Embed Size (px)
DESCRIPTION
Central sleep apnoea (CSA) encompasses a diverse group ofconditions from periodic breathing at altitude to opiateinducedCSA.
Citation preview

Chapter 22
Central sleep apnoeaD.G. McSharry*,#, D.J. Eckert# and A. Malhotra#
SummaryCentral sleep apnoea (CSA) encompasses a diverse group ofconditions from periodic breathing at altitude to opiate-induced CSA. Considerable overlap exists between obstructivesleep apnoea and CSA in terms of pathogenesis andpathophysiology. CSA syndromes can be broadly classifiedinto patients with high drive and those with low drive. Manyforms of CSA can ultimately lead to adverse cardiovascularoutcomes. Treatment can be challenging and varies accordingto the underlying aetiology of the CSA. Some exciting newtherapeutic options (e.g. phasic administration of CO2)require further research, in particular with respect to safetyand potential outcome benefits.
Keywords: Airway, apnoea, control of breathing, lung, sleep-disordered breathing
*St. Vincent’s University Hospital,Elm Park, Dublin, Ireland, and#Brigham and Women’s Hospital andHarvard Medical School, Division ofSleep Medicine, Sleep DisordersProgram, Boston, MA, USA.
Correspondence: D.G. McSharry,Brigham and Women’s Hospital andHarvard Medical School, Division ofSleep Medicine, Sleep DisordersProgram, 221 Longwood Ave,Boston, MA 02115, USA,Email [email protected]
Eur Respir Mon 2010. 50, 381–395.Printed in UK – all rights reserved.Copyright ERS 2010.European Respiratory Monograph;ISSN: 1025-448x.DOI: 10.1183/1025448x.00026109
Central sleep apnoea (CSA) is characterised by a lack of respiratory effort during sleep. Theseevents result in insufficient or absent ventilation and compromised gas exchange. CSA is
defined by a lack of respiratory effort during cessation of airflow, in contrast to obstructive sleepapnoea (OSA) in which respiratory effort is maintained despite upper airway compromise duringrespiratory events. Considerable overlap exists between OSA and CSA in terms of pathogenesisand pathophysiology. In addition, the two conditions frequently co-exist in the same individuals.Moreover, CSA and OSA can result in frequent nocturnal awakenings, excessive daytimesomnolence and increased risk of cardiovascular outcomes [1, 2].
There are numerous manifestations of CSA as outlined in table 1. Unstable ventilatory driveduring sleep is a major underlying feature. However, the exact mechanism varies between thedifferent types of CSA. In many sleep apnoea patients, central apnoeas can lead to obstructiverespiratory events and vice versa [3, 4]. Arbitrarily, CSA is considered the primary diagnosis if.50% of apnoeas are scored as central in origin. However, many patients have an overlap, ormixed apnoea syndrome. Even healthy individuals will have periodic breathing (giving rise tocentral apnoeas) if they ascend to sufficient altitude to cause important alveolar hypoxia [5].
CSA: important pathophysiological and general concepts
Control of breathing
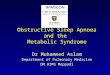
In order to understand the mechanisms by which CSA occurs, an understanding of the control ofbreathing during wakefulness and sleep is vital. Figure 1 illustrates the control of breathing. Centralchemoreceptors in the medulla respond to changes in arterial carbon dioxide tension (Pa,CO2)
38
1D
.G.
MC
SH
AR
RY
ET
AL
.

via shifts in H+ concentration. Peripheral chemoreceptors at the carotid body respond to changes inarterial oxygen tension (Pa,O2) and Pa,CO2. The ventilatory response to changes in Pa,O2 or Pa,CO2
(chemosensitivity) varies between individuals and different disease states. The Pre-Boetzingercomplex (PBC) is thought to be the major central-pattern generator in the brainstem, whichgenerates the respiratory rhythm, although some debate exists regarding the potential role of theretrotrapezoid nucleus (RTN). Afferent signals from Golgi tendon organs and muscle spindles fromthe chest wall and respiratory muscles also contribute to the regulation of ventilation. Duringwakefulness, strong emotional influences can alter the rate and depth of breathing involving limbicforebrain structures. An independent background augmentation of ventilatory drive known as thewakefulness drive to breathe also exists, but is lost at the onset of sleep [7]. Indeed, with thetransition from wakefulness to sleep, there is a withdrawal or downregulation of many of the inputsthat regulate breathing such that the metabolic control of breathing becomes crucially importantduring sleep.
At sleep onset even healthy individuals can demonstrate irregular breathing. Respiratory control isinherently unstable during the transition from wake to sleep [8]. Upper airway resistance increasesthrough a reduction in the tone of the respiratory pump and upper airway dilator muscles. Thus,there is a reduction in ventilation for a given level of drive [9, 10]. Chemosensitivity is probablyreduced at sleep onset [11]. A central apnoea can ensue if the awake-to-sleep transition is quick,with the loss of the wakefulness drive and the delay required to elicit an appropriate compensatoryresponse from the chemoreceptors. Indeed, the chemical apnoea threshold during sleep is typicallyat approximately the waking eucapnic level [12, 13]. This level is 2–6 mmHg below the usualPa,CO2 during stable non-rapid eye movement (NREM) sleep.
During sleep (especially rapid eye movement; REM) there is reduced ventilatory response to hypoxiaand hypercapnia, and reduced respiratory load compensation [14–17]. If sleep is stable, a new CO2
set point is established and the chemoreceptor and respiratory reflex feedback become criticalcomponents regulating ventilation, albeit at a reduced homeostatic level compared to wakefulness.Arousal (brief awakening) from sleep can restore ventilation when other compensatory mechanismsfail but it can sometimes perpetuate apnoeic episodes. The arousal threshold and the ventilatoryresponse to arousal are two key determinants that influence the propensity of an arousal to cause anapnoea. An individual with a low arousal threshold (wake up easily) is susceptible to sleep-state
Table 1 Different manifestations of central sleep apnoea (CSA)
Hypercapnic CSA: impaired central drive - won’t breatheBrainstem pathology, e.g. infarct, tumour or rarities such as prion diseaseCongenital central hypoventilation syndrome (formerly known as Ondine’s curse) defined by
PHOX2B mutationNarcotics: acute and chronic usageObesity hypoventilation syndrome
Hypercapnic CSA: impaired respiratory motor control - can’t breatheCervical cord pathology, e.g. disc diseaseMotor neuron pathology, e.g. amyotrophic lateral sclerosisPost-polio syndromeNeuro-muscular junction pathology, e.g. Myasthenia GravisMyopathies, e.g. acid maltase deficiencyChest wall disease, e.g. Kyphoscoliosis
Nonhypercapnic CSACheyne–Stokes breathingIdiopathic CSAPeriodic breathing: altitude-induced breathing instability
Other CSAMixed CSA and obstructive sleep apnoea
38
2C
EN
TR
AL
SL
EE
PA
PN
OE
A

instability. Obstructive or centralapnoea can result from state instabil-ity depending on the prevailing air-way mechanics. The arousal thresh-old and breathing stability increasewith slow wave sleep [18, 19]. Thisfinding provides the rationale for theuse of hypnotics in a select minorityof non hypercapnic CSA patients [20,21]. Alternatively, slow wave sleepmight be the consequence rather thanthe cause of stable breathing andmore research is required in this area.
The rapid shift to wakefulness froman arousal results in the Pa,CO2
moving rapidly from ,45 mmHgto a lower value. In addition, airwayresistance falls and the wakefulnessdrive reappears and a brisk ventila-tory response occurs; the magni-tude of which is dependent on theextent of the shift between thevarious state-related physiologicalchanges. Moreover, if this indivi-dual promptly falls to sleep again,with a newly reduced Pa,CO2, thechemical apnoea threshold may becrossed resulting in a central orobstructive apnoea [22].
