Embed Size (px)
Citation preview

Ch. 26 – The Urinary System
• The general functions of the major organs of the urinary system are stated here
Fig. 26-1, p. 954

Specific functions of the urinary system• 1. Excretion = the removal of organic metabolic
waste products from body fluids (such as blood)• 2. Elimination = the discharge of these waste
products to the external environment• 3. Regulation of blood plasma volume and solute
concentration, by…– Regulating blood volume and pressure, by…
• Adjusting the volume of water in the urine• Releasing erythropoietin (EPO)• Releasing renin
– Regulating plasma concentrations of Na+, K+, Cl-, Ca2+, etc.
– Helping to regulate blood pH, by…• Excreting or conserving H+ and HCO3
-
– Conserving valuable nutrients– Assisting the liver in detoxifying poisons and deaminating
amino acids

Fig. 26-3, p. 956
FYI (for lecture) – renal gross anatomy is covered in lab

Fig. 26-2, p. 955
FYI (for lecture) – renal gross anatomy is covered in lab

Fig. 26-4, p. 956
FYI (for lecture) – renal gross anatomy is covered in lab

Fig. 26-5, p. 958
FYI (for lecture) – renal gross anatomy is covered in lab

Fig. 26-6, p. 959
Nephrons • Ca2+ reabsorbtion is variable due to PTH and calcitriol
• Na+ reabsorption is variable due to aldosterone
• H2O reabsorption is variable due to ADH
• = the microscopic functional units of the kidneys
• Each consists of a renal corpuscle and a renal tubule
• Function: form urine via filtration of the blood, reabsorption of water and some solutes, and secretion of other solutes
• There are over 1 million nephrons per kidney!
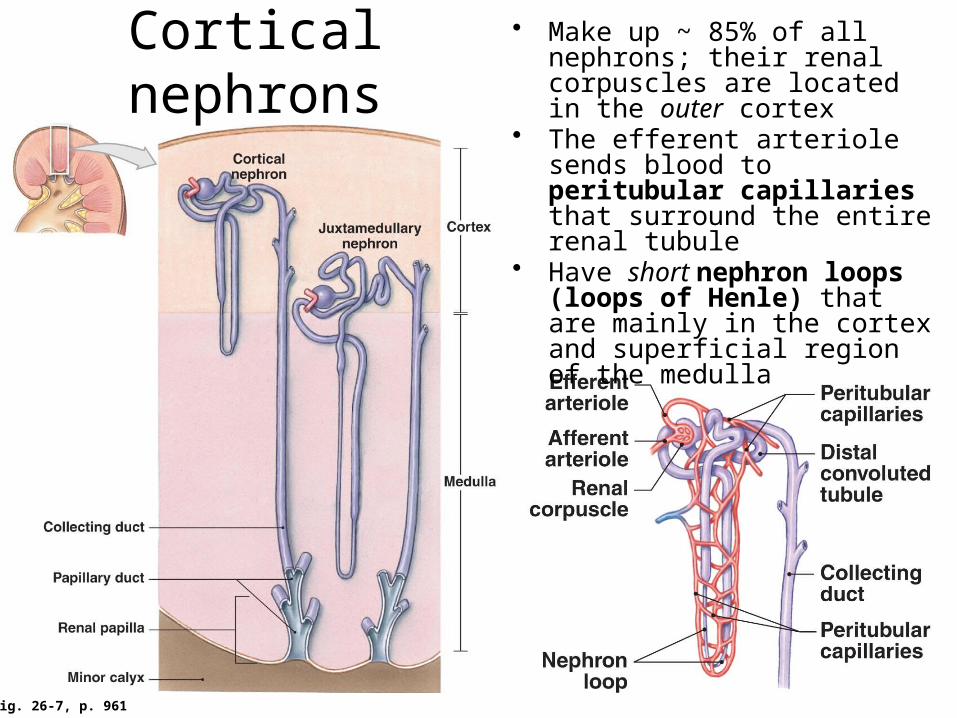
Fig. 26-7, p. 961
Cortical nephrons• Make up ~ 85% of all nephrons;
their renal corpuscles are located in the outer cortex
• The efferent arteriole sends blood to peritubular capillaries that surround the entire renal tubule
• Have short nephron loops (loops of Henle) that are mainly in the cortex and superficial region of the medulla

