Embed Size (px)
Citation preview
CAUSES OF BLEEDINGCAUSES OF BLEEDING
• Defective clot formation Platelet plug Fibrin clot
• Excessive fibrinolysis• Vascular fragility

PLATELET DEFECTSPLATELET DEFECTS
• Thrombocytopenia Increased consumption (ITP, DIC) Decreased production (marrow disease, chemo)
• Defective platelet function (ASA, other drugs most common cause)
• Von Willebrand disease (defective platelet adhesion) Most common inherited bleeding disorder?

DEFECTS IN FIBRIN CLOT FORMATIONDEFECTS IN FIBRIN CLOT FORMATION
• Inherited deficiency of single clotting factor (hemophilia A or B)
• Acquired deficiency of multiple clotting factors Liver disease Vitamin K deficiency/warfarin DIC
• Circulating inhibitor Antibody to factor VIII Heparin
• Defective fibrin crosslinking (factor XIII deficiency - very rare)

EXCESSIVE FIBRINOLYSISEXCESSIVE FIBRINOLYSIS
• DIC• Thrombolytic drug administration• Inherited deficiency of fibrinolytic inhibitor (rare)

VASCULAR DISORDERS THAT CAN VASCULAR DISORDERS THAT CAN CAUSE BLEEDINGCAUSE BLEEDING
• Inherited defect in collagen formation (Ehlers Danlos syndrome)
• Acquired defect in collagen formation (scurvy) (mainly purpura)
• Infiltrative disease (amyloidosis)• Vasculitis (purpura only)

ASSESSMENT OF BLEEDING RISKASSESSMENT OF BLEEDING RISK• History & physical exam*• Platelet count*• Assessment of platelet function
Bleeding time Platelet Function Analysis
• Assessment of fibrin clot formation PT/INR* aPTT Thrombin time
• Assessment of fibrinolytic system
*Part of routine pre-op screen

USEFULNESS OF THE HISTORY IN SCREENING USEFULNESS OF THE HISTORY IN SCREENING FOR BLEEDING DISORDERSFOR BLEEDING DISORDERS
Odds ratios for presence/absence of bleeding disorder by multivariate analysis
Arch Intern Med 1995;155:1409
Symptom Odds ratio 95% CI
Family members with proven bleeding disorder 50.5 12.5-202.9Profuse bleeding from small wounds 30 8.1-111.1Profuse bleeding with tonsillectomy 11.5 1.2-111.9Easy bruising 9.9 3.0-32.3Profuse bleeding after surgery 5.8 1.3-26.4Muscle bleeding 4.8 0.7-31.4Frequent nosebleeds 3.8 0.9-15.7Profuse bleeding with tooth extraction 3.2 0.9-11.3History of blood in stool 2.8 0.7-11.7Family members with bleeding symptoms 2.5 0.7-9.4History of joint bleeding 2.5 0.6-10.2Menorrhagia 2.5 0.6-9.9Profuse bleeding with childbirth 2.1 0.3-13.5Frequent gum bleeding 0.7 0.3-2.0History of hematuria 0.5 0.1-2.3

FAMILY HISTORY IN BLEEDING FAMILY HISTORY IN BLEEDING DISORDERSDISORDERS
• von Willebrand disease: dominant inheritance, variable penetrance
• Hemophilia: sex linked inheritance, high penetrance• Other clotting factor deficiencies - recessive
inheritance
Family tree in hemophilia

PATTERNS OF BLEEDING IN HEMOSTATIC PATTERNS OF BLEEDING IN HEMOSTATIC DISORDERSDISORDERS
Platelet/vascular disorders
Coagulation factor deficiency
Onset Immediate Delayed
Deep tissueSkin, mucosal
surfacesLocation

