Embed Size (px)
Citation preview

CBL REVIE
W
HO
PE
AN
D J
ES
S
MATCH THE DEFINITION TO THE SYMPTOM:
Nocturia -
Polyuria –
Oliguria -
Dysuria –
Glycosuria –
Haematuria –
Proteinuria –
Anuria –
getting up at night to urinate
urinating more frequently
low urine output
pain on urination
glucose in urine
blood in urine
protein in urine
no urine output
GIVE A CONDITION THAT WOULD PRESENT WITH THE FOLLOWING?
Glycosuria
– diabetes mellitus
Oliguria
– dehydration, hypovolaemia, urinary obstruction
Haematuria
– UTI, bladder cancer, stones, BPH, prostate cancer.
WHAT IS A DIPSTICK USED TO MEASURE? (10)
Glucose
Protein
Leukocytes
pH
Blood
Bilirubin
Ketones
Specific gravity
Urobilinogen
Nitrites
WHAT IS THE NORMAL PH OF URINE?
5.5-6.5
WHY MIGHT YOU FIND NITRITES IN URINE?Bacterial conversion of endogenous nitrates to nitrites.Nitrites are not usually found in normal urine. IF YOU FIND NITRITES IN URINE, WHAT ELSE WOULD YOU EXPECT TO SEE ON THE DIPSTICK?
LeukocytesPotentially blood.
WHICH PARTICULAR QUESTIONS WOULD YOU ASK WHEN TAKING A HISTORY OF A PATIENT PRESENTING WITH HAEMATURIA?
• When did it start
• How much blood and how frequently
• What colour/consistency/any clots?
• Mixed in with urine or separate.
• Timing: beginning, middle or end of urination
• Painful or painless
• On anticoagulants (warfarin/aspirin etc)/ known coagulopathies/clotting disorders
• Do they eat a lot of beetroot? On Rifampicin? (both colour urine red)
• Associated symptoms of anaemia (SOB/lethargy/dizziness)
• Red flags – weight loss/loss of appetite/lethargy/night sweats/family history
• Employment history (dye/rubber industry)
• Smoking & alcohol
• Foreign travel (renal TB/schistosomiasis)
QUICK REVIEW: BLADDER CANCERSymptoms: Painless haematuria is the principle symptom (frank or
microscopic), increased frequency, sudden urge to urinate, difficulty to void, incomplete voiding.
Types: Transitional cell carcinoma (90%), squamous cell carcinoma (5%), Adenocarcinoma (1/2%) . Mets from rectum, prostate, uterus, ovaries, cervix.
Note: transitional epithelium lines the bladder and the ureters.
Treatment:
Surgery for wide local excision
Radio therapy +/- chemo therapy
TURBT (transurethral resection of bladder tumour)
Chemotherapy – most common – BCG – thought to stimulate immune response.

VIGNETTE 1:
64-year-old man presents with painless haematuria. He had a similar episode 1 year ago and was given antibiotics for a presumed urinary infection and his bleeding resolved. He has a decreased urinary stream and nocturia twice a night. He has smoked a pack of cigarettes daily for 45 years.
Bladder cancer is suspected.
WHAT WOULD YOU LOOK FOR ON A DIPSTICK OF SOMEONE WITH SUSPECTED BLADDER CANCER?
Blood - Haematuria
WHAT INVESTIGATIONS WOULD YOU ORDER FOR SUSPECTED BLADDER CANCER?CT urogram – can identify areas with filling defects. Ultrasound scans –can show areas of nodular changes Flexible/rigid cystoscopy - permits direct inspection of the bladder and biopsy of suspicious lesions.
WHAT TYPE OF EPITHELIUM LINES THE BLADDER?Urothelium A type of transitional epithelium.
DESCRIBE THE HISTOLOGICAL APPEARANCE OF THIS EPITHELIUM AND WHAT FUNCTION IT IS ADAPTED TO PERFORM. Mixture of squamous and cuboidal epithelium. Allows it to expand and contract.
WHICH CANCER ARISES FROM THESE CELLS? Transitional cell carcinoma.
