Embed Size (px)
DESCRIPTION
case study
Citation preview

AMA Computer Learning CenterSt. Augustine School of Nursing
A Case Study Presented to the faculty of AMA Computer Learning Center
Guagua, Pampanga
Cerebrovascular Accident
Submitted to:Mr. John Eric T. Salvador B.S.N, R.N
Submitted by:
Almario, Jeanette
Cayanan. Gemmalyn Joy
Quitaleg, Mary Jane
Santos, Cariza Joy M.
3k-PN

October ‘09
Table of Content Page
Introduction 1
Personal History 2
Lifestyle and Diet 3
Complete Physical Assessment 4-9
Neurological Assessment 10-11
Laboratory Procedure 12-13
Diagnostic Procedure 14
Anatomy and Physiology 15-17
Pathophysiology of Cerebrovascular Accident 18-19
Drug Study 20-21
Diet and Activity 23
SOAPIE (actual) 24
SOAPIE (potential) 25
Conclusion 26
Recommendations 27
Bibliography 28

NCP(actual/ potential ) 29-33

Introduction
A stroke is damage to part of the brain when its blood supply is suddenly reduced or stopped. A stroke may also be called a cerebral vascular accident, or CVA. The part of the brain deprived of blood dies and can no longer function. Blood is prevented from reaching brain tissue when a blood vessel leading to the brain becomes blocked (ischemic) or bursts (hemorrhagic). The symptoms of a stroke differ, depending on the part of the brain affected and the extent of the damage. Symptoms following a stroke come on suddenly and may include: weakness, numbness, or tingling in the face, arm, or leg, especially on one side of the body trouble walking, dizziness, loss of balance, or coordination inability to speak or difficulty speaking or understanding, trouble seeing with one or both eyes, or double vision, confusion or personality changes, difficulty with muscle movements, such as swallowing, moving arms and legs, loss of bowel and bladder control, severe headache with no known cause, and loss of consciousness.
There are following metabolic disorder that may contribute to stroke, excess weight around the waist (waist measurement of more than 40 inches for men and more than 35 inches for women) triglycerides blood level of 150 mg/dL or more, HDL cholesterol levels below 40 mg/dL for men and below 50 mg/dL for women, blood pressure of 130/85 mm HG or higher and prediabetes (a fasting blood sugar between 100 and 125) or diabetes (a fasting blood sugar level over 125 mg/dL).
Latest Trend(Medication for Cerebrovascular Accident)
Anti-platelet medicines like aspirin, clopidogrel, extended release dipyridamole and aspirin in combination, and ticlopidine help prevent stroke because they keep the blood from clotting. Like aspirin, these medicines keep your blood from clotting. They are available only prescription. dipyridamole and aspirin combination (Aggrenoxl®), clopidogrel (Plavixl®), ticlopidine (Ticlidl®).Anti-coagulant medicines keep you from getting blood clots. You may hear people call these medicines "blood thinners." Warfarin (Coumadinl®) is often used in patients who have heart problems or artificial heart valves. Tissue plasminogen activator (t-PA or thrombolytic therapy) dissolves blood clots, but it may cause bleeding (including bleeding into the brain).This medicine must be given within 3 hours of the start of stroke symptoms. You will not be given t-PA if your blood pressure is too high, if changes on a CT scan show it should not be given, or if the risk of bleeding is too great. Heparin / heparinoid medicines slow the creating of blood clots. But there is little, if any, benefit in treating stroke. The medicines also can cause bleeding.

1.
2. Personal History
Name: Mr. D Address: San Rafael, Guagua
Age: 43 yrs. Old Work: Jeepney Driver
Chief Compliant: Impaired Verbal Communication
2.1 Family Health History

2.
2.2 Past Health History
Mr. D’s wife verbalized that Mr. D was already been confined on the hospital before due to mild stroke last year December 2008 , while he is in their house he experienced sudden headache, dizziness, numbness, blurred vision and that made his wife to bring him into the hospital. Mr. D was confined for 4 days and after a week he was able to work again as jeepney driver though the doctor said he need to take rest from work, avoid stress, smoking, alcohol intake, and high fat/ salt food to avoid the stroke.
2.3 Present Health History
Mr. D was been confined again in the hospital of DPMMH last August 27, 2009 and he spent more than 7 days in the hospital. Mr. D’s wife said that while Mr. D is talking with his friend and drinking alcohol he experienced severe headache, sudden dizziness, paralysis in the right part of his body, numbness, blurred vision and loss of consciousness. And made his family to bring him into the hospital.
3. Lifestyle and Diet
Mrs. D said that his husband was a smoke, he consumed more than 30-40 pieces a day (1 1/2 pack) since 20 years old and he also drink 1 bottle of alcohol since 23 years old. Mrs. D said that her husband likes to eat pork after a long day of handling his jeep.

