Embed Size (px)
Citation preview

登革熱登革出血熱屈公病診斷與治療
疾病管制署
洪敏南醫師
20140510
1
登革熱(Dengue fever)
bull 由蚊子傳播的急性病毒性熱疾
ndash 埃及斑蚊Aedes aegypti
ndash 白線斑蚊Aedes albopictus
bull 以高熱頭部肌肉骨頭關節的奇痛後眼窩痛以及發疹為主要症狀
2
登革熱通報定義
bull 突發發燒≧38且伴隨下列二(含)種以上症狀
1 頭痛
2 後眼窩痛
3 肌肉痛
4 關節痛
5 出疹
6 出血性癥候(hemorrhagic manifestations)
7 白血球減少(leukopenia)
3
屈公病通報定義
bull 臨床條件ndash 急性發燒≧38degC 且有嚴重關節炎或關節痛無法以其他醫學診斷解釋者
bull 流行病學條件 (具有下列任一個條件)ndash (一)住家或活動範圍附近有屈公病確定病例或有與屈公病確定病例接觸史
ndash (二)有屈公病流行地區相關旅遊史
bull 通報定義ndash 符合臨床條件及流行病學條件
4
5Clinical Infectious Diseases 2009 49942ndash8
6
Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Haemorrhagic Fever WHO 2011
7
8
9Handbook for clinical management of dengue WHO 2012
Potential Clinical Issues by Phase (days post fever onset)
bull Febrile phase ndash Dehydration
ndash Febrile seizures
ndash Neurologic manifestations
bull Critical phase ndash Prolonged shock
ndash Organs impaired
ndash Bleeding
bull Recovery phasendash Fluid overload
ndash Worsening effusions
ndash Acute pulmonary edema
10
11
整體評估
bull 鑑別診斷
bull 詢問居住地活動史與接觸史 (TOCC)
bull 要想到登革感染的可能性
bull 發燒初期的血比容值Hct可以當作此病患Hct的基礎值
bull 白血球與血小板下降暗示可能為登革感染
bull 利用止血帶試驗協助診斷
bull 完整的衛教(含回家後應注意事項)
12
WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

登革熱通報定義
bull 突發發燒≧38且伴隨下列二(含)種以上症狀
1 頭痛
2 後眼窩痛
3 肌肉痛
4 關節痛
5 出疹
6 出血性癥候(hemorrhagic manifestations)
7 白血球減少(leukopenia)
3
屈公病通報定義
bull 臨床條件ndash 急性發燒≧38degC 且有嚴重關節炎或關節痛無法以其他醫學診斷解釋者
bull 流行病學條件 (具有下列任一個條件)ndash (一)住家或活動範圍附近有屈公病確定病例或有與屈公病確定病例接觸史
ndash (二)有屈公病流行地區相關旅遊史
bull 通報定義ndash 符合臨床條件及流行病學條件
4
5Clinical Infectious Diseases 2009 49942ndash8
6
Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Haemorrhagic Fever WHO 2011
7
8
9Handbook for clinical management of dengue WHO 2012
Potential Clinical Issues by Phase (days post fever onset)
bull Febrile phase ndash Dehydration
ndash Febrile seizures
ndash Neurologic manifestations
bull Critical phase ndash Prolonged shock
ndash Organs impaired
ndash Bleeding
bull Recovery phasendash Fluid overload
ndash Worsening effusions
ndash Acute pulmonary edema
10
11
整體評估
bull 鑑別診斷
bull 詢問居住地活動史與接觸史 (TOCC)
bull 要想到登革感染的可能性
bull 發燒初期的血比容值Hct可以當作此病患Hct的基礎值
bull 白血球與血小板下降暗示可能為登革感染
bull 利用止血帶試驗協助診斷
bull 完整的衛教(含回家後應注意事項)
12
WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

5Clinical Infectious Diseases 2009 49942ndash8
6
Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Haemorrhagic Fever WHO 2011
7
8
9Handbook for clinical management of dengue WHO 2012
Potential Clinical Issues by Phase (days post fever onset)
bull Febrile phase ndash Dehydration
ndash Febrile seizures
ndash Neurologic manifestations
bull Critical phase ndash Prolonged shock
ndash Organs impaired
ndash Bleeding
bull Recovery phasendash Fluid overload
ndash Worsening effusions
ndash Acute pulmonary edema
10
11
整體評估
bull 鑑別診斷
bull 詢問居住地活動史與接觸史 (TOCC)
bull 要想到登革感染的可能性
bull 發燒初期的血比容值Hct可以當作此病患Hct的基礎值
bull 白血球與血小板下降暗示可能為登革感染
bull 利用止血帶試驗協助診斷
bull 完整的衛教(含回家後應注意事項)
12
WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

7
8
9Handbook for clinical management of dengue WHO 2012
Potential Clinical Issues by Phase (days post fever onset)
bull Febrile phase ndash Dehydration
ndash Febrile seizures
ndash Neurologic manifestations
bull Critical phase ndash Prolonged shock
ndash Organs impaired
ndash Bleeding
bull Recovery phasendash Fluid overload
ndash Worsening effusions
ndash Acute pulmonary edema
10
11
整體評估
bull 鑑別診斷
bull 詢問居住地活動史與接觸史 (TOCC)
bull 要想到登革感染的可能性
bull 發燒初期的血比容值Hct可以當作此病患Hct的基礎值
bull 白血球與血小板下降暗示可能為登革感染
bull 利用止血帶試驗協助診斷
bull 完整的衛教(含回家後應注意事項)
12
WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
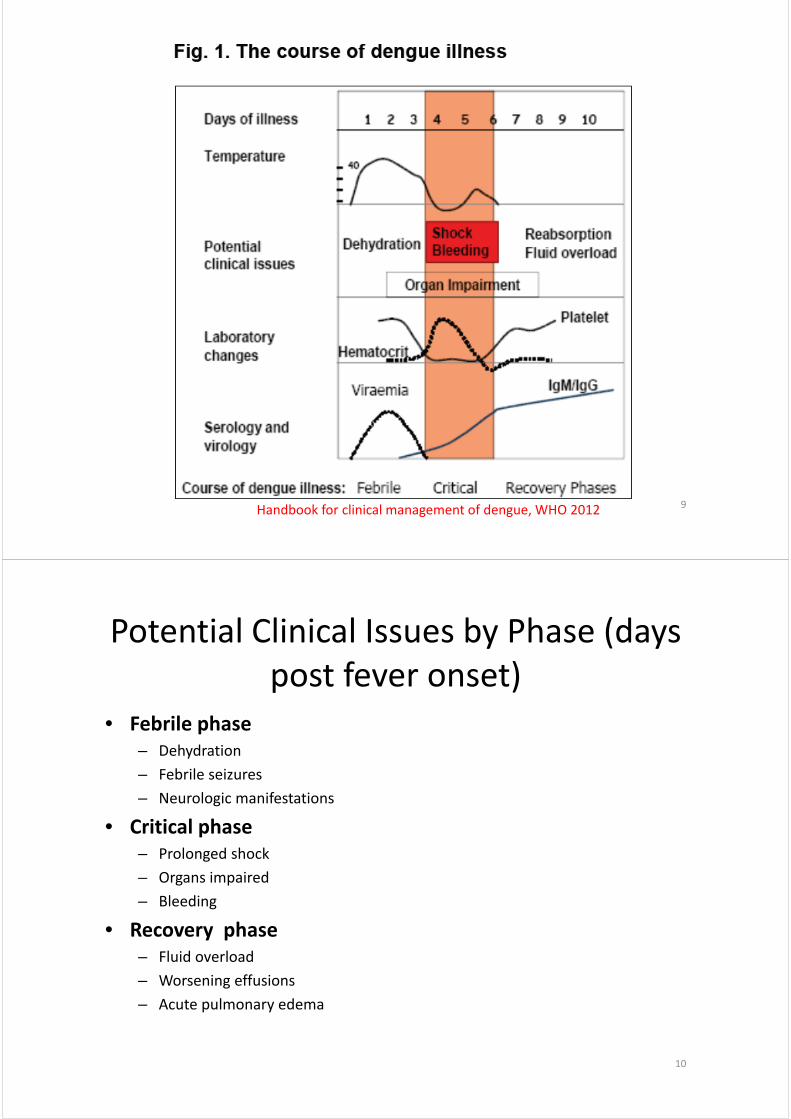
9Handbook for clinical management of dengue WHO 2012
Potential Clinical Issues by Phase (days post fever onset)
bull Febrile phase ndash Dehydration
ndash Febrile seizures
ndash Neurologic manifestations
bull Critical phase ndash Prolonged shock
ndash Organs impaired
ndash Bleeding
bull Recovery phasendash Fluid overload
ndash Worsening effusions
ndash Acute pulmonary edema
10
11
整體評估
bull 鑑別診斷
bull 詢問居住地活動史與接觸史 (TOCC)
bull 要想到登革感染的可能性
bull 發燒初期的血比容值Hct可以當作此病患Hct的基礎值
bull 白血球與血小板下降暗示可能為登革感染
bull 利用止血帶試驗協助診斷
bull 完整的衛教(含回家後應注意事項)
12
WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

