Embed Size (px)
Citation preview

Cellular Hypoxia in Multiple Trauma Patients
Kiki LukmanDivision of Digestive Surgery, Department of Surgery
Hasan Sadikin Hospital/Medical School of Univ. PadjadjaranBandung
Outlines
1. Problems in multiple trauma patients2. Cellular Injury3. Body responses to Injury4. Cellular responses to hypoxia5. Management of Cellular Hypoxia

Problems of trauma in Indonesia
Missed/delayed diagnosis and delayed treatment !!!!

What happens to the patients?
Multiple trauma

What is the body response to trauma?
InitialPhysiological
Condition:Homeostasis
Physiologic Response to restore
Homeostasis:Pain,
HemostasisNeuroendocrine
ReflexInflammation:
Local & SystemicMetabolics
WOUND HEALING
Tissues InjuryHemorrhage:• Hypovolemia• Hypercarbia• Hypoxia• Acidosis• Coagulopathy
Tissue EdemaVolume shift
Insult:TRAUMA
CellInjury
Organ injuries

Organ System Responses
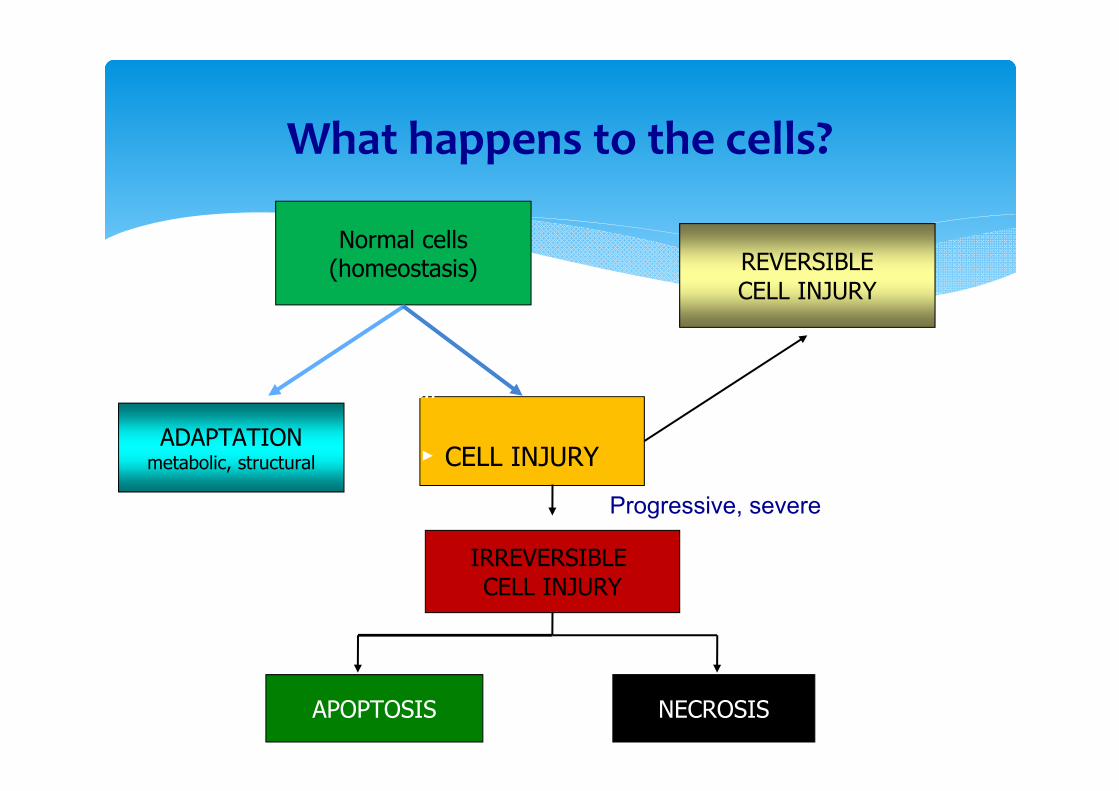
What happens to the cells?
Normal cells(homeostasis)
ADAPTATIONmetabolic, structural CELL INJURY
StressAdaptation
fails
Injuriousstimuli: dose
IRREVERSIBLE CELL INJURY
NECROSIS
REVERSIBLECELL INJURY
APOPTOSIS
Progressive, severe
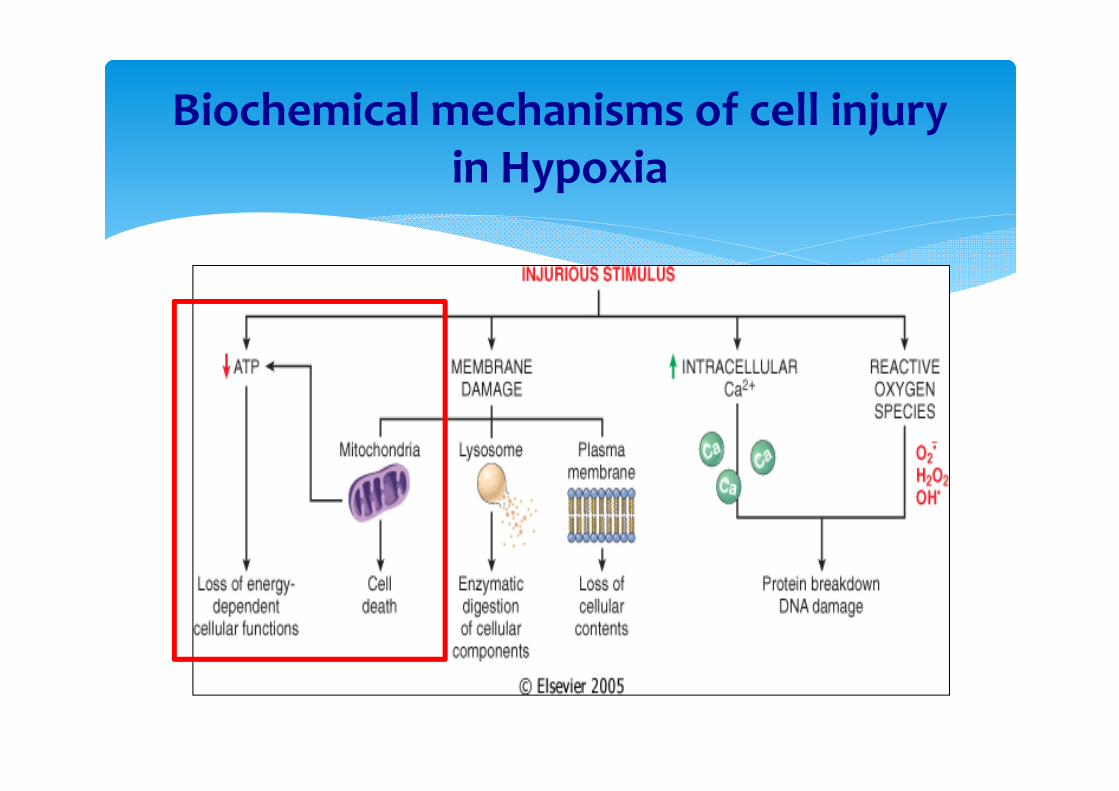
Biochemical mechanisms of cell injuryin Hypoxia

