Embed Size (px)
Citation preview

Promoter: Prof. dr. Katleen Hermans
Co-Promoter: Ilse Moeremans, DVM
Case Report as part of the
Master`s Dissertation
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
Academic year 2015-2016
Casereport: E. cuniculi and other diseases in a geriatric rabbit
By
Marleen PETERMANN
© 2016 Marleen Petermann


Disclaimer
Universiteit Gent, its employees and/or students, give no warranty that the information provided in this
thesis is accurate or exhaustive, nor that the content of this thesis will not constitute or result in any
infringement of third-party rights.
Universiteit Gent, its employees and/or students do not accept any liability or responsibility for any use
which may be made of the content or information given in the thesis, nor for any reliance which may
be placed on any advice or information provided in this thesis.

Promoter: Prof. dr. Katleen Hermans
Co-Promoter: Ilse Moeremans, DVM
Case Report as part of the
Master`s Dissertation
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
Academic year 2015-2016
Casereport: E. cuniculi and other diseases in a geriatric rabbit
By
Marleen PETERMANN
© 2016 Marleen Petermann

Preface
This case report is the second part of my master thesis. I chose to conduct this report about a
frequently seen infectious disease in rabbits, more specifically about Encephalitozoon cuniculi. E.
cuniculi is a common infection that is unfortunately only to a limited extent covered in our veterinarian
education. So I was very pleased that I got the chance to deepen my knowledge about this important
disease. In memory of my pet rabbit that died last year because of E. cuniculi I called the rabbit in this
case report “Mimi”.
The realization of my literature study was enabled by professional assistance and familial support.
In the first place I wish to thank my promoter professor dr. Katleen Hermans and I also want to thank
my parents for their advice, support and for making my dream, becoming a veterinarian, possible.

Table of contents:
Abstract.....................................................................................................................................................1
Samenvatting ............................................................................................................................................2
1. Introduction ...........................................................................................................................................3
2. Case report ...........................................................................................................................................3
2.1.Patient details ........................................................................................................................3
2.2. Anamnesis ............................................................................................................................3
2.3. Physical examination ............................................................................................................4
2.4. Problemlist ...........................................................................................................................4
2.5. Differential diagnoses ...........................................................................................................4
2.6. Additional diagnostics ..........................................................................................................5
2.7. Diagnosis ..............................................................................................................................7
2.8. Therapy ................................................................................................................................7
2.9. Follow up .............................................................................................................................7
2.10. Prognosis ...........................................................................................................................7
3. Literature review ...................................................................................................................................8
3.1. Etiology .................................................................................................................................8
3.2. Epidemiology ........................................................................................................................8
3.3. Pathogenesis ........................................................................................................................9
3.4. Clinical signs ...................................................................................................................... 11
3.4.1. Introduction ....................................................................................................... 11
3.4.2. Neurological variant and differential diagnoses ................................................. 11
3.4.3. Renal form and differential diagnosis ................................................................ 11
3.4.4. Ocular variant and differential diagnosis ........................................................... 11
3.5. Diagnostics and diagnosis ................................................................................................. 13
3.5.1. Introduction ........................................................................................................ 13
3.5.2. Serology ............................................................................................................. 13
3.5.3. PCR .................................................................................................................. 15
3.5.4. Other in vivo tests .............................................................................................. 15
3.5.5. Post mortem diagnostics .................................................................................. 15
3.5.5.1. Histological lesions ............................................................................ 16
3.5.5.2. Special staining .................................................................................. 16
3.6. Therapies .......................................................................................................................... 17
3.7 Eradication ......................................................................................................................... 18
3.8 Prognosis ........................................................................................................................... 19
4. Discussion ......................................................................................................................................... 20
5. References ........................................................................................................................................ 23

1
Abstract
This case study describes the presentation of a female pet rabbit of seven and a half years of age with
classical signs associated with Encephalitozoon cuniculi (E. cuniculi). The rabbit, here called “Mimi”,
was referred to the animal clinic because of a mild head tilt and bilateral eye abnormalities. On clinical
examination the specialists found bilateral opacities of the cornea, an intraocular opacity of the right
lens, serous ocular discharge of the left eye and palpated a mass in the caudal abdomen. Medical
imaging of thorax and abdomen suggested the mass to be most likely a uterine adenocarcinoma.
Serological tests were found to be positive for IgG and IgM for E. cuniculi. The rabbit was
consequently treated with fenbendazole at 20mg/kg PO q24h for 28 days and the owner decided
against surgery to remove the abdominal mass. According to the owner, around eight months later,
Mimi is alive, still with a mild head tilt and eye problems, but apart from that doing fine.
Key words: rabbit –Encephalitozoon cuniculi – neurological – ocular- adenocarcinoma

2
Samenvatting
In deze casus bespreking gaat het om het vrouwelijk intact konijn Mimi, van zeven en een half jaar
oud. Mimi werd aangeboden in de universitaire dierenkliniek met bilaterale oogproblemen en een
scheve kop. Op klinisch onderzoek stelde de behandelende dierenarts bilaterale littekenvorming ter
hoogte van de cornea vast, rechts een intra-oculaire lenstroebeling, sereuze ooguitvloei links en een
massa in het caudale abdomen. Voor verdere differentiatie werd een bloedstaal genomen voor
serologisch onderzoek voor IgG en IgM antistoffen voor E.cuniculi. Bovendien werden röntgenfoto’s
van thorax en abdomen genomen en echografie van het abdomen uitgevoerd. Radiografisch alsook
echografisch was de massa sterk verdacht voor een uterus pathologie. Nog voordat de uitslagen van
de serologie bekend waren, werd een behandeling opgestart met fenbendazole 20mg/kg PO q24h
voor 28 dagen. De serologie was positief voor E. cuniculi. De eigenares koos tegen verder
behandeling en chirurgische verwijdering van de uteriene massa. Acht maanden later leeft Mimi nog.
Volgens de eigenares vertoont zij nog steeds een milde scheve houding van de kop en
oogproblemen, maar doet het verder goed.
Sleutelwoorden: konijn - Encephalitozoon cuniculi – neurologisch – oculair - adenocarcinoma

3
Casereport: E. cuniculi and other diseases in a geriatric rabbit
1. INTRODUCTION
In the past rabbits were mainly kept for their meat and fur. Nowadays they are popular pets, coming
third after cats and dogs, and also still play an important role in the industrial sector and as laboratory
animals (PDSA 2015). Consequent to their popularity pet owners become increasingly knowledgeable
and are willing to pay for advanced treatment and diagnostics (Varga 2014). Together with the
increasing concern in the private, scientific and industrial sector to keep the animals healthy also the
need regarding veterinarian expertise increased. Continuous investigative research provides new
insights in clinical patterns, symptoms, etiologies and pathogenesis of different rabbit diseases to
improve our understanding. An important disease in pet rabbits that clinicians come across regularly
is encephalitozoonosis. Encephalitozoonosis is an infection caused by the parasite Encephalitozoon
cuniculi. It is no newly emerging disease and was actually first described in 1922 in laboratory rabbits
by Wright and Craighead. Later it was discovered that it has a zoonotic potential for transmission to
immunosuppressed humans (Deplazes et al. 1996) as well as to other animals. A study conducted in
2006 revealed a seroprevalence in the UK of 52% making it a potential health hazard for
immunosuppressed people as well as other animals (Keeble and Shaw 2006).
It becomes obvious that E. cuniculi is an important disease that deserves further attention.
In the following case study the case of a pet rabbit is described that showed typical signs of
encephalitozoonosis.
2. CASE REPORT
2.1. PATIENT DETAILS
This case study is about Mimi, a female intact pet rabbit of seven years and five months. She weighed
1.88kg at the time of consultation and is of a mixed breed (Oryctolagus cuniculus forma domestica).
2.2. ANAMNESIS
On 6th of May 2015 Mimi was referred to the faculty of veterinary medicine with complains of bilateral
eye problems. On the cornea of her right eye the owner described a haze that was present for already
several years. The same eye also showed severe serous discharge. The owner went to their own vet
beforehand who prescribed an eye ointment that did however not resolve the problems. Name, brand
or active ingredient of the ointment is not known by the owner. Four weeks before the current
consultation the owner also noticed a haze on the left eye. Discharge was not seen. Mimi additionally
shows a very mild head tilt to the left side for already several months.
She eats commercially available pellet mix, dry bread and vegetables. She is drinking well and her
appetite is also good. She is kept outdoors solitarily and can run around freely on grass and sandy

4
ground, where she likes to dig a lot. Mimi has always been kept solitarily. Two years ago Mimi was
diagnosed with a mammary tumor that was removed surgically (mammectomy). Afterwards there were
no further problems. Her weight stayed stable in this period. Mimi is not vaccinated.
2.3. PHYSICAL EXAMINATION
During inspection a mild head tilt to the left side could be seen.
On abdominal palpation the veterinarian palpated a mass in the caudal abdomen.
During ophthalmological examination a bilateral scar formation on the cornea and neovascularization
could be seen as well as an intra-ocular opacity of the right lens. A fluorescein-test was conducted
bilaterally, which was negative in the right eye and mildly positive in the left eye. The veterinarian also
tried to catheterize the lacrimal duct of the right eye which was however not permeable.
The ophthalmologist of the faculty was consulted as well based on photographs of the eye.
A specific neurological examination was not conducted
2. 4. PROBLEMLIST
Mild head tilt to the left side
Bilateral opacity of the cornea and serous ocular discharge of the left eye
Intraocular opacity of the right lens
Obstructed ductus lacrimalis
Mass in the caudal abdomen
2. 5. DIFFERENTIAL DIAGNOSES
It is clear that this rabbit suffers from a combined problem.
Based on the anamnesis, the head tilt and cataract, an infestation with Encephalitozoon cuniculi is on
top of the list of the differential diagnoses.
Fig. 1: Left eye with scar formation on the
cornea, after fluorescein-staining.
Fig. 2: Right eye with cataract of the lens.

5
Other differentials for a head tilt include a peripheral or vestibular problem that could be caused by an
otitis interna or media, intoxication, encephalitis, neoplasia or trauma.
Serous discharge from the eye can be caused by a stenotic lacrimal duct, keratoconjunctivitis, a
corpus alienum, conjunctivitis follicularis or an ulcerative keratitis.
An intraocular opacity of the lens can be seen with a cataract. Causes for cataract are among others
age related, hereditary, nutrition, medication, E.cuniculi, diabetes mellitus, chronic uveitis, progressive
retina-atrophy, hypocalcemia, radiation, DMSO or oxidative stress.
Opacity of the cornea can occur by edema (mechanical irritation, glaucoma and medication), keratitis,
cellular infiltrates, pigmentation or fibroplasia.
The left eye showed a mildly positive fluorescein test, indicating damage of the cornea, in this case
most likely a superficial ulceration. Possible causes include trauma, viral infections (Myxoma virus),
secondary to bacterial infections (e.g. blepharoconjunctivitis or dacrocystitis), dry eyes (primary or
secondary) or a vitamin A deficiency.
The mass in the caudal abdomen can be caused by neoplasia (uterine adenocarcinoma, lymfoma),
endometrial hyperplasia, pyometra, inflammation of the uterus or an impacted gut.
2.6. ADDITIONAL DIAGNOSTICS
It was decided to conduct further tests to differentiate the abdominal mass and the cause for the head
tilt. Also an ophthalmologist was consulted based on photos of the eyes.
2.6.1 Medical imaging: x-ray and ultrasound
Considering the abdominal mass an ultrasound and radiographic examination was advised.
The specialists took ventro-dorsal as well as left-right lateral x-rays of thorax and abdomen.
In the caudal abdomen a well-defined soft tissue structure could be seen with a possible discrete
mineralization. There were also indications for uterus pathology, most likely an inflammation or
neoplasia. At the level of the right kidney there was a small mineralization. The gastro-intestinal tract
was filled with content and gas.
On the x-rays of the thorax no significant abnormalities, for instance metastases, were found.
On the abdominal ultrasound examination a mass was detected as well, more precisely in the uterus.
The uterus contained a small amount of anechoic fluid and multiple large echoic masses (min 3.7 x
1.8cm) in the corpus and the uterine horns. Both kidneys were normal in size (L2.9cm, R 3.0cm) and
shape with a normal internal architecture. The only aberrance was a mineralization (2.4mm). The
other organs such as ovaries, adrenal glands, intestines, liver, spleen, lymph nodes, bladder and
gallbladder were without clinical findings.

6
Fig. 3: Lateral radiograph of the abdomen.
The gut is filled with gas and a well-defined
structure is visible in the caudal abdomen.
(Picture: Department of Medical Imaging,
Faculty of Veterinary Medicine, UGent).
Fig. 4: Ventro-dorsal radiographs of thorax
and abdomen. Mild mineralization of the right
kidney can be seen. (Picture: Department of
Medical Imaging, Faculty of Veterinary
Medicine, UGent).
).
Fig. 5: Ventro-dorsal radiographs of the thorax.
No metastases in the lungs can be seen.
(Picture: Department of Medical Imaging,
Faculty of Veterinary Medicine, UGent).

7
2.6.2. Bloodwork:
Blood samples were sent to an external laboratory for serological testing of E. cuniculi antibodies. The
test results were positive. The immunoglobulin M (IgM) titer was 1280 and immunoglobulin G (IgG)
1280. The reference value of the laboratory for IgG had to be below 80.
2.7. DIAGNOSIS
Based on the findings of the medical imaging, anamnesis and the age of the rabbit, a uterine
neoplasia is most likely responsible for the uterine mass. Most frequently an adenocarcinoma is found.
The serological test and the symptoms indicate a manifestation of Encephalitozoon cuniculi.
2.8. THERAPY
Because of the strong suspicion of an E. cuniculi infestation and the planned surgery a therapy with
fenbendazole (Panacur puppy®) was started without waiting for the results of the serological tests.
The administered dose was 20mg/kg PO q24h for 28 days. After the medical treatment an
ovariohysterectomy is advised.
The ophthalmologist of the faculty stated that chronic ulcerations are frequently seen in pet rabbits and
that there is the possibility to debride the ulceration with a swab to stimulate healing.
2.9. FOLLOW UP
After the results of the serological tests were known, the owners decided to not have the surgery
performed, but to euthanize Mimi when the clinical picture would get worse. In May she got treated
with fenbendazole for four weeks, no further treatment was done afterwards. After the treatment the
head tilt as well as the eye problems did not improve. Apart from that Mimi is doing fine and there are
no further complains.
2.10. PROGNOSIS
For the prognosis the different problems have to be considered individually. Literature describes cases
in rabbits with encephalitozoonosis with improvement of vestibular signs after fenbendazole treatment,
the chances are however limited. The ocular lesions have a rather poor prognosis as well. The serous
ocular discharge and obstructed lacrimal duct need further investigation, since there might be a causal
link. The cornea ulcerations can be treated with debridement but even then have a guarded prognosis.
The cataract cannot be resolved with medication and the same applies to the uterus deterioration.
Surgery is a possible solution for both. Ovariohysterectomy has a good prognosis as long as there are
no metastases yet.

8
3. LITERATURE REVIEW
3.1. ETIOLOGY
Encephalitozoon belongs to the phylum Microsporidium, kingdom Fungi. Microsporidia are eukaryotic,
unicellular parasites that form highly resistant spores, making them difficult to eradicate. They are
obligatory intracellular and can only be found in animal hosts and some species, most of which are
opportunistic, also infect humans (Lallo 2005, Didier 2005, Deplazes et al.1996).
Three different E. cuniculi strains were identified genetically. Rabbits are mainly infected by the type I
strain, strain II is predominantly found in rodents and strain III in dogs. Strain I and III have been
isolated respectively from humans in Europe and the United States (Didier et al. 1995, Didier et al.
2000).
3.2 EPIDEMIOLOGY
There are big differences regarding the seroprevalence in different countries. It is estimated that more
than one million pet rabbits are kept in the UK alone (PDSA 2015). A study conducted in the UK in
2006 found a seroprevalence for encephalitozoonosis of 52% among clinically healthy rabbits (Keeble
and Shaw 2006). Another study regarding seroprevalence conducted in Germany reported a
seroprevalence of 45.1%. This study was however not limited to healthy rabbits (Ewringmann and
Göbel 1999). A study carried out in Japan found a seroprevalence of 87% (Furuya 2006).
E. cuniculi primarily infects rabbits, it is however also found in other mammals such as rodents,
guinea pigs, foxes, monkeys, cats, dogs, sheep, goats, horses, pigs and even humans (Harcourt-
Brown 2004, Shadduck et al.1979, Pang and Shadduck 1985). The occurring lesions and tissue
distribution vary yet significantly between the species (Shadduck et al. 1979). The parasite also shows
a zoonotic potential for immunocompromised humans. Those include AIDS patients, patients after a
long immunosuppressive therapy or organ transplant recipients (Keeble 2006, Didier et al. 2000).
Infected rabbits can thus pose a potential health hazard to those individuals (Didier 1995, Didier 2000,
Furuya 2009). It is to mention though that a direct zoonotic connection has not been found yet and that
human infection is mainly due to infection by other humans or contaminated water and not by rabbits
(Keeble 2006, Furuya 2009). In a study from 2008 for example, researchers found E. cuniculi DNA in
a high percentage of urban pigeon-feces (Bart et al. 2008). More research is necessary to define
which animal species plays a major (and minor) role as potential reservoir of infection. In human
patients, interstitial pneumonia, diarrhea and muscle wasting are common clinical signs (Harcourt-
Brown 2002).