11
整體評估
bull 鑑別診斷
bull 詢問居住地活動史與接觸史 (TOCC)
bull 要想到登革感染的可能性
bull 發燒初期的血比容值Hct可以當作此病患Hct的基礎值
bull 白血球與血小板下降暗示可能為登革感染
bull 利用止血帶試驗協助診斷
bull 完整的衛教(含回家後應注意事項)
12
WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

WHO (1997) Dengue Haemorrhagic Fever Diagnosis Treatment Prevention and Control 2nd ed
13
The Atlas of Emergency Medicine gt Chapter 21
類似快篩
14
bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

bull 具有以下特質的病患ndash 有警示徵象
ndash 有共病症 (如懷孕嬰幼兒老年人肥胖糖尿病高血壓心衰竭腎衰竭慢性溶血性疾病)
ndash 特定的社經因子
15
何謂 Vital signs ldquostable
bull 要養成親自接觸每個病患(無論是否為登革病人)並且評估病患週邊灌流的習慣
bull Level of consciousness (Use GCS) bull Capillary refill bull Skin temperature color and moisture level (normal
dry or clammy) bull Peripheral pulse volumebull Heart rate
ndash 發燒期心搏過速與肢體冰冷代表
bull Blood pressurendash Not match with the expectations ndash Definition of hypotension
bull Respiratory rate bull Urine output
16
登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

登革病患出現腹痛
bull 腹痛是血漿滲出的早期徵象而且當低血容進展時腹痛也會惡化
bull 也許是上腹痛合併嘔吐因此常被誤診為單純的胃炎而只考慮給予抗腸痙攣劑或制酸劑
bull 如何鑑別ndash 要注意病史如之前有發燒但退燒後反而出現腸胃道症狀如噁心嘔吐腹瀉甚至解黑便等此時應該想到可能是登革感染的警示徵象甚至病患已經呈現休克
ndash 如果經過單純的輸液治療 (5minus10 mlkg over 1 hour)腹痛已減緩暗示外科急症的可能性不大
ndash 大量輸液治療24小時後仍有持續或惡化的腹痛表示是即將發生休克的危險徵兆嗎
17
Case studies
18
Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Case 1
bull 76歲女性
bull 高血壓病史
bull 居住地屏東市長春里號
bull 20131011早上被發現不省人事
bull At ER ndash TPR=36211820
ndash Lab CBC=68KHct=412PLT=25KASTALT=21796
ndash Brain CT severe SDH
19
Case 2
bull 40 歲女性於 2009130 (D1)至急診
bull 主述
ndash 130開始發燒
ndash 伴隨發冷咳白痰呼吸困難喉嚨痛頭痛頸部痠痛雙側膝關節腕關節與踝關節疼痛
ndash 痛到無法行走且背部出現疹子
bull 從馬來西亞回國 (122~130)
20
bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

bull At ER (D1)
ndash TPR=3829720 BP=11055
ndash Lab Hct=393 WBC=4K Neu=86 PLT=139K ALTAST=1220
ndash PE conjunctivitis (+) tenderness over bil ankles and knees skin rash on back (+)
bull Admission
ndash Tentative Dx dengue Flu Chikungunya
ndash Give doxycycline
ndash fu lab WBC=138K PLT=111K afebrile 4 days later
21
Kaohsiung J Med Sci 201026256‐60
Case 3
bull 64 歲男性20111016凌晨4點至急診主述為自昨日起有發燒骨頭痠痛 (D1=1015) ndash 住在東港ndash 有慢性腎病與痛風史ndash BW=78Kg(IBW=60Kg)
bull At ERndash TPR=388319 BP=13886ndash Lab Hb=97 PLT=121K WBC WNL Seg=78 Cr=73ndash Give Keto 1 amp + NS 250ml
bull MBD (11 AM) ndash Dx URIpharyngitisndash Prescription panadal keflex and peace x 3 days
22
Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Revisit ER 3 days later
bull Revisit ER on 7AM 1019 ( D5)
bull CC SOB and chest discomfort for 2 daysndash TPR=37410324 BP=11694
ndash Muscle soreness(+) low grade fever(+) abd pain (+) deny URI symptoms or rash
ndash Lab WBC=75K Hb=15 PLT=37K ALT=73BunCre=12110 ABG=73222263113INR=115 aPTT=394
bull Admission at 11 AMndash Abd echo ascites (+) CXR bil lower lung infiltrate(+) cardiomegaly(+)
ndash Impression DF + thrombocytopenia acute on CKD
23
24
Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Case 4
bull 70歲男性於2011115傍晚七點至急診bull 主述
ndash 發燒三天 食慾不振 解黑便ndash 住鳳山ndash HTN DM (+)
bull At ER ( D3=115)ndash TPR=36910320 BP=161103ndash Lab WBC=561KHb=166 Hct=494 PLT=44KBunCre=2511ALT=115
bull MBD at 11 PMndash Dx 1 fever cause 2 ro UGIB thrombocytopenia
25
Revisit ER next day
bull At ER 7 PM 116 (D4) due to generalized weaknessndash TPR=36813720 BP=9265ndash Lab WBC=614kHb=144Hct=434PLT=16KASTALT=353242Glu=418
ndash sp BT with PLT arrange PES
bull At ER (117)ndash 5AM BT=38 tarry stool BP=9363ndash 6AM WBC=767K Hb=107 Hct=322 PLT=17K sp BT with PRBC PLT FFP
ndash 12 AM SBP=40ndash 4AM skin rash (D5) noted notify denguendash 9PM AAD
26
27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

27
Case 5
bull 24 歲女性 2012824 至急診因為ndash 發燒三天 肌肉痛與虛弱 for 2 days and tea color urine 1 day
bull At ER ( 1500 )ndash BW=64Kg BH=158cm
ndash TPR=3611020 BP=10050
ndash Epigastric pain(+) Murphyrsquos sign (+)
bull GS re‐took Hx ndash epigastric pain for 5 days with worsening abd pain vomiting many times abd soft no guarding
28
bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

bull 初步診斷 UTI acute cholecystitisndash Plan 轉內科並且安排腹超
bull 內科醫師問診 at 1630ndash fever onset on 819 (D1) also had vomiting malaise transient rash intense abd pain on 824 (D6)
ndash TP=36120 BP=10080ndash Petechiae over lower limbs(+) weak pulse ndash Revise Dx
29
Lesson learnt
bull It is not uncommon for dengue to be misdiagnosed at various phases of the disease coursendash Viral hepatitis vs jaundice in dengue
ndash ldquoAcute abdomenrdquo if fever bull an important warning sign of severe dengue
bull acalculous cholecystitis
ndash Polycythemia vs haemoconcentration
bull 仔細問診親自評估病患早期察覺休克
30
31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

31
Take Home Message
bull 要想到登革感染
bull 要確認疾病進程
bull 要避免特定藥物
bull 要嚴密監控病況
bull 要補充適當輸液
bull 要考慮出血可能
32
謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

