Embed Size (px)
Citation preview

CBT for Depression: An Introduction
Debbie SpainTutor – Dept. of Mental Health
Florence Nightingale School of Nursing & Midwifery

Learning outcomes
By the end of the session, you will be able to:
• Define depression• Outline behavioural and cognitive models of
depression• Discuss the application of key CBT principles and
strategies • Begin to critique the evidence-base

Low mood: a continuum of experience?
• Is it ‘normal’ to feel sad?
• Are there any differences between sadness, grief and depression ?
• When does ‘normal sadness’ become depression?
(Horwitz and Wakefield, 2007)

Depression: diagnostic criteria (WHO, 1992)
• Core symptoms:
- Low mood- Pervasive loss of interest or pleasure (anhedonia)- Significant weight change- Sleep disturbance- Observable agitation or retardation- Loss of energy- Feeling worthless or unnecessarily guilty- Poor concentration or attention- Recurrent thoughts of death or suicide
- Pattern must be present for most of the day for at least two weeks
- Causing impairment and some interference to daily functioning

Depression: key stats
• Incidence:Depressive episode = 4 - 10% of adultsDysthymia = 2.5 - 5% of adults (NICE, 2010)
• By 2020, depression will be the second cause of global disability and burden (WHO, 2010)
• High rates of physical and mental health co-morbidities

Depression: key stats
• Positive associations found between depression and the following (e.g. Gilbert, 2000; NICE, 2010):
- Gender - Socio-economic status - Social factors - Adverse life experiences- Physical illness

Depression: aetiology (NICE, 2010)
• Contributory factors for depression may include:
- Neuro-biological factors - Genetic predisposition - Physical illness - Stress vulnerability / social factors- Psychological models
- Behavioural model - Cognitive model

CBT: key principles
• “Man is not affected by events but by the views he takes of them” (Epictetus)
• Links between thoughts, feelings and behaviour
• Emphasis on the ‘here and now’
• Important to establish current maintaining factors

Depression: aims of CBT assessment ?
• Obtain information about current symptoms and impact
• Develop a shared understanding (a formulation)• Provide psycho-education about CBT• Normalise experiences• Start to develop a therapeutic relationship• Instil hope • Risk assessment• Identification of clinically appropriate intervention/s (e.g. Mulhern, 2010; Townend and Grant, 2010)

Depression: CBT assessment
Questions to consider:
• Are there any symptoms of depression that might impact on undertaking an assessment?
• Why might it be important to normalise experiences?
• Why might it be important to instil hope?• What factors might render psychological
interventions unsuitable for someone who is depressed?
• How can we improve the process of assessment?

CBT models for depression
• Behavioural model – Behavioural Activation
• Cognitive model – cognitive therapy
• Cognitive-behavioural models – cognitive and behavioural techniques

Behavioural model: background
• Based on learning theory:
- Classical conditioning Pavlov - stimulant induces a response
- Operant conditioning Skinner – behaviour induces a response(Tyrer and Steinberg, 2008)
• Symptoms and behaviour are the disorder

Classical and operant conditioning

How do behaviours maintain andperpetuate low mood?
Developing a formulation

Behavioural model: Theories of depressionLoss of response-contingent positive reinforcement (Skinner, 1953)
Stimuluse.g. work, social occasions, telephone calls
absence of positive low mood, no interest,
consequences or reward no energy, no motivation
Response inactivity, procrastination, isolation
15

BA: a theoretical framework

BA: Formulation
• Functional analysis
• TRAP:- Triggering events- Responses- Avoidance Patterns
• TRAC:- Triggering events- Responses- Alternative Coping

BA: treatment rationale
BA aims to re-establish the sense of achievement and
enjoyment out of everyday life by:
• Increasing the amount, range, and difficulty of activities
• Balancing different types of activities
• Taking the time necessary for task completion
18

BA: overview of treatment
• Activity monitoring
• Activity rating (MASTERY & PLEASURE)
• Activity scheduling
• Activity grading
19

Activity monitoring / scheduling
Mon Tue Wed Thu Fri Sat Sun
5-6am
6-7am
7-8am
8-9am
9-10am
10-11am
11-12pm
12-1pm
1-2pm