PLATELET COUNT VS BLEEDING RISKPLATELET COUNT VS BLEEDING RISK
• Bleeding risk rises as platelet count falls below 100K• Plts > 50K safe for many invasive procedures
Higher count may be needed if procedure is “blind” and it would be difficult to achieve hemostasis mechanically
• Associated platelet function defects (eg, ASA), liver disease or DIC enhance risk
• Lower bleeding risk at a given platelet count if thrombocytopenia due to consumption (eg, ITP) vs decreased production

ASSESSMENT OF ASSESSMENT OF PLATELET/VASCULAR FUNCTION: PLATELET/VASCULAR FUNCTION:
THE BLEEDING TIMETHE BLEEDING TIME
• Advantages In vivo test; measures vascular as well as
platelet function• Disadvantages
Difficult to standardize Sensitivity and specificity relatively poor Does not predict bleeding risk

ASSESSMENT OF ASSESSMENT OF PLATELET/VASCULAR FUNCTION: PLATELET/VASCULAR FUNCTION: PLATELET FUNCTION ANALYSISPLATELET FUNCTION ANALYSIS
• Advantages In vitro test Well-standardized Better sensitivity and specificity
• Disadvantages Does not assess vascular function No data re: ability to predict bleeding risk
Consider testing when clinical picture or family history suggest bleeding disorder, platelet count normal, AND no concurrent disease or drug known to affect platelet function

FIBRIN CLOT FORMATIONFIBRIN CLOT FORMATION
Fibrin
Xa Va
TF VII(a)
XIa
VIIIa IXa
PLCa++
IIa
XII, HMWK, PK
?Not physiologically important
“Contact" system
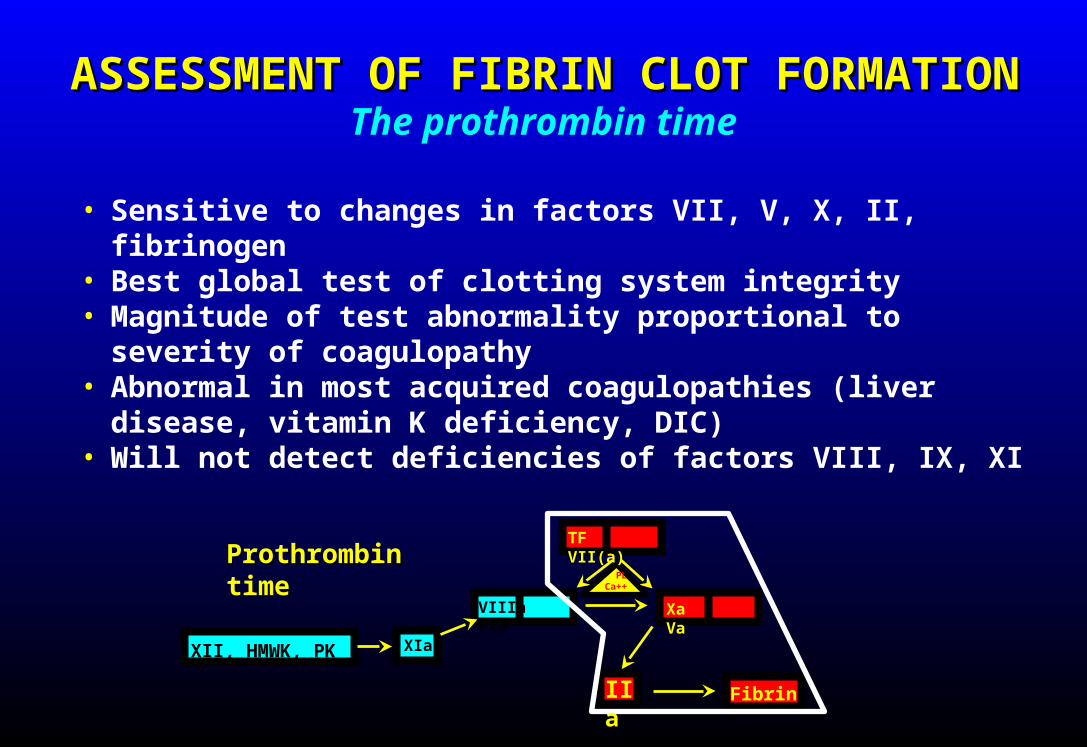
ASSESSMENT OF FIBRIN CLOT FORMATIONASSESSMENT OF FIBRIN CLOT FORMATION
• Sensitive to changes in factors VII, V, X, II, fibrinogen• Best global test of clotting system integrity• Magnitude of test abnormality proportional to severity
of coagulopathy• Abnormal in most acquired coagulopathies (liver
disease, vitamin K deficiency, DIC)• Will not detect deficiencies of factors VIII, IX, XI
The prothrombin time
XIaXII, HMWK, PK
ProthrombinProthrombin time
IIa
PLCa++
VIIIa IXa
TF VII(a)
Xa Va
Fibrin

