-
8/3/2019 Cephalometric Assessment in OSA
1/10
Cephalometric assessment in obstructive sleep apnea
Nonglak Pracharktam, DDS, MSD, a Suchitra Nelson, PhD, b Mark G.
Hans, DDS, M SD, B. Holly Broadbent, DDS, a Susan Redline, MD, MPH,
e Carl Rosenberg, MD,' andKingman P. Strohl, MD gCleveland,
Ohio
It is reported that some specific craniofacial characteristics
are associated with obstructive sleepapnea syndrome (OSAS). To test
this finding, the present study developed and assessed
thefeasibility of a craniofacial index score (CIS) in
differentiating patients with OSAS from habitualsnorers.
Anthropometric measurements and lateral head radiographs were
obtained on 24 maleand 4 female patients with OSAS who had
physician-diagnosed OSAS (respiratory disturbanceindex (RDI)
>20), and 25 male and 5 female habitual snorers (RDI
-
8/3/2019 Cephalometric Assessment in OSA
2/10
American Journal of Orthodontics and Dentofacial Orthopedics P r
a c h a r k ta m et aL4 1 1Volume 109, No. 4
i n d e v e l o p i n g O S A S . Ve r i fi c a ti o n o f c e p
h a l o m e t r i cv a r i a b l e s t h a t p r e d i c t c r a n
i o f a c i a l a n a t o m i c r is k sa s s o c ia t e d w i th O
S A S m a y i m p a c t b o t h t h e d i a g -n o s is a n d t h e
t r e a t m e n t o f t h e s e p a t i en t s . T h e
p u r p o s e o f t h is s t u d y w a s t o d e t e r m i n e t
h e f e a si -b i li ty o f u s i n g a s p e c i fi c s e t o f c
e p h a l o m e t r i c a n da n t h r o p o m e t r i c v a r i a
b l e s t o c la s s if y p e r s o n s i n t o as n o r i n g a n
d a n O S A S g r o u p w i t h a d e r i v ed c r a -n i o f a c i
a l i n d e x s c o r e ( C I S ) t h a t i n c l u d e d a g e a n
dw e i g h t in t h e d i s c r i m i n a n t f u n c t i o n .
M AT E R I A L S A N D M E T H O D SStudy popu la t ion
Tw e n t y - f o u r m a l e a n d f o u r f e m a l e w h i t e
p a t i e n t swi th O SA S an d wi th a c l in i ca l h i s to ry
o f excess ive day-t i m e s l e ep i n e ss , e p i s o d e s o f
o b s t r u c t e d b r e a t h i n g d u r i n g
s leep , and loud sno r ing we re recru i t ed f rom a loca l s
leepl a b o r a t o ry. Tw e n t y - s ix s u b je c t s u n d e r
w e n t a s t a n d a r dp o l y s o m n o g r a p h i c s t u d y
f o r e i t h e r h a l f a n i g h t o r 1 n i g h ta n d h a d a
r e s p i r a t o r y d i s t u r b a n c e i n d e x ( a p n e a a
n dh y p o p n e a p e r h o u r ) g r e a t e r t h a n 2 0 . Tw o
s u b j e c ts w e r ee v a l u a t e d b y t h e i r p h y s i c i
a n w h o u s e d o x y g e n s a t u ra t i o nm o n i t o r i n g
( C r i t i c a r e P u l s e O x i m e t e r m o d e l n o . 5 0
1p lus , Cr i t i ca re Corp . , Mi lwaukee , Wis . ) fo r 2 n igh
t s , andh a d r e p e t it i v e e p i s o d e s o f a r te r i a
l o x y g e n d e s a t u r a t i o nm o r e t h a n 4 % f r o m b
a s e l i n e w i t h t h e c u m u l a t i v e p e r -c e n t a g
e s o f ti m e s p e n t a t n o r m a l s a t u r a t i o n b e l
o w 9 0 %.Al l sub jec t s rece ived con t inuous pos i t ive a i r
p res su ret r e a t m e n t , a n d n o n e h a d a u v u l o p h
a r y n g o p a l a t o p l a s t y o r
o t h e r s u rg i c a l t r e a t m e n t b e f o r e c e p h a
l o m e t r i c r a d i o -g r a p h s w e r e t a k e n .
Twen ty - f ive male and f ive fem ale wh i t e hab i tua l
snor-e r s c o m p o s e d t h e c o n t r o l g r o u p . Th i r t
e e n o f t h e c o n t r o ls u b j e ct s w e r e e v a l u a t e
d w i t h o x y g e n s a t u r a ti o n m o n i t o r -i n g (C r
i t ic a r e P u l s e O x i m e t e r m o d e l # 5 0 1 p l u s )
f o r 2n igh t s . None o f these sub jec t s had a c l in i ca l h
i s to ry o fac t ive day t ime s l eep iness . In add i t ion , t
he pu l se ox imeters h o w e d n o e v i d e n c e o f r ep e t i
ti v e e p i s o d e s o f d e s a t u r a t i o nind ica t ing a l
ack o f subs tan t i a l apn e ic ac t iv ity. S tan dardo v e r n
i g h t p o l y s o m n o g r a p h i c s tu d y w a s p e r f o r
m e d o n 1 0s u b j ec t s i n th e c o n t r o l g r o u p t o e
v a l u a t e h e a v y s n o r i n g a n dt o r u l e o u t O S A
S . S e v e n o f t h e c o n t r o l s u b j e c ts w e r e
e v a l u a t e d f o r a b n o r m a l s l e e p - b r e a t h
i n g c o n d i t io n s w i t h ap o r t a b l e h o m e m o n i t
o r ( E d e n t e c M o n i t o r i n g S y s t e m ,m o d e l 4 7
0 0 S c a n n e r o r Ed e n t r a c e I I , Ed e n P r a ir ie
,Minn . ) . A l l 17 sub jec t s wi th s l eep s tud ies had a resp
i ra to ryd i s tu rba nce index o f l ess than 20 an d a l ack o f
c lin i ca ls y m p t o m s o f O S A S .
