Embed Size (px)
Citation preview

J Neurosurg Pediatrics 12:604–614, 2013
604 J Neurosurg: Pediatrics / Volume 12 / December 2013
©AANS, 2013
The term cerebellar mutism (CM) is used to describe the lack of speech caused by lesions of the cerebel-lum, which is not associated with long tract signs,
cranial nerve palsies, or alteration of consciousness. It usually appears as a consequence of posterior fossa sur-gery in children with cerebellar or fourth ventricle tu-mors.52,82,108 Other causes that have been reported are in-fections,15,19,24,26,72 posterior fossa hematomas (surgically removed31,89 or not60), arteriovenous malformations,33,51,82 a brainstem tumor,82 a pineal gland tumor,23 and trau-matic cerebellar injury.15,82 Although this clinical entity is mainly seen in children, there are also reports of CM in adults.12,16,33,82,85
Historical OverviewIn 1917, Sir Gordon Holmes studied the disturbances
of speech production in World War I soldiers who sus-tained gunshot wounds to the cerebellum. He observed that lesions in one hemisphere produced speech that was usually slow, drawling, and monotonous but at the same time tended to be staccato and scanning; a few of the pa-tients showed additional behavioral disturbances. On the other hand, when the lesion included the vermis the main characteristics were phonation and articulation abnormali-ties.45,96 In 1949 Brown included dysarthria when describ-ing cerebellar syndrome,69 while in 1972 Stein was the first to “incidentally” report CM.31 In 1975 Fraioli and Guidet-ti29 noted complete absence of speech in 2 of 43 patients who underwent bilateral stereotactic dentatolysis for the
Cerebellar mutism
A review
Marina Pitsika, M.D., anD Vassilios tsitouras, M.D.Department of Pediatric Neurosurgery, Mitera Children’s Hospital, Athens, Greece
Mutism of cerebellar origin is a well-described clinical entity that complicates operations for posterior fossa tumors, especially in children. This review focuses on the current understanding of principal pathophysiological aspects and risk factors, epidemiology, clinical characteristics, treatment strategies, and outcome considerations. The PubMed database was searched using the term cerebellar mutism and relevant definitions to identify publications in the English-language literature. Pertinent publications were selected from the reference lists of the previously identified articles. Over the last few years an increasing number of prospective studies and reviews have provided valuable information regarding the cerebellar mutism syndrome. Importantly, the clarification of principal terminol-ogy that surrounds the wide clinical spectrum of the syndrome results in more focused research and more effective identification of this entity. In children who undergo surgery for medulloblastoma the incidence of cerebellar mutism syndrome was reported to be 24%, and significant risk factors so far are brainstem involvement and midline loca-tion of the tumor. The dentate-thalamo-cortical tracts and lesions that affect their integrity are considered significant pathophysiological issues, especially the tract that originates in the right cerebellar hemisphere. Moderate and severe forms of the cerebellar mutism syndrome are the most frequent types during the initial presentation, and the overall neurocognitive outcome is not as favorable as thought in the earlier publications. Advanced neuroimaging techniques could contribute to identification of high-risk patients preoperatively and allow for more effective surgical planning that should focus on maximal tumor resection with minimal risk to important neural structures. Properly designed multicenter trials are needed to provide stronger evidence regarding effective prevention of cerebellar mutism and the best therapeutic approaches for such patients with a combination of pharmacological agents and multidisciplinary speech and behavior augmentation.(http://thejns.org/doi/abs/10.3171/2013.8.PEDS13168)
key WorDs • cerebellum • mutism • children • tumor • posterior fossa surgery • cognitive
Abbreviations used in this paper: CM = cerebellar mutism; CMS = CM syndrome; DTC = dentato-thalamo-cortical; DTI = diffusion tensor imaging; FA = fractional anisotropy; fcMRI = functional connectivity MRI; MSD = mutism and subsequent dysarthria; PFS = posterior fossa syndrome.
This article contains some figures that are displayed in color on line but in black-and-white in the print edition.

J Neurosurg: Pediatrics / Volume 12 / December 2013
Cerebellar mutism
605
treatment of dyskinetic syndrome. In 1979 Hirsch et al.44 reported mutism as a reversible complication in children after posterior fossa surgery for medulloblastomas in ad-dition to other speech disorders as “articulatory problems, slowness of speech and speech retardation.” In 1984 Wi-soff and Epstein110 used the term “pseudobulbar palsy” that included delayed-onset mutism, emotional incontinence, lability, and supranuclear cranial nerve palsies. They sug-gested that retraction pressure on the medial cerebellum and vermian split during the operation is responsible for edema that subsequently tracked along fiber pathways in the middle and superior cerebellar peduncles into the up-per pons and midbrain causing disturbances of the blood supply to the brainstem. In 1985 Rekate et al.80 described CM as a distinct clinical entity. The authors reported on 6 children who developed mutism after posterior fossa sur-gery. Mutism lasted 1–3 months and all patients suffered severe dysarthria during recovery. Later that year Yonema-su presented orally during the 13th Annual Meeting of the Japanese Society for Pediatric Neurosurgery in Tsukuba, Japan, of 4 cases of CM after posterior fossa surgery for tumor resection, but his paper was never published, and it was not reproduced in the proceedings of the meeting.15,33 Since then more than 400 cases have been described.2,5,6,
10,11,13,25,27,34,36,51–53,55,57,61–64,66,68,70,81–83,87,104,105,108
DefinitionsCerebellar mutism refers to the absence of speech
caused by a cerebellar lesion. A synonym for CM is tran-sient cerebellar mutism,39 emphasizing the short duration. The term cerebellar mutism syndrome (CMS) is used to describe a group of symptoms caused by a cerebellar le-sion, which includes muteness, ataxia, hypotonia, and irri-tability,39 while mutism and subsequent dysarthria (MSD) is used to describe the linguistic part of CM.33 Posterior fossa syndrome is a broader term that includes CM and, in addition, movement disorders (ataxia and hypotonia) and a wide spectrum of neurobehavioral abnormalities.39 Some authors regard CMS as a synonym for posterior fossa syndrome (PFS) and use the terms interchange-ably,55,82,109 while others believe that CM is a severe form of cerebellar dysarthria.33,44,68,89,99,103,105 In 1998, Schmah-mann and Sherman84 introduced the term cerebellar cog-nitive affective syndrome to describe a constellation of neuropsychological findings in adult patients with diseas-es confined to the cerebellum. The major deficits involved impairment of executive functions, difficulties with spa-tial cognition, personality changes, and language deficits including agrammatism and dysprosodia.
IncidenceThe incidence of CMS has been reported to range
from 8%46 to 39%,9,15,40,52,55,62,82,108 although there are re-views reporting a lower rate of 1.6%.17 In the largest prospective study so far of 450 children who underwent surgery for medulloblastomas, the incidence of CMS was found to be 24%.82 These variations can be explained by the different definitions of the syndromes (such as PFS and CMS) and the wide spectrum of the clinical char-acteristics. It has been noted that the incidence of CMS
was lower in the past. This fact might have different ex-planations. First, the incidence seems to be lower in ret-rospective studies because of a lack of awareness of this syndrome or even because of difficulty in recalling past events.55 Moreover, there is evidence showing that there might be an actual increase in the incidence. More exten-sive tumor resection along with better overall outcome in children who undergo posterior fossa tumor resections can increase the rate of CMS.76 Korah et al.52 noted that in 2 different periods of time (1990–2000 and 2001–2007) the percentage of gross-total resection or near-total re-section among children who underwent medulloblastoma resection was 83% and 93%, respectively, while the inci-dence of PFS was 17% and 39%, respectively. In addition, all patients with PFS underwent a gross-total resection and there was no radiological evidence of residual tumor.