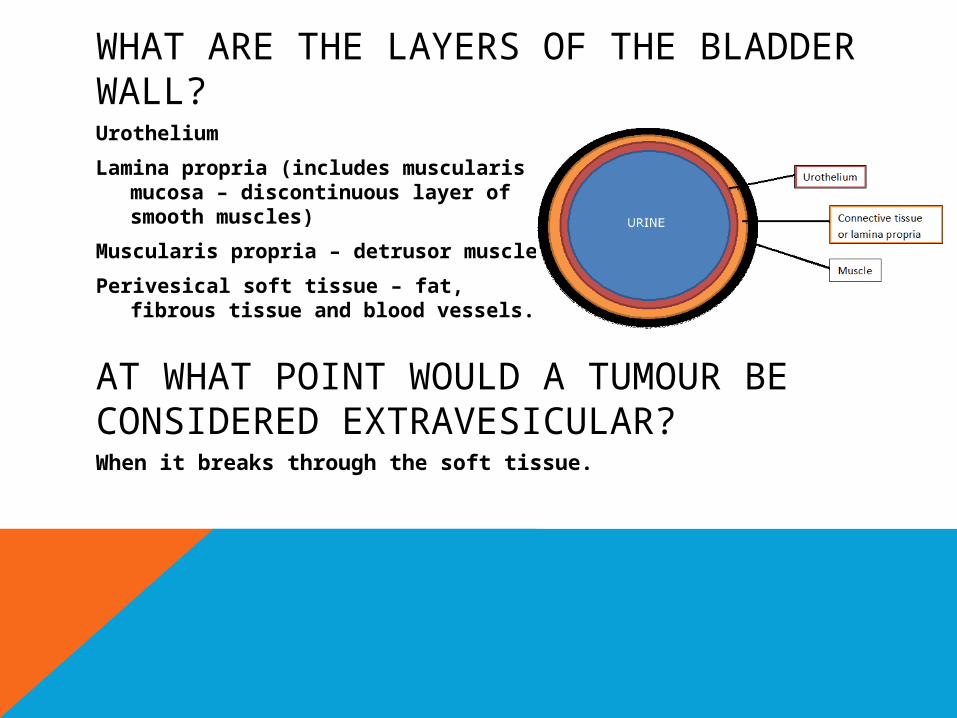
WHAT ARE THE LAYERS OF THE BLADDER WALL?Urothelium
Lamina propria (includes muscularis mucosa – discontinuous layer of smooth muscles)
Muscularis propria – detrusor muscle
Perivesical soft tissue – fat, fibrous tissue and blood vessels.
AT WHAT POINT WOULD A TUMOUR BE CONSIDERED EXTRAVESICULAR?When it breaks through the soft tissue.
WHAT ARE THE RISK FACTORS FOR BLADDER CANCER?
Working in rubber or dye industry
Old age
Smoking
Previous cancer
Diabetes
Family history
Obesity
QUICK REVIEW: BENIGN PROSTATIC HYPERPLASIA
Non-cancerous enlargement of the prostate gland, usually in the transitional zone.
Symptoms – difficulty starting to urinate, decreased strength of the urine stream, dribbling after urination, feeling of incomplete voiding, dysuria, nocturia.
Treatment – monitoring, drugs, surgery
Many men develop BPH with old age – and it is not considered a problem.
QUICK REVIEW: PROSTATE CANCER
Symptoms – asymptomatic until puts pressure on the urethra, dysuria, nocturia, frequency, urgency, dribbling, weak flow.
Types – Most are adenocarcinomas (95%), tumours arise more commonly in the peripheral zone of prostate.
Treatments – Close monitoring, hormone therapy, surgery, chemotherapy.
VIGNETTE 2:
A 65-year-old white man presents to his primary care physician in his normal state of health. He describes nocturia (1 episode per night) and a 3-hour daytime voiding interval. He denies any incontinence, hematuria, dysuria, frequency, or urgency. He has no gastrointestinal complaints.
WHAT SPECIFIC BLOOD MARKER WOULD YOU MEASURE IN THIS PATIENT?PSA
WHAT IS PSA AND WHY WOULD YOU MEASURE IT?
Prostate specific antigen – secreted by the epithelial cells of the prostate gland.
As indication of the size of the prostate gland.
NB Does not necessarily indicate Cancer!