ISI (International Sensitivity Index) is reagent- and method-specific; higher number indicates lower sensitivity to changes in clotting factor levels
INR = INR =
Patient PTPatient PTMean Normal PTMean Normal PT(( ))
ISIISI

INR = INR =
(( ))1.241.24
22.022.012.612.6
= 2.0= 2.0
INR = INR =
(( ))2.462.46
16.216.212.212.2
= 2.0= 2.0
Reagent A: ISI = 1.24, mean normal = 12.6 secReagent A: ISI = 1.24, mean normal = 12.6 sec
PT = 22 secPT = 22 sec
Reagent B: ISI = 2.46, mean normal = 12.2 secReagent B: ISI = 2.46, mean normal = 12.2 sec
PT = 16.2 secPT = 16.2 sec
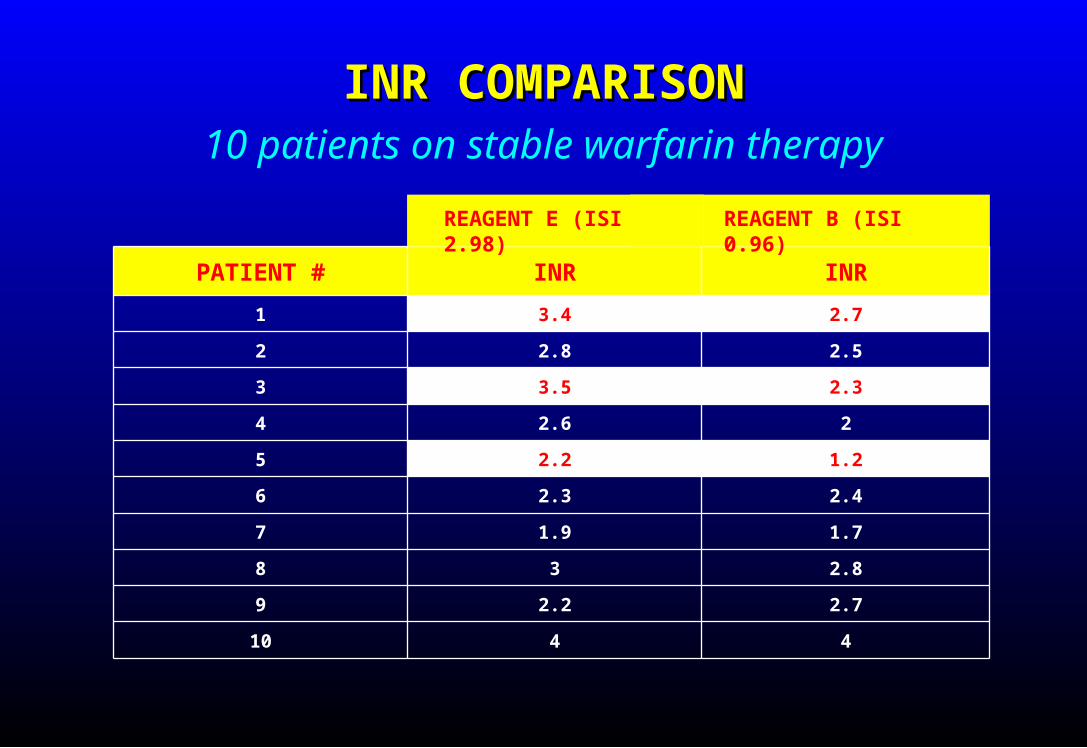
INR COMPARISONINR COMPARISON10 patients on stable warfarin therapy
PATIENT # INR INR
1 3.4 2.7
2 2.8 2.5
3 3.5 2.3
4 2.6 2
5 2.2 1.2
6 2.3 2.4
7 1.9 1.7
8 3 2.8
9 2.2 2.7
10 4 4
REAGENT E (ISI 2.98) REAGENT B (ISI 0.96)

