Embed Size (px)
Citation preview

March 30, 2015
CHALLENGES AND VARIABILITY IN
DYSTROPHIN DETECTION:
IMMUNOFLUORESCENCE,
ANTIBODY STAINING
AND IMAGING METHODOLOGIES
CHANTAL BEEKMAN
AFRODITE LOURBAKOS

2
o Existence and variability of trace dystrophin & revertants
o Dystrophin intensity by a reproducible automated image analysis method
o Limitations: variability, linearity, control, biopsy quality
o Clinical study perspective on biopsy dystrophin analysis, next steps
Agenda

3
Counting positive fibers that look like revertants is complicated
Multiple types of revertant fibers present in a biopsy
Counting fibers that look like revertant fibers is difficult to interpret
Ab15277 (C-terminal) MANDYS106 (exon 43) DMD
Exon 45-50
detection of revertant fibers
Revertant fibers: bright muscle fibers with high levels of dystrophin
Revertants without
exon 43
Revertants with
exon 43
4
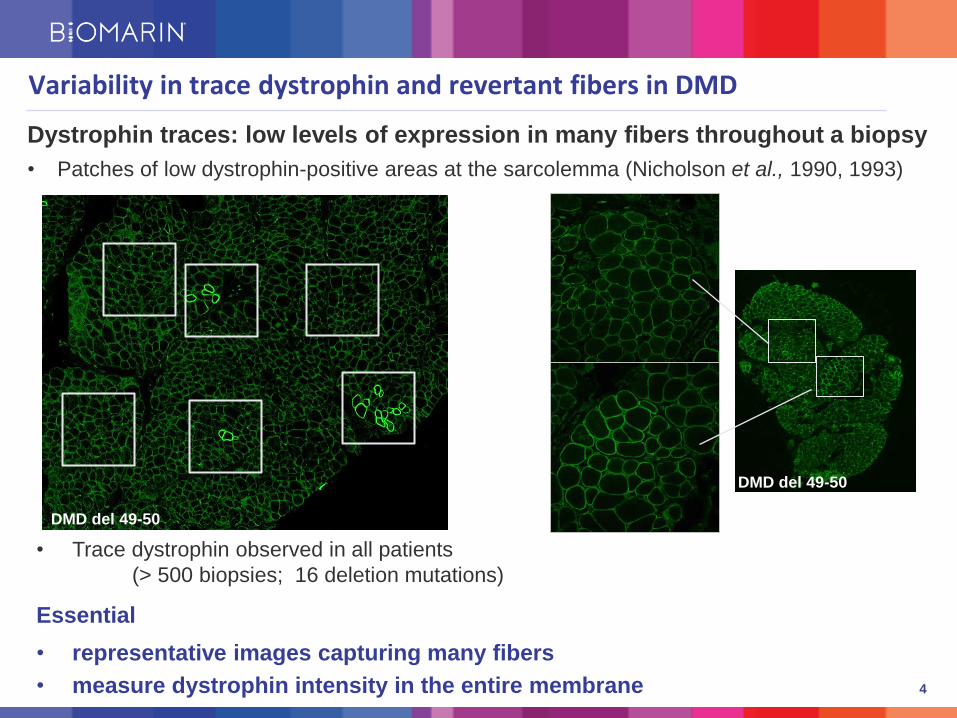
Variability in trace dystrophin and revertant fibers in DMD
• Trace dystrophin observed in all patients
(> 500 biopsies; 16 deletion mutations)
Essential
• representative images capturing many fibers
• measure dystrophin intensity in the entire membrane
DMD del 49-50
DMD del 49-50
Dystrophin traces: low levels of expression in many fibers throughout a biopsy
• Patches of low dystrophin-positive areas at the sarcolemma (Nicholson et al., 1990, 1993)

5
The low trace signal detected in DMD is dystrophin specific
a genetic control analysis
Beekman et al 2014
MANDYS106 (exon 43) Isotype control
DMD del 45
(epitope present)
DMD del 43
(epitope absent)

