Embed Size (px)
Citation preview

CEREBRAL PALSYReported By:
FELVEE M. BASIBAS, PTRP MD

CEREBRAL PALSY
Three part definition: A disorder of movement and posture Caused by a non-progressive injury To the immature brain
Change in muscle tone and posture, both at rest and with voluntary activity.
First year or two of life – included in most definitions
Upper age limit of postneonatal brain insult- unclear

CP: EPIDEMIOLOGY
One of the most common disabling conditions affecting children.
1-2.3/1,000 live births Diagnosis is not made at any specific
age Can resolve in up to 50% of children
diagnosed prior to 2 years of age Or the brain insult might not occur
until later in childhood.
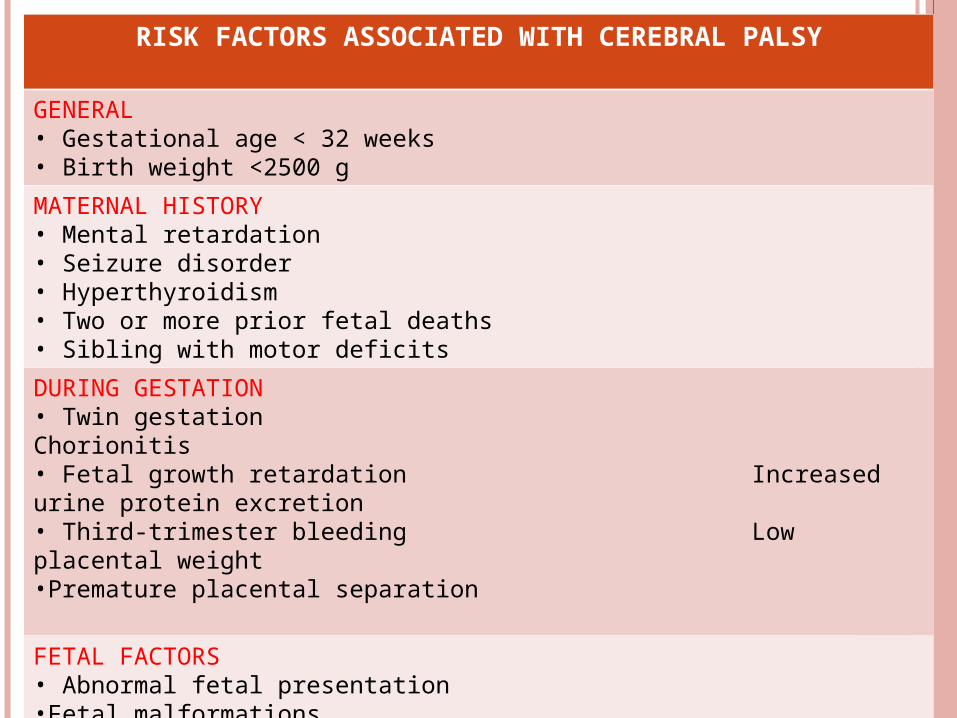
RISK FACTORS ASSOCIATED WITH CEREBRAL PALSY
GENERAL • Gestational age < 32 weeks• Birth weight <2500 g
MATERNAL HISTORY• Mental retardation• Seizure disorder• Hyperthyroidism• Two or more prior fetal deaths• Sibling with motor deficits
DURING GESTATION• Twin gestation Chorionitis • Fetal growth retardation Increased urine protein excretion • Third-trimester bleeding Low placental weight•Premature placental separation
FETAL FACTORS• Abnormal fetal presentation•Fetal malformations•Fetal bradycardia•Neonatal seizures

