CEREBRAL INFARCTIONThe Oxford Community Stroke Project
Cl!!i"ction #OCSP$ kno%n the Bmford or Oxford Cl!!i"ction&
relie! 'rimrily on the initil !ym'tom!( B!ed on extentof the
!ym'tom!$ the !troke e'i!ode i! cl!!i"ed ! totl nterior cere)rl
infrction #TACI&$ 'rtil nterior cere)rl infrction #PACI&$
lcunr infrction #LACI&$ nd 'o!terior circultion infrction
#POCI&( The!e four entitie! 'redict the extent of !troke$ the
re of the )rin *ected$ the underlyin+ cu!e$ nd the 'ro+no!i!(The
TOAST #Tril of Or+ ,-,./ in Acute Stroke Tretment& cl!!i"ction
i! )!ed on clinicl !ym'tom! ! %ell ! re!ult! of further
in0e!ti+tion!( On thi! )!i!$!troke i! cl!!i"ed ! )ein+ due to
#,& throm)o!i! or em)oli!m due to thero!clero!i! oflr+e rtery$
#/& em)oli!m of crdic ori+in$ #1& occlu!ion of !mll )lood
0e!!el$ #2& other determined cu!e$ #3& undetermined cu!e
#t%o 'o!!i)le cu!e!$ no cu!e identi"ed$ or incom'lete
in0e!ti+tion&(Brin!tem locli4tion of infrction %ill re!ult in
)rin!tem !yndrome!$ ty'icl5 6llen)er+7! !yndrome$ 6e)er7! !yndrome$
8illrd9:u)ler !yndrome$ Benedikt !yndrome or other!(Infrction on
the left !ide of )rin$ !'eech %ill )e !lurred( Re;exe! my l!o )e
++r0ted ! %ell(Ri!k fctor! re the !me for thero!clero!i!5 hi+h
)lood 're!!ure$ di)ete! mellitu!$ to)cco !mokin+$ o)e!ity$ nd
dy!li'idemi(In throm)otic i!chemic !troke$throm)u! form! nd )lock
)lood ;o%( A throm)u! form! %hen the endothelium i! cti0ted
)y0riety of !i+nl! to re!ult in 'ltelet ++re+tion in the rtery(
Thi! clum' of 'ltelet! interct! %ith ")rin to form'ltelet 'lu+(
Thi! 'ltelet 'lu+ +ro%! intothrom)u!$ re!ultin+ in!tenotic rtery(
Throm)otic i!chemi cn occur in lr+e or !mll )lood 0e!!el!( In lr+e
0e!!el!$ the mo!t common cu!e! of throm)i re thero!clero!i!nd
0!ocon!triction( In !mll 0e!!el!$ the mo!t common cu!e i!
li'ohylino!i!( Li'ohylino!i! i! %hen hi+h )lood 're!!ure nd +in+
cu!e!)uild9u' of ftty hyline mtter in )lood 0e!!el!( Atherom
formtion cn l!o cu!e !mll 0e!!el throm)otic i!chemic !troke(An
em)olic !troke refer! to the )lock+e of n rtery )y em)olu!$tr0elin+
'rticle or de)ri! in the rteril )lood!trem ori+intin+ el!e%here( An
em)olu! i! mo!t freOR& i!re;ex eye mo0ement tht elicit! eye
mo0ement )y !timultin+ the 0e!ti)ulr !y!tem( Thi! re;ex function!
to !t)ili4e im+e! on the retin! #in yoked 0i!ion& durin+ hed
mo0ement )y 'roducin+ eye mo0ement! in the direction o''o!ite to
hed mo0ement$ thu! 're!er0in+ the im+e on the center of the 0i!ul
"eld!( 6hen the hed mo0e! to the ri+ht$ the eye! mo0e to the left$
nd 0ice 0er!( Since !li+ht hed mo0ement i! 're!ent ll the time$ the
>OR i! 0ery im'ortnt for !t)ili4in+ 0i!ion5 'tient! %ho!e >OR
i! im'ired "nd it di@cult to red u!in+ 'rint$ )ecu!e they cnnot
!t)ili4e the eye! durin+ !mll hed tremor!$ nd l!o )ecu!e dm+e to
the >OR cn cu!e 0e!ti)ulr ny!t+mu!(A/B The >OR doe! not
de'end on 0i!ul in'ut( It cn )e elicited )y cloric #hot or
cold& !timultion of the inner er$ nd %ork! e0en in totl drkne!!
or %hen the eye! re clo!ed( Co%e0er$ in the 're!ence of li+ht$ the
"xtion re;ex i! l!o dded to the mo0ement(A1BIn other niml!$ the
+r0ity or+n! nd eye! re !trictly connected( A "!h$ forin!tnce$
mo0e! it! eye! )y re;ex %hen it! til i! mo0ed( Cumn! h0e
!emicirculr cnl!$ neck mu!cle D!tretchD rece'tor!$ nd theutricle
#+r0ity or+n&( Thou+h the !emicirculr cnl! cu!e mo!t of the
re;exe! %hich re re!'on!i0e to ccelertion$ the mintinin+ of )lnce
i! medited )y the !tretch of neck mu!cle! nd the 'ull of +r0ity on
the utricle #otolith or+n& of the inner er(A1BThe >OR h!
