Embed Size (px)
Citation preview

E L S E V I E R Psychiatry Research: Neuroimaging 61 (1995) 209-229
P S Y C H I A T R Y R E S E A R C H
NEUROIMAGING
Caudate, putamen, and globus pallidus volume in schizophrenia: A quantitative MRI study
Hiroto H o k a m a a, Martha E. Shenton a, Paul G. Nestor a, Ron Kikinis b, James J. Levitt a, David Metcal f b, Cynthia G. Wible a, Brian F. O'Donnel l a,
Ferenc A. Jolesz b, Robert W. McCarley *a
aBrain Imaging Laboratory, Harvard Medical School Department of Psychiatry at Brockton~West Roxbury Veterans Affairs Medical Center and the Massachusetts Mental Health Center, Boston, MA, USA
bSurgical Planning Laboratory, Magnetic Resonance Imaging Division, Department of Radiology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA
Received 28 September 1994; revision received 13 March 1995; accepted 4 April 1995
Abstract
Basal ganglia structures have been reported to be abnormal in schizophrenia. However, while component structures of the basal ganglia are functionally differentiated, there have been no evaluations of their separate magnetic resonance imaging (MRI) volumes with small voxel (1.5 mm 3) spoiled gradient-recalled acquisition in steady state techniques and multi-plane assessments. We examined MRI scans from 15 male, right-handed, neuroleptic-medicated schizophre- nic patients and 15 age-, handedness-, and gender-matched normal volunteers. Compared with normal subjects, schizo- phrenic patients showed enlarged volumes: 14.2% for total basal ganglia, 27.4% for globus pallidus, 15.9% for putamen, and 9.5% for caudate. Increased volumes, especially of the caudate, were associated with poorer neuropsychological test performance on finger tapping and Hebb's Recurring Digits. These findings indicate abnormalities throughout all basal ganglia structures in at least a subgroup of schizophrenic patients.
Keywords: Basal ganglia; Magnetic resonance imaging; Neuropsychology
1. Introduction
Basal ganglia structures have become an impor- tant focus of attention for both basic neuroscience
* Corresponding author, Department of Psychiatry, 116A, Harvard Medical School and Brockton VAMC, 940 Belmont Street, Brockton, MA 02401, USA. Tel: +i 508 583-4500, ext. 3723; Fax: +! 508 586-0894.
studies and clinical neuroscience investigations re- lated to schizophrenia. Although there have been several important magnetic resonance imaging (MRI) studies (see below), separate quantification of the volumes of caudate, putamen, and globus pallidus (GP) has not been done with very high resolution techniques and only one study has pro- vided complete data on volumes (Elkashef et al., 1994) - - despite the clear recent neuroscience evi-
0925-4927/95/$09.50 © 1995 Elsevier Science Ireland Ltd. All rights reserved SSDI 0925-4927(95)02729-H

210 H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229
dence for differentiation of the functional roles of these structures.
More specifically, the input stages of the basal ganglia, primarily the caudate nucleus and putamen, receive excitatory glutamatergic projec- tions from multiple zones, including sensorimotor, cingulate, prefrontal, and insular cortices as well as amygdala (see reviews by Alexander and Crut- cher, 1990; Graybiel, 1990). These multiple inputs have led to the characterization of the basal ganglia as a "multilaned throughway for separate streams of influence over the thalamus and motor structures..." (Goldman-Rakic and Selemon, 1990). The output nuclei of this multilaned throughway consist primarily of the internal seg- ment of the GP and the substantia nigra pars reticulata. Their neurons, via 3,-aminobutyric acid (GABA), exert a tonic inhibitory effect on their target thalamic nuclei, including the ventral ante- rior, ventral lateral, and mediodorsal groups. Input- output coupling in the basal ganglia is (1) by a direct pathway that inhibits output neurons (via GABA and Substance P) and (2) by an indirect pathway: --* the external segment of the GP --* glutamatergic subthalamic nucleus neurons --* neurons in the output nuclei. Modulatory dopaminergic projections from the substantia nigra pars compacta (and also A8) are to the caudate and putamen (striatum) but not to the GP.
The basal ganglia are also now thought to parti- cipate in extensive parallel processing in different functional domains (as well as having parallel pro- cessing within each domain). Each functional do- main is characterized by output links to appro- priate frontal cortex zones for skeletomotor (pri- mary and supplementary motor cortex), oculo- motor (frontal eye fields), cognitive (dorsolateral and lateral orbital prefrontal cortex), and limbic processing (anterior cingulate and medial or- bitofrontal cortex), as reviewed by Chevalier and Deniau (1990) and by Goldman-Rakic and Selemon (1990). It is thus clear that the earlier focus on the basal ganglia as primarily involved in motor functions was too narrow and has been ex- panded to include important cognitive, oculo- motor, and limbic processing as well - - all of which may be important in disorders such as schizophrenia.
Within the field of schizophrenia, extensive dopaminergic input to the striatum, as well as the therapeutic effectiveness of neuroleptics acting on dopamine receptors, stimulates numerous PET functional imaging studies of this region which suggest dopamine receptor abnormalities (for a re- view and discussion, see Sceman et al., 1993).
Carlsson and Carlsson (1990), drawing on the intimate interrelationships between glutamatergic and dopaminergic synapses in the basal ganglia, as well as on data collected from animal phar- macological studies, suggest that a primary abnor- mality of schizophrenia may involve glutamatergic neurotransmission, especially that acting on the basal ganglia by the circuitry described above. Modulatory neurotransmitters such as dopamine may thus act to ameliorate this primary abnor- mality, especially through their basal ganglia ef- fects. Other neural models of schizophrenic pathology have emphasized basal ganglia control over "gating" of sensory stimuli, such as those im- portant for startle, through basal ganglia connec- tions with thalamus and brainstem (e.g., Swerdlow and Koob, 1987; Potkin et al., 1993).
Finally, the phenomenology of schizophrenia includes types of movement disorder associated with basal ganglia dysfunction. Unusual postur- ing, grimacing, and other dyskinesias were ob- served in schizophrenic patients long before the era of neuroleptic therapy and are, in fact, richly illustrated in Kraepelin's (1919/1971) classic photographs of schizophrenic patients.
Thus, the presence and nature of structural ab- normalities in the basal ganglia are of great in- terest in the investigation of schizophrenia, and two reports in this field have been especially seminal. The study by Jeruigan et al. (1991) was the first to present MRI data indicating enlarge- ment of the lenticular nuclei (putamen + GP) in living schizophrenic patients, with a 13% increase in age- and head size-corrected volumes compared with those in normal volunteers; caudate volume was not altered in their samples. Larger lenticular volumes were associated with an earlier onset of schizophrenia, suggesting the possibility of a pro- gressive enlargement. Their MRI technology did not, however, allow direct measurement of total volume. They used 5-ram axial slices with 2.5-mm

