Embed Size (px)
Citation preview

Case Study: Inter-Local Health Zones
(District Health Systems) in a Devolved Setting
Lin-Awa Health Zone in Kalinga
Department of Health–Bureau of Local Health Development
Institute of Health Policy and Development Studies, National Institutes of Health, University of the Philippines, Manila
March 2001
A publication of Management Sciences for Health–Health Sector Reform Technical Assistance Project (MSH-HSRTAP). This publication was made possible through the support provided by the United States Agency for International Development (USAID), under the terms of Contract No. HRN-1-00-98-00033-00.
UNITED STATES AGENCY FOR INTERNATIONAL DEVELOPMENT
HEALTH SECTOR REFORM TECHNICAL ASSISTANCE PROJECT (HSRTAP)

i
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Table of Contents Acronyms Used ................................................................................................ iii
Foreword............................................................................................................ v
Acknowledgements......................................................................................... vii
Executive Summary ..........................................................................................1
1. Inter-Local Health Zone Gains .......................................................2
2. Best Practices................................................................................3
3. Strengths and Weaknesses ...........................................................3
4. Conclusions and Recommendations..............................................5
I. Introduction ....................................................................................................7
1. Project Objectives..........................................................................8
2. Significance of the Study................................................................9
II. Methodology ................................................................................................ 10
1. Proposed Methods vis-à-vis Actual Methods Used ......................10
1.1 Review of records ..................................................... 11
1.2 Key Informant Interviews and Focus Group Dis-cussions.................................................................... 11
1.3 Rapid survey............................................................. 12
2. Data Analysis...............................................................................13
3. Validity and Reliability Checks .....................................................13
4. Data-Yield Description and Constraints........................................13
5. Limitations of the Study................................................................14

ii
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
III. Findings ...................................................................................................... 15
1. Organization and Key Processes Utilized ....................................16
1.1 History and key milestones ....................................... 16
1.2 Motivations in Setting Up the ILHZ............................ 19
1.3 Mission, Vision, and Objectives................................. 20
1.4 Components and Structures ..................................... 21
1.5 Mandates.................................................................. 24
1.6 Roles and Functions of Key Players ......................... 24
1.7 Political Dynamics..................................................... 26
2. Operations of the ILHZ.................................................................27
2.1 Site Characteristics and Description ......................... 27
2.2 External and Internal Environment ............................ 29
2.3 Composition and Nature of Health Services.............. 34
2.4 Management and Support Systems .......................... 36
2.5 Community Participation ........................................... 39
3. ILHZ Gains and Challenges .........................................................40
IV. Analysis: Best Practices, Strengths and Weaknesses............................ 41
1. Best Practices..............................................................................41
2. Strengths and Weaknesses .........................................................41
3. Patterns and Lessons for Sustainability and Replication ..............42
V. Conclusions and Recommendations......................................................... 44
References....................................................................................................... 46
Glossary........................................................................................................... 47
List of Appendices .......................................................................................... 49
iii
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Acronyms Used BHS Barangay Health Station BHW Barangay Health Worker CHD Center for Health Development C-LGU City Local Government Unit COA Commission on Audit COMELEC Commission on Election CRH Core Referral Hospital DAR Department of Agrarian Reform DECS Department of Education Culture and Sports DENR Department of Environment and Natural Resources DHB District Health Board DHS District Health System DILG Department of Interior and Local Government DOH Department of Health DOH-BLHD Department of Health-Bureau of Local Health Development DOH-CHD Department of Health-Center for Health Development EO Executive Order FGD Focus Group Discussion FHS Field Health Services GOP Government of the Philippines HD Health District HDH Health District Hospital HDB-Mancom Health District Board Management Committee HD-TMO Health District Technical Manual Operations HMIS Health Management Information System HRMD Human Resource Management Development ICHSP Integrated Community Health Services Project ICHSP-AA Integrated Community Health Services Project - AusAID
Assisted IHPS Integrated Health Planning System IHS Integrated Health System ILHD Integrated Local Health District ILHS Inter Local Health System ILHZ Inter Local Health Zone IPHO Integrated Provincial Health Office KII Key Informant Interview LCE Local Chief Executive LGAMS Local Government Assistance and Management Service LHAD Local Health Area Development LGU Local Government Unit LHB Local Health Board LHIS Local Health Insurance System LPP Local Government Performance Project MAO Municipal Administration Office MBA Municipal Budget Office MD Medical Doctor M&E Monitoring and Evaluation MEO Municipal Engineer's Office

iv
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
MCRO Municipal Civil Registry Office MHO Municipal Health Officer MOA Memorandum of Agreement MOOE Maintenance Operating and Other Expenditure MPA Minimum Package of Activity MPDC Municipal Planning and Development Council MPDO Municipal Planning and Development Office MSH Management Sciences for Health MSWD Municipal Social Welfare & Development MTO Municipal Treasurer's Office NGO Non-Government Organization NIA National Irrigation Administration OMA Office of the Municipal Assessor PARE Planning to Access Resources for Health PDC Provincial Development Council PHTL Provincial Health Team Leader PH Provincial Hospital PHN Public Health Nurse PHO Provincial Health Office PHO Provincial Health Officer PNP Philippine National Police PNRC Philippine National Red Cross PO People's Organization PPDO Provincial Planning and Development Office PPS Probability Proportionate to Size REACH Resource Access for Community Health RFO Regional Field Office (DOH) RHU Rural Health Unit RSI Rural Sanitary Inspector SGS Small Grant Scheme TCT Technical Coordinating Team (National DOH) TOT Trainer of Trainees

v
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Foreword The mission of the Department of Health-Bureau of Local Health Development (DOH-BLHD) is to provide “technical leadership on local health systems for equitable and quality health care through the development of policies, frame-works, standards, guidelines, models, capacity and capability building and strategic alliances.” Corollary to this mission is the pursuit of three main goals: • To institutionalize local health systems within the context of local autonomy; • To ensure and sustain quality of care in health services; and, • To develop mechanisms for inter-local government units (LGUs) collaboration
and partnership with other government and non-government organizations and private entities under a devolved system.
Through partnerships with other agencies that seek to uphold the goals of local health system development, the Bureau establishes to provide greater under-standing of the local health systems and how they work within a devolved con-text. It is opportune that the DOH-Bureau of Local Health Development and the Institute of Health Policy and Development Studies of the National Institutes of Health, University of the Philippines, Manila, are able to team up on this project. In keeping with a key thrust to conduct policy researches to identify future policy directions, the Institute is honored to be chosen as part of this project. This project was designed to develop five case studies on inter-local health zones (ILHZs) sites in the provinces of Bulacan, South Cotabato, Kalinga, Negros Oriental, and Pampanga. The expectation is that these case studies will provide ample information on the variations of configurations of inter-local health

vi
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
zone characteristics. Further, the studies yield valuable information on best practices, strengths and weaknesses, policy and programmatic directions. The project output consists of six separate volumes: a stand-alone case study on each ILHZ site and a comparative analysis volume that contains consolidated information and analysis on all the case study sites. Outputs of this project will lead to other productive endeavors aimed to institu-tionalize local health systems such as the production of training manuals, policy handbooks and decisions that will initiate programmatic changes to improve the quality of health services within a devolved context. We envision that these case studies will provide valuable information to those who need to learn more about Philippine Local Health Systems. More importantly, the data from the case studies will assist policy makers and health program managers in crafting appro-priate strategic choices in furthering the development of local health systems.
TERESITA M. BONOAN Director Department of Health Bureau of Local Health Development FELY MARILYN E. LORENZO Director Institute of Health Policy and Development Studies, National Institutes of Health, University of the Philippines, Manila

vii
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Acknowledgements These case studies on Inter-Local Health Zones (District Health Systems) in a Devolved Setting are based on an extensive review of records of many agencies and organizations as well as on comments and insights of many individuals. We would like to acknowledge the efforts of many people in facilitating data collection in the different ILHZ areas from January to March 2001. We would like to thank the DOH-Centers for Health Development (CHDs), specifically the directors of the Cordillera Administrative Region, Central Luzon, Southern Mindanao, and Central Visayas for facilitating access to vital records and data in their regions. We are particularly grateful to the following Provincial Health Officers, Dr. Carlito Santos of Bulacan, Dr. Edgardo Sandig of South Cotabato, Dr. Roy Gavino and Dr. Romy Gaerlan of Kalinga, Dr. Ernesto Santos of Pampanga, and Dr. Filemon Flores of Negros Oriental for making arrangements for recruitment of local research assistants, and for designating local coordinators to coordinate ap-pointments and schedules for the conduct of rapid surveys, interviews and focus group in their areas. We are also grateful to the following people who acted as local research coordi-nators and accomplished the difficult tasks of locating precious records for review and identifying and locating important people we had to talk to: Dr. Jason Galleon of Bulacan, Ms. Lorna Lagos and Mr. Joe Siapno of South Cotabato, Ms. Norma Bunaton and Ms. Nora Borlongan of Kalinga, Mr. Servando Maldas and Ms. Lady Lyn Endac of Negros Oriental and Dr. Marilu Malamug of Pampanga. The rapid survey would not have been possible without the contribution of the local re-search assistants who braved weather, stray dogs, and other local hindrances in the conduct of the household interviews. We also acknowledge the valuable efforts of the DOH Bureau of Local Health Development team specifically Dr. Teresita Bonoan, Director, Dr. Regina So-brepeña, Supervising Health Program Officer and Dr. Rissa Yapchiongco, Chief Health Officer for opening doors so that data collection in the study areas was possible. They also shared helpful and constructive comments on the first drafts. We are especially grateful for the Management Sciences for Health Team who facilitated the processes that made this project possible. Special thanks go to Dr. Eddie Dorotan and Dr. Mary Angeles Piñero, who worked with us all the way, championing the convergence concept, spending many hours providing encour-agement, challenges, insightful comments and guidance on the earlier versions of the case studies and the comparative analysis based on their extensive experience with local health systems, and finally for undertaking technical review of the final document; Ms. Celia Marin, Administrative and Finance Manager for guiding and facilitating the administrative requirements of the project .