CP: ETIOLOGY
Brain injury can occur in the following periods:a. Prenatalb. Perinatalc. Postnatal
PRENATAL PERIOD- wherein most causes of CP occur. TORCH infections Intrauterine stroke Genetic malformations
The most common currently understood causes are related to brain injury occurring in children born prematurely.
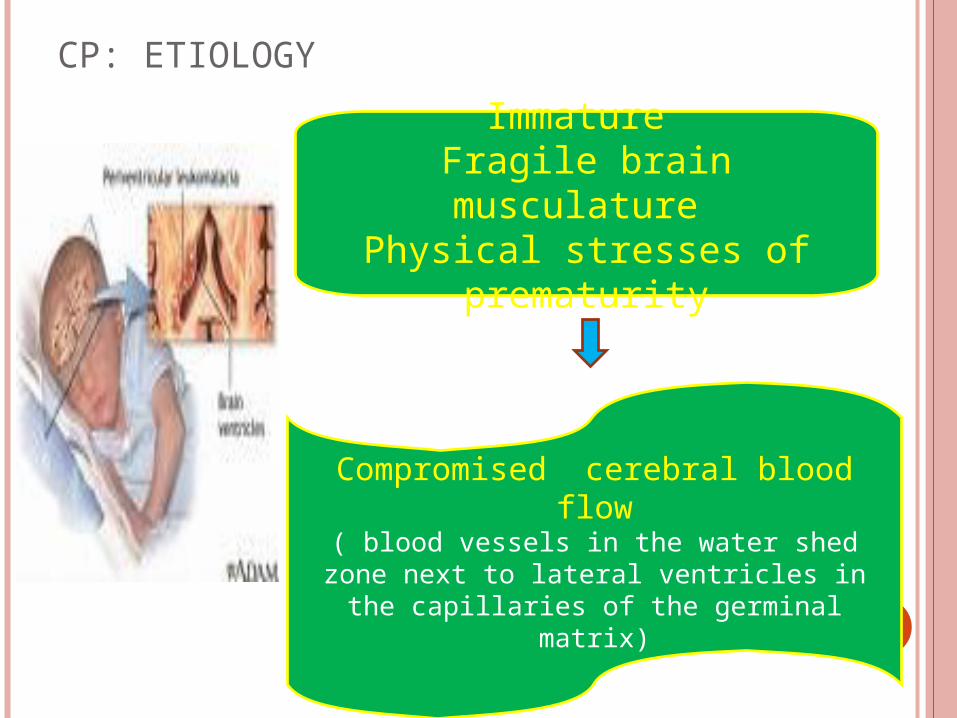
CP: ETIOLOGY
Immature Fragile brain musculature
Physical stresses of prematurity
Compromised cerebral blood flow( blood vessels in the water shed zone next to lateral ventricles in the capillaries of the
germinal matrix)

INTRAVENTRICULAR HEMORRHAGE
Bleeding is arterial in origin Transfontanelle cerebral high-resolution UTZ

Grades of Intraventricular Hemorrhage in the Premature Brain
GRADE HEMORRHAGE
1 Isolated to germinal matrix
2 With normal ventricular size
3 With ventricular dilatation
4 With parenchymal hemorrhage

Very LBW infants – increased risk of periventricular hemorrhagic infarction
Periventricular hemorrhagic infarction Hemorrhagic necrosis lateral to the external angle of
the lateral ventricle. Of venous origin Usually asymmetric With healing – Periventricular leukomalacia ( PVL)
can develop. PVL
One of the strongest predictors of CP in the premature neonate.
Almost always associated with a history of prematurity.

PVL
Extremely LBW infants:Are also at increased
risk of CP.Especially with a history
of resuscitation and prolonged ventilation.
Protective factors: prenatal care and steroids.

CP IN TERM INFANTS
Almost ½ of children with CP were born term.
Cause of brain injury is often elusive. Severe anoxic/ischemic brain injury:
Mechanical difficulties of the placentaUmbilical cordActual delivery itself
Intrapartum asphyxiaMust be severe and prolonged to cause
CP.More global and more severe disability.

ETIOLOGY: ATHETOID CP
Injury to the basal ganglia.
Hyperbilirubinemia. Hearing loss. Incidence has declined
since testing and treatment for Rh incompatibility
Now, relatively rare

ETIOLOGY: POSTNATAL CEREBRAL INJURY AND CP
Major causes:CNS infectionsVascular causesHead injury
Other Causes:AnoxiaIschemiaInflammation