Loop gain
The ventilatory system is controlled by a complex negative-feedback loop. Ultimately, the rate anddepth of ventilation is maintained according to homeostasis. If a ‘‘disturbance’’ occurs to thenormal equilibrium then alveolar ventilation will be altered and the Pa,CO2 will be adjusted by this‘‘corrective action’’. Loop gain is an engineering term used to describe the feedback mechanisms ofa control system. Put simply, when applied to the ventilatory system, loop gain is the ratio of themagnitude of the corrective action (response) to the magnitude of the disturbance (stimulus) [23],i.e. loop gain 5 corrective action/disturbance or ventilatory response.
There are two principal components to loop gain: controller gain and plant gain. Controller gainrefers to the chemoresponsiveness of the system (i.e. hypoxic and hypercapnic ventilatorysensitivity plus responses). Plant gain primarily reflects the efficiency of CO2 excretion (i.e. theability of a given level of ventilation to excrete CO2). Mixing gain is a function of circulatory delay,as well as haemoglobin binding of O2 and CO2. Mixing gain tends to be fairly constant, althoughcirculatory delays may make mixing gain more clinically relevant in patients with congestive heartfailure [24], which is discussed in another chapter [25]. The physical separation of the sensors andeffectors makes the ventilatory feedback control system vulnerable to instability. That is, if thechemoreceptors were located in the pulmonary veins, the oscillatory behaviour seen in periodicbreathing would be unlikely.
For most individuals, breathing is relatively stable, unless periodic breathing is occurring. Forexample, if the ventilatory disturbance were a sigh, such a disturbance would not be self sustaining.A hypopnoea is another example of a disturbance. If the loop gain is high then the system will
Higher brain centres(cerebral cortex: voluntarycontrol over breathing)
+_
+
+
+
+
_
+_
Emotional stimuli actingthrough the limbic system
Peripheralchemoreceptors
CentralchemoreceptorsCO2 , H+
CO2 ,O2 , H+
Pyra
mid
Pons
C C
Receptors inmuscles and joins
Respiratory centres(medulla and pons)
Stretch receptorsin lungs
Receptorsfor touch,temperature, and painstimuli
Figure 1. Schematic diagram showing the control of breathing.Reproduced from [6] with permission from the publisher.
38
3D
.G.
MC
SH
AR
RY
ET
AL
.

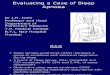
become unstable in response to such a perturbation. That is, if the corrective action wereoverzealous then an abnormal self-sustaining oscillatory system of periodic breathing with apnoeasoccurs. Thus, a high loop gain can increase the propensity for the ventilatory control system todevelop cyclical fluctuations in ventilatory output. A low loop gain, however, indicates a minimalor dampened response to a disturbance and tends to be less inherently unstable from a respiratorycontrol perspective, but if markedly low may result in prolonged hypoventilation. Theproportional assist ventilation (PAV) technique allows measurement of loop gain [26]. Anexample of PAV-induced periodic breathing is shown in figure 2 [27]. For each incremental levelof PAV before periodic breathing occurs, the tidal volume amplification factor (VTAF) ismeasured. Loop gain is measured from the VTAF.
Throughout the course of this chapter we shall return to the concept of loop gain as it relates tothe different forms of CSA.
Manifestations of CSA
CSA can be broadly classified into two groups depending on the wakefulness CO2: hypercapnicand non-hypercapnic. The aetiologies of the different forms of CSA, even within the same class(e.g. hypercapnic), can be quiet different.
Hypercapnic CSA: impaired central drive
Won’t breathe
Brainstem pathology
Traumatic lesions or infarcts of the brainstem can directly diminish ventilatory output which canworsen during sleep resulting in CSA.
Congenital central hypoventilation syndrome
Congenital central hypoventilation syndrome (CCHS; previously known as Ondine’s Curse) resultsfrom a mutation in the PHOX2B gene. CCHS is inherited in an autosomal dominant manner witha stable mutation and affected individuals have diffuse autonomic nervous system dysregulation[28]. CCHS is rare and usually presents in the neonatal period but can present in infancy,childhood, adolescence and even rare cases in adulthood have been reported [29]. Characteristicprofound alveolar hypoventilation during wakefulness and sleep can result in severe hypoxaemiaand hypercapnia [30]. Recognised complications are secondary polycythaemia, pulmonaryhypertension and right heart failure. Hypoventilation during sleep results from reduced tidalvolume but the respiratory rate is near normal [31]. Ventilation is more stable during REM sleepthan NREM sleep in contrast to OSA [32]. Ventilatory responses and sensing of dyspnoea inresponse to hypoxia and hypercapnia and processing of respiratory afferent information, asmeasured by cortical evoked potentials, are diminished in children with CCHS [30, 33]. Themanagement of CCHS is generally supportive (genetic counselling, avoidance of sedatives, etc.) andmay include tracheostomy and mechanical ventilation, diaphragmatic pacing and noninvasiveventilation [30].
Opioid-induced CSA
When used acutely, opioid medications have long been known to cause potent respiratorydepression with accompanying blunting of the hypercapnic and the hypoxic ventilatory responses[34, 35]. The respiratory depression is principally due to a reduction in tidal volume thoughreduced respiratory rate becomes increasingly important with elevated opiate dosage. Under-standably, both acute and chronic opiate usage can cause CSA [36, 37]. At present, there is little in
38
4C
EN
TR
AL
SL
EE
PA
PN
OE
A

the literature about this form ofCSA despite the widespread use ofopioid medication worldwide forcommon medical complaints, suchas back pain, as well as fromnarcotic abuse [38, 39]. However,WANG et al. [37] found 30% ofpatients on a methadone mainte-nance treatment programme (forheroin addiction) to have CSA. Thecycle time of the apnoeas was muchshorter than Cheyne–Stokes breath-ing seen in chronic severe heartfailure; 30 s. The arousal index wassimilar between controls andmethadone patients indicating thatsleep/wake transitional changes areunlikely to be important in theperpetuation of the CSA cycles.There were only minor differencesin Pa,O2 and Pa,CO2 between the methadone and control groups. Methadone blood levels correlatedwith the CSA in only a minority of patients in this study showing that other physiological variableswere also contributing [37]. Thus, the pathophysiology of opiate-induced CSA remains incompletelyunderstood.
The depressant effects of morphine and other m-opiate receptor agonists on breathing probablyrelates to their action on chemosensitive areas in the brainstem and carotid body [34]. Intuitively,it is probable that this central respiratory depressant effect contributes to the central apnoeas. Thecyclical nature of the apnoeas is incompletely understood. Numerous hypotheses exist. MOGRI etal. [40] found that a high proportion of patients on chronic opioid therapy for pain demonstratedimportant nocturnal hypoxaemia. The aetiology of the hypoxaemia varied but central apnoea wasone mechanism. In contrast to studies performed on acute opioid usage, TEICHTAHL et al. [41]showed a heightened hypoxic ventilatory response in a cohort of methadone maintenancetreatment patients. The response was largely mediated by an increase in respiratory rate, unlikeprevious studies. These patients had a blunted hypercapnic ventilatory response. Therefore, wehypothesise that the m-opioid agonist directly depresses respiratory control centrally in thebrainstem triggering a central apnoea. The prevailing low-grade hypoxaemia worsens, pre-cipitating an overzealous peripheral chemoreceptor response which corrects the hypoxia and thenabates. Thus, the Pa,CO2 falls. The blunted central chemoreceptor responds poorly to carbondioxide tension changes and so is vulnerable once again to the depressant effects of the opiate andso the cycle propagates. In addition, the m-opioid receptors have been used by GRAY et al. [42] tolabel the PBC. The PBC is thought to be the major central pattern generator in the brainstemwhich generates the respiratory rhythm. Thus, in theory, narcotics may be reducing output fromthe PBC and yielding cessations in airflow without respiratory effort.