9
3.3 PATHOGENESIS
Infection with E. cuniculi occurs by ingestion or inhalation of spores as well as by vertical
transplacental transmission from doe to fetus (Baneux and Pognan 2002). The most common source
of infection is urine-contaminated food and water (Cox et al 1979). The site of infection depends on
the route of transmission and consequently primarily affects the epithelial cells of the gastro-intestinal
or respiratory tract (Didier et al. 2000). After oral intake the spores infect the intestinal epithelium, pass
the gut-associated lymphoid tissue and travel hematogenously to their target organs as free spores or
via monocytes. E. cuniculi replicates in the reticuloendothelial cells and has an effect on cell-mediated
as well as the humoral immunity. An infection suppresses thus both types of immunity, (Valencakova
et al. 2003) making the rabbits more prone to other infections as well. Meyer-Breckwoldt (1996) found
accordingly that seropositive rabbits were more frequently affected by other diseases.
Microsporidia are eukaryotic organisms but nonetheless lack many typical organelles e.g.
mitochondria and a Golgi-apparatus (Didier et al. 2000). In return the spores have a specific
organelle, the polar tube, which enables the transfer of the sporoplasm from the spore into the host
cell (Harcourt-Brown and Holloway 2003). Replication initially takes place in the cells of lung, liver and
kidneys; the brain and gut are at this point mostly unaffected (Cox et al. 1979). Spreading continues in
the kidney as well as in the central nervous system, the heart and other organs (Cox et al. 1979,
Harcourt-Brown 2004). Proliferation (merogony) takes place in the cell cytoplasm of the host cells in
parasitophorous vacuoles by binary division (Didier 2000). After replication of the parasite the host
cells rupture and release the infectious spores that can again infect adjacent cells. This process is
accompanied by an inflammatory response and granula formation, resulting among others in focal
interstitial granulomatous hepatitis and nephritis, phacoclastic uveitis and focal non-suppurative
granulomatous meningo-encephalitis (Percy and Barthold 2008).
In the ocular form the most affected part is the lens. In adult rabbits the ocular lens is an avascular
segregated compartment and the epithelial cells are surrounded by a thick capsule. It is therefore
suggested that E. cuniculi invades the developing lens of rabbits in utero after vertical transmission.
During uterine development the lens capsule is thin and strongly vascularized. Later the parasite may
cause the lens to rupture at its thinnest point releasing lens material into the anterior chamber. Due to
the lens antigen exposure it leads to phacoclastic uveitis (Wolfer et al. 1993, Ashton et al. 1976).
Supporting this theory Ashton and Wirasinha (1973) described that Microsporidia are unable to
penetrate Descemet`s membrane and that also the mature lens capsule forms a barrier for the
pathogen. Typically the lesions are unilateral, sometimes bilateral (Wolfer et al. 1993, Harcourt-Brown
and Holloway 2003, Künzel et al. 2008). In contrast to the renal lesions and matching the previous
hypothesis, eye diseases are more frequent in young rabbits (Giordano et al. 2005).
Seroconversion generally takes place within three weeks after natural infection and excretion of
spores after a minimum of six weeks. Neonates are normally protected by maternal antibodies until
four weeks post-partum (Kunstyr et al. 1986). 95% of the rabbits born to seropositive does had
maternal antibodies against E. cuniculi. When the maternal antibodies decrease, the offspring
becomes susceptible to natural infection. Young infected rabbits are thus seronegative from four to

10
eight weeks of age, until seroconversion takes place. Transplacental transmission is also possible and
results in seroconversion as a response to an active infection at eight to ten weeks of age (Lyngset
1980).
There are big differences in antibody responses between rabbit. The antibody responses detected
were long, short or episodic, although all rabbits in the study were infected with the same inoculum,
via the same route, with the same dose and kept under the same standardized conditions (Kunstyr et
al. 1986). In a study by Waller and colleagues (1978) affected animals that underwent seroconversion
had high antibody titers for longer than a year after exposure. It also showed that IgM seroconversion
occurs faster than IgG seroconversion. Determining IgM and IgG simultaneously enables the
practitioner thus to detect an active infection (Jeklova et al. 2010). In general the IgM response was
also shorter than that of IgG (Kunstyr et al. 1986). The same study mentioned earlier by Waller and
colleagues (1978) also found that out of six orally exposed rabbits only two responded with
seroconversion. That might indicate the necessity of frequent exposure or higher doses of spores, as
is mostly the case in natural conditions.
Interestingly, in a study that investigated predisposing factors, no correlation between seroprevalence
and age, breed, diet, husbandry (indoors vs outdoors), sex, neuter status, bodyweight, litter training,
access to grass, contact with wild rabbits, contact with other pets (dog, cat, guinea pig etc.),
vaccination or insurance status could be found. Also there was no relation between being seropositive
and being housed together or having contact with other rabbits. Even being in contact with
seropositive rabbits did not increase or decrease the probability of being seropositive (Keeble and
Shaw 2006). This is quite contrary to Meyer-Breckwoldt (1996) who found that rabbits that are in
contact with other animals or outdoor access were more frequently seropositive.
Studies in the past showed zero seroprevalence of E. cuniculi in wild rabbits in England and Scotland
(Cox and Ross 1980). A similar study carried out in 1997 showed however that wild rabbits in Australia
were exposed to E. cuniculi (Thomas et al. 1997). Regarding the high seroprevalence in pet rabbits
there is the possibility of pet rabbits acting as reservoirs for wild rabbits. As mentioned before also
other mammal species can host E. cuniculi and might act as a wildlife reservoir for infection as well
(Keeble and Shaw 2006).
There are still some unanswered questions regarding the pathogenesis. For example what happens
after the acute infection, since many rabbits stay asymptomatic. It is generally assumed that these
asymptomatically infected rabbits remain continuously infected but that the parasite is present in very
low numbers. It is also not known what triggers the disease to develop later in life and what leads the
further evolution of the antibodies (Harcourt-Brown 2004). Probably different factors are involved in a
clinical outbreak such as the immune status of the rabbit, route of infection, the involved strain and/or
stress. So if a rabbit becomes immunosuppressed for example by an immunosuppressive drug, stress
or changes in husbandry the immunological balance between parasite and host shifts in favor of the
pathogen and clinical symptoms are more likely to appear and can even result in death (Keeble 2006,
Horvath 1999). Accordingly, Meyer-Breckwoldt (1996) described that in 61.1% of rabbits with head tilt
changes in animal husbandry were noted.

11
3.4. CLINICAL SIGNS
3.4.1. Introduction
The clinical picture of encephalitozoonosis can vary a lot between individuals. Encephalitis, hepatitis,
cholecystitis, enteritis, nephritis, rhinitis, sinusitis, keratoconjunctivitis and disseminated infection are
described among others (Lallo 2005). The three most common forms are however the neurological
form, the ocular form and the renal form. They can occur individually or in combination. The severity
also knows a broad variety ranging from very mild and vague signs up to sudden death caused by
seizures or myocardial lesions. The seizures can be the result of advanced brain damage or
mineralization of the aorta. Mineralization is due to renal failure and causes hemodynamic problems
(Harcourt-Brown 2004). Besides the three main forms also nonspecific clinical presentations can be
seen marked by diarrhea, weight loss, malaise or sore hocks (Rich 2010).
A study carried out by Harcourt-Brown (2004) investigated the prevalence of the different forms. The
study was however statistically not significant due to an insufficient sample size. 66% of the rabbits
were tested seropositive, 56% of those showed neurological signs, 28% renal signs and 10% ocular
signs (Harcourt-Brown 2004). Another study conducted by Ewringmann and Göbel found 45% of the
tested rabbits being seropositive, 45% of those exhibited neurological signs, 31% renal signs and 13%
ocular signs (Ewringmann and Göbel 1999).
3.4.2. Neurological variant and differential diagnoses
The most common form is the neurological variant (Harcourt-Brown 2004, Ewringmann and Göbel
1999). The signs can range from mildly abnormal behavior, such as docile reactions, up to severe
vestibular disease. Vestibular disease can also range from a very mild head tilt to the inability of the
rabbit to right itself. Most frequently described are head tilt, nodding or swaying, seizures, ataxia,
disorientation, deafness, intermittent aggression, nystagmus, ataxia, muscular weakness and wasting,
seizures, hemiparesis and even quadriplegia. The onset of neurological signs is mostly acute
(Harcourt-Brown 2004).
Differentials for head tilt are ascending bacterial infections from the nasal cavity causing an otitis
interna or media. The causing agent is mostly Pasteurella multocida (P. multocida), which can also
cause meningoencephalitis. P. multocida is more frequently seen in rabbits in intensive housing
conditions than in pet rabbits (Harcourt-Brown 2004). Consequently in pet rabbits with vestibular signs
an Encephalitozoon infection is more frequently seen than pasteurellosis (Kunstyr and Naumann
1983). Other differentials of head tilt that are rare but have been reported include a Baylisascaris
infection (in North America), toxoplasmosis, neoplasia, viral infections (Herpes simplex 1), vascular
pathology, degenerative disease, trauma, lead intoxication (Keeble 2006), listeriosis and malignant
cerebral lymphomas (Csokai et al. 2009b). A combined infection with Encephalitozoon and Pasteurella
is possible as well (Harcourt-Brown 2002). A distinct pathological sign at necropsy to differentiate

12
between encephalitozoonosis and pasteurellosis are the cortical depressions that are typical for E.
cuniculi (Flatt and Jackson 1970).
To rule out the other differentials the practitioner can make use of hematology, serological tests,
radiography of the tympanic bullae and an examination of the external ear canal (Harcourt-Brown
2004).
The most important differentials for hemiparesis and hemiplegia include anything that affects the
spinal cord; among others fractures, subluxations, spondylosis and lesions of the intervertebral discs.
Ataxia can be accredited to diseases such as osteoarthritis, sore hocks, and muscular weakness as
well as cardiac, hepatic or renal disease (Harcourt-Brown 2002, 2004, Harcourt-Brown and Holloway
2003).
3.4.3. Renal form and differential diagnoses
The renal form corresponds with symptoms of a chronic progressive renal failure. Those include non-
specific signs such as weight loss, lethargy and anorexia, but also polyuria and polydipsia and urinary
incontinence. The incontinence might also be due to the neurological problems or E. cuniculi unrelated
problems such as urinary tract infection, urolithiasis, or any reasons that disable the rabbit to lift the
hind legs. As a result urine scald in the perineal region and along the medial side of the hind legs can
be observed (Harcourt-Brown 2004).
3.4.4. Ocular variant and differential diagnoses
In the ocular variant common lesions include cataract (Ashton et al. 1976), uveitis, hypopyon and even
blindness (Harcourt-Brown 2004). The uveitis mostly occurs spontaneously after rupture of the lens
capsule. The extruded lens material can be seen as a yellow- whitish mass. Lens proteins are then
released into the anterior chamber causing a granulomatous uveitis, iris color changes as well as a
synechia posterior. Chronic uveitis can result in phtysis bulbi and secondary glaucoma (Sandmeyer et
al. 2011).The posterior chamber normally stays unaffected, as does the eyesight. There is no sex
predilection, but it is mostly seen in younger rabbits (Pilny 2012, Stiles 1997). In a study by Harcourt-
Brown (2004) with 180 rabbits, ten rabbits exhibited intraocular lesions and all of them tested
seropositive for E. cuniculi. Separate studies by Künzel et al. (2008) and Csokai et al. (2009a)
revealed similar results. They did a PCR analysis on lens material in rabbits with phacoclastic uveitis
secondary to lens rupture and most of the rabbits tested positive. Phacoclastic uveitis is thus highly
suspicious of an E. cuniculi infection.
E. cuniculi bears a close resemblance to Toxoplasma gondii. In toxoplasmosis however, the lens is
usually unharmed and the cataract is due to the inflammatory reaction (Ashton et al. 1976). Other
differentials for a mass within the anterior chamber comprise lens material, an inflammatory mass and
neoplasia (Sandmeyer et al. 2011).

13
3.5 DIAGNOSTICS & DIAGNOSIS
3.5.1. Introduction
Making a definitive diagnosis of encephalitozoonosis in vivo as well as post mortem is difficult for
various reasons. First of all, despite the high seroprevalence in pet rabbits many animals are
subclinically infected (Harcourt-Brown and Holloway 2003, Künzel et al. 2008). A seropositive titer is
therefore not necessarily clinically relevant and the titer is also not correlated with clinical signs
(Harcourt-Brown and Holloway 2003, Keeble and Shaw 2006). A study by Cox and colleagues also
found no correlation between antibody titers and spore shedding or histopathological lesions (1978).
Seropositive animals can show severe histopathological lesions without showing any clinical signs.
Accordingly E. cuniculi cannot be diagnosed based on only histological lesions (Csokai et al. 2009b).
Also organisms cannot always be demonstrated within typical histopathological changes (Percy and
Barthold 2008). A seropositive animal that shows clinical signs can thus still have another causing
agent. It is for that reason important to rule out other differentials. An E. cuniculi infection suppresses
the humoral and cell-mediated immunity (Valencakova et al. 2003) and affected animals are therefore
even more susceptible to other infections.
3.5.2. Serology
The diagnostic tools primarily used in veterinary practice for an in vivo diagnosis are serological tests.
As mentioned earlier rabbits develop circulating antibodies three to four weeks post-infection.
Histopathological changes can normally be seen after seroconversion (Cox and Gallichio 1978).
Around four weeks after the antibody titer increased, alterations can be found in the kidney. Changes
in the brain normally occur later and can be detected about eight weeks after increasing antibody titers
(Harcourt-Brown and Holloway 2003). Another study by Cox and Gallichio (1978) detected the
parasite in the kidney already two weeks after seroconversion and histological lesions were detected
after five weeks. In this study the organism was rarely seen in the brain, cerebral lesions were seldom
and, in accordance with Harcourt- Brown, not seen until eight weeks after seroconversion.
The detection of antibodies against E. cuniculi only indicates previous exposure to the parasite but
does not define the status of the disease. When an animal tests positive it is not diagnostic but only
indicates that it was exposed to E. cuniculi at some point. A seropositive result might thus mean an
active infection, a latent infection or an immune-reaction that was built up without being infected
anymore (Harcourt-Brown 2004). In other words a seropositive rabbit can develop clinical signs,
become an asymptomatic carrier or eliminate the parasite.
As outlined above, rabbits can show a considerable individual variation regarding their immune
response. Some exhibit high antibody levels for years and others turn seronegative shortly after
infection (Cox 1977). Harcourt-Brown (2004) describes an antibody increase three to four week’s post-
infection with a peak concentration after nine weeks. In another study by Cox and colleagues the
antibodies peaked after a couple of weeks and stayed high during the entire proof (400days) (Cox
1978, Waller 1978). Seroconversion furthermore does not prevent re-infection since the T-cell function

14
is the primary immune-mechanism (Didier 1995, Valencakova and Halanova 2012). As a
consequence increasing antibody titers can also be the result of a re-infection.
Serological tests are able to accurately define IgG and IgM antibody levels against the parasite. A
recent infection is indicated if both IgG and IgM are detected simultaneously (Jeklova et al. 2010).
During the further course of infection IgM levels decline and IgG antibody levels rise (Cox 1977).
Following up changes in the IgG and IgM titer thus enables an estimation of infection-time and a link
between clinical signs and infection (Boot 2002, Harcourt-Brown 2004, Csokai et al. 2009a). Four
weeks after the first blood sample a second blood sample could be collected to analyze the evolution
of the antibodies. A single negative result in a sick rabbit however makes it possible to rule out an E.
cuniculi manifestation and the veterinarian must then search for other underlying causes (Keeble and
Shaw 2006).
Concluding, a rising antibody titer indicates an active infection, as does IgM (Harcourt-Brown 2004,
Csokai et al. 2009a).
There are different serological tests available. Those include an indirect immunofluorescence test
(IFA), enzyme-linked immunosorbent assay (ELISA) or a carbon immune assay (CIA) (Boot 2002). A
comparison between two indirect immunofluorescence assays, two ELISAs and the carbon
immunoassay revealed that all of them detected the same number of positive sera and are thus
suitable for a routine health monitoring. The ELISA-test is however inferior in determining the quantity
of antibodies compared to the others. The most commonly used serological test in the UK is the
indirect ELISA test. It measures IgG as well as IgM antibody titers (Harcourt-Brown 2004, Boot et al.
2000).
Another approach of a sophisticated ante-mortem diagnosis is the combination of serology using
ELISA and protein electrophoresis. Research showed that in rabbits with E. cuniculi infections the
albumin/globulin ratio was decreased and the beta-globulin level was increased, compared to clinically
normal rabbits. Those findings can then help to diagnose an infection, to determine the severity,
response to a therapy and determine the clinical course of the disease (Cray et al. 2009).
Generally it also takes at least four weeks after seroconversion that spores are shed in the urine
(Harcourt-Brown 2004). Kunstyr et al. (1986) even described a period of six weeks before spores were
found in the urine. Spores can normally be detected with special staining. One might thus conclude
that examining the urine might be an auspicious approach (Harcourt-Brown 2004). Benefits are among
others that urine can be sampled from the living animal and the organism is directly identified.
However, only 25% of experimentally infected rabbits excrete spores (Pye and Cox 1977) and even
when they do, shedding of spores happens intermittently, therefore making it unreliable as a
diagnostic tool. Moreover, spores are shed by symptomatic as well as asymptomatic rabbits. Detecting
spores does thus not allow the diagnosis of a clinical E. cuniculi manifestation (Cox and Gallichio
1977, Cox et al. 1979, Csokai et al. 2009a).

