Embed Size (px)
Citation preview

CEREBRALCIRCULATION ANDMETABOLISMIN PULMONARYEMPHYSEMAANDFIBROSIS WITH OBSERVATIONSON
THE EFFECTSOF MILD EXERCISE1
By P. SCHEINBERG, I. BLACKBURN,M. SASLAW, M. RICH, AND G. BAUM
(From the Department of Physiology, University of Miami School of Medicine, the Departntof Medicine, Veteran's Administration Hospital, Coral Gables, Fla., and the
Nationa Children's Cardiac Hospital, Miami, Fla.)
(Submitted for publication' November 21, 1952; accepted February 11, 1953)
Chronic pulmonary disease, particularly em-physema and fibrosis, may result in variable al-terations in blood oxygen and carbon dioxide ten-sions, depending upon the severity of the disease.Changes in carbon dioxide and oxygen tensionshave been shown to have a profound influence oncerebral circulation in acute experiments on nor-mal subjects (1). Recently Patterson, Heyman,and Duke (2) demonstrated that cerebral bloodflow was increased above normal in a group ofsubjects with severe chronic pulmonary emphy-sema, most of whomhad cor pulmonale and werein congestive heart failure. Their studies re-em-phasized the importance of the influence of bloodcarbon dioxide and oxygen tensions on cerebralblood flow, even though the alterations in the ten-sions of these gases were chronic. Their patientsall had advanced' pulmonary disease, however, andit was felt that it would be of interest to studythe effects of less severe pulmonary disease, andless profound and more variable alterations inblood gas tensions, on the cerebral physiology.Most of these patients were studied before andduring moderate exercise, since mental statuschanges are known to occur in some patients withchronic pulmonary disease during exertion.
METHODS
Cerebral blood flow studies were carried out by meansof a modification (3) of the original nitrous oxide tech-nique (4) on 9 of 22 subjects with chronic pulmonary dis-ease. The original nitrous oxide technique with intermit-tent sampling was used in the other 13 patients. Twentyof the patients had chronic pulmonary emphysema of vary-ing severity, confirmed by history, physical examination,radiographic and fluoroscopic studies, and, in most cases,
1 This investigation was supported by research grants(H-832 and H-832C) from the National Heart Instituteof the National Institutes of Health, Public HealthService.
by an estimation of maximal breathing capacity, vitalcapacity, and air velocity index (5). Two patients hadpulmonary fibrosis without evidence of significant ob-structive phenomena in the lungs, and this was confirmedby the finding of a normal air velocity index in these twosubjects (S. A. and J. G., Table I). Electrocardiogramswere made on all subjects but one (G. W.), and showedconfirmatory evidences of cor pulmonale in 10 of the sub-jects. Eight of the subjects with cor pulmonale showedevidences of heart failure (though only one, C. A., was insevere failure) at the time of admission. The diagnosisof cor pulmonale in these patients was made by clinicalfindings, electrocardiographic changes, and chest fluoros-copy (evidences of enlargement of the right ventricularoutflow tract). The patients were not studied until clini-cal evidences of congestive failure had disappeared onappropriate management, and none of the patients wasstudied during the acute stages of the illnesses whichprecipitated their admission, usually bronchiolar or pul-monary infections. In this way an effort was made tostudy each patient in a reasonably stable state, so that thepossible effects of infection or heart failure would notinterfere with an accurate interpretation of the results.The patients were classified for severity of pulmonaryinvolvement according to the criteria set forth by Bald-win, Cournand, and Richards (6, 7).
The patients were fasting but no restrictions wereplaced on smoking prior to the procedure. In 12 of thesubjects after the initial blood flow procedure was per-formed, exercise was carried out in the supine position bymeans of a type of exercycle attached to the foot of thetable and supplied with variable resistance loads. Thisproved to be an unsatisfactory type of exercise, for inalmost every instance the patient's legs would becometired before dyspnea appeared; many subjects who wereunable to walk 50 yards without considerable dyspneaexperienced little difficulty, even after performing thesupine exercise for 20 to 35 minutes. The second bloodflow was done after the patient had exercised for atleast 10 minutes and the exercise was continued until thefinal blood samples were drawn. In one subject (T. K.)this exercise was sufficient to produce mild cyanosis, butnone complained of severe respiratory distress, and noneshowed' evidences of mental disturbances followingexercise.
