Embed Size (px)
Citation preview

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 1/29
Nasal and oral cavities, tongue, taste, olfaction,
salivary glands
• Describe the central pathways of olfaction (CN I) andtaste (VII, IX, X)
• Describe the anatomy of the tongue, including motorand sensory (general and taste) innervation, bloodsupply, and lymphatic drainage
• Identify the salivary glands and components of thepalate, nasal and oral cavities, and paranasal air sinuses,
and summarise their innervation and blood supply• Summarise functions of CN I, V, VII, IX, X, XII related
to the above regions

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 2/29
Dissection Lab availability
during study week and exams
• Open
– 5 June – 9 June, 9am-5pm
– 12-13 June, 9am-5pm
•
Written 14 June, 9-11am• Prac 16 June, 1pm – 5pm (4 groups, 1 hour each)

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 3/29
Suprahyoid muscles
• Digastric, anterior (V3) &
posterior bellies (VII)
• Stylohyoid (VII)
• Mylohyoid - floor of mouth (V3)
• Geniohyoid (C1)
• Actions: raise hyoid bone and floor
of mouth during swallowing,
stabilise hyoid, lower mandible
(open mouth)
Netter 47

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 4/29

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 5/29
Teeth• Joints: gomphoses (fibrous peg in socket joint)
between teeth and superior/inferior alveolar
processes of maxilla/mandible
•4 x (2 incisors, 1 canine/cuspid, 2premolars/bicuspids, 3 molars) = 32 permanent
• Crown, root
• Root canal with nerves, vessels
– Mandibular teeth – inferior alveolar n (V3)
– Maxillary teeth – superior alveolar nn (V2)
– Vessels for both from maxillary artery
Netter 50, http://www.ada.org/public/topics/permanent_number.asp
R L
Upper
Lower

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 6/29
Parotid salivary gland
• Key n/a/v relations: facial n,
retromandibular v, external carotid a,superficial temporal aa/vv,
auriculotemporal n
• Parotid duct pierces buccinator, opens
opposite 2
nd
upper molar
N e t t e
r 1 9 , 4 5 , 5
4

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 7/29

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 8/29
Parasympathetic innervation of salivary glands
• Parotid: inferior salivatory nucleus, glossopharyngeal n (IX), oticganglion (synapse), postganglionics via auriculotemporal n (of V3)
• Submandibular and sublingual: superior salivatory nucleus, facialn (VII), chorda tympani to lingual nerve (of V3), submandibular
ganglion (synapse)
N
e t t
e r 1 2
7 , 1 2 8

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 9/29
Tongue muscles• Intrinsic: longitudinal, transverse,
vertical (change shape of tongue)
• Extrinsic: genioglossus (protrudes),
hyoglossus (lowers and retracts),styloglossus and palatoglossus (elevate
and retract)
Netter 54, 53

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 10/29
Innervation of tongue muscles: hypoglossal nerve (CN XII)
• All muscles of tongue by XII except palatoglossus (X)
•
Lower motor neurons in hypoglossal nucleus in medulla• Exit brainstem at preolivary sulcus, cranial cavity at hypoglossal
canal
N e t t e r 1 0 8
F i x 2 3

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 11/29
UMN control over hypoglossal nucleus
LMNs: Corticobulbar tract
• Cell bodies in primary motor cortex and
nearby areas
• Fibres travel through internal capsule,
cerebral peduncle of midbrain, basal pons
• UMNs supply LMNs bilaterally
• Unilateral UMN lesion - usually no observable effect on
tongue
• Unilateral LMN lesion - ipsilateral tongue paralysed,
atrophies with time
– Stick tongue out – deviates towards side of lesion
(paralysis of genioglossus)
N e t t e r 5 3 ,
N o l t e 4 4 7