CLASSIFICATION OF CP
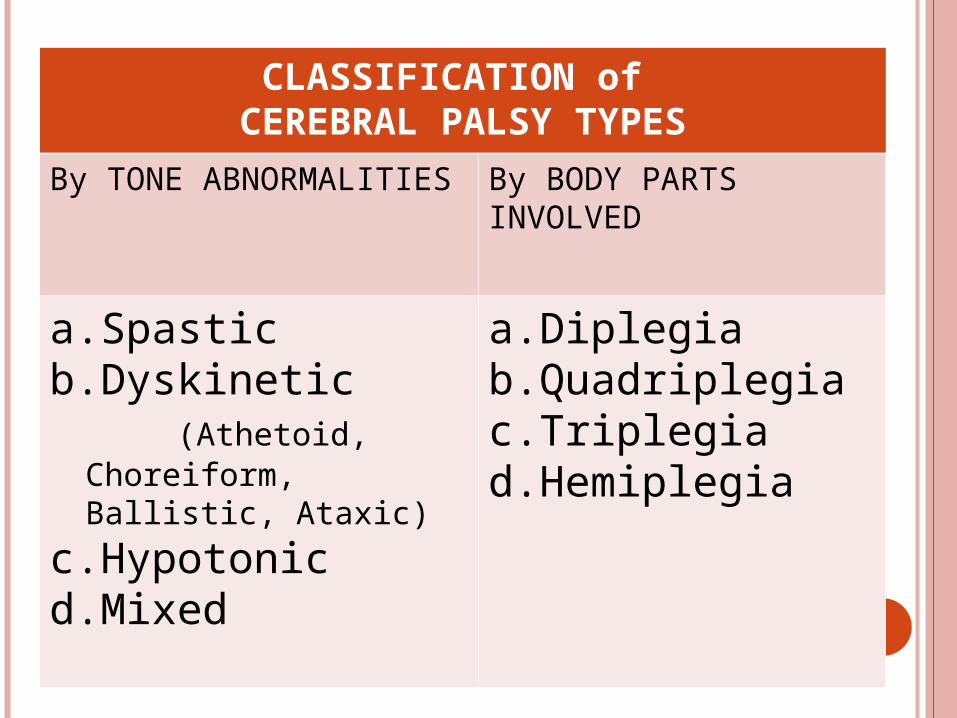
CLASSIFICATION of CEREBRAL PALSY TYPES
By TONE ABNORMALITIES By BODY PARTS INVOLVED
a.Spasticb.Dyskinetic (Athetoid,
Choreiform, Ballistic, Ataxic)
c.Hypotonicd.Mixed
a.Diplegiab.Quadriplegiac.Triplegiad.Hemiplegia
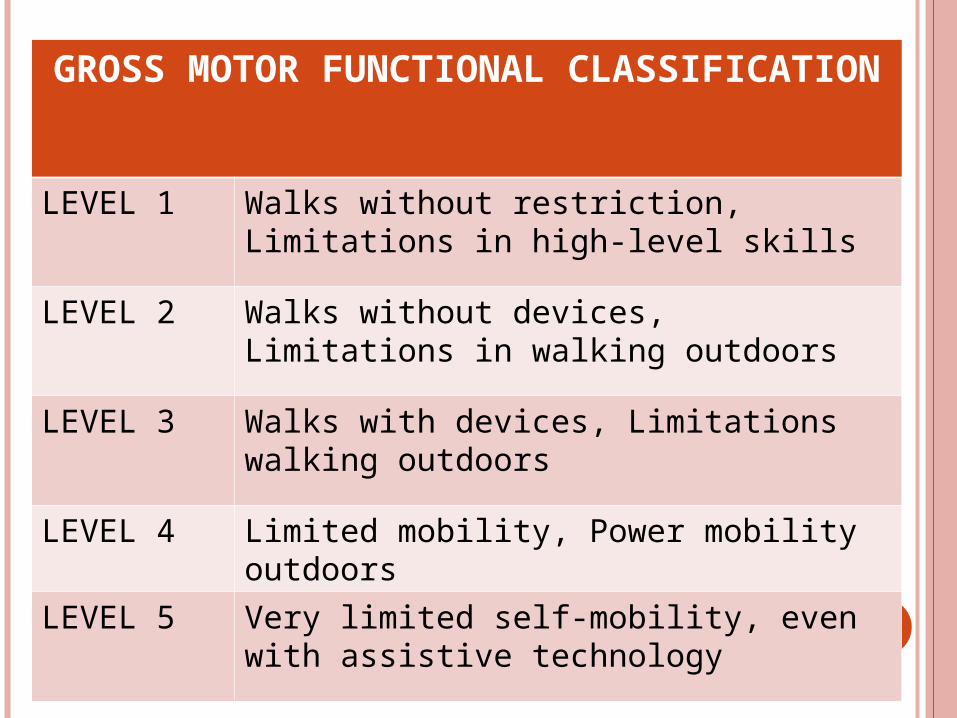
GROSS MOTOR FUNCTIONAL CLASSIFICATION
LEVEL 1 Walks without restriction, Limitations in high-level skills
LEVEL 2 Walks without devices, Limitations in walking outdoors
LEVEL 3 Walks with devices, Limitations walking outdoors
LEVEL 4 Limited mobility, Power mobility outdoors
LEVEL 5 Very limited self-mobility, even with assistive technology
SPASTIC SUBTYPE Most common 75% of children with CP Spasticity:
Velocity-dependent increased toneAssociated with UMN syndrome
findings Increased muscle stretch reflexesBabinski responseWeaknessDifficulty with coordination.
Can be associated with extensor or flexor posturing ( decerebrate and decorticate posturing)