Arterial and venous oxygen contents were determinedspectrophotometrically, according to the method of Hickam
720

CEREBRALCIRCULATION IN PULMONARYEMPHYSEMA
TABLE I
Clinical and pulmonary function data
Per centnormal Per cent
maimal normal Airbreathing vital velocity Clauifi-
Pt. Age Diagnosis and comments capacity capacity index cation
59 Bronchial asthma, severe; pulmonary emphysema;no failure on admission.
72 Tuberculosis, moderately advanced, active; pulmo-nary fibrosis; no failure on admission.
56 Chronic bronchitis, pulmonary emphysema; corpulmonale; no failure on admission.
58 Pulmonary emphysema; cor pulmonale; failure onadmission.
55 Chronic bronchitis; pulmonary fibrosis; no failureon admission.
58 Pulmonary granulomatosis; cor pulmonale; failureon admission.
40 Bronchial asthma, severe; pulmonary emphysema;no failure on admission.
63 Pulmonary emphysema; cor pulmonale; failure onadmission.
54 Intrinsic asthma; pulmonary emphysema; no failureon admission.
53 Bronchial asthma; bronchiectasis; pulmonary em-physema; cor pulmonale; failure on admission.
50 Pulmonary emphysema; cor pulmonale; failure onadmission.
41 Pulmonary emphysema; no failure on admission.56 Bronchial asthma; pulmonary emphysema; cor pul-
monale; no failure on admission.25 Pulmonary emphysema and fibrosis; cor pulmonale;
failure on admission.57 Pulmonary emphysema; cor pulmonale; failure on
admission.63 Bronchial asthma; pulmonary emphysema; no fail-
ure on admission.54 Bronchial asthma; pulmonary emphysema; no fail-
ure on admission.54 Pulmonary emphysema; no failure on admission.47 Bronchial asthma; pulmonary emphysema; no fail-
ure on admission.57 Pulmonary emphysema; cor pulmonale; failure on
admission.55 Bullous emphysema; no failure on admission.74 Bronchial asthma; pulmonary emphysema; no fail-
ure on admission. 0
30 42 0.72 I
60 59 1.0 I
28 41 0.66 IV
27 35 0.77 IV
55 53 1.06 I
- - IV
38 52 0.73 I
28 84 0.33 IV
35 64 0.55 III
38 49 0.78 IV
25 36 0.69 IV
II
- 43 II
36 -- IV
24 56 0.44 IV
- 43 I
42 75 0.56 II
60 79 0.76 II55 99 0.56 II
21 36 0.58 IV
III-- - II
and Frayser (8). Blood samples for oxygen determina-tion were drawn before and after each blood flow measure-ment, and the average was used as the final value forarterial-cerebral venous oxygen difference and arterialoxygen saturation. Carbon dioxide determinations were
carried out on the van Slyke-Neill manometric apparatus,as described by Peters and van Slyke (9). Arterial bloodpressure was recorded at heart level by the auscultatorymethod at intervals of approximately two minutes, andmean pressure calculated from the formula: MP= dia-stolic pressure + %pulse pressure. The calculated mean
pressures checked closely with mean pressures measureddirectly by means of a mercury U-tube manometer.
pH measurements were made with the Model R Cam-bridge pH meter. Blood was drawn into heparin-coated
syringes and immediately transferred to a constant tem-perature room at 33-34° C. The syringes were allowedto stand for three to six minutes to allow the tempera-ture to fall from body temperature to the temperature ofthe room before readings were made. Buffers at pH 4.00(acid phthalate) and 6.99 (phosphate) were used tocheck the instrument for standardization. The Rosenthalfactor was used to correct the readings to 380 C. (10).Arterial and venous oxygen tensions were estimated fromthe pH and the per cent oxyhemoglobin saturation, usingthe dissociation curves of Dill. The values for oxygentension when oxyhemoglobin saturation was above 90 percent were obtained from a chart of interpolated values,using Dill's figures, since it was impossible to read thecurves accurately above this point. Carbon dioxide ten-