What happens in surgical source controls?
Cells
Stress Factors
Trauma Fear Major Surgery
HypoxiaHypo-perfusionInjury
PainInjuryHypoxiaischemia
Metabolic Changes
Neuro-endocrine responseInflammatory mediators

Stressors
Pain
Blood transfusion
StarvationImmobilization
Systemicinflammation Dehydration
Hypothermia
Opioids
Tissue injury
Blood loss
Anaesthesia Hypoxemia
Overhydration
Impaired tissue perfusion
Stressors in surgery

The Metabolic Stress Response to Surgery and Trauma


How to assess?OxygenationMonitoring
LUNGS
BLOOD
TISSUES

P / F (PF ratio)
The ratio between PaO2 (mmHg) and FiO2 (decimal). (Need BGA !!!)
Normal ratio: > 300 (300 – 500).
Clinical Significance:Showing the degree of O2 diffusion in the alveolar-capillary unit. < 200 : ARDS (acute respiratory distress syndrome).200 – 300 : ALI (acute lung injury).
A-a gradient (AaDO2)
O2 partial pressure different between the alveoli and artery (PAO2 – PaO2).
Formula (Clinical use) :AaDO2 = PiO2 – PaCO2/R – PaO2
R=respiratory quotient= 0.8

Normal Values
Room Temperatures (FiO2: 21%) :< 10 mmHg (young) 10-20 mmHg (elderly)
at FiO2 100% :31 mmHg (young)56 mmHg (elderly).