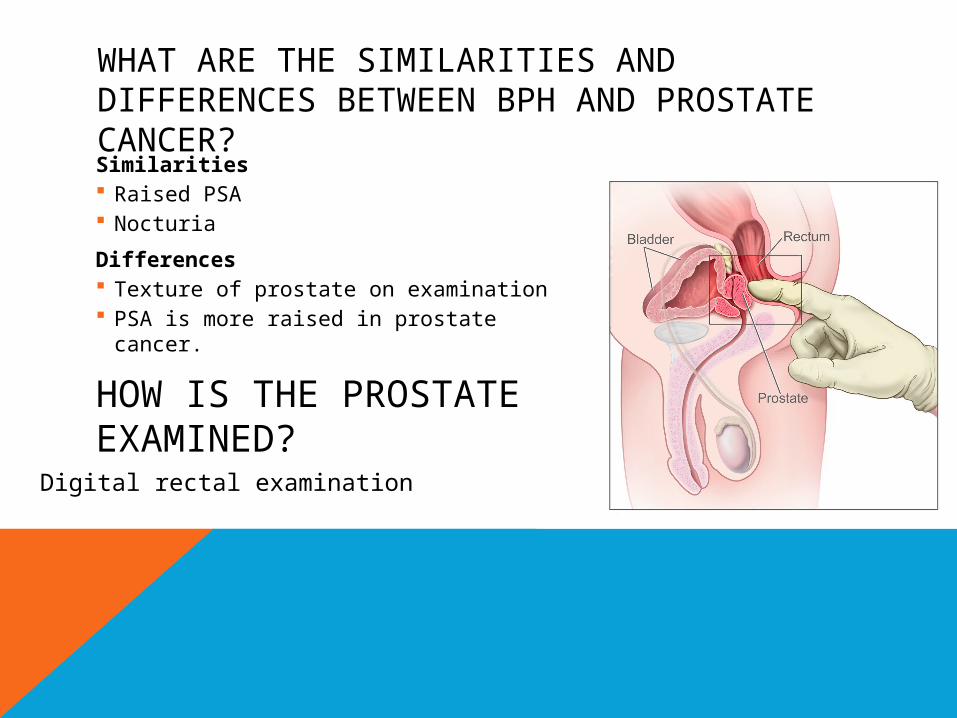
HOW IS THE PROSTATE EXAMINED?
Similarities Raised PSA Nocturia
Differences Texture of prostate on examination PSA is more raised in prostate cancer.
WHAT ARE THE SIMILARITIES AND DIFFERENCES BETWEEN BPH AND PROSTATE CANCER?
Digital rectal examination
HOW DO PROSTATE CANCER AND BPH DIFFER IN TEXTURE ON EXAMINATION?
BPH – smooth and regularProstate cancer – craggy and irregular
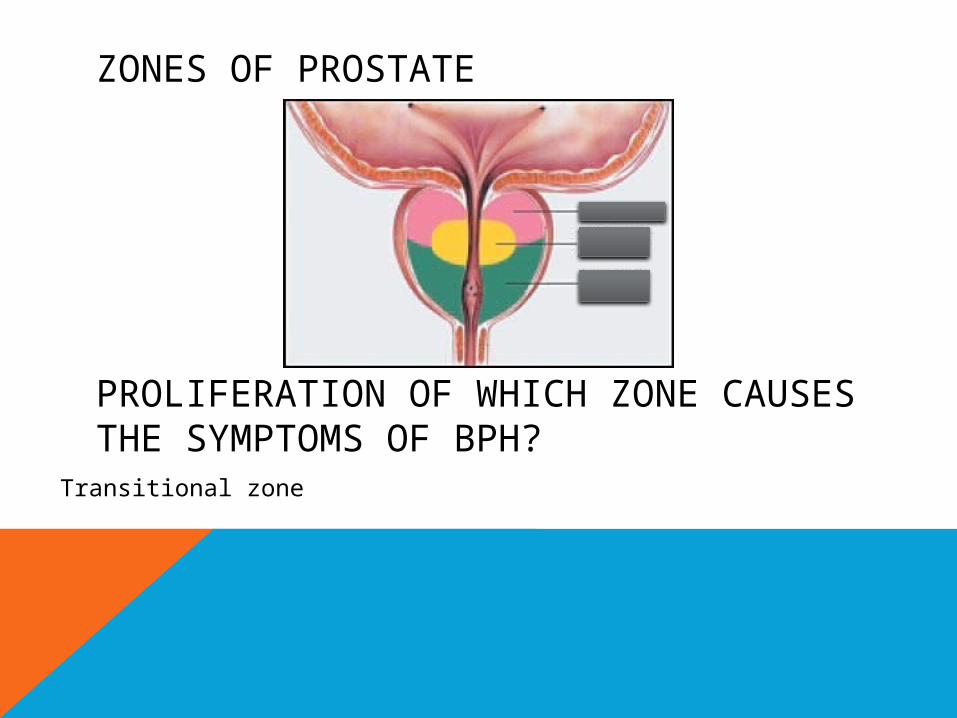
ZONES OF PROSTATE
PROLIFERATION OF WHICH ZONE CAUSES THE SYMPTOMS OF BPH?
