Embed Size (px)
Citation preview

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
177 ISSN 2704-3568
Catheter Care among ICU patients: Basis for Implementation of CDC Guidelines on CAUTI Prevention
Marymie T. Calub and Bella P. Magnaye College of Nursing, Lyceum of the Philippines University, Batangas City, Philippines Abstract: This study aimed to determine the catheter care among ICU patients as basis for the implementation of CDC guidelines on CAUTI prevention. Specifically, it determined catheter care rendered by nurses prior to, during and after indwelling urinary catheter insertion including the risk factor associated with the catheter care. Through that, the researcher came up with a guide that will help nurses in improving catheter care which is called Procedure Manual Based on CDC Guidelines on CAUTI Prevention. The study used quantitative descriptive non –experimental design. This study had 21 participants who were from the Intensive Care Unit (ICU) of four (4) hospitals in Batangas Province and ten (10) of the 21 ICU nurses were permitted to undergo interview. Findings say that most of the ICU nurses are fully aware that the indwelling urinary catheterization requires a sterile aseptic technique. Some of the ICU nurses are not aware and not practicing the appropriate catheter care prior to, during, and after indwelling catheter care insertion. Most of the ICU nurses shared ulimited basic practices/approaches to prevent Catheter-associated urinary tract infection. Thus, CAUTI may be preventable in every institution by strictly implementing and doing proper catherer indwelling catheter care based on at CDC Guidelines on CAUTI prevention at all times. Keywords: Catheter Care, CDC Guideline, CAUTI Prevention INTRODUCTION
The uninterruptedly increasing population of the country, demands for uninterrupted health care and with that, all Filipino nurses are expected to render quality care so as to promote, maintain and restore health and well-being of an individual. To deliver the utmost care possible for every patient is part of nurses’ daily responsibility and with the acquired experiences in relation to providing physical care to each patient especially to hospital units like Intensive Care Unit; nurses are developing their skills to be more efficient making them more assertive and proficient in

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
178 ISSN 2704-3568
performing nursing care. One of the skills that nurse must learn and know is about urinary catheter care. Competence at providing urinary catheter care requires the nurses to understand and apply concepts and practices in preventing infection and also proper techniques that are used to manage patients who have an indwelling urinary catheter throughout the duration of their hospital stay.
One of the greatest risks involved with urinary catheters is infection which is called urinary tract infection (UTI). UTI is an infection anywhere in the urinary tract that contains kidney, ureters, the bladder, and the urethra. In the Philippines, urinary tract infection was the top four (4) leading causes of morbidity in 2014 (DOH, 2016.) Pellowe (2009) cited that he indwelling urinary catheters is the frequent cause of healthcare associated infections. Furthermore, as per Center for Diseases and Prevention [CDC],(2015,) UTIs are one of the most common infections that are hospitally acquired, and almost all caused by instrumentation of the urinary tract which accounts for less than half (30%) hospital related infections described by acute care hospitals. Catheter-associated UTIs (CAUTIs) are on ongoing problem for hospitals since they are linked with increased sickness, death, longer hospital stay, and increased hospital costs (Gould et al, 2009). Usages of urinary catheters are related with a series of adverse results, including death (Pellowe, 2009). Every year, greater than 13,000 deaths are associated with urinary tract infections. Among UTIs that are developed in the hospital, approximately 75% are linked with the usage of urinary catheters (Gould et al, 2009). CAUTI rates in limited resources countries are significantly higher than international standards of developed countries (Rosenthal, 2010.) In order to lower the rates of CAUTI, in adherence to the recommended guidelines on the use of urethral catheters, infection control measures or appropriate catheter care or management in any healthcare facilities should be strictly performed by healthcare providers such as nurses whom can have big influence on the said matter. Regardless of collective efforts, guidelines, programs, standards, and improvements in the healthcare scenery, studies from the Philippines regarding catheter ssociated urinary tract infection and its’ prevention is limited and not well known. In fact, according to the record of Batangas City Health office, they do not have record with regards to catheter associated urinary tract

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
179 ISSN 2704-3568
infection, instead; it was the notifiable diseases, like Measles, Dengue and Malaria, that the hospitals are required to weekly monitor and submit report to them which means that the incidence of CAUTI in community hospitals has not been well documented. This prompted the conduct of this study. Theoretical Framework This study is related to Ajzen’s theory of Reasoned Action (TRA) by Icek Ajzen and Martin Fishbein. According to the Theory of Reasoned Action (TRA), behavior can largely be anticipated by the attitudes of an individual towards performing the behavior in question, through the intervening effect of behavioralintention. The important attitudes in this process are those that are specific to the specific behavior being studied, it is not sufficient to consider the individual’s attitudes more generally (Ajzen 1988; Fishbein & Ajzen 1975). The Theory of Reasoned Action (TRA) by Icek Ajzen and Martin Fishbein is an appropriate theory foundation for creation of the study because the continued use of indwelling urinary catheter is most often due to established behaviors and norms on the nursing unit. This theory provides a framework to study attitudes towards behaviors, and is well supported as a theoretical framework for nursing research in the literature (McEwen & Wills, 2002). The TRA assumes that humans are rational beings and make organized use of the data existing to them, and that individuals ponder the consequences of their actions prior to their decision whether they will participate or not participate in certain actions (Azjen, Czasch, & Flood, 2009). OBJECTIVES OF THE STUDY
This study aimed to determine the catheter care among ICU patients as basis for the implementation of CDC guidelines on CAUTI prevention. Specifically, it determined catheter care rendered by nurses prior to, during and after indwelling urinary catheter insertion including the risk factor associated with the catheter care. METHODS Research Design This study used quantitative descriptive research. It is the second broad class of nonexperimental studies and its purpose is

