Embed Size (px)
Citation preview
www.elsevier.com/locate/jcf
Journal of Cystic Fibrosis
Cellular proteolysis and systemic inflammation during exacerbation
in cystic fibrosis
Alina A. Ionescu, Lisette S. Nixon, Dennis J. Shale*
Section of Respiratory and Communicable Diseases, Department of Medicine, University of Wales College of Medicine, UK
Academic Centre, Llandough Hospital, Cardiff and Vale NHS Hospital Trust, Penarth, South Glamorgan, CF64 2XX, UK
Received 3 March 2004; accepted 27 July 2004
Abstract
Background: Weight loss indicates a poor prognosis in cystic fibrosis (CF). We hypothesised that fat-free mass (FFM) depletion and
increased systemic inflammation would be associated with increased cellular proteolysis during an exacerbation of the respiratory symptoms.
Patients were studied prospectively from the beginning of treatment with antibiotics when admitted to the Adults CF Centre.
Methods: Twenty six patients with CF were studied at the start and end of antibiotic treatment and 2 weeks later. Mean (95% CI) FEV1 when
clinically stable was 54.1 (44.5, 62.6)% predicted. Urinary excretion of Pseudouridine (5-ribosyluracil, PSU) was determined as an indicator
of cellular protein breakdown. Body composition was assessed by dual energy X-ray absorptiometry (DXA).
Results: Patients had increased concentrations of PSU at all assessments ( pb0.01). Those with a low FFM had greater PSU (ratio to FFMI)
than those with a normal FFM at all assessments. At the start of treatment, PSU was related to FFM, C-reactive protein (CRP) ( pb0.05) and
tumour necrosis factor (TNF)a soluble receptors (sr) I and II ( pb0.01). Circulating inflammatory mediators were greater in patients than in
healthy subjects at all assessments.
Conclusion: Increased protein breakdown is associated with a low FFM and increased systemic inflammation and it may be a contributory
mechanism of poor weight preservation in CF.
D 2004 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Keywords: Protein catabolism; Systemic inflammation; Cystic fibrosis; 5-Ribosyluracil; Protein breakdown; Fat-free mass
1. Introduction
Weight loss with depletion of fat-free mass (FFM) is
associated with increased morbidity and mortality in cystic
fibrosis (CF) [1,2]. The cause of such loss is likely to be
multifactorial with reduced nutrient intake contributing to a
negative energy balance. Other factors include an increased
energy and oxygen cost of breathing, which is added to by
systemic inflammatory and catabolic responses, also
1569-1993/$ - see front matter D 2004 European Cystic Fibrosis Society. Publish
doi:10.1016/j.jcf.2004.07.003
* Corresponding author. Section of Respiratory and Communicable
Diseases, University of Wales College of Medicine, Academic Centre,
Llandough Hospital, Penarth, South Glamorgan, CF64 2XX, UK. Tel.: +44
29 20716948; fax: +44 29 20716416.
E-mail address: [email protected] (D.J. Shale).
reported in chronic obstructive pulmonary disease (COPD)
[3–6].
We have reported increased excretion of 5-ribosyluracil
(pseudouridine, PSU), an indicator of RNA and cellular
protein breakdown, in clinically stable adults with CF
compared with matched healthy subjects [7]. Excretion of
PSU has been validated against amino-acid infusion and
used to assess cell turnover in inflammatory diseases,
leukaemia, lymphomas, and solid tumours [8–12]. PSU is
derived from RNA breakdown, is independent of diet, is
neither metabolised further nor re-incorporated, and hence
indicates cell turnover and cell-derived protein breakdown.
PSU was related to leucin turnover (Amol/kg/min, r=0.68,
pb0.01) and to ketoisocaproic acid turnover (r=0.96,
pb0.001) [8]. Excretion of PSU is influenced by age, but
with little reported variation from day to day [13]. In other
3 (2004) 253–258
ed by Elsevier B.V. All rights reserved.

A.A. Ionescu et al. / Journal of Cystic Fibrosis 3 (2004) 253–258254
inflammatory states associated with weight loss and
cachexia, such as rheumatoid arthritis and HIV, PSU has
been found to relate to disease severity and outcome
[11,12]. Excretion of PSU was linked to the severity of
lung disease and to the loss of FFM [7]. A possible link
between inflammation and proteolysis is that IL-6 and
TNFa stimulate proteolysis in skeletal muscle probably by
activation of the ATP-ubiquitin-proteasome pathway [14].