3.
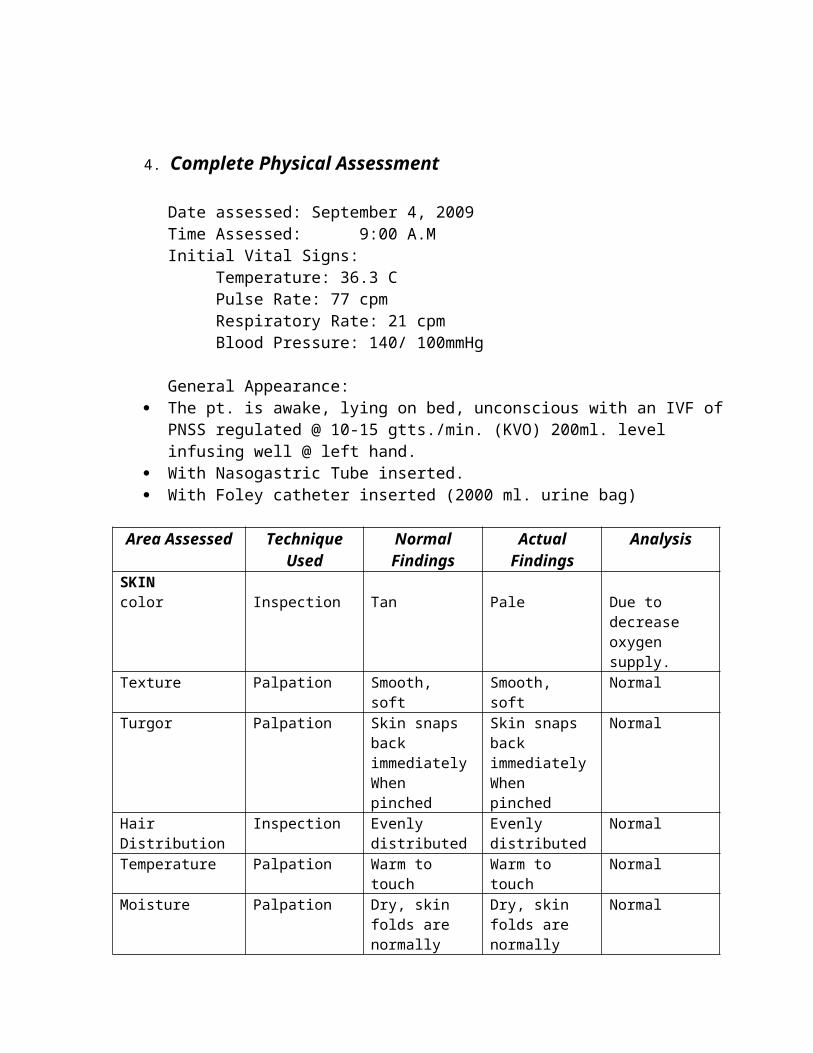
4. Complete Physical Assessment
Date assessed: September 4, 2009Time Assessed: 9:00 A.MInitial Vital Signs:
Temperature: 36.3 CPulse Rate: 77 cpmRespiratory Rate: 21 cpmBlood Pressure: 140/ 100mmHg
General Appearance: The pt. is awake, lying on bed, unconscious with an IVF of PNSS regulated @
10-15 gtts./min. (KVO) 200ml. level infusing well @ left hand. With Nasogastric Tube inserted. With Foley catheter inserted (2000 ml. urine bag)
Area Assessed Technique Used
Normal Findings
Actual Findings
Analysis
SKINcolor Inspection Tan Pale Due to
decrease oxygen supply.
Texture Palpation Smooth, soft Smooth, soft NormalTurgor Palpation Skin snaps
back immediatelyWhen pinched
Skin snaps back immediatelyWhen pinched
Normal
Hair Distribution Inspection Evenly distributed
Evenly distributed
Normal
Temperature Palpation Warm to touch Warm to touch NormalMoisture Palpation Dry, skin folds
are normally moist
Dry, skin folds are normally moist
Normal
NAILSColor of Nail bed Inspection Pink and clear Pink and clear NormalTexture Palpation Smooth Smooth NormalShape Inspection Convex
curvatureConvex curvature
Normal
Nail base Inspection Firm Firm NormalCapillary refill time
Blanch test 2-3 seconds 4 sec. Due to decrease oxygen supply.
HAIR Normal