6
Dystrophin measurement Staining & imaging
0%
20%
40%
60%
80%
100%
0 500 1000 1500
fiber dystrophin intensity (a.u.)
Automated image analysis
Definiens customised software
% c
um
mu
lati
ve f
ibers
revertants
trace
Dystrophin % m
uscle
fib
ers
0%
5%
10%
15%
20%
25%
0 1000 2000
dystrophin mean
of population
Revertants
Trace dystrophin
Method captures the variation in dystrophin intensity between fibers in DMD
Beekman et al 2014 (PLoS One)
• confocal microscopy (25x magnification)
• identification of individual fibers
minimum 90% fibers
generally 250 - 600 fibers / section
• measure per fiber dystrophin intensity
entire membrane for every fiber
operator independent, objective
high reproducibility
Spectrin

7
Reproducibility in dystrophin measurement in different DMD biopsies
• 4 DMD biopsy samples
• 2-3 experiments (over a 1.5 year period) providing inter-assay precision
• 2-4 sections analysed providing intra-assay precision
• 8 operators randomly involved in staining, imaging and image processing
Beekman et al 2014
Sample
Dystrophin membrane
intensity MANDYS106 (a.u)
Ranking
Precision
Exp 1 Exp 2 Exp 3
Intra assay;
CV%
sections
Inter assay;
CV%
experiments
DMD 3 255 241 208 4 3-10% 10%
DMD 1 286 298 228 3 2-8% 14%
DMD 4 306 427 354 2 2-5% 17%
DMD 5 406 - 397 1 4-6% 2%

8
• Negative control differentiates from DMD and is required
• Reproducible differences over a wide range of dystrophin intensity
• Linearity between intensity signal and dystrophin concentration cannot be established
Immunofluorescence can detect differences but is not quantitative
• Different control muscles and donors vary by 30%
• Relative comparison of dystrophin differences between biopsies is informative
CTRL 2
DMD 1
BMD 4
DMD 2
BMD 1
BMD 3
BMD 2
48-50
Ex.19:c.23
80+3A>C
45-50
45-47
03-07
45-47

9
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 200 400 600 800
0207
0507
002001
002002
DMD 5
DMD 4
DMD 3
DMD 1
mean membrane dystrophin intensity (a.u.) c
um
ula
tive
% f
ibers
Assay detects differences accurately in DMD
Dystrophin varies between DMD patients
thus important to compare with pre-treatment biopsy per patient
Beekman et al 2014
DMD 4 del 45
DMD 3 del 50 DMD 1 del 48-50
DMD 5 del 45

10
Image Method comparison: Biological Outcome Measures 2013
Arechavala-Gomeza et al.
10 circles across membranes; measure min & max; divide by spectrin
Taylor et al.
mean membrane intensity per image; threshold approach based on spectrin;
divide by spectrin
Beekman et al.
mean membrane intensity per fiber, not divided by spectrin
Arechavala-Gomeza Taylor
1
2 3
4 5
6 7
8
9 10
11
12
21
13 14 15
16
17
18 19
20
22
23 24
25 26
27
28 29
30
31 32 33 34 35 36
37
38
39 40
41
42
43
44
45
46
47 48
49 50
51
52
Beekman
Anthony et al. 2014 (Neurology)

11
Image Analysis Method comparison by Prosensa
• Analysis Methods are in agreement on the relative comparison between biopsies
• Negative control (PBS) can be 50% of DMD trace values
• Positive control dystrophin intensity vary for different muscles
• Linearity cannot be established due to lack of dystrophin standards
Relative comparison between biopsies is most informative
CTRL 1 CTRL 2 CTRL 3 BMD A DMD B DMD C BMD D DMD E BMD F PBS
0
50
100
Arechavala-Gomeza et alTaylor et al.Beekman et al (Definiens)
Rela
tive d
ystr
op
hin
in
ten
sit
y (
%)

12
Biopsies and DMD biomarkers in clinical programmes
Biopsies are valuable for assessment of disease progression and drug effect
• Dystrophin protein detection
• Exon skip
• Drug concentration in muscle
• Explore other biomarkers of disease
~500 biopsies from multicenter studies (80 sites) covering 16 different DMD deletions
• analysis of biopsies under Good Clinical Laboratory Practices for reliability and
traceability
Potential for surrogate endpoints, but issues to consider:
• Biopsy sampling: which muscle, biopsy size, disease progression
• Quality of handling, shipping and storage (procedures and training)

