Michalowicz et al. (2014); Factors associated with the clinical response to non surgical periodontal therapy in people with type 2
diabetes mellitus. J Am Dent Assoc 145:1227-1239.• Moore PA. (2002) The diabetes-oral health connection. Compendium 23:14-20.• NNOHA. A user’s guide for implementation of interprofessional oral health core clinical competencies: results of a pilot project.
NNOHA, 2015. http://www.nnoha.org/nnoha-content/uploads/2015/01/IPOHCCC-Users-Guide-Final_01-23-2015.pdf • PEW Center on States (2011); The State of Children’s Dental health: Making Coverage Matter. The PEW Charitable Trust.

References• Pfaffe T et al. Diagnostic potential of saliva: current state and future applications. Clinical Chemistry 2011; 57:675-687.• Qvarnstrom M et al (2008); Salivary lysozyme and prevalent hypertension. J of Dental Research 87:5:480484.• Simpson et al. (2010) Treatment of periodontal disease for glycemic control in people with diabetes. Cochrane Database Syst
Rev;5:CD004714• Stauss SM, et al. (2010) The dental office visit as a potential opportunity for diabetes screening: an analysis using NHANES
2003-2004 data. J Public Health Dent 70:156-162.• Stewart JE, et al. (2001) The effect of periodontal treatment on glycemic control in patients with type 2 diabetes mellitus. J
Clin Periodont. 28:306-10.• Stratton et al. (2000) Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes
(UKPDS 35): prospective observational study. BMJ 321:405–12.• Taylor GW et al. (2008) Periodontal disease: associations with diabetes, glycemic control and complications. Oral Dis.
14:191-203.• Truman et al. (2002); Task force on community preventive services. Reviews of evidence on intervention to prevent dental
caries, oral and pharyngeal cancers and sports related craniofacial injuries. Am Journal of Preventative Medicine 23:21-54.• United Concordia Wellness Oral Health Study (2012);
http://directbenefits.com/PDFs%20-%20Tools/United%20Concordia%20Dental%20Wellness%20Study.pdf • United Healthcare and Optum. Medical Dental Integration Study, March 2013.
http://www.uhc.com/live/uhc_com/Assets/Documents/B2H_Study.pdf • US Department of Health and Human Services [USDHHS] (2000); Oral Health in America: a report of the surgeon general.
Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health. http://www.surgeongeneral.gov/library/reports/oralhealth/index.html
• U.S. DHHS-HRSA. Integration of Oral Health and Primary Care Practice, 2014. http://www.nnoha.org/nnoha-content/uploads/2014/04/HRSA-Oral-Health-Core-Competency-Rerport.pdf
• Wiener, R. C., & Sambamoorthi, U. (2014). Cross-Sectional Association between the Number of Missing Teeth and Cardiovascular Disease among Adults Aged 50 or Older: International Journal of Vascular Medicine. BRFSS.

Questions???