DYSTONIA A dyskinetic tone abnormality With alternating tone or cocontraction in the
antagonist and agonist muscle groups Causing varied abnormal postures and often
fluctuating tone. Other dyskinetic forms:
1. Athetosis2. Choreiform3. Choreoathethoid

ATHETOSIS
Involuntary constant rotatory or writhing movements of the distal extremities.
Basal ganglia involvement.
Stop during sleep. Incidence has been
reduced by the advent of treatment for Rh incompatibility.
ATAXIC TYPE
Rare Must be
differentiated from degenerative processes of the cerebellum.

MIXED TYPE
Spasticity + Dystonia
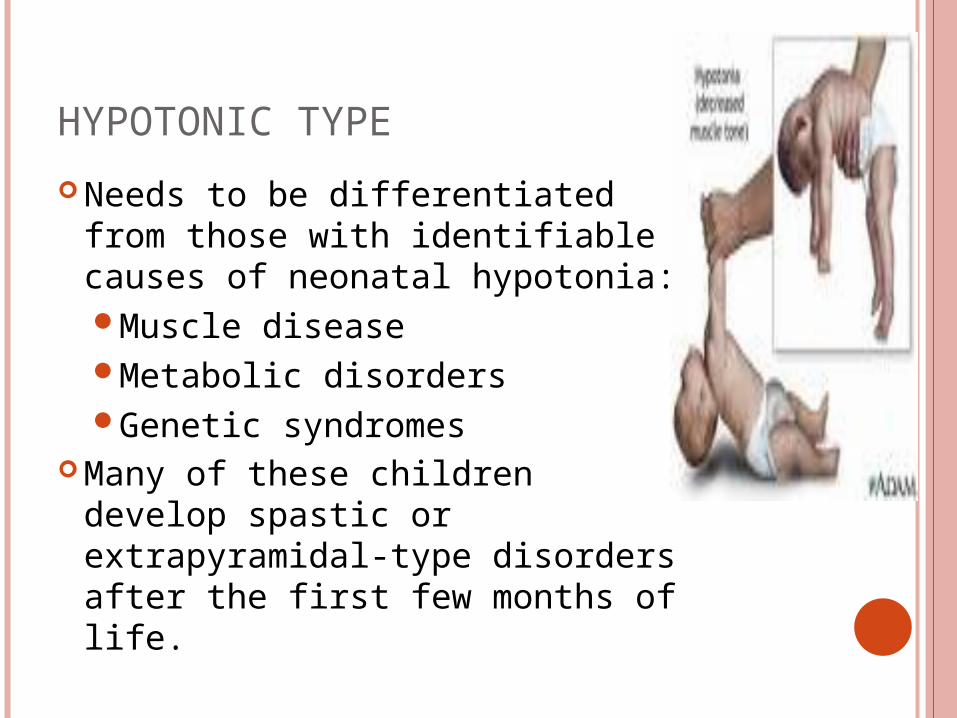
HYPOTONIC TYPE
Needs to be differentiated from those with identifiable causes of neonatal hypotonia:Muscle diseaseMetabolic disordersGenetic syndromes
Many of these children develop spastic or extrapyramidal-type disorders after the first few months of life.
CLINICAL EFFECTS

a. Hypotonia and motor delay- often seen as early signs of CP.
b. UMN injury features Positive findings
Increased tone and reflexes
Positive Babinski’s reflex
Negative findings Reduced strength Selective motor control Balance and
coordination.
c. Tone in the extremities
d. Retention of Primitive Reflexes
e. Irritabilityf. Lethargyg. Weak suck with
tongue thrusth. Poor head controli. High-pitched cryj. Oral hypersensitivityk. Tonic bitel. Asymmetric
movementsm. Unusual posturing

n. Rolling for mobilityo. Combat crawlingp. W sittingq. Bunny hopping r. Adopting a hand
preference before the first birthday
s. Trunk or central hypotonia
t. Muscle weaknessu. Abnormal posturingv. Sensory deficits
Contractures Deformities Kyphosis Scoliosis Respiratory
compromise Atlantoaxial
instability Foot deformities