DOES THE INR SYSTEM WORK IN LIVER DOES THE INR SYSTEM WORK IN LIVER DISEASE?DISEASE?
Comparison of three reagents
Thrombosis and Haemostasis 1994;71:727
Reagent (ISI) A (0.86) B (1.09) C (2.53)
Mean INR (warfarin pts)
2.63 2.75 2.67
Mean INR (liver disease)
1.88 2.17 2.63
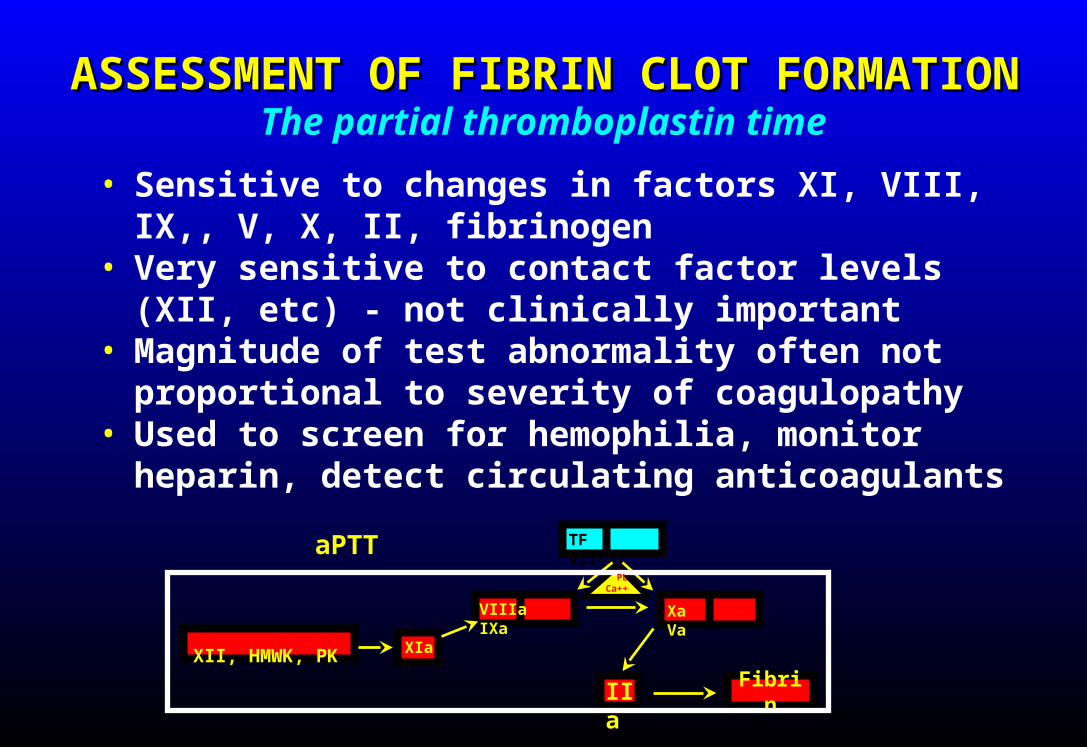
ASSESSMENT OF FIBRIN CLOT FORMATIONASSESSMENT OF FIBRIN CLOT FORMATION
• Sensitive to changes in factors XI, VIII, IX,, V, X, II, fibrinogen
• Very sensitive to contact factor levels (XII, etc) - not clinically important
• Magnitude of test abnormality often not proportional to severity of coagulopathy
• Used to screen for hemophilia, monitor heparin, detect circulating anticoagulants
The partial thromboplastin time
Fibrin
TF VII(a)
XII, HMWK, PK
aPTT
IIa
PLCa++
VIIIa IXa
XIa
Xa Va