Color Inspection Black (varies) Black (varies)Distribution Inspection Evenly
distributedEvenly distributed
Normal
Moisture Inspection Neither excessively dry nor oily
Neitherexcessively dry nor oily
Normal
Texture Inspection Silky, resilient Silky, resilient NormalHEAD
Scalp symmetry Inspection Symmetrical Symmetrical Normal
Skull size Inspection Normocephalic Normocephalic Normal Shape Inspection and
PalpationRound Round Normal
Nodules/ masses Palpation Absence of nodules and masses
Absence of nodules and masses
Normal
FACESymmetry Inspection
Symmetrical Symmetrical Normal
Facial movement Inspection Symmetrical Symmetrical Normal
Skin color Inspection Tan Pale Due to decrease oxygen supply.
EYESEyebrows Inspection
Symmetrically aligned, equal movement
Symmetrically aligned, equal movement
Normal
Eyelashes Inspection Slightly curved upward
Slightly curved upward
Normal
Eyelids Inspection Smooth, tan, do not cover pupil as sclera, close symmetrically
Smooth, tan, do not cover pupil as sclera, close symmetrically
Normal
Ability to blink Inspection Blinks voluntarily and bilaterally
Blinks involuntarily.
Due to damage of Broca’s area.
Frequency of blinking
Inspection 20 blinks per min.
To speech. Due to damage of Broca’s area.
Ocular movement Inspection Eye moves freely
Lack of eye movement
Due to damage of Broca’s area.
Position Inspection Drawn from lateral angel
Drawn from lateral angel
Normal
Size Inspection Medium Medium Normal Texture Palpation Mobile, firm and
non-tenderMobile, firm and non-tender
Normal
CONJUCTIVAColor Inspection Transparent
with light colorTransparent with light color
Normal
Texture Inspection Shiny and Shiny and Normal
smooth smoothPresence of lesions
Inspection No lesions No lesions Normal
APPARATUS
CorneaColor Inspection Black Black Normal Texture Inspection Shiny and
smoothShiny and smooth
Normal
PUPILSColor Inspection Black Black NormalReaction to light Inspection Pupils Equally
Round and React to Light Accommodation (PERRLA)
Pupils Equally Round and React to Light Accommodation (PERRLA)
Normal
Size Inspection Equal Equal NormalShape Inspection Round and
constrict brisklyRound and constrict briskly
Normal
Symmetry Inspection Equal in size Equal in size Normal Visual Acuity Inspection Able to real
news printCannot able to real news print.
Due to damage of the left hemisphere of the brain.
Visual Fields Inspection When looking straight ahead, client can see objects in periphery
With blurred vision and cannot classify objects in periphery.
Due to damage of the left hemisphere of the brain.
Ocular Inspection Eyes move freely
Eyes move freely
Normal
NOSESymmetry, shape, size and color
Inspection Symmetrical, smooth and tan
Symmetrical, smooth and tan
Normal
Mucosa color Inspection Reddish to pinkish
Reddish to pinkish
Normal
NASAL SEPTUMNares
Inspection Oval, symmetrical
Oval, symmetrical
Normal
Nasal discharge Inspection No discharge No discharge Normal Sinuses Inspection Not tender Not tender Normal MOUTHSecretion Inspection (neutral in
color) without mucus production
without mucus production
Normal
LipsColor
Inspection Pinkish to slightly brown
Dark and brown and cracking
Due to decrease

lips oxygen level Symmetry Palpation Symmetrical Symmetrical Normal Texture Palpation Soft, moist,
smoothCrack, rough s Normal
Moisture Palpation Soft and moist Dry Due to decrease oxygen.
GUMSColor Inspection Pinkish Pale Due to
decrease oxygen.
Moisture Palpation Moist Moist Normal BUCCAL MUCOSAColor Inspection Glistening pink Slightly pale Due to
decrease oxygen.
Texture Palpation Soft Soft Normal Moisture Palpation Moist Moist Normal TOUNGEColor Inspection Pinkish Slightly pinkish Due to
decrease oxygen.
Size Inspection Medium Medium Normal Symmetry Inspection Symmetrical Symmetrical Normal Mobility Inspection Moves freely Moves freely NormalUVULALocation Inspection At the midline At the midline Normal Symmetry Inspection Symmetrical Symmetrical Normal TONSILSColor Inspection Pinkish Pinkish NormalDischarges Inspection No discharges No discharges Normal TEETHColor Inspection Ivory/yellowish Yellowish NormalNumber of teeth Inspection 32 28 Due to tooth
decay (teeth extraction)
NECKPosition Inspection Head-centered Head-centered Normal Movement Inspection Moves freely Moves freely Normal Range of motion Inspection Full range No ROM Abnormal due
to neuromuscular impairement.
Consistency Inspection No enlargement No enlargement Normal HEARTHeart rate Auscultation 60-100bpm 77 bpm Normal Heart sounds Auscultation Clear, without
cracklesClear Normal
Lung field Auscultation Resonant Resonant Normal