S t a n d a r d o v e r n i g h t p o l y s o m n o g r a p h y
i n c l u d e d : o r o -nasa l a i r flow me asu red w i th
thermis t e r, resp i ra to ry e ffo r ta s s e s se d b y s u r f
a c e c h e s t w a l l a n d a b d o m i n a l e l e c -t romyo
graphy , a r t e r i a l s a tu ra t ion as sessed by f inger pu l
seox imeter (Nel l co r N-200 Pu l se Ox imeter, Nel l co r Inc .
,Ca l if .) , and s l eep s t ages eva lua ted by e l ec t roence
pha log-raphy, e l ec t roocu lography, e l ec t rocard iography,
and sub-m e n t a l a n d t i b i a l e l e c t r o m y o g r a p h
y. R e c o r d i n g s w e r e
o b t a i n e d w i t h a p o l y g r a p h ( G r a s s M o d e
l 7 8 R e s e a r c hP o l y s o m n o g r a p h , G r a s s I n s
t r u m e n t C o . , M a s s . ). A r e s p i-r a t o r y e v e n
t ( a p n e a o r h y p o p n e a ) w a s d e f i n e d a s acessa
t ion o r d i scern ib le reduc t ion in a i r f low, l as t ing a
tl eas t 10 seconds , and as soc ia t ed wi th e i ther a 4% org r
e a t e r d e c r e a s e i n o x y g e n sa t u r a ti o n , o r a
2 % o r g r e a t e rd e c r e a s e i n o x y g e n s a t u r a t
io n a c c o m p a n i e d b y a na r o u s a l . Th e r e s p i r
a t o r y d i s t u r b a n c e i n d e x ( R D I ) w a sc a l c u
l a t e d b y t h e t o ta l s u m o f a p n e a s a n d h y p o p
n e a sd iv ided by to t a l s l eep t ime .
Anth ropom et r ic and cep ha lome t r ic da ta co l lec t
ion
A n t h r o p o m e t r i c d a t a i n c l u d e d s ex , a g
e, b o d y m a s sindex (kg/m2), as wel l as head/facial form.
Class i f icat iono f h e a d f o r m s a n d f a c i al ty p e s w
a s p e r f o r m e d a c c o r d i n gt o M o n t a g u . 32 C e p
h a l o g r a m s w e r e o b t a i n e d w i t h t h et e e t h t
o g e t h e r i n c e n t r i c o c c l u s i o n a s p r e v i o u
s l y d e -scr ibed . 33 Cen t r i c occ lus ion w as u sed to min
im ize var i -
a b i li ty in m a n d i b u l a r a n d s o f t t is s u e m e
a s u r e m e n t s o f t e nassoc ia t ed wi th res t pos i t ion
. To fu r ther min imize var i a -t ions in so f t t i s sues , t
he l a t e ra l cepha logram was t akenu s i n g n a t u r a l h e
a d p o s t u r e , a t t h e e n d o f t h e e x p i r a ti o np h
a s e , a n d w i t h o u t s w a l l o w i n g . We h a d t h e p
a t i e n tr e s p o n d t o t h e x - r a y t e c h n i c ia n b y
r a is i n g t h e i n d e x f in g e ra s r a d i o g r a p h s w
e r e t a k e n t o i n d i c a t e t h a t t h e p a t i e n tw a
s a w a k e a n d n o t s w a ll o w in g . N a t u r a l h e a d p
o s t u r e w a sf o u n d b y h a v i n g t h e p a t i e n t l o
o k i n t o h i s o w n p u p i l sre f l ec t ed in a m i r ro r
loca ted a t eye l eve l . To c l a r ify theou t l ine o f the o
ro pha ryng ea l so f t t is sues , pa t i en t s swal -l o w e d a
t a b l e s p o o n o f b a r i u m s u l f at e e s o p h a g e a
l c r e a m( Es o p h o t r a s t , R o e r P h a r m a c e u t i c
a l C o r p . , F o r t Wa s h -
ing ton , Pa . ) . The pa t i en t s were asked to f i r s t d i
s t r ibu tet h e c r e a m w i t h i n t h e o r a l c a v it y u
s i n g t h e t o n g u e f o r 1 0s e c o n d s , t h e n t h e p
a t i e n t w a s a s k e d t o s w a l l o w t h er e m a i n i n
g c r e a m .
A l l c e p h a l o m e t r i c l a n d m a r k s w e r e l o c
a t e d a n d d i g i -t i z e d ( S u m m a g r a p h i c s , I n
c . ) b y th e s a m e i n v e s ti g a t o r( N . P. ) , w i t h c
u s t o m i z e d s o f t w a r e d e v e l o p e d f o r t w o -d
i m e n s i o n a l m o r p h o l o g i c a n a ly s is o f a n a t
o m y ( G e o C a l c ,c o u r t e s y o f D rs . J o h n B l a n k
a n d R o b e r t M e n s f o r t h ,Cleve land Sta t e Un ivers i
ty ) . Def in i t ion o f l andm arks ,r e f e r e n c e l i n e s
, a n d c e p h a l o m e t r i c m e a s u r e m e n t s w e r ed
e s c r i b e d i n o u r p r e v i o u s s t u d y ? 3 A d d i t i
o n a l c e p h a l o -m e t r i c v a ri a b l es u s e d i n t h
e p r e s e n t s t u d y a r e p r e s e n t e d
in Tab le I and F ig . 1 . The re l a t ionsh ip be tween ske le
t a la n d s o f t t is s u e c o m p o n e n t s w a s d e t e r m
i n e d b y t h e r a ti oo f th e t o n g u e a r e a t o t h e i
n t er m a x i l la r y s p a c e i n t h es a g it ta l p l a n e
a s p r e v i o u s ly r e p o r t e d b y Vi g a n d C o h e n
34(Fig . 2 ) . Th e cou n terp ar t ana lys is o f En low 3s was u
sed toana lyze c ran ia l fos sa a l ignmen t , ramus wid th re l a
t ive tot h e m i d d l e c r a n i a l f o s s a , a n d r e l a t
i v e c o m p a r i s o n o fmax i l l a ry l eng th wi th mand ibu
la r l eng th (F igs . 3 -4 )
Erro rs in l andmark iden t i f i ca t ion and d ig i t i z ingm
e t h o d w e r e e s t i m a t e d b y e x a m i n i n g d u p l i
c a t e t r a c i n g sof 25% o f the l a t e ra l he ad f i lms (n
= 15 pa i r s ) . Re l i ab i l-i t y was fa i r ly accu ra te wi
th p a i red t t es ts i nd ica t ing n os ign i f i can t d i ffe
rences (p < 0 .05 ) in the dup l i ca t e mea-su rem en t s (
see Tab le IV) . Th e re l i ab i l it y o f a sub jec t ' s
-
8/3/2019 Cephalometric Assessment in OSA
3/10
41 2 P r a c h a r k t a m e t a l. American Journal of
Orthodontics and D entofacial O rthopedicsApril 1996
C 2 t g ~
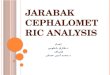
Fig. 1. Conventional linear and angular eephalometric
mea-surement s and additional soft tissue measurem ents (see Fig.