謝謝聆聽
敬請指教
33
20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

20140510
2013-2-21 OO
OO OO
Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Outline
90
WHO 10 facts on malaria
Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Yellow Book 2013 US CDC
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
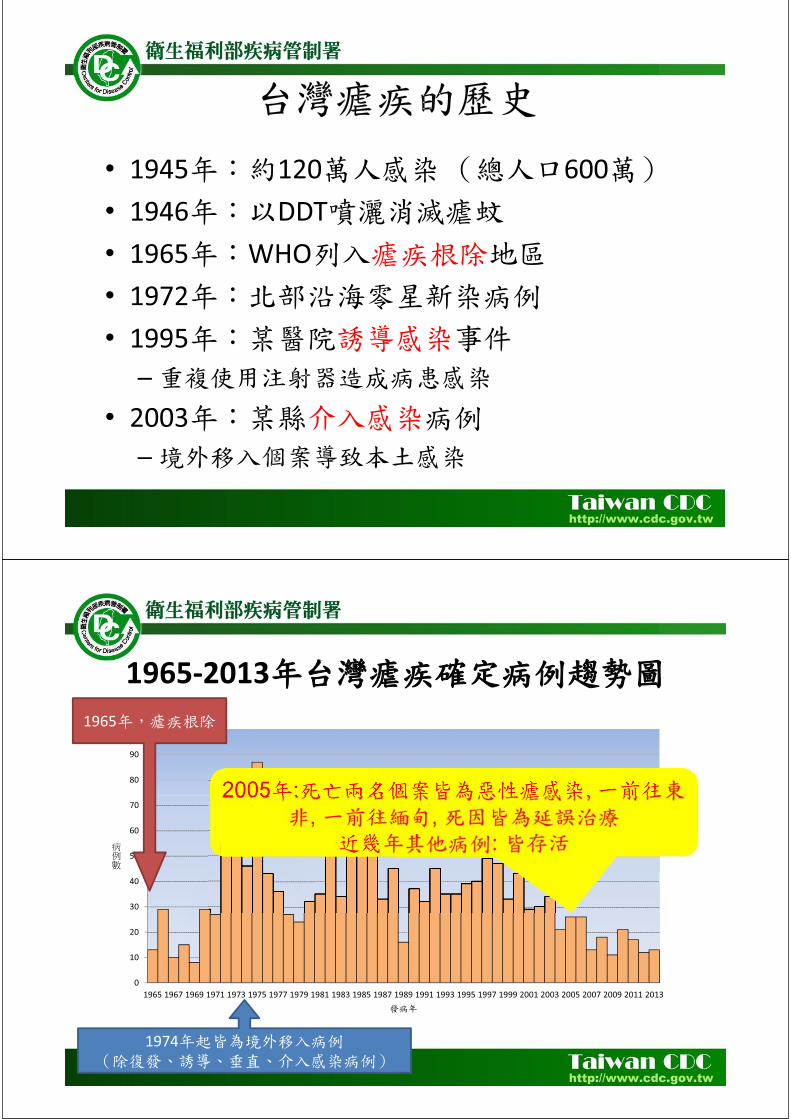
1945 120 600 1946 DDT 1965 WHO 1972 1995
2003
1965-2013
0
10
20
30
40
50
60
70
80
90
100
1965 1967 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013
1965
1974
2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

2009-2013
2009 2010 2011 2012 2013 6 15 9 8 7 45
2 3 2 7 2 4 6 1 3 2 6 1 1 2 4
2 2 1 1 2
1 1 1 1
11 21 17 12 13 74
2009-2013 2009 2010 2011 2012 2013
2 5 3 1 11 1 2 2 2 3 10 1 4 1 1 7
2 1 1 1 1 6 1 1 3 1 6 1 1 1 1 4 1 1 1 3
1 1 1 3 3 3
Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Plasmodium falciparum P vivax P ovale P malariae
()
Dennis L Kasper 2005
2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

2009-2013
+
2009 2010 2011 2012 2013
4 10 12 6 7 39 (52)
1 4 0 5 2 12 (17)
6 7 5 1 4 23 (31)
11 21 17 12 13 74
5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

5-6 8 9 13
48 48 49-50 72
12 13-17 13-17 28-30
420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

420 40
(Anopheles minimus)
7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

7-30 2 3
( 6 10 )
(15 1 )
(2 6 ) (2 4 )
1
2 3
4
( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

( )
11
Severe malaria
10
Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Disconjugate gaze
Decerebrate rigidity
Management of severe malaria a practical handbook WHO 2000
A B C
Management of severe malaria a practical handbook WHO 2000
A
C
B
Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Management of severe malaria a practical handbook WHO 2000
Gold Standard
10-15 100
PCR
5
4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

4-6
( )
2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

2010
hydroxychloroquine
Artemisinin-based combination therapy (ACT)
WHO
Artequin 6001500 Artesunate 3 tabs + mefloquine 6 tabs
quinine + (doxycyline tetracycline or clindamycin) x 7 days
P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

P malariae hydroxychloroquine P vivax P ovale hydroxychloroquine
primaquine (025 mgkg) x 14 days
P vivax ACT + primaquine (
)
24
Artesunate (60mg) 24mgkg stat and q12h2 dose then qd 6 days (made in China)
Quinine (60mg) 20mgkg stat then 10mgkg q8h 7 days ( )
Quinine artemisinin
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
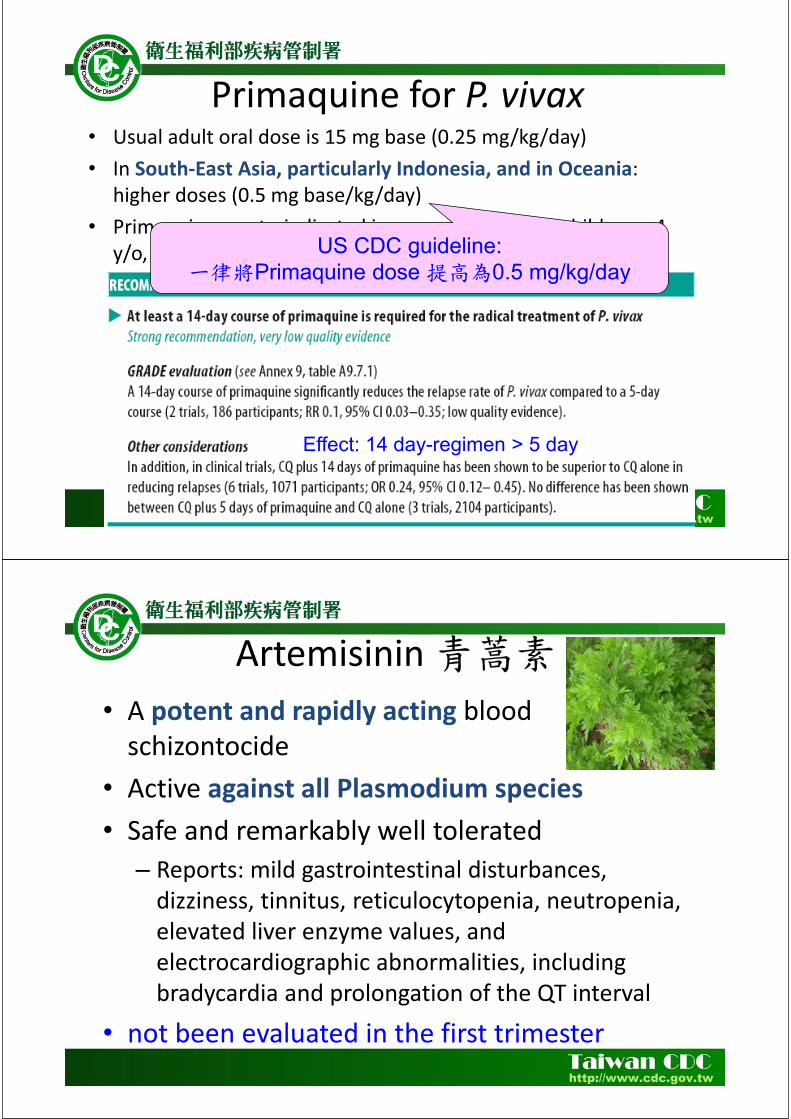
Primaquine for P vivax Usual adult oral dose is 15 mg base (025 mgkgday) In South-East Asia particularly Indonesia and in Oceania higher doses (05 mg basekgday) Primaquine contraindicated in pregnant women children lt 4 yo lactating woman
Effect 14 day-regimen gt 5 day
US CDC guideline Primaquine dose 05 mgkgday
Artemisinin
A potent and rapidly acting blood schizontocide Active against all Plasmodium species Safe and remarkably well tolerated
Reports mild gastrointestinal disturbances dizziness tinnitus reticulocytopenia neutropenia elevated liver enzyme values and electrocardiographic abnormalities including bradycardia and prolongation of the QT interval
not been evaluated in the first trimester
Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Artemisinin Resistance in the Greater Mekong subregion
2014 WHO Status Report on Artemisinin Resistance
Tier maps of the Grater Mekong
subregion
2014 WHO Status Report on Artemisinin Resistance
48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

48 25
(recrudescence) ( )
(wwwcdcgovtw)
Mefloquine Doxycycline
Malarone 100
NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