Activity rating
• Rate each activity using a scale 0-8; 0 meaning “not at all” and 8 meaning “very much”
• Put a P with the rating next to activities that may give pleasure and enjoyment (e.g. watching TV, eating)
• Put an M with the rating next to activities that may give a sense of achievement (doing the housework, taking kids to school)
21

Activity scheduling
• Use a diary to plan hour-by-hour activities
• Schedule in tasks so as to increase the activity levels
• Schedule in tasks which the person has to do in balance with tasks that the person wants to do, so as to maximise mastery & pleasure
22

Activity grading
• Graded task assignment
• Four potential outcomes:
1. Omit, if the tasks exceed the available time 2. Delegate, wherever possible3. Seek help and support whenever possible4. Grade the task
23
BA: the evidence base
Cuijpers, P. et al. (2007). Behavioural activation treatments of
depression: A meta-analysis. Clinical Psychology Review, 27, 318
326.
Mazzucchelli, T. et al. (2009). Behavioural Activation Treatments
for Depression in Adults: A Meta-analysis and Review. Clinical
Psychology: Science and Practice, 16(4), 383-411.
24

Cognitive model: background
• Thinking and cognition shape our view of the world
• The ABC model (Ellis, 1962): Activating eventBeliefs about activating eventConsequence (emotional or behavioural) of belief
(Tyrer and Steinberg, 2008)
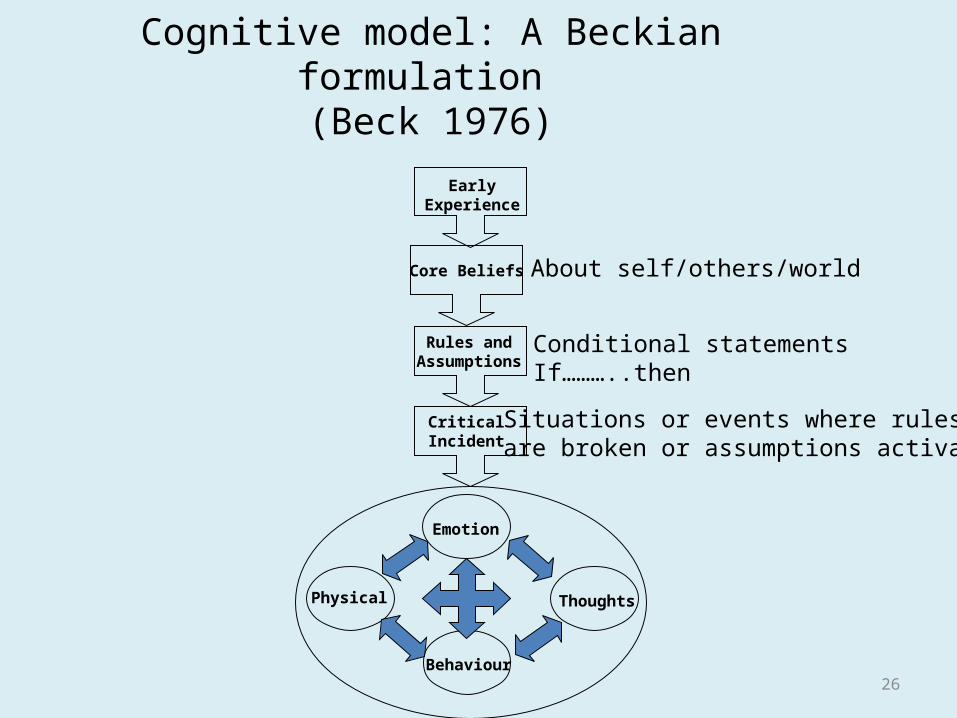
Cognitive model: A Beckian formulation (Beck 1976)
26
EarlyExperience
Core Beliefs
Rules andAssumptions
CriticalIncident
Emotion
Thoughts
Behaviour
Physical
About self/others/world
Conditional statementsIf………..then
Situations or events where rulesare broken or assumptions activated
Cognitive model: key aspects
• Thoughts and thinking style likely contribute to the development and maintenance of depression
• Depression exaggerates processes inherent in all of us:a continuum of functioning
• Depression affects the way we view ourselves, the world and other people
(Mulhern, 2010)