15
3.5.3. PCR
Different studies have been conducted testing PCR analysis as a quick and reliable diagnostic tool for
E. cunculi. Studies were conducted using PCR to detect the organism in vivo in cerebrospinal fluid
(CSF) and urine. Unfortunately both delivered unsatisfying and unreliable results in detecting the
parasite in subclinical as well as in clinically affected rabbits. Spores are only shed in the urine three to
six weeks after the seroconversion and excretion is not continually but intermittently. PCR results also
did not correlate with the severity of the disease (Csokai et al. 2009a). The most sensitive results were
gathered when using phacoemulsified lens material from rabbits with phacoclastic uveitis, possibly
due to a higher spore concentration (Stiles et al. 1997, Wolfer et al. 1993, Künzel et al. 2008, Csokai
et al. 2009a).
3.5.4. Other in vivo tests
Cytological examination of the CSF can also give valuable clues. CSF sampling is feasible but
contains a certain risk for the rabbit. In rabbits with encephalitozoonosis and neurological signs,
researchers found an increased concentration of protein and lymphomonocytic pleocytosis. The same
cytological changes can however also been seen in other CNS disorders (Jass et al. 2008).
Another diagnostic tool that can be used in vivo is the intradermal skin test (Harcourt-Brown 2004).
This proved to be an effective diagnostic tool, detecting circulating antibodies (IgG and IgM) and thus
revealing previous exposure to the parasite. The E. cuniculi antigen is injected intradermally on the
surface of the ear and read three days later. A positive reaction was marked by hyperemia and an
increase of thickness of the ear pinna (Waller 1977, Wosu et al. 1977, Pakes et al. 1984).
Sophisticated laparoscopic equipment might enable biopsy collection of, for example the kidneys, via
endoscopy for histopathological examination to support an in vivo diagnosis in the future.
3.5.5. Post mortem diagnostics
In the dead animal histological examination and special staining can be used for a post mortem
diagnosis. By histopathological examination the pathogen can be identified and histological changes
analyzed (Csokai et al. 2009b). Post mortem examination however does not always lead to a
conclusive diagnosis. In many chronically infected brain and/or renal tissues only small numbers of
the organism are present (Harcourt-Brown 2002, Csokai et al. 2009a, Csokai et al. 2009b), the
parasite is often difficult to find and thus regularly missed on necropsy (Percy and Barthold 2008,
Csokai et al. 2009b). Accordingly in a study the researchers found only very few spores even in
severe cerebral histologic lesions using Ziehl-Neelsen and acid-fast trichrome stains. The examined
renal tissues of clinically ill animals often already underwent chronic fibrotic and granulomatous
changes which also made it difficult to identify the organism (Csokai et al. 2009b). Histologic
demonstration of the organism allows however a definitive diagnosis (Pilny 2012). Besides identifying

16
distinct lesions and detecting the organism, necropsy can also help to detect lesions caused by other
diseases or agents that provoke similar clinical pictures and thus differentiate for other differential
diagnoses.
3.5.5.1. Histological lesions
The most typical histopathological finding of encephalitozoonosis is an altered appearance of the
kidneys. E. cuniculi characteristically causes sites of granulomatous inflammation in internal organs
such as the kidney, liver, heart and in particular the central nervous system. Spores might as well be
present, also in nearby tissues (Harcourt-Brown 2004).
Scars and pits on the surface of the kidneys are a common post mortem finding. E. cuniculi causes
granulomatous interstitial nephritis. Early lesions show focal granulomatous inflammation. Long-
standing lesions show interstitial fibrosis and collapse of the parenchyma, which gives the kidney a
characteristic pitted appearance. These lesions are explicit at post mortem examination and provide a
cheap, simple method of detecting previous E. cuniculi infection in the dead animal (Harcourt-Brown
2004). In a study from 1970 examining kidneys of young slaughtered rabbits all grossly affected
kidneys also had microscopic lesions of Encephalitozoon. The researchers found clusters of gram-
positive, rod-shaped organisms most frequently in the collecting tubes. They were found in groups
within cytoplasmic vacuoles. The parasite was demonstrated in 35% of the grossly affected kidneys.
Interestingly the number of organisms decreased as the lesions became older. The organism was
most common in acute lesions and absent in those of longest duration (Flatt and Jackson 1970).
In the ocular form the observed lesions include cataract, phacoclastic uveitis and hypopyon .When the
lens ruptures, inflammation around the rupture in the lens can be seen on histology. Also
granulomatous inflammatory infiltrations in the uvea were found (Harcourt-Brown 2004, Csokai et al.
2009b).
Necropsy of the brain mostly reveals a granulomatous meningoencephalitis and perivascular cuffs.
The cerebrum is the most frequently affected brain region. Cerebellum and the vestibular cores were
less commonly involved. Surprisingly, although paresis only occurs occasionally, 74.3% of the animals
showed lesions of the spinal cord (Csokai et al. 2009b).
In infected animals non-suppurative and granulomatous inflammatory infiltrations were also found in
various organs, such as heart, liver and lung (Csokai et al. 2009b). Cox et al. (1979) found lesions of
liver and lung especially prominent in the early stages of the infection.
3.5.5.2. Special staining
In order to detect spores special staining can be used such as Ziehl-Neelsen (ZN) and acid fast
trichrome (AFT). This method also enables the differentiation between Encephalitozoon and
Toxoplasma, since both cause similar lesions (Shadduck and Pakes 1971). It was found that ZN-
staining was slightly more sensitive compared to AFT. Compared to the other tests, special staining

17
for spore-detection proved to be the most sensitive method especially in the early stages of infection
(Csokai et al. 2009a).
PCR is another method for post mortem examination of organ samples. Research showed that the
brain was the most appropriate tissue for E. cuniculi DNA detection. As described earlier, the brain
and the kidneys are the main target organs for the parasite (Csokai et al. 2009b). PCR analysis does
nevertheless not allow determining the date of the infection. False negative results are probably due to
a low concentration, an irregular spore distribution in the organ samples or an early stage of infection
(Csokai et al. 2009a).
Summing up the findings, the diagnosis of E. cuniculi is at the moment still challenging and mostly
based on ruling out other differentials with the help of a thorough clinical examination, hematology,
biochemistry and radiology (Harcourt-Brown 2004). In the living animal the most sensitive method is
PCR on lens material in rabbits with phacoclastic uveitis. Not all rabbits have however ocular lesions
and even then is lens material difficult to collect. Hence, the most used technique in the living animal is
serology. When using PCR in the deceased animal the best results were gained when using brain
tissue. Special staining was the most sensitive method post mortem (Csokai et al. 2009). Improved
screening can also be accomplished with an immunofluorescence assay which detects antigen
instead of antibodies (Pilny 2012).
3.6 THERAPIES
Just like the diagnosis also the treatment of encephalitozoonosis is challenging and no uniform
treatment-protocols are available yet. Different drugs have been described in the literature but there is
generally insufficient proof regarding their efficiency. Not to forget the high number of asymptomatic
carriers that might nevertheless shed spores via their urine. Also there are no products registered for
the treatment of E. cuniculi in pet rabbits. Optimal treatment should aim to be parasiticidal, anti-
inflammatory and also symptomatic (Harcourt-Brown 2004).
The clinical signs that can be observed can either be caused directly by the parasite or by the induced
inflammation it provokes in different organs. Some changes are so severe in the chronic stage that
they are irreversible even after parasiticidal treatment (Harcourt-Brown 2004). Then again some signs,
caused by inflammation, can be self-limiting, falsifying results regarding treatment efficiency (Harcourt-
Brown and Holloway 2003).
Albendazole has a parasitostatic effect against Microsporidia (Colbourn et al. 1994) and even
eliminated spores in rabbit kidney cells (Weiss et al. 1994, Franssen et al.1995). It also shows a
good oral absorption (Didier 2000). The required duration of treatment for encephalitozoonosis has not
been determined in rabbits. The author chose for an empirical dose of 20mg/kg for three to 14 days. A
higher dose or longer period may however be necessary to become asymptomatic and prevent
relapse (Harcourt-Brown 2004). Since albendazole has severe side effects in rabbits including bone
marrow suppression and liver failure it is no longer an adequate choice (Mortiz 2004).

18
The study by Franssen and colleagues (1995) tested the susceptibility of different drugs in vitro and
also found fumagillin, oxibendazole and thiabendazole to have a parasitostatic effect. Fumagillin is
however not applicable for veterinary use due to its toxicity.
Another study described the successful prophylactic and chemotherapeutic treatment of E. cuniculi
infections in rabbits with fenbendazole in 2001. Afterwards it became increasingly popular and is at
present the drug of choice. In this very study the author used 20mg/kg daily for 28days. If necessary
the treatment can be repeated after six months. It is however orally not absorbed as good as
albendazole (Suter et al. 2001). Albendazole and fenbendazole are both benzimidazoles. They inhibit
the microtubule, thus blocking extrusion of the polar filament and prevent cell infection (Katyar et al.
1994).
Broad spectrum antibiotics can be beneficial to prevent or eliminate secondary infections as well
(Harcourt-Brown 2004, Ewringmann and Göbel 1999).
Since E. cuniculi triggers an inflammatory reaction, supportive care with anti-inflammatory or
immunosuppressive medication might be necessary too. Corticosteroids are normally the drug of
choice for immunosuppression. Given the immunosuppressive effect of E. cuniculi itself, adding an
immunosuppressive long-time treatment is contraindicated. Alternatively a single dose of a short-
acting corticosteroid (e.g. 1-2mg/kg dexamethasone) can be given to rabbits with acute neurological
signs. It is important to consider the rabbit`s extreme sensibility to their side effects though (Harcourt-
Brown 2004). Another option is to use anti-inflammatory instead of immunosuppressive doses.
Besides corticosteroids there are also anti-inflammatory alternatives available such as Cox-2 inhibitors
or flunixin meglumide (Harcourt-Brown 2004). Another immunosuppressive drug, cyclophosphamide,
which was experimentally used in infected rabbits, resulted in death of the treated animals (Horvath
1999).
For rabbits with vestibular signs it is advisable to start E. cuniculi treatment directly. An alternative
treatment option for vestibular signs is prochlorperazine, a human drug against vertigo, in dosage 0.2-
0.5mg/kg orally every eight hours. This only relieves the symptoms and does not have an effect on the
parasite itself though. For seizures, benzodiazepines such as diazepam or midazolam might be used.
Furthermore rabbits with renal problems can be helped with a supportive and symptomatic treatment.
When suffering from incontinency the hair around the perineum should be clipped to avoid infection.
Also pain medication (carprofen 2-4mg/kg SC/IV or meloxicam 0.1-0.2mg/kg orally) might be
beneficial. Advanced renal disease can only be treated symptomatically. It is important to ensure
hydration and limit calcium intake, since excretion is impaired and can lead to soft tissue
mineralization. Recommended is hay and grass low in calcium as well as fruit and vegetables. Alfalfa
is high in calcium and therefore not recommended. Carrot, apple and cabbage should also only be fed
in restricted amounts. If the animal is severely ill assisted feeding might be necessary (Harcourt-Brown
2004).
For rabbits that suffer from the ocular form different treatment approaches have been tested. The
treatment with systemic and topical oxytetracycline and dexamethasone is described (Ewringmann

19
and Göbel 1999). When presented in an early stage, before developing synechia, phtysis or glaucoma
phacoemulsification of the lens together with topical anti-inflammatory therapy can be considered
(Sandmeyer et al. 2011). However enucleation might be necessary when previous approaches are
insufficient (Stiles et al. 1997, Wolfer et al. 1993).
3.7 ERADICATION
To reduce seroprevalence in rabbit colonies it takes time and money. Ideally rabbits get tested,
isolated if positive and treated with fenbendazole (Waller et al. 1978). Seroconversion occurs before
spore-excretion so infected and seropositive animals can be isolated before infecting others. A
prophylactic treatment of in-contact animals with fenbendazole for 28 days can reduce the risk of
infection and also minimizing infection by good hygiene is highly recommended (Harcourt-Brown
2004). Those include the use of water bottles instead of bowls and to raise the food bowls to prevent
urinary contamination (Keeble and Shaw 2006). Also consider that the spores are very resistant and
can survive in the environment in extreme conditions and up to four weeks at room temperature under
dry conditions (Kucerova-Pospisilova et al. 1999). Spores can be destroyed by boiling, autoclaving
and many standard disinfectants (Waller 1979). Exposure of spores with dilutions of bleach at more
than 1% or 70% ethanol for at least 30 seconds inhibited human fibroblast cell infection, as did diluted
bleach at 0.1% when exposed for seven minutes or longer (Jordan et al. 2006). Furuya (2009) also
found UV-light irradiation and ozone to be effective.
3.8 PROGNOSIS
The different clinical pictures of encephalitozoonosis also reflect the quality of life and the prognosis.
In general the prognosis is rather guarded, but cases have been described where rabbits recovered
completely and the parasite was eliminated. The prognosis also depends on the severity and degree
of histological changes. Some lesions are chronic and irreversible even after parasiticidal treatment.
Generally speaking it was observed that vestibular neurological signs have the least effect on the
wellbeing of the rabbit and also a better prognosis. The degree of torticollis can be used as a
prognostic factor (Künzel et al. 2008). Rabbits with non-vestibular neurological symptoms or the renal
form more often suffered from secondary problems such as anorexia and weight loss and have the
worst prognosis. Patients with renal failure were most likely to die or be euthanized. Rabbits with
neurological signs however showed a survival rate of 50% (Harcourt-Brown and Holloway 2003,
Künzel et al. 2008). The best prognosis and the least effect on well-being, at least in the early stage, is
the ocular form. Via phacoemulsification uveitis can be treated and vision restored. In an advanced
stage however the prognosis is guarded to poor and enucleation the treatment of choice (Sandmeyer
et al. 2011).

20
4. DISCUSSION
The patient was initially presented with bilateral eye problems and was finally diagnosed with multiple
clinical abnormalities.
The right eye had a haze on the cornea for already several years accompanied by scar formation,
neovascularization and serous ocular discharge. The lacrimal duct was impermeable and it was also
the right eye that showed the cataract. The left eye showed a haze without discharge that had
developed just recently and the fluorescein test was mildly positive. Ocular lesions are often
associated with encephalitozoonosis, but not all of the mentioned signs are typical for the disease.
Characteristic for E. cuniculi is cataract, which was present in the right eye and is frequently followed
by hypopyon or a phacoclastic uveitis in case of lens rupture (Harcourt-Brown 2004), which could not
be seen in Mimi. Also a keratoconjunctivitis has been described in the literature concerning E. cuniculi,
even though less commonly (Lallo 2005). Keratoconjunctivitis would explain the bilateral opacity of the
cornea as well as the discharge. Another option for the unilateral ocular discharge could however also
be the obstructed lacrimal duct. In rabbits there is a single nasolacrimal punctum and the duct runs
through the lacrimal and frontal bones, passing close to the molar and incisor tooth roots and is thus
easily affected by dental abnormalities. Also bacterial infection, causing a dacrocystitis, can be seen
regularly. The lacrimal sac accommodates a broad bacterial flora with Pasteurella multocida en
Staphylococcus aureus being the most important ones (Marini et al. 1996, Williams 2007). One would
expect a more purulent discharge then however.
The mildly positive fluorescein test indicates the presence of a superficial cornea ulcer in the left eye.
Reasons therefore include traumatic causes, viral infections (Myxoma virus), secondary to bacterial
infection (e.g. blepharoconjunctivitis or dacrocystitis), dry eyes (primary or secondary) or a vitamin A
deficiency. The lesion to be caused by E. cuniculi is less likely.
Summarizing, it seems that besides E. cuniculi there are more underlying problems responsible for the
eye problems. The unilateral cataract is a typical sign for encephalitozoonosis but the other symptoms
are not. For a definitive diagnosis one could phacoemulsify the lens and use PCR to identify the
parasite. As mentioned earlier, this is the most sensitive method, invasive and expensive however.
Continuing diagnostics are necessary for identifying further causes. A thorough ophthalmological
examination could give further indications, as could a conjunctival swab for a bacteriologic culture or a
dacryocystorhinogram to evaluate the lacrimal duct (Williams 2007).
The lesions of the lens are irreversible. The ulcer of the left eye could be treated by debridement and
antibiotic eye ointments together with analgesics if necessary (Williams 2007).
Diagnostics of an infection with Encephalitozoon cuniculi should always start with a thorough clinical
and neurological examination. Neurological impairment is often and especially since rabbits being prey
animals not very evident and should be interpreted carefully. In the case of Mimi no specific
neurological examination was conducted. In retrospective it is thus impossible to tell if the head tilt was
the only neurological anomaly.
As described during the literature review another variant of encephalitozoonosis is the renal form.