RESULTS OF 1025 CONSECUTIVE aPTT MEASUREMENTSRESULTS OF 1025 CONSECUTIVE aPTT MEASUREMENTS(excluding those ordered for monitoring heparin)
Robbins and Rose, Ann Intern Med 1979;90:796
# TESTS # PATIENTSAbnormal result 143 97
On anticoagulant 64 37
Liver disease 41 27
No cause found, no bleeding 15 14
Normal on repeat testing 9 9Known hemophilia 5 4
History of intestinal bypass 5 4
Other malabsorption (CF) 2 1
Technical problem with test 1 1
Newly dx'd bleeding disorder 0 0
# abnormal: 143 (14%)

RESULTS OF PREOPERATIVE SCREENING RESULTS OF PREOPERATIVE SCREENING IN 1603 CHILDRENIN 1603 CHILDREN
Burk et al, Pediatrics 1992;89:691
PT, aPTT, BT, history
# with abnormal labs on repeat testing
13
# of those in whom bleeding disorder diagnosed (1 mild hemophilia, 1 VWD)
2
# in which bleeding disorder not apparent from history alone (mild hemophilia A)
1

The aPTT can help us decide why a patient is bleeding, but is much less
useful in predicting whether a patient will bleed
To bleed or not to bleed? is that the question for the PTT?

ASSESSMENT OF FIBRIN CLOT FORMATIONASSESSMENT OF FIBRIN CLOT FORMATION
• Measures only conversion of fibrinogen to fibrin, fibrin polymerization
• Very sensitive to heparin; normal or near-normal result essentially rules out heparin as cause of prolonged clotting times
The thrombin time
Xa Va
TF VII(a)
XIa
VIIIa IXa
PLCa++
XII, HMWK, PK
Thrombin time
IIa Fibrin
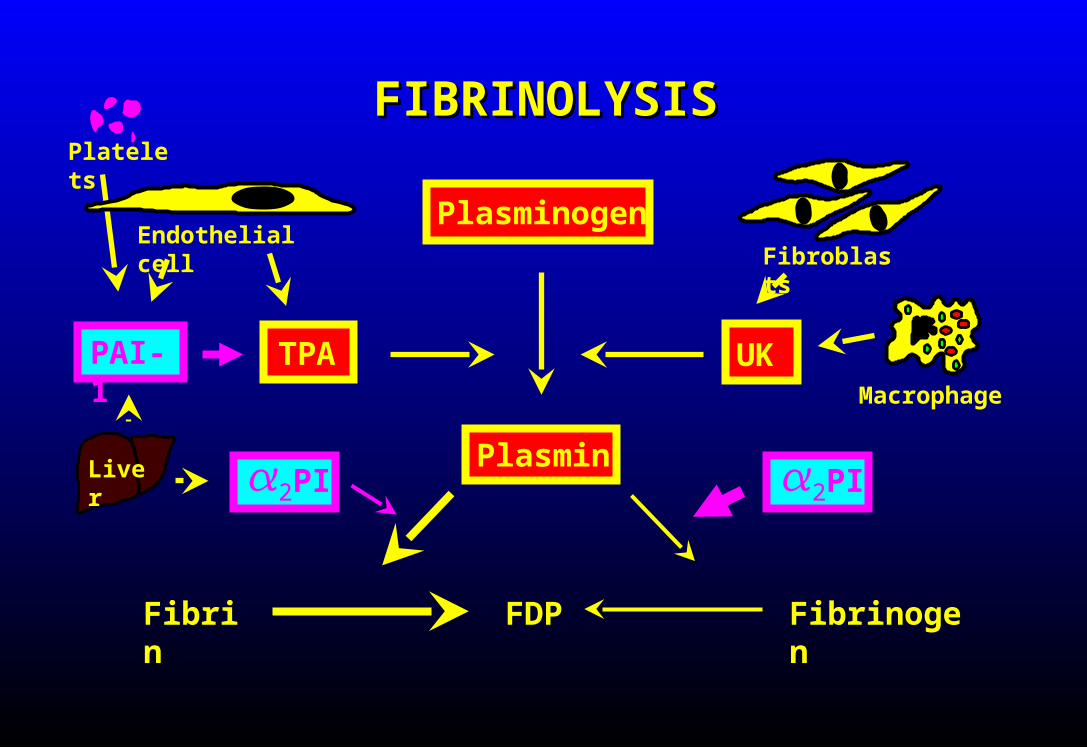
Plasminogen
Plasmin
TPA UK
Fibrin FDP Fibrinogen
2PI2PI
Endothelial cellFibroblasts
Macrophage
PAI-1
Liver
FIBRINOLYSISFIBRINOLYSISPlatelets