1
Health Sector Reform Technical Assistance Project
Executive Summary The passage and implementation of the 1991 Local Government Code (Republic Act 7160) has effected major structural and functional changes in the politico-administrative system, and consequently on the delivery of health care services. As devolution made its way in the health sector throughout the Philippines, the provincial level of local government took charge of hospitals while the municipal and city level managed the public health units. From the point of view of the health sector, this resulted in the fragmentation of health services in contrast to centralized integration at the national level before devolution. To address this situation, the national health department initiated the concept of the Inter-Local Health Zone, in pilot areas in the Philippines, inspired by the concept of Health District System developed by the World Health Organization. The District Health System has been applied in many developed and developing countries, mainly where health services have been decentralized from national to local health authorities. This Inter-Local Health Zone, also called District Health Zone, or simply Health Zone, is an integrated health management and delivery system within a geo-graphical area called health zones or health districts between and among local government units. The concept involves integration in many aspects of health but essentially through a referral system, between public health units and hospi-tals that by devolution have been lodged at different levels of government-- national, provincial, municipal or city. However, there could possibly be variations of the concept when operational and applied in concrete settings, as in the pilot areas in different parts of the Philip-pines. To examine the realities that occurred, the Inter-Local Health Zone Project was undertaken, using the case study design on the initiatives and models developed in sample sites in the Philippines. Hence, the project has five embedded case studies, one of which is in Kalinga Province. Three varying models emerged from the unique cultural, geographical, political, and administrative configuration in Kalinga Province. Using local Kalinga words, one Inter-Local Health Zone was named LIN-AWA, referring to well-being; another, BUMILGAN referring to the Tagalog sumigla or lumakas, or to the upsurge of enthusiasm or strength or life; and the third, CHICO, referring, to the river, the area, the community. The federation of non-government organizations was called Sinangpad, refers to a necklace as commonly worn in the cultural communities suggesting a sense of unity. The Lin-awa Health Zone is an inter-municipality model of three contiguous lowland municipalities in one province. The Balbalan-Bumilgan Health Zone is an inter- (one) municipality (that is, Balbalan)-(one) province (Kalinga) model.

2
Health Sector Reform Technical Assistance Project
The Chico Health Zone is an inter-province-municipality model of two contiguous provinces, consisting of two municipalities in one province and one municipality in the other province. In the Memorandum of Agreement, the zones were called the LIN-AWA ZONE (October 1999 covering Rizal, Tanudan, and Tabuk) and the Chico River District Health System (July 2000 covering Mt. Province with its Zadanga and Bontoc municipalities and Kalinga Province with its Tinglayan municipality). On the other hand, Bumilgan is based on the August 1994 Memorandum of Agreement of the Provincial Government of Kalinga-Apayao (then) and Municipal Government of Balbalan, with effectivity stated as January 1995. This case study of Kalinga Province is one of five multiple embedded case studies in the Inter-Local Health Zones Project. The study was organized around several major concerns, including, the organization, processes, operations; integration and linkages; best practices, success and failure factors, discernible trends; and lessons learned. This report on the Kalinga Province Inter-Local Health Zones focuses in-depth on the Lin-awa Zone, with references to two health zones--the Balbalan-Bumilgan and the Chico River District Health System. In this case study report on Kalinga Province, the concept and practice is variably referred to in the respective areas as the Inter-Local Health Zone or Inter-Local Health System; District Health Zone or District Health System; Health Zone or Health System. 1. Inter-Local Health Zone Gains In two years, modest gains can be observed in the Lin-awa zone, particularly in terms of the following: • Indigenization of the concept and approach indicating a sense of ownership
by the province, and sensitivity to cultural, geographic, socio-political factors. • Proactive creativity for modeling alternative district health zones and systems. • Integration of health and political systems through the functionality of the
District Health Board and the Expanded Provincial Health Board, despite the slow pace of conducting meetings and implementing district health zone poli-cies and plans, not only within levels of government within the province (inter municipal, vertical municipal and provincial, inter provincial levels of govern-ment).
• Integration of health services through the referral system, despite the break in
the chain; thereby, raising issues on the very nature of the referral system and its adaptation to local constraints of geography, topography, terrain, multi-ethnicity and multi-cultural conditions in the province or sites, level of capacities for health services of the district and provincial hospitals.
• Linkages with non-government organizations within the province and foreign
external funding organizations through the Department of Health at national

3
Health Sector Reform Technical Assistance Project
and regional levels for the support systems to institutionalize the inter-local health system/district health system.
• Political Commitment of provincial and municipal local leadership with the
corollary funding support, initially by means of cost sharing of health activities without any transfer of funds, and later by the decision of the District Health Board for respective contributions to a common Trust Fund for the health plan and program implementation within the Lin-awa Zone.
• Implementation of support systems, such as the health human resources
management center, health financing cooperatives (cooperative pharmacy, community based health financing) for the operationalization of the district health system, infrastructure (upgrading of the provincial and district hospi-tals, repair and construction of rural health clinics and barangay health sta-tions).
• Driving force of the Provincial Health Office through periods of political
uncertainties and constraints to initiate, implement, expand, and sustain the inter-local health system and other support systems within the province.
2. Best Practices Kalinga Province is an example of best practices in: • Local adaptation, modeling, and indigenization of the WHO and the DOH
models as seen in the clustering of municipalities and the referral system; • Implementation of integrated support systems to institutionalize the district
health system through collaboration with the DOH at the national level, the RHO at the regional level, foreign external funding organizations, and local non-government organizations;
• Health planning and development that takes serious account of local geogra-
phy, terrain, culture, • Financing the Indigency Program in cooperation with Phil Health to give
people access to health care and help sustain the district health system; com-munity based health financing through cooperatives
• Driving force and advocacy of the Provincial Health Office (Provincial Health
Officers) through periods of political uncertainties and constraints to initiate, implement, expand, and sustain the inter-local health zones.
3. Strengths and Weaknesses However, the system is not without its weaknesses and strengths, success and failures. Specifically, the Lin-awa District Health Zone has faced difficulties in its early stages at the Lin-awa zone. These were:
4
Health Sector Reform Technical Assistance Project
• The uncertainties about the local executive’s authority at the provincial level stalled the process of implementation.
• The rotation of mayors as co-chairs of the District Health Board has not
optimized the work of the zone because local executives have not attended meetings.
• Vague and unclear roles of the DOH representative weakened performance
of monitoring and liaison related to the district health system. • The District Health Board and the Provincial Health Board moved fast at the
beginning but slowed down by the early part of the next year of operation, with the medical and health staff of health centers and the hospitals as the more consistent in pursuing the work of the zone.
• Hospitals were not prepared to provide the secondary and tertiary level of
health care that it was expected to do for the zone and in fact were down-graded.
• The most important and crucial issue consists in the very nature of the
geography, terrain, culture of Kalinga Province that most be understood more deeply for better clustering of district health zones/systems and interventions in structure, policies, plans, and programs.
Given the short time, the case study is useful to discern positive patterns and lessons for sustainability and replication, such as the following. • The referral system is taking place despite the fact that this is not the ex-
pected and normal chain that starts from the BHS, to the RHU, to the District, and to the Provincial Hospital due to the very nature of the terrain, inadequate transportation and road networks, culture, patients’ preference for the ser-vices and capacities of the health facility.
• Hospitals are undergoing upgrading processes for capacity building, to do its
part in the referral system. There are structures in place – the Provincial Health Board and the District Health Board, that wait to be reinforced and strengthened to carry its functions ably. The provincial health officers have acted as the driving force for the operationali-zation of the district health system. Upon debriefing for this case study, they immediately moved to convene the Lin-awa Zone District Health Board to ad-dress the problems raised. In its meeting of March 8, 2001, the board decided on the measures to sustain the Lin-awa zone. At this point in time, the recent (March 8, 2001) policies, actions, and agreements among the DHB members can be considered as sustainability measures since by these the threats have been overcome and the continuance of the Lin-awa is assured:
5
Health Sector Reform Technical Assistance Project
• The DHB will implement the policy that three (3) mayors shall be Co-Chairs of
the DHB and meetings shall be hosted and presided on rotation by the re-spective mayors. The regular meeting is every 3rd Thursday of the 1st month of each quarter. The MHO and staff will be the Secretariat and responsible for logistics.
• The DHB will be constituted to include the SP on health of the province and
the SB on health, MPDO, NGO reps, MHOs, COHs, DOH representatives in Tabuk, Tanudan, Rizal. The functions will operate as revised during this March 8, 2001 meeting.
• Schedules will be followed for performance review in 2nd week of December
and submission of health plan for the next year is every July, while district health plans to be done every September. Calendar of activities was set within a year for presentation of annual health plans, finalization of annual district plans and performance review.
• A Trust Fund will be established with contribution by each established RHU of
P100, 000/year; the hospital of P100, 000/year; and core referral hospital of P200, 000/year.
• Project proposals will be submitted for approval and funding by the DHB. • Each health facility will develop health care financing. • A unified referral system will be adopted in the zone and the staff will be
oriented in a seminar. • Health personnel in Lin-awa shall participate in activities during calamity,
disaster, and epidemics within the zone. 4. Conclusions and Recommendations The strategic value added of the IHLZ lies in the fact that it has “re-integrated” the health system after the adverse effects of devolution have been undeniably determined and the complexities of devolution have been somehow understood. It may be viewed as a creative approach that stands validation in Philippine setting, particularly in Kalinga, where conditions are different from the rest of the Philippines. Kalinga belongs to the Cordillera Administrative Region, the forma-tion of which is an indication of its critical role in national and regional political and administrative integration and development. The three models can be examined for replication when conditions in other sites parallel those in the respective zones. Lin-awa Zone is a model for contiguous lowland municipalities. Chico River District is an inter-province model; Bumilgan (Balbalan) District is a case of a vertical model between municipality and prov-ince. These two are for mountainous areas, and where transportation and road links are weak such that a contiguous model will not apply.