H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229 211
gaps. In the same year, however, a post-mortem study on older schizophrenic subjects (mean age = 62 years) by Heckers et al. (1991) found that schizophrenic patients had, compared with age- matched control subjects, a bilateral 9% increase in the volume of striatum (caudate + putamen + nucleus accumbens) and a bilateral 14% increase in the volume of the GP.
Since the MRI report of Jernigan et al. (1991), Breier et al. (1992) found a 10% increase in left caudate volume in schizophrenic patients. Buch- anan et al. (1993) used the same patients and MRI scans, but they compared deficit and nondeficit patient subgroups. They reported that while there was no difference in left caudate volume, there was a trend for the deficit subgroup to have a larger right caudate than nondeficit patients (8% increase vs. 2% volume decrease, respectively, compared with normal volunteers). Region of interest (ROI) evaluations were exclusively on coronal slices. Al- though none of the studies thus far cited included putamen and GP measurements, bilaterally in- creased putamen volume in males (10%) has been reported in a study using thick (1-cm) slices and planimetric measurements on film (Swayze et al., 1992). This study also reported a trend for bi- lateral caudate enlargement (11%), as did an earlier first episode study (DeLisi et al., 1991). Elkashef et al. (1994) recently reported volume in- creases of putamen and GP using 5-mrn axial slices, and they found a trend for caudate enlarge- ment using 3-mm slices in a subset of the Breier et al. (1992) patient group.
With respect to the onset time and cause of in- creased volumes, Chakos et al. (1994) have noted, compared with normal volunteers, caudate en- largement in first episode schizophrenic patients and a further increase in caudate volume in 18- month follow-up scans. The degree of schizo- phrenic volume increase was correlated with a longer time to remission and a larger cumulative neuroleptic dosage, raising the possibility of a neuroleptic-induced effect.
As this survey of MRI studies of basal ganglia in schizophrenic and normal comparison groups indicates, no studies have used the power afforded by the most recent MRI technology, which in- cludes the precision available in 1.5 mm 3 voxels
and three-dimensional reconstruction/slicing techniques, to allow comparison of ROI defini- tions in multiple planes. Use of these advanced techniques to provide quantification of the volumes of caudate, putamen, and GP as separate ROIs seems an important consideration in view of the evidence for different functional roles. Also, there has been little use of clinical scale measurements and neuropsychological assessment in conjunction with volumetric MRI measure- ments so as to permit delineation of the functional cognitive abnormalities that might be associated with basal ganglia structural abnormalities in schizophrenic patients, Finally, the reports of no enlargement in a number of MRI studies (e.g., Kelsoe et al., 1988; Mion et al., 1991; Young et al., 1991), while perhaps attributable to subject popu- lation differences, also emphasize the need for a study done with the most sensitive and accurate technology (Kikinis et al., 1992).
We thus examined volumes of caudate, putamen, and GP using the latest generation of MRI technology in conjunction with clinical scale and neuropsychological assessment of a group of chronic schizophrenic patients. We here report that, compared with the age-matched normal com- parison group, schizophrenic patients showed an increase in all basal ganglia volumes, most pro- minently in the GP (27%), but also in the putamen (16%) and in the caudate (10%).
2. Methods
2.1. Subjects MR scans from 15 schizophrenic and 15 control
subjects, all right-handed males, were obtained from a previous study, which provides further details about the subjects and MRI methodology (see Shenton et al., 1992). Schizophrenic subjects were recruited from the Brockton Veterans Affairs Medical Center; 13 were hospitalized and 2 were in VA foster homes. They had a mean age of onset of 22.3 years (SD = 2.8), mean duration of illness of 15.7 years (SD = 8.8), and a mean time hospitaliz- ed of 7.1 years (SD = 4.6). Patient diagnoses were made in accord with DSM-III-R criteria (Ameri- can Psychiatric Association, 1987) on the basis of chart review and information obtained from ad-

212 H. Hokama et al . / Psychiatry Research: Neuroimaging 61 (1995) 209-229
ministration of the Schedule for Affective Dis- orders and Schizophrenia (Spitzer and Endicott, 1978).
All schizophrenic subjects were receiving neuroleptic medication (chlorpromazine-equival- ent mean = 881 mg/day, SD = 683). Available medical records and data from the subjects in- dicated that neuroleptic medication had been prescribed throughout the entire course of illness, although they did not permit a reconstruction of a complete medication history. Comparison subjects were recruited through newspaper advertisements. All subjects were between the ages of 20 and 55 years with no history of electroconvulsive shock treatment, neurologic illness, or steroid use, and no lifetime history of drug/alcohol addiction or abuse (as defined in DSM-III-R) within the last 5 years. Comparison subjects were also excluded if they had a history of psychiatric illness in themselves or in their first-degree relatives. All subjects gave informed consent before participa- tion in the study.
There was careful age matching in the two groups, with each pair matched to within 2 years, save for one difference of 3 years; mean age for the schizophrenic patients was 37.6 years (SD = 9.3), while that for the normal volunteers was 37.9 years (SD = 9.8). There were no statistically significant differences between the two groups in height, weight, head circumference, socioeconomic status (SES) of family of origin, or scores on the Wechler Adult Intelligence Scale-Revised (WAIS-R) Infor- mation subscale (Wechsler, 1981). There was a dif- ference between groups in educational level. However, matching on educational level may lead to groups that are unmatched in premorbid ability levels due to the fact that schizophrenic subjects may start to show symptoms at the time when they would normally be finishing high school and going on to college. We therefore matched subjects on parental SES level and WAIS-R Information subscale score, both of which are likely to corre- spond better with premorbid functioning.
2.2. Clinical evaluations Three instruments were used to assess type and
severity of symptoms: The Scale for the Assess- ment of Positive Symptoms (SAPS; Andreasen, 1984), the Scale for the Assessment of Negative
Symptoms (SANS; Andreasen, 1981), and the Thought Disorder Index (TDI; Johnston and Holzman, 1979). The average score on the TDI was 60; normal subjects score < 5. On the basis of the Andreasen classification, 11 of the 15 patients were characterized as having mainly positive symptoms, and four patients were characterized as having mixed symptoms. None of the patients had predominantly negative symptoms, but some nega- tive symptoms were present (mean SANS score = 9.1).
2.3. Movement disorder evaluation Nine of the 15 schizophrenic subjects had for-
mal motor evaluations on the Abnormal Involun- tary Movement Scale (AIMS; Guy, 1976), the Simpson-Angus rating scale (Simpson and Angus, 1970) for extrapyramidal symptoms, and the Brande et al. (1983) akathisia scale.
2.4. Neuropsychological evaluation For comparative purposes, we examined perfor-
mance in this study with the same battery of neuropsychological tests of memory, attention, and abstraction that we found previously to be correlated with volumetric variations in gray mat- ter temporal and frontal lobe structures in the schizophrenic patients (see Nestor et al., 1993, 1994). These measures included: (1) verbal memory, as assessed by the Verbal Paired Associates subtest of the Wechsler Memory Scale- Revised (WMS-R; Wechsler, 1987) (correlated with left temporal lobe ROI volume reductions [Nestor et al., 1993]); (2) abstraction/categoriza- tion, as assessed by both the Similarities subtest of the WAIS-R (Wechsler, 1981) and the number of categories achieved on the Wisconsin Card Sorting Test (WCST; Heaton, 1981) (both previously found to be correlated with bilateral temporal lobe ROI volume reductions [Nestor et al., 1993]); and (3) attention-related processes of temporary storage, as assessed by Hebb's Recurring Digits (Hebb, 1961), and switching, as assessed by Trail- Making Test B and Alternating Semantic Categories (Reitan and Wolfson, 1985) (both previously found to be correlated with variations in volumes of bilateral frontal lobe ROIs [Nestor et al., 1994]).
In addition, given the relationship of basal ganglia to motor control, we examined the rela-

H, Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229 213
tionship of basal ganglia structures to motor speed and dexterity, as assessed by the Finger Tapping Test (Reitan and Wolfson, 1985). Our previous work demonstrated performance on this test was not correlated with Other frontal or temporal lobe volumes in patients with schizophrenia.
Verbal associative memory and learning. The Verbal Paired Associates subtest of the WMS-R presented subjects with eight word pairs, half of which were highly associated (e.g., baby-cries) and half which had a low association (e.g., school- grocery).
Abstraction and categorization. The Similarities subtest of the WAIS-R required the subject to determine how various pairs of words (e.g., dog/lion, fly/tree) were alike. The WCST involved sorting 128 response cards, each of which has a geometric figure that may vary along three dimen- sions (color, form, and number). The task was to sort the cards according to a specific principle (color, form, or number), which the subject had to deduce on the basis of performance feedback.
.4 ttention-related processes of temporary memory storage. Temporary storage was measured by Hebb's Recurring Digits, which may be viewed as a modified digit span test. The subject's immediate digit span (maximum number of digits recalled) was established. Subjects were then asked to re- peat sets of orally presented strings of digits, each of which was one digit longer than their immediate digit span. Without the subjects' knowledge, the same string of numbers was repeated on every third trial. Twenty-four trials were presented, eight of which were repeating strings. The percentage of numbers recalled in the correct sequence for each of the eight recurring trials was used as an index of temporary storage.
Attention switching. Two measures were used: The Trail-Making Test B, a timed pencil-and- paper task, required that subjects connect alter- nating numbered and lettered circles in sequence (e.g., 1, A, 2, B, 3, C...). For the Alternating Semantic Categories, subjects were given 60 s to say as many names as possible while alternating between exemplars in two distinct categories (i.e., boys' names and fruits; e.g., Paul-Orange, Bob- Apple).
Motor functions. The Finger Tapping Test pro- vided a relatively pure measure of motor speed and
dexterity. Subjects pressed a lever with their index finger as rapidly as possible, and the number of taps was recorded. There were five 10-s trials for each hand.
2.5. MRI methodology All MR scans were acquired at the Brigham and
Women's Hospital o n a 1.5-Tesla General Electric SIGNA System (GE Medical Systems, Milwaukee, WI). The MR methodology has been described in detail (see Shenton et al., 1992) and is therefore more briefly described here. For the measurement of specific ROIs, a three-dimensional Fourier transform spoiled gradient-recalled acquisition in steady state (SPGR) was used to obtain scans throughout the entire brain which were reformat- ted into 124 contiguous 1.5-mm coronal slices. This protocol creates images with excellent gray/white matter contrast. The SPGR images were obtained with the following parameters: echo time (TE) = 5 ms, repetition time (TR) = 35 ms, one repetition, nutation angle = 45 °, field of view = 24 cm, acquisition matrix = 256 x 256 x 124, voxel dimensions = 0.9375 x 0.9375 x 1.5 nun.
For the measurement of the intracranial con- tents (e.g., whole gray matter, white matter, and cerebrospinal fluid [CSF]), 108 (54 for each echo) contiguous double-echo, spin-echo 3-ram axial slices were obtained throughout the extent of the brain. Imaging parameters were: TE = 30 and 80 ms, TR = 3000 ms, field of view = 24 cm, acquisi- tion matrix = 256 x 256, voxel dimensions = 0.9375 x 0.9375 x 3 mm. The data for whole brain volume have been presented elsewhere (see Shenton et al., 1992). No gross abnormalities were observed in any of the scans (normal subjects or schizophrenic patients) when they were evaluated by a clinical neuroradiologist.
2.6. Image processing The image-processing stages were slightly dif-
ferent for the whole brain than for the individual ROI measurements (e.g., basal ganglia ROD. The semiautomated image-processing procedures for the measurement of intracranial content (used to compute the relative volume measurements) were based on the 3-ram double-echo axial scans and are described elsewhere (see Cline et al., 1987,