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
180 ISSN 2704-3568
to observe, describe and document aspects of a situation as it naturally occurs. (Polit &Beck, 2012) The researcher used descriptive research to describe the catheter care among ICU patients rendered by ICU nurses specifically piror to, during, and after insertion of indwelling urinary catheter. Participants
This study had 21 participants who were from the Intensive Care Unit (ICU) of four (4) hospitals in Batangas Province since out of 20 hospitals that the researcher tried to request permission to conduct the said study, seven (7) hospitals responded and granted the request. Out of seven (7), only four (4) of them has ICU. The number of the participants was based on the number of ICU nurses permitted by their head nurses. All of the 21 participants were agreed to answer the observation checklist entitled: Indwelling Urinary Catheter Insertion Checklist to Prevent Catheter Associated Urinary Tract Infection (CAUTI) in the Adult Hospitalized Patient. Ten (10) of the 21 ICU nurses were permitted to undergo interview. Moreover, the researcher got the opportunity to become a complete observer to one ICU nurse and one resident on duty who were able to do the actual indwelling urinary catheter insertion to adult patient. Instrument Interview was the main data source of this research. In this study, the researcher used a semi-structured interview for the gathering narrative data for qualitative analysis. This ensured that the specific set was covered in this study (Polit and Beck, 2012). The researcher prepared an interview guide questions as well as observation checklist regarding indwelling urinary catheter insertion that were answered by the key informants and was also used in the actual observation of the insertion of indwelling urinary catheter to adult patient that was executed by the ICU nurse. The said interview guide questions and observation checklist were validated by the expert on that field. The researcher encouraged the key informants to talk and move freely which permitted obtaining of all necessary information. The informants were free to answer in their own words and had the ability to provide as much detail as they wish.

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
181 ISSN 2704-3568
Data Gathering Procedure Semi-structured Interview Preparing for the interview Obtaining pertinent data requires the researcher be well prepared and conversational skills, thus, steps were taken that made the interview more comfortable and more comprehensive for the informants. As part of the preparation for the data gathering, first, letters were made and personally distributed to the hospital directors and chief nurses. These are the letters requesting permission to conduct survey thru their infection control team and to conduct an interview and observation with their ICU nurses who are carrying orders in inserting indwelling urinary catheters to adult patients. Upon presenting the approved request letter to the head nurses of the four (4) Intensive Care Units, informants verbally agreed to participate in this study. The nature and purpose of the study were explained to the informants and the time and place of interview were set with the informants. At the same time, the informants agreed to answer the observation checklists regarding insertion of indwelling urinary catheter and were collected on the day of the scheduled interviews. Prior to the interview, the researcher studied the interview guide, reviewed the interview techniques and communication skills. Materials to be used during interview such as cellphone as audio recorder, pen and papers were also set. Also, the observation checklist for actual insertion of indwelling urinary catheter was always on hand. Conducting the Interview
After establishing positive rapport to the informants, the researcher briefly described the steps of the interview process. The researcher and the informants used a common vocabulary which is, in this case, Filipino and English. Again, all of the informants verbally agreed to audio record and transcribe the whole interview. Each of the face to face interviews lasted for thirty minutes. There was a time that the informant temporarily interrupted the interview to attend to the patient needs and in that case, the researcher stopped the recorder and waited patiently for the informant to return and continue the interview. In all interviews, the researcher tried to get as much information as possible and comprehensive details about the phenomenon under study. Also, the researcher listened carefully and asked follow-up questions in order to prompt informants’ complete knowledge and experience related to the said study.

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
182 ISSN 2704-3568
After the Interview Recorded interviews were checked and listened for clarity
and completeness as soon as the interview was ended. Audio recorded interviews were needed to be transcribed accurately. Participant Observation Here, the researcher had her hospital duties in Intensive Care Unit of the two hospitals in order to witness an actual insertion of indwelling urinary catheter to adult patient. Fortunately, with great patience and prayers, the researcher got the opportunity to observe it- the first one was executed by the ICU nurse and the other one was done by the resident physician as per hospital policy. The study used the complete observer type of participant observation wherein the researcher is a full observer of the informant’s activities so there was no interaction between the researcher and the informant (Streubert and Carpenter, 2011). Data Analysis All the needed data were tallied, encoded and interpreted using statistical tools andt were used based from the objectives of the study. These include frequency and percentage distribution. This was utilized to identify the percentage of participants who agreed or disagree on the statements listed on the prepared checklis The data gathered were presented in tabular form to be able to interpret the results of the survey. Responses from interviews and results from actual observations were considered in the interpretation of the gathered data. Ethical Consideration Every time we conduct study on people, the welfare of research informants must be our top priority. In this study, all of the key informants verbally agreed and audio recorded to participate in this study after reading the approved request letter for conducting of the study. Though, the researcher made it sure to all key informants that their names, their hospital affiliations will not be mentioned in this study and all the collected information were kept with greatest confidentiality; still, they have the right to withdraw theirselves during the interview. Also, the researcher personally transcribed the audio recorded interviews and then deleted afterwards.

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
183 ISSN 2704-3568
RESULTS AND DISCUSSION Table 1. Before Indwelling Urinary Catheter Insertion
Yes No Indicators f % f %
1. Doctor orders for Indwelling Urinary Catheter Insertion
21 100.00
2. Does patient meet CDC, 2009 criteria for Indwelling Urinary Catheter Insertion?
21 100.00
3. Use smallest-gauge catheter possible (Fr. 14, 5ml or 10ml is usually appropriate unless ordered.)
9 42.86 12 57.14
4. Perform hand hygiene and apply nonsterile gloves
14 66.67 7 33.33
5. Wash perineum with wet washcloths (front to back in females), changing to clean area on washcloths each wipe. Wash the penis on males in circular motions.
5 23.81 16 76.19
6. Remove gloves and wash hands
21 100.00
As shown in Table 1, before the indwelling urinary
catheter insertion, all of the participants (100.00%) agreed on the presence of doctor orders prior to the insertion of indwelling urinary catheter and according to the participants, all patients meet Center for Disease Control and Prevention, 2009 criteria for insertion of urinary catheter. Urinary catheterization is an invasive procedure that requires medical order and, institutional settings, aseptic technique with sterile equipment (Gould et.al, 2009; Lo. et. al, 2014). Also, table revealead that it more than half of the particpants (57.14%) were not using the smallest-gauge catheter (French 14) possible to adult patients, instead they use French 16. The size of a urinary catheter is based on the French scale, which mirrors the internal diameter of the catheter. Furthermore, as per