3. Counterpart analysis, as This diagram shows effects ofTable I).
rotational alignment of subject' s own MCF compared with
neutral MCF on corresponding maxi llary and mandibula rplacement
. Clockwise (+) alignment is shown. Relative com-parison of
cumulative maxillary length f rom Ar to A point withcumulative
mandibular length f rom Ar to B point is alsodemonstrated.
Fig. 2. Ratio of tong ue are a to intermaxillary area.
Definition ofthe anterior intermaxillary space height (AntrMxHt),
posteriormaxillary spa ce heigh t (Po strMx Ht), intermaxillary sp
acelength (InMxLth). , and intermaxillary a rea was previou sly
de-scr ibed by Vig and Cohen.34
natural head position tested randomly by selecting 14subjects
and recording the natural head position beforeand after taking the
radiograph, also revealed no signif-icant difference (p
-
8/3/2019 Cephalometric Assessment in OSA
4/10
American ,Journal of Orthodontics and Dentofacia l Orthopedics P
ra ch ar kt a m et a l . 4 1 3Volume109,No. 4
T a b l e I. A d d i t i o n a l c e p h a l o m e t r i c v a r
i a b le s u s e d i n t h e p r e s e n t s t u d y
Variables Interpreta t ion
Hard t i s sues
M C FR a m/ M C FA r A - A r B
H - M P
H - Ve r
N e c k< C2C4-SN
< 2C-SNSof t t i s sues
P-PNSPhw-Psp
T1H e a d p o s tu r e
F H - H o r
R a t i oCI/FITflnMx area
Mid dle cranial fossa and posterior m axillary relat ive al
ignment (Fig . 3) .Ram us width relat ive to m iddle cranial fossa
horizontal d imension (Fig . 4) .Relat ive comparison of cumulative
maxillary length with cumulat ive mand ibular length mea sured
along
the re ference l ine Fig . 3 .Vert ical posi t ion of the hyoid
relat ive to the mand ibular p lane.Vert ical posi t ion of the
hyoid relat ive to a l ine which is perpendic ular to p
terygomaxillary vert ical l ine
(PM) and passes sphenoethm oidal junct ion (SE).
A craniocervical angle formed by a l ine from the most po
sterior-inferior point of the second cervicalverteb ra (C2) to the
forth cervical verteb ra (C4) and S-N plane.
A craniocervical ang le formed by a l ine from C2 to C2 tang ent
(C2tg) and S-N plane.
Soft palate length .Supe rior posterior airway space. Dis tance
betw een the most superior-po sterior point of the soft palate
and p osterior pharyngeal wall , measured along a l ine paral
lel to B-Go.
Tongue length . L ength of the tongue m easured from tong ue t
ip ( t t ) to epig lo t t is base (Eb ).
An gle between the Frank fort horizontal l ine and the
extracranial horizontal line obtained by a f luidlevel device with
a metalic line.
Rat io o f the cranial index to the facial index.Rat io betw een
tongue area to in termaxil lary area Fig . 2 .
t h e m e a n s b e t w e e n t h e t w o g r o up s w a s c o m
p a r e d w i t ht te s t s ( e q u a l v a r i a n c e ) . B e c a
u s e o f t h e h i g h n u m b e r o fc o m p a r i s o n t e s t
s o f t h e m e a n s o f t h e t w o g r o u p s , a
p v a l u e o f l e s s t h a n 0 .0 0 2 , w i t h B o n f e r r
o n i ' s c o r r e c t i o nw a s u s e d t o d e t e r m i n e s
t a t is t i c a l s i g ni f ic a n c e .
L i n e a r c o r r e l a t i o n w a s c o m p u t e d f o r th
e 2 2 c e p h a l o -m e t r i c v a r i a b l e s t o a s s e s s
i n t e r d e p e n d e n c y a m o n g v a r i -a b l e s. I t w a
s d e c i d e d t h a t a s u b s e t o f th e 2 2 c e p h a l o -m
e t r i c v a r i a b l e s w o u l d b e c h o s e n i f s e v e r
a l v a r i a b l e sw e r e v e r y h i g h l y c o r r e l a t e
d w i t h e a c h o t h e r ( p - < 0 . 0 01 ) .I n a d d i t i
o n , t h e f i n a l v a r i a b l e s w e r e c h o s e n i n a c
c o r d a n c ew i t h r e s u l t s o f p u b l i s h e d l i t e
r a tu r e .
F i n a l l y, t h e d i s c r i m i n a n t f u n c t i o n t h
a t b e s t c l a s s i f i e dt h e s u b j e c t s w a s u s e d
t o c a l c u l a t e t h e C I S . T h e C I S w a sd e f i n e d
a s t h e m i d p o i n t o f t h e m e a n f u n c t i o n s c o r
e s o ft h e t w o g r o u p s . F o r t h e d i s c r i m i n a n
t m o d e l , t w o m a i n
m e t h o d s o f v a r ia b l e s e l e c t i o n w e r e u s e
d . F i r s t , a l l t h ef i n al p r e d i c t o r v a r i a b l
e s w e r e i n c l u d e d i n t h e m o d e l .F u r t h e r , a
s t e p - w i s e p r o c e d u r e w a s a l s o c o m p u t e d t
od e t e r m i n e w h e t h e r s o m e v a r i ab l e s w e r e m
o r e i m p o r t a n ti n d i f f e r e n t i a t in g b e t w e e
n t h e t w o g r o u p s . T h e e f f ic i e n cyo f t h e d i s
c r i m i n a n t m o d e l w a s a s s e s s e d b y e x a m i n i
n g t h ee i g e n v a l u e s ( r a t i o o f t h e b e t w e e n
- g r o u p s v a r i a b i li t y t ow i t h i n - g r o u p s s u
m s o f s q u a r e s ) 36 a n d t h e c a n o n i c a l c o r -r e
l a t i o n ( d e g r e e o f a s s o c i a t io n b e t w e e n t
h e d i s c r i m i n a n ts c o r e s a n d t h e g r o u p s ) ?