21
Caused by the renal impairment to excrete minerals, soft tissue mineralization is a common sign.
Interestingly Mimi also showed mineralization of the kidneys, which might be an indication of a renal
involvement. That would also mean that in this case the rabbit showed a combined clinical picture
which comprises all three forms (ocular, neurological and renal).
The cataract and haze of the right eye are chronic lesions that Mimi had for already several years.
Also the scar formation and vascularization on the cornea are indications for an ongoing problem. The
head tilt the owners noticed only several months ago. The problems of the left eye (haze and cornea
damage) are recent.
It is impossible to predict tumor growth, but considering the distinct alterations and increased size of
the uterus I would expect that the uterus pathology is also already present for at least several weeks,
possibly months. Greene (1959) describes in his study growth of a uterine adenocarcinoma in rabbits
up to a hen`s egg within six months and the period from detection to metastasis to take around twelve
months. Uterine adenocarcinomas are the most common neoplasm in rabbits, primarily seen in does
of medium age and are often accompanied by mammary neoplasia (Greene 1959).
Interestingly Mimi was operated two years ago because of a mammary tumor, she is also middle-aged
and not castrated. Subsequently she is predisposed to develop a uterine adenocarcinoma.
A tumor can be an enormous stress factor for an animal. In E. cuniculi infected rabbits stress can be
sufficient to cause an imbalance between the parasite and the hosts’ immunity, shifting it in favor of E.
cuniculi. Let us suppose that the tumor is also present for already a couple of months, as is the head
tilt. That could indicate that the adenocarcinoma might have been the trigger causing the imbalance
between parasite and host, leading to a clinical outbreak, expressed by the head tilt.
It stays uncertain which role the parasite played in the development of the cornea opacities and ulcer,
or if those are two separate problems.
The used diagnostic tools comprise clinical examination, ophthalmologic examination, medical
imaging and serological tests determining IgM and IgG antibodies against E. cuniculi. The
ophthalmologist saw only pictures of Mimi`s eyes and based the prognosis and treatment options
thereupon. Also no specific neurological examination was conducted. Based on the used diagnostic
tools it is not possible to make a definitive diagnosis of encephalitozoonosis for Mimi, nor for an
adenocarcinoma.
The most used diagnostic tool is serology. When determining IgG and IGM it allows identifying an
active infection, as was the case in Mimi. Also taking a second blood sample after four weeks is done
sometimes to follow up the evolution of the antibody titer. That is however time-costly and does not
give any extra information since we already know that we are dealing with a recent infection, re-
infection of re-activation. It is to mention though that a study by Jeklova et al. (2010) found that 24% of
clinically healthy rabbits and 26% of the rabbits that showed clinical signs that were not related to E.
cuniculi, showed E. cuniculi specific IgM antibodies as well.
There are more options that could have been implemented. A general blood count with protein-
electrophoresis can also give a hint regarding an infection. Seropositive animals with clinical

22
symptoms had an increased gamma-globulins and a decreased albumin/globulin ratio. This tool is
however not suitable for a definitive diagnosis and can also be seen in other diseases (Cray et al.
2009). The same goes for analyzing urine-sediment with special staining or immunofluorescence.
Spores are shed intermittently and also by healthy animals (Csokai et al. 2009a). The most promising
tool would be a PCR on lens material of the affected lens (Künzel et al. 2008, Csokai et al. 2009a),
this is however very costly and would not make a difference regarding the treatment protocol, since
cataract cannot be resolved by a parasiticidal treatment. PCR on CSF or urine are further options, but
again of little diagnostic value, due to a low sensitivity of the technique (Csokai et al. 2009a).
All possible diagnostic tests have to be considered in the light of feasibility regarding costs and
facilities/equipment of the animal clinic as well as if they have any added value in making the
diagnosis or influencing the treatment protocol. For example, it is not important to know if the cataract
is caused by E. cuniculi since medical treatment cannot improve the condition and the owner decided
against surgery (e.g. phacoemulsification). The same goes for the uterine mass.
Fenbendazole treatment was started immediately for two reasons. Firstly, the owner decided at the
first consultation for surgery to remove the mass. Surgery puts the animal under a lot of stress,
therefore it is important to have the disease controlled beforehand. Secondly, serology showed
positive IgM titers, which is indicative for an active infection and not just previous exposure. X-ray
photos were also taken, since the presence of metastases would deteriorate the prognosis. The
owners decided later on however against surgery and further treatment.
The rabbit had a very mild head tilt that did not cause discomfort or distress. With the fenbendazole
treatment the chance to resolve the milt head tilt was existing but also rather poor. Further treatment
for the vestibular signs was thought not to be necessary. Except the mineralization of the kidneys,
seen on medical imaging, no signs of renal failure could be seen. Consequently no treatment was
prescribed. It is important however to keep an eye on the renal function and if necessary start a
symptomatic treatment (ensure hydration, limited calcium-intake etc). Regarding the ocular lesions,
except with phacoemulsification or even enucleation, there is not much that can be done about the
cataract. It might however be interesting to conduct further investigation regarding the corneal
opacities, obstructed lacrimal duct and serous discharge. For the ulceration on the left eye the
ophthalmologist proposed debridement to support the healing process, although with a limited chance
of success. Besides the debridement topical antibiotics against secondary bacterial infections and in
case of pain, analgesics such as meloxicam or carprofen might be necessary too.

23
5. REFERENCES
1. Ashton N and Wirasinha PA (1973) British Journal of ophthalmology. 57: 669
2. Ashton N, Cook C and Clegg F (1976) Encephalitozoonosis (nosematosis) causing bilateral
cataract in a rabbit. British Journal of ophthalmology. 60: 618- 631
3. Baneux PJR and Pognan F (2002) In utero transmission of Encephalitozoon cuniculi strain type I
in rabbits. Laboratory animals. 37: 132-138
4. Bart A, Wentink-Bonnema EM, Heddema ER et al. ( 2008) Frequent occurrence of human
associated Microsporidia in fecal droppings of urban pigeons in Amsterdam, The Netherlands.
Applied and environmental microbiology. 74 (22): 7056-7058
5. Beckwith C, Peterson N, Liu JJ and Shadduck JA (1988) Dot enzyme-linked immunosorbent
assay (dot ELISA) for antibodies to Encephalitozoon cuniculi. Laboratory Animal Science. 38(5):
573-576
6. Boot R, Hansen AK, Hansen CK et al. (2000) Comparison of assays for antibodies to
Encephalitozoon cuniculi in rabbits. Laboratory animals. 34: 281-289
7. Boot R (2002) Serologisch onderzoek van konijnen op infectie met Encephalitozoon cuniculi.
Tijdschrift voor diergeneeskunde. 127 (13): 426- 427
8. Colbourn NI, Hollister WS, Curry A and Canning EU (1994) Activity of Albendazole against
Encephalitozoon cuniculi in vitro. European Journal of protistology. 30: 211-220
9. Cox JC (1977) Altered immune responsiveness associated with Encephalitozoon cuniculi infection
in rabbits. Infection and Immunity. 15: 392-395
10. Cox JC, Gallicho HA (1978) Serological and histological studies on adult rabbits with recent,
naturally acquired encephalitozoonosis. Ves Vet Sci 24: 260-261
11. Cox JC, Hamilton RC and Attwood HD (1979) An investigation of the route and progression of
Encephalitozoon cuniculi infection in adult rabbits. J Protozool 26(2): 260-265
12. Cox JC and Ross J (1980) A serological survey of Encephalitozoon cuniculi infection in the wild
rabbit in England and Scotland. Research in Veterinary Science. 28: 396
13. Csokai J, Joachim A, Gruber A et al. (2009a). Diagnostic markers for encephalitozoonosis in pet
rabbits. Journal of Veterinary Parasitology. 163: 18-26
14. Csokai J, Gruber A, Künzel F et al. (2009b) Encephalitozoonosis in pet rabbits (Oryctolagus
cuniculus): pathohistological findings in animals with latent infection versus clinical manifestation.
Parasitol Research. 104: 629-635
15. Deplazes P, Mathis A, Baumgartner R et al. (1996) Immunologic and molecular characteristics on
Encephalitozoon-like microsporidia isolated from humans and rabbits indicate that
Encephalitozoon cuniculi is a zoonotic parasite. Clinical infectious disease. 22: 557-559
16. Didier ES, Vossbrinck CR, Baker MD et al. (1995) Identification and characterization of three
Encephalitozoon cuniculi strains. Parasitology 111 (4): 411-421
17. Didier ES, Didier PJ, Snowden KF et al. (2000) Microsporidiosis in mammals. Microbes and
infection. 2: 709-720

24
18. Didier ES (2005) Microsporidiosis: An emerging and opportunistic infection in humans and
animals. Acta Tropica. 94: 61-76
19. Ewringmann A and Göbel T (1999) Untersuchung zur Klinik und Therapie der Enzephalitozoonose
beim Heimtierkaninchen. Kleintierpraxis. 44: 357-372
20. Flatt RE and Jackson SJ (1970) Renal nosematosis in young rabbits. Path Vet. 7: 492-497
21. Franssen FFJ, Lumeij JT and Van Knapen F (1995) Susceptibility of Encephalitozoon cuniculi to
several drugs in vitro. Antimicrobial agents and chemotherapy. 39 (6): 1265-1268
22. Furuya K (2006) recent epidemiologic status and serodiagnosis of encephalitozoonosis. Journal of
the Japanese society of exotic pet medicine. 8:7-11
23. Furuya K (2009) Spore-Forming Microsporidian Encephalitozoon: Current Understanding of
Infection and Prevention in Japan. Japanese Journal of Infectious diseases. 62: 413-422
24. Giordano C, Weigt A, Vercelli A et al. (2005) Immunohistochemical identification of
Encephalitozoon cuniculi in phacoclastic uveitis in four rabbits. Vet ophtalmol 8(4): 271-275
25. Greene HSN (1959) Adenocarcinoma of the uterine fundus in the rabbit. Annals of the New York
Academy of Sciences. 75: 535-542
26. Harcourt-Brown FM (2002) Textbook of Rabbit Medicine. Oxford, UK, Butterworth Heinemann. Pp
365-368
27. Harcourt-Brown FM, Holloway HRR (2003) Encephalitozoon cuniculi in pet rabbits. Veterinary
records. 152: 427-431
28. Harcourt-Brown FM (2004) Encephalitozoon infection in rabbits. Seminars in Avian and Exotic Pet
medicine. 13 (2): 86-93
29. Horvath M, Leng L, Stefkovic M et al. (1999) Lethal encephalitozoonosis in cyclophosphamide-
treated rabbits (Abstract). Acta Veterinaria Hungarica. 47: 85-93
30. Jass A, Matiasek K, Henke J et al. (2008) Analysis of cerebrospinal fluid in healthy rabbits and
rabbits with clinically suspected encephalitozoonosis. The veterinary record. 10: 618-622
31. Jeklova E, Jekl V, Kovarcik K et al. (2010) Usefulness of detection of specific IgM and IgG
antibodies for diagnosis of clinical encephalitozoonosis in pet rabbits. Veterinary Parasitology.
170: 143-148
32. Jordan CN, DiCristina JA and Lindsay DS (2006) Activity of bleach, ethanol and two commercial
disinfectants against spores of Encephalitozoon cuniculi. Veterinary parasitology. 136: 343-346
33. Katyar SK, Gordon VR, McLaughlin GL and Edlind TD (1994) Antiprotozoal activities of
benzimidazoles and correlations with beta-tubulin sequence. Antimicrobial agents and
chemotherapy . 38 (9): 2086-2090
34. Keeble E (2006) Chapter 15: Nervous and muscoskeletal disorders. In: BSAVA Manual of rabbit
medicine and surgery, 2nd
edition. British Small Animal Veterinary Association, Quedgeley,
Gloucester. Blackwell Publishing Professional. p.107
35. Keeble EJ and Shaw DJ (2006) Seroprevalence of antibodies to Encephalitozoon cuniculi in
domestic rabbits in the United Kingdom. Veterinary record.158:539-544
36. Kucerova-Pospisilova Z, Carr D, Leitch G et al. (1999) Environmental resistance of
Encephalitozoon spores. Journal of Eukaryotic microbiology. 46: 11-13

25
37. Kunstyr I and Naumann S (1983) Head tilt in rabbits caused by Pasteurella and
encephalitozoonosis. Laboratory animal. 19: 208-213
38. Kunstyr I, Lev L and Naumann S (1986) Humoral antibody response of rabbits to experimental
infection with Encephalitozoon cuniculi. Veterinary Parasitology. 21: 223-232
39. Künzel F, Gruber A, Tichy A et al. (2008) Clinical symptoms and diagnosis of encephalitozoonosis
in pet rabbits. Veterinary parasitology. 151: 115-124
40. Lallo MA (2005) Microsporidia Infections in Immunocompromised Hosts. In: Bacterial and Mycotic
Infections in Immunocompromised Hosts: Clinical and Microbiological Aspects. Omics ebooks.
p.2-6 (consulted on 6.12.2016 at 18:04)
41. Lyngset A (1980) A survey of serum antibodies to Encephalitozoon cuniculi in breeding rabbits
and their young. Laboratory animal science. 30: 558-561
42. Marini RP, Foltz CJ, Kersten D et al. (1996) Microbiologic, radiographic and anatomic study of the
nasolacrimal duct apparatus in the rabbit (Oryctolagus cuniculus). Lab Anim Sci. 46:656–662
43. Mortiz C (2004) Reactions in albendazole treated rabbits. Exotic DVM. 6(4): 21-22
44. Pakes SP, Shadduck JA, Feldman DB and Moore JA (1984) Comparison of tests for the diagnosis
of spontaneous encephalitozoonosis in rabbits. Laboratory Animal Science. 34 (4): 356-359
45. Pang VF and Shadduck JA (1985) Susceptibilty of cats, sheep and swine to a rabbit isolate of
Encephalitozoon cuniculi. American Journal of Veterinary Research. 46: 1071-1077
46. PDSA (2015) PDSA Animal Wellbeing Report. Available from: https://www.pdsa.org.uk/get-
involved/our-current-campaigns/pdsa-animal-wellbeing-report. (consulted on December 12th 2015.
47. Percy D and Barthold S (2008) Rabbit. Parasitic diseases. In: Pathology of Laboratory rodents and
rabbits. Third edition. Blackwell Publishing. Ames, Iowa, USA. Pp. 285-297.
48. Pilny AA (2012) Excellence in exotics: case report: Encephalitozoon cuniculi – associated
Phacoclastic uveitis in a dwarf rabbit. Compendium: Continuing Education for Veterinarians® 34
(11): E5 (Consulted on 2. January 2016)
49. Pye D and Cox JC (1977) Isolation of Encephalitozoon cuniculi from urine samples. Laboratory
animals. 11: 233-234
50. Rich G (2010) Clinical update on testing modalities for Encephalitozoon cuniculi in clinically sick
rabbits. Journal of Exotic Pet Medicine. 19 (3): 226-230
51. Sandmeyer SL, Bauer BS and Grahn BH (2011) Diagnostic ophthalmology. Canadian veterinary
journal. 52 (3): 327-328
52. Shadduck JA and Pakes SP (1971) Encephalitozoonosis (nosematosis) and toxoplasmosis.
American Journal of pathology. 64: 657-671
53. Shadduck JA, Watson WT, Pakes SP and Cali A (1979) Animal infectivity of Encephalitozoon
cuniculi. Journal of Parasitology. 65: 123-129
54. Stiles J, Didier E, Ritchie B et al. (1997) Encephalitozoon cuniculi in the lens of a rabbit with
phacoclastic uveitis: Confirmation and treatment. Vet Comp Ophtalmology. 7: 233-238
55. Suter C, Müller-Doblies UU, Hatt JM and Deplazes P (2001) Prevention and treatment of
Encephalitozoon cuniculi infection in rabbits with fenbendazole. Veterinary record. 148: 478-480

26
56. Thomas C, Finn M, Twigg L et al. (1997) Microsporidia (Encephalitozoon cuniculi) in wild rabbits in
Australia. Australian Veterinary Journal. 75: 808-810
57. Varga M, (2014) Questions around Encephalitozoon cuniculi in rabbits. Veterinary Record 174:
347-348
58. Waller T (1977) The india-ink immunoreaction: a method for the rapid diagnosis of
encephalitozoonosis. Laboratory animal. 11: 93-97
59. Waller T, Morein B, Fabiansson E (1978) Humoral immune response to infection with
Encephalitozoon cuniculi in rabbits. Lab Animal 12: 145-148
60. Waller T (1979) Sensitivity of Encephalitozoon cuniculi to various temperatures, disinfectants and
drugs. Laboratory animals. 13: 227-230
61. Weiss LM, Michalakakis E, Coyle CM et al. (1994) The in vitro activity of albendazole against
Encephalitozoon cuniculi. Journal of eukaryotic microbiology. 41: 65S
62. Williams DL (2007) Laboratory Animal Ophthalmology. In: Veterinary Ophthalmology, 4th edition.
Blackwell Publishing: Oxford. pp. 1336 -1369
63. Wolfer J, Grahn B, Wilcock B et al. (1993) Phacoclastic uveitis in the rabbit. Prog Vet Comp
Opthalmol. 3: 92-97
64. Wosu NJ, Shadduck JA, Pakes SP et al. (1977) Diagnosis of encephalitozoonosis in
experimentally infected rabbits by intradermal and immunofluorescence tests. Laboratory Animal
Science. 27 (2): 210-216
65. Wright JH and Craighead EM (1922) Infectious motor paralysis in young rabbits. Journal of
Experimental medicine. 36: 135-140
Figures
Figure 1,2: Prof. dr. Katleen Hermans, Private archive
Figure 3,4,5: Department of Medical Imaging, Faculty of Veterinary Medicine, UGent

Promoter: Prof. dr. Jan Declercq
Co-Promoter: Dr. Elke van der Vekens, ECVDI
Case Report as part of the
Master`s Dissertation
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
Academic year 2015-2016
Case Report: Multiple digital squamous cell carcinomas in a Giant Schnauzer
By
Marleen PETERMANN
© 2016 Marleen Petermann

Disclaimer
Universiteit Gent, its employees and/or students, give no warranty that the information provided in this
thesis is accurate or exhaustive, nor that the content of this thesis will not constitute or result in any
infringement of third-party rights.
Ghent University, its employees and/or students do not accept any liability or responsibility for any use
which may be made of the content or information given in the thesis, nor for any reliance which may
be placed on any advice or information provided in this thesis.