ASSOCIATED MEDICAL AND FUNCTIONAL PROBLEMS
a. Visual Sequelae Strabismus Exotropia/ Esotropia Hemianopsia Retinopathy of prematurity
b. Hearing impairment Ototoxic drug exposure Hyperbilirubinemia TORCH infections in utero

c. Abnormalities of oral motor function Due to weakness and incoordination
of lips, tongue and masticatory and facial muscles.
Drooling, dysphagia and dysarthria Treatments:
Behavioral techniques Speech therapy Anticholinergic medications Botulinium toxin A injections Surgical redirection of the salivary
ducts
d. Dysphagia A problem in the following:
Oral Phase (chewing and bolus preparation)
Laryngeal Phase (propulsion and airway protection problems)
Aspiration - ischemia

e. Undernutrition/ Malnutrition 1/3 of patients with Hemiplegia and
Diplegia (undernourished) > 2/3 of patients with Quadriplegia
(undernourished) 27% of patients – malnourished Treatment:
Gastrostomy Gastrojejunostomy tube
f. GI Symptoms:1. Gastroesophageal reflux
Can result to episodic emesis Interferes with adequate nutrition
and growth Treatment:
a. Medicationsb. Surgical: Nissen fundoplication
or Jejunostomy
2. Chronic constipation Neuromuscular control of the bowel Exaggerated by immobility and
abnormal diet and fluid intake Anorectal manometry Complications:
Large bowel megacolon Volvulus
Treatment: Increase activity Increase fluid and fiber intake
medications

g. Urinary Symptoms: 1/3 of patients – frequency,
incontinence or difficulty urinating. Detrussor instability, vesicoureteric
reflux, DSD

h. Cognitive Impairments: 30% of patients- mental retardation Risk is directly proportional to
severity of motor disability. 20-30% - have specific learning
disabilities 40-50% of Normal BW CP- cognitive
abnormalities

i. Seizure Disorders 1/3 of children with CP Hemiplegic> Quadri > Diplegic Reflects a greater extent of cortical
brain injury Treatment:
Antiseizure techniques Grid mapping and resection of
seizure foci.

j. Osteoporosis Secondary to the following factors:
Feeding difficulties – deficient Ca and Vit D Decreased weight bearing/ Immobilization Muscle stresses Antiseizure meds Weight percentile/ Low triceps skinfold
Treatment: Ca and Vit D supplementation Bisphosphonates (Pamindronate)
Bone age was not found to be significantly different than chronologic age in children with CP

k. Pain Can go undiagnosed and untreated
in patients who are non-verbal. Increased in patients in GMFCS
Levels 3-5 Frequency is correlated with the
following: Severity of motor impairment Presence of gastrostomy Days of schools missed Days spent in bed

l. Mortality Risk factors:
Lack of independent mobility such as rolling
Use of tracheostomy
Lack of any hand function
Prevention: Teach basic life skills (feeding and mobility)
Predictors of survival:Cognitive levelAbility to speakAbility to recognize voices
Ability to interact with persons
Physical activity and mobility
Tube feedingIncontinenceSeizures

m. MorbidityInjuries, abuse and neglect

FUNCTIONAL PROGNOSIS

FUNCTIONAL PROGNOSIS
Children typically develop motor skills craniocaudally.
The age at which these skills are developed help to predict the eventual outcome.
75% of spastic CP eventually ambulate 85% in diplegics 70% in quadriplegics

PROGNOSIS FOR AMBULATION
Hemiplegics/ Ataxic pxs
Achievement of all motor skills by age of 8.
Independent sitting before 2 years
Persistence of fewer than 3 of the primitive reflexes at age 18 months.
Quadriplegics Did not attain
independent sitting by age 4.
Persistence of primitive reflexes beyond 18 months
GOOD Prognosis POOR Prognosis
CHARACTER
Inefficient gaitShorter step lengthDecreased ROM of the
hips and knees Increased energy
expenditure Decreased velocity Decreased endurance