THORAX & LUNGS POSTERIOR THORAXSymmetry Inspection Symmetrical Symmetrical Normal
Respiratory rate Inspection 12-20cpm 21 cpm Normal Spinal Alignment Inspection Spine vertically
alignSpine vertically align
Normal
Skin integrity Inspection Skin intact Skin intact Normal ANTERIOR THORAXBreathing pattern Auscultation Breathing is
automatic and effortless, regular and even and produces no noise
Breathing is automatic and effortless, regular and even and produces nonoise
Normal
Lung/ breath sounds
Auscultation Bronchia-vesicular
Bronchia-vesicular
Normal
ABDOMENContour Inspection Flat Flat NormalTexture Palpation Smooth Smooth Normal Frequency and character
Auscultation Audible; soft gurgling sound occur irregularly and rages from 5-30 mins
Audible; soft gurgling sound occur irregularly and rages from 5-30 mins
Normal
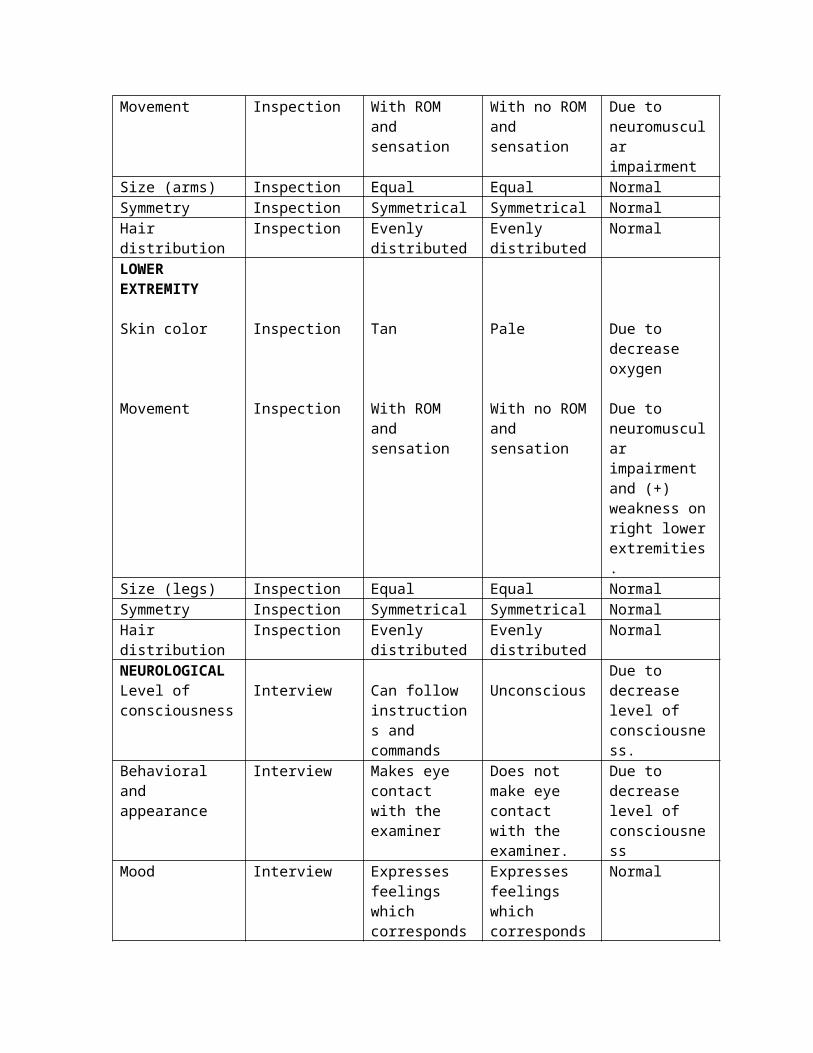
UPPER EXTREMITY Skin color
Movement
Inspection
Inspection
Tan
With ROM and sensation
Pale
With no ROM and sensation
Due to decrease oxygen
Due to neuromuscular impairment
Size (arms) Inspection Equal Equal Normal Symmetry Inspection Symmetrical Symmetrical Normal Hair distribution Inspection Evenly
distributedEvenly distributed
Normal
LOWER EXTREMITY
Skin color
Movement
Inspection
Inspection
Tan
With ROM and
Pale
With no ROM
Due to decrease oxygen
Due to

sensation and sensation neuromuscular impairment and (+) weakness on right lower extremities.
Size (legs) Inspection Equal Equal Normal Symmetry Inspection Symmetrical Symmetrical NormalHair distribution Inspection Evenly
distributedEvenly distributed
Normal
NEUROLOGICALLevel of consciousness
Interview Can follow instructions and commands
UnconsciousDue to decrease level of consciousness.
Behavioral and appearance
Interview Makes eye contact with the examiner
Does not make eye contact with the examiner.
Due to decrease level of consciousness
Mood Interview Expresses feelings which corresponds to the examiner
Expresses feelings which corresponds to the examiner
Normal
MANNERISMS & ACTIONS LANGUAGEVoice inflection Interview Clear and
strongAphasia Due to damage
of Broca’s area in the brain and muscle tone.
Tone Interview Fluent and articulated
Aphasia Due to damage of Broca’s area in the brain and muscle tone.
Manner and speech
Interview Can give appropriate answer to questions
Cannot give answer or talk.
Due to damage of Broca’s area in the brain and muscle tone.
MENTAL STATUSOrientation Interview Oriented with
timeDisoriented with time
Due to decrease level of consciousness
TIMERecall recent and remote memory
Interview Recall events readily, immediate recall of remote information
Cannot recall events readily, immediate recall of remote information
Due to aphasia.
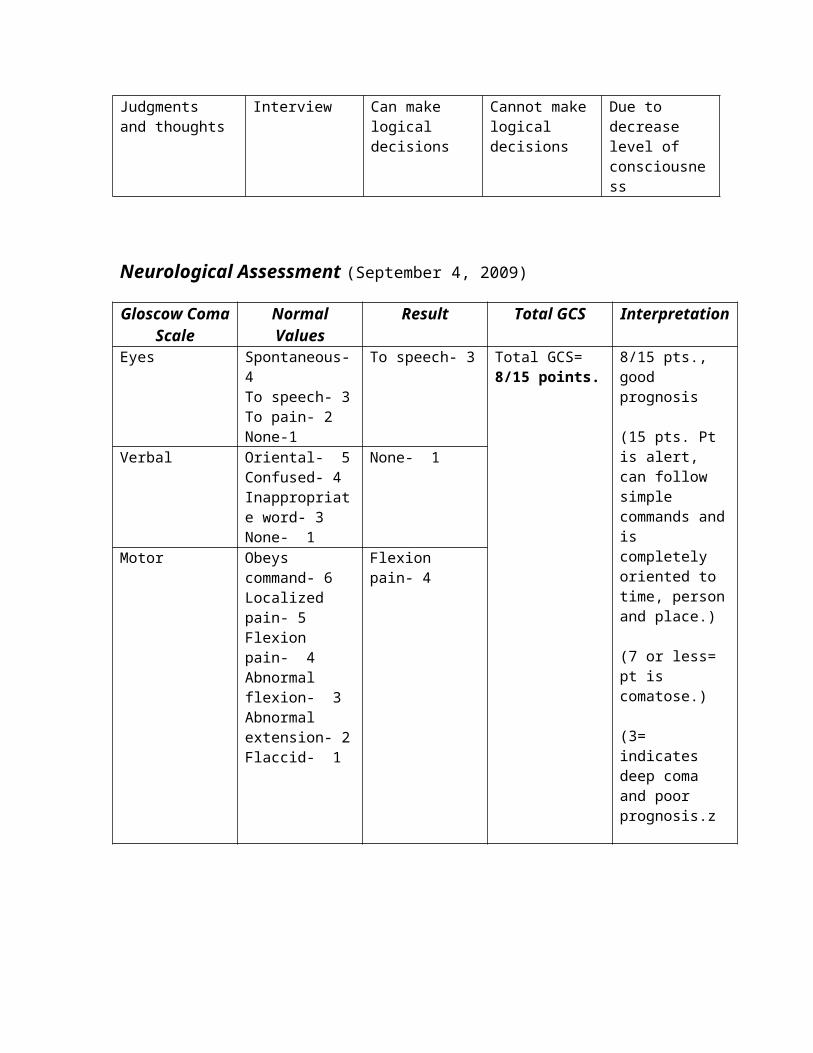
Judgments and thoughts
Interview Can make logical
Cannot make logical
Due to decrease level