NEJM 2008359 603-612
2010
2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

2011 Available at httppptccnLxk
Distribution of Chloroquine- Resistant P falciparum
Yellow Book 2012 US CDC
Distribution of Mefloquine-
Resistant Malaria in the
Grater Mekong subregion
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
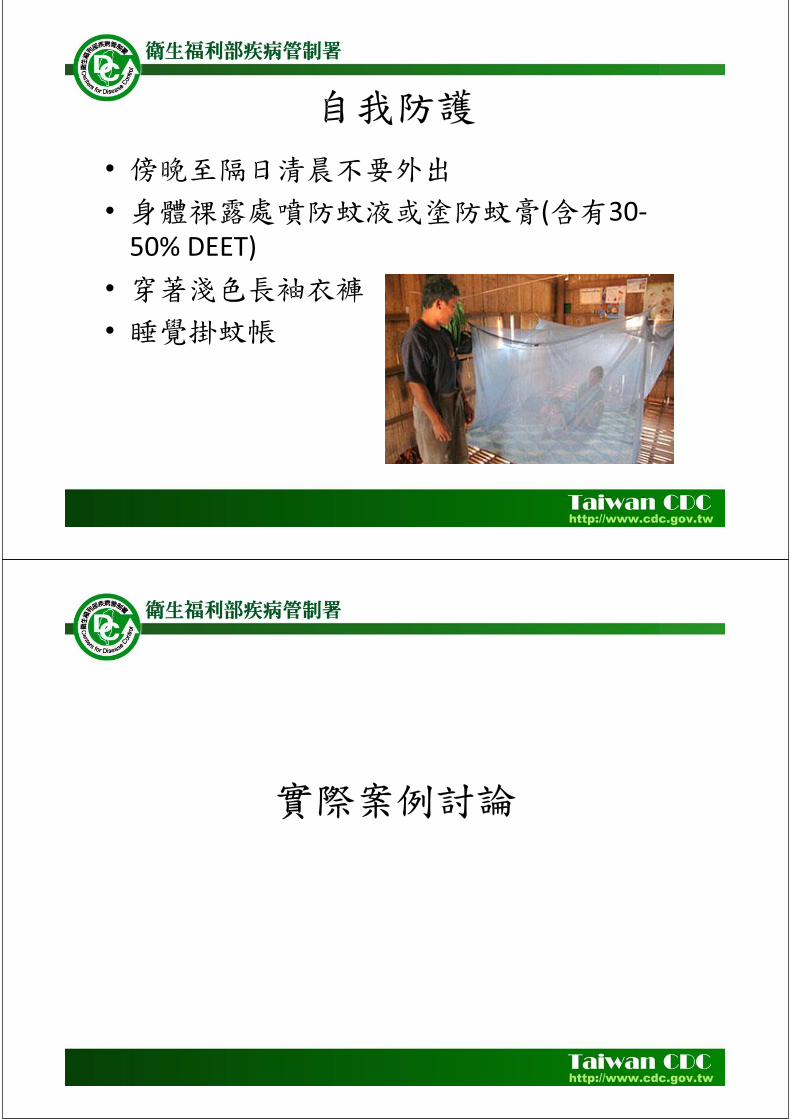
( 30-50 DEET)
29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

29
2010222-223 223-226 227
315
318
PCR ( + )
38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

38 93
66
2008823-1015 2008915-1030
20081015 1031
49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

49
2008117-128
2008417
619 1121
2009 9 50 FRIM Forest Research Institute Malaysia) 9
2009123 P vivax
- 56 yo
2009 3
Mefloquine
hydroxychloroquine
Schizont( ) progress
46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

46 201045-418
(hydroxychloroquine) 425 428 429
428 hydroxychloroquine
-
THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

THANK YOU FOR YOUR ATTENTION
日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

日本腦炎恙蟲病之診斷與治療
高雄市立小港醫院
(委託高雄醫學大學經營) 感染管制室 主任
張科
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
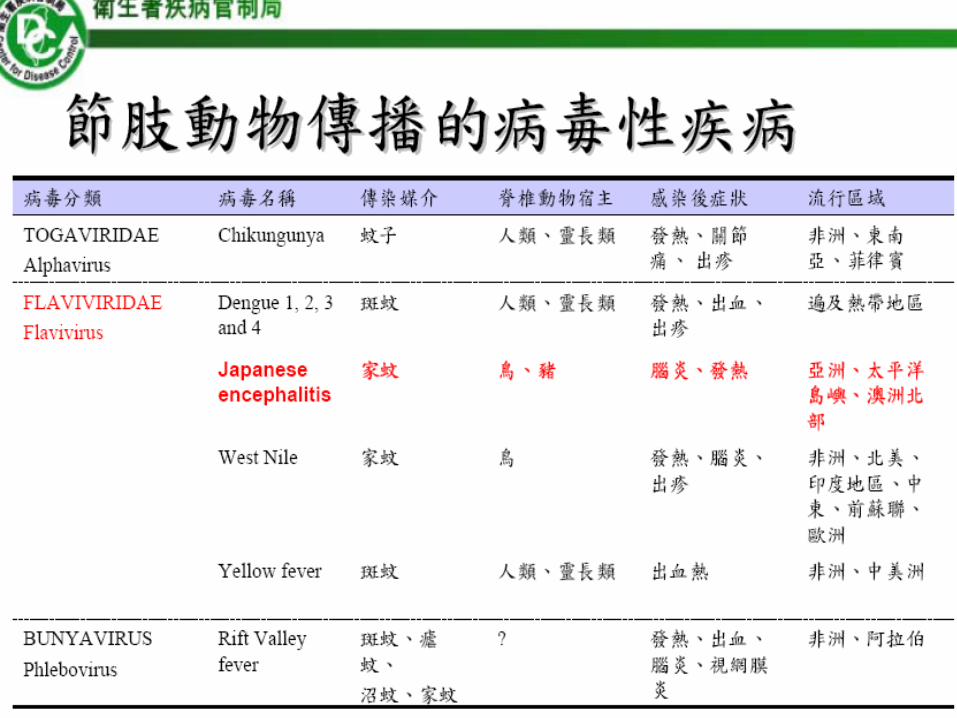
Figure 1 Global distribution pattern of Japanese encephalitis The areas shaded in yellow are Japanese encephalitis
risk-prone regions The areas encircled in red such as Karachi (Pakistan) and Torres Strait islands (Australia) and
parts of the northern Australian mainland are newer areas affected by Japanese encephalitis
Kaushik Bharati httpwwwantimicrobeorgmid
Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Year Incident
1871 First recorded clinical case of JE reported from Japan
1924 Large outbreak of JE in Japan with gt6000 cases and a fatality rate
of 60 Isolation of JEV from human brain
1933 First cases of JE reported from the Korean peninsula
1935 Isolation of Nakayama strain of JEV
1938 Isolation of JEV from Culex tritaeniorhynchus mosquitoes
1940 First cases of JE reported from the Chinese Mainland
1950 First cases of JE reported from the Philippines
1950s Elucidation of transmission cycle of JEV with pigs and ardeid birds
identified as amplifying hosts and Culex tritaeniorhynchus as
primary vector species
1955 First cases of JE reported from Vellore India
1965 Major epidemic in northern Vietnam
1969 and 1970 Major epidemic in Chiang Mai Valley Thailand
1973 First epidemic in India in the state of West Bengal
1978 Major epidemic in Terai region of Nepal
1983 JE reaches Pakistan the furthest geographical extension to the West
1985-86 and
1987
Major epidemics in Sri Lanka
1995 JE reaches Papua New Guinea and Torres Strait islands (Australia)
the furthest geographical extension to the South
2005 Major epidemic in Gorakhpur Uttar Pradesh state of India 5737
cases with 1344 deaths
India imports live-attenuated SA 14-14-2 vaccine from China
Table 1 Japanese Encephalitis An Historical Timeline
日本腦炎
bull 1924年在日本爆發大流行
bull 1938年日本學者
得知經由蚊蟲為媒介
而傳染
bull 1956年發展出不活性的
疫苗
bull 臺灣地區每年都
有日本腦炎病例發生
流行地區遍部全省
日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