The transgenic IL-6 mouse constitutively secretes IL-6 and
develops a severe proteolytic myopathy, which was reversed
by an IL-6 receptor blocking antibody [15]. Infusion of
TNFa into the forearm arteries of healthy subjects leads to a
rapid efflux of amino acids and in vitro acts via the NF-kB
pathway to inhibit the differentiation of myoblasts into
myocytes [16]. Previous studies in children with CF have
reported abnormalities of protein turnover related to poor
nutrition, but the relationship to systemic inflammation has
not been explored [17,18].
Based on such findings, we hypothesised that increased
cellular proteolysis occurs during an exacerbation of
respiratory symptoms, persists after the antibiotic treatment
and is linked to a reduced FFM and increased systemic
inflammation. We tested this hypothesis by investigating the
relationship between a marker of cellular proteolysis and
systemic inflammatory mediators in adults with CF during
and after the treatment of an exacerbation of respiratory
symptoms.
2. Materials and methods
2.1. Patients
Twenty six patients (12 male) with known CF (clinical
findings, sweat Na+ and Cl� N70 mmol/L and appropriate
genotype) mean (95% CI) age 23.8 (22.2, 25.4) years were
included at the beginning of a 14-day course of antibiotic
treatment for an exacerbation of their respiratory symptoms.
Mean (95% CI) FEV1 when clinically stable was 54.1 (45.5,
62.7)% predicted. An exacerbation was defined as increased
cough, sputum production and purulence, shortness of
breath, systemic symptoms such as fever or weight loss,
and a reduction in FEV1N10% compared with values when
clinically stable in the preceding year. All patients were
colonised with Pseudomonas aeruginosa, defined as more
than three isolations from sputum in the preceding 6
months. All patients had a DF508/DF508 genotype, all
received enzyme supplements with meals for pancreatic
insufficiency and had no clinical signs of malabsorption
when studied. Diabetes mellitus, liver cirrhosis, chronic
respiratory failure with cor pulmonale and oral cortico-
steroid treatment were exclusion criteria. The study had
Local Research Ethics Committee approval and all patients
gave written consent. The study was carried out over an 8-
month period, which allowed 26 consecutive patients to be
included.
2.2. Healthy subjects
Twenty five age matched healthy subjects (11 male) age
24.6 (23.3, 25.9) years had blood samples taken for
concentrations of inflammatory mediators and urine samples
for concentrations of pseudouridine and creatinine.
2.3. Methods
2.3.1. Body composition
Height and weight were measured and the body mass
index calculated (kg/m2). Fat mass and FFM were assessed
by dual energy X-ray absorptiometry (DXA, Hologic,
Waltham, Ma, USA, software denhanced body composition
v5.70T). Two groups of patients were identified: (1) low
FFM if less than the lower 5th percentile for healthy age
matched subjects who had previously been studied with
the same methodology [7]; (2) normal FFM if more than
the lower 5th percentile for healthy subjects. This cut-off
point was used in order to clearly identify those patients
with severe depletion of FFM [7]. DXA was assessed once
within the study period, when the patients were clinically
stable.
2.3.2. Food intake assessment
The nutritional intake was assessed over three consec-
utive days, at the beginning and end of antibiotic treatment
and 2 weeks later. All patients were reviewed by a dietician
on admission and all received nutritional supplement drinks.
Three patients received supplementary overnight feeding
through naso-gastric (two patients) or percutaneous gastro-
stomy tubes (one patient). The mean energy intake of the 3
days was reported, including nutritional supplements, as
calculated.
2.3.3. Urinary pseudouridine
Pseudouridine was measured by high-performance
liquid chromatography in the second void dspotT morning
urine sample and reported as a ratio to urinary creatinine
(Amol/mmol) [19,20]. Repeated measurements from our
laboratory of PSU in patients with CF during clinical
stability and in healthy adults have found a day to day
variability of less than 10%. Patients with CF had PSU
measured at the start and end of antibiotic treatment and 2
weeks later. The healthy subjects had PSU measured on
one occasion. Excretion of PSU was also reported as ratio
to FFM index (FFMI, (Amol/mmol/kg/m2) to control for
the differences in body composition and height between
individuals (a greater protein turnover would be expected
for a larger FFM).