214 H. Hokama et al . / Psychiatry Research." Neuroimaging 61 (1995) 209-229
A
13

H. Hokama et al./ Psychiatry Research: Neuroimaging 61 (1995) 209-229 215
1988, 1990; Kikinis et al., 1992; Shenton et al., 1992). The algorithms used for postprocessing of MR images are part of the MRX software package, a joint project of GE Medical Systems, Schnectedy, NY, and the Surgical Planning Labo- ratory of the Brigham and Women's Hospital. They were also used for SPGR image evaluation and included: (1) a preprocessing filter; (2) a non- parametric clustering algorithm for classifying voxels as to tissue type (i.e., CSF, gray and white matter) on the basis of double-echo intensity infor- mation; (3) a connectivity algorithm for linking regions of similar tissue type; (4) voxel summation for computing volumes; and (5) three-dimensional reconstructions for ROI visualization.
The postprocessing steps for basal ganglia ROI volume measurements were done on the SPGR im- ages. The first step was to filter the images to reduce noise. Then, after separation of brain and surrounding CSF from skull and tissue bridges, the images were segmented into CSF, gray matter, and white matter on the basis of operator-selected sample points and a nonparametric clustering al- gorithm. Finally, this segmentation was used as the basis for operator outlining of the basal ganglia ROI, as defined below, on a slice-by-slice basis, with continuous cross-reference of coronal (best for dorsoventral margins) and axial (best for anterior-posterior and some mediolateral margins) slices on the computer workstation screen. The slice editor of the MRX image-processing program contained algorithms to perform manual drawing of ROI, connectivity, island removal, erosion and dilation of tissue classes; a color editor to assign colors to different ROIs; and a magnifier to magnify the image to a user-chosen level of magnification. An especially useful feature is the capability for virtual reslicing of the slice series so that the user may operate on any plane or thickness, with preservation of ROI boundaries defined in another plane (see Metcalf, 1995), allowing the "best view" of any anatomical struc- ture to be used for editing and definition of ROIs.
A dividing cubes algorithm was used to reconstruct the segmented ROls to allow for a three-dimensional view of each tissue class (Cline et al., 1988, 1990). Finally, the voxels for each tis- sue class were summed to compute the volume for each slice and the cumulative volume.
2. 7. Overview of ROI definition Crosby et al. (1962), Carpenter (1978), and
Duvernoy (1991) were used as primary anatomical references. Throughout the development of the ROIs, we were quite conscious of partial volume (PV) constraints on reliability: when voxels in- clude more than one tissue component, such as both gray and white matter, reliability is greatly reduced. Our rule was that if reliable tracing of the boundaries of a portion of a ROI could not be per- formed, this portion was excluded from analysis (such as most of the tail of the caudate - - see ROI descriptions below). The basic definitions of land- marks used for the basal ganglia ROI (caudate, putamen, and GP) are described below, and a more detailed description is available in the Ap- pendix, which illustrates the entire extent of ROIs on coronal slices for one case.
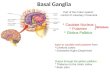
Caudate nucleus. This ROI included the head and body of the caudate and the tail portion as it curved ventrally abutting the lateral portion of the atrium of the ventricle (Figs. la and lb). Tracing of the tail portion stopped when it turned to course anteriorly, since, even with our small vox- els, PV effects rendered more extensive tracing unreliable. The caudate ROI also included most of the nucleus accumbens; the accumbens is on- togenetically and phylogenetically related to the caudate-putamen and cannot be reliably differen- tiated on MR images.
Putamen. This included its ventral extension, termed the peduncle of the lentiform nucleus (see Fig. 1).
Globus pallidus. The medial and lateral GP are separated by a very thin white matter layer (medial medullary lamina) which, because of its thinness
Fig. 1. A: Coronal MRI slice illustrating region of interest of caudate (yellow outline), putamen (red outline), and globus pallidus (orange, medial). The green line indicates the plane of B. B: Axial reconstruction showing head and tail of caudate and lenticular form of putamen/globus pallidus. Green line indicates plane of A.

216 H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229
and consequent PV effects, is lumped together with medial and lateral GP to form the GP ROI (see Fig. 1).
2.8. Reliability Anterior-posterior boundaries. Each of three
raters was within ± one 1.5-mm slice for all three ROIs.
Intrarater reliability. H.H. measured all cases. Reliability was assessed by duplicate measure- ments, 6 months apart, by H.H. on the entire data set of two randomly selected cases. There was an excellent agreement for caudate (4.4% and 4.3% volume differences on the two cases for the two measurements), putamen (2.0% and 3.2% differ- ences), and GP (0.5% difference for both cases).
Segmentation reliability. The excellent reliability measurements for the segmentation of total gray matter, white matter, and CSF on the double- echo/spin-echo images have been described elsewhere (Kikinis et al., 1992; Shenton et al., 1992).
2.9. Statistical analyses Volumetric analyses were corrected for intracra-
niai volume to control for variations in head size. As described elsewhere (Shenton et al., 1992), there were no group differences between the nor- mal volunteers and the schizophrenic patients on total intracranial contents, total CSF, total gray matter, or total white matter. All tests for statistical significance of ROI volume differences were performed on corrected (relative) volumes (ROI volume/intracranial contents); the results of statistical significance tests for absolute volumes are also reported where these substantially differed from tests on relative volumes. For comparative purposes, we also present absolute volume data. Laterality and region effects for basal ganglia ROIs were examined by a mixed-model analysis of variance with one between factor, group (schizo- phrenic vs. normal), and two within factors, laterality (left vs. right), and region (caudate, putamen, GP). This analysis was followed by planned comparisons with statistical significance set at P < 0.05. Based on the literature, we used one-tailed t tests for comparisons because we hypothesized that schizophrenic patients would
show an increase in basal ganglia volume. Al- though the normal volunteers and schizophrenic patients were closely matched (see below), we con- servatively used unpaired t tests.
As age can affect volumetric measures, even within a restricted age range (Zipursky et al., 1992), age comparability of normal and schizo- phrenic groups is important. This is especially critical for basal ganglia measurements, since one hypothesis derived from the literature is that nor- mal subjects will show a trend for age-related reduction in relative volume whereas schizophre- nic patients will show volume increases - - in- creases related to the disease process and/or to neuroleptic medication, and hence be progressive with time. We emphasize the scrupulous age matching of our two groups as a critical control for age confounds. (Since the two groups are predicted to show different age-basal ganglia volume relationships, a covariance control is not appropriate.)
For correlations among neuroanatomical, neuropsychological, and clinical/motor measures within groups, the nonparametric Spearman's rho (r) and two-tailed significance tests were used. For these correlations, relative ROI volumes were always used to correct for head-size differences. Because of the multiple correlations performed, the analyses of the relationship between basal ganglia ROI and the neuropsychological and clini- cal/motor measures are to be regarded as ex- ploratory and in need of confirmation in another study.
3. Results
3.1. Basal ganglia Basal ganglia volumes. The total volume of the
basal ganglia was increased by 14.2% in the schizo- phrenic group compared with the normal com- parison group, a statistically significant increase (P < 0.007, see Table 1). The analysis of variance also showed a significant laterality effect, with larger left-sided structures (F = 5.563; df= 1, 28; P = 0.0256). This laterality effect did not differ in the two groups (laterality x group interaction: P = 0.238). There was a significant region x later- ality interaction (F = 5.586; df= 2, 56; P = 0.007),