Animal studies [43] have shown that m-opioid agonists acting on the hypoglossal motor nucleushave a depressant effect on the genioglossus muscle (the chief airway dilator) which might underliethe coexistence of OSA with CSA in some chronic opiate users [40]. However, ROBINSON et al. [44]observed no major increase in OSA severity among normal individuals given narcotic therapy.There is a mounting body of evidence to suggest that poor sleep can worsen pain. Theoretically, ifthe patient on opiates has opiate-induced CSA then ironically the resultant sleep disturbance mayincrease the pain and hence the opiate requirement. Treatment specific to opiate-induced CSA isobviously cessation of the opioid agonist though this is often impractical. Some reports of a dose-dependence to narcotic-induced central apnoeas would suggest that a reduction in medication
-2.5250 s
Flow
L. s
-1V
T L
P mas
kcm
H2O
0.02.55.0
-0.50.00.51.01.5
102030
-1000
EEG
µV
100200a)
b)
c)
d)
Figure 2. An example of periodic breathing induced by propor-tional assist ventilation (PAV). V T: tidal volume; Pmask: maskpressure. Arrows from left to right represent increase in PAV andoccurrence of an arousal reducing PAV to 0, respectively.
38
5D
.G.
MC
SH
AR
RY
ET
AL
.
dose may be helpful in alleviating the central apnoeas [45]. Reduced narcotic doses can sometimesbe achieved with local analgesia (e.g. warm compresses for back pain) or using non-narcoticanalgesics (e.g. gabapentin). Some data suggest that newer positive-pressure devices may have arole in stabilising breathing in these patients [46]. Other agents such as acetazolamide andtheophylline have received minimal investigation in this area. Thus, further investigation is clearlyneeded. Moreover, the literature is extremely sparse on the beneficial effects that opioidwithdrawal has on opiate-induced CSA [47].
Obesity hypoventilation syndrome
Obesity hypoventilation syndrome (OHS) is defined as a combination of obesity (body mass index.30 kg?m-2) and arterial hypercapnia (Pa,CO2 .45 mmHg) during wakefulness not explained byother known causes of hypoventilation [48]. Hypoventilation worsens during sleep andhypoxaemia ensues. Patients can present with morning headaches and daytime hypersomnolence.Obesity-related impairment of respiratory mechanics is at least partly responsible for thedevelopment of OHS. These patients are unable to compensate for the worsened respiratorymechanics and ‘‘permissive’’ hypercapnia and other sequelae, including cor pulmonalae, can ensue.However, the factors determining which obese people develop OHS are incompletely understood.The failed compensation may relate to differences in the anatomical distribution of fat combinedwith ventilatory control deficits, such as blunted chemosensitivity [49–51]. The hormone leptinmay be important in obesity-related hypoventilation in some animal models [52].
Whilst the incidence of OHS is likely to increase [53], it is probably underdiagnosed. Indeed, inour experience OHS is often misdiagnosed as congestive cardiac failure probably due to thepresence of cor pulmonalae. In addition, the chest radiograph in OHS can give the impression ofpulmonary congestion owing to the overlying adiposity. Also, the obesity-related restriction canaccentuate pulmonary interstitial markings. In addition, OHS patients often present to theintensive care unit with acute decompensation, with blood gases revealing acute on chronicrespiratory failure. During these acute presentations, hypoxaemia can impair left ventricularrelaxation [54], and elevated right ventricular pressures can raise left ventricular pressures throughdiastolic interdependence [55]. As such, some mild pulmonary oedema may be present in thesepatients at presentation although left ventricular function is relatively normal once the acuteexacerbation has resolved. Management of OHS principally involves the use of bi-levelnoninvasive ventilation. The expiratory pressure may need to be relatively high to treat OSA, acondition which is frequently co-existent. In addition, weight loss is likely to improve sleep-disordered breathing in these patients [48]. Indeed surgical weight loss may be an option formorbidly obese patients with OHS [56].
Hypercapnic CSA: impaired respiratory motor control
Can’t breathe
Hypercapnic patients with CSA and an intact central respiratory output from pattern generatorneurons may have a defect anywhere from the upper motor neurons to the respiratory muscles.This diverse group of conditions are listed in table 1. The aetiology and severity of the CSA relatesto the underlying condition [57].
Nonhypercapnic CSA
Cheyne–Stokes breathing
The renowned Irish physicians, J. Cheyne and W. Stokes, gave their names to this characteristiccrescendo/decrescendo pattern of breathing with a long circulation time and arousal occurring
38
6C
EN
TR
AL
SL
EE
PA
PN
OE
A

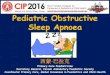
during the hyperpneic phase of respiratory effort. Figure 3 illustrates Cheyne–Stokes breathing(CSB) and evidence of the long circulation time is seen because each oxygen desaturationcorresponds to the previous apnoea. The cycle time of the unstable breathing is consequently long,typically 60–90 s. The most common cause of CSB is congestive cardiac failure (CCF). CSBassociated with CCF and its treatment is comprehensively dealt with later on in this monograph.
Idiopathic CSA
Patients who have central apnoeas during sleep who do not display the typical CSB pattern orsleep transition apnoea and who have normocapnia or hypocapnia during wakefulness fall into thecategory of idiopathic CSA (ICSA). The apnoeas may occur in isolation or in cycles lasting 40 s.Arousals typically occur at the end of apnoeas, which are themselves more common in stage 1 or 2sleep. Patients may present with insomnia or hypersomnolence. The pathophysiology is poorlyunderstood but is thought to relate to elevated hypercapnic ventilatory responses leading tohypocapnia and respiratory control instability [58–60]. Arousal and the ensuing hypocapnia canfurther destabilise breathing [22]. These factors render the patient vulnerable to crossing theapnoea threshold, which may lie perilously close to the sleeping eucapnic Pa,CO2, particularly inthose with daytime hypocapnia. Acetazolamide has been shown to improve sleep-disorderedbreathing in a study involving seven patients with ICSA [61]. Its mechanism of action is discussedlater in this chapter. A recent report suggests that non-benzodiazepine hypnotics may be beneficialin some patients with ICSA [20]. However, randomised, controlled studies are required before thiscan be recommended as a safe and effective treatment approach. In our experience ICSA is quiteuncommon, making definitive studies difficult to accomplish.