2.3.4. Spirometry
FEV1 was measured by dry wedge spirometry and
expressed as % predicted. The number of exacerbations of
respiratory symptoms treated with i.v. antibiotics in the year
previous to the study was recorded from the patients files.
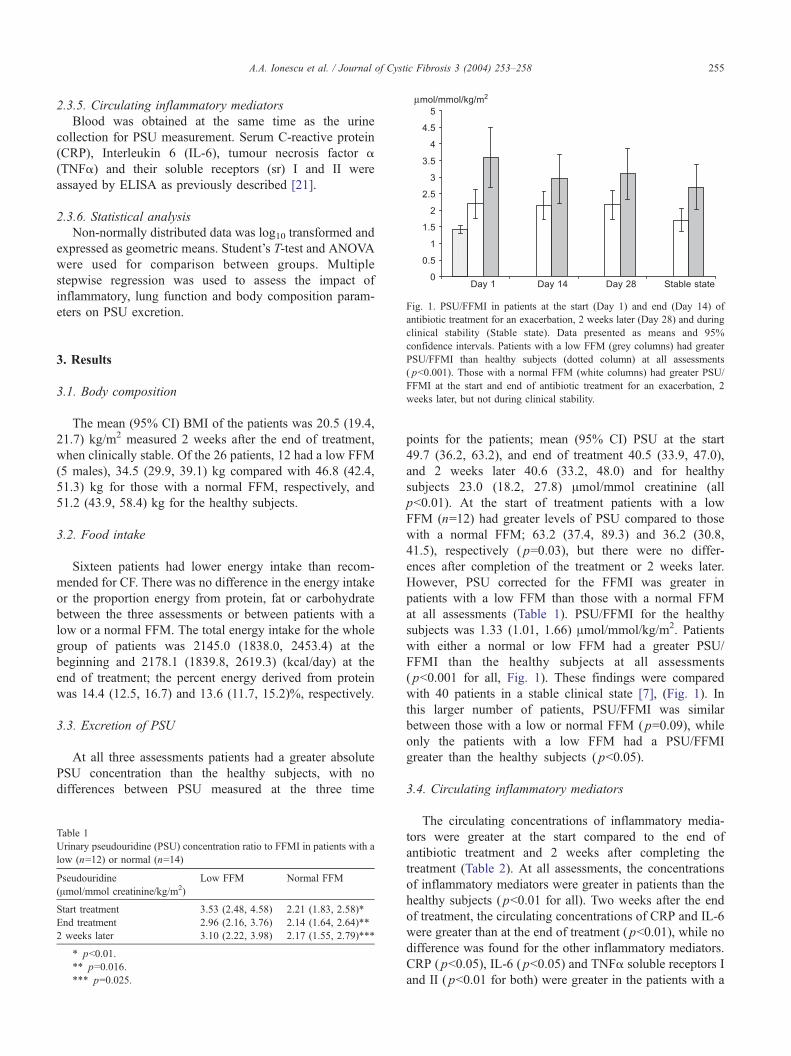
Fig. 1. PSU/FFMI in patients at the start (Day 1) and end (Day 14) of
antibiotic treatment for an exacerbation, 2 weeks later (Day 28) and during
A.A. Ionescu et al. / Journal of Cystic Fibrosis 3 (2004) 253–258 255
2.3.5. Circulating inflammatory mediators
Blood was obtained at the same time as the urine
collection for PSU measurement. Serum C-reactive protein
(CRP), Interleukin 6 (IL-6), tumour necrosis factor a
(TNFa) and their soluble receptors (sr) I and II were
assayed by ELISA as previously described [21].
2.3.6. Statistical analysis
Non-normally distributed data was log10 transformed and
expressed as geometric means. Student’s T-test and ANOVA
were used for comparison between groups. Multiple
stepwise regression was used to assess the impact of
inflammatory, lung function and body composition param-
eters on PSU excretion.
clinical stability (Stable state). Data presented as means and 95%
confidence intervals. Patients with a low FFM (grey columns) had greater
PSU/FFMI than healthy subjects (dotted column) at all assessments
( pb0.001). Those with a normal FFM (white columns) had greater PSU/
FFMI at the start and end of antibiotic treatment for an exacerbation, 2
weeks later, but not during clinical stability.