C. M.
S. A.
R. C.
S. G.
J. G.
M. E.
L. S.
N. S.
H. J.
W. G.
T. B.
G. W.T. K.
J. H.
C. A.
H. McD.
G. C.
W. E.R. S.
N. V.
C. K.L. S.
7.21

P. SCHEINBERG, I. BLACKBURN, M. SASLAW, M. RICH, AND G. BAUM
._ I "If)coa0I,in co ei.M lho entoNcoo0-C4 In~0 t- Os it- 00 q* ( - C4 In'* 0-No' t
- 0E) t-. 00fc o- 0 - -'o C°N NO- 00
A
a~~~~* m-W;c>*SIoo I " co51
fg__ _ _ _ U~~~~~I) _ if) -c'NS> tc eo or_++ou N *+eO Cco oo".|:. <o<+ - o I uab I oo I b I I I IO I Ia~~~~~~~~cotenon 0eIeN lS ;g- 7 U- gI mb i cI6 el_ v
b~~~~~~9c o 0 st . omI mWSYP" e e "t" > +o o%o-0 00
's A
A
UL e0+ N1e0moo IMc N o
co% 0~ nC -W40 -.i %m
A
if)ONNO )No in Io
w&n"oo O Iooil Im
14
0co
1 ;X*b N~de4 ) O > v + O> O O _ e 0 0
b i < 00% 0%O%O%0%0 0%000%Os%00s0Cs%000000 0% 0O 0%0s 0s 0\ co
42oW M"S¢1>W 1o1 11n11'56. co %Zo-io
Ifi¢t¢+¢ I ft¢X*tt¢t¢1*ee¢o
I I*.PX°l00 C o m- Uso0 0nt( oI- _o I Y
z Yva_sOoOOOC I n05O 1 0e 1 1 bm0\ en \0 _t ~ ~~~ ~~+ 8)\0U )U ) +U )+S ) u
wiuiir;
e0000'00%'- 0%
to in'IO o o o 0o ooo >o O - O 0000 "WnIno.OX 00ooo_ +
e1l 1 g g g co o|O_e6|6 oco*6 e- cm |6| - |t,: q odq Iq .q I ue I I I
X Z9.0 -oo co oco _o_Seo_ _in C4 o
>1 C~~~~(4 0000ocN 0
'0
co I10~~~~~~~~~~~~~~~~~~~~~~
,.4~~~ 14.4C4.0
Uot0%fo)ooroo4oo0t'. 0n'I) _
2- -' - -- - - - - - - --0
ci A010~1f001~000t..~f)4 01401 - 140m~~~.
co44 C4"00 co Nro XOwOsin uo thtrC0 _qwIncs3ri%
en4r'
)" 'IC i o N0WD
f)00'0rI)Sf)'0' n131 %f) w- 'W10 t4.4' o '40ao noIt
t~~~* * ** * 06
r. co~~~~~00| (;o XX,,03X32=>Q->2.0 | t ft 0 f|;
722

CEREBRALCIRCULATION IN PULMONARYEMPHYSEMA
sions were estimated from the nomograms of Peters andvan Slyke (9).
RESULTS
Comparison with normal subjects. A clinicalsummation of the patients is given in Table I, andthe results of the studies are given in detail inTable II. The patients ranged in age from 25 to74 years, with an average of 55 years. They werecompared with a group of 32 normal subjects whoranged in age from 38 to 79 years, averaging 56years (11). It was felt necessary to compare thesubjects with others in a similar age group, asdefinite changes in cerebral circulation and metab-olism accompany advancing age ( 11 ). There wasno significant alteration in cerebral blood flow, ar-terial-cerebral venous 02 difference, cerebral 02consumption, or cerebral vascular resistance(Table II).
The blood gas tensions indicate that the chemi-cal effects of pulmonary disease in most of thesepatients were not extensive. Only five of the pa-tients had values for pCO2 of 50 mm. Hg or above;
so
.0%a
aso
do
C
I..
_0
i
UoI.:
AU
6%la
60
4o
40
4
however, pCO2 determinations were not obtaifiedin the three patients with the lowest arterial 02saturation and tensions because of technical er-ror. Were these figures available, it is possiblethat a much higher mean for pCO2 would havebeen obtained, but even so the mean value for cere-bral blood flow is within, normal limits. ArterialpH did not differ significantly from the normal,and mean per cent arterial oxygen saturation was91.3, both indications that this group representsrelatively mild, or at least well-compensated pul-monary disease.
If the subjects are divided into two groups ac-cording to clinical severity of their disease, bycontrasting those subjects in group I and II withthose in groups III and IV, there are no significantdifferences observed in cerebral blood flow, cere-bral oxygen consumption, and arterial pH betweenthe two groups. Since the clinical classification isitself partially dependent upon arterial PO2 andpCO2 values, the value for PO2 is significantlylower and that for pCO2 higher in the second
0
.