Periodic breathing at high altitude
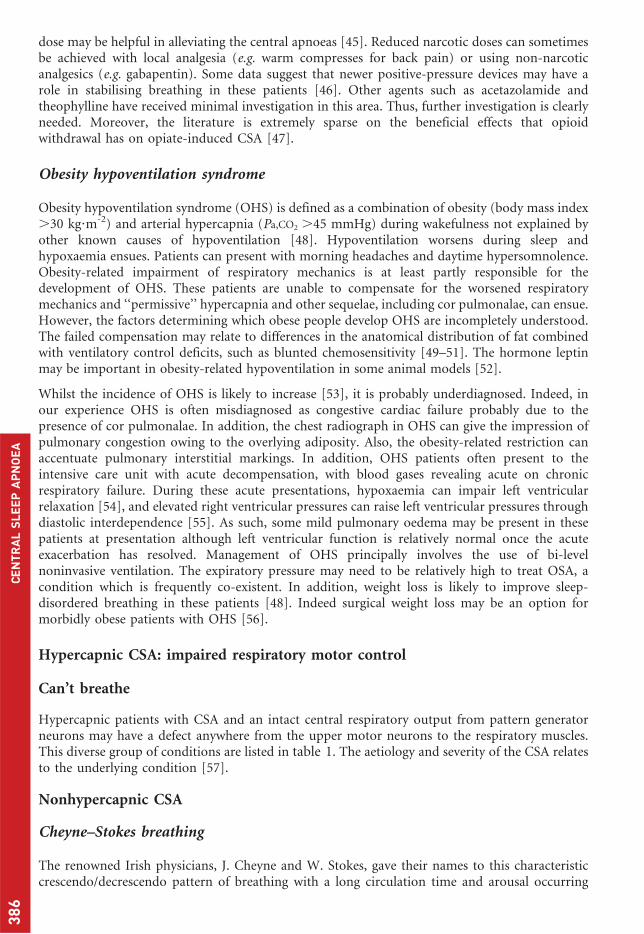
The term periodic breathing (PB), in accordance with the Chicago criteria [62], refers to thecharacteristic cyclical breathing patterns with central apnoeas that occur at high altitude. Thecharacteristics of hypobaric hypoxic PB are well described by BERSSENBRUGGE et al. [63] as follows:1) repetitive breathing oscillations of reproducible cycle length (21.2¡1.8 s); 2) clusters of two tofive breaths of highly variable tidal volume and breath-to-breath ventilation alternating with aprolonged expiratory pause of the last breath of each cluster (apnoea); and 3) apnoeas of centralorigin occupying half the cycle time. PB is best appreciated graphically. Figure 4 shows the cyclicalbreathing pattern [64]. The cycle length (,20 s in this example) shortens as the climber ascends[65]. Disrupted sleep and tiredness can ensue and difficulty sleeping is one of the diagnosticcriteria of acute mountain sickness (AMS) according to the Lake Louise Consensus of 1991.However, periodic breathing occurs as readily at high altitude in those without AMS as in thosewith it [66]. PB occurs in virtually all individuals given sufficient ascent and accompanying hypoxia.However, the altitude at which PBoccurs and the characteristics of thePB pattern vary between individualsbased, in part, on differences inphysiological responsiveness to hy-poxia. LAHIRI et al. [67] comparedventilatory response to hypoxia inHimalayan sherpas to sojourners to5,200 m and the relationship of thisresponse to nocturnal sleep apnoeaand PB. Sojourners with a high ven-tilatory response to hypoxia mani-fested periodic breathing and apnoeaswhile sleeping. In contrast the sherpaswho had a low ventilatory response to
EEGSa,O2
Airflow
Chest
Abdomen
1 min
Figure 3. Cheyne–Stokes breathing in a patient. &%: spontaneousarousals; &%: desaturation; &%: central apnoea. Sa,O2: arterial oxygensaturation. Reproduced from [45] with permission from thepublisher.
38
7D
.G.
MC
SH
AR
RY
ET
AL
.

hypoxia had no sustained apnoeas/PB. However, central apnoeas can occur in highlanders at veryhigh altitudes [68].
The hypobaric hypoxia at altitude results in relative hyperventilation via activation of the peripheralchemoreceptors. The resultant hypocapnia during sleep triggers a central apnoea if Pa,CO2 falls below thechemical apnoea threshold. Thus, respiratory alkalosis ensues. However, what causes the periodicity ismore complex. Using hypobaric hypoxic studies in normal individuals, BERSSENBRUGGE [63] theorisedthat the periodicity resulted from oscillations in Pa,CO2 around a CO2-apnoea threshold whosefunctional expression was critically linked to sleep state. In essence, hypoxia results in increased gain ofthe peripheral chemoreceptors with resultant hyperventilation, which drives the CO2 below the CO2-apnoea threshold and an apnoea ensues. Meanwhile, during the apnoea the hypoxia worsens, furtherincreasing the gain on the peripheral chemoreceptors. Thus, rather than slowly increasing tidal volumetriggered by increasing CO2, a vigorous ventilatory response initiated by the peripheral chemoreceptor’sresponse to hypoxia ensues. Hence, the process is self-sustaining and periodic. Therefore, chemicalcontrol instability, not present when the individual was at sea level, is present at altitude.
Continuous hypoxia increases baseline carotid body activity and sensitises the response to acutehypoxia. The enhanced hypoxic response is due to alterations in ion current densities, changes inneurotransmitter dynamics and recruitment of additional neuromodulators (endothelin-1) inglomus cells [69]. Moreover, hypoxia-induced central depression has been suggested to contribute tothe PB [70]. Sleep fragmentation is common at altitude with resultant fatigue the following day [71].
Arousals can influence the occur-rence of PB. In a simulated high-altitude study, ANHOLM et al. [71]showed that brief arousals increasedfrom 22¡6 arousals?h-1 of sleep atsea level to 161¡66 arousals?h-1 at282 mmHg. A study investigatingthe effects of the hypnotic zolpidemat simulated high altitude found thatarousals occur in synchrony withthe hyperpnoeic phase of PB [72].However, GOLDENBERG et al. [73]found that the intercurrent wakeful-ness duration correlated best withPB and not the number of arousalsper se.
WHITE et al. [5] studied the effects ofacclimatisation at high altitude duringthe first week in seven healthy males.Acclimatisation resulted in augmen-ted hypoxic ventilatory responsive-ness and the slope of the hypercapnicventilatory response increased initi-ally. The sleep-induced decrements inventilation and hypercapnic respon-siveness were equivalent to those atsea level and the quantity of PB wasvariable, occurring more frequently inthose with higher hypoxic and hyper-capnic responsiveness. The authorsalso found that acclimatisation re-duced the latency to PB and that sleepquality improved [73].
6040
Time in 5-s intervals
120e)
HR
bea
ts. m
in-1
80100
6070
100d)
Sp,O
2 % 8090
00.3
1.2c)
AB L
0.60.9
00.3
1.2b)
RC
L
0.60.9
00.3
1.2a)
Sum
vol
L
0.60.9
Figure 4. A nocturnal polygraph recording from a mountaineer at4,559 m. The inductive plethysmographic volume signals of a) thesum volume of the ribcage (RC) and abdomen (AB). b) The RCvolume and c) the AB volume show periodic breathing. Sp,O2:arterial oxygen saturation measured by pulse oximetry; HR: heartrate. Reproduced from [64] with permission from the publisher.
38
8C
EN
TR
AL
SL
EE
PA
PN
OE
A

Medications suggested as putative treatment options for PB/apnoeas include respiratorystimulants (theophylline, medroxyprogesterone acetate, almitrine and acetazolamide) and, somemight say, paradoxically hypnotics. Results have been mixed. Studies have shown that hypnoticshave generally improved sleep quality (measured subjectively in some studies) without affectingoxygen saturations [72, 73]. However, the studies are both small and sparse. In addition, thesubjects were healthy individuals, reducing the risk/impact of respiratory depression. Anotherstudy of temazepam showed a reduction in PB at 5,000 m and no effect on performance the nextday but with a significant reduction of 2% in the arterial oxygen saturation (Sa,O2) [74].Theophylline reduces PB/central apnoeas and seems well tolerated [75, 76]. Medroxyprogesteroneremains unproven at altitude as does almitrine, which might actually increase PB [77].Acetazolamide, a carbonic anhydrase inhibitor, has been shown to reduce PB and increase Sa,O2
during sleep at high altitude [77]. The respiratory stimulant action of acetazolamide at altitudeprobably comes from its induction of a metabolic acidosis rather than from another of its othernumerous pharmacological effects [78], although the precise mechanisms of action remainuncertain.