6
Health Sector Reform Technical Assistance Project
Finally, the Kalinga case raises the following policy issues: • The unilinear referral chain that cannot be observed during transition period
where hospitals are upgrading and patients prefer to go to facilities based on accessibility, location, culture, services and capacities of the health facility.
• To upgrade hospitals raised the issue of revenue retention, from income
derived from their services. • With respect to the Provincial Health Board and the District Health Board, the
issue of leadership presents the options favoring the health officials than po-litical leaders in the position of chair; and
• On health financing, the legal aspects of LGU budget allocation and resource
generation must be explored to fund the health zones. In a macro scale, the Kalinga experience can be explored when considering the local health zone component of the Health Sector Reform Agenda. The perform-ance of the health sector under devolution hinges on the synergy of health stakeholders in the local health system and in convergence zones to counter-act the fragmentation in the early years of devolution. There is a need to bring down health objectives from the national to the local level in a coordinated and inte-grated way, as well as, to pool resources and capacities of various stakeholders. The Kalinga experience can be compared with the other cases to extract a more general pattern of how local health systems can achieve positive results for the people’s health. It has made possible the linkages of the national, regional, and local government units and within its jurisdiction, the integration of public health units and hospitals. Given this take-off and its results, the inter-local health system or district health system can be optimized. Policies, even legislative action, can ensure that the gains will be pursued.

7
Health Sector Reform Technical Assistance Project
I
Introduction The passage and implementation of the 1991 Local Government Code (Republic Act 7160) has effected major structural and functional changes in the politico-administrative system, and consequently on the delivery of health care services. As devolution made its way in the health sector throughout the Philippines, the provincial level of local government took charge of hospitals while the municipal and city level managed the public health units. From the point of view of the health sector, this resulted in the fragmentation of health services in contrast to centralized integration at the national level before devolution. To address this situation, the national health department initiated the concept of the Inter-Local Health Zone, in pilot areas in the Philippines, inspired by the concept of Health District System developed by the World Health Organization. The District Health System has been applied in many developed and developing countries, mainly where health services have been decentralized from national to local health authorities. This Inter-Local Health Zone, also called District Health Zone, or simply Health Zone, is an integrated health management and delivery system within a geo-graphical area called health zones or health districts between and among local government units. The concept involves integration in many aspects of health but essentially through a referral system, between public health units and hospi-tals that by devolution have been lodged at different levels of government-- national, provincial, municipal or city. However, there could possibly be variations of the concept when operational and applied in concrete settings, as in the pilot areas in different parts of the Philip-pines. To examine the realities that occurred, the Inter-Local Health Zone Project was undertaken, using the case study design on the initiatives and models developed in sample sites in the Philippines. Hence, the project has five embedded case studies, one of which is in Kalinga Province. Three varying models emerged from the unique cultural, geographical, political, and administrative configuration in Kalinga Province. Using local Kalinga words, one Inter-Local Health Zone was named LIN-AWA, referring to well-being; another, BUMILGAN referring to the Tagalog sumigla or lumakas, or to the upsurge of enthusiasm or strength or life; and the third, CHICO, referring, to the river, the area, the community. The federation of non-government organizations was called Sinangpad, refers to a necklace as commonly worn in the cultural communities suggesting a sense of unity.
8
Health Sector Reform Technical Assistance Project
The Lin-awa Health Zone is an inter-municipality model of three contiguous lowland municipalities in one province. The Balbalan-Bumilgan Health Zone is an inter- (one) municipality (that is, Balbalan)-(one) province (Kalinga) model. The Chico Health Zone is an inter-province-municipality model of two contiguous provinces, consisting of two municipalities in one province and one municipality in the other province. In respective Memorandum of Agreement, the zones were called the LIN-AWA ZONE (October 1999 covering Rizal, Tanudan, Tabuk) and the Chico River District Health System (July 2000 covering Mt. Province with its Sadanga and Bontoc municipalities and Kalinga Province with its Tinglayan municipality). On the other hand, Bumilgan is based on the August 1994 Memorandum of Agree-ment of the Provincial Government of Kalinga-Apayao (then) and Municipal Government of Balbalan, with effectivity stated as January 1995. This case study of Kalinga Province is one of five multiple embedded case studies in the Inter-Local Health Zones Project. The study was organized around major concerns, namely: the organization, processes, operations; integration and linkages; best practices, success and failure factors, discernible trends, and lessons learned. This report on the Kalinga Province Inter-Local Health Zones focuses in-depth on the Lin-awa Zone, with overview discussions on the two health zones--the Balbalan-Bumilgan and the Chico River District Health System. In this case study report on Kalinga Province, the concept and practice is variably referred to in the respective areas as the Inter-Local Health Zone or Inter-Local Health System; District Health Zone or District Health System; Health Zone or Health System. 1. Project Objectives The ILHZ case study project conducted multiple embedded case studies to determine the processes and initial outcomes of existing models of inter-local health zones with reference to certain configurations of health zone characteris-tics that include organizational, managerial, financing and information variables. It sought to determine motivating factors in establishing ILHZs and to describe the organization and management schemes of current local health systems. Moreover, it described existing management structures including financing schemes, information systems and tools used in planning and referrals. Specifically the project aimed to: • Identify and describe the contexts of the multiple cases that will be the units
of analysis in this study; • Conduct review of documents and literature that will provide valuable back-
ground information and inputs to the case studies;

9
Health Sector Reform Technical Assistance Project
• Conduct interviews of key stakeholders at central, regional and provincial levels involved in the development of the inter-local health systems;
• Conduct focus group discussions of selected key players/implementers of local health systems and their counterparts at the provincial and regional lev-els;
• Conduct a rapid survey of community perceptions of local health care system
performance and outcomes in selected case study barangays; • Conduct review of documents to ascertain the functionality of local health
systems; • Identify variables that influence viability and sustainability of local health
systems; • Accomplish with-in case and cross-case analyses to determine similarities
and distinctions across cases that impact local health system performance and outcomes;
• Identify issues and problems encountered by existing local health systems
and their corresponding alternative solutions; and • Identify policy and programmatic reform directions that may be recommended
as a result of the case studies. 2. Significance of the Study As the operationalization of the concept has been at its early stages, the study in the sample sites, and particularly in Kalinga Province is mainly significant in describing what actually occurred compared to what it should have been. More than this, the study brought out the unique features of each site for cross-comparison of lessons and various nuances that made this possible, including the cultural, geographic, political, socio-economic, and administrative factors. Primary data that have been gathered are vital to all stakeholders in the health sector that aim at bringing health care accessible to all segments of the popula-tion. For the Department of Health at the national level and local government, the data can be used to re-examine the concept and the strategies, and make decisions on future directions, particular on the clustering of areas, the roles of participating stakeholders, and various aspects of the management system.

10
Health Sector Reform Technical Assistance Project
II Methodology
1. Proposed Methods vis-à-vis Actual Methods Used Kalinga Province was chosen as the case study subject because it is a pilot area in the northern part of the Philippines for two initiatives of the Department of Health's Bureau of Local Health Development with the local provincial govern-ment. These initiatives are the Integrated Community Health Services (ICHSP) Program funded by the AUSAID; and, the Inter-Local Health Zone. The use of the embedded multiple case study design (Yin, 1992) for five cases of the IHLZ has made it possible to analyze in-depth at least one model in Kalinga Province, that is Lin-awa, though the two other models were also explored, and then to make a cross-case analysis with other selected pilot sites. With this method, the Kalinga Lin-awa model was examined in terms of its contexts at the national, municipal, provincial and regional levels. The unit of analysis is the district health system or inter-local health system because the integration of the public health system under the municipal or city government and the hospital system under the provincial government level is expected to occur at this level. Also, the Management Sciences for Health (MSH) and the Department of Health (DOH) Bureau of Local Health Develop-ment (BLHD) have designated the district health systems as the cases for this project since these have been the operational units for the health reform initiative on integrated health management. Specific variables for analysis of the cases, including Lin-awa in Kalinga Province were the following: ILHZ utilization rates; budgets, funding and resource genera-tion capabilities- private - public mix; organization variables such as decision-making structures and processes, sharing or resources, communication patterns, and information mechanisms; human resource development schemes; commu-nity and private sector participation patterns; and selected health service quality measures. For triangulation of findings, the study used three methods for data gathering: (1) the review of records of selected district hospitals and their selected correspond-ing catchment municipalities; (2) key informant interviews of key stakeholders including, chiefs of hospital, municipal health officers, provincial health officers, and selected local health board members i.e. mayors and DOH representatives; (3) focus group discussions to determine perceptions of sample households in