U v
)5 40 45 SO 5S 60Arterial PCO2 (mm. HS)
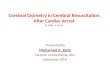
FIG. 1. CORRELATIONBETWEENARTERIAL PCO2 AND CBFr=0.63 p <O.O1
I
11
I
I
I
723

1P. SCHREINBERG, I. BLACKBURN, M. SASLAW,, -M. RICH, AND G. BAUM
I
0
.0~~~~~~~~~~~~
.
0
0.
0
*.0
0
50 55 60 65 70 75 80
Arterial pOz (mm. Hg)
FIG. 2. CORRELATIONBETWEENARTERIAL PO, AND CBFr-0.03
group than in the first. When considering all thepatients together, however, there is an adequatecorrelation between arterial pCO, and cerebralblood flow and no correlation between arterial PO0and cerebral blood flow (Figures 1 and 2). There
TABLE III
Efects of mild exercise on cerebral metabolic functions(mean values in 12 subjects)
Before Duringexercise exercise p value
Art. p02 70.8 70.4 >0.5CBF 52.8 58.3 >0.2Art. 02 content 17.2 17.0 >0.5Venous O, content 10.8 11.0 >0.5A-V O 6.48 5.88 >0.1Art. C02 content 53.5 53.1 >0.5Venous CO, content 54.7 54.2 >0.5Art. pH 7.38 7.34 <0.02*Art. pCO2 45.8 49.2 >0.2Venous pCO, 50.1 51.1 >0.5Per cent art. 02 sat. 91.7 89.8 >0.2Per cent venous 02 sat. 57.5 58.6 >0.5Venous p02 3217 33.7 >0(A5CMRO2 3.23 3.18 >0.5MAP 90.7 101.2 <0.01*CVR 1.85 1.88 >0.5
* Denotes statistically significant change.
is also no correlation between cerebral blood flowand clinical severity of the ventilatory defect as
expressed by reduction in percentage normalmaximal breathing capacity.
Effects of exercise. The effects of exercise on
the 12 subjects in whom it was studied are sum-
marized in Table III. The only statistically sig-nificant changes were the drop in arterial pH from7.38 to 7.34 and the increase in niean arterial pres-sure. 'It is of interest that the nly tswo subjectswho showed a considerable rise in cerebral bloodflow during exercise also had a sizable increase inpCO, (S. A. and T. K., Table Ul), although twoother subjects showed some increase in pCO,without accompanying significant elevation of cere-
bral blood flow. There is no evidence of even
a trend toward an increase in cerebral blood flowor decrease in arterial-cerebral venous 02 differ-ence during exercise, for-the c1*nges were quitevariable, and only one patient (T. K.) was actu-ally responsible for the apparent change in themean values of these functions. Cerebral oxygenconsumption and cerebral vascular resistance were
724
S SO
C
S10.
0
d
IAC
40
30 L41
a

CEREBRALCIRCULATION IN PULMONARYEMPHYSEMA
not altered by exercise, although there was a fairlyconsistent increase in mean arterial pressure.There was no consistent change in per cent arterial02 saturation or arterial PO2' the only striking re-duction in either occurring in T. K. This is fur-ther evidence of the relative mildness of this typeof exercise or the relative lack of severity of pul-monary disease in these patients, or both.
Pulmonary fibrosis. The two patients with pul-monary fibrosis showed no differences in cerebralmetabolic functions from the patients with em-physema.
Intermittent vs. continuous sampling techniques.There was no significant difference in any of thecerebral metabolic functions in the nine subjectsstudied by the continuous sampling technique ascompared to the 13 studied by the original inter-mittent sampling technique, as seen in Table IV,and for that reason both groups were combinedfor final statistical analysis in this study. Thestudies were done by both techniques as a partof planned observations to determine the possible
3.60
3A
1 2400
1M
1 0
h
0.00
's
TABLE IV
Comparison of intermittent and continuous samplingtechniques (mean values)
Intermittent Continuous(13 subjects) (9 subjects)
CBF 57 51CMRO2 3.3 3.5CVR 1.69 1.89
All p values >0.3.
reason for the differences in m-ean values in nor-mal subjects as reported by Kety and Schmidt (4),Scheinberg and Stead (3) and Patterson, Hey-man, and Nichols (12). In this group of sub-jects, at least, there is no significant difference be-tween results obtained by the two techniques.