Juxtamedullary nephrons
• Make up ~ 15% of all nephrons; their renal corpuscles are located deep in the cortex
• The efferent arteriole sends blood to both peritubular capillaries and the vasa recta
• Have long nephron loops which penetrate deep into the medulla and are surrounded by the vasa recta– The ascending and descending limbs of the
nephron loop have different permeability characteristics, allowing the production of concentrated urine (more on this later)
Fig. 26-7, p. 961

Fig. 26-8, p. 962
The renal corpuscle
• = the glomerular (Bowman’s) capsule + the glomerulus– The glomerular capsule is made up of an outer parietal layer
of simple squamous cells called the capsular epithelium and an inner visceral layer of simple squamous cells that cover the glomerulus called the visceral epithelium (the individual cells of the visceral epithelium are called podocytes), with the capsular (Bowman’s) space in between
– The glomerulus is a bed of fenestrated capillaries

Fig. 26-8b, p. 962
The glomerular filtration membrane• Consists of 3 layers:
– 1. The glomerular capillary endothelium is fenestrated (i.e., the capillary endothelial cells have fenestrations, or pores)
• But fenestrations do not let blood cells or platelets pass into the filtrate– 2. The dense layer (part of the basement membrane) is between the
glomerular endothelium and the visceral epithelium (podocytes)• This prevents the
filtration of large plasma proteins
– 3. The visceral epi- thelium covers the glomerulus
• It is a simple squamous epi- thelium made up of cells called podocytes
– Podocytes have pedicels (“little feet”), between which are filtration slits
Fig. 26-10a, p. 968

Fig. 26-9, p. 965
Renal physiology:
urine formation

Renal physiology: urine formation• Urine is formed by 3 distinct processes:
– 1. Filtration = the production of filtrate (“pre-urine”) from blood plasma• Essentially, anything except blood cells, platelets, and most
plasma proteins can be filtered (but may not be—see “secretion” below)
• It occurs due to blood pressure within the glomerulus of the renal corpuscle
– 2. Reabsorption = the removal of “wanted” substances from the filtrate (which is now called tubular fluid) • It occurs via diffusion or active transport along the renal tubule and
collecting duct• The reabsorbed substances will ultimately be returned to the blood
– 3. Secretion = “unwanted” substances that did not get filtered from the blood originally are added to the tubular fluid • E.g. metabolic wastes like urea, creatinine, and uric acid• It also occurs via diffusion or active transport along the renal
tubule and collecting duct

Table 26-2, p. 964
How efficient is urine formation?
Don’t memorize the numbers; just note that the kidneys are good at keeping nutrients and getting rid of wastes

Fig. 26-10, p. 968
Glomerular filtration
• Essentially, the hydrostatic (blood) pressure within the glomerulus (= the GHP) forces water and small solutes through the filtration membrane into the capsular space
• Net filtration pressure = NFP = (GHP – CsHP) – BCOP
• So NFP = (50 mm Hg – 15 mm Hg) – 25 mm Hg = 10 mm Hg

The glomerular filtration rate (GFR)• = the volume of filtrate produced by both kidneys in
one minute• The kidneys have a HUGE filtration surface area
(6 m2/64 ft2 per kidney), so…– Average GFR = 125 mL/minute = 180 L/day!!!
• But 99% of the filtrate is reabsorbed
• Control of the GFR occurs on 3 interacting levels:– 1. Autoregulation (local)
• If autoregulation is insufficient to restore normal GFR, then…
– 2. Hormonal regulation• Via the renin-angiotensin system and natriuretic peptides
– 3. Autonomic (nervous) regulation• Mostly by the sympathetic division of the ANS (only in a crisis
situation)

Autoregulation of the GFR
• Maintains the GFR when local BP and blood flow through the glomerulus change–1. ↓ GHP or blood flow causes:
• Dilation of afferent arterioles• Constriction of efferent arterioles
–2. ↑ GHP or blood flow causes:• Constriction of afferent arterioles