It is known that CMS mainly appears after posterior fossa tumor resection in children and there are a few case reports of CMS in adults. A profound reason for this is that posterior fossa—and even more so midline—tumors appear more often in children than in adults.76 However, it seems that pathophysiological mechanisms contribute to the high incidence of CMS in children. The incomplete development of motor speech control and language is the first factor.8 Additionally, the immaturity and incomplete myelination of the reciprocal links in childhood, connect-ing the cerebellum to thalamus, sensory areas, motor, and supplementary motor area, makes the children more vul-nerable.47 However, this can be considered an advantage for faster and more efficient redirection and recovery.69
Cerebellum and SpeechThe cerebellum’s contribution to speech was origi-
nally thought to be restricted to the coordination of pur-poseful motor movement. However, the increasing num-ber of case reports on CMS led many neurophysiologists to study extensively the role of the cerebellum in cogni-tion and speech production.
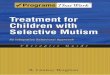
In 1992 Turkstra and Bayles100 assumed that there are 5 stages in the production of speech and language: 1) arousal (ascending reticular system); 2) affect and drive (prefrontal and limbic areas); 3) cognition (dominant hemisphere speech areas); 4) initiation, planning, and co-ordination (Broca’s region, the supplemental motor area, the basal ganglia, the thalamus, and the cerebellum); and 5) execution (brainstem and cranial nerve nuclei). Stud-ies in monkeys have shown that there is a direct neuronal connection between Brodmann’s area 46 (prefrontal area, involved in spatial working memory and planning) and the dentate nuclei,87 while major reciprocal neural path-ways between the cerebellum and frontal areas of the language-dominant hemisphere, including Broca’s area and the supplementary motor area, have been discovered in humans as well.67 Today it is strongly believed that ef-ferent fibers from the dentate nuclei leave the cerebellum through the superior cerebellar peduncle, decussate in the mesencephalic tegmentum, and synapse in the ventral lat-eral and ventral anterior nuclei of the thalamus. The cor-responding postsynaptic neurons project to widespread cortical areas, including the primary motor, premotor, and prefrontal cortices (Fig. 1).63

M. Pitsika and V. Tsitouras
606 J Neurosurg: Pediatrics / Volume 12 / December 2013
Apart from the aforementioned anatomical findings, there are many theories regarding the cerebellum’s role in speech production. In 1993 Tohgi et al.98 proposed that nonmotor pathways of speech subserve the internal generation of words, word choice, speech rehearsal, and vocal intonation used in speech production and can be lo-calized to the posterior lateral hemisphere of the cerebel-lum, while neuroimaging studies have shown the activa-tion of the cerebellum when mentally imaging speech59 or during tasks requiring word selection and production (not related to motor verbal response).73 Petersen et al.74 were among the first to report the cerebellar changes in blood flow using PET scanning during a word generation task. Kim et al.,50 by utilizing PET scanning, reported activa-tion of the dentate nuclei during planning to be greater than what was observed during automatic motor tasks.
Some neurophysiologists believe that the cerebellum contributes to the coordination of orofacial muscles dur-ing verbal production and internal generation of words, as well as the timing and intonation of speech and the choice of words.69 Others consider that the cerebellum plays a more significant role, including language, cog-nitive and behavioral regulatory control, and executive functions (initiation, novel problem solving, and working memory).81 In addition, the right cerebellar hemisphere
seems to contribute in sequential memory and language processing, whereas the left is more important for spatial and visual sequential memory.81
Recent advances in neuroimaging have allowed a fur-ther exploration of the cerebellum’s contribution to cogni-tion and higher cortical functions. Traditional transneural tracing techniques (using virus strains) showed polysyn-aptic connections of cerebral motor areas and the anterior and posterior lobe of the cerebellum in monkeys.49 Task-based functional MRI confirmed such somatomotor rep-resentations within the cerebellum in humans.37 High and ultrahigh magnetic fields (> 3 T) are used to map brain sys-tems in the human by detecting intrinsic, low-frequency functional correlations.41,42 These correlations were found to be anatomically selective, and the new tool was termed functional connectivity MRI (fcMRI).102 Using fcMRI, Krienen and Buckner54 discovered 4 segregated fronto-cerebellar circuits mainly between prefrontal regions and a large portion of the posterior cerebellar hemispheres. Similarly, Strick et al.95 found that closed-loop circuits represent the major architectural unit of cerebrocerebel-lar interactions and allow the cerebellum to influence the control of movement and cognition. Resting-state fcMRI was used by Buckner et al.7 to study 1000 young adults and establish an organization map of the cerebellum. It was found that the cerebellum possesses 3 distinct maps of the cerebral cortex (including somatomotor, premotor, and association cortices): a homotopic one that begins in the anterior lobe somatomotor representation and ends near Crus I/II, a mirror-image secondary map that begins in Crus I/II and ends with the second somatomotor repre-sentation near the paramedian lobule (HVIII), and finally a provisional map at the farthest extent of the posterior lobe. No representation was found only for the primary visual and auditory cortices.
PathophysiologyThe pathophysiology of CM has not been entirely
established. There are many theories considering the re-sponsible factors, but none of them provides an entirely satisfactory explanation.
The functional hypothesis supports that CM is a kind of negativism on the part of the child who feels betrayed by his parents and doctors (form of “elective mutism”).96 The fact that many patients recover as soon as they get home, in addition to the absence of cranial nerve deficits and the integrity of supratentorial speech centers, sup-ports this theory. Moreover, most of the patients seem to understand spoken language, while some manage to com-municate using gestures. However, it cannot be explained why mutism appears almost exclusively after posterior fossa surgery. The observance that in almost every case patients suffer from dysarthria during the recovery phase supports that there is as organic basis of this syndrome. It is widely accepted that stress and a long hospital stay might retard the recovery of speech and contribute to the common finding among patients with CM of a refusal to eat,27 while the psychological trauma in general is a con-tributing factor for CMS.33
Damage to a specific anatomical substrate has been proposed as a pathogenetic factor. The dentate nucleus
Fig. 1. Connection of dentate nucleus, thalamus, and frontal cortex as presented through the DTC tract. The tract ascends through the su-perior cerebellar peduncles, crosses the midline at the level of the mes-encephalic tegmentum, and reaches the ventrolateral nucleus of the thalamus. From there it ascends through the frontal white matter and spreads to the premotor, supplementary motor and motor cortex. Image created using the iOS application Brain Tutor 3D 2008, Rainer Goebel: http://www.brainvoyager.com/iOS/BrainTutorHD.html.

J Neurosurg: Pediatrics / Volume 12 / December 2013
Cerebellar mutism
607
was the first region that was hypothesized to be involved. Fraioli and Guidetti29 reported on 2 patients with com-plete absence of speech after bilateral stereotactic lesion-ing of the dentate nuclei. Later on many authors proposed that bilateral damage of the dentate nuclei is a critical factor for CM.2,25,53,57,69 Asamoto et al.6 assumed that post-operative edema led to disturbance of the venous circu-lation, which was responsible for the dysfunction of the dentate nuclei. Dietze and Mickle18 observed that injury to the midportion of the cerebellum caused speech dis-orders and if a dentate lesion coexisted, CMS was pres-ent. Ozimek et al.70 noted that a more frequent and more extensive involvement of the dentate nuclei was present in mutistic children, and evident dentate involvement was present in 73.5% of patients with CM in the study by DiRocco et al.17 The authors also noted an even higher rate of dentate nuclei involvement among children with preoperative language impairment (90% when preopera-tive language impairment existed vs 65.2% when it did not exist). Neuroimaging studies have shown bilateral hy-podense areas at the level of the dentate nuclei2,5 or abnor-malities in T2 signal on MRI, within the dentate nuclei, mainly bilaterally.65 However, Dailey et al.14 reported on 9 patients with CM with no edema or infarction of the dentate nucleus postoperatively; in addition, most of the children with CM were still able to perform other func-tions that diffuse dentate destruction or swelling would render impossible. Moreover, Morris et al.65 suggested that neither unilateral nor bilateral dentate damage was required for CMS to appear.