3. Results
3.1. Body composition
The mean (95% CI) BMI of the patients was 20.5 (19.4,
21.7) kg/m2 measured 2 weeks after the end of treatment,
when clinically stable. Of the 26 patients, 12 had a low FFM
(5 males), 34.5 (29.9, 39.1) kg compared with 46.8 (42.4,
51.3) kg for those with a normal FFM, respectively, and
51.2 (43.9, 58.4) kg for the healthy subjects.
3.2. Food intake
Sixteen patients had lower energy intake than recom-
mended for CF. There was no difference in the energy intake
or the proportion energy from protein, fat or carbohydrate
between the three assessments or between patients with a
low or a normal FFM. The total energy intake for the whole
group of patients was 2145.0 (1838.0, 2453.4) at the
beginning and 2178.1 (1839.8, 2619.3) (kcal/day) at the
end of treatment; the percent energy derived from protein
was 14.4 (12.5, 16.7) and 13.6 (11.7, 15.2)%, respectively.
3.3. Excretion of PSU
At all three assessments patients had a greater absolute
PSU concentration than the healthy subjects, with no
differences between PSU measured at the three time
Table 1
Urinary pseudouridine (PSU) concentration ratio to FFMI in patients with a
low (n=12) or normal (n=14)
Pseudouridine
(Amol/mmol creatinine/kg/m2)
Low FFM Normal FFM
Start treatment 3.53 (2.48, 4.58) 2.21 (1.83, 2.58)*
End treatment 2.96 (2.16, 3.76) 2.14 (1.64, 2.64)**
2 weeks later 3.10 (2.22, 3.98) 2.17 (1.55, 2.79)***
* pb0.01.
** p=0.016.
*** p=0.025.
points for the patients; mean (95% CI) PSU at the start
49.7 (36.2, 63.2), and end of treatment 40.5 (33.9, 47.0),
and 2 weeks later 40.6 (33.2, 48.0) and for healthy
subjects 23.0 (18.2, 27.8) Amol/mmol creatinine (all
pb0.01). At the start of treatment patients with a low
FFM (n=12) had greater levels of PSU compared to those
with a normal FFM; 63.2 (37.4, 89.3) and 36.2 (30.8,
41.5), respectively ( p=0.03), but there were no differ-
ences after completion of the treatment or 2 weeks later.
However, PSU corrected for the FFMI was greater in
patients with a low FFM than those with a normal FFM
at all assessments (Table 1). PSU/FFMI for the healthy
subjects was 1.33 (1.01, 1.66) Amol/mmol/kg/m2. Patients
with either a normal or low FFM had a greater PSU/
FFMI than the healthy subjects at all assessments
( pb0.001 for all, Fig. 1). These findings were compared
with 40 patients in a stable clinical state [7], (Fig. 1). In
this larger number of patients, PSU/FFMI was similar
between those with a low or normal FFM ( p=0.09), while
only the patients with a low FFM had a PSU/FFMI
greater than the healthy subjects ( pb0.05).
3.4. Circulating inflammatory mediators
The circulating concentrations of inflammatory media-
tors were greater at the start compared to the end of
antibiotic treatment and 2 weeks after completing the
treatment (Table 2). At all assessments, the concentrations
of inflammatory mediators were greater in patients than the
healthy subjects ( pb0.01 for all). Two weeks after the end
of treatment, the circulating concentrations of CRP and IL-6
were greater than at the end of treatment ( pb0.01), while no
difference was found for the other inflammatory mediators.
CRP ( pb0.05), IL-6 ( pb0.05) and TNFa soluble receptors I
and II ( pb0.01 for both) were greater in the patients with a
Table 2
Inflammatory mediators in patients at the start and end of antibiotic treatment and 2 weeks later (n=26); geometric means (95% CI)
Start End 2 weeks later
CRP (Ag/ml) 27.5 (15.1, 51.2)* 4.6 (2.4, 9.5) 12.5 (3.9, 25.1)*
IL-6 (pg/ml) 5.9 (3.9, 8.7)* 2.9 (2.1, 3.9) 6.1 (3.3, 12.5)*
IL-6 sr (ng/ml) 42.6 (37.1, 46.7)* 43.6 (38.9, 48.9) 39.8 (31.6, 50.1
TNFa (pg/ml) 3.7 (3.1, 4.6)* 2.9 (2.5, 3.6) 2.8 (2.1, 3.6)
TNFa sr I (ng/ml) 1.3 (1.1, 1.6)* 1.0 (0.9, 1.2) 1.0 (0.8, 1.3)
TNFa sr II (ng/ml) 3.5 (3.1, 3.9)* 2.8 (2.6, 3.3) 2.5 (2.0, 3.9)
* pb0.01 compared to the end of treatment; 2 weeks after the end of treatment CRP and IL-6 were greater than at the end of treatment, but not the othe
inflammatory mediators.