6 A l a r g e v a l u e o f b o t h i s a ss o -c i a t e d w i th
a g o o d d i s c r i m i n a n t fu n c t i o n . A l l c o m p u
t a -t i o n s w e r e p e r f o r m e d w i t h t h e S t a t i s
t ic a l P a c k a g e ( S P S SI n c . , C h i c a g o , I l l. )
f o r t h e S o c i a l S c i e n c e s ( S P S S - P C + f o rw i
n d o w s ) .
R E S U LT S
T h e d e m o g r a p h i c a n d a n t h r o p o m e t r i c d
a t a fo rt h e s u b j e c t s i n v o lv e d in t h e s t u d y a
r e p r e s e n t e d i n
T a b l e s I I a n d I I I . A s e x p e c t e d , t h e b o d
y m a s s i n d e x( B M I ) o f t h e s u b j e c t s w i t h O S
A S w a s s i g n i fi c a nt lyg r e a t e r t h a n t h e c o n t
r o l g r o u p ( p _ 0 . 0 0 1 ). P o l y -s o m n o g r a p h i c
m o n i t o r i n g o f t h e O S A S g r o u p d e m -o n s t r a
t e d m o d e r a t e t o s e ve r e a p n e a ( m e a n R D I =5 2
.9 2 _+ 2 7 .5 9 ) . T h e c o n t r o l s w h o u n d e r w e n t
p o l y -s o m n o g r a p h i c m o n i t o r in g h a d a m e a n
R D I o f5 .1 _+ 3 . 9 2 t h a t r e p r e s e n t e d a p n e i c
a c t i v i t y w i t h i nt h e n o r m a l r a n g e .
C o m p a r i s o n o f t h e 2 2 c e p h a l o m e t r ic a n a
t o m i cv a r i a b l e s a r e p r e s e n t e d i n T a b l e I
V. S i g n i fi c a n td i f f e r e n c e b e t w e e n g r o u p
s w a s n o t e d f o r h y o i d
b o n e p o s i t i o n re l a t iv e to t h e m a n d i b u l a
r p l a n e( H - M E p -< 0 .0 0 1 ). S u b j e c t s w i t h O
S A S a l s o h a dm o r e o b t u s e c r a n i o c e rv i c a l a
n g l e s ( < C 2 C 4 - S N ,p _< 0 . 00 2 ) t h a n t h e s
n o r e r s . A l t h o u g h m a n y c e p h a -l o m e t r i c v
a r i a b l e s , p a r t i c u l a r l y s o f t t i s s u e m e a
s u r e -m e n t s , s h o w e d s o m e t r e n d s t o w a r d d
i f f e r e n c e b e -t w e e n t h e O S A S a n d s n o r i n g
g r o u p s , t h e d i f fe r -e n c e s w e r e s t a t i s ti c
a l l y s i g n i fi c a n t o n l y fo r t h e h y o i db o n e p
o s i t i o n a n d c r a n i o c e r v ic a l a ng l e .
L i n e a r c o r r e l a t i o n c o m p u t e d f o r ex a m i
n i n g t h ei n t e r r e l a t i o n s h i p s a m o n g t h e 2
2 a n a t o m i c m e a s u r e -m e n t s i n d i c a t e d t h a
t t h e r e w a s s o m e l e v el o f r e d u n -d a n c y i n u s
i n g a l l o f t h e s e v a r i a b l e s i n t h e d i s c r i m
i -
-
8/3/2019 Cephalometric Assessment in OSA
5/10
4 1 4 Pr ac ha rk ta m et aL American Journal of Orthodontics
and Dentofacial OrthopedicsApril1996
T a b l e II. Demographic and anthropometric data of the study
population
Var~b/es
Snore
Mean I SD
O S A S
M e a n S D p Value
Male: Femal e 25:5 24:4Age 49.60 14.29 47.36 12.86 0.533BMI
(kg/m 2) 31.81 4.91 42.34 13.49 0.000"**CI/FI 0.84 0.08 0.84 0.07
0.797Head position a 3.85 5.15 4.98 4.56 0.380RDI 5.10" 3.92
52.92"* 27.59 -
*For 17 subjects; **for 26 subjects; ***p -< 0.002."Head
position relative to the extracranial horizontal line, recorded
from a fluid level device.
T a b l e III. Percentage distribution of the head forms and
facial forms
GroupsBrachycephalic
(>_81.o)
H ead fo rms Fac ia l f o rms
Mesocephalic Dolichocephalic(76-80. 9) ( 90.0)
Sno rer (%) 20 63.3 16.7 - 13.3 86.7OSAS (%) 46.2 42.9 10.7 3.6
7.1 89.3
nant model. Accordingly, the 22 anatomic variableswere redu ced
to 13 predictor variables that were inaccordance with previously
published results. Thediscriminant function included 13
cephalometric
( < BaSN, < C2C4-SN, A-PNS, H-M R InMxLth,MCF, P-PNS,
Phw-Psp, PNS-Ba, RAM/MCF,T/InMx, T-area, T-l) and 4 anthropometric
(age,BMI, CI/FI, head post) variables in the first model.The CIS
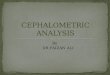
computed from this model was 0.03505(Table V). On the basis of this
score, the model wasable to correct ly classify 23 of the 28 OSAS
subjects(82.1%) and 26 of the 30 snoring subjects (86.7%)(Table VI
and Fig. 5).