The role of a lesion in the cerebellar hemisphere in CM has also been discussed. Robertson et al.82 noted that bilateral lesion involvement of the cerebellar hemisphere is necessary since CM rarely occurs after resection of tu-mors involving only one hemisphere. Erşahin et al.25 dis-covered an association of left cerebellar hemisphere hy-poperfusion on SPECT scans in patients with CM. Blood flow returned to normal when mutism resolved. Later26 Erşahin and colleagues reported on 1 patient with right cerebellar hemisphere hypoperfusion. Sagiuchi et al.83 reported a case of CM in a 4-year-old boy with atrophy of both cerebellar hemispheres, predominately the right hemisphere, on MRI and circulatory disturbance in both hemispheres secondary to tumor resection in SPECT scans. Besides SPECT perfusion imaging, an alternative technique called arterial spin-labeling perfusion MRI was used on a girl with postoperative CM and showed bi-lateral hypoperfusion in the cerebellar hemisphere, thala-mus, and frontal lobe. Watanabe et al. suggested that this technique was less invasive and more suitable for pediat-ric patients.107 Ozimek et al.70 reported 4 cases of CM with bilateral extension of the tumor into the cerebellar hemi-spheres. There have also been cases of CM with isolated hemispheric lesions such as contusion51 or metastasis.85 Neurophysiological studies have shown that the left cer-ebellar hemisphere is important for the executive func-tions. Lesions of the cerebellar hemisphere lead to deficits in complex mental activities.53 In addition, Ackermann et al.1 proposed that there is tight functional connectivity between the language-dominant frontal lobe and the con-tralateral cerebellar hemisphere, having a significant role
in supporting motor speech function and in the tempo-ral organization of a prearticulatory verbal code (“inner speech”) as well. Riva and Giorgi81 found that children with right cerebellar tumors presented with disturbances of auditory sequential memory and language processing, whereas those with left cerebellar tumors showed deficits on tests of spatial and visual sequential memory. Simi-larly, linguistic processing was found to be impaired in patients with right cerebellar infarction,84 manifested as agrammatism in one case,88 and impaired error detection and practice-related learning of a verb-for-noun genera-tion task in another.28 In a recent case report60 an adult developed PFS after a right cerebellar hemisphere stroke; SPECT imaging that followed demonstrated bilateral ce-rebral perfusional deficits suggesting a phenomenon of “transcallosal” or “transhemispheric diaschisis.” Others have demonstrated that bilateral cerebellar involvement especially of the dentate nuclei is crucial for the devel-opment of cerebellar mutism.57 However, most authors believe that cerebellar hemisphere lesions do not play a significant role in CM. Van Dongen et al.103 believe that a lesion isolated in the cerebellar hemisphere is not able to cause CM. Pollack et al.77 reported that among patients with CM, the postoperative images showed no evidence of discrete areas of infraction, hypoperfusion, or decreased metabolic activity within the cerebellar hemi-sphere. Pollack later noted that CM was absent in cases of large cerebellar hemisphere tumors, resected without splitting the vermis.76 Robertson et al.82 reported a nega-tive correlation between cerebellar hemisphere lesions and CM; they showed that the risk of developing CM was 6.7 times higher in one study53 and 8.2 in another one14 if tumor was located in the cerebellar midline versus the lateral cerebellar hemisphere.
The majority of case reports and studies support that CM can occur after the resection of a midline tu-mor and, as a rule, the vermis is involved.11,25,69,83 Dailey et al.14 were the first to officially suggest that the splitting of the vermis, especially the inferior part, is responsible for the development of CM and that, to avoid oropharygneal apraxia, it must be preserved. Different studies have come to different conclusions since then. Incision of the ver-mis has been associated with a low performance IQ36 and neurophysiological and psychiatric problems.93 Riva and Giorgi81 supported that vermian lesions led to 2 different profiles: postsurgical CM, which evolved into speech dis-orders or language disturbances similar to agrammatism, and behavioral disturbances (ranging from irritability to autistic behavior) supporting the role of vermis as part of a “cerebellar limbic system.”94 Sagiuchi et al.83 reported a case of CM that was associated with atrophy of the ver-mis on MRI and decreased blood flow in the same region on the SPECT scan, and proposed that CM resulted from damage to the vermis with or without a bilateral cerebellar hemisphere lesion. In addition, Frassanito et al.31 reported a case of CM after spontaneous intratumoral bleeding involving the upper cerebellar vermis and believed that the localization of bleeding provided confirmation of the role played by the upper vermis in speech control. Puget et al.78 found that persistent clinical cerebellar signs or fine motor dexterity impairment was significantly related

M. Pitsika and V. Tsitouras
608 J Neurosurg: Pediatrics / Volume 12 / December 2013
to the extent of injury (pre- or postsurgical) to both the inferior vermis and the dentate nuclei. Animal models were also used, and a recent study found that juvenile rats that had vermian splitting operations showed deficient so-cial behavior and vocalization postoperatively, compared with sham-lesioned rats and healthy controls.4 However, other data showed that damage to the vermis is not as important as originally thought. Robertson et al.82 found no correlation between the vermian location of tumor and the development of CM, although there was a nega-tive association between cerebellar hemispheric lesions and CM. Moreover, the authors noticed that the majority of children with posterior fossa tumors undergo radical resection through the vermis and do not develop CMS. Thus, the vermis and surgical approach cannot be the only determinants. Pollack et al.77 hypothesized that if the vermis were responsible for CM then the condition would be more common and more persistent. The delayed onset of CM after posterior fossa surgery is also a negative clue of the role of vermis in CM.76,77
One of the most famous theories about the patho-physiology of CM involves the dentato-thalamo-corti-cal (DTC) tract. This pathway projects to and from the dentate nucleus of the cerebellum on either site, travels through the superior cerebellar peduncle, crosses the mid-line to the opposite side in the decussation of the superior cerebellar peduncle, continues through the brainstem to the contralateral ventrolateral nucleus of thalamus and then to the contralateral motor cerebral cortex (premotor and supplementary motor cortices).90 Mutism can occur after lesion anywhere along this tract,11,32,52 although after posterior fossa surgery, is more likely to involve proximal parts of the tract (dentate nucleus, cerebellar peduncles, and/or brainstem connections).53,82 Miller et al.,63 using another perfusion imaging technique (dynamic suscepti-bility-weighted contrast-enhanced perfusion MRI), found that there is a strong (potentially predictive) relationship between bilateral damage to proximal efferent cerebel-lar pathways and the development of PFS. This finding was also supported by Kusano et al.57 and Morris et al.,65 the first who used diffuse-tensor imaging (DTI). Authors of a recent study from Berlin91 also used DTI in a 3-T MRI suite and showed that volumes of frontocerebellar fibers had significantly diminished fractional anisotropy (FA) values in pediatric patients with CMS after surgery compared with patients without CMS and healthy peers. Diminished fiber signal intensities were localized at the level of the superior cerebellar peduncles and the midline cerebellar structures. Similarly, a case report of an adult who suffered from CM after a left pontine infarction and was investigated using DTI exhibited asymmetry in FA values in the superior cerebellar peduncle.101 Law et al.58 used DTI to investigate the integrity of the cerebello-thalamo-cerebral pathways bilaterally in children who presented with CMS after posterior fossa tumor surgery, and the authors found that right cerebellar white matter within the cerebello-thalamo-cerebral pathway was sig-nificantly compromised in children with CMS compared with children without CMS and healthy children. They suggested that disruption of the connection between the right cerebellum and the left frontal cortex could con-
tribute to the speech and language problems in children with CMS. As potential predictors, they distinguished left-handedness, medulloblastoma tumor type, and large tumor size. Diffusion-tensor imaging could be useful as a screening tool of high-risk patients preoperatively and further randomized large trials could focus on that. A high incidence of brainstem compression preoperatively in addition to edema in brainstem and superior cerebel-lar peduncle among patients with CMS postoperatively seems to confirm their role in CMS.108 Di Rocco et al.17 suggested that dominant-site DTC tract involvement was adequate enough for CMS to appear. Transient dysfunc-tion of the neurons of the A9 to A10 dopaminergic cell group in the mesencephalon, which play a major role in the mesencephalofrontal activating system, has also been proposed as a possible anatomical substrate of CM.10 Apart from a pure anatomical lesion along the DTC tract, cerebellocerebral diaschisis seems to be a possible mech-anism explaining the pathophysiology of CM. Diaschisis is traditionally defined as sudden inhibition of function in an area of the brain remote from, but anatomically con-nected through transsynaptic neural pathways, the site of primary injury. The most common form of diaschisis is crossed cerebellocerebral diaschisis.63 Multiple stud-ies have supported the theory of cerebellocerebral dias-chisis using different imaging techniques that revealed decreased blood flow, metabolic action, and function within supratentorial structures that play a crucial role in speech production, such as the thalami, inferior frontal gyrus, and temporal lobe.26,34,63,65,83 In almost every case the abnormal findings returned to normal when mutism resolved.