11
Health Sector Reform Technical Assistance Project
communities, of health workers at the municipal health unit and at the referral hospital. The rapid survey obtained the community perception of ILHZ perform-ance and outcomes in selected barangays particularly on stakeholder satisfac-tion, as one of the important measures for quality of service. The study combined qualitative data with quantitative data to for robust case study findings and analysis.
1.1 Review of records Strategic and development plans, maps, annual reports, various documents and records were collected from various sources in the province (Appendix 1). At the provincial level, pertinent information about the Provincial Health Office, the Kalinga Provincial Hospital, and the district hospitals, were gathered. On the Lin-awa Inter-Local Health Zone, pertinent reports and documents were available from various provincial, municipal, and hospital units – from officials and staff. Vital data on Lin-awa were obtained from: the memoranda of agreement estab-lishing the ILHZ; the District Health Board minutes of meetings and health plan; the provincial and municipal development plans and annual reports, and the district/provincial/municipal hospital development plans and reports. Health plans and reports were gathered about each of the Lin-awa member municipal local government units (Tabuk, Tanudan, and Rizal), as well as, the municipal community hospital in Tanudan and the district hospital in Rizal. When information surfaced about the two other models, the Balbalan-Bumilgan District Health Zone and the Chico District Health Zone, attempts were made to get some documents though not to the extent as those gathered on Lin-awa. Also, materials were gathered concerning the Integrated Community Health Services Project and the PhilHealth Indigency Program, which are deemed to be essential contexts for the district health zones and systems in Kalinga.
1.2 Key Informant Interviews and Focus Group Discussions The key informant interviews and the focus group discussions were mainly designed to elicit important details about the processes of setting up and manag-ing the ILHZ these probed into the key factors that influenced the success or failure of local health system operations. Data from the interviews and discus-sion were intended to triangulate data derived from the review of records and rapid survey of community perceptions on their health services utilization and participation patterns. The study team based on known key stakeholders in the IHLZ prepared an initial list of key informants and FGD participants in the FGDs. However, these were later refined for the final list while in the field as soon as changes in assignments or identification of other key informants and participants was recognized (Appendix 2 List of FGD and Key Interview Participants). Data collection was accomplished from February 28, March 1 to 2, 2001 by a research team composed of one case study writer, one co-investigator, two research associates and ten local research assistants who assisted in the survey. De-briefing was done on March 2 among the key informants. New data or updates were obtained from key informants upon pre-final report validation.

12
Health Sector Reform Technical Assistance Project
1.3 Rapid survey The rapid survey method utilized in IHS study was in accordance with the WHO prescribed method of RSM (Frerichs and Tar, 1998b and 1989). It aimed to gather data on prevailing community health seeking behavior and community perceptions on health, utilization patterns and satisfaction at different levels of the health service system in the district health zone—from Barangay Health Station, Rural Health Unit, District Hospital, and at the Provincial Hospital levels. This method was also used to determine satisfaction for the health services that they utilized and factors underlying or influencing such behavior. All these were intended to completely describe the current health environment in the study sites. Sampling. A two-stage cluster sampling was utilized to determine the population sample to be interviewed. Clusters of barangays within the catchment municipali-ties were selected at the first stage and households within the clusters at the second stage. From a list of all barangays and municipalities within the catch-ment area of the reference hospital, a municipality cluster was randomly identi-fied from which a cluster of barangays was derived, with the probability of selection proportionate to the size of the resident population (PPS or probability proportionate to size). The defining criterion was their location from the core referral or district hospital utilized in the study. The population was differentiated according to whether they lived close to the reference hospital, i.e. within five kilometers or whether they lived beyond five kilometers from the hospital. At the second stage, the first household to be visited was randomly selected. Thereaf-ter, households to be interviewed were sampled from the nearest households until the determined proportion for the barangay has been fulfilled. For Kalinga, a 5% sample of the total households in an identified cluster was interviewed. The municipality of Tabuk was the study site for the sampling of household clusters whose population live within 5 kilometers from the hospital and therefore has ready access to hospital services and the municipality of Rizal with population located beyond 5 kilometers from the hospital with less geo-graphical access to District hospital services. The different barangays in each municipality and the corresponding respondent size are shown in Appendix 3. In each household, responsible adults such as mothers, fathers, or anyone over 18 years old responsible for the household were interviewed with a preference for mothers. Respondents. FGDs were done in Kalinga among a total of 58 participants in 8 different groups and 8 key informants were interviewed. Please refer to Appen-dix 2 for list of FGD and KII participants. The DOH Regional Health Officer responded by questionnaire and the LHAD representative was interviewed. At the provincial level, these included the Sangguniang Panlalawigan Chair for Health Committee who was also sent by the Governor, the Provincial Health Officer II as over-all in charge and the Provincial Health Officer I who is also Chief of the Kalinga Provincial Hospital. FGD groups at this level were the hospital staff and the DOH representatives. At the municipalities of Lin-awa District Health Zone, FGDs were done in one rural health unit each in Tabuk and Rizal; also as they are available, among the municipal officer, planning officer,

13
Health Sector Reform Technical Assistance Project
chief of local municipality and district hospitals, Sangguniang Bayan Chair of the Committee on Health. For the two other models, Bumilgan and Chico River, the DOH Representatives were interviewed and the regional and provincial health officers provided other information. In the rapid survey of the Lin-awa District Health Zone, a total of 309 household respondents were interviewed. The target, of which 225 were from Tabuk representing the people with more access to the Kalinga Provincial Hospital as core referral hospital of the Lin-awa District Health Zone and 84 from Rizal representing the people from the more distant area and therefore less access to the core referral hospital. Please refer to Appendix 3- Sampling Frame for Kalinga. This number comprises 5% of the number of households in their respec-tive barangay clusters. 2. Data Analysis Data derived from the Focus Group Discussions and the Key Informant Inter-views were transcribed, coded and displayed in qualitative data matrices using Microsoft Word. Survey data was encoded using Epi-Info 6 and summarized, and organized using Microsoft Excel. Statistical analysis including trend analysis was accomplished using STATA 7. Data display tables were crafted using Microsoft Word to aid the report. Records were reviewed for content and analyzed vis-à-vis key informant inter-views and focus group discussion data. These were then clarified with respon-dents in the debriefing session immediately after the data collection period. New data were surfaced by the Provincial Office at the time of pre-final report valida-tion which showed their efforts to address the problems raised during the de-briefing and make their health zones and system viable. 3. Validity and Reliability Checks Pre-testing the instruments in Maragondon, Cavite, safeguarded validity and reliability of the research instruments used, the FGD and KII topic guides and the survey questionnaire. Furthermore, researchers ensured triangulation by source and method during the data collection process. Some information sought in the review of records was validated in the rapid survey as well as in the FGDs and KIIs. Also, similar questions were posed to different respondents to determine the degree of concurrence and variance of perspectives. The de-briefing session was conducted to clarify the data collected among the key informants. Conferring with the key implementers at the provincial office who provided updates on the initiatives to address the problems and gaps previously identified by the study steam and presented during the de-briefing also ensured validity. 4. Data-Yield Description and Constraints The data set is a mix of qualitative and quantitative data. The former consisting mainly of transcriptions of interviews and discussions and the latter comprised of
14
Health Sector Reform Technical Assistance Project
tables of summarized survey results. The corresponding data matrices that were crafted to organize and display data are useful in determining patterns and trends. However, the body of information is constrained by some factors. An initial list of respondents for the FGDs and KIIs were initially drawn as pre-determined from the proposed methodology of the study. However, it was found that many of the respondents had multiple responsibilities and titles. Hence, in the end there were fewer interviews conducted than planned, as the same people comprised the different groups that needed to be interviewed. The records and documents that were reviewed were voluminous and necessi-tated meticulous organization. Hence, there may be some data that have been inadvertently left out in the analysis. 5. Limitations of the Study While the study initially aimed to analyze selected trends in health status and health services indicators that would cover 10 years to account for the pre-devolution, devolution, and post-devolution periods, due to unavailability of data for some years, trend analysis was limited to 5 years at best for some indicators. Also the findings in this study are limited to observable phenomena regarding the development of the Inter-local Health Zones in Kalinga Province, particularly on the Lin-awa Zone. Constraints of time and resources did not allow a parallel study on the two other zones that appeared to provide viable locally adapted systems. But the Provincial Office has indicated future plans to document and examine the two other zones. The case study has only been able to describe the processes, identify problem areas, and probe on future plans to sustain the system. It is too early to deter-mine the various outcomes and effects. But as a value-added to the objectives of the study, the debriefing session with some key members of the provincial and the district health boards on the data collection helped them identify the issues and problems in the operations of the Lin-awa Zone. Subsequently, on March 8, 2000, the Lin-Awa District Health Board was convened to formulate the policies and action to address the identified problems, which were relayed by the provin-cial health officials to the study team for inclusion in the final study report.
15
Health Sector Reform Technical Assistance Project
III Findings
The Province of Kalinga has a unique contribution to the concept and operations of the inter-local health zone or district health zone given the nature of its topog-raphy and ethnocultural communities. Indigenized Local Models. The Kalinga Province is an example of local indigeni-zation of the District Health Zone developed by the World Health Organization and its adaptation by the Philippines Department of Health in the concept called the Inter-Local Health Zone. It is an example of modeling culturally and geo-graphically sensitive local integrated health systems under a politico-administrative decentralized setting or devolution. Despite birth pangs and constraints, stakeholders in Kalinga’s development proactively shaped the Inter-Local Health Zone or District Health Zone with serious consideration of the varying ethnocultural, political, socio-economic, and geographic complexities of the province. Words in the local dialect used for the names of the district health zones denote the local adaptation. Lin-awa (Lin-awa Zone) is said to be a Kalinga term for well being or comfort. Bumilgan (Bumilgan Zone) is another Kalinga term for the Tagalog “sigla” or for English words joy, strength, alive. Sinangpad is the name of the federation of non-government organizations referring to the neck-lace of different beads and colors worn in the cultural communities and suggest-ing unity amidst differences. Concept Clarification and Reformulation. There is a consensus among stake-holders in Kalinga Province that the Inter-Local Health Zone and District Health Zone is the same in concept and practice and the terms can, therefore, be interchanged. These terms refer to the functional integration of the public health system and the hospital system in a geographical area, that is Kalinga Province and the local cluster of areas, although different levels of local government administer these separately. That is, the municipal local government managed the public health system that includes the Rural Health Clinics and its catchment of Barangay Health Stations, while the provincial local government managed the hospitals. The terms Inter-Local Health System and District Health System denote not only the geographical area or zone but also the referral system that links the levels of health care services under the provincial and the municipal local government levels. This consists of the chain of patient referral starting
16
Health Sector Reform Technical Assistance Project
from primary health care in the public health system (RHUs and BHS) under municipal/city local government (where the Local Chief Executive is the Mayor), to the secondary and to tertiary health care by hospitals administered by the higher provincial local government level (where the Local Chief Executive is the Governor). The integration of the political system and the health system also takes place through the District Health Board for the zone and the Provincial Health Board. Respectively, the membership is taken from the area's local government chief executives, health officers, council members who chair the Committee on Health, and even from the non-government organizations. Operationalizing the Prototypes. Kalinga began by adopting the initial WHO and DOH models by selecting the cluster of three contiguous municipalities in the lowland areas. But recognizing Kalinga’s unique terrain and topography, culture and varying levels of socio-economic development, the provincial au-thorities and stakeholders ventured into other models. In effect, the initiatives raised conceptual challenges on the very nature of integration involving levels of government and health services. For Kalinga, the system need not be an unbroken linear chain from one health care level to the next in specific sites; nor simply a prescribed horizontal integration or conver-gence of municipalities. The three initial modes of political and administrative convergence zones and integration of health services are: • At inter-municipality level and contiguous areas as in the case of the three
municipalities (Tabuk, Tanudan, Rizal) comprising the so-called Lin-awa Zone.
• At the level of one municipality (Balbalan) and the province (Kalinga) where it
belongs based on geographic, cultural, and developmental factors as in the case of the Balbalan-Bumilgan Health Zone.
• Integration between provincial level of government as in the case of the so-
called Chico River District Health System with one municipality (Tin-glayan) in Kalinga Province and two municipalities (Bontoc and Sadanga) in Mountain Province.
Each district health zone has a core referral hospital and catchment areas (Please see Appendix 4 for maps of the zones, referral hospitals, barangay health stations). The establishment, structure, operations, patterns of the system in the respective health zones is discussed in the subsequent sections. 1. Organization and Key Processes Utilized
1.1 History and key milestones Prior to the 1991 Local Government Code that called for devolution in the Philip-pines, the World Health Organization had introduced the District Health System model (1983) and the Department of Health had partially or fully implemented it