OUTCOME MEASURES

OUTCOME MEASURES FOR CEREBRAL PALSY REHABILITATION
OUTCOME OF INTEREST
MEASURE
SPASTICITY Ashworth ScoreTardieu angles
RANGE of MOTION Goniometer
DYSTONIA Barry Albright Dystonia Scale
SRENGTH Medical Research Council Muscle Grade (0-5)Modified SphygmomanometerHydraulic Strength or TorqueMaximun 10 Repetitions Weight Lift
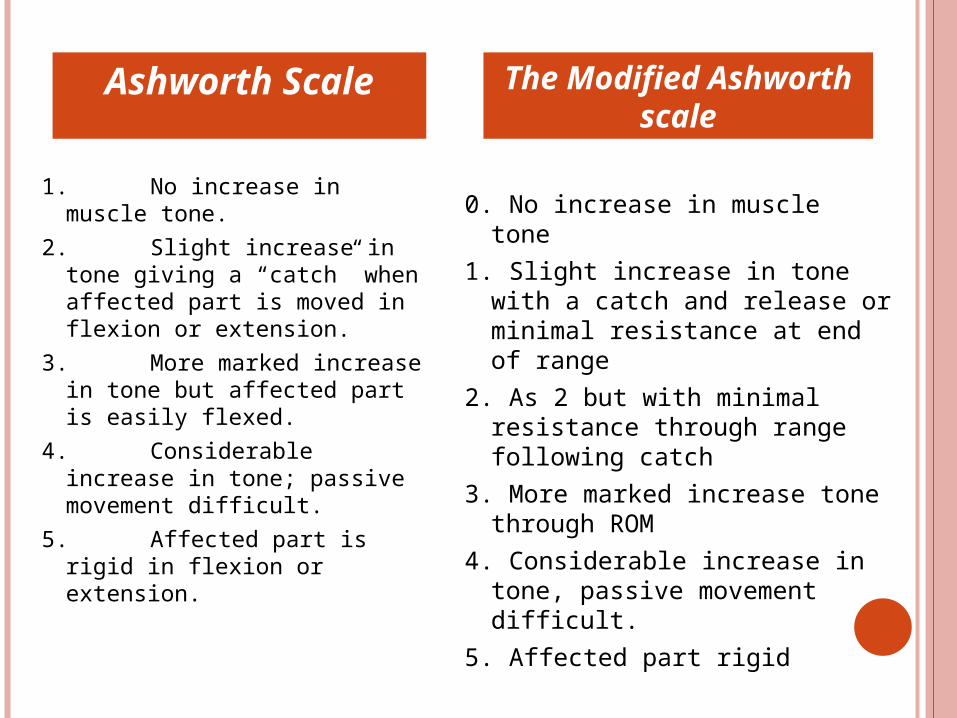
1. No increase in muscle tone.
2. Slight increase in tone giving a “catch” when affected part is moved in flexion or extension.
3. More marked increase in tone but affected part is easily flexed.
4. Considerable increase in tone; passive movement difficult.
5. Affected part is rigid in flexion or extension.
0. No increase in muscle tone
1. Slight increase in tone with a catch and release or minimal resistance at end of range
2. As 2 but with minimal resistance through range following catch
3. More marked increase tone through ROM
4. Considerable increase in tone, passive movement difficult.
5. Affected part rigid
Ashworth Scale The Modified Ashworth scale

OUTCOME MEASURES FOR CEREBRAL PALSY REHABILITATION
OUTCOME OF INTEREST
MEASURE
COGNITION IQ
SPEECH Intelligibility
HEALTH Short Form 12 or 36
SOCIAL AND SELF-CARE SKILLS
WeeFIM, Pediatric Outcomes Data CollectionInstrumentCanadian Occupational Performance Measure
PAIN Faces Pain Scale Non-Verbal Pain Scale

OUTCOME MEASURES FOR CEREBRAL PALSY REHABILITATION
OUTCOME OF INTEREST
MEASURE
COMMUNITY INTEGRATION
Child Health QuestionnaireDemographics, Craig Handicap Assessment and Reporting Technique
HAND and ARM FUNCTION
Melbourne Upper Extremity TestQuality of Upper Extremity Skills Test
GROSS MOTOR FUNCTION
Gross Motor Function MeasurePeabody Scales of Infant Development
GAIT Velocity, stride length, balanceOxygen costKinetics or kinematics on gait analysis

THERAPEUTIC MANAGEMENT
GOALS OF REHABILITATION (MOLNAR)
1. To decrease complications of CP.2. To enhance or improve acquisition of
new skills.
ADDITIONAL GOALS by ROTHERY and Colleagues:
1. Parent and caregiver education2. Decrease skeletal deformity3. Improve mobility

EARLY INTERVENTION
“ Early institution of physical therapy can decrease the impact of the brain injury in the development of CP”. – Kong
The rationale for early intervention is closely connected to concepts that stress the importance of the early years for normally developing children, and the role that environmental factors play in the development.