The anatomical regions mentioned above can be damaged during the operation or later. Retraction during surgery might cause edema postoperatively, disturbing the venous circulation of the adjacent structures.5,6,18,25,27 However, the course of CMS outlasts the resolution of edema.87 Vasospasm plays a similar role.68,99 Coagulation of the perforators from the posterior inferior cerebellar artery to the brainstem results in the disturbance of blood supply to the pons.6 Alterations in neurotransmitter levels and synaptic or transsynaptic degeneration of connecting structures has also been proposed but not yet confirmed.87 Disturbances in CSF circulation and hydrocephalus as well as postoperative meningitis were considered to play a significant role in CMS, especially hydrocephalus as an exacerbating factor,99 but this significance has been ques-tioned by many authors.9,33,39
Risk FactorsMultiple factors have been studied regarding wheth-
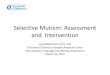
er they predispose to the occurrence of CMS, and some seem to statistically increase the incidence of this syn-drome (Fig. 2). Brainstem involvement seems to be the most important, including preoperative tumor invasion or postoperative edema.26,52,108 Moreover, McMillan et al.61 supported that brainstem compression could be used as a predictor of postoperative CM. Some authors believe that midline location predisposes to the occurrence of CM,9,36,53,55 while others have found no significant differ-ence.26,82 Tumor size had been considered as an indepen-

J Neurosurg: Pediatrics / Volume 12 / December 2013
Cerebellar mutism
609
dent risk factor, but later studies with larger populations showed that it maintains a significance but only in cases of medulloblastomas. Catsman-Berrevoets et al.9 reported that each increase in tumor size by 1 cm in the medullo-blastoma group resulted in a multiplication of the odds to develop “mutism and subsequent dysarthria” (MSD) by 1.76 while Kotil el al.53 reported a multiplication by 1.53 and suggested that medulloblastoma is a risk factor for CM only when the tumor is larger than 5 cm. Küpeli et al.55 reported an increase of the odds by 7.2 if medullo-blastoma occurred and by 5.7 if the family of the patient had a low socioeconomic level. In a multivariate analy-sis Korah et al.52 found that younger age and absence of radiographic evidence of residual tumor were signifi-cant risk factors for CM, while Robertson et al.82 found no significant difference regarding the extent of tumor resection. Di Rocco et al.17 concluded that preoperative language impairment can be considered as a subclini-cal state of CMS in some children and can be used as a predictor. By investigating the relationship between pre-surgical and clinical valuables and the incidence of CMS along with DTI, Law et al.58 found that left-handedness, medulloblastoma tumor type, and large tumor size were features that distinguished between patients with CMS and patients without CMS. Sex, meningitis, and preop-erative hydrocephalus are generally considered as insig-nificant.26,36,82
Surgical AspectsThe splitting of the vermis has been considered as
an important factor for the occurrence of CM as already mentioned. As a result multiple efforts have been made to avoid the splitting or to minimize the extent of the inci-sion. In their study Dailey et al.14 observed that postopera-tive mutism or oropharyngeal apraxia was only seen in children who had a vermian split that included the entire inferior portion of the vermis. Erşahin et al.26 reported that both superior and inferior vermian incisions have been associated with postoperative mutism. However, Siffert et al.87 reported that despite a change in the in-stitutional practice to the non–vermis splitting technique, cases of PFS continued to emerge; the authors did not mention whether there was a decrease in the incidence of the syndrome. Moreover, Pollack76 tried to minimize the length of the vermian incision without eliminating the problem of CM. Thus, he recommended that surgeons make a conscious effort to avoid extensive paravermian manipulation.
In 1997 Kellogg and Piatt48 proposed that the cer-ebellomedullary fissure approach yields exposure com-parable to what can be achieved by splitting the vermis and that the approach minimizes the risk of neurological complications, including MSD. The telovelar approach was originally thought to be a promising new technique for posterior cranial tumors. El-Bahy21 used this approach to the fourth ventricle in 16 patients, and CMS was not observed in any patient. However, among these patients only 3 harbored medulloblastomas while the remaining patients had low-grade tumors and nontumoral lesions; it is not clear how many of these patients were children.
Fig. 2. Diagram illustrating the current knowledge regarding the risk factors that can contribute to the appearance of postop-erative cerebellar mutism.

M. Pitsika and V. Tsitouras
610 J Neurosurg: Pediatrics / Volume 12 / December 2013
Considering these facts together, we can assume that in general the risk of CMS in this group was low, and we cannot come to a conclusion whether this approach was beneficial. Rajesh et al.79 considered that to avoid the sig-nificant incidence of postoperative apraxia and mutism seen with this approach for large tumors, staged dissec-tion of the uvulotonsillar cleft should be achieved with initial arachnoid release, followed by decompression of the tumor and subsequent complete dissection of the uvu-lotonsillar cleft. Frassanito and Massimi30 regarded that the telovelar approach cannot provide significant advan-tages in the prevention of CMS at tumors involving the cerebellar vermis or the brainstem, as both these struc-tures are already damaged by the tumor itself. However, they agreed that it remains an elegant and effective way to reach tumors of the fourth ventricle. Lastly, Hermann et al.43 used a combined transventricular and supracer-ebellar approach to preserve the cerebellar vermis. No instances of akinetic mutism occurred postoperatively. However, since the semisitting position is required for this approach, there is skepticism with regard to the po-tential hazards,75 especially in young children and infants. Apart from the approaches, the neurosurgeon’s qualifica-tion was studied, and Robertson et al.82 found no differ-ence between patients who underwent surgery performed by pediatric neurosurgeons and those who underwent sur-gery performed by general neurosurgeons. Centers with increased experience in pediatric neurosurgical service routinely use brain and cranial nerve electrophysiological monitoring, less aggressive retraction, and minimal ultra-sonic aspiration during their procedures, although there is no significant evidence to support these precautions.108 A recent nonrandomized clinical study22 compared 60 chil-dren who underwent surgery for posterior fossa tumors. Thirty of these children underwent surgery with the aid of with navigated ultrasonography and 30 underwent con-ventional neurosurgical techniques. In the ultrasonogra-phy group only 1 patient with medulloblastoma suffered from CM (3.3%) while in the conventional neurosurgery group, 6 patients were diagnosed with CM (20%); 2 of these patients had medulloblastomas. The difference did not reach statistical significance.