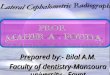
For the step-wise procedure, the first variablethat entered the
model was H-MP. At subsequentsteps, BMI and the soft palate length
(P-PNS) were
selected in the model. These three variables alonewere
successful in classifying 19 of the 28 (67.9%)OSAS subjects and 25
of the 30 (83.3%) snoringsubjects (Table VI and Fig. 6).
In addition, findings from the present studyindicated that
approximately 39% (canonical cor-relati on in the stepwise
procedure r = 0.63, f =0.39) o f total variance of the discriminant
score wasattributabl e to between-group variability.
However,approximately 52% (canonical correlation, r =0.72, r ~ =
0.52) of tota l va riance of discriminantscore was attributable to
differences between thegroups when all anthropometric and
cephalometric
predictor variables were included in the model.There fore
inclusion of anthropometr ic and soft andhard craniofacial
cephalomet ric variables improvedthe discriminant function to a
considerable extent.
D I S C U S S I O N
In an attempt to test the validity of usingcephalometric
radiographs to identify patients atrisk for OSAS, an index was
first constructed fromanthropometric and cephalometric variables.
Dis-criminant analysis was used to predict group mem-bership for
new cases. The step-wise variable selec-tion model examines each
variable and selectsthose with the highest predictive value.
Variableselection terminates when there are no more vari-ables that
meet the selection criteria. The limita-
tion of this method is that variables with lowindividual
discriminant power may be ignored eventhough they may have high
discriminant powerwhen considered as part of a group. Because of
thislimitation, the present study examined another op-tion for
selecting variables for the index. The othermethod forces all the
predictor variables into themodel. When the step-wise method was
used, onlythree variables met the selection criteria.
Thesevariables reflected, or were related to, the softtissues
(H-MP, BMI, and P-PNS). With this model,67.9% in the OSAS group and
83.3% in the snorersgroup were correctly classified. However, the
clas-
-
8/3/2019 Cephalometric Assessment in OSA
6/10
American Journal o f Orthodontics and Dentofacial Orthopedics Pr
ach ar k t am e t a l. 415Volume 109,No. 4
==
LL
6
iD i s c r i m i n a n t S c o r e s
OSAS SNORERS
Fig. 5. All-groups stacked histogram: su mma ry of
classification by including all pred ictor variables.
4"
3 '
2 '
1'
0
l,,,i lil,liscriminant ScoresI~10SAS
SNO~
Fig. 6. All-groups stacked histogram: summary of classification
by step-wise method.
sification rate increased when we forced all thepredictor
variables into the equation, with 82.1%correctly classified in the
OSAS group and 86.7%in the snoring group. Further, the effectivene
ss ofthis model was proved with a higher eigenvalue andcanonical
correlation.
Some studies have suggested that there may besubgroups of
patients with OSAS based on inter-related anatomic and functional
factors. Partinenet al. 21 used eepha logra phy to study th e rela
tion-ship between abnormal upper airway anatomy andbody mass in 157
OSAS patients. They found whenthe BMI is low, the severity of
airway collapse, asassessed by the RDI, appears associated with
ab-normal craniofacial cephalometric findings. Theyhave further
stated that when BMI increases, par-ticularly in obese patients
with a BMI greater than30, the RDI appears to be less dependent on
thecephalometric results. Further support for the hy-
pothesis that patients with OSAS may belong to atleast two
subgroups, based on the origin of thedisease, can be fou nd in the
repo rt of Tsuchiya andcoworkers. = They proposed th e existence of
OSASsubtypes based on the degree of obesity, the sever-ity of OSAS,
and craniofacial and demographic
data. With cluster analysis the patients with OSASwere
subdivided into two groups. One group had ahigh apnea index (AI)
and low BMI, and the othergroup had low AI and high BMI. Each
subgroupwas, then, evaluated with craniofacial and demo-graphic
data by means of multiple regression anal-ysis. In the first group,
a high AI was related to alarge skeletal anteroposterior
discrepancy, a steepmandibular plane, and an inferoanterior
position ofthe hyoid bone. In contrast, a high AI was associ-ated
with a large tongue and a small upper airwayin the latter group.
They concluded that in patientswith a high AI/low BMI ratio and mod
erat e obesity,
-
8/3/2019 Cephalometric Assessment in OSA
7/10
41 6 P r a c h a r k t a m e t al. American Journal of
Orthodonticsand D entofacial OrthopedicsApril1996
Table IV. Compar ison of means of cephalometr ic var iables
between OSAS and snor ing groups using t tests
Snore (25M, 5F)
M ean SD
OSA S (24M, 4F)
M ean SD p value Reliability (Re
Cranial baseM C F 0 . 0 4< B a S N 1 2 8 .8 6
Maxilla< S N A 8 1 .7 5< A r N - P M 5 6 . 8 1A - P N S 5
1 . 4 2P N S - B a 4 7 . 3 3
MandibleR a m / M C F 1 . 7 9< S N B 7 9 . 1 2
A r A - A r B - 0 .1 9Hyoid
H - M P 1 8 . 0 1H v e r 1 2 5 . 5 4
N eck< C 2 C 4 - S N 1 0 7 .3 9< C 2 - S N 1 0 0 .1 0
H ead postu reF H - H o r 4 . 1 7
Soft tissueP h w - P s p 7 .71P - P N S 4 1 . 0 5To n g u e l e
n g t h 84 .91To n g u e a r e a 4 2 6 9. 95
RatioA n t r M x H t 7 3 . 5 2P o s t r M x H t 4 2 . 4 9
I n M x L t h 84 .41T / I n M x a r e a 0 .8 9
2 .144 .63
- 0 . 3 5 3 . 9 4 0 . 6 3 9 0 . 9 8 81 2 8 . 7 9 6 . 1 8 0 . 9 6
3 0 . 9 8 8
3 . 5 1 8 1 . 2 0 4 . 6 5 0 . 6 1 03 .47 56 .46 5 .01 0 .7604 .