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
184 ISSN 2704-3568
the information disclosed by the informants during interview, based on their experience, they rarely used the smallest-gauge catheter possible like French 14. Based on the American Nurses Association CAUTI prevention tool, nurses should select the smallest appropriate, unless ordered otherwise indwelling urinary catheter which is French 14, 5ml or 10 ml balloon. Potter et. al. (2017) taught that most of the adults with an indwelling catheter should use a size 14 or 16 Fr to minimize trauma and risk of infection. Hence, some of the informants revealed that French 16 is the most commonly preferred by the physician.
This result may be observed to the following statements: “Usually, French 16, adults. Pag maliit minsan 14 pero
mostly 16 kami..” “Kapagka sa adult patients, kalimitan namin ay 16, pag
malaki yung tao,18 “For adult, madalas ginagamit namin is 16. Kasi minsan
pag yung smallest nagle-leak siya. Kaya mas madalas namin 16.” It is stated in 2009 CAUTI guideline and 2014 Infectious
Diseases Society of America (IDSA) guidelines for catheter-associated urinary tract infections that healthcare facilities should use the smallest size of urinary catheter as possible consistent with proper drainage, to minimize urethral trauma. Larger catheter diameter increases the risk of urethral trauma (Cottenden et.al, 2013). Furthermore, only 23.81% agreed that they washed perineum from front to back in females with wet washcloths, changing to clean area on washcloths each wipe and also washed the penis on males in circular motions while 76.19% revealed that instead of using washcloths to clean perineum, they are using sterile cotton balls. Also, it can be seen from table 1 that prior to indwelling urinary catheter insertion, more than half of the participants (66.67% agreed that they performed hand hygiene and applied non sterile gloves prior to cleaning of patient’s perineum and all of them removed gloves and washed hands. Non sterile gloves including wet washcloths are being used in washing the perineal area of patients (White, Duncan, & Baumle, 2011).
During interviews, participants shared their common practices or catheter care before inserting the indwelling urinary catheter to their patients. They said:
“Eh di yun nga, syempre handwashing tapos prepare yung materials, dapat on hand na lahat kasi ang hirap nung ready na yung patient tapos saka ka palang mag-ga-gather

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
185 ISSN 2704-3568
ng equipments. Tapos check mo yung site ng patient, ah tapos, eto naman yung na-oobserve sa ROD. Tapos yun, Edi pag ready na ang patient saka lahat start na ng insertion.”
“Preparation, edi yung equipments needed, yung size ng catheter na applicable sa pasyente, yung ating KY nasa sachet or lubricaring gel, Betadine, sterile gloves, urine bag, tapos kelangan ang patient ay li-linising mo munang maigi ah ang kanyang urethra bago mag insert, para sure na hindi tayo mag-a-add ng additional infection or anumang mga complication.”
“Syempre mag-co-consent kasi muna yun eh. Humihingi kami ng consent dun sa patient or kung hindi kaya ng patient umano, ang magdedecide ay yung relatives kung bakit ah minsan kasi na-explain na ng attending physician na kailangn nating insert-an ng foley cath so kami i-re-reiterate lang namin or kung may questions pa yung mga relatives saka namin sasagutin kung hindi natanong sa doctor. Tapos ah kahit naman ano, kahit coma yung pasyente, syempre nagpapaalam, nag-i-inform kami na si sir lalagyan naming kayo ng sunda para sa pag-ihi para makatulong sa pag-ihi niyo. Ganun.”
”Oo,di icle-clean mo muna yung pagka sa female, yung kanyang vagina. Tapos depende ma-a-assess naman yung kung anong French ang gagamitin na foley catheter. So laging aseptic technique din, sterile gloves.
Based on the above statements, it can be summarized
that they did acceptable techniques prior to insertion. Gathering the equipment prior to executing the insertion promotes efficiency in the procedure. This result is congruent to what the researcher observed during the actual insertion of indwelling urinary catheter to ICU adult patients. Catheter should be inserted following aseptic technique and using sterile equipment (Lo et al, 2014).
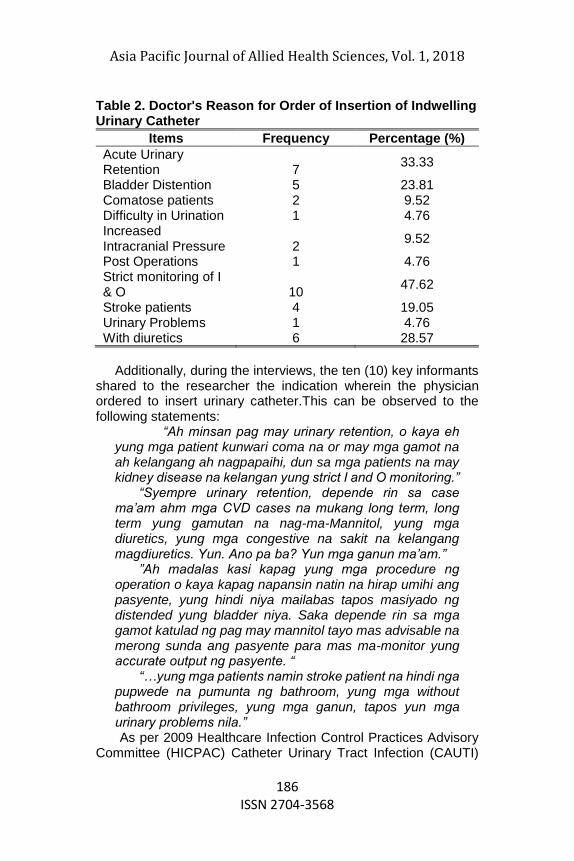
Based on the checklist answered by the ICU nurses, Table 2 shows the doctor's reason in ordering insertion of indwelling urinary catheter. As shown in table 1.1. the most common indication in inserting indwelling urinary catheter was strict monitoring of I & O (47.62%) which is matching to one of the indications stated in 2009 HICPAC CAUTI guidelines.
Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
186 ISSN 2704-3568
Table 2. Doctor's Reason for Order of Insertion of Indwelling Urinary Catheter
Items Frequency Percentage (%)
Acute Urinary Retention 7
33.33
Bladder Distention 5 23.81 Comatose patients 2 9.52 Difficulty in Urination 1 4.76 Increased Intracranial Pressure 2
9.52
Post Operations 1 4.76 Strict monitoring of I & O 10
47.62
Stroke patients 4 19.05 Urinary Problems 1 4.76 With diuretics 6 28.57
Additionally, during the interviews, the ten (10) key informants
shared to the researcher the indication wherein the physician ordered to insert urinary catheter.This can be observed to the following statements:
“Ah minsan pag may urinary retention, o kaya eh yung mga patient kunwari coma na or may mga gamot na ah kelangang ah nagpapaihi, dun sa mga patients na may kidney disease na kelangan yung strict I and O monitoring.”
“Syempre urinary retention, depende rin sa case ma’am ahm mga CVD cases na mukang long term, long term yung gamutan na nag-ma-Mannitol, yung mga diuretics, yung mga congestive na sakit na kelangang magdiuretics. Yun. Ano pa ba? Yun mga ganun ma’am.”
”Ah madalas kasi kapag yung mga procedure ng operation o kaya kapag napansin natin na hirap umihi ang pasyente, yung hindi niya mailabas tapos masiyado ng distended yung bladder niya. Saka depende rin sa mga gamot katulad ng pag may mannitol tayo mas advisable na merong sunda ang pasyente para mas ma-monitor yung accurate output ng pasyente. “
“…yung mga patients namin stroke patient na hindi nga pupwede na pumunta ng bathroom, yung mga without bathroom privileges, yung mga ganun, tapos yun mga urinary problems nila.” As per 2009 Healthcare Infection Control Practices Advisory
Committee (HICPAC) Catheter Urinary Tract Infection (CAUTI)