Clinical PresentationThere are some core characteristics of the clinical
presentation of CM. First, mutism in almost every case appears after 1–6 days of normal speech postoperatively (delayed onset). Second, the mutism has a limited du-ration (transient mutism). The CM usually lasts from a few weeks until 6 months, although there are reports of patients whose mutism lasted much longer. Finally, mut-ism is followed by severe dysarthria during the recovery phase, which might last even 2 years.14 Recent studies, however, imply that there are long-term, even permanent, cognitive abnormalities other than dysarthria.71,77
Additional features have been described in the ma-jority of the patients. Motor disorders include ataxia, axial hypotonia,69,104,109 flaccid hemiparesis,8,10,26 and de-creased spontaneous movements or hypokinesia.62,87,109 Recovery of gait and coordination usually take longer than speech.87 Oropharyngeal apraxia is another common
symptom that accompanies CM. The patients refuse to eat and have a difficulty in swallowing,10 although they have an intact gag response14 and normal tongue move-ments on command. Visual disturbances are found in many cases and include persistent eye closure without any oculomotor nerve palsy, horizontal gaze paralysis, and lack of response to visual stimuli.69 Vision loss without cranial nerve palsy has also been reported.87,109 Facial and abducent nerve palsies have been reported but as coexist-ing findings.83,87 Patients with urinary incontinence and loss of bowel control have also been reported.77 Von Hoff et al.106 described the presence of ataxia, nystagmus, and dysmetria in patients after posterior fossa surgery as the “cerebellar syndrome.”
The spectrum of neurobehavioral abnormalities seen in CM is wide. Children can be seen lying curled in bed crying whenever asked to speak,8,66,87 are emotionally la-bile,2,8,70 and show either apathy or irritability.2,52,65,103 Dif-ficulty in eating and loss of bladder and bowel control might also be a form of behavioral disturbance. Behavior returns to normal earlier than speech.8 A recent review56 proposed that the clinical features can be explained as mutism itself mediated primarily by supratentorial dys-function, and clinical findings following mutism are me-diated by direct (surgical) injury of cerebellar and brain-stem structures.
TreatmentThere are quite a few suggestions for treatment in-
terventions for CM. Apart from some individual reports, there are no clinical trials indicating possible beneficial options. Shyu et al.86 reported a case of a 4-year-old boy with CM who was given daily 2.5 mg of zolpidem (a short acting nonbenzodiazepine hypnotic) starting from postoperative Day 21. There was obvious neurological and behavioral improvement, and after 14 days he started using single words and continued to improve steadily. Bromocriptine was used by another team in a 9-year-old girl without the desirable results.25 Catsman-Berrevoets and et al. hypothesized that the lack of speech may be explained by transient dysfunction of the neurons of the A9 to A10 dopaminergic cell group into the mesencepha-lon,10 and the administration of dopamine agonists could reverse this effect. However, neither van Dongen103 nor Echiverri et al.20 found significant results when using this kind of medication in patients with CM. Pretreat-ment with the calcium channel antagonist nimodipine has also been proposed to prevent postoperative vasospasm99 but still more extensive studies need to take place. Gor-don35 has proposed the use of similar treatment for CM as for the elective type (when no organic causes for CM can be found), especially with drugs such as fluoxetine, bromocriptine, and phenelzine. There is a case report of the favorable results of fluoxetine (a selective serotonin reuptake inhibitor) on a child with CM,3 but more clinical trials should take place for further information.
One of the most significant parts of the treatment of patients with CM is the counseling of the parents and the patient about the basis of CM, the duration, and the pos-sible long-lasting speech and language deficits when the mutism resolves. Therapy to improve physiological func-

J Neurosurg: Pediatrics / Volume 12 / December 2013
Cerebellar mutism
611
tioning as well as compensatory strategies to improve in-telligibility, and speech naturalness should be included. Thus far, there have been no clinical trials proving the contribution of speech therapy in the improvement of the neurocognitive status of these children.
OutcomeCerebellar mutism was originally thought to be a
benign self-limiting condition.53 Its short duration is ac-tually part of the definition of CM. However, a signifi-cant number of reports have shown that some children are left with mild residual dysarthria, ataxia, or dysmetria after the resolution of mutism.2,14,27,76,87 As a result some scientists have tried to evaluate the long-term neurocog-nitive outcome in these patients. Children with cerebel-lar damage in general are considered to be at high risk for long-term neurophysiological dysfunction including problems of attention, memory, processing speed, verbal fluency, and behavioral deficits.36,93 Studies with children who had suffered CM showed that they had problems in solving novel situations; moderate difficulty in speed of speech, processing, and reasoning; decreased verbal ini-tiation; and significantly poor performance in reading, spelling, math, and working memory.71,105 These children also seemed more dysfluent, speaking at a slower speech rate than children without CM. Huber et al.46 considered that motor speech deficits persist for a long period of time (> 5 years), and similar findings were made by other au-thors.52,81,92 Lastly, Robertson et al.82 tried to analyze the neurological outcome of their patients, and they found that there is a significant relationship among the level of initial severity of the syndrome and the severity of ataxia and language dysfunction and global intellectual handi-cap after 1 year. It is worth mentioning than in a develop-ing child such persistent symptoms have a lasting impact on global language and cognitive skills.
ConclusionsThe clinical entity of cerebellar mutism after pos-
terior fossa tumor surgery is currently well recognized, and significant clinical and research data have highlight-ed some basic features. An important issue remains the ambiguity regarding the current nomenclature, although some recent reports have provided very useful terminol-ogy.38,97 Advanced imaging techniques are used to identi-fy possible preoperative risk factors (tumor location, size, type, and extension) and to provide a better understanding of the relationship between important anatomical struc-tures and clinical findings. Selection of the less hazardous surgical approaches could be achieved by detailed study of sophisticated neuroimaging and solid knowledge of the surrounding anatomy. High-risk patients can be rec-ognized, and proper counseling of the caregivers is essen-tial in such cases for the potential sequelae and possible outcome. A variety of treatment options are under inves-tigation, and a promising field of research could be that of early speech and behavioral rehabilitation. It should be emphasized that the overall cognitive outcome of this syndrome is not as favorable as previously thought and that periodical neurocognitive assessments of such pa-
tients—especially of younger age, with malignancy, and potentiality for radiation therapy—should be considered.
Acknowledgments
We are grateful to Nikolaos Skoulios, M.D., for his assistance in figure formatting and to Dr. David Arnold for editing the manu-script.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript preparation include the following. Conception and design: Tsitouras. Acquisition of data: Pitsika. Analysis and interpretation of data: Pitsika. Draft-ing the article: Pitsika. Critically revising the article: both authors. Reviewed submitted version of manuscript: both authors. Approved the final version of the manuscript on behalf of both authors: Tsi-touras.