0 6 5 1 . 6 2 4 . 8 4 0 . 8 6 53 . 7 3 4 6 . 6 6 3 . 9 2 0 . 5 0
4
3 .34 2 .80 4 .31 0 .3233 . 9 4 7 8 . 1 0 4 . 5 4 0 . 3 6 34 .66
0 .45 3 .93 0 .576
6 . 0 5 2 4 . 9 4 6 . 4 3 0 . 0 0 0 " * *9 .64 132 .23 9 .46 0
.010
7 . 9 3 11 4 . 3 9 8 . 3 6 0 . 0 0 2 * * *7 .63 105 .81 9 .78 0
.016
4 . 2 4 5 . 3 6 4 . 6 4 0 . 3 1 0
3 . 5 2 6 . 2 8 2 . 5 0 0 . 0 8 34 .70 44 .93 6 .77 0 .0137 . 4
7 9 0 . 5 4 6 . 7 5 0 . 0 0 4
4 5 6 . 0 6 4 6 2 9 . 0 2 4 9 4 . 2 3 0 . 0 0 6
6 . 3 0 7 3 . 3 8 5 . 0 2 0 . 9 3 16 .79 46 .36 7 .59 0 .045
5 . 6 9 8 1 . 1 4 7 . 0 8 0 . 0 5 70 .10 0 .96 0 .09 0 .008
0 . 9 8 9
0 . 9 6 7
0 . 9 9 2
0 . 9 6 0
0 . 9 8 5
0 . 9 7 60 . 9 9 2
0 . 9 4 3
***p -< 0 .002 .
Ta b l e V. Discr iminant funct ions evaluated atg roup
means
M eth o d 1 M eth o d2(All predictor va ria bl es )
(Step-wise)
G r o u p 1 - 0 .981 4 - 0 .7622G r o u p 2 1 . 0 5 1 5 0 . 8 1
6 6
C I S 0 . 0 3 5 0 5 0 . 0 2 7 2
skeletal abnormal i t ies may be more imp or tant e t io-logic
factors. In contrast , atypical soft t issue struc-tures (a large
tongue and/or sof t palate possiblyrelated to obesi ty) may resul t
in a smal l upperai rway in pat ients wi th a low AI and high
BMI.These f indings may indicate that our CIS may bemore effect ive
in ident i fying OSAS sufferers whohave low BMI because
craniofacial anatomy maybe a more impor tant predisposing factor in
th is
subgroup. We have elected to include both BMIand age in the CIS
to a l low the index to begeneral ized to a larger populat ion.
W ith the step-wise procedure, the present s tudyfound tha t hyo
id bone pos i t ion (H-MP) was themost important predictor variable
in the discrimi-
nant funct ion. Other authors have also repor ted asimi lar re
la t ionship between hyoid bone posi t ionand apnea severity.
1~'14"21-22However, the posi t ion ofthe hyoid bone is subject to a
h igh degree ofvar ia t ion because of physiologic adaptat ion
andchanges of the head posi t ion. 37 Recen t ly pub l ishedrepor
ts suppor t the conten t ion that low hyoid boneposi t ion is a
compensory response to a i rway ob-st ruct ion and not a
predisposing f a c t o r. 3 s '3 9
Solo w and associates 39 assessed the effect ofai rway obst ruct
ion on the posture of the head andthe cervical column in pat ients
wi th OSAS. Cepha-lom etric radiographs of the subjects wer e
obtained
-
8/3/2019 Cephalometric Assessment in OSA
8/10
Am erican Journal of Orthodontics and Dentofacia l Orthopedics
Pracharktam et aL 4 1 7Volume109,No. 4
T a b l e VI. Cla ss i fi ca tion re su l t s o f bo th m e tho
ds o f va r iab le se lec t ion (a l l p red ic to r va r iab le s
an dS t e p - w i s e m e t h o d )
A c t u a l g r o u p N u m b e r o f c a s esPe r c e n t c o r
r e c t ly c l a s s i f i e d Pe r c e n t c o r r e c t ly c l a
s s i f i e d
A l l p r e d i c t o r ( 1 , 2 ) S t e p w i s e ( 1 , 2 )
Snor i ng 30 26 ( 86 .7% ) 25 ( 83 .3% )OSA S 28 23 ( 82 .1% )
19 ( 67 .9% )Eige nva lue 1 1 .0687 0 .6446Ca non i c a l c o r r e
l a t i on2 0.7188 0.6261
i n n a t u r a l h e a d p o s t u r e . T h e y f o u n d t h
a t t h e p a -t i e n t s w i t h O S A S s h o w e d m a r k e d
l y l a rg e r c r a n i o -c e rv i c al a n g u l a ti o n ( <
C 2 - S N ) t h a n r e f e r e n c e d a t af o u n d i n t h e ir
p r e v i o u s s t u d y o f n o r m a l h e a l t h yadults . In
teres t ingly, they d id not f ind a s ignif icant
d i f f e r e n c e i n t h e c r a n i o v e r t i c a l p o s
t u r e ( S N - Tr u eVe r t ic a l ). T h u s , t h e y p o s t u
l a t e d t h a t t h e s e c h a n g e smigh t be phys io log ic
adap ta t ions to ma in ta in anadequa te a i rway. In con t ra s t
, the head , and thusthe v isual ax is , was main ta ined in i ts
or ig ina l or i -en ta t ion in r e la t ion to the t rue ve r t i
ca l .
Con s i s ten t wi th the se f ind ings , sub jec t s wi thOSAS
in the p re sen t s tudy showed s ign i f ican t lym o r e e x t e
n d e d c r a n i o c er v i ca l a n g u l a ti o n ( < C 2 C 4
-S N ) a n d a t e n d e n c y t o w a r d d i f f e r e n c e s i
n c r a n i o -ce rv ica l angu la t ion (
-
8/3/2019 Cephalometric Assessment in OSA
9/10
4 1 8 P ra ch ar kt am et al. American Journal of Orthodontics
and Dentofacial OrthopedicsApril 1996
of phys io log ic com pen sa t ion s to cl in ica l d i sease .