Purpose
To know the causes of hypoxemia :AaDO2 normal : hypoventilationAaDO2 abnormal :
Gas diffusion dysfunction VA/Q dysfunctionshunting

Blood Oxygen Content
Ca O2 = 1,34 x Hb x SaO2 + 0,003 x PaO2
To monitor:
SaO2
PaO2

SaO2 (Oxygen Saturation)
Showing the Hb capacity to bind O2.SaO2 : arterialSpO2 : by pulse oximetry0% : No O2
100% : saturated with O2

(SaO2)

PULSE Oximetry SpO2

SaO2 vs SpO2 Correlation
1. SpO2 > SaO2:1. Hypoxemia2. Carboxyhemoglobinemia3. Methemoglobinemia4. Sickle cell crises5. Skin pigmentation6. Bright overhead fluorescent light7. Probe malposition

1. SpO2 < SaO2:1. Intravenous dye (meth.blue, indigo carmine)2. Nail polish3. Chylomycron, intravenous lipid
2. Inaccurate reading.1. Low perfusion2. Shivering3. Motion artefacts
SaO2 vs SpO2 Correlation

Etiology of SaO2 (SpO2) ↓
1. Respiratory problems1. Airway2. Ventilation3. Diffusion problems in alveolar-capillary unit
2. Circulatory System Problems (preload, contractility, HR, afterload)
3. FiO2 <4. Installation and Device problems

PaO2 (Oxygen partial pressure in the blood)
Normal : Average value : PaO2 = 5 x FiO2 (%)
( 80 – 100 mmHg ) Age adjusted : 100 – 0,3 { umur (th) – 25 }
Low : - HYPOXEMIA – Mild: 60- 80 mmHg Moderate : 40- 60 mmHg Severe: < 40 mmHg

HYPOXEMIA
Causes:
FiO2 < Hypoventilation Shunt Ventilation-perfusion mismatch O2 diffusion dysfunction alveoli-capillary.

PAO2 < 80 (104 mmHg)
PACO2=40 mmHg
75% 100%
FiO2 <

How to manage?
TISSUE OXYGENATION
Target: To meet the needs of tissue oxygen
How to know?

StO2
Cell Monitoring

StO2

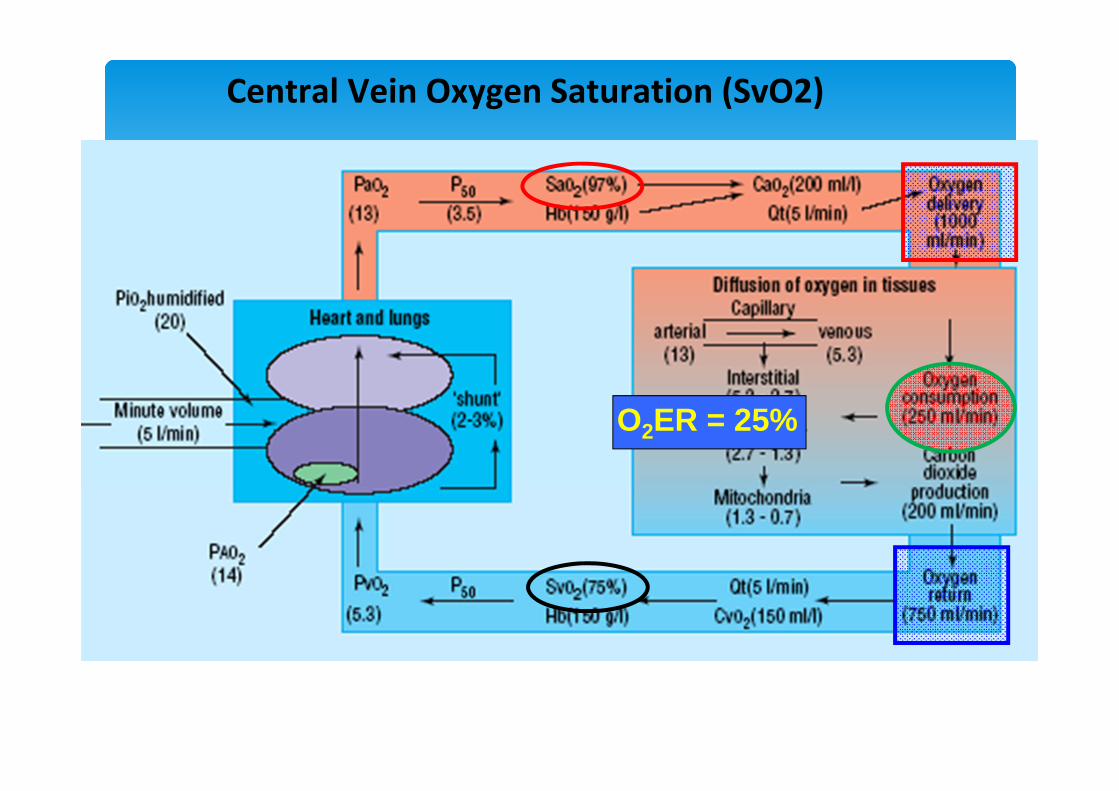
O2ER = 25%
Central Vein Oxygen Saturation (SvO2)
1 Kpa ~ 8 mmHg