17
Health Sector Reform Technical Assistance Project
in provinces. As devolution was carried out, the Department of Health docu-mented the decline in the provision and quality of health care services in different parts of the country. There were breakdowns in the referral system, planning, health information, training, and drug procurement. The effects were seen in the re-emergence of communicable diseases, low quality of health services, and high infant and maternal mortality rate (MSH 2000). These were traced to the fragmentation in the health system as the public health services were placed under the municipal local government, while the hospital services, under the provincial government. The national government no longer exercised direct centralized control over these local government units and the health system. The beginnings of the District Health System in Kalinga can be traced to various initiatives, including the conceptualization of the Integrated Community Health Services Project in 1995, the separation of Kalinga from Apayao in 1995, and the DOH plan for the Inter-Local Health Zone in the Cordillera Administrative Region. With the inception of the Integrated Community Health Services Project in Kalinga in the last quarter of 1997, the province became the recipient of the grant from the DOH (through a soft loan from the Asian Development Bank) and a grant from the Australian Agency for International Development. The strategy of a convergence area was planned to implement the integration process of seven subsystems. Consequently, the idea of the District Health System was presented to the provincial government. The ICHSP intended to install and implement the subsys-tems in the context of the District Health System. A Memorandum of Agreement was signed by Kalinga Province for the ICHSP in cooperation with the DOH with funding support from ADB and AUSAID (1997). The Memorandum of Agree-ment creating the Lin-awa Zone was signed in October 1999. This MOA men-tioned the Health Covenant 1999 signed by the Department of Health, Department of Interior and Local Government, and the League of Governors, as well as, adopted Presidential Executive Order No. 205 that directed LGUs to establish inter-Local Government Cooperation. This MOA also cited the DOH support for the implementation of the Health Covenant and appropriation of funds for the provinces, including Kalinga for its Lin-awa Zone. Parallel to the developments surrounding the ICHSP and the abovementioned documents, the Department of Health had ventured into the Health Sector Reform Agenda (January 2000) that includes the interventions to address the complexities of devolution implemented since the 1991 Local Government Code. In the immediate early post-devolution period, health services declined and delivery system was fragmented as the municipal governments took over rural health units and barangay health units and provincial managed the hospitals. In Kalinga, general observations were validated that the health referral system was constrained by various factors such as local government jurisdiction, difficult terrain, and lack of roads, low priority and budget allocation for health, among others. The District Health System was deemed the appropriate intervention that will allow co-management of health services, particularly in health financing, cost sharing, health planning, and health referral system. The health zones will be
18
Health Sector Reform Technical Assistance Project
the focus for integrated management systems being developed and funded through the ICHSP. For implementation, the study tour was organized for the mayors in the zones, Sanggunian members, and DOH representatives to visit South Cotabato, for them to learn the experiences in organizing and managing the district health zone and system. The Regional Health Office at CAR and the Provincial Health Office of Kalinga informed the local chief executives about the fund support to the zone. The Provincial Health Officer informed and advised the mayors to ask authority from their respective Sanggunian Bayan. An Orientation session was conducted in December 7, 1999 followed a week after by the Strategic Planning meeting where the Vision and Mission statements were crafted (District Health System Report 2000). Actual funds released by DOH to Kalinga totaled P2M. Of this amount, P1M went to the municipalities, that is, P200,000 for each of the three RHUs of Tabuk or P600,000; P200,000 for Tanudan, and P200,000 for Rizal. The other P1M went to the province, of which P600,000 was given to the Kalinga Provin-cial Hospital, P200,000 to the Tanudan Municipal Hospital, and P200,000 to the Juan M. Duyan Memorial District Hospital. The Lin-awa Zone was also piloted for the Benefit Monitoring and Evaluation Program, which shall monitor the progress of the District Health System; and the Performance Management and Evaluation System that shall evaluate the per-formance of the health workers. The RHO monitored the planning processes at the LGU, fund releases, liquidation, and schedule of future releases. By April 11, 2000, the Lin-awa District Health System report reflected the expan-sions by setting up the Bumilgan Zone of the Municipality of Balbalan and the Chico Zone between the Municipality of Tinglayan in Kalinga and the Bontoc Provincial Hospital in Mountain Province. It should be noted that a Memoran-dum of Agreement was prepared for signing in August 1994 and effectivity in January 1995 establishing the inter LGU cooperation between Balbalan munici-pality with the provincial government of Kalinga. The DIRFO-CAR was men-tioned as having spearheaded the zone with Mt. Province. In creating these new zones, the factors of road and transportation accessibility, terrain and topography, even the aggrupation of ethnocultural communities in certain sites played a crucial part in deciding to veer away from the Lin-awa model and be sensitive to realities. In the three zones’ implementation, key informants’ sketches of the peoples’ customary travel routes showed that they availed of health facilities that were nearer or could be reached at shorter time or lesser transportation costs. They did not take the sequence in the regular referral chain but proceeded directly from either the BHS or RHU to the accessible secondary hospitals. The people also tended to go to facilities in areas where they had friendly cultural relations or cultural affinity. Tribal conflicts that would occur from time to time generally constrained the peoples’ movement and availment of the facilities. After at least a year of operation, positive gains have been noted such as the re-linking of the public health centers and the hospitals as it was before devolution

19
Health Sector Reform Technical Assistance Project
but now under an innovative set-up in the context of devolution. The district health zone and system contributed to the impetus for upgrading the hospitals and the public health centers. However, the geographic clustering of the Lin-awa Zone has been subject to reconsideration since Rizal and Tanudan are still not easily accessible to the Provincial referral hospital based in Tabuk. Attention has also been directed at aspects of the system for review, such as the role of the DOH representative. Compared to Lin-awa, there has been a perceived operational success in the Bumilgan Zone because of the easy access of the people to the West Kalinga District Hospital. In the case of the Chico Zone, the set-up appears feasible and operational despite what could have been difficult as two provinces were in-volved. The active and enthusiastic response of the stakeholders in Chico has been attributed to friendly cultural and social relations of the tribes in the area and accessibility despite the provincial boundaries. At this point in its history, the existing district health zones have yet to fully actualize its objectives. But initial conditions point to discernible patterns and areas for change that can push the feasibility of convergence and integration for health. On March 8, 2001, the District Health Board was convened upon the initiation of the Provincial Health Officers to respond to the issues and problems raised during the de-briefing on data collected by the study team on the Kalinga Inter-Local Health Zones. In this meeting, policies were agreed upon to strengthen the Lin-awa Zone.
1.2 Motivations in Setting Up the ILHZ Financial support, also referred to as augmentation funds, from the DOH through the CAR Regional Health Office somehow helped stir the enthusiasm of the provincial and municipal governments to participate in organizing the district heath zones. Records showed that the RHO-CAR released one million (P1,000,000) to the RHUs of the Lin-awa zone, i.e., P200,000 for three RHUs of TABUK (P600,000); P200,000 for Rizal RHU; P200,000 for Tanudan RHU. Another P1 M was given to the province, of which P200,000 was allocated for the Tanudan Municipal Hospital; P200,000 for the Juan M. Duyan Memorial District and P600,000 for the Kalinga Provincial Hospital. Equipment, supplies and medicines were purchased according to the Work and Financial Plan with corresponding liquidation. In the case of Bumilgan Zone, key informants mentioned the release of P750,000; while Tinglayan received P250,000 making a total of P1,000,000 for the two new zones. Supposedly, the amount was P1M was intended for the Bumilgan Zone but eventually, the P250,000.00 from this amount was allocated and released to Tinglayan as the Chico River Zone was just organized. Public information (Health Journal Chico River health District 2000) showed that DOH CAR gave initial fund of P1M of which P500,000 went to Bontoc General Hospi-tal as core referral hospital, P500,000 for both Sadanga and Bontoc municipali-ties in the Mountain Province.