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
187 ISSN 2704-3568
guideline by Centers for Disease Control and Prevention, in order to minimize the use of indwelling urinary catheter and duration of use in all patients, it is imperative to keep in mind and to put into act that the indwelling urinary catheter should only be inserted to patients with valid indications and leave in place only as long as necessary rather than routinely. Furthermore, here are the examples of recommended indications for indwelling urethral catheter use includes (1) patient has acute urinary retention or bladder outlet obstruction; (2) critically ill patients need accurate measurements of urinary output; (3) to improve comfort for end-of-life care if needed; (4) GU surgery/colorectal surgery; (5) patients need monitoring of urinary output and anticipated to receive large volume of fluids or diuretics during surgery; (6) to assist in healing open sacral or perineal wounds in the incontinent patient; (7) patients require prolonged immobilization (e.g., potentially unstable thoracic or lumbar spine, multiple traumatic injuries such as pelvic fractures.) As shown in Table 3, all of the participants agreed that the indwelling catheter is being placed using aseptic technique and sterile equipment. Also, majority of the participants (90.48%) were using sterile gloves during insertion of indwelling urinary catheter which is a good catheter care while only 9.52% bravely answered that they were not using sterile gloves when inserting a urinary catheter which is not a good example of catheter care.
Meanwhile, during interview, it was sad to know that one of the intervieweeshonestly mentioned “…di ba ano gloves, pero usually ang ginagamit naming dito ay clean lang hindi sterile. Minsan may doctor na gamit ay sterile pero mas marami ang clean lang ang ginagamit, kahit kami clean lang pero dapat sterile.”
In the acute care hospital setting, patients in hospitals should have indwelling urinary catheters inserted using aseptic technique with sterile equipment (Potter et. al, 2017; Lo et.al, 2014, Gould et al, 2009). Moreover, most of the participants (95.24%) agreed that they performed cleansing of urethral meatus of male and female patients in ideal way while 4.76% agreed that they did not do it in an ideal way. During the actual observation, the researcher witnessed the proper way of cleansing of meatus of patient wherein the ICU nurse used sterile gloves. After exposing and identifying the meatus, then she continued holding the labia and meatus then begun cleaning. Each stroke begun at the anterior and moves toward the anus and kept the labia separated with your nondominant hand until the catheter is inserted (Duncan W.L., & Baumle W. 2011).

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
188 ISSN 2704-3568
Table 3. Patient Preparation/Insertion of Indwelling Urinary Catheter
Yes No Indicators f % f %
1. Catheter is placed using aseptic technique and sterile equipment.
21 100.00
2. Use sterile gloves. 19 90.48 2 9.52 3. Cleanse the urethral meatus with an antiseptic solution
20 95.24 1 4.76
4. Use a sterile single-use packet of lubricant jelly for insertion
20 95.24 1 4.76
5. Insert lubricated indwelling urinary catheter to appropriate length smoothly, approximately 2 to 3 inches into the female and 10 to 12 inches into the male and check the urine flow before the balloon inflation to prevent urethral trauma.
21 100.00
6. Inflate indwelling urinary catheter balloon correctly. (Inflate to 10ml of catheters labeled 5ml or 10ml manufacturer’s instructions.)
21 100.00
Whereas during interviews done, interviewees shared
their ideas on how to cleanse the urethral meatus of their adult patients. They said:
“Meatus? Ah eh di sa babae, naka sterile gloves tapos yun nga tatlong swab kami dito, after ng isang swab, discard. Sa lalaki naman, circular motion tapos gamit din swab tapos discard after magamit;” ”Ah yun lang, mahirap kasi eh, from ah upper pababa, upper downward.” and “Ang sa male kasi circle,from inner to outer tapos isang ganun, discard mo yung cotton. Sa female, ah syempre paganun naman yun, pababa so downward ang stroke nun tapos tapon yung cotton balls.”