A.A. Ionescu et al. / Journal of Cystic Fibrosis 3 (2004) 253–258256
low FFM compared to those with a normal FFM at the start
of treatment, but not at the end of treatment or 2 weeks later.
Patients with a low FFM had a greater number of
exacerbations in the year previous to the study compared
with those with a normal FFM; mean (95% CI) was 7.4 (4.6,
10.2) and 3.4 (2.4, 4.3), respectively ( pb0.01).
Analysis of regression showed that the following factors
were related to the concentration of PSU when commencing
treatment with antibiotics; FFM (r2=0.2, p=0.04), CRP (r2=
0.21, p=0.02), IL-6 (r2=0.37, p=0.02), (TNFa sr I (r2=0.3,
pb0.01), TNFa sr II (r2 0.25, p=0.01), and the number of
exacerbations (r2=0.3, pb0.01).
4. Discussion
Increased breakdown of cellular protein as indicated by
urinary PSU concentrations was present in adult patients at
the beginning and end of antibiotic treatment for an
exacerbation of respiratory symptoms and 2 weeks later.
The concentration of PSU was approximately twice that of
the matched healthy subjects. Patients with a low FFM had a
greater output of PSU compared with those with a normal
FFM at all assessments. To allow for differences in total
FFM and height, which was most variable in the patients
and could reflect either impaired growth as a child or current
loss of FFM, we expressed PSU concentration in terms of
the FFMI. Using this ratio, patients with a low FFM had
consistently greater PSU concentrations than those with a
normal FFM, and both had markedly greater concentrations
than the healthy subjects at all assessments. In both patient
subgroups, PSU concentrations were unaffected by anti-
biotic treatment, indicating that the underlying protein
catabolic state was not modified by such treatment.
However, the mean PSU decreased by nearly 20% after
treatment, but the concentration was not statistically differ-
ent from the start of treatment, possibly due to the wide CI
of the mean. We have previously demonstrated that
antibiotic treatment was associated with a reduction in
resting energy expenditure, correction of the cortisol–IGF1
ratio, a reduction in lipolysis and circulating catecholamines
and modest weight gain [3,7], and it might be expected that
such changes would be associated with a reduction in
proteolysis. However, our finding of no change in PSU is in
keeping with those of N-telopeptides of Collagen 1 (NTx) in
)
r
CF where antibiotic treatment led to a reduction in
excretion, but not to levels similar to those in healthy
subjects [22]. These data taken together with the PSU
findings reported in clinically stable adults with CF suggest
that protein catabolism in adults with CF and chronic
pulmonary bacterial infection is a chronic or near contin-
uous process, linked to the persistent systemic inflammatory
response, and is likely to contribute to the loss of skeletal
muscle and bone mineral density, and their associated
complications [22,23]. The inappropriately high protein
breakdown in patients with a low FFM suggests a non-
adapting catabolic response, which was related to a greater
inflammatory response in this group.
Our findings support the view that loss of skeletal muscle
is not due purely to an inadequate energy intake, as this did
not change after the treatment, while it was likely that at the
beginning of treatment, the intake may have been inad-
equate for the increased energy requirements. In the patients
with CF, there is circumstantial evidence of a possible effect
of the increased concentration of systemic inflammatory
mediators and increased proteolysis [7]. While correlation
does not imply causation, the analysis of regression
suggested that at the beginning of an exacerbation, the
circulating concentrations of inflammatory mediators have
an effect on PSU excretion. The increased systemic
inflammation could be one of several mechanistic factors
in the breakdown of cellular protein. The precise source of
increased PSU excretion in our patients is unknown, but
skeletal muscle is likely to be involved, because it
constitutes a large proportion of tissue-related protein. In
other chronic inflammatory lung disease, such as COPD,
altered amino-acid metabolism occurred in both the
circulation and in lower limb muscles at rest and after
exercise [24]. Such changes were related to the acute phase
inflammatory response and to metabolic derangements
[4,5]. It is unclear if changes in amino-acid metabolism
relate to loss of muscle mass, though they could indicate
muscle protein breakdown, particularly during exercise. In
addition to potential inflammatory factors and altered
muscle metabolism, the effect of a negative energy balance
secondary to increased energy costs and an insufficient
energy intake for these needs may be another factor. This
would represent an adaptation in intermediary metabolism
to allow storage and structural tissues, such as skeletal
muscle, to be utilised for energy. Lung disease itself may

A.A. Ionescu et al. / Journal of Cystic Fibrosis 3 (2004) 253–258 257
contribute to extra energy costs as approximately 50% of the
excess in resting energy expenditure was explained by
increased oxygen cost of breathing and 30% by the systemic
inflammatory response [3,25,26].