Electroencephalograms. Electroencephalogramsperformed on eight of the subjects were all withinnormal limits.
DISCUSSION
The data reported here cannot be comparedwith the observations on cerebral circulatory func-tions in pulmonary emphysem reported by Pat-
.
..
0
0
0
0
0
440 4s5 o 4 " .6
AvtrWI pCOZl ol!MW_FIG. 3. CORRELATIONBETWEENCVRANDARTERIAL PCO,
r=0.51 0.05 > p >O.O1
1
725
L

P. SCHEINBERG, I. BLACKBURN, M. SASLAW, M. RICH, AND G. BAUM
90'
_ soa
0* 70
4
560
0
40
5075 so 55 90 9S
%Oxygen Saturat,ionFIG. 4. CORREIATION BETWEENPER CENT OXYGENSATURATIONAND CBF
r = 0.03
terson, Heyman, and Duke (2), since most of our
subjects suffered less pulmonary disability thandid theirs. In both groups of subjects there was
adequate correlation between cerebral blood flowand pCO2, and cerebral vascular resistance andpCO2. In our subjects the p values for these cor-
relations were < 0.01 and between 0.01 and 0.05,respectively (Figures 1 and 3). We found no
correlation, however, between pO2 and cerebralblood flow or between per cent arterial 02 satura-tion and cerebral blood flow (Figures 2 and 4),and we are unable to explain this discrepancy.Our patients were not studied until the effects ofthe acute illnesses which precipitated admissionto the hospital had subsided and the patients were
reasonably stable. Patterson, Heyman, and Dukemake no statement concerning whether this pre-
caution was observed in their group. In additionfive of the nine patients they reported had evidenceof congestive heart failure due to cor pulmonale.Since this type of failure reportedly is accompanied'frequently by an increased cardiac output (13),there is a possibility that the failure itself rather
than pulmonary emphysema may be responsiblefor the elevated cerebral blood flow in these sub-jects. Two of their subjects had low and normalcardiac indices (T-1824 dye), however, makingsuch an explanation dubious without further in-vestigation.
The correlation between cerebral blood flow andpCO2 in our subjects confirms previous observa-tions on the effects of inspired CO, on cerebralcirculation (1), and the normal mean value forcerebral blood flow obtained in this group is com-
patible with an essentially normal mean value forpCO2. The absence of correlation between cere-
bral blood flow and arterial PO2 is surprising, as isthe apparent absence of effect of a decreased mean
value for arterial PO2 in the whole group. Pre-vious observations (1) have indicated that a de-crease in PO2 is a fair stimulus for producingcerebral vasodilatation in normal subjects; per-
haps the absence of this phenomenon in the groupof subjects reported here indicates the developmentof a tolerance and diminished response to the cere-
bral vasodilating effect of a low oxygen environ-
I
0 .
9
0
.
a
0
100
726
I

CEREBRALCIRCULATION IN PULMONARYEMPHYSEMA
ment if the oxygen deprivation is chronic ratherthan acute.
Little was learned about the effects of exercisein this study, except that patients with only moder-ately severe functional pulmonary disability have aremarkable tolerance to this type of exercise.One might anticipate an increase ini cerebral bloodflow to accompany a rise in arterial pCO2 in thosepatients whose limitation of ventilatory capacityprevents compensatory hyperventilation, and suchseemed to be the case in the two subjects whoshowed the most striking chemical responses toexercise. It is of interest that the reduction inarterial pH during exercise was not associatedwith a change in cerebral blood flow. This is fur-ther evidence that alteration in arterial pH per seis not the important factor in the regulation ofcerebral blood flow (14). Since none of our sub-jects developed signs of mental confusion duringthis relatively mild exertion, one of the purposesof this study, which was to investigate the physio-logical basis for the confusion which occurs duringphysical exertion in many such patients, was notachieved.
These studies verify the previously establishedrelationship between arterial pCO2 and cerebralblood flow and demonstrate a relative lack ofimportance of individual changes in arterial pH,arterial PO2' and arterial CO2content in the regu-lation of cerebral circulation. They also demon-strate that cerebral vascular and metabolic func-tions in chronic pulmonary diseases are unrelatedto the severity of the clinical and spirometric dis-turbance, but are rather related to alteration ingaseous exchange in the lungs, and specifically tocarbon dioxide retention.