The hypoxic ventilatory response is key to the development of PB. The original experiments ofBERSSENBRUGGE et al. [63] demonstrated elimination of PB with restoration of normoxia,coincident with a 3–6 Torr increase in Pa,CO2. Unsurprisingly oxygen therapy has been shown toimprove PB and reduce apnoeas at altitude in the few studies addressing this issue [79, 80].
Other CSA
Mixed CSA and OSA
In clinical practice CSA is frequently encountered in patients with predominant OSA. This‘‘complex apnoea’’ syndrome is quite common with .50% of the apnoeas usually beingobstructive. Considerable controversy exists regarding the entity of complex sleep apnoea, inpart because its definition is quite vague. Some literature has suggested that OSA patients whodevelop central apnoeas upon initial continuous positive airway pressure (CPAP) exposureshould be labelled as complex apnoea. These patients were traditionally labelled as having‘‘treatment-emergent central apnoea’’ with spontaneous resolution of central apnoea occurringin the majority of these individuals. Significant pathophysiological similarities exist betweenOSA and CSA and interestingly central apnoeas lead to upper airway closure [3, 4]. SANKRI-TARBICHI et al. [4] have shown that central hypopnoeas lead to pharyngeal narrowing during theexpiratory phase. They concluded that reduced ventilatory drive leads to increased expiratory,but not inspiratory, upper airway resistance [4]. During this study central hypocapnichypopnoeas were induced by noninvasive positive-pressure ventilation. The drive to thegenioglossus (as well as the other respiratory muscles) is reduced during a central apnoea [81],promoting upper airway collapse/obstruction. Like CSA, patients with OSA have unstablerespiratory control [82, 83]. Thus, in patients with complex apnoea different perpetuatingfactors determine which type of apnoea occurs. For example, during REM sleep obstructiveapnoeas will predominate. Generally, OSA worsens during REM sleep probably from reducedupper airway tone and reduced chemosensitivity [16, 84]. In contrast, CSA severity improvesduring REM probably from increased respiratory neuronal activity that occurs in this sleep state[85]. Also, mucosal factors such as the surface tension of the upper airway lining liquid (whichis increased in OSA [86]) may play a role in the type of apnoea that occurs and how quickly theairway reopens.
Treatment emergent CSA occurs in ,10% of patients diagnosed with OSA on the first night ofCPAP treatment [87]. Important risk factors for this phenomenon are cardiac disease and somepre-existing CSA. Although poorly studied, these patients also probably have robustchemosensitivity compared to those without treatment-emergent CSA. The exact mechanisms
38
9D
.G.
MC
SH
AR
RY
ET
AL
.

by which CSA emerges on treatment are poorly understood. Reduced upper airway resistancemight increase CO2 excretion leaving the patient vulnerable to crossing the apnoea threshold[88]. The application of CPAP also may wash out the anatomical dead space, particularly in thesetting of mask leak leading to a fall in Pa,CO2 for a given minute ventilation. Lung stretchreflexes may also be important in inhibiting ventilatory motor output in some patients. Thesecentral apnoeas typically resolve on CPAP and so their clinical significance is uncertain. Indeed,SALLOUM et al. [89] recently showed ventilatory instability in OSA that was reversed after1 month of CPAP. An increasingly used treatment option in these patients is adaptiveservoventilation [90]. In a recent 2-week pilot study, RANDERATH et al. [91] studied the effects ofcombined adaptive servo-ventilation and automatic positive airway pressure on 12 patients with co-existing OSA and CSA syndrome and periodic breathing. Seven of the patients had cardiovasculardisease. Considerable abolition of the apnoeas and improvements in arousals, O2 saturation andsleep profile were noted [91].
Treatment of CSA
CSA has diverse manifestations and aetiologies. Accordingly, the treatment options reflect thisdiversity and vary widely between the different forms of CSA. For example, noninvasive bi-levelventilation can be of benefit in OHS but could cause clinical worsening of some patients withhypocapnic CSB. Throughout the chapter we have discussed the specific treatment options of thevarious manifestations of CSA. The main treatment options for CSA are discussed further in thissection. The treatment of CSB in heart failure is described in more detail elsewhere in thismonograph.
Oxygen
Hypoxia can be sustained in OHS or intermittent in other forms of CSA. Hypoxia can impairrespiratory sensory processing and arousal responses to respiratory stimuli during sleep [92, 93].This implies that hypoxia can worsen CSA syndromes such as OHS, which are characterised bysustained episodes of hypoxia. One case report provides evidence for the use of oxygen in OHS[94]. Oxygen is of benefit in periodic breathing at altitude, which has a much different aetiology[79, 80]. Indeed several forms of nonhypercapnic CSA (with heightened chemosensitivity) canpotentially benefit from the stabilising respiratory control effects of oxygen. Improvements onoxygen therapy have been noted in ICSA and CSB. However, these trials have been short term[95–97]. Larger trials are required to determine which CSA patients may benefit from oxygentherapy.
Carbon dioxide
Increasing the sleeping Pa,CO2 (eucapnic level) further above the apnoeic threshold could have astabilising effect on some forms of CSA, minimising the risks of apnoeas. Recent studies haveshown that mild increases in the inspired concentration of CO2 (by addition of CO2 or byincreasing the dead space via a mask) have beneficial effects on central apnoeas in ICSA [98] andCSB [99]. The improved apnoea/hypopnoea index does not always translate into improved sleepquality [100] and concerns exist regarding CO2-induced sympatho-excitation [101]. A recentstudy using a standard mathematical model suggested that dynamic administration of CO2,adjusting the dose and duration in real time, could treat periodic breathing/CSA efficiently withmuch lesser doses than continuous administration [102]. If such a model was developed clinicallyit could lessen the acidosis and sympatho-excitation associated with CO2 administration. Thestudies so far have had small numbers and larger, longer studies are needed to determine theefficacy and safety of CO2 administration.
39
0C
EN
TR
AL
SL
EE
PA
PN
OE
A

Noninvasive ventilation
CPAP has shown benefit in patientswith ICSA possibly from stoppingthe inhibitory reflex mechanismsthat arise during airway closureand increasing lung volumes andoxygen stores [103]. One could alsospeculate that in some cases theincrease in physiological dead spacefrom CPAP might be mildly in-creasing the CO2 further above theapnoeic threshold. CPAP has beenshown to improve sleep-disorderedbreathing and haemodynamics inheart failure patients [104]. Thelargest study on the effects of CPAPon CSA did not show improvedmortality and only showed a mildimprovement in apnoea/hypopnoeaindex [105]. Limited data supportthe role of increased inspired CO2 asan adjunct to CPAP in the treatmentof mixed obstructive and centralapnoeas [106]. Larger trials on CO2
administration are needed before itcan be recommended given thedanger of sympatho-excitation and other deleterious effects. Bilevel noninvasive ventilation canimprove some forms of CSA (e.g. OHS [107]) but can worsen others by inducing hypocapnia[108]. The newer adaptive pressure support servo-ventilation can improve CSA in certain cases(e.g. CSB in heart failure [109]), although outcome data remain sparse precluding definitiverecommendations.
Respiratory stimulants
The carbonic anhydrase inhibitor, acetazolamide, improves CSA in heart failure [110] and ICSA[61]. It induces a metabolic acidosis and its benefit in CSA probably relates to shifting thehypercapnic ventilatory response and lowering the apnoeic threshold [61, 111]. Acetazolamide hasbeen shown to improve periodic breathing at high altitude [77]. Long-term, larger trials arerequired before acetazolamide can be safely recommended. Theophylline and progesterone haveshown benefit in some types of CSA. However, theophylline has been associated with possiblearrhythmias [112] and long-term safety data are not available for progesterone.