日本腦炎
bull All world
bull Approximately 35000-50000 people
suffer from JE every year with a
mortality rate of 10000-15000 people
per year China still accounts for 50 of
the reported JE cases worldwide
bull Zheng Y Rev Med Virol 2012 Mar 8
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12
male
female
Male 239 cases
Female153 cases
台北區 合計
55
北區 合計 34
中區 合計 91
南區 合計 89
高屏區 合計
80
東區 合計 43
Japanese encephalitis cases
from 1998 to Feb2013 in Taiwan
httpwwwcdcgovtw
0
10
20
30
40
50
60
70
80
90
100
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

2012年5月
bull 高雄市出現首例本土型日本腦炎病例籲請市民提高警覺
bull 高雄市出現今年(2011)首例本土型日本腦炎確定病例個案為64歲男性美國人居住於高雄市大寮區患者於5月16日開始出現頭痛發燒全身無力等症狀5月19日出現行動及反應遲緩5月20日因意識混亂由友人護送至市立聯合醫院急診求治並由醫院通報為日本腦炎疑似個案採檢送驗6月5日經行政院衛生署疾病管制局綜合研判結果為陽性該患者於5月26日因出現呼吸急促等危急症狀已由醫師給予插管呼吸器輔助呼吸目前意識狀況呈現昏迷昏迷指數約7分持續於加護病房加強照護中
疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

疫情調查
bull 經環境調查該名個案居住地點周邊有大量雜草叢生的空地防疫人員在空地內側隱密處查獲民眾飼養豬支豬圈舍前方即為水池現場亦捕獲數隻斑蚊與家蚊整體衛生環境條件不良是十分有利傳播日本腦炎的病媒蚊-三斑家蚊孳生的環境
大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

大寮戰區防治作為
本府衛生局已依傳染病防治法對國防部總政治作戰局及國有財產局權管之影劇七新村病媒蚊孳生源開出舉發通知書
臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

臨床症狀
bull 患者通常在經過5~15天的潛伏期後出現臨床症狀其典型的病程演進可分為四個時期 ndash 前驅期 (2~3天)
bull 前驅症狀發作快主要出現頭痛噁心嘔吐食慾不振精神不安發燒或輕微呼吸道感染症狀
ndash 急性期 (3~4天) bull 高燒部份兒童呈現抽筋症狀頸部僵硬四肢僵硬深部及淺部反射異常震顫言語困難神智不清對人時地不能辨別甚至昏迷或死亡
ndash 亞急性期 (7~10天) bull 中樞神經的侵犯較緩部分病例仍有生命危險
ndash 恢復期 (4~7週) bull 大部分存活病例的神經功能缺損仍存在其中包括四肢僵硬無力腦神經及錐體外徑路的異常
病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

病媒蚊 在台灣傳播日本腦炎之病媒蚊
bull 三斑家蚊環紋家蚊
孳生於
ndash 水稻田
ndash 灌溉溝渠
ndash 地上小水池
ndash 牛足印
ndash 水泥槽
ndash 池塘
ndash 溪流
ndash 濕地
ndash 人工容器
bull 白頭家蚊
孳生於
ndash 濕地
ndash 溪流
ndash 臨時性積水漥地
潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

潛伏期與可傳染期
bull 潛伏期
ndash 5 ~ 15天
bull 可傳染期
ndash 人不會經由人直接傳染給人
ndash 蚊子一旦被感染則終生具感染力
ndash 豬及鳥類的病毒血症期通常為2~5天
bull 感染性及抵抗力
ndash 通常小孩及老人感染後較容易發生臨床症狀其他年齡層則較多不顯性感染
病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

病例定義
bull 臨床病例
ndash 出現下列急性神經症狀發燒意識障礙嘔吐頸部僵硬抽筋肌張力異常頭痛腦膜刺激症狀及精神症狀(譫妄意識不清等)
檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

檢體採檢送驗事項
實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

實驗室診斷
ndash 符合下列檢驗結果之任一項者定義為檢驗結果陽性 臨床檢體(組織腦脊髓液或其他體液)分離並鑑定出日本腦炎病毒
臨床檢體分子生物學核酸檢測陽性腦脊髓液中日本腦炎病毒特異性之IgM抗體陽性
急性期(或初次採檢)血清中日本腦炎病毒特異性IgM或IgG抗體為陽性者
在最近未接受預防注射及排除其他黃病毒交叉反應的情形下成對血清(恢復期及急性期)中日本腦炎病毒特異性IgM或IgG抗體(二者任一)有陽轉或≧4倍上升
疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

疾病分類
bull 極可能病例
ndash 符合臨床條件及檢驗結果陽性定義之第三項
bull 確定病例
ndash 符合檢驗結果陽性定義之第一二四項之任一項
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
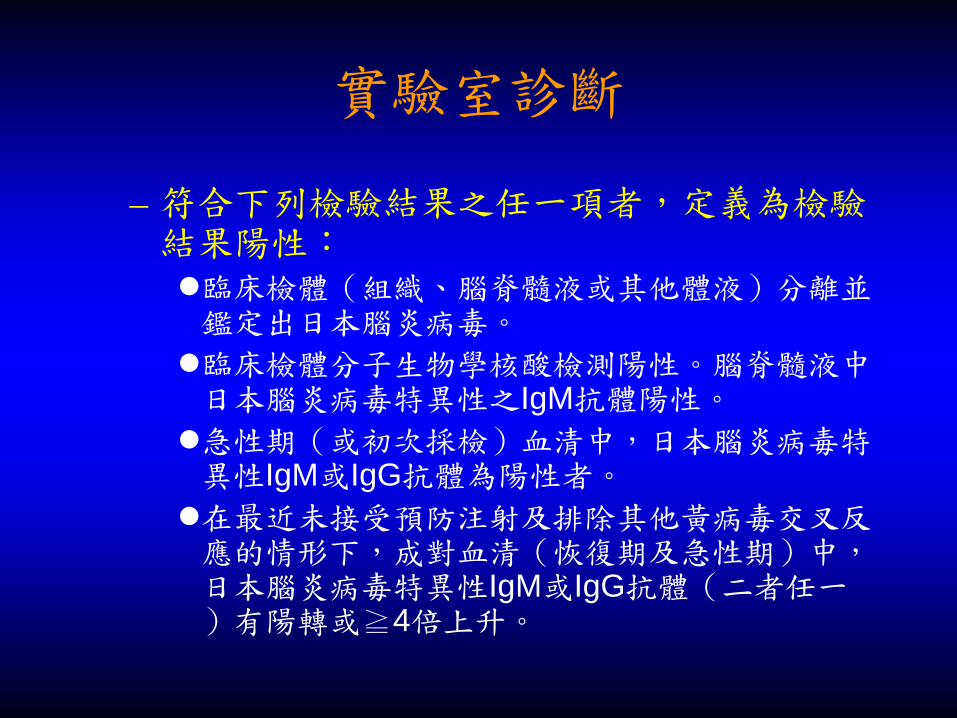
法定傳染病規範
bull 疾病分類
ndash 屬第三類傳染病
bull 通報定義
ndash 具有下列任一個條件
ndash符合臨床條件
ndash醫師高度懷疑與確定病例具有流行病學上相關
bull 通報期限
ndash 於1週內進行通報
bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