ASSESSMENT OF THE FIBRINOLYTIC ASSESSMENT OF THE FIBRINOLYTIC SYSTEMSYSTEM
• Euglobulin lysis time (not well standardized)• Alpha2-antiplasmin level* (depletion implies
poor fibrinolytic control)• PAI-1 activity
* Available at UW

Bleeding severity vs antiplasmin activityBleeding severity vs antiplasmin activitypatients with platelets > 30,000
< 50% 50-75% > 75%Antiplasmin activity
0
20
40
60
80
100
% o
f pat
ient
s
0-2+ bleeding
3-4+ bleeding
VON WILLEBRAND DISEASEVON WILLEBRAND DISEASE• Inherited deficiency or dysfunction of von Willebrand
factor Type I = partial quantitative deficiency Type II = partial qualitative deficiency Type III = severe deficiency
• Defective platelet adhesion, (slightly) decreased factor VIII activity
• Mild or moderate bleeding tendency in most type I and type II pts
• Diagnosis: von Willebrand antigen, factor VIII, ristocetin cofactor activity, platelet function analysis
• Treatment: DDAVP (type I); intermediate purity factor VIII concentrate (types II, III)

VARIABILITY IN VON WILLEBRAND FACTOR LEVELS OVER TIMEVARIABILITY IN VON WILLEBRAND FACTOR LEVELS OVER TIME
NORMALS TYPE I VWD
Abildgaard et al, Blood 1980;56:712

HEMOPHILIAHEMOPHILIA
• Inherited deficiency of factor VIII (Hemophilia A) or IX (Hemophilia B)
• Sex-linked inheritance: almost all patients male• Bleeding into joints, soft tissues; mucosal/skin/CNS
bleeding rare• Severity inversely proportional to factor level:
<1% = severe: frequent "spontaneous" bleeds 1-5% = moderate: spontaneous bleeding less common > 5% = mild: bleeding mainly after trauma/surgery; may
go undiagnosed until adulthood

HEMOPHILIAHEMOPHILIA
• Unexplained pain in a hemophiliac should be considered a bleed until proven otherwise
• External signs of bleeding may be absent, particularly early in course
• Treatment: factor replacement, pain control• 1 U/kg factor VIII should increase plasma level by
about 2%• Test for inhibitor if unexpectedly low response to
factor replacement
Treatment of bleeding episodes