With regression analysis, the number of exacerbations in
the year prior to the study was shown to have an effect on
protein catabolism. Patients experiencing more frequent
exacerbations may enter a dvicious spiralT where they have
increased proteolysis and weight loss during exacerbations
and are unable to recover the loss of weight and FFM after
each exacerbation because of a high frequency of exacer-
bations. This interpretation would explain our findings for
both PSU and NTx in this and other studies of increased
protein catabolism in adults with CF [7,22]. Such a spiral
associated with severe impairment of lung function and loss
of FFM suggests that it is important to identify such patients
who are more likely to have difficulties in recouping the
weight loss between exacerbations due to sustained protein
catabolism.
4.1. Limitations of this study
This study could be criticised for only determining tissue
protein breakdown by an indirect method, rather than
protein turnover. Generally methods to determine protein
turnover are not applicable to routine clinical use or large
group investigations, because they are laborious and costly
[8,13]. The urinary excretion of methylated nucleosides has
been previously used as a non-invasive method for the
assessment of protein metabolism [9].
This study found, with a non-invasive method, persis-
tently increased cellular proteolysis in adults with CF and
chronic pulmonary bacterial infection. This was associated
with FFM status, exacerbation rates and persistent systemic
inflammation. Future studies will be needed to clarify the
relationship between the increased proteolysis and protein
synthesis in CF.
Acknowledgements
This work was supported by Glaxo Smith Kline, the
Cystic Fibrosis Trust (UK), the Astra Foundation (UK), the
British Lung Foundation and the British Thoracic Society.
The authors would like to thank Dr. Derek Buss and Mr.
Paras Mavani for their assistance in setting up the method
used for the measurement of pseudouridine and Professor
PA Routledge for permitting access to some of the
laboratory equipment.
References
[1] Elborn JS, Shale DJ, Britton JR. Cystic fibrosis: current survival and
population estimates to the year 2000. Thorax 1991;46:881–5.
[2] Davis PB, Drumm M, Konstan MW. Cystic fibrosis. Am J Respir Crit
Care Med 1996;154:1229–56.
[3] Bell SC, Bowerman AM, Nixon LS, Macdonald IA, Elborn JS,
Shale DJ. Metabolic and inflammatory responses to pulmonary
exacerbations in adults with cystic fibrosis. Eur J Clin Invest 2000;
30:553–9.
[4] Schols AMWJ, Buurman WA, Brekel AJS, Dentener MA, Wouters
EFM. Evidence for a relation between metabolic derangements and
increased levels of inflammatory mediators in a subgroup of patients
with chronic obstructive pulmonary disease. Thorax 1996;51:819–24.
[5] Eid A, Ionescu AA, Nixon LS, Lewis-Jenkins V, Matthews S, Grifiths
TL, et al. Inflammatory response and body composition in COPD. Am
J Respir Crit Care Med 2001;164:1414–8.
[6] Ionescu AA, Nixon LS, Routledge PA, Shale DJ. Protein catabolism
in Cystic Fibrosis and COPD. Am J Respir Crit Care Med
2003;167(7):A918 [Abstract presented (poster) at the International
Conference of the ATS, Seattle 2003.].
[7] Ionescu AA, Nixon LS, Luzio S, Lewis-Jenkins V, Evans WD, Stone
MD, et al. Pulmonary function, body composition, and protein
catabolism in adults with cystic fibrosis. Am J Respir Crit Care
Med 2002;165:495–500.
[8] Bohles H, Brendel L, Forster H, Trager K, Vogt J, Georgieff M. The
effect of human growth hormone therapy on l-(methyl-2H3)-leucine
turnover and urinary pseudouridine concentration in patients with
Ullrich–Turner syndrome. Eur J Pediatr 1996;155:275–80.