20
Health Sector Reform Technical Assistance Project
1.3 Mission, Vision, and Objectives The Lin-awa Zone has provided the convergence zone for an integrated health-management system. The drafting of the Lin-awa Zone Health Plan is the signifi-cant result of creating the health zone such that three municipalities and the province can share common vision, mission, and objectives. Formulated in a planning workshop soon after it was constituted, the Vision of the Lin-awa Zone, by year 2004, is to become a self reliant, healthy and productive people in the Lin-awa Zone having access to Quality and affordable health services provided by competent health workers, fully supported by a strong inter-LGU partnership and in collaboration with other GOs, NGOs, POs and the community. Its Mission is to provide quality health care services to people in the Lin-awa Zone in a culture of caring, teamwork and professionalism. Specifically, the objectives in the document (Lin-awa Annual District Health Plan) were: Reintegration. Reintegration of the health system through the development of the Provincial Health Office as the focal point of integration, particularly in relation to communications, program technical assistance, human resource develop-ment and integrated planning and information systems; Development. Development of a strengthened inter-LGU Health System with the following health facilities: • Establishment of the Kalinga Hospital to be able to provide t tertiary level of
care; • Construction of the Tanudan Municipal Hospital as a facility with a defined
mix of services that includes emergency surgery; • Construction of the rural health unit of Tanudan in a strategic location with
complete basic equipment and with improved transport and communication facilities; and,
• Strengthen the RHUs of Tabuk and Rizal by providing complete basic equip-
ment Promotion. Promotion of an affordable and financially viable inter LGU Health System through the following strategies: • More rational resource allocation through health sector reforms; • Introduction of systems of Local Health Accounts to facilitate improved
financial planning; • Strengthening of the systems of revenue collection of the Tanudan Municipal
Hospital, Juan M. Duyan Memorial District Hospital and the Provincial Hos-pital;

21
Health Sector Reform Technical Assistance Project
• Introduction of Systems of inter LGU sharing; and, • Testing and development of alternative health financing scheme like devel-
opment of the Provincial Hospital Pharmacy into a cooperative pharmacy
1.4 Components and Structures In structure, the Lin-awa Zone was established following the WHO and DOH models (Appendix 5 Memorandum of Agreement). In principle, the zone is composed of the municipalities of Tabuk, Rizal, and Tanudan with the Kalinga Provincial Hospital based in Tabuk as the core referral hospital. In the zone are 5 rural health units, one 15 bed municipal hospital at Tanudan, one 25-bed district hospital located in Rizal, and a 100 bed provincial hospital at Tabuk. The health system should be able to provide promotive, preventive, curative and rehabilitative services through the integrated public health and hospital service system through a referral chain. These elements and the objectives of the zone appear to be parallel to the seven key subsystems of the ICHSP-- which in-cluded the following: • Local Health Planning • Health and Management Information • Human Resources Management and Development • Health Care Financing • Hospital Regulations and Management • Community and NGO Mobilization • Benefit Monitoring and Evaluation While there are respective local health boards in the three municipalities man-dated by the Local Government Code, another structure, the Lin-awa District Health Board was created with the following functions: • To propose annual budgetary allocation. • To serve as a technical and advisory committee to the Sanggunian con-
cerned. • To establish working committees to guide health agencies on matters related
to health cooperation. • To determine the supplementary local costs of meeting health service needs. • To engage in joint health and human resource development planning

22
Health Sector Reform Technical Assistance Project
• To share expertise and programs and establish clear mechanisms for refer-rals.
• To build joint health information base As noted by the Provincial Health Officers, the District Health Board met in March 8, 2001 during which the issues and problems raised in the debriefing by the study team were taken up (Appendix 12 Sustainability Interventions). The functions of the District Health Board were re-stated as follows: • Formulate strategic health plan, operational (annual) district health plan,
policies, guidelines, programs, projects and activities to promote and main-tain health in the convergence area.
• Recommend approval of district health plans to the provincial health board for
inclusion to the integrated provincial health plan. • Review, finalize and integrate individual operational plans of RHUs, dis-
trict/municipal hospitals and core referral hospitals into the district health plan. • Determine funding requirements to implement district health plan, identify
and access other sources of funding. The district health board will represent in accessing external funds, both local and foreign.
• Recommend/propose staffing requirements of the different health facilities in
the convergent zone. • Determine and integrate the health personnel's training program needed in
order to improve, upgrade, and sustain the delivery and management of health services in the convergent zone.
• Analyze and recommend management, utilization, and sharing of resources
(manpower, equipment, logistics) in the zone. • Direct and supervise the development and maintenance of a district health
management information system. • Supervise and monitor the upgrading and maintenance of all health facilities
in the convergence area to certified Sentrong Sigla facilities. • Formulate policy guidelines in the installation and maintenance of a functional
health referral system and health care financing schemes. • Monitor, evaluate, and give feedback on the different health programs,
programs and other activities in the convergence area for policy formulation. • Coordinate, collaborate, and cooperate with other government organizations,
POs, NGOs, involved in health activities.
23
Health Sector Reform Technical Assistance Project
• Serve as advisory committee to legislative bodies of participating LGUs on health matters in the convergence area such as, but not limited to the appli-cation of local appropriation for public health purposes.
• Perform other related functions as maybe authorized by competent authority
or law. The membership of the Lin-awa District Health Board encompass the vital stakeholders to link the elements of the public and hospital service system, the legislative and executive authorities, as shown below (see Appendix 12 for amendments done in the March 8, 2001 meeting): Chairs. • Mayors of the three municipalities (initially with one of the mayors, Mayor of
Tabuk, currently as Chair; amended in the March 2001 meeting as co-chairs on rotation).
Members. • Local Health Workers represented by MHOs, Provincial Health Officer I
(also as the Chief of the Kalinga Provincial Hospital which is the core referral hospital, initially as co-Chair, then as member as of March 8, 2001), Chief Of Hospitals of Juan M Duyan Memorial District Hospital, and the Tanudan Municipal Hospital, Administrative Officer III and Chief Nurse of Kalinga Pro-vincial Hospital (as of March 8, 2001).
• Sangguniang Panlalawigan member as chair of the Health Committee. • Sangguniang Bayan member as chair of the Health Committee in Tabuk,
Tanudan, Rizal. • Municipal Planning and Development Officers of Tabuk, Tanudan and Rizal. • NGO representative – from NGOs in Tabuk, Tanudan, Rizal. • DOH representatives of Tabuk, Tanudan, Rizal.
The Local Government Code’s mandated Provincial Health Board and the respective municipal local health boards still exist and are expected to handle their own unique concerns apart from the common agenda of the health zone. But the municipal local health boards have not been actively functional as a result of setting up Lin-awa District Health Board. At the provincial level, the Provincial Health Board has been expanded to include the district health zones as shown below: • Governor as Chair • Provincial Health Officer II, co-chair

24
Health Sector Reform Technical Assistance Project
• NGO representative • Sangguniang Panlalawigan chair of committee on health • Provincial Health Team Leader • Chief of co-referral hospitals - Juan M. Duyan Memorial Hospital, Tanudan
Municipal Hospital, • DOH representative per municipality • 3 Sanggunian Bayan members/chairs of committees on health On the other hand, since the PHO served as the locus of the ICHSP and the district health system, the Provincial Health Officer II acted as coordinator while the Governor was designated as Project Director (as stated in the MOA on the ICHSP) The PH Officer is assisted by the Provincial Technical Staff and the Provincial Health Team, with its leader supervising the DOH representatives for each municipality, particularly in the health zones. A five-year contractual Project Support Unit for the ICHSP, with a Program Evaluation Officer, has been at the forefront of the implementation in Kalinga. At the regional level, the DOH-Regional Health Office and the LHAD are the structures for linking the health zones to the national level and to technical assistance.
1.5 Mandates The Memorandum of Agreement (Appendix 5) setting up the Lin-awa Zone was executed by the provincial government of Kalinga, the municipal governments of Tabuk, Rizal and Tanudan and signed by their chief local executives in Tabuk in October 1999. The document stipulated the creation of the District Health Board called the Lin-awa Zone Board as a health administrative unit that is not at the same time the political unit. The PHO is the focal point for technical assistance in the delivery of health services. It also ensured the construction and establishment of the Tanudan Municipal Hospital and strengthening of the Juan M Duyan Memorial District Hospital, as well as the strengthening of the role of RHUs by construction of rural health clinics in Tanudan and Rizal, by rendering a mix of services, and requiring the lying in clinic in Tanudan because of its difficult geography by providing for two or three beds and a mix of services in all RHUs. The Kalinga Provincial Hospital was designated as the core referral hospital.
1.6 Roles and Functions of Key Players Given the mandate, the Provincial Health Office has a crucial role in the district health system as it is the focal point for technical assistance for the delivery of health services. In practice, this has occurred as the Provincial Health Office, and therefore the Provincial Health Officer, has been the anchor for implemen-tation of the ICHSP and the district health systems.