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
189 ISSN 2704-3568
In terms of lubiricant jelly,it is recommended by 2009 HICPAC CAUTI guideline and 2014 Infectious Diseases Society of America (IDSA) guidelines for catheter-associated urinary tract infections to use a sterile single-use packet of lubricant jelly for urinary catheter insertion. With that, though 4.76% answered no, they were not using a sterile single-use packet of lubricating jelly, it was good to know that 95.24% answered yes, they were using single-use packet of lubricant jelly for insertion. On one of the interviews, an informant mentioned:" yung ating KY jelly or lubricating gel, single pack kami dito." When it comes to actual observations, it was observed the usage of single-use packet and in tube form of lubricant jelly for insertion. Table 4. After Indwelling Urinary Catheter Placement Completion/Urinary Catheter Access & Maintenance
Yes No Indicators f % f %
1. Hand hygiene is performed before and after any manipulation of the catheter site or apparatus
21 100.00
2. Catheter is properly secured after insertion
21 100.00
3. Catheter tubing is unobstructed and free of kinking
21 100.00
4. Urine bag is kept below level of bladder at all times.
21 100.00
5. Urine bag is emptied using a separate, clean collection container for each patient
21 100.00
Table 4 shows statements regarding after indwelling
urinary catheterplacement completion as well as about urinary catheter access and its maintenance. It was good to know that all of the participants agreed that hand hygiene is being performed before and after any manipulation of the catheter. Hand hygiene is a general term that applies either for hand washing which means washing of hands with the use of water and plain or non-antimicrobial soap; antiseptic hand wash that means washing of hands with the use of water and soap containing an antiseptic agent; antiseptic hand rub which means applying an antiseptic hand rub product, like alcohol-based hand sanitizer including foam

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
190 ISSN 2704-3568
and gel, to all surfaces of our hands in order to reduce the number of microbes present; or surgical hand antisepsis (CDC,2017).
With regards to urinary catheter placement, 100% of the participants agreed on the statement that catheter is properly secured after insertion. As per 2009 CDC CAUTI guideline, proper securing of indwelling catheters after insertion is one of the recommended proper techniques for urinary catheter insertion that aid in the prevention of movement, urethral traction as well as inadvertent catheter removal. This was observed by the researcher during actual insertions of urinary catheter to two (2) different adult ICU patients. Catheters were both secured on patients’ thigh.
During interviews, informants mentioned their ways on how to secure indwelling urinary catheter on their patients and it may be observed in these staments:
“Yung tubing ina-attach naming sa may tape naming nasa thigh ng patient then sa right side, depende eh kung saan sa patient mas okay yung placement.” and “Dun sa inner leg, inner thigh pala, dun namin tine-tape. Basta parang yung penis ng pasyente is naka-downward ba. Pagbabae, saan nga ba namin, ah san ti-ne-tape? Parang sa inner leg din.”
Furthermore, the catheter can be secured according to
institutional policy and securing the catheter to the patient’s thigh is usually acceptable and leaving enough slack so that it does not pull on the bladder (White L., Duncan G., Baumle W., 2011). Additionally, when it comes to proper techniques for urinary catheter maintenance, 100% of the participants had good practices in maintaining an unobstructed urine flow for the indwelling urinary catheter. By keeping the catheter and collecting tube free from kinking and keeping the collecting bag below the level of the bladder at all times, unobstructed urine flow for urinary catheter can be maintained. According to CDC (2015), making sure that the the urine bag and its tube free from kinking is the most important and basic technique of maintaining unobstructed urine flow for the indwelling catheter because obstruction increases urinary bladder tension, and bacterial colonization. In addition to that, all have been agreed on keeping the urine bag below level of the bladder at all times. Also the urine bag should not be rested on the floor. That technique was suggested also by CDC 2015 to maintain unobstructed urine flow suggested. These actions were also being observed during the duty hours of the

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
191 ISSN 2704-3568
researcher to two hospitals. Also, these actions may be observed on the statements disclosed by the interviewees during interviews as they asked on how they manage patients with catheter in place and on placement of urine bag after insertion. Some said:
”Ahmn, ay di i-o-observe urine output. Then, every morning care, every diaper change dapat yung site niya thoroughly nalilinis kasi para ma-prevent ang infection. Yun, perineal care, very important kasi dito sa ICU naka-diaper ang patients, every diaper change, we make it sure na nalinis para iwas infection. Kasi nga pwedeng pwede yung maging source ng fever saka infection ng pasyente.”
”Proper observation. Every shift naman ganun. Iwasang magbara ang tubing o kaya ma-kink. Mga ganun.”
“Observe urine output, kung adequate baga. Make it sure na walang obstruction, hindi naka-kink ang tubing. Tapos yung urine bag nga dapat hindi sayad sa sahig. Ganun.”
“Things to consider?Yun the urine output if adequate kung hindi ay di assess natin. Baka nga o kaya naman baka nagkink, minsan kasi pwede yun pag malikot ang patient. O kaya namanyun nga baka may clog or dehydrated. So titingnan natin ang pwedeng bakit walang adequate amount ng output Kailangan ang nurse ay talagang maalam ng proper assessment at independent nursing care.”
All of the participants who answered the checklist, they agreed on the ratio of collecting container used per patient, emptying the collecting bag of the They agreed that they were using a separate, clean collecting container for each of their patients just to empty the collecting or urine bag. While during interviews, the researcher learned that not all are using a separate, clean collecting container for each of their patient to empty the urine bag.
With honesty and sincerity, an ICU nurse mentioned: “Pero pag dito sa ICU na, yung mga indigent na
pasyente, merong naka-prepare na container para ma-drain pero dalawa lang siya for sa limang patient, pag lahat sila ay indigent.”
Another ICU nurse said: “Ah sa amin kasi dito meron na kami nung urinal, dun nalang namin dine-drain” Also, an ICU nurse said: “Hindi, isang urinal sa lahat.” During actual observations, on one institutions, the researcher observed that usage of separate clean container in emptying the urine bag while