decisions decisions of consciousness
Neurological Assessment (September 4, 2009)
Gloscow Coma Scale
Normal Values
Result Total GCS Interpretation
Eyes Spontaneous- 4To speech- 3To pain- 2None-1
To speech- 3 Total GCS= 8/15 points.
8/15 pts., good prognosis
(15 pts. Pt is alert, can follow simple commands and is completely oriented to time, person and place.)
(7 or less= pt is comatose.)
(3= indicates deep coma and poor prognosis.z
Verbal Oriental- 5Confused- 4Inappropriate word- 3None- 1
None- 1
Motor Obeys command- 6Localized pain- 5Flexion pain- 4Abnormal flexion- 3Abnormal extension- 2Flaccid- 1
Flexion pain- 4

10.
Cranial Nerve Date Done Normal Result Actual Result Interpretation
Olfactory Nerve September 04. 2009
Can smell on both nostrils.
Cannot able to extinguish smell
Due to decrease LOC.
Optic Nerve With 20/20 vision
Without 20/20 vision.
Due to the damage of left hemisphere and decrease LOC.
Occulomotor Nerve
PERRLA PERRLA Normal
Abducens Nerve Lateral movement.
Cannot move eyes in lateral direction.
Due to the damage of left hemisphere and decrease LOC.
Trochlear Nerve Up and down movement.
Pt. cannot move eyes up and down.
Due to the damage of left hemisphere and decrease LOC.
Trigeminal Nerve For touch and pain sensation.
Pt. cannot localize sensation.
Due to the damage of left hemisphere and decrease LOC.
Facial Nerve Can smile, frown, puff the cheek and can feel the cotton.
Cannot follow specific command.
Due to the damage of left hemisphere and decrease LOC.
Acoustic Nerve Can hear on both ears.
Cannot follow specific command.
Due to the damage of left hemisphere and decrease LOC.
Glossopharengeal Can swallow. Inability to swallow due to presence of
Due to the damage of left hemisphere and

NGT. decrease LOC.
Vagus Nerve Check for gag reflex
With NGT inserted.
Due to the damage of left hemisphere and decrease LOC.
Accessory Nerve With strength on both shoulder.
With no muscle strength.
Due to the damage of left hemisphere and decrease LOC.
Hypoglossal Nerve
Sense of taste. Cannot localize taste.
Due to the damage of left hemisphere and decrease LOC.
5. Laboratory Procedures
LaboratoryProcedure
Date Done
Normal Values
Result Nursing Interpretatio
n
NursingResponsibilities
Creatine August 28, 2009
53-115.0 63.6 Normal Pretest:Explain the procedure to the patient.
Instruct the patient to wear easily manipulated clothing to get blood samples easily.
HDL 0.78-2.21 1.30 Normal Tell the pt. to relax because the procedure is painless.
Hematocrit0.37-0.54
g/l
0.44 g/l
Normal Intra-test:Instruct the patient to look away when the needle is being inserted.
Leucocytes5-10 x 10
12.4 x 10 g/l
Abnormal due to infection
Post-test:Put cotton balls
g/l weakened immune response.
on the puncture site to avoid bleeding.
Platelets150-450 x
10/l
648 x 10/l
Abnormal due to blood clot formation.
Tell the patient to rest after the test.
12.
LaboratoryProcedure
Date Done
Normal Values Result Nursing Interpretation
NursingResponsibilities
URINALYSISAugust 29, 2009
ColorStraw/ yellow amber
Yellow Normal Pre-test:Explain the procedure to the pt. and how he can cooperate.
TransparencyClear
Turbid Due to infection
Provide privacy.
Reaction4.5-8.0
6.0 Normal Intra-test:Instruct the pt. on how to get urine samples (it should be midstream/ sterile technique).
Specific Gravity1.010-1.025
1.030 Normal Tell the pt. that the procedure is painless.