The meaning of Svs O2
SvsO2 < 75 % (PvO2 < 42,8 mmHg) :1. DO2 ↓ :
Anemia, hypovolaemia, cardiogenic shock, hypoxemia, R - L shunting, ventilation –perfusion dysfunction.
2. Oxygen need ↑ :Febrile, convulsion, shivering, pain, activity ↑,
hyperthyroidism.
SvsO2 = 75 - 80% (PvO2 = 42 - 44 mmHg):Normal DO2 & O2 consumpti
SvsO2 > 80% (PvO2 > 44 mmHg) :
DO2 ↑ : Cardiac output ↑,L – R shunting, hiyperbaric O2, FiO2 ↑, sepsis.
Oxygen need ↓ :Hypothermia, general anesthesia, neuromuscular block drugs, hypothyroidism, cell necrosis.
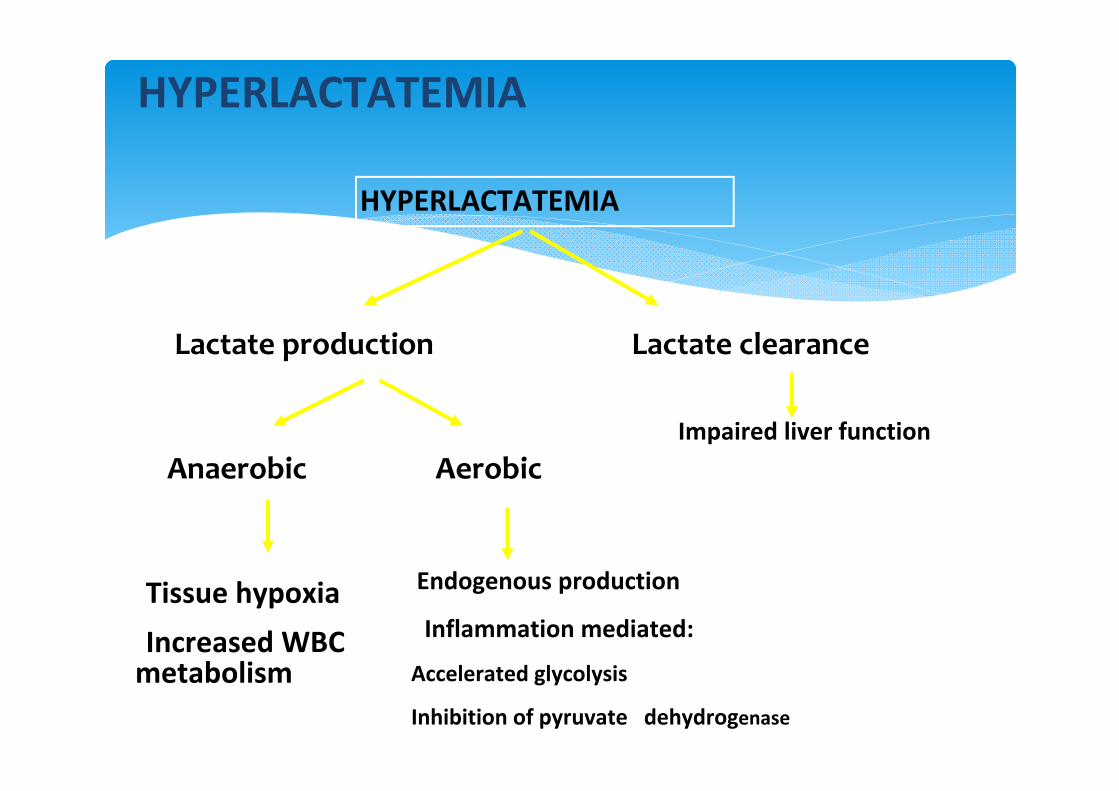
HYPERLACTATEMIA
Lactate production Lactate clearance
Anaerobic Aerobic
•Tissue hypoxia•Increased WBC metabolism
• Endogenous production
• Inflammation mediated:
•Accelerated glycolysis
•Inhibition of pyruvate dehydrogenase
• Impaired liver function
HYPERLACTATEMIA