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 12/29
Gustatory sensation
• “Taste” includes smell, gustatory sense,
general sensation (touch, temperature)
• Dorsum of tongue contains papilla, most
without taste buds (filiform), some with
(fungiform, foliate, vallate)
•
Taste buds detect salty, sweet, sour,bitter, umami (glutamate)
N e t t e r 5 3 ,
W h e a t e r 3 1 6
7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 13/29
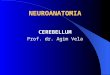
Taste pathways
• Anterior 2/3 tongue: VII,
geniculate ganglion (1o
)• Posterior 1/3 tongue: IX,
petrosal ganglion (1o)
• Epiglottis, pharynx: X,nodose ganglion (1o)
• Nucleus of solitary tract (2o)
• Pontine taste area (3o)
• Thalamus (VPM) (4o)
• Insula, postcentral gyrus (5o)
• Limbic system, hypothalamus,orbital cortex of frontal lobe
Netter 129 Fix 23
7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 14/29
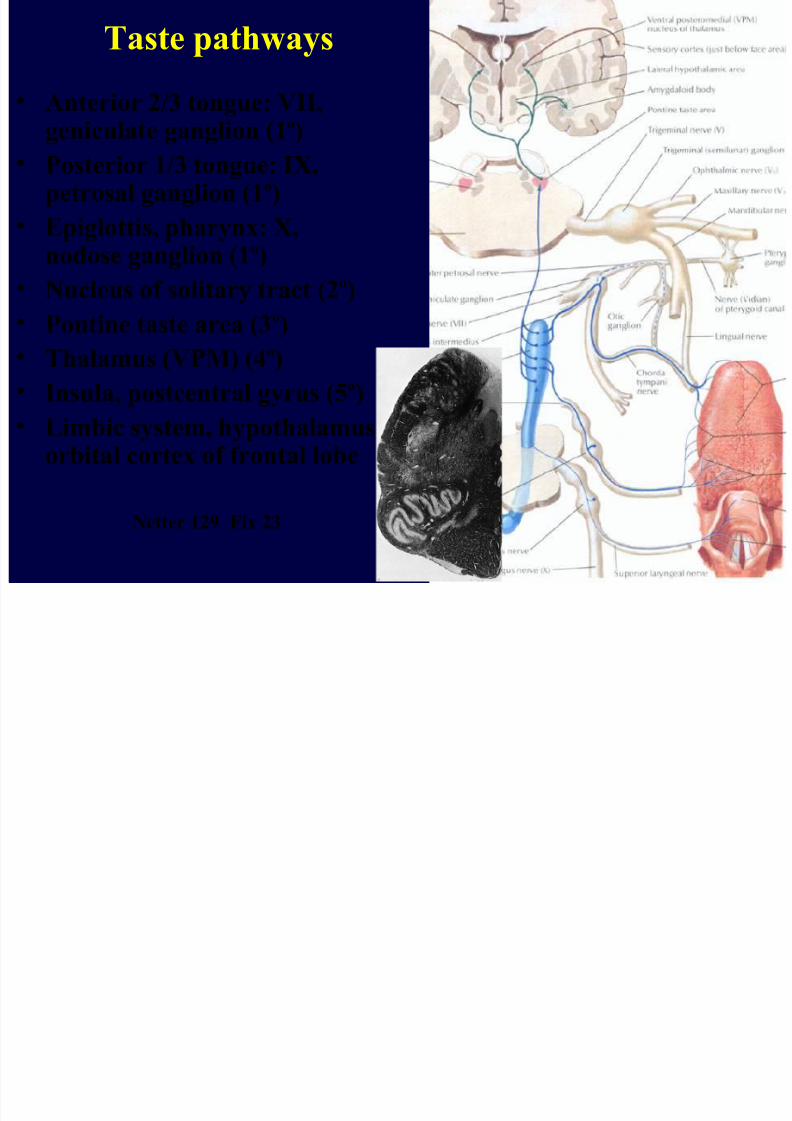
General sensation from tongue
• Anterior 2/3 of tongue: V3
• Posterior 1/3 of tongue: IX
• Trigeminal, petrosal ganglia(1o)
• Same pathway as generalsensation from face:
• Descending (pain,temp), main(touch) nuclei of V (2o)
• (cross) trigeminothalamic tract
• VPM thalamus (3o)
• Postcentral gyrus of cortex (4o)
Haines 230; Drake 8.248

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 15/29
Glossopharyngeal n (IX), hypoglossal nerve (XII),
and lingual n (V3 branch)
• Lingual n: deep to mandible
• Hypoglossal n: superficial toexternal and internal carotid
aa and hyoglossus, superior to
mylohyoid – motor to tongue
• Glossopharyngeal n: close tostylopharyngeus (supplies it),
between external and internal
carotid arteries
–
Sensory (general and taste) toposterior 1/3 of tongue
– Sensory to much of pharynx
– Supplies carotid sinus and body
– Parasympathetic to parotid
N e t t
e r
6 5