SugarNegative
Albumin Negative
Negative
Positive
Normal
Due to nearly kidney damage and hypertension.
Post-test:Bring the urine samples in the
laboratory.
13.
6. Diagnostic Procedure
Diagnostic Procedure
Date Done Result Interpretation Nursing Responsibilities
Electrocardiogram Report
September 1, 09
Rhythm:Sinus
Sinus tachycardia
Post-test:Explain the procedure to the pt.and how he can cooperate.
AL:120/m
Tell him to remove all jewelry and coins.
PR:0.20 sec.
Tell him to relax and lie still.
QRS:0.40 sec.
Intra-test:Monitor for the result.
QT:0.32 sec.
Post-test:Assist the pt. when he will stand.
Axis:+250
Remind him about his jewelry
and coins or any metal he remove will he is doing the procedure.
14.
7. Anatomy and Physiology
Cerebellum
The cerebellum is involved in the coordination of voluntary motor movement, balance and equilibrium and muscle tone. It is located just above the brain stem and toward the back of the brain. It is relatively well protected from trauma compared to the frontal and temporal lobes and brain stem.
Cerebellar injury results in movements that are slow and uncoordinated. Individuals with cerebellar lesions tend to sway and stagger when walking.
Damage to the cerebellum can lead to: 1) loss of coordination of motor movement (asynergia), 2) the inability to judge distance and when to stop (dysmetria), 3) the inability to perform rapid alternating movements (adiadochokinesia), 4) movement tremors (intention tremor), 5) staggering, wide based walking (ataxic gait), 6) tendency toward falling, 7) weak muscles (hypotonia), 8) slurred speech (ataxic dysarthria), and 9) abnormal eye movements (nystagmus).

Cerebellum
The cerebrum is the part of the brain that occupies the top and front portions of the skull. It is responsible for control of such abilities as movement and sensation, speech, thinking, reasoning, memory, sexual function, and regulation of emotions. The cerebrum is divided into the right and left sides, or hemispheres.
Depending on the area and side of the cerebrum affected by the stroke, any, or all, of the following body functions may be impaired:
movement and sensation speech and language eating and swallowing vision cognitive (thinking, reasoning, judgment and memory) ability perception and orientation to surroundings self-care ability bowel and bladder control emotional control sexual ability
15.
Limbic System
The limbic system is a set of evolutionarily primitive brain structures located on top of the brainstem and buried under the cortex. Limbic system structures are involved in many of our emotions and motivations, particularly those that are related to survival. Such emotions include fear, anger, and emotions related to sexual behavior. The limbic system is also involved in feelings of pleasure that are related to our survival, such as those experienced from eating and sex.
Broca's Area
An area located in the frontal lobe usually of the left cerebral hemisphere and associated with the motor control of speech. Also called Broca's center.
Temporal Lobe
The temporal lobes are involved in the primary organization of sensory input (Read, 1981). Individuals with temporal lobes lesions have difficulty placing words or pictures into categories.

Language can be effected by temporal lobe damage. Left temporal lesions disturb recognition of words. Right temporal damage can cause a loss of inhibition of talking.
The temporal lobes are highly associated with memory skills. Left temporal lesions result in impaired memory for verbal material. Right side lesions result in recall of non-verbal material, such as music and drawings.
Parietal Lobe
Damage to the left parietal lobe can result in what is called "Gerstmann's Syndrome." It includes right-left confusion, difficulty with writing (agraphia) and difficulty with mathematics (acalculia). It can also produce disorders of language (aphasia) and the inability to perceive objects normally (agnosia).
Damage to the right parietal lobe can result in neglecting part of the body or space (contralateral neglect), which can impair many self-care skills such as dressing and washing. Right side damage can also cause difficulty in making things (constructional apraxia), denial of deficits (anosagnosia) and drawing ability.
16.
Occipital Lobe
The occipital lobes are the center of our visual perception system. They are not particularly vulnerable to injury because of their location at the back of the brain, although any significant trauma to the brain could produce subtle changes to our visual-perceptual system, such as visual field defects and scotomas. The Peristriate region of the occipital lobe is involved in visuospatial processing, discrimination of movement and color discrimination (Westmoreland et al., 1994). Damage to one side of the occipital lobe causes homonomous loss of vision with exactly the same "field cut" in both eyes.
Frontal Lobe
The frontal lobes are considered our emotional control center and home to our personality. There is no other part of the brain where lesions can cause such a wide variety of symptoms. The frontal lobes are involved in motor function, problem solving, spontaneity, memory, language, initiation, judgement, impulse control, and social and sexual behavior. The frontal lobes are extremely vulnerable to injury due to their location at the front of the cranium, proximity to the sphenoid wing and their large size.