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
192 ISSN 2704-3568
on the other hospital, the researcher observed the usage of one urinal for all ICU patients.
Likewise, those participants who answered yes on the checklist that they were using separate container for every patient is may be attributed to the fact that they answered it based on the knowledge they have learned since college days not based on their hospital experience.
Meanwhile one of the ICU nurses mentioned during interview: “pero pag may kaya siya at meron na siyang urinal, eh di dun nalang, yun ang ginagamit. Another ICU nurse said “Yes po. Ay! kapag private ma’am, kung halimbawang, kapag halimbawang may urine bag na sila na nacharged kapag may na-charged na sa kanila yun ginagamit, personal. ” It is attributed to the fact the some of the hospital implemented that all admitted patients should have an admission kit which comprises individual essential items for each patient that also includes a container for draining the catheter. According to CDC (2015), one container for draining the catheter should be used by one and the same patient all throughout the hospital stay so as to prevent infection transmission. Also during interviews, the researcher aired some questions related to urinary catheter access and urinary maintenance or care that may help the researcher to identified risk factors that can contributes to the development of catheter associated urinary tract infection. As said by the 2014 Infectious Diseases Society of America (IDSA) guidelines for catheter-associated urinary tract infections, the most important risk factor for developing infection is the duration of catheterization. Other risk factors include female sex, older age, and not maintaining a closed drainage system. One of the ICU nurses mentioned during interviews that sometimes the urinary catheters were being in placed for almost weeks. Verbally, informant said: “…umaabot ng weeks, months, sa part namin ay di doble alaga nalang sa foley cath.” Additionally, the researcher learned during interviews that some of the ICU nurses were practicing poor techniques in managing indwelling catheters. As per recommendation of 2014 Infectious Diseases Society of America (IDSA) guidelines for catheter-associated urinary tract infections, as part of urinary catheter management, if there is breaks in aseptic technique, disconnection, or leakage, replacement of the catheter and collecting system using aseptic technique and sterile equipment should be done but during the

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
193 ISSN 2704-3568
interviews, informants disclosed the truth that based on their experiences, they do not have standard protocol in managing that cases. One ICU nurse mentioned:
Pag may leakage, ah minsan, pag may leakage, ang ginagawa namin di observe muna namin, kunwari sa shift ko, pag nagpalit kami ng diaper may ihi, eh di i-endorse ko yun, papa- observe ko yun tapos pag may leak pa rin, di dati kasi ni-re-refer naming ay ang minsan naman ang pinapagawa ng ROD ay pina-pa-inflate niya, tawag dito yung deflate - inflate pag hindi pa rin, observe pa rin. Pag ganun eh misan ay ganun nalang tapos dadating na yung times na mawawala na yung leak, parang ganun.”
Likewise, it’s sad to hear that one of the ICU nurses shared that due to financial problem of their patients, even though the need arises, they were not able to change the catheter. Verbally, ICU nurse said:” (Smiled) Dito ma’am, depende po sa case, pag halimbawa ang mga VIP palit agad, walang problema sa kanila basta kumbaga ayaw nilang masira yung aseptic technique pero kapag mga indigent na patients, wala, ano nalang gloves, linis nalang.” Moreover with regards to collecting fresh specimen for examination, it is recommended by the 2014 Infectious Diseases Society of America (IDSA) guidelines for catheter-associated urinary tract infections, as part of urinary catheter management, is to collect a small sample by aspirating urine from the needleless sampling port with a sterile syringe/cannula adaptor after cleansing the port with disinfectant but in reality and when the informants asked on how they collect urine from indwelling urinary catheter for examination, it was alarming that their answers were different from what is recommended. This is attributed to the fact that the indwelling catheters that they are using are no sample port .This may be observed with the following statements:
”Pag small amount lang, clina-clamp muna namin tapos hindi kami dun sa tubings mismo ng urine bag. Ah dun sa may pinagkabitan, dun kami nag-o-obtain.” “Eh di sa ano, magcla-clamp lang kam tapos ay ang sa akin kasi pag ako’y ang kukuha kunwari pag yung paalis na, para baba na sa lab, pero i-aano ko muna yung first na urine, sa catheter na mismo, hindi sa bag, dun sa pinagco-conect-an” “Nag-cla-clamp kami dun sa yellow rubber ng catheter tapos after siguro mga ilang minutes mga 30 minutes,

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
194 ISSN 2704-3568
tinatanggal namin yung tubing na connected sa urine bag then nilalagay naming yung specimen bottle dun sa outlet nung urinary catheter tapos sumasahod kami dun.”
“Ah, okay, icla-clamp muna yung kanyang catheter. Tapos inatayin natin ang 30 minutes tapos saka idi-disconnect yung sa urine bag saka yung catheter, doon mag-ca-catch doon sa bottle, kunyari for urinalysis.”
“Sa small volume hindi ka dun sa urine bag ka kukuha,kundi dun sa mismong port dun, tatanggalin mo yung urine bag tapos yung sa port ka kukuha aseptically ah nilalagyan ng Betadine.”
It was starling to know that not all of the ICU nurses know how to obtain larger amount of urine when it is going to be used for special analyses. It is recommended to obtain aseptically from the urine bag when large volumes of urine are needed for special analyses. Majority of the participants knew that they can collect small and large volumes of urine in same location. As one ICU nurse mentioned
“Large volume? Kasi kami ang large volume lang pag 24-hour urine collection, so ang ganun may lalagyan din kami. Dapat hindi, ganto kasi, pagka matagal ng existing yung urine bag, hindi ka allowed na dun ka kukuha kasi hindi magiging accurate ang result ng like 24-hour urine collection or urinalysis kasi syempre matagal na yung naka-hang up doon. Dapat sterile ka pa rin. “
and another statement:
”Pag large amount, actually dun din kami kumukuha. Kasi pag sa urine bag eh contaminated na yung dulo so hindi na rin sterile.”
Besides, the insufficient knowledge of some of the ICU nurses regarding specimen collection via indwelling urinary catheters may be attributed to the fact that they were not able to attend up to date trainings specifically about urinary catheters. Despite of being registered nurses, all ICU nurses who got interviewed admitted that they never experienced attending seminars or trainings regarding indwelling/Foley catheter insertion. They said:
”Wala naman. Kasi syempre ang catheter insertion naman kumbaga sa school palang talagang tinuturo na sa atin so wala naman talagang trainings for that. By experience, nakikita naming yung mga residents, so aware na kami ng