25
Health Sector Reform Technical Assistance Project
In the referral chain, the barangay health stations are the starting point for primary health care and should refer the patient to the succeeding points in the referral chain, usually to the rural health unit, then to the secondary and tertiary hospitals. Mainly, the BHS and the RHUs are at the frontline in servicing the community through services expected to decongest the secondary and tertiary hospitals. It has been found essential that the BHS and RHUs be aware of the referral chain and carry out the process accordingly. However, it has been difficult to impose and sustain the unilinear referral chain as the people choose to go to other health services for reasons of accessibility, transportation, and quality of facilities. Considering the vital role of primary health care at rural health clinics, the ICHSP targeted the RHUs for capacity building, particularly through renovation as in Rizal and construction in Tanudan. The MOA for Lin-awa zone also stipulated that at least two or three beds for emergency cases and for patients be provided according to standards. The district hospitals are expected to provide secondary health care and the provincial hospital the tertiary care. However, due to problems with equipment and infrastructure, secondary hospitals in Lin-awa have been downgraded to primary hospital level, hence the plans for improvement. Given the plans of the ICHSP, expectations have been somewhat high and positive that the provincial and district hospitals will be upgraded not only in infrastructure but also in human resources development to effectively and efficiently render the required mix of services. Respectively, the member of the Sangguniang Panlalawigan and Sangguniang Bayan as chair of the committee on health at their level also serve as members of the Provincial Health Board and the District Health Board of the zone. They are expected to help in advocacy and budget allocation for health and attend to other health concerns and needs. Actually, the incumbent members showed varying levels of familiarity on the health zones, as well as interactions with the technical health staff. However, as members of the District Health Board, they have so far done their part in presenting health plans and budget requirements for approval by the Sanggunian. The SP member participated in the study tour from Kalinga to South Cotabato for the purpose of learning experiences in setting up and managing the health zones. The local chief executives (Mayors) are co-chairs on rotation basis of the District Health Board (Appendix 6- Organizational Structure). The Governor is chair of the Provincial Health Board. They are expected to provide the leadership to ensure the accomplishment of the purposes of the District Health Board and the Provincial Health Board. Generally, they have a positive attitude toward the district health zone concept. But in the case of Lin-awa, commitment has yet to be sustained even in attending the District Health Board meetings. The Gover-nor has accepted the selection of Kalinga as pilot site of ICHSP and the district health system but has not committed counter part funds, except for the Phil-Health Indigency program. Tabuk has also demonstrated commitment with its counterpart for the indigency health program with PhilHealth. Tinglayan has committed funds to contribute to the construction of a dormitory for patients and

26
Health Sector Reform Technical Assistance Project
watchers in the Chico River zone while undergoing treatment at the Bontoc General Hospital because transportation to and fro is difficult. In the case of the DOH representatives, the role has been perceived as vague and confusing such that expectations and performance have not always matched. DOH reps that are mainly active in monitoring and liaison are usually associated with the zone's active status. Other DOH reps perform other profes-sional health or medical duties with less time for monitoring work on the zone. On the other hand, the DOH Regional Health Office has been perceived as the provider of financial and technical support. The LHAD has taken charge of monitoring the planning processes, fund release, accounting, and performance of the district health zones. In the case of non-government organizations, the Sinangpad is a federation of 24 NGOs involved in varied activities in Kalinga Province (Appendix 14-Sinangpad Directory). Representatives have been invited to the meetings and activities of the ICHSP, the Provincial Health Board, and the District Health Board (Minutes of PHO and ICHSP meetings in 2000). The ICHSP has provided the NGO profile forms for detailed information and background, the capacity assessment tool particularly on project implementation, and self-awareness questionnaire on the level of knowledge and skills in community health develop-ment work. The representative of Sinangpad or of respective NGOs generally attend meetings as these are within their areas of concern, even within the health sector, such as school based or community based health promotion, community organizing and mobilization, medical and health missions. Sinang-pad also holds its own consultative workshops. On the other hand, the PHO and the ICHSP provide opportunities for project proposal submission to the Small Grant Scheme by Sinangpad or any of the NGOs, as well as links NGOs to coordinative mechanisms and health management support systems. Given the political context of the District Health Board of the health zones, the Munici-pal Health Board in each municipality, and the Provincial Health Board, not a few NGOs are said to have taken a back seat at some point in time. In the end, key informants point to the people, the community, as the principal stakeholders in health. However, there are constraints in their availment of services through the regular referral chain, as already discussed (transportation, road access, quality of facilities and services). It is an individual choice about which facility and service to utilize. On the other hand, key informants perceive the necessity for government action on the constraints to help shape the people’s behavior toward a prescribed referral chain.
1.7 Political Dynamics The three District Health Zones proceeded in its course despite the condition of political ambivalence that the province experienced when there were three governors at one time. The elected incumbent governor was put to jail and was substituted in the meanwhile by the vice-governor taking the office as the acting governor. The situation was complicated by the victory of the electoral protest by the other candidate for governor. Consequently, the mere signing of neces-sary papers and approval of transactions were delayed as it was not certain who

27
Health Sector Reform Technical Assistance Project
held the authority. There is anticipation for the May 2001 elections as a way to settle uncertainties in political leadership and authority. A more long-term issue is tribal conflict. Kalinga Province is home to various ethnocultural communities, some of which have historically rooted customs and traditions for resolving conflicts. When tribal conflicts occur, even tribal wars, the delivery health services are adversely affected such that the people and health personnel are unable to go to the health facilities. Furthermore, the personal leadership style, political affiliation and interests, and political will of the local chief executives were perceived factors affected the zone's status of activity and functionality. Hence, it has been pointed that that the leadership and the structure of the district and provincial health boards be re-examined. Since elections take place periodically, the health officers are the best stakeholders to sustain the system through transition and change, and other instabilities. 2. Operations of the ILHZ
2.1 Site Characteristics and Description The Inter-Local Health Zones/System in Kalinga Province is seriously affected by the factors of topography and terrain, interrelated with culture. The clustering of municipalities constituting the three district health zones was directly a conse-quence of physical characteristics. The Lin-awa zone was based on the lowland configuration of its three member contiguous municipalities. The Bumilgan District Health Zone can be constituted by one only municipality, Balbalan, and linked to the provincial hospital; while the other municipalities are constrained by lack of land and road access. The Chico District Health Zone is constituted with one municipality inside Kalinga Province and two municipalities of the Mountain Province by reason of geographic proximity. Furthermore, tribal communities are configured in the context of such physical space and the complexities of tribal conflicts. The situation can be understood as one views the map of the province. Public information sources (planning documents and reports) in Kalinga province show its location in the central part of the Cordillera Administrative Region bounded and landlocked on the north by the province of Apayao, east by Cagayan, West by Abra, and on the south by Mt. Province. It used to be a sub-province in Kalinga-Apayao Province until passage of the Republic Act 7878 in February 14, 1995 when it became a province of its own with 8 municipalities and 152 baran-gays (District Health System Lin-awa Zone: 1). Tabuk is the capital town and the other municipalities are Balbalan, Tinglayan, Lubuagan, Pasil, Pinukpuk, Tanudan, Rizal, and Tabuk as capital town (Province of Kalinga Medium Term Development Plan 1991-2004). It has an area of 3, 119 km, which is 17% of the Cordillera. The topography is described as “rugged and sloping with moun-tain peaks of 1,500 and 2,500 meters in height.” There are “sharp crested interlinking peaks of steep slopes, isolated flatlands, plateaus, and valleys” on the western side and “gradually sloping foothills. ” (Please refer to Appendix 4 for Maps).

28
Health Sector Reform Technical Assistance Project
Accounts on the history and culture of Kalinga trace its name to the Ibanag word Kali-nga and the Gaddang word Kalinga referring to the people who conducted headhunting attacks and who lived by the tradition of tribal wars and head-taking. The Kalinga is one of the major ethno linguistic groups inhabiting Northern Luzon, whose language consists of a mix of thirty-nine dialects spoken and understood among the ethnic grouping (Province of Kalinga Medium Term Development Plan 19991-2004, citing Billet and Lambrecht 1970: 1). Human Resources. Kalinga province has a total population of 151,145 (NSO Kalinga; please see Appendix 7). Tabuk in the Lin-awa District Health Zone has the highest population of 63, 507 persons as reported in 1995 (Province of Kalinga Medium Term Development Plan 1999-2004:1), though NSO placed this at 57,208 as of 1990. Key informants noted that Tabuk is a first class municipal-ity and “cosmopolitan” as it is a center of migrants of various cultures, religion, and language. Tabuk is already densely populated at 99 per square km. Province-wide, Kalinga has a dependency ratio of 79 for every 100 productive persons. Generally across municipalities, male population is 50-51%. Growth rate for is 2.32% for the male and 2.13% for female population (NSO 1995; please see Appendix 7). Average growth rate is 2.23 for the province by end of 1995. Economic Activities. Observations point to low income and farm occupation of most of the population in Kalinga and mainly in the health zones. Consequently, low income makes it difficult for the people to pay for various services including health and education. Statistics showed the 62,200 employed persons or 72 percent of potential labor force, most of who are in agriculture as farmers, fishermen, foresters (77%) and the others in the service and trading sectors, at 18% and 3% respectively (see Appendix 7). Cooperative development is one strategy that has been pursued considering its potential to boost the agricultural sector. In manufac-turing, efforts have been exerted to generate investments and jobs. The province has taken note of the development opportunities in two Lin-awa District Health Zones, Tabuk and Rizal, and another municipality, Pinukpuk. For economic resources, generally 65.75% were identified as protected areas, including Tanudan in the Lin-awa District Health Zone, Balbalan and Tinglayan which are in the two other district health zones (Province of Kalinga Medium Term Development Plan 1999-2004:5). The province reported a total aggregate land area devoted to agriculture of 22.40%. As far as resources are concerned, it has enough forest cover of about 60%, fishing ground, reserves of metallic minerals. This implies that the province has available resources and room for socio-economic development. As observed by key informants, the increase in income attributed to provision of and access to socio-economic opportunities, has contributed to better conditions of living such as in nutrition, health care, education. Growth patterns were noted but still far below maximum in crop production, poultry and livestock production, while food consumption require-ments cannot be fully met.