17.
8. Pathophysiology (Patient Base)

Pathophysiology (Book Base)

9. Drug Study

Drugs Classification
Indication Side Effect Nursing Responsibilities
Generic Name: Mannitol
Brand Name:Osmitrol
Diuretic Reduction of intracranial pressure and brain mass.
Pulmonary congestion, fluid and electrolyte imbalance, electrolyte loss, dryness of mouth, thirst, marked diuresis, urinary retention, edema, headache, blurred vision, convulsions, nausea, vomiting, rhinitis, arm pain, skin necrosis, chills, dizziness, dehydration, hypotension, tachycardia, fever and angina-like chest pains.
Monitor blood pressure.
Check for hypervolemia, urinary tract obstruction and signs of fluid imbalance.
Generic Name:Hydralazine
Brand Name:Apresoline
Anti-hypertensive drug
Severe essential hypertension when the drug cannot be given orally or when there is an urgent need to lower blood pressure.
Difficulty of breathing, swelling of face, lips, tongue or throat, fast pounding heart beats, numbness, joint pain and loss of appetite.
Patient must avoid orthostatic position.
Pt. must get up slowly to avoid fall.
Monitor Bp.
Generic Name: Metropolol
Brand Name:Neobloc
Anti-hypertensive drug
Metoprolol tartrate tablets are indicated for the treatment of hypertension. They may be used alone or in combination with
Tiredness and dizziness, Shortness of breath, diarrhea and alopecia.
Metoprolol should be used with caution in patients with impaired hepatic function.

other antihypertensive agents.
Should not be given in breast feeding mother.
Generic Name: Aspirin
Brand Name:Zorprin
Anti-thrombosis Treatment of mild to moderate pain; fever; various inflammatory conditions; reduction of risk of death or MI in patients with previous infarction or unstable angina pectoris or recurrent transient ischemia attacks or stroke in men who have had transient brain ischemia caused by platelet emboli.
Nausea, vomiting, tinnitus, dizziness, respiratory alkalosis, metabolic acidosis, hemorrhage, convulsions.
Take Aspirin by mouth with or without food. If stomach upset occurs, take with food to reduce stomach irritation.
Swallow Aspirin whole. Do not break, crush, or chew before swallowing.
Take Aspirin with a full glass of water (8 oz/240 mL).
Generic Name:
Nicholin
Brand Name:
Citicoline
Cerebral circulation stimulant
Disturbances of consciousness associated with head and brain injury.
Dropped blood pressure, chest discomfort, dyspnea, nausea, headache and dizziness.
Monitor blood pressure.
Check for the correct site for injection.
21.

10. Diet and Activity
Activity Date Ordered Indication Nursing Responsibilities
Turn side to side (every 2 hrs.)
August 28, 2009 To prevent bed sores and
pneumonia.
Accompany the relative whenever mobility is done
(q2 hrs.)
Diet Date Ordered Indication Nursing Responsibilities
Osteorize feeding
August 30, 2009 To prevent aspiration (NGT).
Make sure that the NGT is intact whenever feeding is to be made.
Check for stomach content to prevent overfeeding.
23.

11. SOAPIE (actual)
Subjective“Nahihirapan siyang magsalita, kung minsan umuungol din siya, as verbalized
by Mr. D’s wife.”
Objective
Received pt. on lying position on bed, unconscious , with ongoing PNSS 1L regulated @ 10-15 gtts./min. (KVO) 200 ml. level infusing well @ left hand. (+) difficulty in speaking (+) weakness (+) headache (+) dizziness (+) blurred vision (+)Paralysis on right part of the body With NGT inserted With Foley catheter inserted
Assessment Impaired verbal communication related to impaired cerebral circulation possibly
evidence by impaired articulation.
PlanningAfter 4-6 hrs. of N.I the patient will learn techniques on how to communicate
with others.
Interventions Established rapport. Monitored and recorded vital signs. Maintained good verbal/ non-verbal means of communication. Thought the patient that loss of ability to talk does not mean loss of
intelligence. Provided time for the patient to respond. Conversation should be continue to practical and concrete matter,
supplemented with gestures, pictures, and object. Medications compliance on time (with the doctor’s permission).
Evaluation Goal met as evidence by the patient learn techniques on how to communicate non-verbal cues and in which needs are can be expressed.

24.
11. SOAPIE (potential)
Subjective:
Objective
Received pt. on lying position on bed, unconscious , with ongoing PNSS 1L regulated @ 10-15 gtts./min. (KVO) 200 ml. level infusing well @ left hand.
(+) difficulty in speaking (+) weakness (+) headache (+) dizziness (+) blurred vision (+)Paralysis on right part of the body With NGT inserted With Foley catheter inserted
Assessment Risk for aspiration related to decreased level of consciousness.
PlanningAfter 2-4 hrs. of N.I the client/ SO shall be able to identify causative factor that
may lead to aspiration.
Interventions Established rapport. Monitored and recorded vital signs. Monitored administration of NGT feeding. Checked for the NGT if intact in the stomach. Provided information about the effect of aspiration in the lung. Always keep the bed elevated whenever feeding. Keep wire cutter or scissor at bedside all the time.
Evaluation Goal partially met as evidence by the pt./SO was able to avoid factors that may
cause aspiration.

25.
13. Conclusion
We therefore conclude that CVA or stroke may lead to permanent brain
damage or death to individuals with sedentary lifestyle. People who consumed large
amount of food high in cholesterol, alcohol, cigarette smoking, obesity, and high blood
pressure can increase the possibility of stroke. This may also lead to heart disease
and maybe worsen if we don’t prevent the common factors that cause Stroke. Self
discipline is very important for us not to acquire this feared or killing disease.
26.