H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229
Table 1 Basal ganglia absolute volumes (in ml) in schizophrenic patients and normal subjects
217
Structure Schizophrenic patients Normal subjects Increase in schizophrenia
Mean SD Mean SD (%)
Statistical significance
Basal ganglia Total 22.56 1.77 Caudate nucleus Total 9.99 ! .09 Left 5.00 0.55
Right 5.00 0.55 Putamen Total 9.70 0.77 Left 4.92 0.50
Right 4.78 0.32 Globus pallidus Total 2.87 0.37 Left 1.41 0.20
Right ! .46 0.20
19.75 2.18 14.2
9.13 1.13 9.5 4.58 0.57 9.0 4.55 0.57 9.9
8.37 1.09 15.9 4.28 0.61 15.0
4.10 0.50 16.8
2.26 0.33 27.4 1.15 0.19 23.2
1.11 0.17 31.6
F = 8.53; df= 1, 28; P = 0.007
t = !.33, P = 0.098 t = 1.24, P = 0.113
t = 1.40, P = 0.087
t = 3.04, P = 0.0025 t = 2.56, P = 0.002 t = 3.34, P = 0.001
t = 3.82, P = 0.0005 t = 3.26, P = 0.0015 t = 3.48, P = 0.001
Note. Statistical significance levels are based on relative volumes; t-tests are l-tailed.
indicating that the three basal ganglia structures differed in the degree of lateralization, with the putamen being most lateralized. Schizophrenic pa- tients and normal volunteers did not, however, dif- fer in the degree of region x laterality interaction (region x laterality x group: P = 0.872). Since the two groups did not differ in laterality effects, subsequent volumetric data presentations are based on combined left and right structures.
Table 1 shows that the schizophrenic group, compared with the normal comparison group, had a volume increase of 9.5% in the caudate, 15.9% in the putamen, and 27.4% in the GP. When relative volumes were analyzed, t tests revealed that the GP and the putamen were statistically different in schizophrenic patients and normal volunteers (Ps < 0.003); caudate volumes differed at the trend level when relative volumes were used; but when absolute volumes were used in the comparison, the P value was 0.02 (t = 2.24). These volume differ- ences were sufficiently great to be visible in three- dimensional reconstructions. Fig. 2 provides color-coded three-dimensional volume renderings of caudate (red), putamen (green), and GP (violet) for the schizophrenic subject (viewer left) and the
control subject (viewer fight) whose total basal ganglia volumes fell just above and closest to their respective group means. There was no region x group interaction ( F = 1.408; df=2, 56; P = 0.253), indicating that the degree of regional volume differences (i.e., 9.5%, 15.9%, versus 27.4%) did not reach statistical significance.
Fig. 3 illustrates the mean volume differences in a bar graph and provides the individual volume values for each member of the schizophrenic and normal groups for the caudate, putamen, and GP. The individual values show that the group mean differences are not the result of outliers, but stem from an overall population shift in values. Par- ticularly remarkable are the population differences on the putamen and GP volumes, where all members of the schizophrenic group have values above both the mean and median of the normal group.
Correlations between basal ganglia volume ROIs for normal volunteers and schizophrenic patients. With respect to correlations between the volumes of basal ganglia ROIs, our hypothesis was that the same abnormal process acted on all these struc- tures to increase volume relative to normal values.

218 H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229
Fig. 2. Color-coded three-dimensional volume renderings of caudate (red), putamen (green), and globus pallidus (violet) for the schizophrenic subject (viewer left) and the normal subject (viewer right) whose total basal ganglia volumes fell just above and closest to their respective group means. Note the visually greater volumes in the schizophrenic subject.
We reasoned that evidence for this common ab- normal process would consist of higher correla- tions between volumes in schizophrenic patients relative to those found in normal subjects, since a common abnormal process would leave a "foot- print" in a joint and hence correlated change in the different basal ganglia structures. In contrast, in normal subjects, multiple independent processes
would be acting to control volume and hence inter- correlations would be less. To correct for total in- tracranial volume differences, we used relative volumes and Spearman rank-order correlations to control for nonnormality of statistical distribu- tions. Table 2 shows the matrix of intercorrela- tions between the basal ganglia ROIs for the schizophrenic and normal groups (the correlations

_¢
Z @
10.0
5.0
0.0
H. Hokama et al. / Psychiatry Research,: Neuroimaging 61 (1995) 209-229
4.0
1o.o
i S.O
0.0
3.0
.~ 2.0
1.0
o
©
©
' 09 ! i
Sz Control Sz Control Sz Control
219
Fig. 3. Bar graph of schizophrenic and control group mean values and standard errors of the mean overlaid with individual subject volume values (open circles) for the caudate, putamen, and globus pallidus. See text for further discussion.
between left and right sides of the same structure are omitted since our hypothesis addresses between- and not within-structure correlations). There was a statistical trend for the correlation
coefficients for the schizophrenic group to be larger than those of the normal group (P = 0.07, Wilcoxon matched-pairs signed rank test, a non- parametric test that uses the ranks of the
Table 2 Spearman correlation coefficients between relative volumes of basal ganglia components for the schizophrenic group (boldfaced type) and for the normal group (P values are below the r values, in parentheses)
Caudate Putamen GIobus pallidus
Left Right Left Right Left Right
Caudate Left
Right
Putamen Left
Right
Globus pallidus Left
Right
E
0.47 0.54 (0.076) (0.040) 0.40 0.48 (0.138) (0.069)
0.69 0.61 0.46 0.49 (0.007) (0.020) (0.094) (0.078) 0.70 0.61 0.45 0.53 (0.005) (0.021 ) (0.111 ) (0.052)
0.14 0.28 0.51 0.44 (0.627) (0.317) (0.051) (0.104) 0.03 0.18 0.64 0.50 (0.920) (0.512) (0.010) (0.059)
0.19 0.37 (0.506) (0.198) 0.39 0.50 (0.165) (0.071)