Cognitions: contributing to development and persistence of depression?
• Content: themes of loss, self devaluation, hopelessness
• Process:- bias towards the negative - reduced flexibility
- cognitive style
• Interpretation bias:- negative events are explained by internal factors- positive events are explained by external factors not attributed to self
• Bias results in an absence of positive experience past and present
28
Common thinking styles
• Jumping to conclusions
• Predicting the future • All or nothing
thinking• Emotional reasoning • Discounting the
positive• Catastrophising
• Dwelling on the negative
• Egocentric thinking• Rumination • Reduced meta-
cognitive awareness(Gilbert, 2000)

Cognitive therapy: planning treatment
• Treatment plan is informed by conceptualisation• Structured and time limited• Focus upon maintaining factors• Collaborative, not confrontational • Reliant upon guided discovery not didactic• Socratic questioning is key• Educational - promoting self application of CBT
skills

Cognitive interventions
• Cognitive interventions broadly address:
- What the person thinks (the content)
- The way they think (the process)
- Their interpretation of their thinking and events (the meaning)

Cognitive interventions contd.
Some common cognitive interventions:
- Identifying and challenging negative thoughts - Continuums- Behavioural experiments- Surveys- Role plays
One thought leads to another. And another. And another…
NATs have several characteristics:
- seem to occur automatically, without any effort- typically followed by a string of other thoughts- appear logical and plausible- often distorted- unhelpful- involuntary

Challenging negative automatic thoughts
• Helpful to consider the following:
- What is the evidence for and against my thoughts?
- What is the effect of thinking the way I do?- What alternative views are there?- What thinking errors am I making?

Continuum work
• Use of continuums to explore thoughts and beliefs is very common
• This is not about telling people that their thoughts are wrong
• A way of generating further evidence about a situation
• Involves guided discovery and socratic dialogue
• Ideal to write things down
Behavioural experiments: an overview
• A way to test out beliefs• Informed by a shared formulation
• Identify the specific belief to test• Rate the strength of belief• Devise a way of testing this out• Make predictions • Identify and problem-solve around any obstacles• Drop safety-behaviours• Conduct experiment• Rate outcome, belief

Planning therapy
• How do you decide which interventions to use first?
• Positive outcomes in cognitive therapy for depression may be predicted by the extent to which early sessions focus on specific concrete interventions (Feeley et al 1999)
• Key questions to consider when deciding which strategies to use with individuals and at what stage:
– How severe is the depression?– At what point in therapy is the client?– What problem is most distressing to client?– What area is most amenable to change?– Risk issues
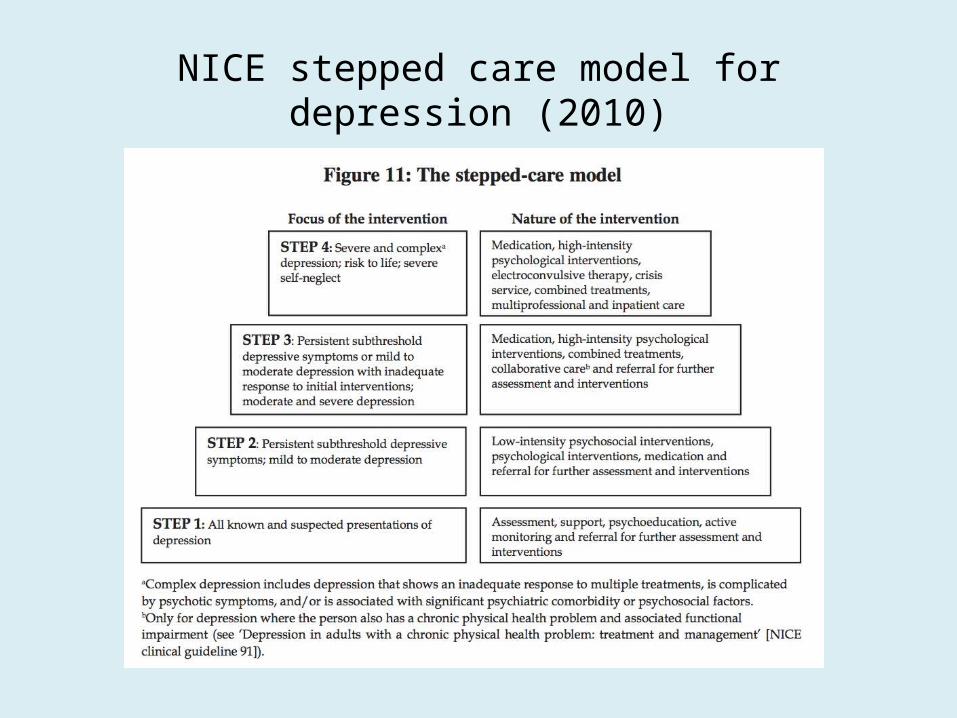
NICE stepped care model for depression (2010)