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
195 ISSN 2704-3568
proper technique doon. Yun, enough na yun, wala ng mga trainings.”
“Ano nalang yung sa school na lang, yung mga pinag-aralan natin?”
”Oo, yun, sa tunay, yung sa school na lang, yung mga pinag-aralan natin. (Smiling.) An ICU head nurse recalled that five (5) years ago, she
attended seminar tackling CAUTI bundle and she said: “Naku wala eh yung mismong regarding urinary
catheter. Ay para palang meron five (5) years ago about CAUTI, yung prevention bundle kaso hindi naman na-i-implement dito sa amin.” It is recommended by the 2014 Infectious Diseases Society of
America (IDSA) guidelines for catheter-associated urinary tract infections that all acute care hospitals should provide education and training to all healthcare personnel who are involved in usage of urinary catheters. According to the said guideline, by means of educating healthcare personnel like nurses involved in the insertion, care, and managing of urinary catheters regarding CAUTI prevention, including alternatives to indwelling catheters, and procedures for catheter insertion, management, and removal and by assessing the healthcare professional competency in catheter use, catheter care, and maintenance, CAUTI can be prevented. In addition to that, during interviews, they also shared their ideas concerning their practice on routine catheter change. They openly shared that:
“Ano, eh di yun nga, yung kung ilang days siya, usually within three (3) day dapat mapaltan na yung catheter, ano dito. Tapos yun nga, proper sterile technique while insertion, ah ano yun talaga ini-imply namin.”
“Ano, eh di yun nga, yung kung ilang days siya, usually within three (3) days dapat mapaltan na yung catheter, ano dito. Tapos yun nga, proper sterile technique while insertion, ah ano yun talaga ini-imply namin.” “…basta yung change of foley catheter every five (5) days. Strict kami dun.
Changing of catheters routinely is one of the approaches that should not be considered as a routine part of CAUTI prevention Rather, it is recommended to change catheters and drainage bags based on clinical indications such as infection, obstruction, or when the closed system is compromised (Lo et al. 2014).

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
196 ISSN 2704-3568
Additionaly, it is suggested that only the properly trained persons insert catheters using sterile technique (Gould et.al 2009; Lo et.al, 2014; Hooton et.al 2010). However, it can be learned from the interviews that majority of them only assist resident duty or main attending physician in the insertion of urinary catheter. As per their policy, when each of the informants are being asked if they are allowed to insert indwelling urinary catheter to ICU patients, only two (2) out of the ten (10) informants revealed that their ICU nurses are allowed and forefront to do indwelling urinary catheter insertion.
Verbally, two of the informants said:”Ah dito sa ICU, kami pero aseptic technique naman yung gamit namin.” Furthermore, the rest of the informants revealed same answers that in their respective hospital, it’s the resident doctor on duty or attending physician who can insert indwelling urinary catheter to their patients. Their role is to assist them. They are the one responsible in the preparation of the materials needed for the insertion and prepare the patient before the insertion. This result may be observed in the following statements: “Ah so far ay ano doctor yung kanilang ano yung pinag-iinsert nila,” “Ah, hindi dito allowed ang mga nurses eh. Di ano, assist kami.” However, even though they revealed that it’s in their policy that it’s the physician who will insert urinary catheter, they all admitted that as the need arises, they disobeyed what their policy says. There were times that the ICU nurses do the indwelling urinary catheter insertion to their patients. They said:
“Ah dito sa ICU, doctor yung nag-iinsert pero depende rin naman sa doctor, pwedeng sabihing insertan nalang namin, ayun itatawag sa residente tapos depende sa residente kung kami pag iinsert-in or assist lang kami.” "Ahm oo pero depende rin sa doctor halimbawa eh siya eh magpa-pa-insert, yun lang, sasabihin na insertan niyo nalang, parang ganun, pero madalang naman yun, depende rin sa ROD.” “…pero yun nga ma’am, minsan na-ba-bypass lalo na kapag busy ang resident on duty, pinapayagan na yung mga ICU nurses, mga supervisors para mag-insert. Ayun po.”
Lastly, with regards to CAUTI surveillance, it’s however alarming that all ICU nurses interviewees revealed that there were no programs being implemented regarding CAUTI prevention like CAUTI surveillance. This may be due to the fact that they declared that there were no reported cases of CAUTI in their incidence or

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
197 ISSN 2704-3568
maybe they were not aware and maybe also CAUTI is not seen to be as serious as other infections. Orally, the following statements were mentioned during their interviews: “Walang survey dyan. Oo, parang wala talaga kaming reported cases ng CAUTI. Kalimitan kasi mga needle prick ung ni-rereport naming o di kaya pag na-splash-an ng infected fluid..Actually ako yung head dati ng infection control kaso pinasa ko na.”
“Walang nagsu-survery saka wala pa akong narinig na ni-report na catheter related urinary tract infection.
According to the 2014 Infectious Diseases Society of America (IDSA) guidelines for catheter-associated urinary tract infections, accomplishment of surveillance for CAUTI if indicated on the basis of facility risk assessment is one of the basic practices for preventing CAUTI that should be implemented. CONCLUSION
Most of the ICU nurses are fully aware that the indwelling urinary catheterization requires a sterile aseptic technique. Some of the ICU nurses are not aware and not practicing the appropriate catheter care prior to, during, and after indwelling catheter care insertion. Most of the ICU nurses shared ulimited basic practices/approaches to prevent Catheter-associated urinary tract infection Thus, CAUTI may be preventable in every institution by strictly implementing and doing proper catherer indwelling catheter care based on at CDC Guidelines on CAUTI prevention at all times.
RECOMMENDATIONS
Hospital Administrators and nursing service department may approve and utilize the Procedure Manual Based on CDC Guidelines on CAUTI Prevention made by the researcher as guide in proper indwelling catheter insertion and its proper maintenance. All nursing procedure manuals must be readily available in every Intensive Care Unit of each hospital to direct the practice like in terms of insertion of indwelling catheter.
Ensure that all nurses who are involve in the insertion, care, maintenance of urinary catheters about CAUTI prevention and removal must be given periodic in-service training regarding techniques and procedures for urinary catheter insertion, maintenance, and removal then their competency in catheter use, catheter care and management should be evaluated.
To nurses and future nurses, though the hospital was not able to provide education and training regarding techniques and