Ont h e o t h e r h a n d , c r a n i o fa c i a l a n a t o m y m
a y b e a n u n -der ly ing f ac to r tha t con t r ibu tes to the
deve lopmento f c l in ica l i l l ness . C epha lom et ry i s a
wide ly ava i l ab le
a n d i n e x p e n s i v e t e s t. Va l u a b l e i n f o r m
a t i o n h a s b e e nd e r i v ed f r o m a n u m b e r o f s t u
d ie s c o n c e r n i n g c e p h a -lomet r i c assessment in
snore r s and pa t i en t s wi thOS AS. How ever, i t is e ssen t i
a l t o c r i ti ca lly eva lua tethe va l id i ty o f ceph a lom
et ry in iden t i fy ing sub jec t s a tr i sk fo r deve lop ing
obs t ruc t ive s l eep apnea . Givent h e l i m i ta t i o n s o f
t h e c e p h a l o m e t r i c t e c h n i q u e a n dt h e p o l
y g e n e t i c b a s i s f or O S A S , i n o u r o p i n io n , t
h eb e s t u s e o f c e p h a l o m e t r i c s w o u l d b e t o
h e l p d e l i n-e a t e t h e s u b g r o u p s o f O S A S a n d
t o i d e n t if y c li n ic a lcharac te r is t ic s tha t m ay
cor r e l a t e wi th these c r an io -facial character is t ics .
Const ruct ing the CIS is the
f ir st s t ep in t e s t ing the u t i li t y o f us ing cep ha
lom et r i csas a d i agnos t i c t e s t f o r OSAS and a l a rger
s tudy i sp lanned to t e s t t he va l id i ty o f t he index in
the gen-e ra l popu la t ion .
C O N C L U S I O N S
These resul ts indicate that a CIS const ructedfrom cephalometr
ic and anthropometr ic measure-ments can b e used to di fferent ia
te habitual snorerswi th and wi thout apneas. In addi t ion, the f
indingssuggest that the CIS co uld have significant value as
adecision m aking tool for c l in icians t reat ing pat ients
wi th obst ruct ive sleep apnea syndrome and/or ha-bitual
snoring. Further studies are planned to deter-mine the feasibi l i
ty of using the index to help thecl in ician choose t reatment in
tervent ions that havethe highest l ikel ihood o f success.
REFERENCES
1. Y oung T, Pal ta M, Dem psey J , Skatrud J , Web er S, Badr
S.The occurrence of sleep-disordered brea thing among mid-dle aged
adults. N E ngl J Med 1993;328:1230-5.
2. St rohl KP, Sul livan CE, Sau nders NA. Sleep apne a
syn-dromes. In: Saun ders NA, Sul l ivan CE, eds. Sleep
andbreathing. Vol. 21. New York: Marcel, Dekker, Inc.,
1984:365-402.
3. Sul l ivan CE, Issa FG, Saund ers NA, B erthon-Jones
M.Pathophysiology of sleep apnea . In: Saunde rs NA, Sul l ivanCE,
eds. Sleep and breathing. Vol. 21. New York: Marcel,Dekker, Inc.,
1984:299-363.
4. DeBerry-Borowiecki B, Pollak CP, W eitzm an ED, R akoff
S,Impera to J . Fibro-opt ic study of pharyngeal a i rway
duringsleep in pa t ients wi th hypersom nia obst ruct ive sleep a
pneasyndrome. Laryngoscope 1978;88:1310-3.
5. S ura t t PM, D ee P, Atkinso n RL, Arm strong P, Wilhoi t
SC.Fluoroscopic and computed tomographic fea tures of thepharyngeal
a i rway in obst ruct ive sleep apnea . Am RevRespir Dis
1983;127:487-92.
6. Rivlin J, Ho ffstein V, Kalbfleisch J, McN icholas W, Zam el
N,
Bryan AC. U ppe r a i rway morphology in pa t ients wi th
idio-
pathic obst ruct ive sleep apnea . Am Rev Respir Dis
1984;129:355-60.
7. Haponik EF, Smith PL, Bohlman ME, Al len RP, GoldmanSM,
Bleecker ER. Com puter ized tomography in obst ruct ivesleep apnea:
correlation of airway size with physiology
during sleep and wakefulness. Am Rev Resp ir Dis
1983;127:221-6.
8. Ryan CF, Lowe AA, Li D, Flee tham JA. Three-dim ensionalupper
a i rway computed tomography in obst ruct ive sleepapnea . A m Rev
R espir D is 1991;144:428-32.
9. Hoffman EA , G efter WB. Mul t imo dal i ty imaging of
theupper airway: MRI, MR spectroscopy, and ultrasfast CT.Prog Clin
Biol Res 1990;345:291-301.
10. Baco n WH, T urlot JC, Krieger J, St ier le JL. C ephalometr
icevaluat ion of pharyngeal ob st ructive factors in p a t ients wi
thsleep apnea s syndrom e. Angle O rthod 1989;60:115-21.
11. An dersson L, B ra t tst rom V. C ephalometr ic analysis of
per-man ent ly snoring pat ients wi th and w i thout obst
ructivesleep apnea syndrome. Int J Oral Maxillofac Surg
1991;20:159-62.
12. Strelzow VV, Blanks RHI, Basie A, Strelzow AE.
Cephalo-metric airway analysis in obstructive sleep apnea
syndrome.Laryngoscope 1988;98:1149-58.
13. Jamieso n A, Gu i l leminau l t C, Par t inen P, Quera-Salva
MA.Obstruct ive sleep apneic pa t ients have
cranio-mandibularabnormalit ies. Sleep 1986;9:469-77.
14. DeBerry-Borowiecki B, Kuk wa A, Blank s RH I. Ceph alo-metr
ic analysis for diagnosis and t rea tment of obst ruct ivesleep
apnea. Laryngoscope 1988;98:226-34.
15. Lyberg T, Krogstad O, Djupeslan d G. Cep halometr ic anal
-ysis in pa t ients wi th ob st ruct ive sleep ap noea syndrome: 1
,skeletal morphology. J Laryn gol Otol 1989;103:287-92.
16. Rivlin J, Hoffstein V, Kalbfieisch .1, McN icholas W, Zam el
N,Bryan AC. U ppe r a i rway m orphology in pa t ients wi th
idio-
pathic obst ruct ive sleep apnea . Am Rev Respir Dis
1984;129:355-60.
17. Ri ley R, Gu i l leminau l t C, Herran J , Powel l N. Ceph
alo-metric analyses and flow-volume loops in obstructive sleepapnea
patients. Sleep 1983;6:303-11.