References
1. Ackermann H, Mathiak K, Riecker A: The contribution of the cerebellum to speech production and speech perception: clinical and functional imaging data. Cerebellum 6:202–213, 2007
2. Aguiar PH, Plese JP, Ciquini O, Marino R: Transient mutism following a posterior fossa approach to cerebellar tumors in children: a critical review of the literature. Childs Nerv Syst 11: 306–310, 1995
3. Akhaddar A, Salami M, El Asri AC, Boucetta M: Treatment of postoperative cerebellar mutism with fluoxetine. Childs Nerv Syst 28:507–508, 2012
4. Al-Afif S, Staden M, Krauss JK, Schwabe K, Hermann EJ: Splitting of the cerebellar vermis in juvenile rats—effects on social behavior, vocalization and motor activity. Behav Brain Res 250:293–298, 2013
5. Ammirati M, Mirzai S, Samii M: Transient mutism following removal of a cerebellar tumor. A case report and review of the literature. Childs Nerv Syst 5:12–14, 1989
6. Asamoto M, Ito H, Suzuki N, Oiwa Y, Saito K, Haraoka J: Tran-sient mutism after posterior fossa surgery. Childs Nerv Syst 10:275–278, 1994
7. Buckner RL, Krienen FM, Castellanos A, Diaz JC, Yeo BT: The organization of the human cerebellum estimated by in-trinsic functional connectivity. J Neurophysiol 106:2322–2345, 2011
8. Catsman-Berrevoets CE, Aarsen FK: The spectrum of neu-robehavioural deficits in the Posterior Fossa Syndrome in children after cerebellar tumour surgery. Cortex 46:933–946, 2010
9. Catsman-Berrevoets CE, Van Dongen HR, Mulder PG, Paz y Geuze D, Paquier PF, Lequin MH: Tumour type and size are high risk factors for the syndrome of “cerebellar” mutism and subsequent dysarthria. J Neurol Neurosurg Psychiatry 67:755–757, 1999
10. Catsman-Berrevoets CE, van Dongen HR, Zwetsloot CP: Transient loss of speech followed by dysarthria after removal of posterior fossa tumour. Dev Med Child Neurol 34:1102–1109, 1992
11. Clerico A, Sordi A, Ragni G, Festa A, Cappelli C, Maini CL: Brief report: transient mutism following posterior fossa sur-gery studied by single photon emission computed tomography (SPECT). Med Pediatr Oncol 38:445–448, 2002
12. Coplin WM, Kim DK, Kliot M, Bird TD: Mutism in an adult following hypertensive cerebellar hemorrhage: nosological dis-cussion and illustrative case. Brain Lang 59:473–493, 1997

M. Pitsika and V. Tsitouras
612 J Neurosurg: Pediatrics / Volume 12 / December 2013
13. D’Avanzo R, Scuotto A, Natale M, Scotto P, Cioffi FA: Tran-sient “cerebellar” mutism in lesions of the mesencephalic-cerebellar region. Acta Neurol (Napoli) 15:289–296, 1993
14. Dailey AT, McKhann GM II, Berger MS: The pathophysiolo-gy of oral pharyngeal apraxia and mutism following posterior fossa tumor resection in children. J Neurosurg 83:467–475, 1995
15. De Smet HJ, Baillieux H, Catsman-Berrevoets C, De Deyn PP, Mariën P, Paquier PF: Postoperative motor speech produc-tion in children with the syndrome of ‘cerebellar’ mutism and subsequent dysarthria: a critical review of the literature. Eur J Paediatr Neurol 11:193–207, 2007
16. De Smet HJ, Mariën P: Posterior fossa syndrome in an adult patient following surgical evacuation of an intracerebellar haematoma. Cerebellum 11:587–592, 2012
17. Di Rocco C, Chieffo D, Frassanito P, Caldarelli M, Massimi L, Tamburrini G: Heralding cerebellar mutism: evidence for pre-surgical language impairment as primary risk factor in posterior fossa surgery. Cerebellum 10:551–562, 2011
18. Dietze DD Jr, Mickle JP: Cerebellar mutism after posterior fossa surgery. Pediatr Neurosurg 16:25–31, 1990-1991
19. Dimova PS, Bojinova VS, Milanov IG: Transient mutism and pathologic laughter in the course of cerebellitis. Pediatr Neu-rol 41:49–52, 2009
20. Echiverri HC, Tatum WO, Merens TA, Coker SB: Akinetic mutism: pharmacologic probe of the dopaminergic mesen-cephalofrontal activating system. Pediatr Neurol 4:228–230, 1988
21. El-Bahy K: Telovelar approach to the fourth ventricle: opera-tive findings and results in 16 cases. Acta Neurochir (Wien) 147:137–142, 2005
22. El Beltagy MA, Atteya MM: The benefits of navigated intra-operative ultrasonography during resection of fourth ventricu-lar tumors in children. Childs Nerv Syst 29:1079–1088, 2013
23. Ellis DL, Kanter J, Walsh JW, Drury SS: Posterior fossa syn-drome after surgical removal of a pineal gland tumor. Pediatr Neurol 45:417–419, 2011
24. Erol I, Ozkale Y, Saygi S, Alehan F: Cerebellar mutism caused by primary varicella infection in an immunocompetent child. J Child Neurol [epub ahead of print], 2013
25. Erşahin Y, Mutluer S, Saydam S, Barçin E: Cerebellar mut-ism: report of two unusual cases and review of the literature. Clin Neurol Neurosurg 99:130–134, 1997
26. Erşahin Y, Yararbas U, Duman Y, Mutluer S: Single photon emission tomography following posterior fossa surgery in pa-tients with and without mutism. Childs Nerv Syst 18:318–325, 2002
27. Ferrante L, Mastronardi L, Acqui M, Fortuna A: Mutism after posterior fossa surgery in children. Report of three cases. J Neurosurg 72:959–963, 1990
28. Fiez JA, Petersen SE, Cheney MK, Raichle ME: Impaired non-motor learning and error detection associated with cer-ebellar damage. A single case study. Brain 115:155–178, 1992
29. Fraioli B, Guidetti B: Effects of stereotactic lesions of the den-tate nucleus of the cerebellum in man. Appl Neurophysiol 38: 81–90, 1975
30. Frassanito P, Massimi L: Cerebellar mutism: review of the lit-erature. Childs Nerv Syst 27:867–868, 2011 (Letter)
31. Frassanito P, Massimi L, Caldarelli M, Di Rocco C: Cerebel-lar mutism after spontaneous intratumoral bleeding involving the upper cerebellar vermis: a contribution to the physiopatho-genic interpretation. Childs Nerv Syst 25:7–11, 2009
32. Frim DM, Ogilvy CS: Mutism and cerebellar dysarthria after brain stem surgery: case report. Neurosurgery 36:854–857, 1995
33. Gelabert-González M, Fernández-Villa J: Mutism after poste-rior fossa surgery. Review of the literature. Clin Neurol Neu-rosurg 103:111–114, 2001
34. Germanò A, Baldari S, Caruso G, Caffo M, Montemagno G,
Cardia E, et al: Reversible cerebral perfusion alterations in children with transient mutism after posterior fossa surgery. Childs Nerv Syst 14:114–119, 1998
35. Gordon N: Mutism: elective or selective, and acquired. Brain Dev 23:83–87, 2001
36. Grill J, Viguier D, Kieffer V, Bulteau C, Sainte-Rose C, Hart-mann O, et al: Critical risk factors for intellectual impairment in children with posterior fossa tumors: the role of cerebellar damage. J Neurosurg 101 (2 Suppl):152–158, 2004
37. Grodd W, Hülsmann E, Lotze M, Wildgruber D, Erb M: Sen-sorimotor mapping of the human cerebellum: fMRI evidence of somatotopic organization. Hum Brain Mapp 13:55–73, 2001