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
198 ISSN 2704-3568
procedures for urinary catheter insertion, may you still possess initiative and have positive will to up to date and share your learnings. Learnings that may help in providing quality safety nursing care to patients. Rather than attending sessions of seminars and trainings, continuous learning can be acquired through reading current issues of reputable nursing journals, pamphlets, and online references.
Future researchers may conduct follow-up study on a larger population in order to verify the result of the present findings. REFERENCES American Nurses Association. (2017). Catheter Associated
Urinary Tract Infection (CAUTI). Data Retrieved April 18, 2017, from http://nursingworld.org/MainMenuCategories/WorkplaceSafety/Healthy-Work-Environment/ANA-APIC/Healthcare-Associated-Infections/Catheter-Urinary-Tract-Infection.html
American Nurses Association. (2017. ANA CAUTI Prevention Tool. Data Retrieved April 15, 2016 from http://www.nursingworld.org/MainMenuCategories/ThePracticeofProfessionalNursing/Improving-Your-Practice/ANA-CAUTI-Prevention-Tool
Association for Professionals in Infection Control and Epidemiology (APIC). (2014). APIC Implementation Guide: Guide to Preventing Cather-Associated Urinary Tract Infections. Data Retrieved April 12, 2017 from http://apic.org/Resource_/EliminationGuideForm/0ff6ae59-0a3a-4640-97b5-eee38b8bed5b/File/CAUTI_06.pdf
Azjen, I., Czasch, C., & Flood, M. (2009). From intentions to behavior: Implementation intention, commitment, and conscientiousness. Data Retrieved: March 20, 2017, from https://www.researchgate.net/profile/Icek_Ajzen/publication/229558752_From_Intentions_to_Behavior_Implementation_Intention_Commitment_and_Conscientiousness1/links/0a85e539f12a0a0b3d000000.pdf
Center for Disease Control and Prevention. (2015). Catheter-associated Urinary Tract Infections (CAUTI). Data Retrieved: April 19, 2016, from http://www.cdc.gov/HAI/ca_uti/uti.html
Centers for Disease Control and Prevention. (2010). CAUTI Guideline Fast Facts. Data Retrieved: April 19, 2016 from http://www.cdc.gov/hicpac/CAUTI_fastFacts.html

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
199 ISSN 2704-3568
Center for Disease Control and Prevention. (2015). FAQs about Catheter-associated Urinary Tract Infection. Data Retrieved: April 19, 2016 from http://www.cdc.gov/hai/pdfs/uti/CA-UTI_tagged.pdf
Centers for Disease Control and Prevention. (2017). Hand Hygiene in Healthcare Settings. Data Retrieved: April 17, 2017 from https://www.cdc.gov/handhygiene/providers/index.html
Department of Health. (2016). Morbidity: Ten (10) Leading Causes. Data Retrieved: April 17, 2017 from http://www.doh.gov.ph/morbidity
Fortu, T (2017). Administrative Assistant V. Batangas City Health Gould, C.V., Umsched, C.A., Agarwal, R.K., Kuntz, G., Pegues,
D.A., & HIPACPAC. (2009). GUIDELINE FOR PREVENTION OF CATHETERASSOCIATED URINARY TRACT INFECTIONS 2009. Data Retrieved: April 20, 2016, from http://www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf
Hooton, T.E., Bradley, S.F., Cardenas, D.D., Colgan, R., Geerlings, S.E. & et al. (2010). Diagnosis, Prevention, and Treatment of CatheterAssociated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Data Retreived: April 30, 2017 from http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/Comp%20UTI.pdf
Infection Control. Data Retrieved: April 16, 2016, from http://www.wpro.who.int/vietnam/topics/infection_control/factsheet/en/
Lee, N. G., Marchalik, D., Lipsky, A., Rushton, H. G., Pohl, H. G., & Song, X. (2016). Risk factors for catheter associated urinary tract infections in a pediatric institution. The Journal of urology, 195(4 Part 2), 1306-1311.
Lo, E., Nicole, L.E., Coffin, S.E., Gould, C.V.,Maragakis, L.L.,Meddings, J., & et al. (2014). Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Data Retrieved: April 15, 2016, from http://www.jstor.org/stable/pdf/10.1086/675718.pdf
McEwen, M., & Wills, E. (2002). Theoretical basis for nursing (3rd ed.). Philadelphia: Wolters Kluwer.
Pellowe, C. (September 17, 2009). Reducing the risk of infection with indwelling urethral catheters. Date Retrieved: March 1, 2017, from https://www.nursingtimes.net/nursing-practice-clinical research/specialists/infection- control/reducing-the-

Asia Pacific Journal of Allied Health Sciences, Vol. 1, 2018
200 ISSN 2704-3568
risk-of-infection-with-indwelling-urethral-catheters/5005830.article
Polit, D. F., & Beck, C. T. (2012). Nursing Research: Generating and Assessing Evidence for Nursing Practice. Ninth Edition. Lipincott Williams & Wilkins. Philadelphia, Pa.
Potter, P.A., Stockert, P.A., Perry, A.G. & Hall, A.M. (2017). Fundamentals of Nursing. Ninth Edition. Elsevier (Singapore) Pte.Ltd.
Rosenthal et al. (2010). Impact of Outcome and Process Surveillance on Catheter-Associated Urinary Tract Infection Rates in 6 ICUs of 2 Cities of Philippines: Findings of the International Nosocomial Infection Control Consortium (INICC). Data Retrieved: April 24, 2016 from https://shea.confex.com/shea/2010/webprogram/Paper2214.html.
White L., Duncan G., & Baumle W. (2011). Foundations of Basic Nursing. Third Edition. Clifton Park, N.Y.: Delmar Cengage Learning





