Hormonal regulation of the GFR• Natriuretic peptides (ANP and BNP)
– Are released when ↑ systemic BP and blood volume stretch the walls of the heart
– Some effects (there are more—see Ch. 18 or 21) include:• Dilation of the afferent arterioles → ↑ GHP → ↑ GFR → ↑ urine
output → ↓ systemic BP and blood volume• Constriction of the efferent arterioles, with the
same effect as above• Renin
– Is released by the juxtaglomerular complex (JGC) when:• It detects ↓ GHP• It’s stimulated by the sympathetic
division of the ANS• Its macula densa cells detect
↓ [osmotic] in the tubular fluid within the DCT
– Effect: it ultimately activates angiotensin II (see the next slide)…
Fig. 26-8a, p. 962

Fig. 26-11, p. 971
Once again, the renin-angiotensin system
Autonomic regulation of the GFR• Most renal innervation is by the sympathetic
division of the ANS• An acute ↓ in systemic BP or blood volume
due to a life-threatening emergency (e.g. a heart attack, anaphylaxis, major blood loss, etc.) → sympathetic activation, causing:– Powerful constriction of the afferent arterioles → ↓ GHP → ↓ GFR
I.e., “this is a crisis situation…I must maintain systemic blood volume and pressure at the expense of kidney perfusion and function!”

Fig. 26-12, p. 973
Reabsorption and secretion at the PCT
• Reabsorption of 60-70% of the filtrate occurs here– Reabsorbed substances enter the
peritubular fluid (= the interstitial fluid that surrounds the renal tubule), then diffuse into the peritubular capillaries
• Limited secretion occurs here
Fig. 26-7c, p. 961

Reabsorption and secretion at the PCT
Fig. 26-12, p. 973
• Reabsorption of: – Organic nutrients: vitamins, and
99% of the glucose and amino acids that were filtered
– Ions: Na+, K+, HCO3- (CO2), Cl-,
urea, and others– Water (which osmotically follows
the solutes)• Secretion (a limited amount) of:
– H+, NH4+, creatinine, drugs, and
toxins

Fig. 26-13a, p. 975
Reabsorption at the nephron loop• ~ 25% of the water and 20-25% of the Na+ and Cl- present in the original
filtrate are reabsorbed via countercurrent multiplication (see the next two slides for more details)…– Fluid in the descending and ascending limbs of the nephron loop run in
opposite directions (i.e., countercurrent)– The limbs have different permeability characteristics:
• The thin descending limb is permeable to water, but not to Na+ and Cl- • The thick ascending limb is not permeable to water, and pumps Na+ and Cl- out

Countercurrent multiplication at the
nephron loop• 1. Na+ and Cl- are pumped out of the
thick ascending limb of the nephron loop
• 2. This results in ↑ [osmotic] in the peritubular fluid of the medulla
• 3. Water is attracted to the Na+ and Cl- in the peritubular fluid, and thus it (water) leaves the thin descending limb by osmosis
• 4. This results in ↑ [Na+ and Cl-] in the tubular fluid of the descending limb as it moves toward the ascending limb
• 5. The arrival of highly concentrated tubular fluid in the thick ascending limb allows the Na+/Cl- pumps to work more efficiently, pumping even more Na+ and Cl- out to the peritubular fluid (this is a repeat of step #1, so countercurrent multiplication is a positive feedback loop)
Fig. 26-13b, p. 975

Fig. 26-13c, p. 975
More on countercurrent multiplication• Urea adds even
more to the [osmotic] in the peritubular fluid of the deepest parts of the medulla
• The overall functions of CCM are to:– Efficiently
reabsorb NaCl and water
– Create and maintain ↑ [osmotic] in the peritubular fluid of the medulla for water reabsorption at the thin descending limb of the loop and the collecting duct

Fig. 26-14ab, p. 978
Reabsorption and secretion at the DCT
• Reabsorption of: – Ions: Na+ (variable with
aldosterone levels*), Cl-, Ca2+ (variable with PTH and calcitriol levels), and HCO3
- (CO2)
– Water (vari- able with ADH levels)
• Secretion (more than what occurs at the PCT) of:– H+, K+ (counter-
transported with Na+) NH4
+, creatinine, drugs, and toxins
*Aldosterone stimulates the synthesis of Na+/K+ pumps and Na+ channels