38. Gudrunardottir T, Sehested A, Juhler M, Grill J, Schmiegelow K: Cerebellar mutism: definitions, classification and grading of symptoms. Childs Nerv Syst 27:1361–1363, 2011 (Letter)
39. Gudrunardottir T, Sehested A, Juhler M, Schmiegelow K: Cer-ebellar mutism: incidence, risk factors and prognosis. Childs Nerv Syst 27:513–515, 2011 (Letter)
40. Gudrunardottir T, Sehested A, Juhler M, Schmiegelow K: Cerebellar mutism: review of the literature. Childs Nerv Syst 27:355–363, 2011
41. Habas C: Functional imaging and the cerebellum: recent de-velopments and challenges. Editorial. Cerebellum 11:311–313, 2012
42. Habas C, Kamdar N, Nguyen D, Prater K, Beckmann CF, Me-non V, et al: Distinct cerebellar contributions to intrinsic con-nectivity networks. J Neurosci 29:8586–8594, 2009
43. Hermann EJ, Rittierodt M, Krauss JK: Combined transven-tricular and supracerebellar infratentorial approach preserv-ing the vermis in giant pediatric posterior fossa midline tu-mors. Neurosurgery 63 (1 Suppl 1):ONS30–ONS37, 2008
44. Hirsch JF, Renier D, Czernichow P, Benveniste L, Pierre-Kahn A: Medulloblastoma in childhood. Survival and func-tional results. Acta Neurochir (Wien) 48:1–15, 1979
45. Holmes G: The symptoms of acute cerebellar injuries due to gunshot injuries. Brain 40:461–535, 1917
46. Huber JF, Bradley K, Spiegler BJ, Dennis M: Long-term ef-fects of transient cerebellar mutism after cerebellar astrocyto-ma or medulloblastoma tumor resection in childhood. Childs Nerv Syst 22:132–138, 2006
47. Ildan F, Tuna M, Erman T, Göçer AI, Zeren M, Cetinalp E: The evaluation and comparison of cerebellar mutism in children and adults after posterior fossa surgery: report of two adult cases and review of the literature. Acta Neurochir (Wien) 144:463–473, 2002
48. Kellogg JX, Piatt JH Jr: Resection of fourth ventricle tumors without splitting the vermis: the cerebellomedullary fissure approach. Pediatr Neurosurg 27:28–33, 1997
49. Kelly RM, Strick PL: Cerebellar loops with motor cortex and prefrontal cortex of a nonhuman primate. J Neurosci 23:8432–8444, 2003
50. Kim SG, Uğurbil K, Strick PL: Activation of a cerebellar out-put nucleus during cognitive processing. Science 265:949–951, 1994
51. Koh S, Turkel SB, Baram TZ: Cerebellar mutism in children: report of six cases and potential mechanisms. Pediatr Neurol 16:218–219, 1997
52. Korah MP, Esiashvili N, Mazewski CM, Hudgins RJ, Tighi-ouart M, Janss AJ, et al: Incidence, risks, and sequelae of posterior fossa syndrome in pediatric medulloblastoma. Int J Radiat Oncol Biol Phys 77:106–112, 2010
53. Kotil K, Eras M, Akçetin M, Bilge T: Cerebellar mutism fol-lowing posterior fossa tumor resection in children. Turk Neu-rosurg 18:89–94, 2008
54. Krienen FM, Buckner RL: Segregated fronto-cerebellar cir-cuits revealed by intrinsic functional connectivity. Cereb Cortex 19:2485–2497, 2009
55. Küpeli S, Yalçın B, Bilginer B, Akalan N, Haksal P, Büyük-

J Neurosurg: Pediatrics / Volume 12 / December 2013
Cerebellar mutism
613
pamukçu M: Posterior fossa syndrome after posterior fossa surgery in children with brain tumors. Pediatr Blood Cancer 56:206–210, 2011
56. Küper M, Timmann D: Cerebellar mutism. Brain Lang [epub ahead of print], 2013
57. Kusano Y, Tanaka Y, Takasuna H, Wada N, Tada T, Kakizawa Y, et al: Transient cerebellar mutism caused by bilateral dam-age to the dentate nuclei after the second posterior fossa sur-gery. Case report. J Neurosurg 104:329–331, 2006
58. Law N, Greenberg M, Bouffet E, Taylor MD, Laughlin S, Strother D, et al: Clinical and neuroanatomical predictors of cerebellar mutism syndrome. Neuro Oncol 14:1294–1303, 2012
59. Lotze M, Montoya P, Erb M, Hülsmann E, Flor H, Klose U, et al: Activation of cortical and cerebellar motor areas during executed and imagined hand movements: an fMRI study. J Cogn Neurosci 11:491–501, 1999
60. Mariën P, De Smet HJ, Wijgerde E, Verhoeven J, Crols R, De Deyn PP: Posterior fossa syndrome in adults: a new case and comprehensive survey of the literature. Cortex 49:284–300, 2013
61. McMillan HJ, Keene DL, Matzinger MA, Vassilyadi M, Nzau M, Ventureyra EC: Brainstem compression: a predictor of postoperative cerebellar mutism. Childs Nerv Syst 25:677–681, 2009
62. Mei C, Morgan AT: Incidence of mutism, dysarthria and dysphagia associated with childhood posterior fossa tumour. Childs Nerv Syst 27:1129–1136, 2011
63. Miller NG, Reddick WE, Kocak M, Glass JO, Löbel U, Morris B, et al: Cerebellocerebral diaschisis is the likely mechanism of postsurgical posterior fossa syndrome in pediatric patients with midline cerebellar tumors. AJNR Am J Neuroradiol 31:288–294, 2010
64. Morgan AT, Liégeois F, Liederkerke C, Vogel AP, Hayward R, Harkness W, et al: Role of cerebellum in fine speech control in childhood: persistent dysarthria after surgical treatment for posterior fossa tumour. Brain Lang 117:69–76, 2011
65. Morris EB, Phillips NS, Laningham FH, Patay Z, Gajjar A, Wallace D, et al: Proximal dentatothalamocortical tract in-volvement in posterior fossa syndrome. Brain 132:3087–3095, 2009
66. Mortimer DS: Clinical case study: a 4-year-old boy with pos-terior fossa syndrome after resection of a medulloblastoma. J Neurosci Nurs 43:225–229, 2011
67. Murdoch BE: The cerebellum and language: historical per-spective and review. Cortex 46:858–868, 2010
68. Nagatani K, Waga S, Nakagawa Y: Mutism after removal of a vermian medulloblastoma: cerebellar mutism. Surg Neurol 36:307–309, 1991
69. Ozgur BM, Berberian J, Aryan HE, Meltzer HS, Levy ML: The pathophysiologic mechanism of cerebellar mutism. Surg Neurol 66:18–25, 2006
70. Ozimek A, Richter S, Hein-Kropp C, Schoch B, Gorissen B, Kaiser O, et al: Cerebellar mutism—report of four cases. J Neurol 251:963–972, 2004
71. Palmer SL, Hassall T, Evankovich K, Mabbott DJ, Bonner M, Deluca C, et al: Neurocognitive outcome 12 months following cerebellar mutism syndrome in pediatric patients with medul-loblastoma. Neuro Oncol 12:1311–1317, 2010
72. Papavasiliou AS, Kotsalis C, Trakadas S: Transient cerebel-lar mutism in the course of acute cerebellitis. Pediatr Neurol 30:71–74, 2004
73. Petersen SE, Fox PT, Posner MI, Mintun M, Raichle ME: Pos-itron emission tomographic studies of the cortical anatomy of single-word processing. Nature 331:585–589, 1988
74. Petersen SE, Fox PT, Posner MI, Mintum M, Raichle ME: Positron emission tomographic studies of the processing of single words. J Cogn Neurosci 1:153–170, 1989
75. Piatt JH, Kellogg JX: A hazard of combining the infratento-
rial supracerebellar and the cerebellomedullary fissure ap-proaches: cerebellar venous insufficiency. Pediatr Neuro-surg 33:243–248, 2000