SUMMARY
1. Cerebral blood flow, oxygen consumption,and vascular resistance were measured in 22 pa-tients with chronic pulmonary disease of moderatefunctional severity, and compared with a group ofnormal controls of the same average age. The ef-fects of mild exercise were studied in 12 of thepatients.
2. There was no significant difference in cere-bral blood flow as measured by the intermittentsampling technique in 13 of these subjects as
compared to the continuous sampling techniquein the remaining nine subjects.
3. Mean values for cerebral blood flow, cere-bral A-V 02 difference, cerebral oxygen consump-tion, and cerebral vascular resistance did notdiffer significantly from the normal control sub-jects.
4. The correlation between cerebral blood flowand arterial pCO2 was good, whereas no correla-tion was found between cerebral blood flow andarterial POi or per cent arterial 02 saturation.
5. The effects of exercise on cerebral metabolicfunctions in these patients were variable andwithout a significant trend. A reduction in ar-terial pH during exercise did not influence cere-brat blood flow.
6. These studies re-emphasize the importantrelationship between arterial pCO2 and cerebralblood flow and demonstrate the relative unim-portance of the clinical' and spirometric severityclassification on cerebral blood flow in chronicpulmonary disease.
ACKNOWLEDGMENT
The authors gratefully acknowledge the technical as-sistance of Mrs. Janet Fetner.
REFERENCES
1. Kety, S. S., and Schmidt, C. F., The effects of al-tered arterial tensions of carbon dioxide and oxygenon cerebral blood flow and cerebral oxygen con-sumption of normal young men. J. Clin. Invest.,1948, 27, 484.
2. Patterson, J. L., Jr., Heyman, A., and Duke, T. W.,Cerebral circulation and metabolism in chronicpulmonary emphysema. With observations on theeffects of inhalation of oxygen. Am. J. Med., 1952,12, 382.
3. Scheinberg, P., and Stead, E. A., Jr., The cerebralblood flow in normal male subjects as measuredby the nitrous oxide technique. Normal values forblood flow, oxygen utilization, glucose utilizationand peripheral resistance, with observations on theeffect of tilting and anxiety. J. Clin. Invest., 1949,28, 1163.
4. Kety, S. S., and Schmidt, C. F., The nitrous oxidemethods for the determination of cerebral bloodflow in man: Theory, procedure and normal values.J. Clin. Invest., 1948, 27, 476.
5. Gaensler, E. G., Air velocity index. A numerical ex-pression of the functionally effective portion ofventilation. Am. Rev. Tuberc., 1950, 62, 17.
727

P. SCHEINBERG, I. BLACKBURN, M. SASLAW, M. RICH, AND G. BAUM
6. Baldwin, E. de F., Cournand, A., and Richards, D. W.,Jr., Pulmonary insufficiency. I. Physiologicalclassification, clinical methods of analysis, stand-ard values in normal subjects. Medicine, 1948, 27,243.
7. Baldwin, E. de F., Cournand, A., and Richards, D.W., Jr., Pulmonary insufficiency. III. A study of122 cases of chronic pulmonary emphysema. Medi-cine, 1949, 28, 201.
8. Hickam, J. B., and Frayser, R., A spectrophotometricmethod for determining blood oxygen. J. Biol.Chem., 1949, 180, 457.
9. Peters, J. P., and van Slyke, D. D., Quantitative Clini-cal Chemistry, Vol. II, Methods. Williams &Wilkins, Baltimore, 1932.
10. Rosenthal, T. B., The effect of temperature on the
pH of blood and plasma in vitro. J. Biol. Chem.,1948, 173, 25.
11. Scheinberg, P., Blackburn, I., Rich, M., and Saslaw,M., The effects of aging on cerebral circulationand metabolism. In manuscript.
12. Patterson, J. L., Jr., Heyman, A., and Nichols, F. T.,Jr., Cerebral blood flow and oxygen consumptionin neurosyphilis. J. Clin. Invest., 1950, 29, 1327.
13. Harvey, R. M., Ferrer, I., Richards, D. W., Jr., andCournand, A., Influence of chronic pulmonary dis-ease on the heart and circulation. Am. J. Med.,1951, 10, 719.
14. Schieve, J. F., and Wilson, W. P., The changes incerebral vascular tone in experimental metabolicalkalosis and acidosis. J. Clin. Invest., 1952, 31,659.
728