220 H. Hokama et al. /Psychiatry Research: Neuroimaging 61 (1995) 209-229
magnitude of the differences between correlation coefficients for the same structures in the two groups).
Basal ganglia volume correlations with prefrontal and temporal lobe volume measures. Because of their neuroanatomical interconnectivity, we fur- ther examined the correlations of basal ganglia ROIs with the volumes of left and right prefrontal gray and white matter and of amygdala/anterior hippocampus (ROIs that had been previously measured for these subjects [Shenton et al., 1992; Wible et al., 1994]). As just discussed, we reasoned that a common process acting in the same direc- tion would increase the magnitude of positive cor- relation coefficients, whereas a common process acting to increase basal ganglia volume and to decrease prefrontal and amygdala volume would increase the magnitude of negative correlation coefficients. Separate processes acting on prefron- tal/amygdalar and basal ganglia structures would likely decrease the absolute magnitude of the cor- relations. For the prefrontal-basal ganglia volume correlations in normal subjects, the largest values were between left prefrontal gray and right putamen (0.51, P = 0.052) and right caudate (0.41, P = 0.13); the magnitude of these and other cor- relations was generally slightly reduced in the schizophrenic group, but not to a statistically sig- nificant degree (P > 0.2, Wilcoxon matched-pairs signed rank test). Neither normal nor schizo- phrenic subjects showed large-magnitude correla- tions between amygdala/anterior hippocampus ROIs (boundaries described in Shenton et al., 1992) and any basal ganglion structure (maximal r = 0.35, Ps > 0.2).
Basal ganglia volume correlations with demo- graphic and clinical data. We next analyzed the re- lationship between relative basal ganglia volumes and age of subjects in the two groups. As expected, age and relative volumes showed an inverse rela- tionship in the normal group. Spearman correla- tion coefficients were -0.722 for caudate (P < 0.01) and -0.698 (P < 0.01) for putamen, with GP showing a lesser correlation (r =-0.335, P < 0.30). In marked contrast, there were no strong correlations with age in the schizophrenic group, with r values being -0.115, -0.315, and 0.095 for
caudate, putamen, and GP, respectively (all Ps > 0.20). Neither estimated verbal IQ nor parental SES showed large-magnitude correlations with re- lative ROI volumes in either the schizophrenic group or the normal group (rs < 0.30, Ps > 0.20)
Since results from a first episode study (Chakos et al., 1994) have suggested that volumetric in- creases in schizophrenic patients might be second- ary to neuroleptic medication, we examined the correlation between relative ROI volumes and several measures relevant to this variable, al- though the absence of detailed medication history precluded our using actual dosage, which would have been a more direct and desirable variable. There were no large-magnitude correlations with either current chlorpromazine-equivalent neuro- leptic dosage level or several measures of disease duration and severity: duration of illness, age of onset, or percentage and absolute time hospitaliz- ed since onset. The maximum r value was only -0.279 (with the set of r values having Ps > 0.2).
We next turned to an exploratory analysis of the relationship between relative basal ganglia vol- umes in the schizophrenic group and clinical symptomatology, as measured by the TDI and by the SANS and SAPS scales; these measures were available for correlation in 13 patients. There were no large-magnitude correlations with the TDI (total thought disorder) or with the global and subscale scores of the SANS. For both the TDI and the SANS, the largest correlations were with caudate volume. For the TDI, the correlation was only r = -0.281 (P > 0.2), while the largest SANS correlation (with total score) was only r = -0.206 (P > 0.3). There were larger magnitude correla- tions between the SAPS bizarre behavior subscale score and the relative volumes of the GP (r = -0.633, P < 0.03) and putamen (r = -0.591, P < 0.05). The caudate showed a lesser correla- tion (r = -0.483, P = 0.09). The negative sign of these correlations indicates that increased volume was associated with less bizarre behavior.
Basal ganglia volume correlations with measure- ment of motor function. With respect to motor ab- normalities, there were no large-magnitude cor- relations between the Simpson-Angus scores, ex- pressed either as a sum of items or as individual

H. Hokama et al. / Psychia(ry Research: Neuroimaging 61 (1995) 209-229 221
items, and the basal ganglia ROI relative volumes. The maximal Spearman's rho was 0.358 (P = 0.34). However, there was a large magnitude in- verse correlation between the Simpson-Angus total score and the relative volume of the left amygdala/anterior hippocampus (r = -0.749, P = 0.02). Only two patients, however, had abnor- mal (nonzero) AIMS scores. The patient scoring 5 had the largest putamen volume in the group, and the patient with a score of 2 had a volume in the upper third of the group. (In fact, the Spearman's r for the total [relative] basal ganglia volume-total AIMS score was 0.667 [P = 0.05], although we consider the correlation unreliable because of the presence of abnormal AIMS values in only two subjects.) There were no large-magnitude correla- tions between the akasthisia scale and basal ganglia volumes (e.g., when the correlations for left and right caudate, putamen, GP, and left and right total basal ganglia were examined, the max- imal value was r = -0.35 [all Ps > 0.35]).
3.2. Neuropsychological test results An overview of the neuropsychological results
suggests that the strongest correlations were found between basal ganglia volume ROI and relatively pure tests of motor speed and dexterity. There was also evidence suggesting that basal ganglia pathology influenced attentional processes. By contrast, performance on tests of memory and ab- straction/categorization did not correlate with basal ganglia volumes. Since there was the possibility of lateralized effects, in addition to ex- amining the total relative volumes of basal ganglia ROI, we also examined the left and right ROI volumes of caudate, putamen, and GP; these r values are included in this report.
With respect to motor speed and dexterity, poor right-hand performance on the Finger Tapping Test correlated significantly with increased volume in both left caudate (r = -0.62, n = 14, P = 0.013) and right caudate (r = -0.67, n = 14, P < 0.01) while poor left-hand performance correlated with increased volume in right GP (r = -0.53, n = 14, P = 0.053). Thus, poorer performance was associ- ated with abnormally enlarged basal ganglia ROI volumes. Attention-related processes of temporary
storage, as assessed by Hebb's Recurring Digits, were negatively correlated with right caudate volume (r =-0 .62, n = 13, P = 0.025) and, to a lesser extent, with left caudate volume (r = -0.53, n = 13, P = 0.063). The negative correlation in- dicates that poorer performance on this test was associated with an abnormally enlarged caudate. Other basal ganglia structures did not correlate so highly. Left and right putamen correlations were -0.42 and -0.44, respectively (Ps > 0.15), while left and right GP correlations were -0.27 and -0.28, respectively (Ps > 0.30).
Tests of attention-related processes of rapid switching or shifting showed lesser correlations with basal ganglia structures. Attention switching, as assessed by Trails B, had the largest correlation with right GP (r = -0.42, n = 14, P = 0.135) and left GP (r = 0.38, n = 14, P = 0.183); other cor- relations had absolute values < 0.18 (Ps > 0.50). Attention switching, as assessed by Alternating Semantic Categories, had low magnitude r values, with the largest being r = 0.19 (Ps > 0.50).
Performance on tests of memory and abstrac- tion/categorical thinking, which had correlated significantly with volumetric reductions in bi- lateral temporal lobe structures, did not strongly correlate with volumes of basal ganglia ROIs. Specifically, performance on the Verbal Paired Associates subtest from the WMS-R had negative r values whose absolute magnitude was small (<0.30, Ps > 0.276, n = 15). Abstraction/ categorization, as assessed by the number of categories achieved on the WCST, had small magnitude r values, both positive and negative, with the absolute magnitude of the r values being < 0.25 (Ps > 0.40). Abstraction/categorization, as assessed by the Similarities subtest of the WAIS-R, had the largest correlation with left GP volume (r =-0 .42, n = 15, P = 0.125); however, other r values were all of small magnitude, with absolute values <0.28 (Ps > 0.30).
4. Discussion
This study is, to our knowledge, the first to use small voxel (1.5 mm 3) SPGR acquisitions and ad- vanced image-processing techniques to define the

222 H. Hokama et al . / Psychiatry Research: Neuroimaging 61 (1995) 209-229
volume of each major component of the basal ganglia in schizophrenic patients and matched normal volunteers. The small voxels minimized PV errors, and the image-processing techniques in- cluded a slice editor that enabled the simultaneous use of multiple planes of section to assist in the precise bounding of ROIs. These features likely were key in our obtaining a high reliability of ROI definition and, by reducing variability due to mea- surement error, in obtaining statistically signifi- cant schizophrenic-normal differences. The pres- ent study confirms previous reports of basal ganglia enlargement in schizophrenic patients, as cited in the Introduction.
The magnitude of the schizophrenic group's mean volume increases was 9.5% in the caudate, 15.9% in the putamen, 27.4% in the GP, and 14.2% overall. All volume increases were statistically sig- nificant when relative volumes were used for tests, save for a trend level in caudate, where the increase was statistically significant when absolute volumes were used. Our interpretation of the caudate findings is that a volume increase is likely present, but of lesser magnitude than in putamen and GP; thus, statistical significance is less robust in the present group of 15 subjects.
There was considerable group separation on putamen and GP volumes, with the lowest schizo- phrenic volume for the putamen and GP being larger than the mean and medial normal values. The finding of a 27% enlargement in the GP sug- gests that this structure should be of particular in- terest to MRI studies of schizophrenic patients, especially those, such as first episode studies, look- ing for the presence of change in volume over time. We note that the volumes of both normal subjects and schizophrenic patients reported in the present study closely approximate those of post-mortem measurements (Heckers et al., 1991).
There was a trend (P = 0.07) for correlations be- tween volumes of the caudate, putamen, and GP to be higher in the schizophrenic than in the nor- mal group, thus providing some supporting evi- dence for our hypothesis of a similar pathologic process (or processes) acting on each of these three basal ganglia structures. Further neuropathologic studies will be needed to determine which neural
elements (somata, dendrites, and/or neuropil) are primarily involved in this volume increase.
From a functional point of view, the new evi- dence for a very strong change in the output ele- ments of the basal ganglia (GP) indicates that the abnormal process is neither confined to basal ganglia regions innervated by glutamatergic cor- tical and amygdalar input (striatum) nor to regions receiving dopaminergic input and having a high concentration of dopamine receptors (also the striatum).
Neuropsychological evaluation indicated the most prominent clinical associate of enlarged basal ganglia was lessened speed and dexterity of motor performance. Performance inversely correlated with volume, which was abnormally increased. Poor right-hand performance on the Finger Tap- ping Test correlated significantly with increased volume in both left caudate (r = -0.62) and right caudate (r =-0.67) while poor left-hand perfor- mance was associated with increased volume in right GP (r = -0.53, n = 14, P = 0.053).
Consistent with basal ganglia involvement in nonmotor processing, a correlation was also ob- served between attention-related processes of tem- porary memory storage. As assessed by Hebb's Recurring Digits, performance was significantly and inversely correlated with right caudate volume (r = -0.62); and, at a trend level, with left caudate volume (r = -0.53). We note that volumes of pre- frontal lobe structures, assessed in this same sub- ject group, also showed correlations with Hebb's Recurring Digits and with other relatively pure neuropsychologlcal tests of working memory (Trails B and Alternating Semantic Categories). Thus, there was partial overlap of basal ganglia and prefrontal MRI volume correlations with neuropsychologlcal performance. In contrast, per- formance on tests of memory and abstraction/ categorization (including the total score on the TDI), which strongly correlated with temporal lobe volumes (Nestor et al., 1993), did not cor- relate with basal ganglia volumes. The different degree of commonality with prefrontal and tempo- ral lobe neuropsychologlcal correlations appears reasonable in terms of relative density of prefron- tal and temporal lobe neuroanatomical intercon-