Case Report as part of the
Master`s Dissertation
Promoter: Prof. dr. Jan Declercq
Co-Promoter: Dr. Elke van der Vekens, ECVDI
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
Academic year 2015-2016
Case Report: Multiple digital squamous cell carcinomas in a Giant Schnauzer
By
Marleen PETERMANN
© 2016 Marleen Petermann

Preface
This case report is the second part of my master thesis and is about a neoplastic disease that is
regularly seen in the Giant Schnauzer, more precisely about digital squamous cell carcinomas. I have
a special interest in dermatology as well as in medical imaging. This case report includes both. I
followed the patient in the teaching hospital of the veterinary university and I instantly found the case
incredibly interesting. Consequently I was very pleased that I was allowed to use it as my case report
to deepen my knowledge in both fields.
This thesis is dedicated to my parents and their beloved dog Henry.
The realization of my literature study was enabled by professional assistance and familial support. In
the first place I wish to thank my promoters prof. dr. Jan Declercq and dr. Elke van der Vekens for
their time and constructive criticism and also my parents for their advice, support and enabling (most
of) the ideas that get stuck in my head.

1
Table of contents
Abstract.....................................................................................................................................................1
Samenvatting ............................................................................................................................................2
1. Introduction ...........................................................................................................................................3
2. Case report ...........................................................................................................................................3
2.1.Patient details ........................................................................................................................3
2.2. Anamnesis ............................................................................................................................3
2.3. Physical examination ............................................................................................................4
2.4. Problem list ..........................................................................................................................4
2.5. Differential Diagnoses...........................................................................................................4
2.6. Diagnosis ..............................................................................................................................5
2.7. Therapy ................................................................................................................................7
2.8. Follow up .............................................................................................................................8
2.9. Prognosis .............................................................................................................................8
3. Literature review ...................................................................................................................................9
3.1. Introduction ...........................................................................................................................9
3.2. Differential Diagnoses...........................................................................................................9
3.3. Etiology .............................................................................................................................. 10
3.4. Epidemiology ..................................................................................................................... 10
3.5. Pathogenesis ..................................................................................................................... 12
3.6. Clinical signs ...................................................................................................................... 14
3.7. Metastases and recurrence ............................................................................................... 14
3.8. Diagnostics and Diagnosis ................................................................................................ 15
3.9. Therapies ........................................................................................................................... 18
3.10. Prognosis ......................................................................................................................... 20
4. Discussion ......................................................................................................................................... 21
References .................................................................................................................................................

Abstract
This case study describes the presentation of a male intact Giant Schnauzer of almost 11 years of
age. He was referred to the veterinary teaching hospital because of a digital mass on the right
forelimb. Previously the third toes of both fore limbs were amputated due to a presumptive diagnosis
of squamous cell carcinoma. Radiography of the front legs revealed osteolysis of the phalanges of
several toes. No pulmonary metastases were detected. The findings from radiology as well as
cytology suggested the mass to be a malignant neoplasm, most likely a digital squamous cell
carcinoma. The patient consequently underwent amputation of the affected digits except one, to avoid
functional impairment. According to the owner, 6 months later no visible recurrence was noted and the
dog is doing fine.
Digital squamous cell carcinomas are most commonly seen in dark-coated dogs of large breeds in the
age group of 7-11 years. Certain breeds including the Giant Schnauzer seem to be predisposed.
Symptoms include abnormal nails or onychomadesis, swollen toes, nailbed
ulceration and/or proliferation and limping. The tumors occur most frequently on one digit but multiple
tumors on different toes can be present or develop over a period of time. There is no consensus about
the incidence of metastases; the literature describes varying rates between 5 and 24%. Metastases
generally affect the regional lymph nodes and lungs. Surgical excision, like amputation of the involved
digit is the treatment of choice for dogs. Clinical reports suggest that 95% of dogs that underwent
amputation, showed 1 year survival. If the tumors developed in other parts of the digit besides the
nailbed, only 60% survived one year or more. Excision may be supplemented with radiation and
chemotherapy.
Key words: squamous cell carcinoma - Giant Schnauzer - digit - amputation - black coat

2
Samenvatting
In deze casus wordt een mannelijke intacte Reuzenschnauzer van bijna 11 jaar oud besproken. De
patient werd aangeboden in de universitaire dierenkliniek met een massa ter hoogte van de vijfde teen
van de linker voorpoot. Voorafgaand aan de opname werd de derde teen van beide voorpoten
geamputeerd op basis van het vermoeden van een plaveiselcelcarcinoom. Met behulp van
röntgenonderzoek werd osteolyse aan meerdere tenen van de voorpoten vastgesteld. Ook cytologisch
onderzoek van de massa wees op een kwaadaardig proces. Op de röntgenfoto’s van de thorax
werden geen metastasen vastgesteld. Na overleg tussen radiologen, dermatologen en chirurgen werd
besloten om alle aangetaste tenen, behalve de vierde van de linker voorpoot, te amputeren. Deze
teen heeft men niet geamputeerd omdat, dit de enige gewicht dragende teen was en tevens minder
aangetast door de osteolyse. Zes maanden na de amputatie doet de patiënt het voor de eigenares
goed en heeft geen klachten die wijzen op verdere recidieven of metastasen.
Digitale plaveiselcelcarcinomas zijn maligne tumoren die bovengemiddeld worden gediagnostiseerd
bij grote rassen met een donkere vacht. Bepaalde rassen blijken gepredisposeerd te zijn, waaronder
de Reuzenschnauzer. Klinische symptomen zijn afwijkende nagels of nagelverlies, dikke tenen,
nagelbed ulceratie en/of proliferatie en manken. Meestal is slechts één teen betrokken. Er kunnen
echter meerderde tenen simultaan aangetast zijn of achtereenvolgend aangetast worden. Metastasen
zijn minder frequent aanwezig en tasten de regionale lymfeknopen en /of de long aan. Chirurgische
amputatie met ruime marges is de meest aangewezen therapie. Verschillende studies beschrijven een
overlevingskans van 95% na één jaar. Ontstaan deze tumoren echter op andere plaatsen dan het
nagelbed, dan is de prognose minder gunstig en wordt er slechts een overlevingskans van 60% na
één jaar beschreven. Indien nodig kan de amputatie ondersteund worden door radio- en
chemotherapie.
Sleutelwoorden: overgangscelcarcinoma - Reuzenschnauzer - teen - amputatie - zwart vacht

3
Case Report: Multiple digital squamous cell carcinomas in
a Giant Schnauzer
1. INTRODUCTION
Nail problems are regularly seen in dogs and the innocent looking lesions can cover up malignant
neoplastic processes underneath. Digital canine squamous cell carcinomas (SCCs) are no recent
finding, but have been described more than 50 years ago (Liu et al. 1977). More recent findings are,
however, that some breeds seem to be over-represented including the Giant Schnauzer and in
general large breeds with black coats. Also SCCs are no rarity but account for the majority of
malignant digital neoplasms (Wobeser et al. 2007). There is scant scientific research on digital SCCs,
although the disease is well known and a hot topic in kennel clubs of predisposed breeds.
The following case report is about a Giant Schnauzer that developed multiple digital squamous cell
carcinomas over a period of time on different toes of the front feet.
2. CASE REPORT
2.1. PATIENT DETAILS
This case study is about a 10 years and 7 months old male intact Giant Schnauzer with a body weight
of 47.35kg and a completely black hair coat.
2.2. ANAMNESIS
The patient was referred to the faculty of veterinary medicine because of a digital mass and to get a
second opinion. In the beginning of 2014 and 2015 he underwent amputation of 2 separate digits that
showed abnormalities around the nails and were suspected of SCCs. The examination and surgery
were performed in another animal clinic. Due to technical problems in the latter clinic the radiographs
were no longer available. No histopathological examination of the amputated toes was furthermore
conducted. One week before presentation at the dermatologic unit of the faculty the owner noticed a
mass on the left fifth toe. Their own veterinarian once again recommended amputation of the affected
toes thereupon the owners decided to come to the faculty for a second opinion. The patient has no
medical history except for the toe abnormalities and according to the owner none of his siblings or
parents were ever diagnosed with SCCs. He ate and drank well and showed no functional impairment
due to the lesion.
At the time of presentation the patient received tramadol 300mg (Contramal®, Grünenthal GmbH) BID
and meloxicam oral suspension (Metacam ®, Boehringer Ingelheim GmbH) in a decreasing dose
starting from 0.1mg/kg. The owners furthermore bath the foot three times a day in a saline solution for
the unpleasant smell.

4
2.3. PHYSICAL EXAMINATION
On physical examination the dog was alert and very active, especially during manipulation. When
palpating the toes he showed a pain reaction.
During inspection the veterinarian noticed the absence of the third digits of both front legs.
Additionally, the fifth digit of the left front limb showed a proliferative and ulcerative lesion. The mass
was pink with a wet aspect, had a diameter of approximately 3 cm (figure 1 and 2) and the nail was
absent. On the same limb the fourth digit was swollen but the skin was intact and unremarkable. The
first digit of the right front leg was also enlarged but otherwise looked normal. The extant nails showed
no abnormalities and also the digits of the hind limbs seemed unaffected. The left prescapular lymph
node was moderately enlarged. The patient was not limping, but intermittently relieved the left
forelimb.
There were no other abnormalities detected on physical examination.
2. 4. PROBLEM LIST
proliferative and ulcerative lesion of the fifth toe of the left front limb
enlarged fourth digit of the left front limb and first digit of the right front limb
prominent left prescapular lymph node
2. 5. DIFFERENTIAL DIAGNOSES
Different or the same of the following pathologies can be responsible for the involvement of multiple
digits.
Neoplasia
o Malignant
Squamous cell carcinoma
Fig. 1: Giant Schnauzer with a visible mass on
the fifth left digit. The third toe of both front legs
is amputated (Picture: Jan Declercq).
Fig. 2: Detail photograph of the fifth digit of the
left front leg. The nail is missing and a pink
mass is visible (Picture: Jan Declercq).

5
Fig. 3: Photomicropgraph of an FNA
performed on the digital mass stained with
H&E. Pleomorphic population of nucleated
squamous cells with numerous features of
malignancy (Picture: Private archive Jan
Declercq).
Fig. 4: A small cluster of cells in an
inflammatory background displays
anisokaryosis, multinucleation and high
cytoplasmic-nuclear ratio
(Picture: Private archive Jan Declercq).
Nailbed melanoma
Hemangiosarcoma
Osteosarcoma
Others, including soft tissue sarcoma, mast cell tumor and
hemangiopericytoma
o Benign
Subungual keratoacanthoma
Inflammatory lesions
o Paronychia
o Pyogranulomatous inflammation
o Trauma
o Osteomyelitis
o Foreign body
Hair follicle inclusion cyst
To rule out some of the differentials it was decided to conduct a fine needle aspiration of the
proliferative lesion under sedation for cytology and to take radiographs of the digits and thorax to
evaluate involvement of the underlying structures and detect potential metastases.
2.6. DIAGNOSIS
Cytology of the digital mass revealed a malignant process that was consistent with a tentative
diagnosis of a squamous cell carcinoma. The prescapular lymph node was not further inspected. The
examined cells show malignancy criteria such as anisokaryosis, multinucleation, a high cytoplasmic-
nuclear ratio and a pleomorphic population of nucleated squamous cells (figure 3). The background
shows inflammatory cells including neutrophils (figure 4).

6
Fig. 5: Left lower limb with prominent
osteolysis of the 3rd
phalanx of the 5th
digit (Picture: Department of Medical
Imaging, Faculty of Veterinary
Medicine, UGent).
Fig. 6: Right lower limb of a dog with
multicentric digital squamous cell
carcinomas. The third phalanges of digit
2 and 4 show osteolysis and mild
osteopenia of the 3rd
phalanges of the
2nd
and 5th digits (Picture: Department of
Medical Imaging, Faculty of Veterinary
Medicine, UGent).
The radiographs showed the following alterations.
Dorsopalmar radiograph of the left foot:
The radiographs show soft tissue swelling most pronounced
surrounding the 5th digit, but subjectively also present around
the 2nd
and 4th digit. Absence of all the phalanges of the 3
rd
digit can be seen. Moreover there is osteolysis of the distal
part of the third phalanx of the fifth digit, a beginning
osteopenia of the third phalanges of the 2nd
and 4th digits.
These findings were consistent with an ongoing aggressive
osteolytic process involving the third phalanx of the 5th, 4
th and
2nd
digit (figure 5).
Dorsopalmar radiograph of the right foot:
The radiograph of the right foot shows soft tissue swelling most
pronounced surrounding the 4th digit and subjectively also
present around the 1st, 2
nd, and 5
th toe. Additionally the absence
of phalanx 3, 2 and the distal part of phalanx 1 of the 3rd
digit is
visible. There is osteolysis of the distal part of the 3rd
phalanx of
the 1st and 4
th digits and mild osteopenia of the 3
rd phalanges of
the 2nd
and 5th digits (figure 6).

7
Fig. 7: .Left lateral radiograph of the thorax.
Spondylosis deformans between T5-8 is visible
(Picture: Department of Medical Imaging,
Faculty of Veterinary Medicine, UGent).
Fig. 8: Ventro-dorsal radiograph of the
thorax. A mild broncho-interstitial lung
pattern is detectable. No pulmonary
metastases can be seen (Picture:
Department of Medical Imaging, Faculty of
Veterinary Medicine, UGent).
Thorax radiographs:
Thoracic vertebral spondylosis deformans (T5-T8), a mild diffuse broncho-interstitial lung pattern
(most likely age-related) and no radiographic signs of pulmonary metastasis are visible on the thoracic
radiographs (figure 7, 8).
2.7. THERAPY
The lesions were due to a malignant neoplastic process and it was decided to amputate the toes that
showed osteolysis. The surgeons let the owners decide between preventively amputating all the
phalanges of the front feet or only the most affected digits. The owners chose the latter.
The skin incision during surgery was made dorsally starting proximal of the respective joint and
continuing lateral and medial to the palmar side. Hemostasis was ensured by bipolar
electrocoagulation. On the left front limb the 2nd
and 5th toes were amputated. Although the 4
th toe
showed osteolytic signs as well the surgeons decided against amputation to retain a weight-bearing
toe. On the right front limb 1st
and 4th
digit were amputated. The 4th toe was amputated, although
being the only remaining weight-bearing toe, due to more severe bone invasion.
Consequently, the 1st and 4
th digit of the left foot remained and the 2
nd and 5
th toe of the right foot.
On the right 4th digit and digit 2 and 4 of the left front limb the dissection was carried out through the
proximal interphalangeal joint. The distal phalanges of the 1st right digit were amputated at the
metacarpophalangeal joint. The sesamoid bones were removed and the incisions sutured. No
histopathological examination was conducted on the excised toes.