76. Pollack IF: Neurobehavioral abnormalities after posterior fos-sa surgery in children. Int Rev Psychiatry 13:302–312, 2001
77. Pollack IF, Polinko P, Albright AL, Towbin R, Fitz C: Mutism and pseudobulbar symptoms after resection of posterior fossa tumors in children: incidence and pathophysiology. Neuro-surgery 37:885–893, 1995
78. Puget S, Boddaert N, Viguier D, Kieffer V, Bulteau C, Gar-nett M, et al: Injuries to inferior vermis and dentate nuclei predict poor neurological and neuropsychological outcome in children with malignant posterior fossa tumors. Cancer 115: 1338–1347, 2009
79. Rajesh BJ, Rao BR, Menon G, Abraham M, Easwer HV, Nair S: Telovelar approach: technical issues for large fourth ven-tricle tumors. Childs Nerv Syst 23:555–558, 2007
80. Rekate HL, Grubb RL, Aram DM, Hahn JF, Ratcheson RA: Muteness of cerebellar origin. Arch Neurol 42:697–698, 1985
81. Riva D, Giorgi C: The cerebellum contributes to higher func-tions during development: evidence from a series of children surgically treated for posterior fossa tumours. Brain 123: 1051–1061, 2000
82. Robertson PL, Muraszko KM, Holmes EJ, Sposto R, Packer RJ, Gajjar A, et al: Incidence and severity of postoperative cerebellar mutism syndrome in children with medulloblas-toma: a prospective study by the Children’s Oncology Group. J Neurosurg 105 (6 Suppl):444–451, 2006
83. Sagiuchi T, Ishii K, Aoki Y, Kan S, Utsuki S, Tanaka R, et al: Bilateral crossed cerebello-cerebral diaschisis and mutism after surgery for cerebellar medulloblastoma. Ann Nucl Med 15:157–160, 2001
84. Schmahmann JD, Sherman JC: The cerebellar cognitive af-fective syndrome. Brain 121:561–579, 1998
85. Sherman JH, Sheehan JP, Elias WJ, Jane JA Sr: Cerebellar mutism in adults after posterior fossa surgery: a report of 2 cases. Surg Neurol 63:476–479, 2005
86. Shyu C, Burke K, Souweidane MM, Dunkel IJ, Gilheeney SW, Gershon T, et al: Novel use of zolpidem in cerebellar mutism syndrome. J Pediatr Hematol Oncol 33:148–149, 2011
87. Siffert J, Poussaint TY, Goumnerova LC, Scott RM, LaValley B, Tarbell NJ, et al: Neurological dysfunction associated with postoperative cerebellar mutism. J Neurooncol 48:75–81, 2000
88. Silveri MC, Leggio MG, Molinari M: The cerebellum con-tributes to linguistic production: a case of agrammatic speech following a right cerebellar lesion. Neurology 44:2047–2050, 1994
89. Sinha AK, Rajender Y, Dinakar I: Transient cerebellar mut-ism after evacuation of a spontaneous vermian haematoma. Childs Nerv Syst 14:460–462, 1998
90. Snell RS: Clinical Neuroanatomy for Medical Students, ed 5. Baltimore: Lippincott Williams & Wilkins, 2001, pp 237–238
91. Soelva V, Hernáiz Driever P, Abbushi A, Rueckriegel S, Bruhn H, Eisner W, et al: Fronto-cerebellar fiber tractography in pediatric patients following posterior fossa tumor surgery. Childs Nerv Syst 29:597–607, 2013
92. Steinbok P, Cochrane DD, Perrin R, Price A: Mutism after posterior fossa tumour resection in children: incomplete re-covery on long-term follow-up. Pediatr Neurosurg 39:179–183, 2003
93. Steinlin M, Imfeld S, Zulauf P, Boltshauser E, Lövblad KO, Ridolfi Lüthy A, et al: Neuropsychological long-term sequel-ae after posterior fossa tumour resection during childhood. Brain 126:1998–2008, 2003
94. Stoodley CJ, Schmahmann JD: Evidence for topographic or-ganization in the cerebellum of motor control versus cognitive and affective processing. Cortex 46:831–844, 2010

M. Pitsika and V. Tsitouras
614 J Neurosurg: Pediatrics / Volume 12 / December 2013
95. Strick PL, Dum RP, Fiez JA: Cerebellum and nonmotor function. Annu Rev Neurosci 32:413–434, 2009
96. Tasdemiroğlu E, Kaya M, Yildirim CH, Firat L: Postoperative cerebellar mutism and autistic spectrum disorder. Childs Nerv Syst 27:869–878, 2011
97. Thomale UW, Driever PH: Inconsistent terminology for cer-ebellar mutism. Childs Nerv Syst 29:717–718, 2013 (Letter)
98. Tohgi H, Takahashi S, Chiba K, Hirata Y: Cerebellar infarc-tion. Clinical and neuroimaging analysis in 293 patients. Stroke 24:1697–1701, 1993
99. Turgut M: Transient “cerebellar” mutism. Childs Nerv Syst 14:161–166, 1998
100. Turkstra LS, Bayles KA: Acquired mutism: physiopathy and assessment. Arch Phys Med Rehabil 73:138–144, 1992
101. van Baarsen K, Kleinnijenhuis M, Konert T, van Cappellen van Walsum AM, Grotenhuis A: Tractography demonstrates dentate-rubro-thalamic tract disruption in an adult with cerebellar mutism. Cerebellum [epub ahead of print], 2013
102. Van Dijk KR, Hedden T, Venkataraman A, Evans KC, Lazar SW, Buckner RL: Intrinsic functional connectivity as a tool for human connectomics: theory, properties, and optimiza-tion. J Neurophysiol 103:297–321, 2010
103. van Dongen HR, Catsman-Berrevoets CE, van Mourik M: The syndrome of ‘cerebellar’ mutism and subsequent dysar-thria. Neurology 44:2040–2046, 1994
104. van Mourik M, Catsman-Berrevoets CE, van Dongen HR, Neville BG: Complex orofacial movements and the disap-pearance of cerebellar mutism: report of five cases. Dev Med Child Neurol 39:686–690, 1997
105. Vandeinse D, Hornyak JE: Linguistic and cognitive deficits associated with cerebellar mutism. Pediatr Rehabil 1:41–44, 1997
106. von Hoff K, Kieffer V, Habrand JL, Kalifa C, Dellatolas G, Grill J: Impairment of intellectual functions after surgery and posterior fossa irradiation in children with ependymoma is related to age and neurologic complications. BMC Cancer 8:15, 2008
107. Watanabe Y, Yamasaki F, Nakamura K, Kajiwara Y, Takayasu T, Nosaka R, et al: Evaluation of cerebellar mutism by arte-rial spin-labeling perfusion magnetic resonance imaging in a patient with atypical teratoid/rhabdoid tumor (AT/RT): a case report. Childs Nerv Syst 28:1257–1260, 2012
108. Wells EM, Khademian ZP, Walsh KS, Vezina G, Sposto R, Keating RF, et al: Postoperative cerebellar mutism syndrome following treatment of medulloblastoma: neuroradiographic features and origin. Clinical article. J Neurosurg Pediatr 5: 329–334, 2010
109. Wells EM, Walsh KS, Khademian ZP, Keating RF, Packer RJ: The cerebellar mutism syndrome and its relation to cere-bellar cognitive function and the cerebellar cognitive affec-tive disorder. Dev Disabil Res Rev 14:221–228, 2008
110. Wisoff JH, Epstein FJ: Pseudobulbar palsy after poste-rior fossa operation in children. Neurosurgery 15:707–709, 1984
Manuscript submitted April 4, 2013.Accepted August 12, 2013.Please include this information when citing this paper: published
online September 27, 2013; DOI: 10.3171/2013.8.PEDS13168.Address correspondence to: Vassilios Tsitouras, M.D., Depart-
ment of Pediatric Neurosurgery, Mitera Children’s Hospital, 6 Ery -throu Stavrou St., Marousi, Athens 151 23, Greece. email: vatsitouras @yahoo.gr.