H. Hokama et al . / Psychiatry Research: Neuroimaging 61 (1995) 209-229 223
nections with basal ganglia. Our neuropsychol- ogical tests were selected to include measures thought most likely to correlate with frontal and temporal lobe abnormalities. Measures of pro- cedural memory (Schwartz et al., 1992) and of memory related to visuospatial/oculomotor tasks, such as saccades (Park and Holzman, 1992), would appear useful in future studies of basal ganglia- functional correlations, given the evidence for a basal ganglia role in these functions.
With respect to the AIMS scores, our data sug- gest further work may be useful but are not con- clusive in themselves. Only two subjects showed abnormal scores, although the degree of abnor- mality correlated remarkably well with extreme putamen volumes. A possible confounding factor is that involuntary movements may interfere with MRIs and hence subjects with such movement dis- orders may not be selected for study or may not be successful in completing the MRI (as happened with one subject in our pool). Other potential con- founds include possible masking by continued an- tipsychotic administration and fluctuation of abnormal movements over time. Basal ganglia evaluation of more schizophrenic subjects, in- cluding unmedicated patients and perhaps patients selected to have AIMS abnormalities, is needed. There was no evidence for an association between extrapyramidal movement disorder, as assessed by the Simpson-Angus scale, and abnormal basal ganglia volumes. However, the presence of neuroleptic medication may have obscured any correlations that might be observable in a never- medicated population. We note that Elkashef et al. (1994) failed to find any association between tar- dive dyskinesia and basal ganglia volume (in- cluding that of the putamen).
With respect to the overall paucity of correla- tions between basal ganglia volumes and SAPS or SANS measures, it should be kept in mind that most of the correlations in the literature (usually with caudate volume, see Introduction) were with negative (deficit) symptoms and that our subjects had predominantly positive symptoms. The strong inverse correlation between the SAPS bizarre be- havior score and GP volume is, nonetheless, in- teresting, although caution is needed in interpre- tation because of the small number of subjects and
the large number of correlations performed. The inverse correlation indicates that the abnormal increase in volume was associated with a decrease in bizarre behavior. Although needing confirma- tion in a subsequent study, this association may in- dicate a suppressive effect on motor activity by this abnormality of the output part of the circuit of the basal ganglia. This point also underscores the usefulness of determining whether any startle gating abnormalities might be associated with basal ganglia enlargement. Another possible ex- planation is that increased neuroleptic dosage might both decrease bizarre behavior and increase GP volume.
It is important to note that the generalizability of our basal ganglia findings to other groups of schizophrenic patients, such as those with severe deficit and negative symptoms, remains an open question. Also unknown is whether the findings might appear in other psychiatric disorders, such as mood disorders with psychotic features, as sug- gested in a recent study by Aylward et al. (1994). Finally, we emphasize that the relatively small number of subjects limited power to detect true differences and true correlations with smaller effect sizes, and that negative results in this article should be viewed with this point in mind. Also the patient group's restricted range in certain vari- ables, such as in age of onset, may have lessened the ability to detect correlations.
From a neuropathological standpoint, the basal ganglia remain a fascinating enigma, being enlarg- ed in schizophrenic patients while other brain regions are reduced in volume. Neuroleptic dosage studies in animals show that neuroleptics induce plastic changes, including enlargement of neural elements, that may be reversible at the ultrastruc- tural level, but thus far have not examined whole structure volumetric changes (Benes et al., 1983, 1985, Klintzova et al., 1989; Meshul and Casey, 1989). Such animal studies, as well as follow-up studies of first episode patients (e.g., Chakos et al., 1994), may help answer the question of whether the enlargement is neuroleptic-related, partly or completely. Studies at the in vivo MRI level can- not offer insight as to which neuronal or glial structures are altered, but the large-scale involve- ment of the GP, a structure not heavily innervated

224 H. Hokama et al. /Psychiatry Research: Neuroimaging 61 (1995) 209-229
by cortical glutamatergic or brainstem dopamin- ergic projections, suggests to us that these elements are not likely to be directly causative (although their abnormalities may cause a chain of events that eventuates in enlargement) and also em- phasizes the need for study of this structure in first episode test-retest studies (Chakos et al. [1994] examined only caudate). While such mechanisms are speculative, the evidence for control of neuro- peptide gene expression (transcription) by striatal inputs and several neurotransmitters (Graybiel, 1990) suggests that similar control of expression of
other genes, including those possibly related to ab- normal enlargement, is a possibility. A develop- mental origin of basal ganglia volume alteration also remains a possibility; for example, Loopuijt and Villablanca (1993) have recently reported caudate enlargement secondary to lesions of fron- tal or parietal cortex in fetal kittens.
Appendix
Definition of ROls for caudate, putamen, and GP. Although both coronal and axial formats were
Fig. 4. Regions of interest. See text for description.

H. Hokama ei al. /Psychiatry Research! Neu~imaging 61 (1995) 209-229 225
used in the manually guided delineation of gray matter, we here describe the ROIs primarily in terms of the coronal images. This description will facilitate the reader's cross-referencing with stan- dard anatomical texts. To give the reader a sense
of the distance between landmarks, we describe the ROIs as they would be encountered going anterior to posterior on a set of 1.5-mm coronal images that encompass the basal ganglia structures (n = 42 slices) obtained from a typical normal
A
4
8
12
16
20
24
Fig. 5. Basal ganglia area. See text for description.