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 16/29
Blood supply of tongue
• Lingual artery from external carotid artery
– branches include dorsal lingual, sublingual, deep lingual aa
• Lingual veins (with lingual a and XII) drain to internal jugular
vein (usually join facial vein first)
Netter 53

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 17/29
Lymphatic drainage
of tongue
• Important in spread of cancer
• Anterior tongue: to
submental, submandibular
nodes and then to deepcervical nodes (including
juguloomohyoid node)
• Posterior tongue: to deep
cervical nodes (including jugulodigastric node)
• Central part of tongue -
bilateral drainage
Netter 66
7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 18/29
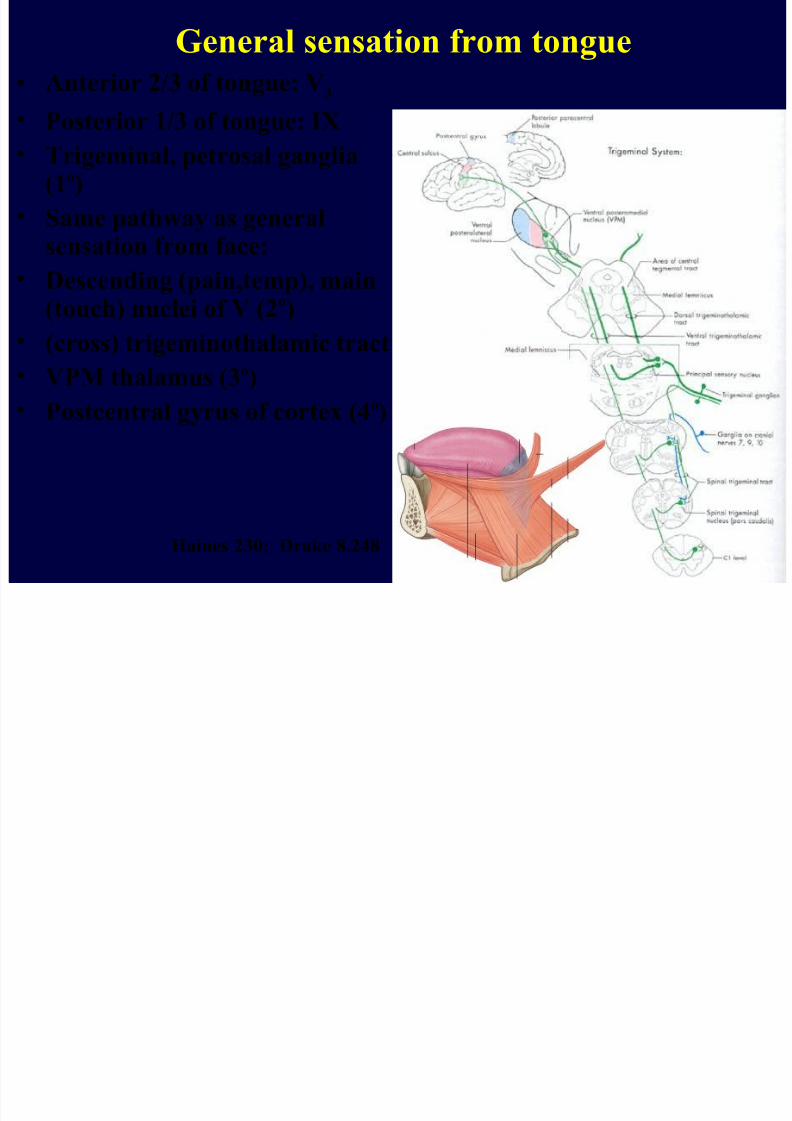
External nose
• Bony margins: nasal bones, maxillae
• Major cartilages:
– lateral nasal cartilage
– greater alar cartilage - lateral crus and
medial crus
Netter 31
7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 19/29

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 20/29
Nasal septum
• Separates nasal cavity on midline
•Bony: vomer, perpendicular plate of ethmoid
• Cartilaginous: septal cartilage, medial crura of greater alarcartilages
N e t t e r 3 4 ,
W e i r 9 e