Conclusion
We have reviewed that CSA encompasses a diverse group of conditions from periodic breathing ataltitude to opiate-induced CSA. The pathogenesis of CSA is summarised in figure 5. This diversityis reflected in the differing pathogenesis and treatment options. Indeed, a certain treatment whichimproves one form of CSA may have deleterious effects on another (e.g. bilevel noninvasiveventilation). However, all forms of CSA can ultimately lead to adverse cardiovascular outcomes.Some exciting new therapeutic options (e.g. phasic administration of CO2) require furtherresearch, in particular with respect to safety.
"Can't breathe" factors i.e. respiratory motor output
Inhibitoryreflexes
Chemosensitivity
Obstructiveapnoea/
hypopnoea
Drive
Centralapnoea/
hypopnoea
Hypocapnia
Hypercapnia
Metabolic production
Chemosensitivity
ArousalArousal threshold
Ventilatory responseto arousal
UA anatomyHyperventilation
Loss of wakefulnessstimulus
Change between eupnoeaCO2 and apnoea threshold
Loss of behavioural
inputs
"Won't breathe" factorsi.e. CNS depression and CCHS
Figure 5. The pathogenesis of central sleep apnoea. CNS: centralnervous system; CCHS: congenital central hypoventilation syn-drome; UA: upper airway. Reproduced from [45] with permissionfrom the publisher.
39
1D
.G.
MC
SH
AR
RY
ET
AL
.

Statement of Interest
D.J. Eckert is a consultant for Apnex Medical, receiving less than US$20,000 per year. Within thepast 5 years, A. Malhotra has received consulting and/or research income from Philips, Ethicon,Medtronic, Pfizer, Sepracor, Cephalon, Apnex, SGS, SHC, Merck, NMT, IMI and Itamar.
References1. Javaheri S, Parker TJ, Liming JD, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure. Types
and their prevalences, consequences, and presentations. Circulation 1998; 97: 2154–2159.
2. Lanfranchi PA, Somers VK, Braghiroli A, et al. Central sleep apnea in left ventricular dysfunction: prevalence and
implications for arrhythmic risk. Circulation 2003; 107: 727–732.
3. Badr MS, Toiber F, Skatrud JB, et al. Pharyngeal narrowing/occlusion during central sleep apnea. J Appl Physiol
1995; 78: 1806–1815.
4. Sankri-Tarbichi AG, Rowley JA, Badr MS. Expiratory pharyngeal narrowing during central hypocapnic
hypopnea. Am J Respir Crit Care Med 2009; 179: 313–319.
5. White DP, Gleeson K, Pickett CK, et al. Altitude acclimatization: influence on periodic breathing and
chemoresponsiveness during sleep. J Appl Physiol 1987; 63: 401–412.
6. Roca D, Yim Yeh S, Eckert D, et al. Control of breathing. In: Meir H, Kryger MD, Eds. Atlas of Clinical Sleep
Medicine. London, Elsevier, 2010; pp. 37–43.
7. Orem J. The nature of the wakefulness stimulus for breathing. Prog Clin Biol Res 1990; 345: 23–30.
8. Trinder J, Whitworth F, Kay A, et al. Respiratory instability during sleep onset. J Appl Physiol 1992; 73:
2462–2469.
9. Kay A, Trinder J, Bowes G, et al. Changes in airway resistance during sleep onset. J Appl Physiol 1994; 76:
1600–1607.
10. Worsnop C, Kay A, Pierce R, et al. Activity of respiratory pump and upper airway muscles during sleep onset.
J Appl Physiol 1998; 85: 908–920.
11. Dunai J, Wilkinson M, Trinder J. Interaction of chemical and state effects on ventilation during sleep onset. J Appl
Physiol 1996; 81: 2235–2243.
12. Meza S, Mendez M, Ostrowski M, et al. Susceptibility to periodic breathing with assisted ventilation during sleep
in normal subjects. J Appl Physiol 1998; 85: 1929–1940.
13. Skatrud JB, Dempsey JA. Interaction of sleep state and chemical stimuli in sustaining rhythmic ventilation. J Appl
Physiol 1983; 55: 813–822.
14. Douglas NJ, White DP, Weil JV, et al. Hypoxic ventilatory response decreases during sleep in normal men. Am
Rev Respir Dis 1982; 125: 286–289.
15. Skatrud JB, Dempsey JA, Badr S, et al. Effect of airway impedance on CO2 retention and respiratory muscle
activity during NREM sleep. J Appl Physiol 1988; 65: 1676–1685.
16. White DP, Douglas NJ, Pickett CK, et al. Hypoxic ventilatory response during sleep in normal premenopausal
women. Am Rev Respir Dis 1982; 126: 530–533.
17. Wiegand L, Zwillich CW, White DP. Sleep and the ventilatory response to resistive loading in normal men. J Appl
Physiol 1988; 64: 1186–1195.
18. Gugger M, Bogershausen S, Schaffler L. Arousal responses to added inspiratory resistance during REM and non-
REM sleep in normal subjects. Thorax 1993; 48: 125–129.
19. Ratnavadivel R, Stadler D, Windler S, et al. Upper airway function and arousability to ventilatory challenge in
slow wave versus stage 2 sleep in obstructive sleep apnoea. Thorax 2010; 65: 107–112.
20. Quadri S, Drake C, Hudgel DW. Improvement of idiopathic central sleep apnea with zolpidem. J Clin Sleep Med
2009; 5: 122–129.
21. Saboisky J, Eckert D, Malhotra A. Stable breathing through deeper sleeping. Thorax 2010; 65: 95–96.
22. Xie A, Wong B, Phillipson EA, et al. Interaction of hyperventilation and arousal in the pathogenesis of idiopathic
central sleep apnea. Am J Respir Crit Care Med 1994; 150: 489–495.
23. Khoo MC, Kronauer RE, Strohl KP, et al. Factors inducing periodic breathing in humans: a general model. J Appl
Physiol 1982; 53: 644–659.
24. Stanchina ML, Ellison K, Malhotra A, et al. The impact of cardiac resynchronization therapy on obstructive sleep
apnea in heart failure patients: a pilot study. Chest 2007; 132: 433–439.
25. Naughton MT, Andreas S. Sleep apnoea in chronic heart failure. Eur Respir Mono 2010; 50: 396–420.
26. Meza S, Younes M. Ventilatory stability during sleep studied with proportional assist ventilation (PAV). Sleep
1996; 19: Suppl. 10, S164–S166.
27. Wellman A, Malhotra A, Jordan AS, et al. Chemical control stability in the elderly. J Physiol 2007; 581: 291–298.
28. Weese-Mayer DE, Rand CM, Berry-Kravis EM, et al. Congenital central hypoventilation syndrome from past to
future: model for translational and transitional autonomic medicine. Pediatr Pulmonol 2009; 44: 521–535.
29. Antic NA, Malow BA, Lange N, et al. PHOX2B mutation-confirmed congenital central hypoventilation
syndrome: presentation in adulthood. Am J Respir Crit Care Med 2006; 174: 923–927.
39
2C
EN
TR
AL
SL
EE
PA
PN
OE
A

30. Idiopathic congenital central hypoventilation syndrome: diagnosis and management. American Thoracic Society.
Am J Respir Crit Care Med 1999; 160: 368–373.
31. Weese-Mayer DE, Silvestri JM, Menzies LJ, et al. Congenital central hypoventilation syndrome: diagnosis,
management, and long-term outcome in thirty-two children. J Pediatr 1992; 120: 381–387.
32. Fleming PJ, Cade D, Bryan MH, et al. Congenital central hypoventilation and sleep state. Pediatrics 1980; 66: 425–428.