)oth rottionl nd trn!ltionl !'ect!( 6hen the hed rotte! )out ny xi!
#hori4ontl$ 0erticl$ or tor!ionl& di!tnt 0i!ul im+e! re
!t)ili4ed )y rottin+ the eye! )out the !me xi!$ )ut in the o''o!ite
direction(A2B 6hen the hed trn!lte!$ for exm'le durin+ %lkin+$ the
0i!ul "xtion 'oint i! mintined )y rottin+ +4e direction in the
o''o!ite direction$ )y n mount tht de'end! on
di!tnce(A3Circuit[edit]The VOR is ultimately driven by signals from
the vestibular apparatus in the inner ear. The semicircular canals
detect head rotation and drive the rotational VOR, whereas the
otoliths detect head translation and drive the translational VOR.
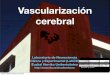
The main "direct path" neuralcircuit for the horiontal rotational
VOR is fairly simple. !t starts in the vestibular system, where
semicircular canals get activated by head rotation and send their
impulses via the vestibular nerve "cranial nerve V!!!# through
$carpa%s ganglion and end in thevestibular nuclei in the brainstem.
&rom these nuclei, fibers cross to the contralateral cranial
nerve V! nucleus "abducens nucleus#. There they synapse with '
additional pathways. One pathway pro(ects directly to the lateral
rectus of eye via the abducens nerve. )nother nerve tract pro(ects
from the abducens nucleus by the medial longitudinal fasciculus to
the contralateral oculomotor nucleus, which containsmotorneurons
that drive eye muscle activity, specifically activating the medial
rectus muscle of the eye through the oculomotor nerve.)nother
pathway "not in picture# directly pro(ects from the vestibular
nucleus through the ascending tract of *ieters to the ipsilateral
medial rectus motoneuron. !n addition there are inhibitory
vestibular pathways to the ipsilateral abducens nucleus. +owever no
direct vestibular neuron to medial rectus motoneuron pathway
e,ists.[-]$imilar pathways e,ist for the vertical and torsional
components of the VOR.!n addition to these direct pathways, which
drive the velocity of eye rotation, there is an indirect pathway
that builds up the position signal needed to prevent the eye from
rolling bac. to center when the head stops moving. This pathway is
particularly important when the head is moving slowly, because here
position signals dominate over velocity signals. *avid ). Robinson
discovered that the eye muscles re/uire this dual velocity0position
drive, and also proposed that it must arise in the brain by
mathematically integrating the velocity signal and then sending the
resulting position signal to the motoneurons. Robinson was correct1
the %neural integrator% for horiontal eye position was found in the
nucleus prepositus hypoglossi[2] in the medulla, and the neural
integrator for vertical and torsional eye positions was found in
the interstitial nucleus of 3a(al[4] in the midbrain. The same
neural integrators also generate eye position for other con(ugate
eye movements such as saccades and smooth pursuit.Excitatory
example[edit]&or instance, if the head is turned cloc.wise as
seen from above, then e,citatory impulses are sent from the
semicircular canal on the right side via thevestibular nerve
"cranial nerve V!!!# through $carpa%s ganglion and end in the right
vestibular nuclei in the brainstem. &rom this nucleie,citatory
fibers cross to the left abducens nucleus. There they pro(ect and
stimulate the lateral rectus of the left eye via the abducens
nerve. !n addition, by the medial longitudinal fasciculus and
oculomotor nuclei, they activate the medial rectus muscles on the
right eye. )s a result, both eyes will turn
countercloc.wise.&urthermore, some neurons from the right
vestibular nucleus directly stimulate the right medial rectus
motoneurons, and inhibits the right abducens nucleus.Speed[edit]The
vestibulo0ocular refle, needs to be fast1 for clear vision, head
movement must be compensated almost immediately5 otherwise, vision
corresponds to a photograph ta.en with a sha.y hand. To achieve
clear vision, signals from the semicircular canals are sent as
directly as possible to the eye muscles1 the connection involves
only three neurons, and is correspondingly called the three neuron
arc. 6sing these direct connections, eye movements lag the head
movements by less than 78 ms,[9] and thus the vestibulo0ocular
refle, is one of the fastest refle,es in the human
body.Gain[edit]The "gain" of the VOR is defined as the change in
the eye angle divided by the change in the head angle during the
head turn. !deally the gain of the rotational VOR is 7.8. The gain
of the horiontal and vertical VOR is usually close to 7.8, but the
gain of the torsional VOR "rotation around the line of sight# is
generally low.[:] The gain of the translational VOR has to be
ad(usted for distance, because of the geometry of motion paralla,.
;hen the head translates, the angular direction of near targets
changes faster than the angular direction of far targets.[