BASE DEFICIT / EXCESS (BD/E)
The amount of acid/base needed to normalize 1L blood (SBC = standard bicarbonate concentration : 22,9 mEq/L ), t : 37oC & PaCO2 : 40 mmHg.
• Classification : Mild : 2 – 5 mmol / L• Moderate : 6 – 14 mmol /L• Severe : > 15 mmol / L

Lactate & Base Deficit Correlation
Husain et al Am J Surg 2003: 185: 485-491

Correlation: Base Deficit & Mortality
Rixen and Siegel , Critical Care 2005 Vol 9 No 5
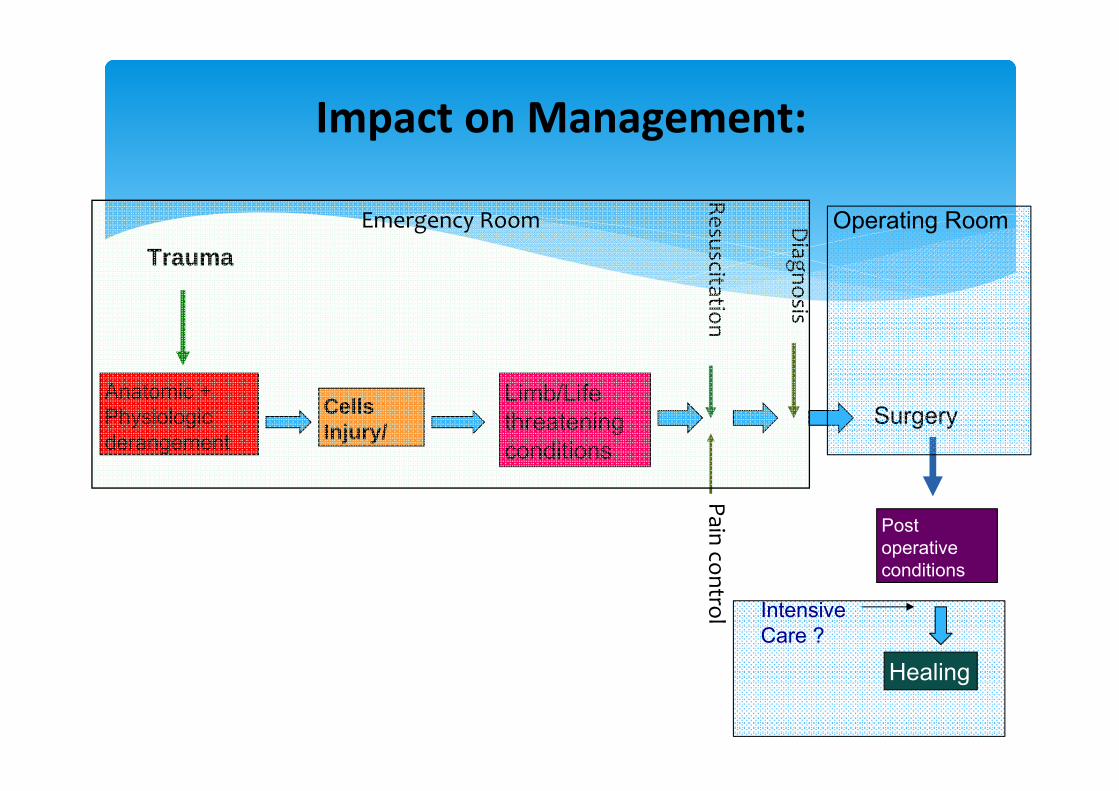
Impact on Management:
Trauma
Limb/Life threatening conditions
Resuscitation
Post operative conditions
Anatomic + Physiologic derangement
Cells Injury/
Diagnosis
Surgery
Intensive Care ?
Healing
Operating Room
Pain control
Emergency Room
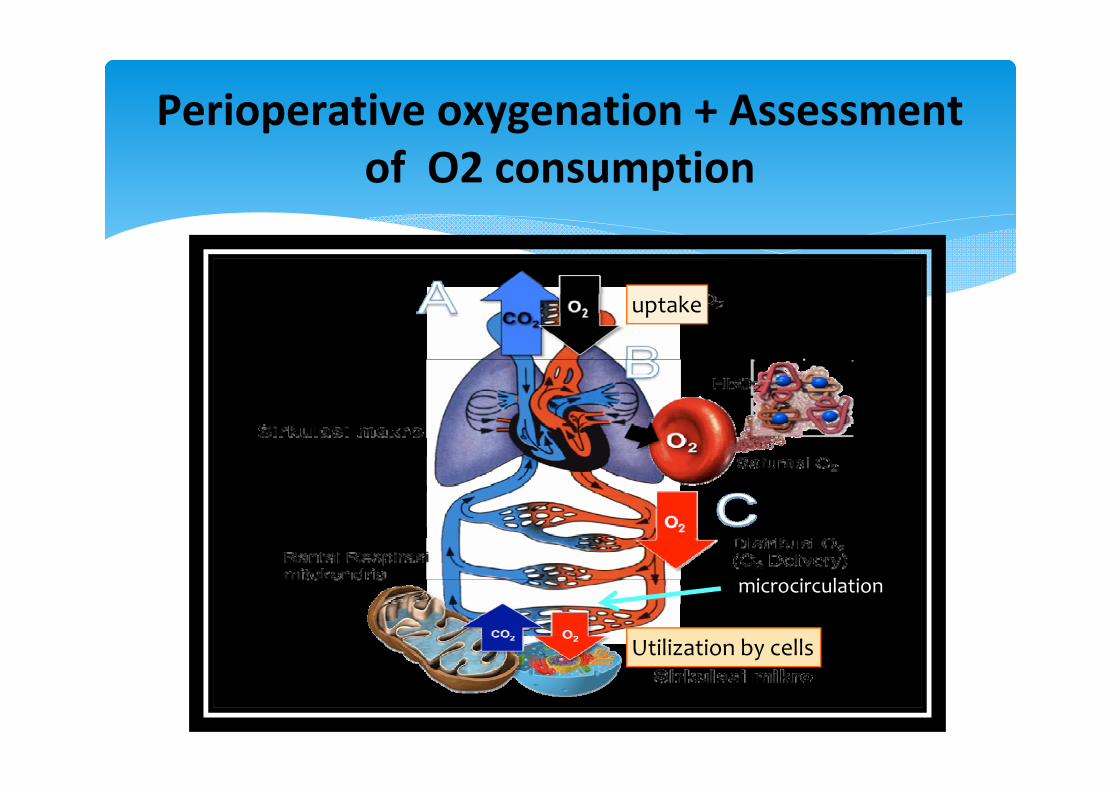
Perioperative oxygenation + Assessmentof O2 consumption
uptake
Utilization by cells
microcirculation

SUMMARY
1. Cellular hypoxia is the initial event of MODS in trauma patients, if left untreated, may lead to MOF.
2. The duration of cellular hypoxia is correlated with the patient outcome.
3. Prolonged cellular hypoxia leads to irreversible cell injury and cell death.
4. The mainstay of the treatment of cellular hypoxia is cell oxygenation, not only by oxygen administration, but also by ensuring oxygen delivery into microcirculation.