8
2.8. FOLLOW UP
The patient consequently received antibiotics and analgesics for 5 days; the bandage had to stay on
for 5 days also and was then exchanged twice for a bandage that stayed on for respectively 1 week.
The sutures were removed after 2 weeks. The healing of the wound went without any complications.
Six months after surgery the patient was doing well, he is not limping, does not show lesions, nail
problems or swelling on the extant toes. He tolerated the amputation of the digits very well, and can
walk without functional impairment.
2.9. PROGNOSIS
The prognosis after the amputation of the digits after a SCC is good to guarded. Metastases to the
regional lymph nodes develop in 5-29% of the patients (13% already have metastases at time of
diagnosis; Henry et al. 2005, Marino et al. 1995, Frese et al. 1983). According to different studies 60-
95% of the patients survive for more than one year and 43-74% for more than two years (O`Brien et
al. 1992, Marino et al. 1995, Foale and Demetriou 2010, Kessler 2012).
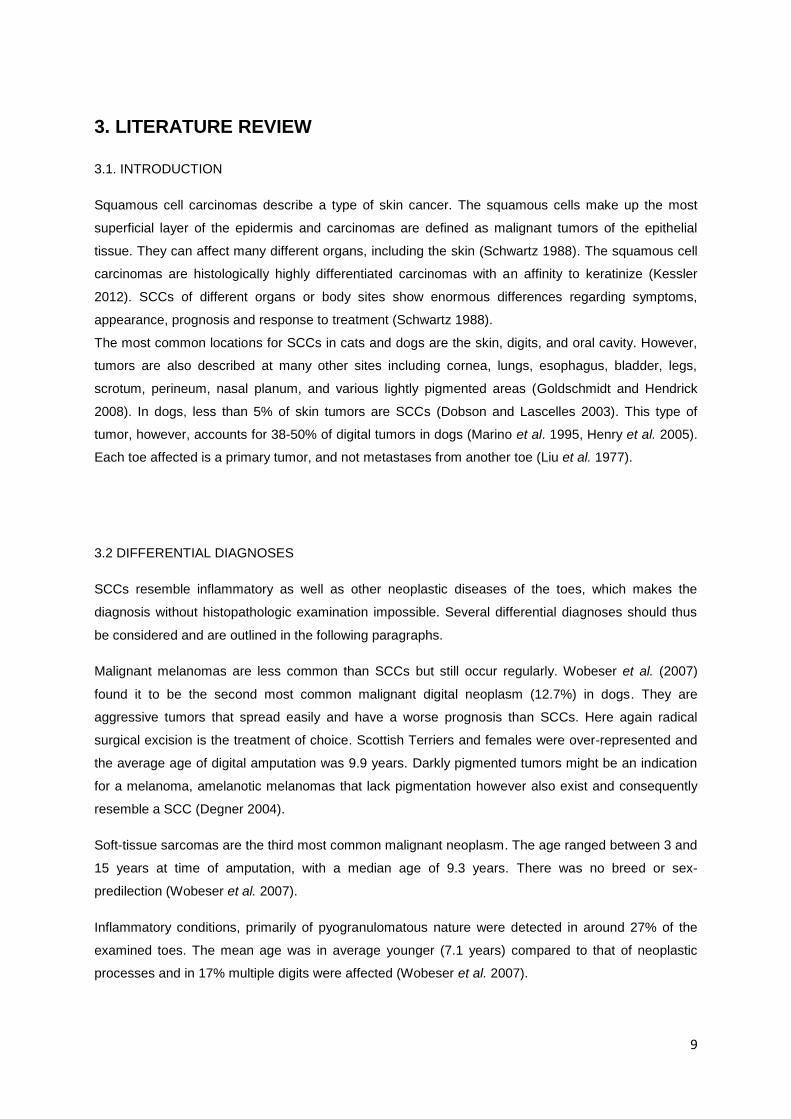
9
3. LITERATURE REVIEW
3.1. INTRODUCTION
Squamous cell carcinomas describe a type of skin cancer. The squamous cells make up the most
superficial layer of the epidermis and carcinomas are defined as malignant tumors of the epithelial
tissue. They can affect many different organs, including the skin (Schwartz 1988). The squamous cell
carcinomas are histologically highly differentiated carcinomas with an affinity to keratinize (Kessler
2012). SCCs of different organs or body sites show enormous differences regarding symptoms,
appearance, prognosis and response to treatment (Schwartz 1988).
The most common locations for SCCs in cats and dogs are the skin, digits, and oral cavity. However,
tumors are also described at many other sites including cornea, lungs, esophagus, bladder, legs,
scrotum, perineum, nasal planum, and various lightly pigmented areas (Goldschmidt and Hendrick
2008). In dogs, less than 5% of skin tumors are SCCs (Dobson and Lascelles 2003). This type of
tumor, however, accounts for 38-50% of digital tumors in dogs (Marino et al. 1995, Henry et al. 2005).
Each toe affected is a primary tumor, and not metastases from another toe (Liu et al. 1977).
3.2 DIFFERENTIAL DIAGNOSES
SCCs resemble inflammatory as well as other neoplastic diseases of the toes, which makes the
diagnosis without histopathologic examination impossible. Several differential diagnoses should thus
be considered and are outlined in the following paragraphs.
Malignant melanomas are less common than SCCs but still occur regularly. Wobeser et al. (2007)
found it to be the second most common malignant digital neoplasm (12.7%) in dogs. They are
aggressive tumors that spread easily and have a worse prognosis than SCCs. Here again radical
surgical excision is the treatment of choice. Scottish Terriers and females were over-represented and
the average age of digital amputation was 9.9 years. Darkly pigmented tumors might be an indication
for a melanoma, amelanotic melanomas that lack pigmentation however also exist and consequently
resemble a SCC (Degner 2004).
Soft-tissue sarcomas are the third most common malignant neoplasm. The age ranged between 3 and
15 years at time of amputation, with a median age of 9.3 years. There was no breed or sex-
predilection (Wobeser et al. 2007).
Inflammatory conditions, primarily of pyogranulomatous nature were detected in around 27% of the
examined toes. The mean age was in average younger (7.1 years) compared to that of neoplastic
processes and in 17% multiple digits were affected (Wobeser et al. 2007).

10
Mast cell tumor can also account for digital masses. In a study the affected dogs were between 5 and
17 years of age and multiple tumors on one foot were described. The 1- year survival rate was 75%
and after 2- years 62.5% were still alive. In this study however, only a limited number of patients was
available (Wobeser et al. 2007).
3.3 ETIOLOGY
The exact etiology of digital squamous cell carcinomas in dogs is still unknown, but different factors
seem to be involved (Dobson and Lascelles 2003).
Squamous cell carcinomas are generally known to be related to solar exposure and usually arise in
un- or lightly pigmented and sparsely haired skin (North and Banks 2009, Hargis et al. 1977). Digital
SCCs on the other side are not associated with UV-light exposure (Dobson and Lascelles 2003) and
heavy pigmentation seems, paradoxically, even to be a predisposing factor (Paradis et al. 1989,
Dobson and Lascelles 2003). Also, no hereditary factors seem to be involved in non-digital SCCs
(Frese et al. 1983, O`Rourke 1985), in contrast to digital SCC where a significant breed-predisposition
could be revealed. Moreover an inherited predisposition for developing SCCs seems likely. Single or
multiple digital SCCs were diagnosed in 3 related Giant Schnauzers (mother, daughter, son; Paradis
et al. 1989).
In men, besides solar irradiation other etiological factors have been identified, including chronic
infection and trauma, caustics and ultraviolet radiation. Different chemical carcinogens (e.g. tar or
arsenical compounds) are known to produce pre-malignant epidermal lesions that might progress to
squamous cell carcinomas (Paradis et al. 1989, Byers and Fleischman 1984). More research is
necessary to identify specific etiologies for digital SCCs in dogs.
3.4 EPIDEMIOLOGY
3.4.1. Prevalence of common digital tumors
Neoplastic disease in the digit of dogs is common as well as diverse. Tumors are responsible for 12%
of the disorders of the nail and nailbed in dogs (O`Brien et al. 1992). A study revealed that 101 of 124
digital masses were neoplasms, comprising 61% malignant neoplasms, 20% benign neoplasms and
19% pyogranulomatous inflammations (Marino et al. 1995). Another study analyzed the prevalence of
different diagnoses of surgically amputated canine digits. Around 73% of the amputated digits showed
neoplastic alterations, whereof 30 different neoplastic processes were identified. The other 27%
showed exclusively inflammatory lesions. The majority of the neoplasms (77.7%) were malignant, with
SCCs (36.3%) being the most common one. Following SCCs, other frequent digital neoplasms include
melanomas (17.3%), soft-tissue sarcomas (9.7%) and mast cell tumors (6.7%; Wobeser et al. 2007).
In a comparable retrospective study about canine digital tumors SCCs accounted for an even higher
number of diagnosed digital tumors, namely 51.6%. Here again second came malignant melanomas
accounting for 15.6% of the tumors, then osteosarcomas (6.3%), hemangiopericytomas (4.7%),

11
benign soft tissue tumors (7.8%) and malignant soft tissue tumors (14%; Henry et al. 2005). Similar
results were obtained by Belluco et al. (2013) who found 47.4% of all malignant canine digital lesions
to be squamous cell carcinomas.
In summary the prevalence of digital neoplasms is high in dogs with digit masses and they are more
frequently malignant than benign. SCCs are the most common digital tumors (Marino et al. 1995).
3.4.2. Breed predisposition
Squamous cell carcinomas are most commonly seen in large breed dogs with black coats (Vail and
Withrow 2007). In a study 92% of the dogs with digital SCCs were dark-haired and 75.2% belonged to
large and giant breeds (Belluco et al. 2013). Moreover, certain breeds seem to be over-represented.
Standard Poodles, Rottweilers and Giant Schnauzers were the breeds with the highest percentages of
malignant neoplasms present in amputated digits, with respectively 88.9%, 86.4% and 80% (Wobeser
et al. 2007, O`Brien et al. 1992). Those findings are in accordance with another study that found 40%
of the diagnosed canine squamous cell carcinomas in Standard and Giant Schnauzers (Kessler
2012). Interestingly the Miniature Schnauzer is not over-represented. More than 95% of the SCCs in
the Schnauzers were furthermore located at the digits.
Besides increased prevalence of digital SCCs in Standard Poodles, Rottweilers and Giant
Schnauzers, also Beaucerons (Belluco et al. 2013), Briards (Henry et al. 2005, Belluco et al. 2013)
and Labrador Retrievers (Henry et al. 2005, O`Brien et al. 1992) were described to be more frequently
affected. Although being a small breed the Dachshund was over-represented in one study as well. In
the latter study, five out of six amputated toes were diagnosed with a SCC (Wobeser et al. 2007).
There is an ongoing research of the National Genome Research Institute investigating the genetic
susceptibility to digital SCCs of some of the breeds mentioned above (Davis and Ostrander 2014).
3.4.3. Location
The toes of the front legs are more frequently concerned with SCCs compared to the hind legs
(Wobeser et al. 2007, Henry et al. 2005, Belluco et al. 2013). There is no significant difference
regarding the prevalence between the right and left forelimb (Belluco et al. 2013). The digits are also
affected equally, except the dew claw being affected less frequently (6.9% of the digits; Wobeser et al.
2007). Furthermore Marino et al. (1995) recorded that most digital SCCs arise from the subungual
epithelium (66%).
3.4.4. Age and sex
SCC is primarily a disease of the geriatric dog, but can be found in dogs as young as 3 years of age.
Different authors describe similar outcomes regarding the mean age of the dogs with digital tumors.
The age range of affected dogs is nevertheless very wide. Wobeser et al. (2007) describe the

12
amputation of digits with SCCs in dogs ranging from 3 up to 17years of age, with a mean age of 9.8
years. Henry et al. (2005) detected a range between 3 and 16 years and a mean age of 9.7 years and
Belluco et al. (2013) described a mean age of 10.2 with a range between 4 and 16 years.
The mean age of inflammatory digital lesions is lower. Wobeser et al. (2007) describe a mean age of
7.1 years and an age distribution from 1 to 14 years.
Malignant melanomas had a similar age distribution as SCCs, ranging from 5 to 13 years (mean age
9.3years). Dogs with benign digitals tumors ranged from 4 to 11 years of age (mean age 7.8years)
and dogs with osteosarcomas were between 8 and 14 years with a mean age of 9.7 years (Henry et
al. 2005).
Kessler (2012) found 77% of the dogs with SCCs to be male or male castrated. Henry et al. (2005)
and Belluco et al. (2013) found no sex predisposition.
3.5 PATHOGENESIS
3.5.1. Hereditary factors
Just like the etiology, the pathogenesis is also not completely resolved yet. Some theories suspect a
link between digging behavior and thereby more exposure to carcinogenic substances of the front
legs. Additionally, the front legs bear more weight than the hind legs and are thus subject to more
stress. The same reasoning can be used to explain why more large breeds are affected (Wobeser et
al. 2007). Accordingly, the Standard and Giant Schnauzer seem to be predisposed, whereas the
Miniature Schnauzer is not (Kessler 2012). Considering the breed predisposition, the size of the
breeds, location of the tumor, and the multicentric nature of the canine digital squamous cell
carcinomas a genetic predisposition related to pigmentation in combination with repeated micro-
traumata might play an essential role in the pathogenesis. A theory describes repeated micro-
traumata to the digital epithelial cells as a potential cause for genetic modifications resulting in a
neoplastic phenotype (Belluco et al. 2013).
3.5 2. UV-exposure
In humans exposure to UV-radiation is the major risk factor for establishing skin cancer. Additionally,
burns, chemicals and x-ray radiation are considered potential threats and humans with lighter skin and
less pigmentation seem predisposed. Contrary, in digital SCCs pigmentation appears to be a risk
factor and sun exposure does not seem to play a role in the pathogenesis (Belluco et al. 2013).
3.5.3 EMT
Epithelial-mesenchymal transition (EMT) describes a process where epithelial cells lose their typical
characteristics and acquire a mesenchymal phenotype. It occurs during embryogenesis, in wound
healing and in carcinogenesis.

13
Epithelial cells and mesenchymal cells express different marker proteins. Epithelial cells express high
levels of E-cadherin, which is an adhesion glycoprotein whereas N-cadherin, fibronectin and vimentin
are specific for mesenchymal cells. Those markers can be used to determine the transition. During
carcinogenesis epithelial cells lose the expression of epithelial markers such as E-cadherin and start
expressing mesenchymal markers such as vimentin or N-cadherin. This finding can be used to identify
a malignant phenotype. In a study regarding SCCs the percentage of tumor cells that are positive for
vimentin and E-cadherin were evaluated. In some SCCs the researchers detected mesenchymal
phenotypes, which were linked to the differentiation degree of the tumor cells. The less differentiated
the tumor, the higher the percentage of vimentin positive and E-cadherin negative results (Belluco et
al. 2013).
3.5.4 Papilloma virus
Also viral etiologies have been linked to certain SCCs. The link between previous papilloma virus
infection and subsequent development of subungual squamous cell carcinomas requires further
investigation (Goldschmidt and Shofer 2005, Zaugg et al. 2005). Papillomavirus DNA has been
detected in in around 20% of canine and feline cutaneous and mucosal SCCs, the significance of this
outcome is however unknown (Zaugg et al. 2005).
3.5 5. Genetic Predisposition
Dark-coated Standard Poodles are at high risk of developing digital squamous cell carcinomas,
whereas light colored Standard Poodles are almost entirely unaffected. This suggests that multiple
pathways are involved in the oncogenesis. The Genome-wide association study (GWAS), identified
the KIT Ligand (KITLG) locus to be strongly associated with digital SCCs in Standard Poodles.
Interestingly, light and dark-colored Standard Poodles carry the putative causal variant of the allele at
the same frequency but light-colored Standard Poodles are protected from SCCs (Karyadi et al. 2013).
This is most likely due to a compensatory mutation in the coat color locus MC1R (Davis and Ostrander
2014). Sequencing revealed that all affected dogs, regardless of breed, carry the same founder
mutation that affects the expression of KITLG (Karyadi et al. 2013).
3.5 .6 Cyclooxygenase
Cyclooxygenases (COX) are enzymes that are essential for, among others the prostaglandin
syntheses. There are two isoenzymes called COX-1 and COX-2. Research showed that COX-2 was
strongly expressed by neoplastic keratinocytes in canine squamous cell carcinomas, but not detected
in normal skin. Immunoblotting revealed staining of COX-1 in normal skin and SCCs to only a limited
extent. Those findings suggest that SCCs induce COX-2 gene expression. Further research is
necessary to investigate the role and regulation of COX-2 gene expression in naturally occurring
squamous cell carcinomas (De Almeida et al. 2001). Similar findings were gathered by Mohammed et
al. (2004). The team found that COX-2 was strongly expressed in epithelial tumors (17 of 26 SCCs)
but was absent in normal tissues and minimal or absent in mesenchymal tumors. This implies new