13
DMD Healthy control muscle
Connective
tissue
Disease progression and heterogeneous sampling can affect analysis
Connective tissue
Muscle fibers Adipose cells
DMD -Extensive disease
progression:
• Sufficient number of muscle fibers required
• Small biopsies and low muscle content are prone
to experimental artifacts

14
H&E staining
Spectrin staining
good intermediate poor
Freeze artefacts influence staining and ability to compare biopsies
No reliable comparison can be made between biopsies that differ in quality
% of subjects with evaluable biopsies
phase II DMD114117 (13 sites) 88%
phase II DMD114876 (13 sites) 66%
phase III DMD114044 (46 sites) 50%

15
• Dystrophin immunofluorescence analysis using intensity measurements
• dystrophin signal localisation at entire membrane
• variable presence of trace dystrophin and revertant fibers
• requires good quality biopsies
• reproducibly and accurately detects differences between DMD biopsies
- intra-assay precision typically <10%; inter-assay precision <25%
• Advancing immunofluorescence methods for quantification requires
development and purified dystrophin protein control with a signal dilution
relevant to DMD patients
• Further effort and development to correlate dystrophin to clinical outcome in
randomized placebo controlled clinical trials is required
CONCLUSIONS

16
• Biomarin/Prosensa: Stavros Giannakopoulos, Janwillem Testerink, Tjadine Holling, Niki Heuvelmans, Ronald
Jan Baptiste, Dyonne Kreuger, Dirk Duinsbergen, Umut Akinci Corbacioglu, Roelof Kuper, Jessica Sipkens,
Petra de Bruijn, Simone van Wijngaarden, Karin Boekhoorn, Carla Persoon-Deen, Nico Yau, Karolina
Kozaczynska, Anneke Janson, Alison Foster, Claire Wardell, Judith van Deutekom, Afrodite Lourbakos, Sjef de
Kimpe, Giles Campion
• LUMC: Jan Verschuuren for BMD samples, VUMC: H.W. Niessen and Asterand for control samples
• GSK: Steve Hood, Rob Geeske, Katja Remlinger, John Kraus
• BOM consortium: Anthony V, Arechavala-Gomeza LE, Taylor BS, Vulin A, Kaminoh BS, Torelli S, Feng L,
Janghra L, Bonne G, Beuvi, M, Barresi R, Henderson, M, Laval S, Lourbakos A, Campion G, Straub V , Voit T,
Sewry C , Ellis J, Morgan JE , Flanigan KM, Muntoni F.
• Clinical Investigators : Alexandra Araujo , Elena Belousova , Enrico Bertini , Peter Born, Craig Campbell ,
Claude Cances, Brigitte Chabrol, Jong-Hee Chae, Jaume Colomer Oferil, Giacomo Pietro Comi , Jean-Marie
Cuisset , Guy D'Anjou Isabelle Desguerre , Alberto Dubrovsky, Ricardo Erazo Torricelli, Raúl Escobar, David
Feder , Alessandra Ferlini , Roberto Giugliani, Ágnes Herczegfalvi , Yuh-Jyh Jong , Shigemi Kimura , Jan-Bernd
Kirschner, Karin Kleinsteuber , Hirofumi Komaki , Anna Kostera-Pruszczyk , Martin Kudr , Eugenio Maria
Mercuri , Valentina Ricotti, Wolfgang Mueller-Felber, Erik Niks, Katsuhisa Ogata, Ignacio Pascual , Yann Pereon,
Salmo Raskin, Jan Verschuuren, Michela Guglieri, Viera Darin, Magnhild Rasmussen, Laurent Servais,
Umbertina Reed, Ulrike Schara, Kathryn Selby, Claudia Sobreira, Yasuhiro Takeshima, Haluk Topaloglu, Juan
Jesus Vilchez Padilla, Ayse KaradumanGiuseppe Vita, G. Buyse, Kevin Flanigan, K., Petr Vondracek, Gert
Wiegand, Ekkehard Wilichowski, Nicholas Deconinck, Brenda Wong, Francesco Muntoni,Volker Staub, Haluk
Topaloglu, Greg MacDonald, Thomas Voit, Mar Tulinius, Nathalie Goemans
• DMD patients and families
Acknowledgements





