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 21/29

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 22/29

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 23/29
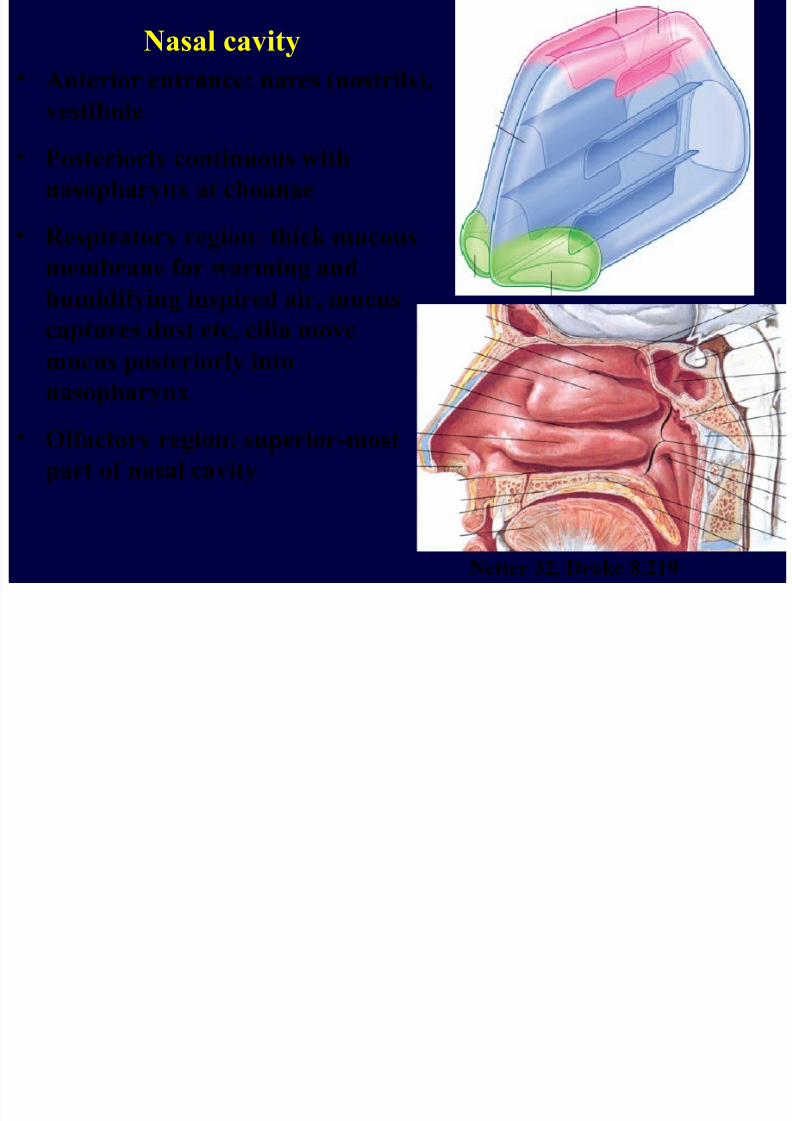
Paranasal air sinuses
• Maxillary sinus
– Opens into semilunar hiatus of middle meatus
• Ethmoid air cells
– open into middle and superior meatuses
• (Note: nasolacrimal duct opens into
inferior meatus)
N e t
t e r 3 2 ,
W e i r 8 d
, D r a k e 8 . 2
1 8

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 24/29
Palate
• Separates nasal and oral cavities, and can
separate naso- and oro-pharynx
• Hard palate: maxilla and palatine bones
• Soft palate: posterior to hard palate
N e t
t e r 5 , W e i r
1 8 b

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 25/29
Muscles of soft palate• Levator veli palatini, tensor veli palatini,
palatoglossus, palatopharyngeus, musculus uvulae
• Elevated during swallowing, depressed during
chewing• Innervated by vagus n (X), with LMNs in nucleus
ambiguus (Exception: tensor veli palatini by V3)
• Unilateral LMN or CN X lesion: uvula deviates awayfrom side of lesion, soft palate droops on affected side
N e t t e r
4 6 , 5 8 , D r a
k e 8 . 2 5 7 , 8 . 2
5 8