14
treatment approaches using COX- inhibitors and selective COX-2 inhibitors such as piroxicam in
antitumor therapy.
3.6. CLINICAL SIGNS
Digital tumors and digital inflammatory processes both show similar symptoms. The most frequent
signs of digital tumors comprise digital masses (73%), limping (42%) or both (26.5%). Also ulcerations
(28%) and breaking toenails (12.5%) were frequently seen. The period between noticing clinical signs
and presentation to a veterinarian was in average 2 weeks. The range however goes from 1 week up
to 3 years (Henry et al. 2005). Digital tumors cause swelling of the toe and frequently look harmless at
first sight. Often the tumor is initially misdiagnosed as an inflammatory or traumatic lesion, and
therapies such as antibiotics and corticosteroids may have been used before diagnosis. If the nail is
affected it is usually cracked, deviated, elongated, hollow or missing all together. Bleeding, discharge
and ulceration are also common complaints (Kessler 2012).
Mostly one toe at a time is involved; however, multiple digits are regularly affected over a period of
time. At initial diagnosis Wobeser and colleagues (2007) recorded that 6.4% of the patients had
developed SCCs on multiple digits, Henry et al. (2005) found 9% and Belluco et al. (2013) 8.4%. In the
latter study 22.4% of the patients developed new tumors on other digits over a varying period of time,
ranging from 1 month to 2 years. Similar results were gained by Kessler (2012) where 20% of the
patients with SCCs developed multiple digital tumors simultaneously or over a course of time on
different toes. It is important to mention that those are separate primary tumors and no metastases
from the initial one. Also different types of digital tumors can be present simultaneously (Kessel 2013).
All of the dogs that developed SCCs on multiple digits were large breeds with a black coat (Belluco et
al. 2013).
The tumor cells can travel to the lymphatic system and enlargement of the draining lymph nodes can
be a sign of spreading (Webb et al. 2009, Marino et al. 1995). If the tumor spreads to the lungs clinical
signs include dyspnea, coughing, weight loss, (partial) anorexia and malaise (Degner 2004).
3.7. METASTASES AND RECURRENCE
Different authors describe diverging outcomes regarding metastatic rates of digital SCCs. Metastases
are found in the regional lymph nodes and in the lung, occasionally also at other places. A case of a
dog was described with histologically confirmed metastases to the tongue (Henry et al. 2005).
Metastases in general were recorded in 24% of the patients at the time of presentation (Wobeser et al.
2007). Pulmonary metastases were detected by radiography in 13% of the patients before surgery and
17% of the dogs developed pulmonary metastases after surgery according to Marino and colleagues
(1995). O`Brien and colleagues (1992) found post-surgical pulmonary metastases in only 5% of the

15
patients though. In the study of Henry et al. (2005) only one of 33 patients (5%) with SCCs had
pulmonary metastases at the time of presentation and Frese et al. (1983) describe distant metastases
in 2.7% of the dogs. Summarizing, at the time of presentation pulmonary metastases were detected in
2.7- 13% of the presented patients.
Frese and colleagues (1983) recorded 21.6% metastases in the lymph nodes after digit amputation
and 30% of the patients died within a year because of local recurrence and/or metastases. In contrast,
Henry et al. (2005) recorded only one out of 33 patients (5%) with metastases in the regional lymph
nodes. The average time for metastases to develop was 309 days (Wobeser et al. 2007).
The study by Wobeser et al. (2007) additionally implies that digital SCCs might have a higher
metastatic potential than SCCs on other parts of the body.
More aggressive tumors can involve the articular cartilage or alternatively the bone at the periphery of
the articular surface. The neoplastic cells can invade the joint space and spread along the bursae of
the flexor and extensor tendons. Consequently tumor recurrence can occur within the subcutaneous
tissue of the amputation site (Goldschmidt and Hendrick 2008).
3.8 DIAGNOSTICS & DIAGNOSIS
3.8.1. Introduction
Squamous cell tumors can resemble different diseases such as paronychia, nail problems, hair follicle
inclusion cysts or other neoplasms. SCCs may be suspected based on the gross appearance of a
lesion, the anamnesis and its location, but definitive diagnosis requires microscopic examination of the
affected tissue. A thorough medical work-up is necessary and contains preferably several of the steps
mentioned below. Diagnostics should always start with a thorough physical examination to make a
presumptive diagnose and examine the overall condition of the patient. Attention should particularly be
paid to the regional lymph nodes. If the forelimbs are affected the axillary and prescapular lymph
nodes are most likely to be enlarged, if the hind limbs show lesions attention should be paid especially
to the popliteal and inguinal lymph nodes (O`Brien et al. 1992). A complete blood count, chemistry
profile and urine testing might be required to evaluate the health status and anesthesia suitability prior
to and in case of surgery (Webb et al. 2009).
3.8.2. Medical imaging
Radiographs of the abnormal toes generally help to further differentiate the lesions. Squamous cell
carcinomas are usually aggressive, invasive and destructive. In an advanced state osteolysis of the
third phalanx can be seen, sometimes also of the second phalanx (Kessler 2012). However,
radiographs alone are not sufficient for a conclusive diagnosis. When examining 124 digital masses
21.8% showed osteolysis of the affected phalanges (Marino et al. 1995). Bone lysis can be present in
malignant neoplasms, benign neoplasms, non-neoplastic non-inflammatory disease and inflammatory
disease (Wobeser et al. 2007, Marino et al. 1995). In a study by Henry et al. (2005) the majority (71%)

16
of the examined digital tumors showed radiographic signs of bone invasion. Among those, 79% of the
SCCs caused osteolytic signs as did 40% of the malignant melanomas, 75% of the osteosarcomas
(n=3) and one dog with an epidermal inclusion cyst (Henry et al. 2005). Absence of bone lysis thus
does not allow the exclusion of SCCs from the list of differentials.
Besides osteolysis, soft tissue swelling and osteopenia are also common signs. Osteopenia describes
a process of diminished bone density and includes osteoporosis, osteomalacia and osteolysis.
Osteolysis is defined as an increased rate of bone resorption by osteoclasts. This sign is generally
considered to be a focal loss of bone in direct response to a pathologic process such as infection,
neoplasm or other focal processes. Those developments are initiated by osteoclast-activating factors
excreted by cancer cells (Bonakdarpour et al. 2009).
Additionally thoracic radiographs are used to help rule out the spread of cancer to the lungs and lymph
nodes. To increase the sensitivity, radiographs should always be taken in three views, namely left and
right lateral and a ventro-dorsal view (Ober and Barber 2006). A CT-scan has an even higher
sensitivity in detecting pulmonary metastases (Davis 1991), but is also more cost-intensive.
Abdominal ultrasound might be performed to rule out spread of tumor to the internal organs (Webb et
al. 2009) as well as to check on the sublumbar lymph nodes if the hind limbs are affected (O`Brien et
al. 1992).
3.8.3. Cytology and Histopathology
Cytology
Cytology is a rapid, easy and noninvasive technique that is frequently used as the first diagnostic
method but is often non-diagnostic (Webb et al. 2009, Medleau and Hnilica 2006). There are several
methods to collect cells. The most suitable one depends on the location and gross appearance of the
lesions. Fine needle aspiration is most suitable for nodular lesions, whereas scrapings or surface
imprints are used to collect cells from superficial lesions. Accompanying inflammation often impedes a
cytological diagnosis. Since many SCCs are inflamed and ulcerated superficial sampling may retrieve
only the inflammatory cells and miss the underlying neoplastic cells. Inflammatory processes can thus
mask neoplasms but contrary also induce epithelial hyperplasia causing dysplastic changes that
imitate neoplasia (Webb et al. 2009).
It is also recommended to take a fine needle aspiration of regional lymph nodes, regardless of whether
they are enlarged or not.
Neoplasia is generally characterized by a monomorphic cell population and absent inflammation.
Additional classification in malignant and benign is based on cytomorphologic features. Tumors of the
epithelia likewise have specific characteristics. They exfoliate easily and the collected cells are
organized in adherent clusters (Raskin and Meyer 2001). The cells are subsequently stained and

17
evaluated under the microscope (Webb et al. 2009). Epithelial cells are typically large and round to
polygonal with distinct cellborders, with round to oval nuclei.
Neoplastic cells lose their specific characteristics and develop cytological features of malignancy.
Typical for SCCs are large, fully keratinized cells that retain large nuclei. Other criteria of malignancy
that can be found in SCCs include anisokaryosis, macrokaryosis, pleomorphism of cell size, nuclear
molding, a high cytoplasmic-nuclear ratio, enlarged, multiple or variably shaped nucleoli, multi-
nucleation, an elevated mitotic index, abnormal mitotic figures and a coarse or blotchy chromatin
pattern. Nuclear fragmentation, budding and emperipolesis might also be observed. Emperipolesis
defines the presence of an intact cell within the cytoplasm of another cell (Raskin and Meyer 2001).
Keratohyaline granules can sometimes be seen as small, round, cytoplasmic vacuoles situated around
the nucleus (Webb et al. 2009).
Histopathology
In case of an equivocal diagnosis or severe inflammation histopathologic examination is necessary
(Raskin and Meyer 2001). It can be carried out on a partial biopsy or excisional biopsy, depending on
tumor size and location. If not excisional, the biopsy should always contain the transition from grossly
normal to abnormal epithelium (Webb et al. 2009). In digital SCCs the toe is normally amputated and
histopathological examination should always be conducted.
Canine digital squamous cell carcinomas are histologically similar to SCCs in other parts of the body
(Meleo 1997). They originate in the nail-bed or plantar epithelium and are histologically highly
differentiated carcinomas that tend to keratinize (Kessler 2012).
Histological examination includes several criteria such as the differentiation degree, mitotic index,
presence of emboli and immunohistochemical expression of vimentin and E-cadherin (Belluco et al.
2013).
In a study the histopathologically examined tumors were situated in the superficial, mid and deep
dermis. The nail bed was involved in some samples and the tumors often invaded the adjacent bone.
Neoplastic cells can infiltrate and spread through the lamina basale of the nailbed epithelium to invade
the medullary and cortical bone of the phalanges. This process is often accompanied by fibroplasia
and infiltration by neutrophils, plasma cells and lymphocytes (Goldschmidt and Hendrick 2008,
Medleau and Hnilica 2006).
The tumors presented were multilobular, not encapsulated and moderately cellular. In most tumors
multiple stages of differentiation were present at the same time, ranging from well-differentiated to
poorly-differentiated. The well-differentiated parts possessed a squamous cell differentiation; the cells
were arranged in a lobular pattern with copious amounts of keratin in the center (Belluco et al. 2013).
The epithelial cells still mature from basal layer to stratum corneum, but instead of growing toward the
skin surface they are arranged in clusters, surrounded by stroma with the keratin-producing cells in the
center. This arrangement creates the typical appearance of so called keratin pearls, which can be
seen as central keratinization within concentric layers of abnormal squamous cells (Webb et al. 2009).

18
In less differentiated tumors, epithelial layering is indistinct, cells and lobes were smaller with less
keratin in the center. Highly anaplastic SCCs may require special histochemical staining for a
conclusive identification of the origin of the cells (Webb et al. 2009, Belluco et al. 1995).
In the poorly differentiated zones cells were even smaller with amphophilic cytoplasm, arranged in
cords or isolated and without signs of keratin or dyskeratosis. The stroma in the inspected tumors was
infiltrated by lymphocytes and plasma cells. When keratin-containing lobules rupture, the keratin can
cause a pyogranulomatous reaction.
Belluco et al. (2013) examined the mean tumor proportions. The studied tumors predominantly
consisted of well-differentiated tissue with 61.2%; 27% of the tumors was moderately and 11.8%
poorly differentiated. The histological differentiation is also important for the tumor grading system.
In a few cases the author also detected neoplastic emboli in the adjacent lymphatic vessels and in one
case in the capsular sinus of a lymph node. The emboli showed diverging morphological features.
They could be small or large, contained few or up to 50 cohesive cells with severe anisocytosis and
anisokaryosis, they were differentiated or anaplastic. Dyskeratosis can be present in the emboli as
well (Belluco et al. 2013).
3.9 THERAPIES
3.9.1. Introduction
For a digital squamous cell carcinoma amputation of the affected phalanges is mandatory to prevent
the tumor from spreading to adjacent lymph nodes and major organs. Adjuvant therapy is used
infrequently. Chemotherapy can be used in patients with metastases but little information is available
regarding expected remission rate or mean survival time (MST). Inoperable local recurrent SCCs
might be treated with radiotherapy (Kessler 2012).
3.9.2. Amputation
Amputation of the neoplastic toes is generally the treatment of choice. Depending on the lesions and
osteolytic processes the toe can be amputated at different levels, to be precise at the
metacarpophalangeal, metatarsophalangeal or proximal interphalangeal joints. Usually adjuvant
therapy is not required in SCCs (O`Brien et al. 1992). In metastatic disease excision, limb amputation
and/or adjuvant chemotherapy is however recommended (O`Brien et al. 1992).
In a study by Kaufman and Mann (2013) the short- and long-term outcomes after digital amputation
have been investigated in 33 dogs. Digit 3 and 4 are the primary weight-bearing toes and might thus
cause more functional problems after amputation compared to digit 1, 2 or 5. Short-term complications
besides lameness were noticed in 39.4% of the dogs post-surgery. The complications included
(partial) wound-dehiscence with or without infection, soft-tissue inflammation and swelling,
serosanguinous, serous or mucoid discharge of the incision-site and delayed healing. The most
frequent complication was dehiscence at the surgical site. On the front legs dogs developed
significantly more short-term complications after digit amputations compared to the hind legs. In this

19
study there was no link between short-term complications and other variables including bodyweight,
amputated digit, breed, diagnosis or at which level the amputation was carried out.
Twenty-five percent of the patients, where follow-up information was available, developed long-term
complications, the main problem was lameness. Here again there was no link between long-term
complications and the weight of the dogs, front or hind leg, amputated digit or the level of amputation.
Concluding, most dogs appear to tolerate digit amputation quite well. Liptak et al. (2005) furthermore
reported no functional impairment and a good tumor control when amputating both central weight
bearing digits.
Other studies however accredited negative prognostic effects to amputation of digits 3 and 4,
amputation of two adjacent digits, amputation of digits at the level of the joint and failure to remove the
associated sesamoid bones (Probst and Mills 2003, Muir and Pead 1998, Liptak et al. 2005).
Post-surgery analgesics should be administered for pain relief and exercise should be limited for 3
weeks. For at least 1 week a bandage should be placed to protect the wound. The wound should be
checked regularly for signs of infection or complications, such as wound dehiscence (Degner 2004).
3.9.3. Chemotherapy
Although SCCs are generally not known to respond well to chemo-therapy it may, however, be
considered for tumors that are inoperable, anaplastic or in case of lymph node involvement (Brooks et
al 1988, O`Brien et al. 1992). Single-agent or combination therapy protocols containing cisplatin,
carboplatin, cyclophosphamide, doxorubicin, and 5-fluorouracil have been described (Brooks et al.
1988). Henry et al. (2005) for example describe in their study two different protocols. Two dogs with
SCCs were treated with a single dose of cisplatin (60mg/m2 IV) and two were treated with respectively
one and four doses of mitoxantrone (5mg/m2 q21d). The outcome was not mentioned. Another author
described the successful use of cisplatin to treat two dogs with metastatic squamous cell carcinomas.
One dog had a complete remission whereas the other dog had a partial remission of the tumor, but
relapsed and was euthanized 4.5 months after the beginning of treatment. Both dogs tolerated the
treatment well (Himsel et al. 1986).
As mentioned earlier, SCCs induce the expression of the COX-2 gen. Piroxicam is a non-steroidal
anti-inflammatory drug, inhibiting COX-enzymes and has known anti-tumor properties. In a clinical trial
the maximum tolerated dose was 1 mg/kg q48h, before unacceptable gastro-intestinal side-effects and
renal papillary necrosis occurred. No complete remission was achieved, but partial remission was
documented in different tumor types including three of five dogs exhibiting squamous-cell carcinomas
(Knapp et al. 1992). Another trial evaluating piroxicam for the treatment of oral SCCs in dogs resulted
in one complete remission of a maxillary tumor, two partial remissions (lingual tumor and tonsillar
tumor) and five dogs with stable disease treatment. The used dosage was 0.3 mg/kg PO q24h. The
results suggest that piroxicam may be useful in the treatment of dogs with oral squamous cell
carcinoma (Schmidt et al. 2001). Another clinical trial evaluated cisplatin in combination with piroxicam
for the treatment of oral SCCs and malignant melanomas. The maximum tolerated dose of cisplatin
when administered together with piroxicam was 50 mg/m2. Tumor remission occurred in five of the

20
nine dogs with oral SCCs and piroxicam had no significant effects on the pharmacokinetics of
cisplatin. The most common side-effect observed was renal toxicosis (Boria et al. 2004). For
superficial solar-induced and pre-neoplastic skin lesions, retinoids (etretinate) have been used (Marks
et al. 1992)
The role of chemotherapy has not really been established yet in the management of canine SCC and
is currently not scientifically confirmed. To the authors knowledge there are no universal
chemotherapy treatment protocols described in the veterinary literature that are specifically adapted to
canine digital squamous cell carcinomas. Some of the drugs mentioned above show however
promising results.
3.9.4. Radiation therapy
Radiation therapy is not regularly used in the treatment of digital SCCs but can be used as an
adjuvant when it is impossible to obtain tumor-free surgical margins or in case of inoperable tumors
(Webb et al. 2009). It has been shown to prevent or delay the onset of tumor regrowth (Goldschmidt
and Shofer 2005, O`Brien et al. 1992). A possible protocol includes radiation on a Monday-
Wednesday-Fridays basis with either a Cobalt-60 unit or a linear accelerator. The total doses ranged
from 42 to 55.8 Gy (Henry et al. 2005). Radiation is nevertheless carcinogenic and can thus induce
neoplasia. Therefore the primary goals are to support pain relief, stabilize tumor growth and decrease
dysfunction caused by the tumor (Webb et al. 2009).
3.10 PROGNOSIS
Patients with well-differentiated tumors that can be completely excised and that have no evidence of
metastatic disease have a fair prognosis (North and Banks 2009, Webb et al. 2009).
According to different studies 60-95% of the patients survive for more than one year and 43-74% for
more than two years (O`Brien et al. 1992, Marino et al. 1995, Foale and Demetriou 2010, Kessler
2012).
Digital SCCs originate in the nail-bed or plantar epithelium. Marino et al. (1995) found that the majority
(66%) of the digital SCCs arose from the subungual epithelium and of those patients 95% survived 1
year and 74% more than 2 years. SCCs originating from other parts of the digit appeared to have
higher rates of metastatic disease and a worse prognosis (Foale and Demetriou 2010). Only 60%
were still alive after 1 year, and only 44% were still alive after 2 years. Belluco et al. (2013) additionally
might have found hints that subungual SCCs have a smaller risk of emboli and metastasis compared
to other digital regions. However, in the latter study only 14 cases with nailbed involvement were
represented.
Furthermore, metastatic disease from digital tumors at time of diagnosis has no negative impact on
survival; however it did have an impact on likelihood of local tumor recurrence. So if metastases are
present, treatment is still a valuable option but one has to keep in mind that recurrence is more likely.
Also early detection and surgical intervention are important for a favorable prognosis. Concluding,
early surgical intervention regardless of present metastases should be considered (Henry et al. 2005).