14. Recommendations
For the Patient and Family Members
Patient and family members should be given proper instruction and knowledge
on how to help the patient to cope in his condition. Dealing with emotional stress and
changing his sedentary lifestyle can reduce the risk of stroke. Patient way of living
should be carefully understand to limit the anxiety and self-pity. Showing emotional
and moral support can aid the anxiety and self-pity. If family members adjusted to this
kind of treatment to the patient, a fast recovery can be possibly.
For Health Care Provider/ Institutions
Cerebrovascular accident is one of the most common disease that cause dead
in the world. It can happen to anyone, especially to those of people who have
sedentary lifestyle and most commonly to people who acquired it through genes.
Though we don’t know when it will come, we have to be aware of the main factors that
bring our lives into danger. Maintaining good lifestyle and avoiding smoking, alcohol
intake, high fat and salty food, exercise, and low sugar food can decrease the possible
stroke. Health care provider and Institutions should give the enough knowledge to
everyone. Dealing with this kind of condition is one of the healthy processes of fast
recovery. It helps the patient and family members to adapt this knowledge and
behavior for the sake of the wellness of their love ones.
27.

15. Bibliography
Website source:
http://www.lancastergeneral.org/content/search.htm?inCtx9txtKeyword=CVA&inCtx9cmdKeywordSearch=search&inCtx9txtMode=site
http://www.lancastergeneral.org/content/stroke_2008_physician_chronicles.htm
http://ww2.allina.com/ac/pharmacy.nsf/
http://www.supportafterstroke.com/whatisahemorrhagicstroke.html
http://adam.about.com/reports/Stroke.htm
http://www.sciencedaily.com/releases/2008/06/080625123002.htm
http://brainmind.com/LeftHemisphere.html
http://psychology.wikia.com/wiki/Cerebrovascular_accident
http://answers.yahoo.com/question/index?qid=20070902172810AApbHou
http://healthlibrary.epnet.com/GetContent.aspx?token=af362d97-4f80-4453-a175-02cc6220a387&chunkiid=30616
http://www.neuroskills.com/search/search.php
http://dictionary.reference.com/browse/broca%27s+area?qsrc=2446
http://biology.about.com/sitesearch.htm?terms=frontal%20lobe&SUName=biology&TopNode=99
Book Source:
NANDA Book
Medical-Surgical Nursing
Anatomy and Physiology
Mims Annual
28.

The objective of the information in past and future anatomy articles is about
generalizations. My intent is not to address specifics. The objective is to provide
information and education. The left brain hemisphere, or logic brain, acts as a feature
combiner and comprehends spoken language by performing phonetic analysis of the
sounds, as opposed to the right brain method of comprehending language by matching
acoustic sound patterns. The left brain has the ability to extract isolated details from
spoken words or sentences, can generate correct spelling from scratch and can learn
from reading by reading for meaning even if the topic is dull. Where the right brain lacks
the short-term memory capabilities to be able to follow long sentences and extract their
meanings, the left hemisphere can. If a sentence is long and complex grammatically, it
falls into the realm of the left hemisphere for comprehension and de-coding for meaning.
The left hemisphere is able to work with both slow and rapid speech where the right brain
can only deal effectively with slow speech. Complex syntax, semantics, phonics, sight
words, new vocabulary (read or heard) are all shuttled to the left brain for comprehension.
The left brain is also where re-worded sentences or explanations, even if redundant, are
processed. The information processing that one hemisphere isn’t capable of processing is
switched to the other via the corpus callosum. The left hemisphere’s speaking and
listening vocabulary is almost as large as that for reading and sight and allows it to be
able to equally extract meaning from written or spoken words. When we read and hear
the words in our head, they’re formed (sub-vocalized) in the left brain because it, and not
the right hemisphere, has the ability to de-code written words acoustically. The left brain
doesn’t have the ability to handle ambiguity (needs absolutes, clear cut patterns and
predictability), doesn’t handle receiving input from changing sources, doesn’t do well if
required to make changes in solution strategies or changes in timing of responses. Left is
the logical and analytical side and processes information in a sequential manner. It works
best with life and projects when they’re presented in a planned and structured manner.
It’s the side that works best with multiple choice questions, prefers authority structuring,
controls feelings, is future oriented and time conscious, sees distinct right or wrong
according to the prevailing cultural/beliefs system and discerns sharp perceptual and
conceptual boundaries. This makes the left brain more involved in seeing differences
when dealing with others who are felt to be of lower caste or intelligence. Even though the
left brain prefers talking and writing it’s also the hemisphere that’s more likely to suspect
everyone and alienate friends. Those who are left brain dominant are more likely to buy,
buy, buy, test the limits of credit cards (and their ability to pay) clean everything, buy

everything and stock up for suspected or unknown eventualities, reorganize shelves,
cupboards, retrace their steps and reorganize shelves, etc. perpetually. They’re also
more likely to quit their job before being fired. If we go back and review the information on
all aspects of the brain it’s easy to see why we have differences and difficulties.
Fortunately, few of us are totally dominated by one hemisphere or the other. If that were
the case it would be a world of, “In this corner are the right brainers and in this corner the
lefties. Prepare your agendas and come out fighting.” Which, by the way, is how we seem
to handle most difficult problems anyway? All of us are endowed with two sides of the
brain and a way for the information to travel from one hemisphere to the other. The brain
is the area that heredity can be the largest or smallest factor in the way we interpret life
around us. If we don’t like our life and our health, the brain gives us the means with which
to change. The choices are also up to one of the brain’s functions but the mind and the
brain aren’t the same.





