33. Huang J, Marcus CL, Bandla P, et al. Cortical processing of respiratory occlusion stimuli in children with central
hypoventilation syndrome. Am J Respir Crit Care Med 2008; 178: 757–764.
34. Santiago TV, Edelman NH. Opioids and breathing. J Appl Physiol 1985; 59: 1675–1685.
35. Weil JV, McCullough RE, Kline JS, et al. Diminished ventilatory response to hypoxia and hypercapnia after
morphine in normal man. N Engl J Med 1975; 292: 1103–1106.
36. Mogri M, Khan MI, Grant BJ, et al. Central sleep apnea induced by acute ingestion of opioids. Chest 2008; 133:
1484–1488.
37. Wang D, Teichtahl H, Drummer O, et al. Central sleep apnea in stable methadone maintenance treatment
patients. Chest 2005; 128: 1348–1356.
38. Elliott AM, Smith BH, Penny KI, et al. The epidemiology of chronic pain in the community. Lancet 1999; 354:
1248–1252.
39. Luo X, Pietrobon R, Hey L. Patterns and trends in opioid use among individuals with back pain in the United
States. Spine (Phila Pa 1976) 2004; 29: 884–890.
40. Mogri M, Desai H, Webster L, et al. Hypoxemia in patients on chronic opiate therapy with and without sleep
apnea. Sleep Breath 2009; 13: 49–57.
41. Teichtahl H, Wang D, Cunnington D, et al. Ventilatory responses to hypoxia and hypercapnia in stable
methadone maintenance treatment patients. Chest 2005; 128: 1339–1347.
42. Gray PA, Rekling JC, Bocchiaro CM, et al. Modulation of respiratory frequency to peptidergic input to
rythmogenic neurons in the preBotzinger complex. Science 1999; 286: 1566–1568.
43. Hajiha M, DuBord MA, Liu H, et al. Opioid receptor mechanisms at the hypoglossal motor pool and effects on
tongue muscle activity in vivo. J Physiol 2009; 587: 2677–2692.
44. Robinson RW, Zwillich CW, Bixler EO, et al. Effects of oral narcotics on sleep-disordered breathing in healthy
adults. Chest 1987; 91: 197–203.
45. Eckert DJ, Jordan AS, Merchia P, et al. Central sleep apnea: pathophysiology and treatment. Chest 2007; 131:
595–607.
46. Javaheri S, Malik A, Smith J, et al. Adaptive pressure support servoventilation: a novel treatment for sleep apnea
associated with use of opioids. J Clin Sleep Med 2008; 4: 305–310.
47. Ramar K. Reversal of sleep-disordered breathing with opioid withdrawal. Pain Pract 2009; 9: 394–398.
48. Olson AL, Zwillich C. The obesity hypoventilation syndrome. Am J Med 2005; 118: 948–956.
49. Sampson MG, Grassino K. Neuromechanical properties in obese patients during carbon dioxide rebreathing. Am
J Med 1983; 75: 81–90.
50. Sharp JT, Henry JP, Sweany SK, et al. Effects of mass loading the respiratory system in man. J Appl Physiol 1964;
19: 959–966.
51. Zwillich CW, Sutton FD, Pierson DJ, et al. Decreased hypoxic ventilatory drive in the obesity-hypoventilation
syndrome. Am J Med 1975; 59: 343–348.
52. Phipps PR, Starritt E, Caterson I, et al. Association of serum leptin with hypoventilation in human obesity.
Thorax 2002; 57: 75–76.
53. Poulain M, Doucet M, Major GC, et al. The effect of obesity on chronic respiratory diseases: pathophysiology and
therapeutic strategies. CMAJ 2006; 174: 1293–1299.
54. Gomez A, Mink S. Interaction between effects of hypoxia and hypercapnia on altering left ventricular relaxation
and chamber stiffness in dogs. Am Rev Respir Dis 1992; 146: 313–320.
55. Fessler HE. Heart-lung interactions: applications in the critically ill. Eur Respir J 1997; 10: 226–237.
56. Gastrointestinal surgery for severe obesity. Proceedings of a National Institutes of Health Consensus
Development Conference. March 25–27, 1991, Bethesda, MD. Am J Clin Nutr 1992; 55: Suppl. 2, 487S–619S.
57. Malhotra A, Berry RB, White DP. Central sleep apnea. Carney PR, Berry RB, Geyer JD, eds. Clinical Sleep
Disorders. Philadelphia, Lippincott Williams and Wilkins, 2004; 331–349.
58. Solin P, Jackson DM, Roebuck T, et al. Cardiac diastolic function and hypercapnic ventilatory responses in
central sleep apnoea. Eur Respir J 2002; 20: 717–723.
59. Solin P, Roebuck T, Johns DP, et al. Peripheral and central ventilatory responses in central sleep apnea with and
without congestive heart failure. Am J Respir Crit Care Med 2000; 162: 2194–2200.
60. Xie A, Rutherford R, Rankin F, et al. Hypocapnia and increased ventilatory responsiveness in patients with
idiopathic central sleep apnea. Am J Respir Crit Care Med 1995; 152: 1950–1955.
61. White DP, Zwillich CW, Pickett CK, et al. Central sleep apnea. Improvement with acetazolamide therapy. Arch
Intern Med 1982; 142: 1816–1819.
62. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement
techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999;
22: 667–689.
63. Berssenbrugge A, Dempsey J, Iber C, et al. Mechanisms of hypoxia-induced periodic breathing during sleep in
humans. J Physiol 1983; 343: 507–524.
39
3D
.G.
MC
SH
AR
RY
ET
AL
.

64. Erba P, Anastasi S, Senn O, et al. Acute mountain sickness is related to nocturnal hypoxemia but not to
hypoventilation. Eur Respir J 2004; 24: 303–308.
65. West JB, Peters RM Jr, Aksnes G, et al. Nocturnal periodic breathing at altitudes of 6,300 and 8,050 m. J Appl
Physiol 1986; 61: 280–287.
66. Eichenberger U, Weiss E, Riemann D, et al. Nocturnal periodic breathing and the development of acute high
altitude illness. Am J Respir Crit Care Med 1996; 154: 1748–1754.
67. Lahiri S, Maret K, Sherpa MG. Dependence of high altitude sleep apnea on ventilatory sensitivity to hypoxia.
Respir Physiol 1983; 52: 281–301.
68. Normand H, Vargas E, Bordachar J, et al. Sleep apneas in high altitude residents (3,800 m). Int J Sports Med 1992;
13: Suppl. 1, S40–S42.
69. Prabhakar NR, Peng YJ, Kumar GK, et al. Long-term regulation of carotid body function: acclimatization and
adaptation. Adv Exp Med Biol 2009; 648: 307–317.
70. Dempsey JA, Smith CA, Harms CA, et al. Sleep-induced breathing instability. University of Wisconsin-Madison
Sleep and respiration Research Group. Sleep 1996; 19: 236–247.
71. Anholm JD, Powles AC, Downey R 3rd, et al. Operation Everest II: arterial oxygen saturation and sleep at
extreme simulated altitude. Am Rev Respir Dis 1992; 145: 817–826.
72. Beaumont M, Goldenberg F, Lejeune D, et al. Effect of zolpidem on sleep and ventilatory patterns at simulated
altitude of 4,000 meters. Am J Respir Crit Care Med 1996; 153: 1864–1869.
73. Goldenberg F, Richalet JP, Onnen I, et al. Sleep apneas and high altitude newcomers. Int J Sports Med 1992; 13:
Suppl. 1, S34–S36.
74. Dubowitz G. Effect of temazepam on oxygen saturation and sleep quality at high altitude: randomised placebo
controlled crossover trial. BMJ 1998; 316: 587–589.