[9] Sander G, Hulsemann J, Topp H. Protein and RNA turnover in
preterm infants and adults: a comparison based on urinary excretion of
3-methylhistidine and of modified one-way RNA catabolites. Ann
Nutr Metab 1986;30:137–42.
[10] Lu JY, Lai RS, Liang LL, Wang HC, Lin TI. Evaluation of urinary
pseudouridine as a tumour marker in lung cancer. J Formos Med
Assoc 1994;93:25–9.
[11] Tebib JG, Reynaud C, Cedoz JP, Letroublon MC, Niveleau A.
Relationship between urinary excretion of modified nucleosides and
rheumatoid arthritis process. Br J Rheumatol 1997;36:990–5.
[12] Intrieri M, Calcagno G, Oriani G, Pane F, Zarilli F, Cataldo PT, et al.
Pseudouridine and 1-ribosylpyridin-4-one-3-carboxamide serum con-
centrations in human immunodeficiency virus type 1-infected patients
are independent predictors for AIDS progression. J Infect Dis
1996;174:199–203.
[13] Itoh K, Aida S, Ishiwata S, Sasaki S, Ishida N, Mizugaki M. Urinary
excretion patterns of modified nucleosides, pseudouridine and 1-
methyladenosine in healthy individuals. Clin Chim Acta 1993;
217:221–3.
[14] Mitch WE. Insights into the abnormalities of chronic renal disease
attributed to malnutrition. J Am Soc Nephrol 2002;13:S22–7.
[15] Tsujinaka T, Fujita J, Ebisui C, Yano M, Kominami E, Suzuki K,
Tanaka K, Katsume A, Ohsugi Y, Shiozaki H, Monden M. Interleukin
6 receptor antibody inhibits muscle atrophy and modulates proteolytic
systems in interleukin 6 transgenic mice. J Clin Invest 1996;197:
244–9.
[16] Starnes Jr HF, Warren RS, Jeevanandam M, Gabrilove JL, Larchian
W, Oettgen HF, et al. Tumour necrosis factor and the acute
metabolic response to tissue injury in man. J Clin Invest 1988;82:
1321–5.
[17] Kien CL, Zipf WB, Horswill CA, Denne SC, McCoy KS, O’Dorisio
TM. Effects of feeding on protein turnover in healthy children and in
children with cystic fibrosis. Am J Clin Nutr 1996;64:608–14.
[18] Shepherd RW, Holt TL, Johnson LP, Quirk P, Thomas BJ. Leucine
metabolism and body cell mass in cystic fibrosis. Nutrition 1995;
11:138–41.
[19] Li Y, Wang S, Zhong N. Simultaneous determination of Pseudouridine
and creatinine in urine of normal children and patients with leukaemia
by HPLC. Chromatography 1992;6:191–3.
[20] Gehrke CW, Kuo KC, Waalkes TP, Borek E. Patterns of urinary
excretion of modified nucleosides. Cancer Res 1979;39:1150–3.
[21] Nixon LS, Yung B, Bell SC, Elborn JS, Shale DJ. Circulating
immunoreactive Interleukin-6 in cystic fibrosis. Am J Respir Crit Care
Med 1998;157:1764–9.

A.A. Ionescu et al. / Journal of Cystic Fibrosis 3 (2004) 253–258258
[22] Ionescu AA, Nixon LS, Evans WD, Stone MD, Lewis-Jenkins V,
Chatham K, Shale DJ. Bone density, body composition and inflamma-
tory status in Cystic Fibrosis. Am J Respir Crit Care Med 2000;
162:789–94.
[23] Aris RM, Renner JB, Winders AD, Buell HE, Riggs DB, Lester GE,
Ontjes DA. Increased rate of fractures and severe kyphosis; sequelae of
living into adulthood with cystic fibrosis. Ann Intern Med
1998;128:186–93.
[24] Pouw EM, Schols AM, Deutz NE, Wouters EF. Plasma and muscle
amino acid levels in relation to REE and inflammation in stable
COPD. Am J Respir Crit Care Med 1998;158:797–801.
[25] Bell SC, Saunders MJ, Elborn JS, Shale DJ. REE and oxygen
cost of breathing in patients with cystic fibrosis. Thorax 1996;
51:126–31.
[26] Elborn JS, Cordon SM, Western P, Macdonald IA, Shale DJ. TNFa,
resting energy expenditure and cachexia in cystic fibrosis. Clin Sci
1993;85:563–8.