Transitional zone
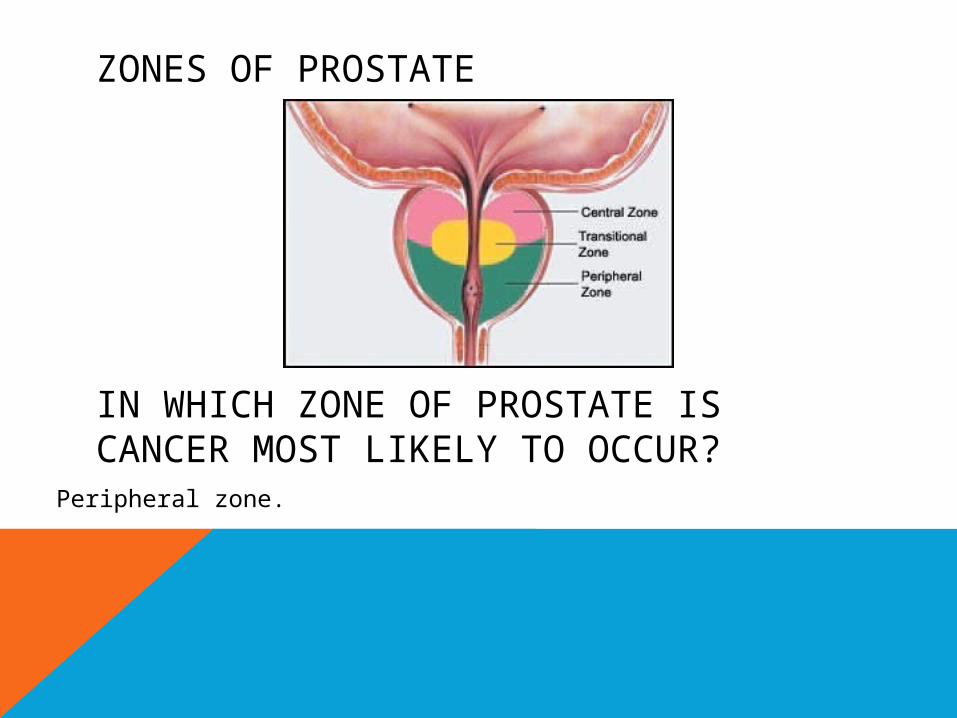
ZONES OF PROSTATE
IN WHICH ZONE OF PROSTATE IS CANCER MOST LIKELY TO OCCUR?
Peripheral zone.
VIGNETTE 2: CONT.
The man presents to A & E, having been unable to pass urine for 4 hours and is experiencing increasing pain in his lower abdomen.
WHAT DO YOU CALL THIS PRESENTATION?
Urine retention.
WHAT IS IT’S CAUSE?Hyperplasia (benign or malignant) of the prostate has occluded the prostatic urethra. Other causes of urinary retention could be calculi or blood clots.
WHAT IS THE IMMEDIATE MANAGEMENT REQUIRED?Catheterisation: urethral or suprapubic.
THANK EWE!







![A Key for Diabetes Management – A Review - Journalsbmrjournals.com/uploads... · sylvestre as a destroyer of Madhumeha [glycosuria and other urinary disorder]. ... Gymnema sylvestre](https://img.dokumen.tips/doc/110x75/5b61d0d87f8b9a36488cd369/a-key-for-diabetes-management-a-review-sylvestre-as-a-destroyer-of-madhumeha.jpg)