bull 白血球上升 嗜中性白血球增加 輕微貧血
bull 腦脊髓液蛋白質約 50個案會上升
bull 腦脊髓液早期會以嗜中性白血球為主
bull 腦脊髓液晚期為淋巴球為主
實驗室檢查
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
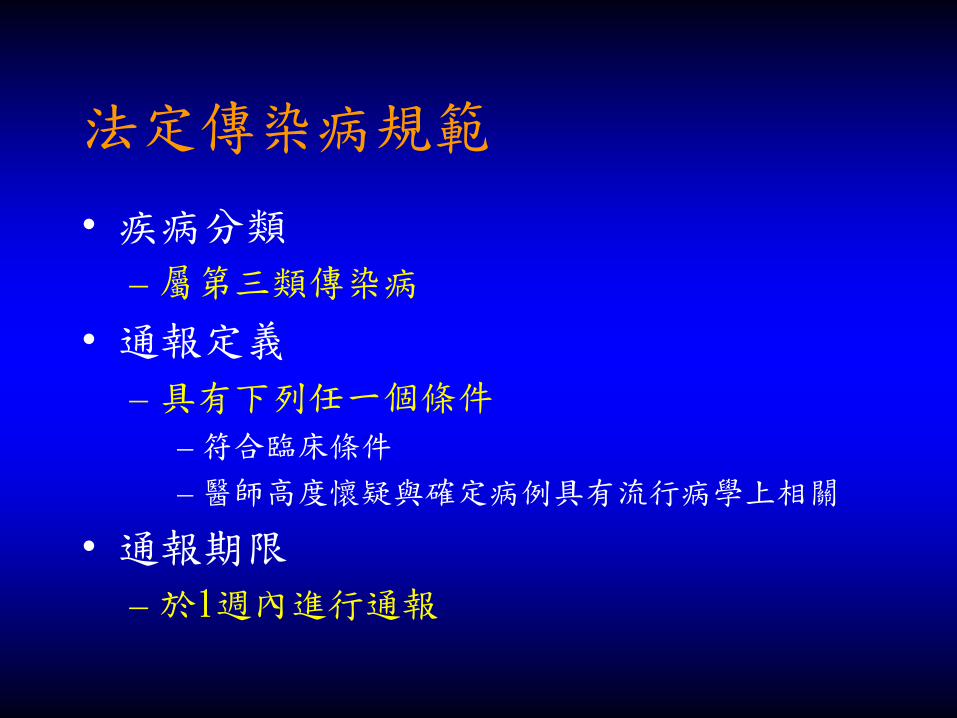
KMHKH bull Case presentation
bull 23 male
bull consciousness change and
bull irritable mood
bull CSF Glu60
TP 32
Lactate11
Appearclear
cell count0
PMNMN0
VDRL(-)
Cryptococcus (-)
HSV IgM(-)
blood Glu85
Lactate18
IgG1240
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
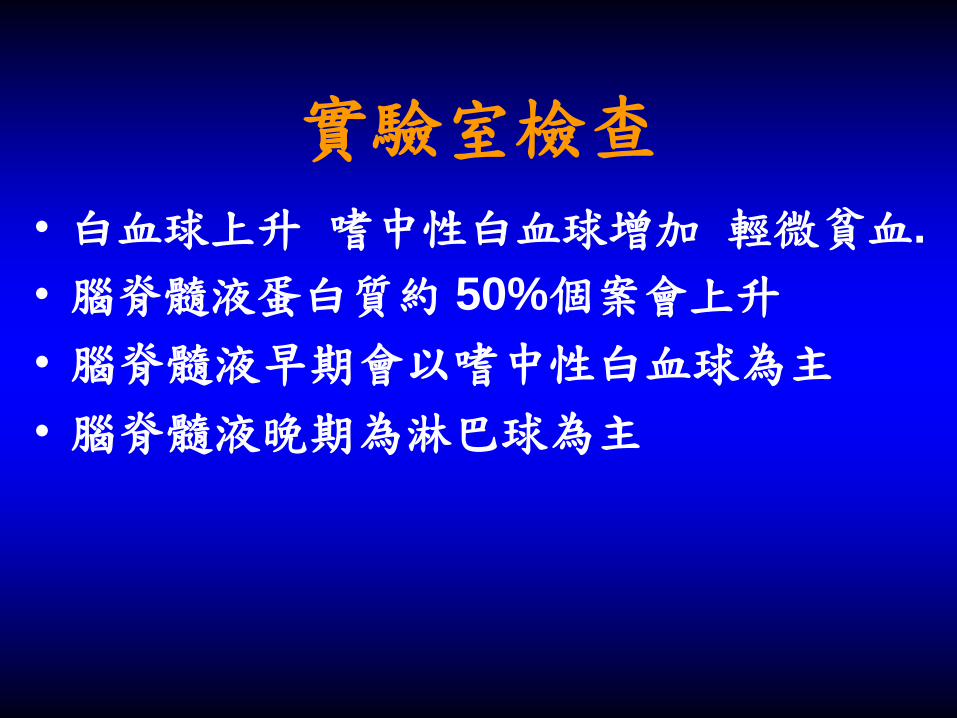
Chief Complaint and Present
Illness
bull 43 yrs old Car repair workers
bull Admission Date20091011
bull Chief Complaint
Sudden onset of left lower limb weakness for one day
Present Illness
suffered from fever muscle soreness since 2 days ago
sudden onset of progressive left proximal lower limb
weakness noted 1 day before admission
bull headache dizziness general malaise vomiting intermittent
left thigh numbness and neck pain
bull visited LMD but in vain then visited our ER (1011)
Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Physical Exam bull Consciousness Alert E4V5M6
BP113 68 mmHg PR109 bpm RR18cpm BT379
Lower limbs left lower limb weakness
free activity
Rrsquot
Lrsquot
upper limbs
proximal
5 4
distal 5 4+
lower limbs
proximal
5 2
distal 5 3-4
Muscle Power
DTR(0-
+ + + +)
Rrsquot Lrsquot
Biceps reflex + + + +
Triceps + + + +
Brachiaradia is + + + +
Knee jerk + + -
Ankle jerk + + + +
Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Differential diagnosis
bull Cranial nerve intact
bull MP
ndash R L
ndash 5 5
ndash 5 2
ndash 5 4-
bull DTR
bull R L
bull 2 2
bull 2 2
bull EPS
bull Rigidity (-)
bull Bradykinesia (-)
bull Bilateral upper limbs postural Tremor (+)
bull DD
bull L2~L3 level (no sensory level)
bull Suspect drug related (EPS)
bull L-spine radiculopathy
bull Myopathy
bull Femoral nerve lesion
bull Plan
bull GOTGPT
bull CK lactate
bull T3T4 TSH
bull influenza
Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Admitted on 1011
1011
bull Fever up to 39 (1930)
bull Give stin and Blood culture
bull Intermittent bilateral upper limbs tremor and spasm (2030) left predominant tonic ndashflexor posture suspect seizure 30 seconds~1 min
bull Suspect novamin induced EPS
Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Clinical Course
1012
bull Generalized skin rash (0040) and fever suspect stin allergy
bull Drowsy consciousness generalized skin rash + fever suspect stin allergy
bull WBC = 1253 10^3ul Segament Neutro = 886 CRP = 694 mgl
bull Highly suspect meningoencephalitis
bull Focal seizure
Consult Infection check HIV TB JBE
Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Clinical Course
1013
Course
bull Drowsy consciousness E3V3M5
bull Lumbar puncture for suspected CNS infection (open pressure 218mmHg)
Transfer to KMU- NICU
Lab
bull Cell count = 177X119 mm^3 [0~5]
bull PMNMN = 8614 [298~595]
bull TP = 019 gdl [660~852]
bull Glu = 59 [120~200] Smear CSF negative
bull Pathology Increased leukocytes and lots of neutrophils suggest meningitis
Medication
bull Ceftriaxone 2g IV Q12H + Vancomycin 1g IVD Q8H + Acyclovir 750mg IVD Q8H
bull Doxycycline 100mg PO QD
1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

1017-1024 at KMUH
bull 1017 respiratory failure Intubation Right lower lobe pneumonia
bull EEG no seizure wave was found
bull lumbar puncture again due to consciousness not improved
CNS infection was partial relieved WBC was lymphocyte dominent stop using Vancomycin Consciousness was improved
bull 1024 consciousness and pneumonia improved gradually Extubation
1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

1030
bull Pneumonia relieved gradually
bull Pre-renal acute renal failure was impressed so we increased fulid amount of hydration Following renal function improved gradually
bull transferred to general ward on 1028
bull JBE confirmed by positive IgG and IgM (981013)
治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

治療及預後
bull 治療方式
ndash 無針對日本腦炎病毒之抗病毒藥物
ndash 依病情給予支持療法
ndash 嚴重時要加護病房照護
bull 併發症
ndash 神經性後遺症
bull 不正常肌張力
bull 語言障礙
bull 運動肌無力等
ndash 精神性後遺症
bull 脾氣暴躁
bull 性格不正常
bull 智力不足
ndash 常發生在年輕的小孩
日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

日本腦炎防治策略
bull早期診斷 早期治療
bull病媒蚊防治
A)降低幼蟲 B)病媒蚊控制
bull 預防 施打疫苗
bull 國內自民國57年起新生兒全面施打日本腦炎疫苗之前出生的人多半都沒有接種過疫苗
疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

疫苗接種條件及限制
bull 接種對象
ndash 年滿15個月的幼兒應接受2劑注射其間相隔2週隔年再接種一劑小學一年級時再追加接種一劑
ndash 工作或生活中有感染之虞且有意願接種的成人可前往全國26家署立醫院或分院自費接種
bull 接種時程
ndash 每年3至5月
bull 禁忌
ndash 發高燒
ndash 患有嚴重疾病者
疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