HEMOPHILIAHEMOPHILIAFactor replacement in severe hemophilia A
Site of bleed Desired factor level Dose Other
Joint 40-50% 20-40 U/kg/day Rest, immobilization, PT
Muscle 40-50% 20-40 U/kg/dayRisk of compartment syndrome or neuro
compromise
Oral mucosa 50% initially 25 U/kg x 1Follow with
antifibrinolytic therapy
EpistaxisInitially 80-100%, then 30%
until healed40-50 U/kg then 30-40
U/kg dailyPressure, packing,
cautery
GIInitially 100%, then 30%
until healed40-50 U/kg then 30-40
U/kg dailyEndoscopy to find lesion
GUInitially100%, then 30%
until healed40-50 U/kg then 30-40
U/kg dailyR/O stones, UTI
CNSInitially100%, then 50%
until healed50 U/kg then 25 U/kg q
12h infusion
Trauma or surgeryInitially100%, then 50%
until healed50 U/kg then 25 U/kg q
12h infusionTest for inhibitor before
surgery!

VITAMIN K DEFICIENCYVITAMIN K DEFICIENCY
• Deficiency of factors II, VII, IX, X, protein C, protein S• Causes:
Decreased vitamin K intake Decreased production of vitamin by gut flora
(antibiotics) Poor absorption - sprue, biliary obstruction, etc Inhibition of vitamn K action (warfarin, certain
antibiotics)• Bleeding tendency roughly correlated to INR
• Treatment: vitamin K (oral or parenteral); FFP
<2 2.0-2.9 3-4.4 4.5-6.9 >7
INR
0
50
100
150
200
Ble
edin
g e
ven
ts/1
00 p
atie
nt-
yr

LIVER DISEASELIVER DISEASE
• Pathophysiology: Diminished synthesis of most clotting proteins
and inhibitors platelet sequestration low grade intravascular coagulation?
• Bleeding due to impaired fibrin formation and (in some cases) increased fibrinolytic activity
• INR, platelet count, antiplasmin level help predict bleeding risk
• Treatment: FFP, platelets, Amicar

COAGULATION INHIBITORSCOAGULATION INHIBITORS
• Heparin: prolongs thrombin time, aPTT, high levels prolong PT/INR
• Factor VIII antibodies: prolong aPTT only• Bovine thrombin antibodies: prolong all clotting
times, minimal bleeding• Lupus anticoagulant (does not cause bleeding)
• Diagnosis: prolonged clotting time that does not correct after mixing with normal plasma
• Treatment depends on type of inhibitor

THROMBOLYTIC DRUGSTHROMBOLYTIC DRUGS
• t-PA, streptokinase, urokinase, etc• Activate plasminogen, initiate fibrinolysis
Depletion of plasminogen may limit efficacy• Most lysis initially at surface of clot; antiplasmin
inhibits plasmin in blood Depletion of antiplasmin increases risk for systemic
fibrinolysis• Life-threatening bleeding may occur despite normal
fibrinogen, clotting times• Risk of bleeding greater with higher dose, longer
duration of therapy• Antidote: antifibrinolytic drug (Amicar)

DISSEMINATED INTRAVASCULAR DISSEMINATED INTRAVASCULAR COAGULATIONCOAGULATION
• Rapid formation and lysis of intravascular fibrin• Consumption of clotting factors, platelets, inhibitors• Lifethreatening underlying disease in most pts• Bleeding due to uncontrolled fibrinolysis,
thrombocytopenia, etc• Large vessel thrombosis unusual• Tissue necrosis due to microvascular occlusion,
hypotension, endothelial damage, direct effects of cytokines
• Most deaths due to underlying disease

DISSEMINATED INTRAVASCULAR DISSEMINATED INTRAVASCULAR COAGULATIONCOAGULATION
DIAGNOSISASSESS SEVERITY
GUIDE TREATMENT
D-Dimer Antithrombin Prothrombin time
Fibrinogen Plasminogen Fibrinogen
Prothrombin time Alpha2-antiplasmin Platelet count
Platelet count Protein C Alpha2-antiplasmin
Fibrin monomer

• TREAT UNDERLYING DISEASE!
• Clotting factor & inhibitor replacement IF patient bleeding or at high risk Fresh frozen plasma (if INR > 1.6) Cryoprecipitate (if fibrinogen < 50-100) Platelets (if count < 30-50K)
• Pharmacologic inhibitors (selected pts) Heparin Antifibrinolytics
TREATMENT OF DICTREATMENT OF DIC