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 26/29
General sensory innervation and blood supply
of nasal cavity and palate• Nerves: Mostly branches of maxillary division of trigeminal n (V2)
–
Anteriorly, branches of ophthalmic division of trigeminal n (V1)• Arteries: Mostly from maxillary artery (from external carotid a)
– Anteriorly and superiorly from ophthalmic artery (from internal carotid a)
– Near vestibule from facial artery (from external carotid a)
N e t t e r
3 6 , 3
7

7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 27/29
Parasympathetic innervation of nasal cavity and palate
• Supplies mucus glands
• Superior salivatory nucleus
• Facial nerve (CN VII)
• Pterygopalatine ganglion (synapse), postganglionic fibres viabranches of maxillary nerve (V2) (also to lacrimal gland)
N e t t
e r 1 2
7
Olf i ( ll)
7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 28/29
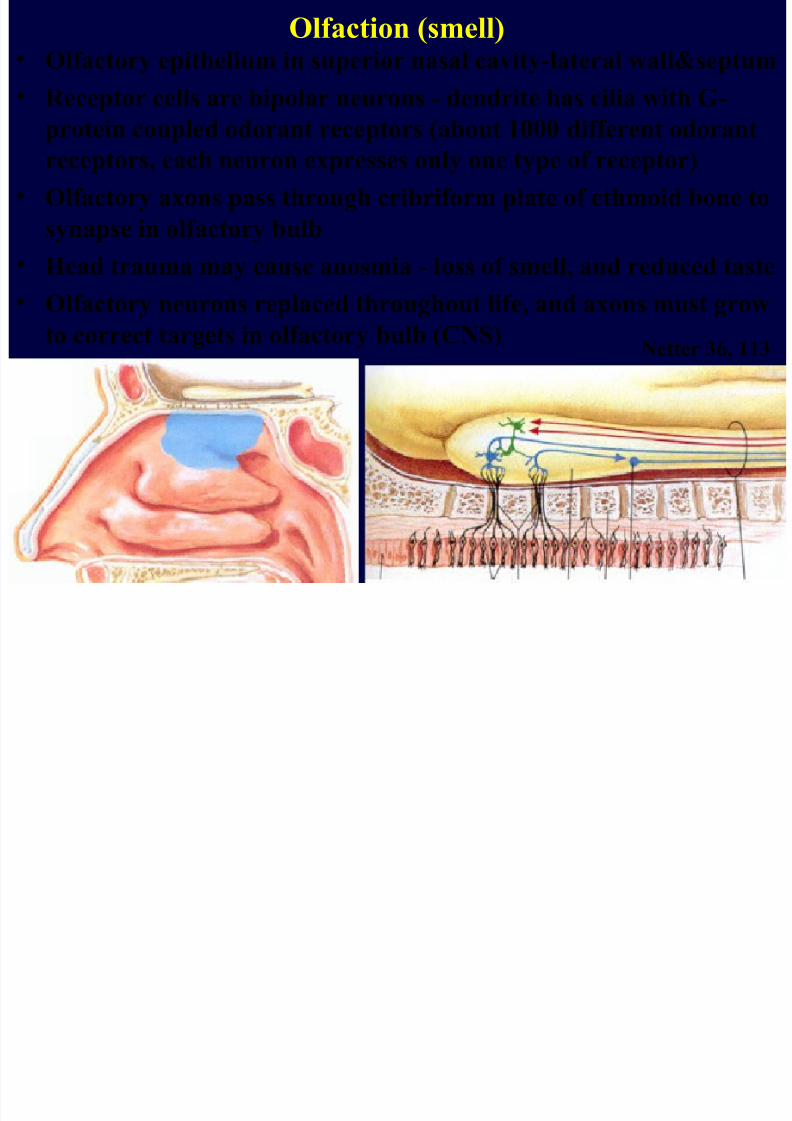
Olfaction (smell)• Olfactory epithelium in superior nasal cavity-lateral wall&septum
• Receptor cells are bipolar neurons - dendrite has cilia with G-
protein coupled odorant receptors (about 1000 different odorantreceptors, each neuron expresses only one type of receptor)