2 Main models for the delivery of Developmental Early Intervention:1. Direct Therapy Service Model2. Consultation Model

THERAPY APPROACHES
I. Integrated Therapy Programs in SchoolII. Caregiver Participation/ Home TherapyIII. Physical TherapyIV. Individual Therapy Programs
Speech Therapy Occupational Therapy
V. Conductive EducationVI. Constraint-induced or Forced Use
TherapyVII. FES and BiofeedbackVIII.TES

CONDUCTIVE EDUCATION
Intervention that melds educational theory and PT.
A mode of therapy that integrates rhythmic movement and activities in a group setting, with a class leader.
Improvement in functional skills such as toileting for children in conductive education programs versus those in regular school therapy.

CONSTRAINT-INDUCED OR FORCED USE THERAPY
Has promise and supports the theory of motor plasticity.
Restrains the sound limb to increase the use of the affected side.
Gains in the areas of motor performance were maintained up to 6 months post intensive training in one study.

THERAPEUTIC ELECTRICAL STIMULATION
Use of low-voltage, high frequency ES. Increase blood flow and improve
muscle growth and strength.
MEDICAL AND SURGICAL MANAGEMENT

MANAGEMENT OF HYPERTONIA
Oral Medicationsa. Baclofenb. Dantrolenec. Diazepam
Specific Medications for Dystonia:a. Trihexyphenidyl HClb. Levodopa-carbidopa (Sinemet)
Botox Injections Phenol Injection
Reappraisal of spasticity or hypertonia in a growing child with CP every 6 months is necessary.
BOTULINIUM TOXIN TYPE A (BOTOX) Effective in improving ROM and reducing tone. Also effective in improving motor control. Best results: Botox + Serial casting Indications for Use of Botox:
a. Calf injection for dynamic equinus persistent throughout the gait cycle
b. Hamstring injection for dynamic knee flexionc. Adductor injection for scissoringd. Diagnostic measures before surgerye. Management of focal limb dystoniaf. Analgesia for pain and spasm in the perioperative
periodg. In the UE, persistent thumb in palm, wrist posture
preventing hand use, and elbow flexion.

NEUROSURGICAL INTERVENTIONS
I. Selective Dorsal Rhizotomy (SDR)II. Intrathecal Baclofen (ITB) PumpIII. Stereotactic ablation of selected
thalamic nucleiIV. Chronic ES of the Cerebellum or
Posterior Columns Has shown promise in adults with
dystonia.
SELECTIVE DORSAL RHIZOTOMY (SDR)
Since 1980’s Reduces spasticity by interrupting the sensory
input in the dorsal horn. Ideal Candidates for SDR:
1. Premature child with spastic diplegia.2. Good balance3. Good selective motor skills4. Aged 4 or 5 years5. With minimal contactures6. Able to walk unassisted
Athetosis – contraindication for SDR Dystonia – can become more problematic post
SDR
Candidates for rhizotomy usually are already involved in an active physical therapy program.
Because the procedure involves intensive follow-up therapy, children who can understand and follow directions generally are ideal candidates.

Two groups of children who benefit from selective dorsal rhizotomy:1. Spastic Diplegics (Borderline
ambulators) The goals of surgery : better gait and
leg function2. Severe Spastic Quadriparetics
increase their independence by allowing them to sit for longer periods of time, use a potty seat, or power a wheelchair on their own.

INTRATHECAL BACLOFEN
In addition to spasticity reduction, it also has impact on dystonia.
Complications with ITB are as high as 50%.Improvements in technology
with catheters and pumps might reduce the mechanical risk.
Experience in management.Abrupt withdrawal in children
must be treated aggressively.

ORTHOPEDIC INTERVENTION
Nearly all children with CP develop an abnormality of physical form and/or function.
Children with CP should have regular orthopedic consultations.
If pain or discomfort is present, especially around the hip, surgical relief may be necessary.

THANK YOU