PLATELET TRANSFUSIONPLATELET TRANSFUSION
• Plts < 20K (except ITP, TTP) Most beneficial in marrow failure states 10K trigger safe for most patients
• Plts < 50K AND significant bleeding OR invasive procedure/surgery planned within six hours
• Plts < 100K AND major CNS or eye surgery (up to 48 hours postop)
UWHC/VA TRANSFUSION INDICATIONSstandard adult dose = 5 units

FRESH FROZEN PLASMAFRESH FROZEN PLASMA
• Active bleeding and INR > 1.6• Invasive procedure planned within 6 hours and INR > 1.6• Immediate reversal of warfarin effect for emergency
surgery or active bleeding• Surgery with massive transfusion (> 10 units RBC/24
hours)• Replacement during plasmapheresis• TTP
UWHC/VA transfusion indications
adult dose = 10-15 ml/kg
Contains: all clotting factors and inhibitors
CRYOPRECIPITATECRYOPRECIPITATE
• Fibrinogen deficiency (<100 mg/dl) For DIC: give 1 bag/2-3 Units FFP
• Factor VIII or VWF deficiency Rarely used for this indication; factor
concentrates preferable• Fibrin glue
UWHC/VA transfusion indications
Contains: fibrinogen, factor VIII, von Willebrand factor

DDAVPDDAVP
• Vasopressin analog; stimulates VWF release from endothelium• Intravenous administration (0.3 mcg/kg); intranasal (Stimate)• Increased plasma VWF levels for 18-24 hours, enhanced
platelet adhesiveness• Effective in
Type I von Willebrand disease Mild hemophilia A (some cases) Other disorders of primary hemostasis (variable efficacy) Reducing surgical blood loss (conflicting data)
• Can give q 24 hours with little tachyphylaxis• Few side effects in adults (flushing, occasional hyponatremia,
rare thromboembolism)
(Desmopressin)

AMICARAMICAR
• Antifibrinolytic: Inhibits plasmin activation by tPA, fibrin degradation by plasmin
• Short plasma half-life; need frequent dosing, up to 24 gm/day• Oral, intravenous, or topical (mouthwash)• Uses:
Treatment of bleeding due to hyperfibrinolytic states: DIC, thrombolytic drugs, post cardiac bypass, liver disease
Prophylaxis in severely thrombocytopenic patients Treatment of GI or urinary tract bleeding Treatment of menorrhagia Prophylaxis after dental extractions in hemophilia
(mouthwash)• Risks & side effects: GI symptoms, orthostatic hypotension,
rhabdomyolysis, rarely thrombosis
(Epsilon-aminocaproic acid)
VITAMIN KVITAMIN K
• Oral, subcutaneous, or iv administration (potential for anaphylaxis with iv form)
• Indications: Correction of vitamin K deficiency Treatment of warfarin or superwarfarin overdose Treatment of warfarin-induced skin necrosis Prophylactic use in patients on TNA or at high risk for vitamin K
deficiency

REVERSAL OF WARFARIN REVERSAL OF WARFARIN ANTICOAGULATIONANTICOAGULATION
INR ACTION
< 6, no bleedingWithhold warfarin until INR therapeutic, restart at lower dose
< 6, rapid reversal needed for surgery, etc.
Vitamin K 1-2 mg po
6-10 or significant bleedingVitamin K 1-2 mg iv or 2.5-5 mg po; give additional 0.5-1.0 mg if INR still supratherapeutic at 24 hours
10-20Vitamin K 3 mg slow iv, recheck INR q 6h and repeat as needed
> 20Vitamin K 10 mg slow iv; repeat q 6-12 hours as needed
Add FFP for major bleeding if INR > 2 Avoid subcutaneous Vit K (unreliable absorption)





