21
4. DISCUSSION
The patient was initially presented with a digital mass on the fifth toe of the left front limb. The third
toes of both forelimbs were previously amputated due to a tentative diagnosis of squamous cell
carcinoma. When an additional third toe showed ulcerative lesions the owners came to the veterinary
teaching hospital for a second opinion on how to proceed best. No histopathological examination of
the previously amputated toes was performed.
At the teaching hospital the toes and the dog were thoroughly examined by the attending veterinarian
and a tentative diagnosis of SCC was confirmed. Cytology was performed on the digital mass, but not
on the enlarged left prescapular lymph node. The collected cells suggested a malignant tumor and
medical imaging reinforced the assumption of a malignant, invasive and destructive process. The
documented osteolysis of the phalanges is however unspecific and not exclusively seen in SCCs. It
was detected in malignant processes (SCC, melanoma, osteosarcoma, adenocarcinoma and others),
benign processes (epidermal inclusion cysts, keratoacanthoma) and inflammatory processes
(Wobeser et al. 2007). As mentioned before, the clinical presentation of neoplastic and inflammatory
disease of the toes is very similar, which makes a definitive diagnosis without histopathologic
examination impossible. The age can give a hint as well, since neoplastic processes are more
common in older dogs of around nine years of age, but the age-ranges reported in the literature were
broad and overlapping.
Based on the radiographs the radiologists recommended the amputation of at least the fifth digit of the
left forelimb, although digit two and four were also affected, and of digit one and four of the right
forelimb. The surgeons eventually amputated digit two and five of the left forelimb (digit four remained)
and digit one and four of the right forelimb. Digit four of the left forelimb showed radiological signs of
osteolysis but was not amputated to avoid functional impairment, since digit one is not weight-bearing
and would have been the only remaining digit after amputation.
Summarizing, the presented Giant Schnauzer still has the first and fourth digit of the left forelimb and
the second and fifth digit of the right forelimb after surgery. To limit the costs the owner decided
against the standard procedure of the teaching hospital to perform histopathology on the amputated
digits. Unfortunately that also means that a definitive diagnosis of digital SCC cannot be made and it
also remains uncertain if the margins of the resection site are free of tumor cells. To the knowledge of
the author there was also no bloodwork conducted prior to surgery. The dog was almost eleven years
of age, to get an impression of his overall health and reassure anesthesia suitability, a bloodwork
including a hematology and biochemistry profile is strongly recommended. Also a FNA of the lymph
node would have been interesting to differentiate between reactive or metastatic lymph node
enlargement.
The presented patient is a prime example of digital squamous cell carcinomas in dogs. He is a large
dog with a black coat that belongs to one of the predisposed breeds and the toes of the forelimbs are
affected. The mean age described in the veterinary literature was between 9.7 and 10.2 years, our

22
patient was nine years old when the first toe was amputated. Over a period of time he furthermore
developed multicentric tumors on different digits and additionally he showed typical signs including
regional lymph node enlargement, a missing nail, swollen toes and an ulcerated mass. The dog also
displayed radiological signs of osteolysis of the affected digits. According to the owner none of his
siblings or ancestors suffered from the same disease though.
Several breeds were mentioned to be predisposed. It was remarkable however that the described
predisposed breeds alternated according to the country where the research was conducted.
Depending on the country and the popularity of certain breeds the prevalence shifted. For example, in
a study conducted in France Briards and Beaucerons were represented more frequently, but not in
studies conducted in other countries (Belluco et al. 2013).
Literature describes all digits, except the dew claw, to be equally affected. It is not mentioned if that
was due to dew claw removal as puppy’s or because those claws bear less weight, have less contact
with potential carcinogens and are less prone to trauma. As mentioned earlier a hypothesis states that
the increased susceptibility of the front legs is due to more contact with potential carcinogens, more
trauma and more weight-bearing stress compared to the hind limbs. All digits are however equally
affected although the third and fourth digits carry most of the weight. According to this theory the third
and fourth toe should have a higher risk of developing digital SCCs.
The treatment of choice is amputation of the affected digits with subsequent histopathological
examination and evaluation of the margins. Adjuvant radiation and chemotherapy is only used
occasionally in metastatic disease or when the tumor cannot be excised completely. There is quite
some research conducted concerning oral squamous cell carcinomas in cats and dogs, but little can
be found about the digital variant. It is not apparent in how far those results can be extrapolated. Some
protocols have been described including some promising new approaches including piroxicam. No
uniform or effective protocols however have been established yet. Since the reported patient exhibited
unilateral lymph node enlargement, chemotherapy could have been an option worth considering.
There is also ongoing genetic research that already located the presumptive causative genetic locus.
This might also be a starting point for future therapies or prophylaxis (e.g. breeding programs).
Goldschmidt and Hendrick (2008) describe infiltration of tumor tissue in the joint space between
phalanx three and two and a possible extension of tumor cells along the bursae of the digital flexor
and extensor tendons. Consequently recurrence of the tumor may develop within the subcutaneous
tissue at the amputation site. The patient suffered from multicentric tumors, no histopathologic
examination was conducted to confirm tumor free margins, the enlarged lymph node was not further
examined and some of the affected toes were not amputated. On radiological examination no thoracic
metastases were detected, but the sensitivity of radiographs is limited. A CT-scan would have had a
higher sensitivity in detecting pulmonary metastases (Davis 1991). A study reported that the threshold
to reliably detect pulmonary nodules on thoracic radiographs is 7-9mm, compared to 1mm to detect
pulmonary metastases on CT-scans (Nemanic et al. 2008). Moreover, the owners were to decide if
they want to preventively amputate all toes of the front limbs or only the most affected ones and
chose the latter. Although the prevalence is slightly less also the toes of the hind limbs can be

23
affected. Six months after the latest amputation the patient shows no visible signs of recurrence or
metastatic disease according to the owner. Considering all those facts mentioned above the patient
has an increased risk to develop recurrence or metastatic disease and should be monitored closely.
Considerable research is done especially concerning the prevalence of digital SCCs. Adjuvant
chemotherapy has been reported seldom and non-uniform. The protocols varied and treatment
outcome was not described, analyzed or examined, making it impossible to draw conclusions. Future
research should focus on the etiology and hereditary factors, as well as on the various adjuvant
treatment options, including promising new approaches such as piroxicam.
Concluding, digital SCCs are a common and important disease in the Giant Schnauzer that should be
taken seriously since early surgical intervention regardless of present metastases implies a better
outcome. Increased surveillance for digital masses should become part of routine examinations,
especially in large dog breeds with black coats.

1
References
1. Belluco S, Brisebard E, Watrelot D et al. (2013) Digital Squamous cell carcinomas in dogs:
Epidemiological, Histological and Immunohistochemical study. Veterinary Pathology. 50:
1078-1082
2. Bonakdarpour A, Reinus WR and Khurana JS. (2009) Diagnostic Imaging of
Musculoskeletal Diseases: A systematic approach. 1st edition. Humana Press, New York.
Pp: 17-19
3. Boria PA, Murry DJ, Bennet PF et al. (2004) Evaluation of cisplatin combined with
piroxicam for the treatment of oral malignant melanoma and oral squamous cell carcinoma
in dogs. Journal of the American Veterinary Medical Association. 224: 388-394
4. Brooks MB, Matus RE, Leifer CE et al. (1988) Chemotherapy versus chemotherapy plus
radiotherapy in the treatment of tonsillar squamous cell carcinoma in the dog. Journal of
veterinary internal medicine. 2:206-211.
5. Byers JC and Fleischman RW (1984) A case report: Canine Digital Neoplasia. Canine
practice. 1: 25-33
6. Davis BW and Ostrander EA (2014) Domestic dogs and cancer research: A Breed-based
genomic approach. Institute for Laboratory Animal Research (ILAR). 55: 59-68
7. Davis SD (1991) CT evaluation for pulmonary metastases in patients with extrathoracic
malignancy. Radiology.180: 1-12
8. De Almeida EMP, Piche C, Sirois J et al. (2001) Expression of cyclo-oxygenase-2 in
naturally occurring squamous cell carcinomas in dogs. Journal of Histochemistry and
Cytochemistry. 49:867-876
9. Degner DA (2004). Digital tumors. Available:
http://www.vetsurgerycentral.com/oncology_digital_tumors.htm. Consulted: 2.April 2016
10. Dobson JM and BDX Lascelles (2003) BSAVA Manual of Canine and Feline Oncology.
Chapter 14: Epithelial and other solitary skin tumors. 2nd
edition. BSAVA, Gloucester. Pp:
156- 158
11. Foale R and Demetriou J (2010) Saunders Solutions in Veterinary Practice: Small Animal
Oncology. 1st
edition. Saunders Elsevier, St Louis. Pp: 148-150
12. Frese K, Frank H and Eskens U (1983): Plattenepithelkarzinome der Zehen beim Hund.
Deutsche tierärztliche Wochenschrift . 90: 359-363
13. Goldschmidt MH and Hendrick MJ (2008) Tumors in Domestic Animals: Tumors of the
Skin and Soft Tissues. 4th
edition. Iowa State University Press, Ames Iowa. Pp. 45–119.
14. Goldschmidt MH and Shofer FS (2005) Subungual Squamous Cell Carcinoma. OncoLink
Vet.
Available:http://oncolink.org/types/article.cfm?c=0&s=69&ss=807&id=9527 Consulted: 2nd
April 2016
15. Hargis AM, Thomassen RW and Phemister Rd (1977) Chronic dermatosis and cutaneous
squamous cell carcinoma in the beagle dog. Veterinary Pathology. 14: 218-228

2
16. Henry CJ, Brewer Jr WG, Whitley EM et al. (2005) Canine digital tumors: A veterinary
Cooperative Oncology Group Retrospective study of 64 dogs. Journal of veterinary
internal medicine. 19: 720-724
17. Himsel CA, Richardson RC and Craig JA. (1986) Cisplatin chemotherapy for
metastatic squamous cell carcinoma in two dogs. Journal of the American Veterinary
Medical Association. 189:1575-8
18. Karyadi DM, Karlins E, Decker B et al. (2013) A copy number variant at the KITLG locus
likely confers risk for canine squamous cell carcinoma of the digit. PLoS Genetics. 9:
e1003409
19. Kaufman KL and Mann FA (2013) Short- and long-term outcomes after digit amputation in
dogs: 33 cases (1999-2011). Journal of the American Veterinary Medical Association.
242: 1249-1254
20. Kessler M (2012) Kleintieronkologie. Diagnose und Therapie von Tumorerkrankungen bei
Hund und Katze. 3rd
Edition. Enke Verlag, Stuttgart. Pp: 428-429
21. Knapp DW, Richardson RC, Bottoms GD et al. (1992) Phase I trial of piroxicam in 62 dogs
bearing naturally occurring tumors. Cancer Chemotherapy Pharmacology. 29:214-218
22. Liptak JM, Dernell WS, Rizzo SA et al. (2005) Partial foot amputation in 11 dogs. Journal
of the American Animal Hospital Association. 41: 47-55
23. Liu SK, Dorfman HD and Patnaik AK (1977) Primary and secondary bone tumours in the
dog. Journal of small animal practice. 18: 313-326
24. Marino DJ, Mathiesen DT, Stefanacci JD et al. (1995)Evaluation of dogs with digit
masses: 117 cases (1981-1991) Journal of the American Veterinary Medical Association.
207: 726-728
25. Marks SL, Song MD, Stannard AA et al. (1992) Clinical evaluation of etretinate for the
treatment of canine solar-induced squamous cell carcinoma and pre-neoplastic lesions.
Journal of the American Academy of Dermatology. 27: 11-16
26. Medleau L and Hnilica KA (2006) Small animal dermatology. A color atlas and therapeutic
guide. 2nd
edition .Saunders Elsevier, Philadelphia. Pp. 369
27. Meleo KA (1997) Tumors of the skin and associated structures. Veterinary Clinics of North
America: Small Animal Practice. 27: 73-94 (only abstract)
28. Mohammed SI, Khan KN, Sellers RS et al. (2004) Expression of cyclooxygenase-1 and 2
in naturally-occurring canine cancer. Prostaglandins, Leukotrienes and Essential Fatty
Acids. 70:479-483
29. Muir P and Pead MJ (1998) Chronic lameness after digit amputation in three dogs.
Veterinary record. 143: 449-450
30. Nemanic S, London CA and Wisner ER (2008) Comparison of thoracic radiographs and
single-breath-hold helical CT for detection of pulmonary nodules in dogs with metastatic
neoplasia. Journal of veterinary internal medicine. 20: 508-515
31. North S and Banks T (2009) Small animal oncology: An introduction. Chapter 18: Tumours
of skin and subcutaneous tissues. 1st
edition. Saunders Elsevier, London. Pp: 173-175

3
32. Ober CP and Barber D (2006) Comparison of two- vs. three-view thoracic radiographic
studies on conspicuity of structured interstitial patterns in dogs. Veterinary Radiology and
Ultrasound. 47: 542-545
33. O`Brien MG, Berg J and Engler SJ (1992) Treatment by digital amputation of subungual
squamous cell carcinoma in dogs: 21 cases (1987-1988). Journal of the American
Veterinary Medical Association. 201: 759-761
34. O`Rourke M (1985) Multiple digital squamous cell carcinomas in 2 dogs. Modern
Veterinary practice. 66:644–645
35. Paradis M, Scott DW and Breton L (1989) Squamous cell carcinoma of the nailbed in
three related Giant Schnauzers. Veterinary record. 125: 322-324
36. Probst CW and Mills DI (2003) Carpus and digits. In: Slatter DH Textbook of small animal
surgery. 3rd
edition. Saunders Elsevier, Philadelphia. Pp:1987
37. Raskin RE and Meyer DJ (2001) Atlas of canine and feline cytology. Chapter 2: General
categories of cytologic interpretation. 1st edition. Saunders Elsevier, Philadelphia. Pp: 20-
26
38. Schmidt BR, Glickman NW, DeNicola DB et al. (2001) Evaluation of piroxicam for the
treatment of oral squamous cell carcinoma in dogs. Journal of the American Veterinary
Medical Association. 218:1783-1786
39. Schwartz R (1988) Skin cancer: Recognition and management. Chapter 5: Squamous cell
carcinoma. 1st
edition. Springer Publishing. Pp: 36-47
40. Vail DM and Withrow SJ (2007) Withrow & Mac Ewen`s small animal clinical oncology.
Tumors of the skin and subcutaneous tissues. 4th edition. Saunders, St Louis. Pp: 699-
784
41. Webb JL, Burns RE, Brown HM et al. (2009) Squamous cell carcinoma. Compendium on
Continuing Education for the Practising Veterinarian. 31:E9
42. Wobeser BK, Kidney BA, Powers BE et al. (2007) Diagnoses and clinical outcomes
associated with surgically amputated canine digits submitted to multiple veterinary
diagnostic laboratories. Veterinary Pathology. 44: 355-361
43. Zaugg N, Nespeca G, Hauser B et al. (2005) Detection of novel papillomaviruses in
canine mucosal, cutaneous and in situ squamous cell carcinomas. Veterinary
dermatology. 16: 290-298
Figures
Figure 1,2,3,4: Private archive prof. dr. Jan Declercq
Figure 5,6,7,8: Department of Medical Imaging, Faculty of Veterinary Medicine, UGent






