疫苗接種條件及限制
bull 保護力
ndash 疫苗的有效性約85
bull 副作用
ndash 局部
紅腫腫脹疼痛
ndash 全身
發燒惡寒頭痛倦怠感
ndash 通常2~3天內消失
避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

避免病媒蚊叮咬
bull 盡量避免於病媒蚊活動的高峰期(黃昏)在豬舍其他動物畜舍或病媒蚊孳生地點附近活動
bull 請穿著長袖長褲身體裸露處塗抹防蚊藥劑避免蚊蟲叮咬以降低感染風險
bull 居家環境管理疏通水溝清除雜草處理積水及家中需設置紗門紗窗以消滅病媒蚊及其幼蟲
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
Rickettsial Infection
1 Gram (-) obligate intracellular bacteria
2 Vectorborne ( tick mite fleashellip)
3 Spotted fever and typhus groups
vasculitis
rickettsiae proliferate in the endothelial lining cells of small arteries capillaries and veins
Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Topic1Scrub typhus-history bull AD 313 晉朝rdquo葛洪rdquoldquo人行經草處沙地被依微小沙虱叮咬即發生紅疹三日後發熱叮咬局部潰瘍節痂rdquo
bull 1810 Hakuju Hashimoto Japanese first described this disease
bull 1927緒方規雄(Ogata norio) patient serum injected into the rabbitrsquos testis-repeat this procedure 5 times-gall bladder swelling -isolated Rickettsia orientia
bull 1931 Formal name Rickettsia tsutsugamushi
bull 範圍西至巴基斯坦阿富汗
東至日本本州北端南到整個東南亞至
澳洲東北部及西南太平洋群島
Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Scrub typhus-pathogen bull 1恙蟲病 (Tsutsugamushi disease
tsutsu是惡疾之意而mushi是指恙蟲)
又名叢林型斑疹傷寒〈Scrub typhus〉
bull pathogen Orientia tsutsugamushi
( Rickettsia tsutsugamushi)
vector Leptotrombidium deliense
bull 2Transmitted by a bite of chigger
(a larval stage mite) through the
chiggerrsquos saliva
bull Endemic in Asia Australia New Guinea
Pacific Islands
Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Host
bull Orientia tsutsugamushi
in mites will be vertical
transmission in every
stages including ovarylarvadeutonymphadult permanent
infection
bull Animal host rodentsmammals (sheeppigdogcat)avian (birdchicken) Rodents are
the major host
38 Jerome Goddard Infect Med 17(4)236-239 2000
bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

bull Incubation period
- 1~2 weeksusually 9~12
days not human to human
bull Immunity protection
- One man got secondary infection of scrub typhus he may have long term immunity for protection if the strain of scrub typhus is same as previous but only short term immunity for protection if the strain of scrub typhus is different from previous
- Second or third infection of scrub typhus in endemic area may occur but the symptoms and signs will be mild
httpwwwcdcgovtw
Transmission method
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
Scrub typhus 1996~20132
台北區 合計 1636 No1
北區合計 230
中區合計 640
南區合計 216
高屏區合計 1277 No3
東區合計 1481 No2
合計 5480
0
200
400
600
800
1000
1200
lt14 15-19 20-29 30-39 40-49 50-59 60-69 gt70
female
male
male
female
male3515 cases
Female1915 cases
0
100
200
300
400
500
600
700
800
900
1000
1 2 3 4 5 6 7 8 9 10 11 12
Scrub typhus cases from 1996 to Feb2013 in Taiwan
httpwwwcdcgovtw
bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

bull Seasons all year in Taiwan the peak period May~December
bull Location scrub typhus favor high temperature and high humidity outsides grass
bull occur in Taiwan high prevalence in Kingman Matsu Penghu Lanyu Hualien Taitung Kaohsiung
Epidemioloy
bull genotype Karp Gilliam Kato
Kawasaki Boryong Taguchi
KandaKawasaki
Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Clinical Manifestation (1) bull Fever chills headache muscle pain
lymphadenopathy
bull Rash ndash 5 days after insect bite
9-10 days later subsided
ndash from trunk to extremities
ndash maculerarrpapule
Eschar (about 50-80 in scrub
typhus patients painless)
bull Splenomegaly may be seen
bull Complication ndash Pneumonia ARDS myocarditis renal failure septic shock
ndash After two weeks incubation central nervous system occur meningoencephalitis acute transverse myelitis
httpwwwcdcgovtw
SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