18. Gui l lem inaul t C, Ri ley R, Powell N. Obst ruct ive
sleepapnea and abnorma l cepha lome t r i c measurement s . Ches
t1984;86:793-4.
19. Djupesland G, Lyberg T, Krogstad O. Cephalometr ic anal
-ysis and surgica l t rea tm ent o f pa t ients wi th obst ruct ive
sleepapn ea syndrom e. Ac ta Otolaryn gol (Stockh)
1987;103:551-7.
20. Pae EK . A com parat ive study of the re la t ionship
betweensize, tongue activity, and body position. (Thesis.) Van couv
er:Universi ty of Bri t i sh Columb ia , 1989.
21. Par t inen M, G uiUem inaul t C, Quera-Salva MA, JamiesonA.
Obst ruct ive sleep apnea and cephalometr ic roentgeno-grams: th e
role o f anatomic uppe r a i rway abnormal i t ies inthe def ini t
ion of abn orma l brea thing during sleep.
Chest1988;93:1199-205.
22. Tsuchiya M, Lowe AA, Pae EK, F lee tham JA. O bst ruct
ivesleep apnea subtypes by cluster analysis. AM J ORTHODDENTOFAC
ORTHO P 1992;101:533-42.
23. Lyberg T, Krogstad O, Djupesland G. Cephalometr ic anal
-ysis in pa t ients wi th obst ruct ive sleep apn oea syndrome: 2
.Soft t issue morphology. J Laryngol Otol 1989;103:293-7.
24. Lowe AA, Santamaria JD, Flee tham JA, Pr ice C. Facia
lmorphology and obst ruct ive sleep apnea . AM J ORTHODDENTOFAC
ORTHO P 1986;90:484-91.
25. Linder-A ronson S. Adenoids: the i r e ffect on mod e of
brea thing and nasa l a i r f low and the i r re la t ionship to
char-
-
8/3/2019 Cephalometric Assessment in OSA
10/10
American Journal of Orthodontics and Dentofacial Orthopedics P
ra ch ar kt am et al .41 9Volume109,No. 4
acter is t ics of the fac ia l ske le ton and the dent i t ion.
ActaOtolaryngol (Suppl) 1970;265:1-132.
26 . Ada m id i s IP, Spyropou la s M N. T he e ffe c ts o f
lympha de no idhype r t rophy on the pos i t ion o f the tongue , t
he ma nd ib le ,and the h yoid bone . Eur J Orth od
1983;5:287-94.
27 . B re s o l in D , Sha p i ro PA, Sha p i ro GG, C ha pko M
K, D a s s e lS. Mouth brea thing in chi ldren: i t s re la t
ionship to dentofa-c ia l morpho logy. A M J ORTHOD
1983;83:334-40.
28 . C he ng M C , En low DH , Pa ps ide ro M , B roa dbe n t B
H, Oye nO, Sa ba t M . De ve lop me n t e ffec t s o f impa i re d
b re a th ing inthe face o f the grow ing chi ld . Angle O rthod
1988;58:309-20.
29. Harvold EP, Chier ic i G, Vargerwik K. Experiments on
thedevelopment of denta l malocclus ions . AM J ORTHOD
1972;61:38-44.
30 . Wa ts on R M , Wa rre n DW, F i s c he r ND. Na s a l r e s
i s t a nc e ,ske le ta l c lass i f ica t ion and mouth brea thing
in or thodont icpatients. AM J ORTHOD 1968;54:367-79.
31 . Vig PS , Sa rve r DM , Ha l l DJ , Wa r re n DW. Qua n t i
t a t iveevalua t ion of nasa l a i rf low in re la t ion to fac ia
l morphology.AM J ORT HOD 1981;79:263-72.
32 . M on ta gu M F. M e thods o f me a s u re m e n t . In : A
ha ndbook o fanthropo metry. Chicago, I l l inois : Charles C Thom
as 1960:15-19, 49-53.
33 . P ra c ha rk ta m N, Ha ns M G, S t roh l KP, R e d l ine S
. Upr igh ta nd s up ine c e pha lome t r i c e va lua t ion o f
Obs t ruc t ive S le e pApn e a Syn drome a nd s no r ing Sub jec t
s . Ang le Or thod 1994 ;64:63-74.
34 . Vig PS , C ohe n A M . T he s i z e o f the tongue a nd the
in t e r-maxi l la ry space . Angle O rthod 1974;44:25-8.
35 . En low DH, Kuroda T, Le wis AB . The morpho log ic a l a
ndmorphoge ne t i c ba s i s fo r c ra n io fa c ia l fo rm a nd pa
t t e rn .Angle Orthod 1971;41:161-88.
36. Lach enbruc h PA. Discrim inant analys is . New York: Ha
fnerPress, 1975:1-23.
37. H el ls ing E. Changes in the pharynge al a i rway in re la
t ion toextens ion of the head. E ur J Ortho d 1989;11:359-65.38 .
Da v ie s R IO, S t ra d l ing J R . The re l a t ions h ip be twe
e n ne c k
circum ference , radiographic pharyngeal ana tomy, and theobs
truc t ive s leep apnoea syndrome. Eur Respir J 1990;3:509-14.
39. Solow B, Ove sen J , W urtze n P, Nie lsenm , Wildschiodtz
G.C ra n io -c e rv ic a l pos tu re in Obs t ruc t ive S le e p
Apne a . (Ab-s t rac t) J Dent Res 1991;70:607.
40 . Tourne LPM . Growth o f the pha rynx a nd i t s phys io log
icimplica t ions . A M J ORTHOD DENTOFAC ORTHOP 1991;99:129-39.
41 . B e nc h B W . Grow th o f the c e rv ic a l ve r t e b ra
e a s re l a te d totongue , face and dentu re b ehavior. AM J
ORTHOD 1963;49:183-214.
42. Coh en AM , Vig PS. A ser ia l growth s tudy of the tongue
andintermaxi l la ry space . Angle Orth od 1976;46:332-7.
Re prin t requests to:Dr. M a rk G . Ha nsDe pa r tme n t o f Or
thodon t i c s , Sc hoo l o f De n t i s t ryC a s e We s te rn R e
s e rve Un ive rs i tyCleveland, OH 44106-4905