75. Fischer R, Lang SM, Leitl M, et al. Theophylline and acetazolamide reduce sleep-disordered breathing at high
altitude. Eur Respir J 2004; 23: 47–52.
76. Kupper TE, Strohl KP, Hoefer M, et al. Low-dose theophylline reduces symptoms of acute mountain sickness.
J Travel Med 2008; 15: 307–314.
77. Hackett PH, Roach RC, Harrison GL, et al. Respiratory stimulants and sleep periodic breathing at high altitude.
Almitrine versus acetazolamide. Am Rev Respir Dis 1987; 135: 896–898.
78. Swenson ER, Leatham KL, Roach RC, et al. Renal carbonic anhydrase inhibition reduces high altitude sleep
periodic breathing. Respir Physiol 1991; 86: 333–343.
79. McElroy MK, Gerard A, Powell FL, et al. Nocturnal O2 enrichment of room air at high altitude increases daytime
O2 saturation without changing control of ventilation. High Alt Med Biol 2000; 1: 197–206.
80. Windsor JS, Rodway GW. Supplemental oxygen and sleep at altitude. High Alt Med Biol 2006; 7: 307–311.
81. Guilleminault C, Hill MH, Simmons FB, et al. Passive constriction of the upper airway during central apneas:
fiberoptic and EMG investigations. Respir Physiol 1997; 108: 11–22.
82. Hudgel DW, Gordon EA, Thanakitcharu S, et al. Instability of ventilatory control in patients with obstructive
sleep apnea. Am J Respir Crit Care Med 1998; 158: 1142–1149.
83. Wellman A, Jordan AS, Malhotra A, et al. Ventilatory control and airway anatomy in obstructive sleep apnea. Am
J Respir Crit Care Med 2004; 170: 1225–1232.
84. Wiegand L, Zwillich CW, Wiegand D, et al. Changes in upper airway muscle activation and ventilation during
phasic REM sleep in normal men. J Appl Physiol 1991; 71: 488–497.
85. Orem J. Neuronal mechanisms of respiration in REM sleep. Sleep 1980; 3: 251–267.
86. Kirkness JP, Madronio M, Stavrinou R, et al. Surface tension of upper airway mucosal lining liquid in obstructive
sleep apnea/hypopnea syndrome. J Appl Physiol 2003; 95: 1761–1766.
87. Lehman S, Antic NA, Thompson C, et al. Central sleep apnea on commencement of continuous positive airway
pressure in patients with a primary diagnosis of obstructive sleep apnea-hypopnea. J Clin Sleep Med 2007; 3:
462–466.
88. Eckert DJ, Malhotra A, Jordan AS. Mechanisms of apnea. Prog Cardiovasc Dis 2009; 51: 313–323.
89. Salloum A, Rowley JA, Mateika JH, et al. Increased propensity for central apnea in patients with obstructive sleep
apnea: effect of nasal continuous positive airway pressure. Am J Respir Crit Care Med, 181: 189–193.
90. Morgenthaler TI, Gay PC, Gordon N, et al. Adaptive servoventilation versus noninvasive positive pressure
ventilation for central, mixed, and complex sleep apnea syndromes. Sleep 2007; 30: 468–475.
91. Randerath WJ, Galetke W, Kenter M, et al. Combined adaptive servo-ventilation and automatic positive airway
pressure (anticyclic modulated ventilation) in co-existing obstructive and central sleep apnea syndrome and
periodic breathing. Sleep Med 2009; 10: 898–903.
92. Eckert DJ, Catcheside PG, McDonald R, et al. Sustained hypoxia depresses sensory processing of respiratory
resistive loads. Am J Respir Crit Care Med 2005; 172: 1047–1054.
93. Hlavac MC, Catcheside PG, McDonald R, et al. Hypoxia impairs the arousal response to external resistive loading
and airway occlusion during sleep. Sleep 2006; 29: 624–631.
94. McNicholas WT, Carter JL, Rutherford R, et al. Beneficial effect of oxygen in primary alveolar hypoventilation
with central sleep apnea. Am Rev Respir Dis 1982; 125: 773–775.
95. Franklin KA, Eriksson P, Sahlin C, et al. Reversal of central sleep apnea with oxygen. Chest 1997; 111: 163–169.
96. Hanly PJ, Millar TW, Steljes DG, et al. The effect of oxygen on respiration and sleep in patients with congestive
heart failure. Ann Intern Med 1989; 111: 777–782.
39
4C
EN
TR
AL
SL
EE
PA
PN
OE
A

97. Javaheri S, Ahmed M, Parker TJ, et al. Effects of nasal O2 on sleep-related disordered breathing in ambulatory
patients with stable heart failure. Sleep 1999; 22: 1101–1106.
98. Xie A, Rankin F, Rutherford R, et al. Effects of inhaled CO2 and added dead space on idiopathic central sleep
apnea. J Appl Physiol 1997; 82: 918–926.
99. Lorenzi-Filho G, Rankin F, Bies I, et al. Effects of inhaled carbon dioxide and oxygen on cheyne-stokes
respiration in patients with heart failure. Am J Respir Crit Care Med 1999; 159: 1490–1498.
100. Steens RD, Millar TW, Su X, et al. Effect of inhaled 3% CO2 on Cheyne-Stokes respiration in congestive heart
failure. Sleep 1994; 17: 61–68.
101. Andreas S, Weidel K, Hagenah G, et al. Treatment of Cheyne-Stokes respiration with nasal oxygen and carbon
dioxide. Eur Respir J 1998; 12: 414–419.
102. Mebrate Y, Willson K, Manisty CH, et al. Dynamic CO2 therapy in periodic breathing: a modeling study to
determine optimal timing and dosage regimes. J Appl Physiol 2009; 107: 696–706.
103. Krachman SL, Crocetti J, Berger TJ, et al. Effects of nasal continuous positive airway pressure on oxygen body
stores in patients with Cheyne-Stokes respiration and congestive heart failure. Chest 2003; 123: 59–66.
104. Arzt M, Bradley TD. Treatment of sleep apnea in heart failure. Am J Respir Crit Care Med 2006; 173: 1300–1308.
105. Bradley TD, Logan AG, Kimoff RJ, et al. Continuous positive airway pressure for central sleep apnea and heart
failure. N Engl J Med 2005; 353: 2025–2033.
106. Thomas RJ, Daly RW, Weiss JW. Low-concentration carbon dioxide is an effective adjunct to positive airway
pressure in the treatment of refractory mixed central and obstructive sleep-disordered breathing. Sleep 2005; 28:
69–77.
107. Storre JH, Seuthe B, Fiechter R, et al. Average volume-assured pressure support in obesity hypoventilation: a
randomized crossover trial. Chest 2006; 130: 815–821.
108. Johnson KG, Johnson DC. Bilevel positive airway pressure worsens central apneas during sleep. Chest 2005; 128:
2141–2150.
109. Teschler H, Dohring J, Wang YM, et al. Adaptive pressure support servo-ventilation: a novel treatment for
Cheyne-Stokes respiration in heart failure. Am J Respir Crit Care Med 2001; 164: 614–619.
110. Javaheri S. Acetazolamide improves central sleep apnea in heart failure: a double-blind, prospective study. Am J
Respir Crit Care Med 2006; 173: 234–237.
111. Nakayama H, Smith CA, Rodman JR, et al. Effect of ventilatory drive on carbon dioxide sensitivity below eupnea
during sleep. Am J Respir Crit Care Med 2002; 165: 1251–1260.
112. Suissa S, Hemmelgarn B, Blais L, et al. Bronchodilators and acute cardiac death. Am J Respir Crit Care Med 1996;
154: 1598–1602.
39
5D
.G.
MC
SH
AR
RY
ET
AL
.