SCRUB TYPHUS IN JAPAN EPIDEMIOLOGY AND
CLINICAL FEATURES OF CASES
REPORTED IN 1998
bull A total of 462 cases
bull Seventy-six percent of the patients were more than 51 years old and 36 and 16 of the patients were engaged in farm work and forestry respectively
bull Fever rash and eschar were detected in 98 93 and 97 of
bull the patients respectively
bull Elevated levels of C-reactive protein aspartate transaminase and alanine transaminase were detected in 96 87 and 77 of the patients respectively
bull Disseminated intravascular coagulation developed in 34
bull cases and had a unique regional distribution Am J Trop Med Hyg 67(2) 2002 pp 162ndash165
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
Acute respiratory distress
syndrome in scrub typhus
bull 72 patients with scrub typhus from 19981 to 20068 in KCGMH in Taiwan
bull Eight of 72 scrub typhus patients with ARDS included in the study the other patients without ARDS were used as controls The mortality rate for the scrub typhus patients with ARDS was 25
bull Initial presentations of dyspnea and cough white blood cell count hematocrit total bilirubin and delayed used of appropriate antibiotics use were significant predictors of ARDS
bull Multivariate analysis showed that albumin prothrombin time and delayed use of appropriate antibiotics were independent predictors of ARDS
Am J Trop Med Hyg 2007 Jun76(6)1148-52
Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Scrub typhus complication bull Be aware of the potential for complications scrub
typhus are older (ge 60 years) presents without eschar or WBC counts gt 10 000mm3 and serum albumin level le 30 gdL Close observation and intensive care for scrub typhus patients with the potential for complications reduction in its mortality rate Kim et al BMC Infectious Diseases 201010108
bull Bilateral simultaneous facial palsy following scrub typhus meningitis a case report and literature review
LinWL Kaohsiung J Med Sci 2011Dec27(12)573-6
Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Diagnosis bull 1 PCR amplification of O tsutsugamushi DNA from blood of febrile
patients or eschar lesion
2 IFA (indirect fluorescent antibody) acute stage IgM Ab ≧180
and IgG Ab ≧1320
3 IFA (acute stage amp recovery stage)
IgM or IgG Ab seroconversion or ≧4x elevation
bull Weil-Felix slide agglutination test lower sensitivity and specificity
half patients have antibody reaction to
Proteus spp OX-K
Weil-Felix slide agglutination test is not specific
sensitive or specificity is not high
Proteus spphave similar antigen with rickettsial antigen When human got rickettsial infection human body will induce anti-rickettsial antibody which will be cross reaction with Proteus spp
Proteus OX-K (+) ---may be associated with scrub typhus infection
Proteus OX19 (+) -- may be associated with murine typhus infection
Proteus OX-K(-) OX19(-) OX2(-)mdashQ fever
Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Treatment and prophylaxis
bull 1 inadequate treatment (insufficient treatment course) induce
high relapse tendency all patient need two weeks treatment
course doxycycline 100 mg bid po for 7-14 days
tetracycline minocycline
bull 2ciprofloxacin levofloxacin
chloramphenicol rifampicin
3 oral azithromycin was administered in a 500mg dose on
the first day followed by 250 mg daily on days 2 to 5
( in children and pregnant women)
Prophylaxis doxycycline 200 mg every week keep 3-4 weeks wearing long-sleeve clothes and trousers bootleg use insect repellent
Prognosis treatment-mortality less than 5
第四類法定傳染病 一週內通報
Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Scrub typhus prevention Personal prevention
bull wearing long-sleeve clothes and trousers
bootleg while in adventure travel
bull use insect repellent Diethyltoluamide
(DEET) for prevention mite bite
bull After leaving an endemic area take a bath
and wear the clean dress
Environment improve
grass cutting nearby a residence house for decreasing the possibility of mite contact
Deratization- decresae the numbers of mites
httpwwwcdcgovtw
Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Patient profile amp
Chief complaint
bull Age58 yo female
bull Occupation housewife
bull Residence 高雄縣大寮鄉
bull Admission date 941114 via ER
bull CC sudden onset fever up to 392
degrees on and off for 2-3 days
Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Present illness
bull This 58 female a case with
hypertension with diet and activity
control without other major systemic
diseases
bull About 7 days ago she came back from
澎湖娘家 and then felt general malaise
headache since last W2(118)
Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Present illness
bull Due persistent symptoms she went
LMD for help and medications was
prescibed on last W6(1112) for
tonsillitis
bull However after LMD visit fever on and
off was noted for 2-3 days and chillness
dizziness sore throat persisted
Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Present illness
bull she came to our ER for help
bull Other associated symptomssigns
- Fever(+) chillness(+) general malaise(+) headache(+) myalgia(-) arthralgia(-) retro-orbital pain(-) night sweating(-) rash(-)
- Neck stiffness(-) conscious change(-) facial muscle weakness(-) photophobia(-) seizure(-) limb weakness(-)
- Sorethroat(+) cough(-) rhinorrhea(-)dyspnea(-)
- Abdominal pain(-) diarrhea(-) nauseavomiting(-)
- Painful urination(+) low back soreness(+) frequency(-) urgency(-)
Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Physical examination
bull Consciousness alert oriented
bull Vital signs BT 378 BP 13080 PR 84
RR 20
bull HEENT
Sclera mildly pink but not icteric
Oral cavity swelling of injected bil
Tonsils discharge(-)
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
Physical examination
bull Neck
-Lymphadenopathy (+) over left side of neck 2 lymph nodes size 1x1 cm tenderness(-) movable
-Jugular vein engorgement(-)
-Kernigrsquos sign(-) Brudzinskirsquos sign(-)
Chest
-Heart sound regular heart beat no murmur no S3S4 normal S1S2
-Breath sound bil clear No crackles No wheezing
Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Physical examination
bull Abdomen
-Soft flat tenderness(-) Murphyrsquos sign(-)
-Liverspleen impalpable
-RUQ knocking pain(+)
-Rrsquot flank knocking(+)
-Normoactive bowel sound
Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Physical examination
bull Extremities
-Lower legs pitting edema(-)
bull Skin
-Erythematous maculopapules(+) over lower abdomen itching(-) pain(-)
-Black-central scared wound (+) with erythematous base over rrsquot inguinal area itching(-) pain(-) discharge(-) Eschar
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
Clinical impresison
bull Fever
Acute tonsillitis
(sore throat swelling tonsils)
susp APN rrsquot
( kocking pain)
susp Viral infections
Reckettsia infection (scrub typhus)
Dengue fever
( hx eschar regional lymphadenopathy rash)
susp Liver disease
( RUQ knocking pain)
Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Plans
bull General survey CBCDC CRP electrolytes liver function renal function coagulation profile GOTGPT bilirubin AC sugar
bull HBsAg anti-HCV
bull Urine routine
bull Abdominal echo
bull Chest X-ray 12-lead EKG
bull Well-Felix test LDH
bull IFA PCR
bull Antibiotics Cefazolin 1g IV q8h
Doxycyclin 100mg bid
Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Laboratory surveys CBC 1114 ER 1116 1118
WBC x1000ul 403 467 699
RBC x10^6ul 409 388 392
HGB gdl 117 112 106
HCT 345 326 329
MCV fl 848 84 839
PLT x1000ul 94 105 182
SEGEMENT BAND
282
LYMPH 1794 44
EOSIN 024 1
MONO 5
BASO 074
RDW-CV
RDW-SD fl
CRP ugml 64
Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Laboratory surveys Urine 1114 ER Urine 1114
GLU - RBC HPF 2-5
BIL - WBC HPF 0-2
KET - Epith HPF 0-2
SG =lt1005 Crystal -
OB + Cast -
PH 70
PRO -
URO 01
NIT -
WBC -
Color YellowClear
normal
Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Laboratory surveys Blood
chemistry
1114 ER 1115 1116
T-BIL mgdl 047
D-BIL mgdl 013
GOT IUL 56
GPT IUL 46
PRO mgdl 602
ALB mgdl 328
GGT UL 23
ALK-P IUL 145
LDH 1207
Cholestreol 147
TG 185
PT p second 119
PT c second 108
PT(INR) 107
PTT P 357
PTT C 282
Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Laboratory surveys
1114 ER 1118
BUN mgdl 58
CREA mgdl 076
NA m molL 129 133
K m molL 41 38
Sugar(AC) mgdl 108
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus
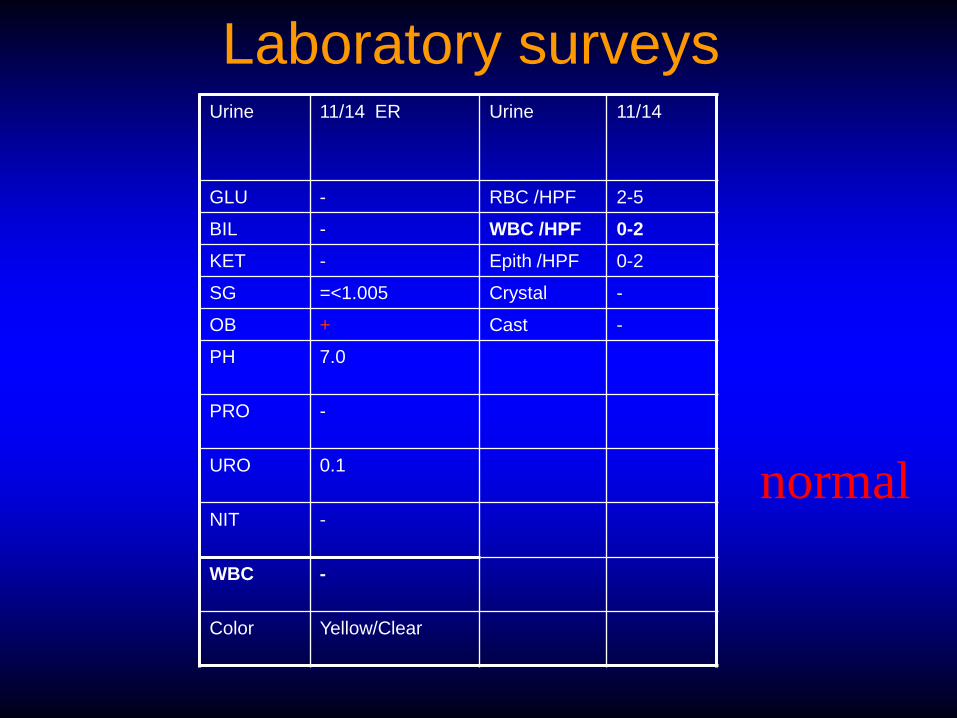
Abdominal echo
Finding Liver cyst at S2 single lt5 cm
Splenomegaly(-) hepatic parenchyma change(-)
normal kidney size parenchyma hydronephrosis(-)
Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Tentative Diagnosis
bull Atypical infection suspect scrub typhus
(thrombocytopenia normal or low WBC impaired liver function eschar relative bradycardia rash lymphadenopathy travel history)
Differentials Dengue fever typhoid fever leptospirosis other viral infections
bull Acute tonsillitis
Cefazolin and Doxycyclin use
Watch out CNS pulmonary renal complications
Dx Confirmation
Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Progression
bull Fever(+) but decreased gradually under
treatment with Cefazolin and Doxycyclin
bull No complications occurred during
admission
bull Fever subsides on 1119 (day 6) and
due to stable condition MBD arranged
with OPD FU and oral antibiotics
prescribed
bull Her husband
Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus

Fever with headache without obvious focus
1Endemic areasouth-east asia
2headachemuscle painjoint painretrobulbar painback painrash
3Laboratory
WBC<5000ul or normal
PLT<100000ul
GOTGPT elevation and GOT > GPT
aPTT prologationPT normal
initial 3 days Segment elevation
the 4th ~6th day after infected
monocytosis
Endemic + 2 kind
clinical symptoms +
laboratory
One or two items
compatible but not very
likely
Inform
CDC
May inform
CDC
DD Dengue fever and Rickettsial diseases
Relative bradycardia No Yes
Eschar
Yes No
mountains
Climbing
Taitung or
Hualien
travel
history
suspect
Q fever
suspect
Murine typhus
WBC<5000ul
or normal
PLT lower
GOTGPT
elevated and GOT
lt GPT
aPTT
prolongation
PT normal
Animal contact
Anticardiolipin Ab
elevation
WBC<5000ul or
normal
PLT lower
GOTGPT
elevated andor
GOT gt GPT
aPTT
prolongation
PT abnormal
OX 19 (+)
suspect scrub
typhus






