Fig. 26-14c, p. 979
Reabsorption and secretion along the collecting system• Reabsorption of:
– Ions: Na+ (variable with aldosterone levels), Cl-, HCO3
- (CO2) or H+, and
urea (at the papillary ducts only)
– Water (variable with ADH levels)
• Secretion of:– H+ or HCO3
-, and K+
(counter-transported with Na+)
Note: H+ and HCO3- generally
move in opposition to one another to help regulate the pH of body fluids

Forming dilute vs. concentrated urine• This is regulated by the absence or presence of ADH
– ADH causes water channels (aquaporins) to be inserted into the membrane of the DCTs and collecting ducts, which greatly enhances osmosis
Fig. 26-15, p. 980

Table 26-5, p. 981
The general characteristics of normal urine
• Note that normal urine is slightly acidic, mostly water, clear (not cloudy or opaque), sterile, and while we may produce 180 L of filtrate per day, only about 1-2 L of urine is actually formed per day
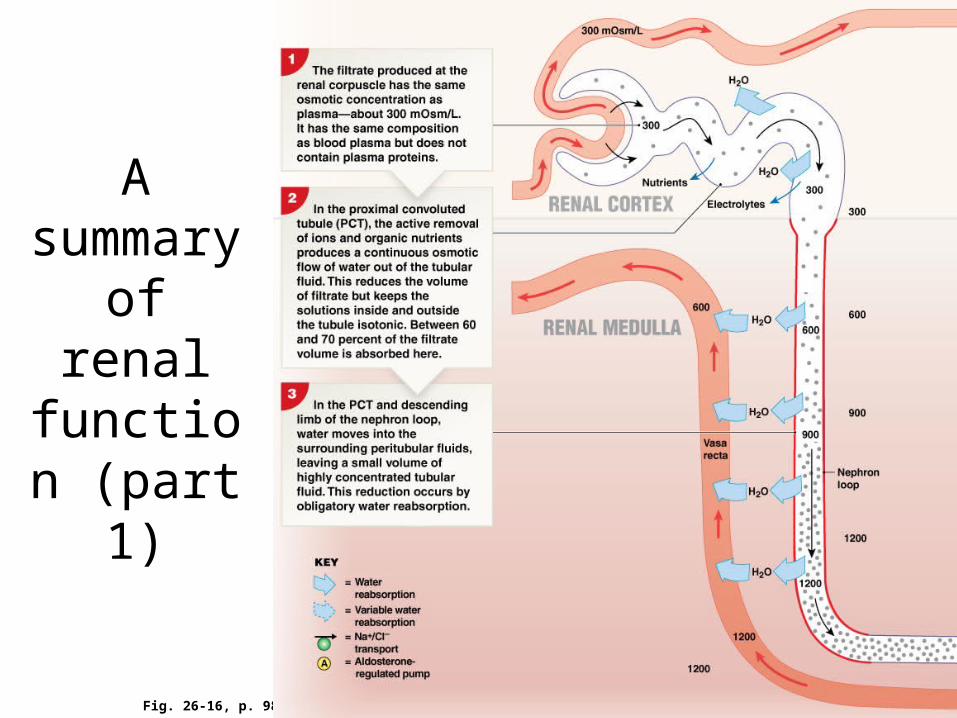
Fig. 26-16, p. 982
A summary of renal function (part 1)

Fig. 26-16, p. 983
A summary of renal function (part 2)

Urine transport, storage, and elimination
Fig. 26-17, p. 985
FYI (for lecture) – gross anatomy is covered in lab

FYI (for lecture) – gross anatomy is covered in lab
Fig. 26-18, p. 987
Urine transport,
storage, and
elimination

Urine transport, storage, and elimination
Fig. 26-19, p. 988
FYI (for lecture) – histology is covered in lab

Fig. 26-20, p. 989
The micturition reflex and urination
• The reflex begins to function when ~ 200 mL is in the bladder
• If you don’t voluntarily go (step C3-4), the bladder relaxes and the cycle repeats (with increasing intensity) within an hour
• Once the volume reaches ~ 500 mL, the pressure generated by the detrusor muscle may be high enough to force open the sphincters
• Typically < 10 mL will remain in the bladder after urination is completed

Admit it: urine love with your kidneys, aren’t you?




















![26 [chapter 26 the urinary system]](https://img.dokumen.tips/doc/110x75/5a6496117f8b9a2c568b5ff7/26-chapter-26-the-urinary-system.jpg)