226
B
14. Hokama et al . / Psychiatry Research: Neuroimaging 61 (1995) 209-229
28
32
36
40
42
brain. Fig. 4 shows the ROIs for this case on a sin- gle complete coronal slice to orient the reader to Fig. 5 (panels A and B), which display only the basal ganglia area. The caudate is outlined in yel- low, the putamen in red, and the GP in green. Fig. 5 (panels A and B) will be referred to extensively as the reference images for the ROIs defined below. All references to slice numbers are to the numbered slices on Fig. 5.
Description of ROI on coronal slices, with ante- rior to posterior progression. As can been seen in
Fig. 5, the coronal slices are examined sequentially until the caudate gray matter (head portion) ap- pears (subsequently referred to as the "first slice"). This is bounded by frontal lobe white matter, with a small portion of the lateral ventricle also appear- ing medial to the caudate (see the first five coronal slices in Fig. 5). For the most anterior segment of caudate, a small portion may appear superior to the lateral ventricle, but it may not be included be- cause of unreliability attributable to PV; the caudate must initially appear with a volume of at

H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229 227
least one voxel and with gray matter intensity com- parable to cortex (to rule out PV effects). The caudate cross-section enlarges during succeeding slices, being bounded medially (and with more posterior slices, superiorly) by the lateral ventricle and elsewhere by frontal white matter. About 7.5 mm posterior to the appearance of the caudate (first slice), the putamen appears, ventrolateral to the caudate and separated from it by the anterior limb of the internal capsule (slice 6 in Fig. 5). The caudate and putamen have small bands of gray matter streaming between and bridging these two structures; because of PV effects, however, these are not included in the ROIs, which are defined by the bounds of the main compact masses of gray in these two structures. The putamen is bounded laterally and ventrally by the external capsule.
Progressing posteriorly, these relationships are maintained until about 12 mm posterior to the first slice, at which point the caudate and putamen gray matter masses appear to become linked by another gray matter mass at their most ventral point: this is the nucleus accumbens (slices 9-10, Fig. 5). It is impossible to differentiate accumbens gray from caudate gray, and thus they are grouped together in our ROI labeled "caudate." Progressing pos- teriorly, the separation ofcaudate/accumbens from the putamen is accomplished by drawing a vertical line from the most ventral extension of the internal capsule, with caudate being lateral to this line (see slices 11-13, Fig. 5). At this point, the body of the caudate has assumed a position directly lateral to the lateral ventricle. Also, the ventromedial por- tion of the accumbens/caudate is bounded by the white matter of the diagonal band of Broca/medial olfactory stria, as well as the ventral portion of the cingulate gyrus, which has assumed a position just ventral to the lateral ventricle at this point.
About 18 mm posterior to the first slice (slice 13), the accumbens becomes separated from the more dorsal caudate, and almost immediately (within 1 slice more posteriorly) ends. This small separated portion of the accumbens is not included in the caudate ROI. About 19.5 mm posterior to the first slice (slice 14), the GP appears, just medial to the ventral portion of putamen, with two struc- tures separated by the lateral medullary lamina. Other bounds for the GP are the internal capsule
(dorsally and medially) and the substantia in- nominata ventrally. For reference, we note that the anterior commissure appears 24 mm posterior to the first slice (see slice 17). By about 31 mm posterior to the first slice (slice 22), the GP has reached its maximal cross-sectional area, while the putamen has reduced its mediolateral extent, and the ventral portion of the putamen has become contiguous with a gray matter extension, called the peduncle of the lentiform nucleus, included with the putamen ROI in our classification. The GP then decreases in volume, ending about 43.5 mm posterior to the first slice (slice 30). In this same slice, the caudate has assumed a nearly circular cross-sectional area and is positioned at the very lateral-most extent of the lateral ventricles. As one proceeds further posteriorly, the putamen shrinks to a slender fusiform structure, ending 48 mm posterior to the first slice (slice 33). It should be noted that the posterior extent of both putamen and GP is best determined from axial slices and three-dimensional reconstructions, as was done for this description. By about 58.5 mm posterior to the first slice (slice 40), the ventricular atrium (nearly vertical connection between lateral and temporal horns) is present without PV effects, and the tail of the caudate has moved ventrally to course along the lateral margin of the atrium, before turning anteriorly. As noted, PV effects meant that this anterior-coursing portion of the tail could not be reliably outlined, and so it is not included in the ROI.
Acknowledgments
This study was supported by the Medical Re- search Service and Brockton Schizophrenia Center of the Department of Veterans Affairs and a Senior Investigator Award from the National Alliance for Research in Schizophrenia and De- pression (Dr. McCarley); by grants R01 40799 (Dr. McCarley), 1K02 MH-01110-01 (Dr. Shen- ton), and 1R29 MH-50747-01 (Dr. Shenton) from the National Institute of Mental Health; by the Commonwealth of Massachusetts Research Center (Dr. McCarley); by the Scottish Rite Foun- dation (Dr. Shenton); by the Theodore and Vada

228 H. Hokama et al. /Psychiatry Research: Neuroimaging 61 (1995) 209-229
Stanley F o u n d a t i o n (Drs. S h e n t o n a n d Kikin is ) ; by the W h i t a k e r F o u n d a t i o n (Dr. Kik in is ) ; a n d by
the N a t i o n a l Ins t i tu tes o f Hea l th (Dr. Jolesz). Th e au thors t h a n k M a r i a K a r a p e l o u , Br ian Ch iango , M a u r e e n Ainsl ie , J o h n M a r t i n , M a r k A n d e r s o n , Susan Law, a n d Mar ie F a i r b a n k s for the i r ex-
cel lent technical a n d admin i s t r a t ive suppor t .
References
Alexander, G.E. and Crntcher, M.D. (1990) Functional ar- chitecture of basal ganglia circuits: neural substrates of parallel processing. Trends Neurosci 13, 266-271.
American Psychiatric Association. (1987) DSM-III-R: Diag- nostic and Statistical Manual of Mental Disorders. 3rd rev. edn. American Psychiatric Press, Washington, DC.
Andreasen, N.C. (1981) The Scale for the Assessment of Nega- tive Symptoms. University of Iowa, Iowa City, IA.
Andrcasen, N.C. (1984) The Scale for the Assessment of Positive Symptoms. University of Iowa, Iowa City, IA.
Aylward, E.H., Roberts-Twillie, J.V., Barta, P.E., Kumar, A.J., Harris, G.J., Geer, M., Peyser, C.E. and Pearlson, G.D. (1994) Basal ganglia volumes and white matter hyperinten- sities in patients with bipolar disorder. Am J Psychiatry 151, 687-693.
Benes F.M., Paskevich P., Davidson, J. and Domesick, V.B. (1983) Haioperidol-induced plasticity of axon terminals in rat substantia nigra. Science 221,969-971.
Benes, F.M., Paskevich, P., Davidson, J. and Domesick, V.B. (1985) The effects of haloperidol on synaptic patterns in rat striatum. Brain Res 329, 265-274.
Brande, W.M., Barnes, T.R.E. and Gore, S.M. (1983) Clinical characteristics of akathisia: a systematic investigation of acute psychiatric inpatient admissions. Br J Psychiatry 143, 139-150.
Breier, A., Buchanan, R.W., Elkashef, A., Munson, R.C., Kirkpatrick, B. and Gellad, F. (1992) Brain morphology and schizophrenia: a magnetic resonance imaging study of limbic, prefrontal cortex, and caudate structures. Arch Gen Psychiatry 49, 921-926.
Buchanan, R.W., Breier, A., Kirkpatrick, B., EIkashef, A., Munson, R.C., Gellad, F. and Carpenter, W.T., Jr. (1993) Structural abnormalities in deficit and nondeficit schizophrenia. Am J Psychiatry 150, 59-65.
Carlsson, M. and Caflsson, A. (1990) Interactions between glutamaterglc and monoaminerglc systems within the basal ganglia - - implications for schizophrenia and Parkinson's disease. Trends Neurosci 13, 272-280.
Carpenter, M.B. (1978) Core Text ofNeuroanatomy. 2nd edn. Williams & Wilkins (~ompany, Baltimore, MD.
Chakos, M.H., Lieberman, J.A., Bilder, R.M., Borenstein, M., Lerner, G., Bogerts, B., Wu, H., Kinon, B. and Ashtari, M. (1994) Increase in caudate nuclei volumes of first-episode schizophrenic patients taking antipsychotic drugs. Am J Psychiatry 151, 1430-1436.
Chevalier, G. and Deniau, J.M. (1990) Disinhibition as a basic
process in the expression ofstriatal function. Trends Neurosci 13, 277-280.
Cline, H.E., Dumoulin, C.L., Hart, H.R., Lorensen, W. and Ludke, S. (I 987) 3D reconstruction of the brain from magne- tic resonance images using a connectivity algorithm. Magn Reson Imaging 5, 345-352.
Cline, H.E., Lorensen, W.E., Kikinis, R. and Jolesz, F. (1990) Three-dimensional segmentation of MR images of the head using probability and connectivity. J Comput Assist Tomogr 14, 1037-1045.
Cline, H.E., Lorensen, W.E., Lodke, S., Crawford, C.R. and Teeter, B.C. (1988) Two algorithms for the three- dimensional reconstruction of tomograms. Med Phys 15, 320-327.
Crnsby, E., Humphrey, T. and Lauer, E.W. (1962) Correlative Anatomy of the Nervous System. The MacMillan Company, New York.
DeLisi, L.E., Hoff, A.L., Schwartz, J.E., Shields, G.W., Halthore, S.N., Gupta, S.M., Henn, F.A. and Anand, A.K. (1991) Brain morphology in first-episode schizophrenic-like psychotic patients: a quantitative magnetic resonance imag- ing study. Biol Psychiatry 29, 159-175.
Duvernoy, H.M. (1991) The Human Brain: Surface, Three- Dimensional Sectional Anatomy and MR1. Springer-Verlag, Vienna/New York.
EIkashef, A.M., Buchanan, R.W., Oellad, F., Munson, R.C. and Breier, A. (1994) Basal ganglia pathology in schizophrenia and tardive dyskinesia: an MRI quantitative study. Am J Psychiatry 151,752-755.
Ooldman-Rakic, P.S. and Selemon, L.D. (1990) New frontiers in basal ganglia research. Introduction [see comments]. Trends Neurosci 13, 241-244.
Graybiel, A.M. (1990) Neurotransmitters and neuromodu- lators in the basal ganglia. Trends Neurosci 13, 244-254.
Guy, W. (Ed.) (1976) Abnormal Involuntary Movement Scale. in: ECDEU Assessment Manual for Psychopharmacology, Revised. (DHEW Publication No. [ADM] 76-338). Superin- tendent of Documents, U.S. Government Printing Office, Washington, DC.
Heaton, R.K. (1981) The Wisconsin Card Sorting Test Manual. Psychological Assessment Resources, Odessa, FL.
Hebb, D.O. (! 96 I) Distinctive features of learning in the higher animal. In: Delafresnaye, J.F. (Ed.), Brain Mechanisms and Learning. Blackwell Scientific Publications, Oxford, UK.
Heckers, S., Heinsen, H., Heinsen, Y. and Beckmann, H. (1991) Cortex, white matter, and basal ganglia in schizophrenia: a volumetric postmortem study. Biol Psychiatry 29, 556-566.
Jernigan, T.L., Zisook, S., Heaton, R.K., Moranville, J.T., Hesselink, J.R. and Braff, D.L. (1991) Magnetic resonance imaging abnormalities in ienticular nuclei and cerebral cor- tex in schizophrenia. Arch Gen Psychiatry 48, 881-890.
Johnston, M.H. and Holzman, P.S. (1979) Assessing Schizo- phrenic Thinking. Jossey-Bass, San Francisco, CA.
Kelsoe, J.R., Jr., Cadet, J.L., Pickar, D. and Weinberger, D.R. (1988) Quantitative neuroanatomy in schizophrenia: a con- trolled magnetic resonance imaging study. Arch Gen Psychiatry 45, 533-541.
Kikinis, R., Shenton, M.E., Gerig, G., Martin, J., Anderson,