• Olfactory axons pass through cribriform plate of ethmoid bone to
synapse in olfactory bulb
•
Head trauma may cause anosmia - loss of smell, and reduced taste• Olfactory neurons replaced throughout life, and axons must grow
to correct targets in olfactory bulb (CNS)Netter 36, 113
Olf ti ( ll)
7/31/2019 Cerebellum (2)
http://slidepdf.com/reader/full/cerebellum-2 29/29
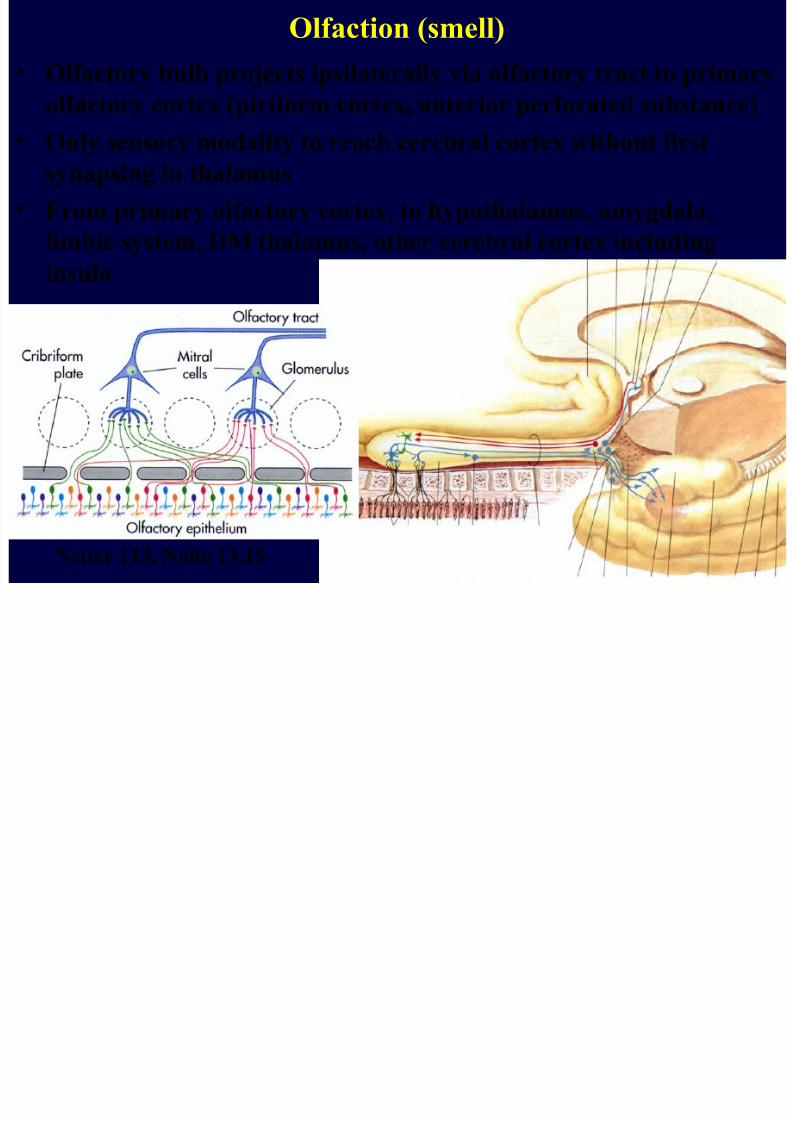
Olfaction (smell)
• Olfactory bulb projects ipsilaterally via olfactory tract to primary
olfactory cortex (piriform cortex, anterior perforated substance)
• Only sensory modality to reach cerebral cortex without firstsynapsing in thalamus
• From primary olfactory cortex, to hypothalamus, amygdala,
limbic system, DM thalamus, other cerebral cortex including
insula
Netter 113, Nolte 13.15




![The Cerebellum - download.e-bookshelf.de€¦ · [DNLM: 1. Cerebellum. 2. Executive Function. 3. Neural Pathways–physiology. 4. Psychomotor Performance–physiology. WL 320] QP379](https://img.dokumen.tips/doc/110x75/5f0a6af27e708231d42b88bf/the-cerebellum-downloade-dnlm-1-cerebellum-2-executive-function-3-neural.jpg)