Developing a therapeutic alliance
• The importance of the therapeutic relationship?
“A good relationship between client and therapist is, at the very least, considered to be the base from which all therapeutic work takes place” (Hardy et al. 2007, in Grant & Townend, 2010)
• Threats to the therapeutic relationship?
• Key components of effective therapeutic relationships?

Goal setting in depression
• Important to identify personally meaningful goals
• Be pragmatic
• Plan for contingencies
• Helpful to record goals and successes promptly
‘Homework’ contd.
• The importance of homework?
• Homework in practice
• Understanding reasons for non-completion of tasks is an important aspect of CBT therapy

Outcome measures in depression
• Standardised measures e.g. CORE-OM, HADS, BDI
• Idiosyncratic measures
• Subjective units of distress (SUDS rating)

Keeping track of who said what during therapy sessions?
“I know you think you understood what you
thought I said, but I don’t think you understood
that what you heard is not what I meant”

Additional interventions and relapse prevention
• Looking after physical health
• Exercise • Be aware of triggers
for stress• Sleep hygiene• Problem-solving
techniques• Assertiveness training
• Addressing low self-esteem
• Mindfulness-based cognitive therapy
• Compassionate-focused therapy
• Follow up sessions • Relapse prevention • Create a self-help tool
box: “therapy blueprint”

CBT: Therapy blueprint
Questions to consider:
• What are my ongoing problem areas?• What are my beliefs, assumptions that keep
these problems going?• What have I learnt in therapy?• What CBT skills do I have?• What are the potential obstacles in the future
that may influence my mood / prevent me from using my CBT skills?
• What resources are available to me?

Some considerations
• CBT for depression typically involves changing unhelpful / avoidance behaviours, and examining unhelpful thoughts and patterns of thinking
• Increasing evidence for several modes of CBT delivery
• Therapy outcomes are determined by several key factors including a shared formulation, consideration of non-specific variables, and ongoing assessment of risk and need
• Proactive strategies are as important as reactive strategies

References
Cuijpers, P. et al. (2007). Behavioural activation treatments of depression: A meta-analysis. Clinical Psychology Review, 27, 318-326.
Gilbert, P. (2000). Overcoming Depression. (2nd ed). London: Constable & Robinson.
Horwitz, A. and Wakefield, J. (2007). The Loss of Sadness. Oxford: Oxford University Press.
Keedwell, P. (2008). How sadness survived. The evolutionary basis of depression. Oxford: Radcliffe Publishing.
Kuyken, W and Dimitrios, T. (2009). Therapist competence, Comorbidity and Cognitive-Behavioural Therapy for Depression. Psychotherapy and Psychosomatics, 78(1), 42-48.
Mazzucchelli, T. et al. (2009). Behavioural Activation Treatments for Depression in Adults: A Meta-analysis and Review. Clinical Psychology: Science and Practice, 16(4), 383-411.

References
Mulhern, R. (2010). Depression. In A Grant, M Townend, R Mulhern and N Short (2010). Cognitive Behavioural Therapy in Mental Health Care. London: SAGE.
Neff, K. www.self-compassion.org
NICE. (2010). CG90 – Depression. London. HM Publications.
Richards et al (2012) Computer-based psychological treatments for depression: A systematic review and meta-analysis. Clinical Psychology Review. 32, 4, 329-342.
Townend, M. and Grant, A. (2010). Fundamentals. In A Grant, M Townend, R Mulhern and N Short (2010). Cognitive Behavioural Therapy in Mental Health Care. London: SAGE.
Tyrer, P. and Steinberg, D. (2008). Models for Mental Disorder: Conceptual Models in Psychiatry. (4th ed). Chichester: John Wiley & Sons.
WHO. (1992) ICD-10. WHO.





