H. Hokama et al. / Psychiatry Research: Neuroimaging 61 (1995) 209-229 229
M., Metcalf, D., Guttman, C.R.G., McCarley, R.W., Lorensen, W., Cline, H. and Jolesz, F.A. (1992) Routine quantitative analysis of brain and cerebrospinal fluid spaces with MR imaging. J Magn Reson Imaging 2, 619-629.
Klintzova, A.J., Haselhorst, N.A., Ranova, N.A., Schenk, H. and Istomin, V.V. (1989) The effects of haloperidol on synaptic plasticity in rat's medial prefrontal cortex. J Hirn- forsch I, 51-57.
Kraepelin, E. (1919/1971) Dementia Praecox. Translated by E. Barclay and S. Barclay. Churchill Livingstone, Inc., New York.
Loopuijt, L.D. and Villablanca, J.R. 0993) Increase in size of the caudate nucleus of the cat after a prenatal neocortical le- sion. Dee Brain Res 71, 59-68.
Meshul, C.K. and Casey, D.E. (1989) Regional, reversible ul- trastructural changes in rat brain with chronic neuroleptic treatment. Brain Res 489, 338-346.
Metcalf, D. (1995) The Slice Editor: A Tool of Manual Segmen- tation of Medical Images. Master's Thesis, Department of Biomedical Engineering, Boston University, Boston, MA.
Mion, C.C., Andreasen, N.C., Arndt, S., Swayze, V.W. II and Cohen, G.A. (1991) MRI abnormalities in tardive dyskinesia. Psychiatry Res 40, 157-166.
Nestor, P.G., Shenton, M.E., McCarley, R.W., Haimson, J., Smith, S., O'Donnell, B.F., Kimble, M., Kikinis, R. and Jolesz, F.A. (1993) Neuropsychological correlates of MRI temporal lobe abnormalities in schizophrenia. Am J Psychiatry 150, 1849-1855.
Nestor, P.G., Shenton, M.E., Wible, C.G., Kimble, M., Smith, L., Kikinis, R. and McCarley, R.W. (1994) Neuropsycho- logical correlates of MRI measures of schizophrenia. (Ab- stract 384) Biol Psychiatry 35, 722.
Park, S. and Holzman, P.S. (1992) Schizophrenics show spatial working memory deficits. Arch Gen Psychiatry 49, 975-982.
Potkin, S.G., Jin, Y., Rinaldi, P.C., Buchsbaum, M., Byrd, R., Melander, G., Sandman, C., Hetridge, R. and Young, R.F. (1993) Neuropsychological, EEG, and PET scan effects of thalamic stimulation in humans: a model for schizophrenia. (Abstract) Schizophr Res 9, 108.
Reitan, R.M. and Wolfson, D. (1985) The Halstead-Reitan Neuropsychological Test Battery: Theory and Clinical Inter- pretation. Neuropsychology Press, Tucson, AZ.
Schwartz, B.L., Rosse, R.B. and Deutsch, S.I. (1992) Toward a neuropsychology of memory in schizophrenia. Psychophar- macol Bull 28, 341-351.
Sceman, P., Guan, H.C. and Van Tol, H.H. (1993) Dopamine D 4 receptors elevated in schizophrenia. Nature 365, 441-445.
Sbenton, M.E., Kikinis, R., Jolesz, F.A., Pollak, S.D., Lemay, M., Wible, C.G., Hokama, H.H., Martin, J., Metcalf, D., Coleman, M. and McCarley, R.W. (1992) Abnormalities of the left temporal lobe and thought disorder in schizophrenia: a quantitative magnetic resonance imaging study. N Engl J Med 327, 604-612.
Shrout, P.E. and Fleiss, J.L. (1979) Intraclass correlations: uses in assessing rater reliability. Psychol Bull 86, 420-428.
Simpson, G.M. and Angus, J.W.S. (1970) A rating scale for ex- trapyramidal side effects. Acta Psychiatr Scand Suppl. 212, ll-19.
Spitzer, R.L. and Endicott, J. (1978) Schedule for Affective Dis- orders and Schizophrenia - - Lifetime Version. New York State Psychiatric Institute, New York.
Swayz¢, V.W. II, Andreasen, N.C., Alliger, R.J., Yuh, W.T.C. and Ehrhardt, J.C. (1992) Subcortical and temporal struc- tures in affective disorder and schizophrenia: a magnetic res- onance imaging study. Biol Psychiatry 31,221-240.
Swerdlow, N.R. and Koob, G.F. (1987) Dopamine, schizophrenia, mania, and depression: toward a unified hy- pothesis of cortico-striatal-pallido-thalamic function. Behav Brain Sci 10, 197-245.
Wechsler, D. (1981) WAIS-R Manual: Wechsler Adult Intelli- gence Scale, Revised. Harcourt Brace Jovanovich, New York.
Wechsler, D. (1987) WMS-R Manual: Wechsler Memory Scale, Revised. Psychological Corporation, New York.
Wible, C.G., Sbenton, M.E., Hokama, H., Kikinis, R., Jolesz, F.A. and McCadey, R.W. (1994) Relationships between tem- poral and frontal brain volume in schizophrenics. (Abstract 386) Biol Psychiatry 35, 722.
Young, A.H., Blackwood, D.H.R. and Roxborough, H. (1991) A magnetic resonance imaging study of schizophrenia: brain structure and clinical symptoms. Br J Psychiatry 158, 158-164.
Zipursky, R.B., Kim, K.O., Sullivan, E.V., Brown, B.W. and Pfefferbaum, A. (1992) Widespread cerebral gray matter volume deficits in schizophrenia. Arch Gen Psychiatry 49, 195-205.