29
Health Sector Reform Technical Assistance Project
Infrastructure and Utilities. Key informants called attention to the crucial role of transportation and road networks in the referral system. The existing road length of 911.402 km distributed among the 8 municipalities is not enough as many more dirt roads and inaccessible areas, hence the prescribed referral chain in the District Health Zone has not been fully observed. The province reported that condition of existing roads is generally poor, due to network deficiencies and poor maintenance. Only 3% are concrete and 3% asphalt, while the earth roads constitute a total of 357.07 kms. Transportation facilities, particularly bus lines, are generally registered in Tabuk, the capital town, and there are only 6 bus lines operating in and out of the province going to Manila. Hence, there is an impera-tive for the province to address transportation problems. On the other hand, potable water supply is still inadequate even with abundant water resources and irrigation services cover only 33% of total hectares. River controls and flood controls are also necessary since these have been damaged by typhoons. Social infrastructures for health and education also still need to be constructed. The province has also analyzed the lack of barangay health sta-tions and hospitals and schools. Communication facilities have been installed such as telephone lines, television stations, and postal stations; but still need expansion. The province has only one existing power source, generated by the National Power Corporation covering 30% of total potential household. Of 8 municipalities, only 4 have been ener-gized, though 41 barangays have been served with solar energy of 1.23% of total potential household. Social Services. Education and its impact on health promotion are major con-cerns. Key informants noted that Tabuk has become a center for education in the province, validated by the report that the only three colleges in the province are located in the capital town of Tabuk. Pre-school education is offered by 63 schools, 51 of which are community-based while elementary education is offered by 133 schools in the province, of which 129 are run by government. Non-formal education is also offered by the national government agencies. With devolution, health services have been provided separately by the municipal local government through the public health units and by the provincial govern-ment through hospitals. Provincial records, plans and reports showed that Kalinga has 1 provincial hospital and 5 district and municipal hospitals, 11 main health centers (RHUs), and 19 barangay health stations (BHS). Generally, municipalities have two barangay health stations, except for Tabuk and Rizal with three barangay health stations. The health sector in Kalinga is precisely the arena for the innovative intervention of the Inter-Local Health Zone –or the District Health System has it has also been called.
2.2 External and Internal Environment Health Needs and Demands. Health is perceived to be a priority concern in the province by local officials and by medical and health staff, though the local government budget has not been adequate to provide all the needed funds. As a context for health services, the top 10 leading causes of morbidity and mortal-ity are taken into account. The ranked unmet minimum basic needs are also

30
Health Sector Reform Technical Assistance Project
basis for determining health needs and demands to shape health programs. These include: families at income above subsistence threshold level, unem-ployment, family planning practices, children for pre-school and day care, single parents, access to sanitary toilets, immunization, infant breastfeeding, pre-natal and post-natal care, potable water, literacy and education, housing, clothing (Appendix 8, Table 8.15). Consequently, for the past five years, health planning and development has been geared at intensifying health service delivery and health promotion particularly to address high crude birth rate, promote family planning, prevent respiratory and water borne and sanitation related diseases and malnutrition of mothers, chil-dren, and adults. The key province based programs include the s nutrition, sanitation, family planning, manpower, and facilities. National DOH programs have guided the province and parallel health programs are implemented (EPI, Nutrition Program, Family Planning Program, Control of Diarrheal Diseases Program, Control of Acute Respiratory Infection, Malaria Control Program, Tuberculosis Control Program, Under Five Program, and Dental Health Pro-gram. Health manpower has been considerably inadequate. Hence, the province has targeted the municipalities without municipal health officers. The lack of a complete health personnel staff in every RHU has often been bewailed and solved temporarily by an exchange or rotation of staff and by projects of medical missions. RHUs require repair and rehabilitation and additional BHS have been noted as necessary to give immediate primary health care and ease congestion in the hospitals. Though training for health personnel has been perceived as equitably distributed and adequate given their local resources, this still has to be expanded and upgraded particularly in hospitals. To achieve the purposes of the inter-local health zones, the upgrading and licensing of secondary hospitals has been deemed a necessity and a priority. The province has targeted the construction of new municipal hospitals in Luna, Pasil, and in Tanudan and Tinglayan in the Lin-awa and Chico district health zones respectively. The ICHSP has done a service in identifying the infrastructure requirements of the province and within the health zones, as well as in providing the funds for construction and rehabilitation of BHS, RHUs, district and provincial hospitals. In addition, there is a view that the communities be organized and oriented toward community-based health, that they be adequately informed about the referral system. However, it was pointed out that the communities' utilization of these facilities is contingent upon proximity, accessibility, and quality of ser-vices. Health Statistics. For the province, crude birth rate moved from 24.54 in 1995 to 22.7 in 2000, while crude death rate was at 2.06 in 1995 to 3.6 in 2000. For the five-year period 1995-2000, infant mortality rate increased from 15/79 to 19.19 and maternal mortality rate decreased from at 1.24 to 1.02. The leading causes of maternal mortality post partum hemorrhage, hypertension, retained placenta, and RHD. Leading causes of infant mortality per 1000 births include pneumonia, prematurity, congenital anomaly. Malaria, measles, diarrhea are still in the top

31
Health Sector Reform Technical Assistance Project
10 health problems. For the population, leading causes of death, pneumonia, pulmonary, hypertension, accidents, peptic ulcer, CVD, cancer, assault, malaria, old age, bronchial asthma. Leading causes of morbidity include: bronchi-tis/bronchiolitis, malaria, diarrhea, pneumonia, influenza, pulmonary T.B., mea-sles, dysentery, chicken pox, conjunctivitis, ARI, heart diseases. Hospital records also show parallel causes for patient consultation, treatment, and discharges, with varying rankings. (Please see Appendix 8 for the statistics; Province of Kalinga Provincial Health Plan 2001; Provincial Health Annual Report 2000). In the district health zone of Lin-awa, the three RHUs in Tabuk have infant mortality rate of 10.25 -13.58 and infant mortality of 2.47 and 2.71 in two RHUs. (Appendix 8 Table 8.12; for health problems and plans, refer to Rizal Rural Health Unit Operational Plan 2001; Tabuk Rural Health Unit Operational Plan 2001). Health System Description. The Office on Health Services is part of the organi-zation and management system of the provincial government in a devolved set-up, under the leadership of the governor (who is Project Director for the ICHSP). Policymaking is by the Sangguniang Panlalawigan and the Expanded Provincial Health Board -- as it has included the principal representatives from the health zones' District Health Board. Please see Appendix 6. With the recent changes, the Provincial Health Officer II heads the Provincial Health Office and now takes charge of the ICHSP as coordinator, as well as, oversees the hospitals and the district health zones. The Provincial Health Officer I serves as Chief of Hospital of the Kalinga Provincial Hospital. The PHO II is vice chair of the Provincial Health Board and the Provincial Health Officer I was initially co-chair of Lin-awa District Health Zone but this was changed to member as of March 2001. The province has 6 government hospitals with a total of 265 beds and 14 private hospitals with a total of 357 beds and a general ratio of 1 hospital bed to 461 persons in the population (Kalinga Office on Health Services District Hospital Plans 2001). These hospitals are:
Tabuk. Kalinga Provincial Hospital Balbalan .Western Kalinga District Hospital Rizal. Juan M Duyan Memorial District Hospital Pinukpuk. Pinukpuk District Hospital Lubuagan. Kalinga District Hospital Tanudan. Tanudan Municipal Hospital (to be upgraded to Tanu-dan District Hospital )
Municipalities generally have two RHUs but Tabuk has 3 RHUs giving the province a total of 11 main health centers and 19 barangay health stations.

32
Health Sector Reform Technical Assistance Project
Health manpower ratio is 1:28 for physicians; 1:16 for nurse, 1:15 for midwife, 1:14 for medical technologist, and 1: 20 for dentist , which are all, still considered inadequate. (Appendix 8 Table 8.10) The provincial income is estimated at P228, 915, 133.70 for 2001 as it was P224, 472,371 in 2000. Health budget is estimated at P71,02, 158.80 for 2001 with actual disbursement of P79,739,530.69 in 2000. The Internal Revenue Allotment for the province in 2000 was P215,077, 476. This showed a 35.80% actual expenditure for health (Province of Kalinga Accounting Office 2001) As mentioned earlier, the Integrated Community Health Services Project is a vital support to the Province of Kalinga from the Department of Health, through the Asian Development Bank and the Ausaid. According to the ICHSP Work and Financial Plan 2001 Local Counterpart, P5M has been intended for the Kalinga Provincial Hospital from the congressional fund, of which P500,000 is the support for the District Health System. ICHSP has infused various management support systems into the provincial health system. The major components of the project include: (1) community health services support, (2) provincial health service delivery system develop-ment. The Community Health Services Support includes: (1) institutional strengthening, (2) strengthening of the referral system --provincial hospital as core referral center, primary health services, communication system; (3) Com-munity and NGO mobilization; (4) support to priority health programs. For the Provincial Health Service Delivery System Development, the project will develop, test and document subsystems for: health services planning, health care financing, health management and information, hospital regulations and management, human resource management and development, community and NGO mobilization strategy development. Quick Survey Results-Satisfaction and Performance Measures. The quick survey showed that the referral system was not availed of in a sequential or linear chain and that variables of age, education, sex, income did not seem to disturb the patterns of utilization that could be based on proximity, accessibility, and quality of the services and the conditions of the facility. The focus group discussion showed that these factors affecting the use of the public hospitals. Generally, people in Tabuk used the provincial hospital (Kalinga Provincial Hospital) and private hospitals (private practitioners). Those in Rizal, which is farther from the Tabuk-based Kalinga Provincial Hospital, tended to use the RHU and the district hospital. For frequencies, percentages, ranks, please refer to Appendix 9. • Nearest Facility. In Rizal, respondents with incomes less than P2500 and
P5001-10000 were nearest to the RHUs compared to those at P2501-5000 who said they were nearest to the district hospital. For upper bracket at P10001 and above, the nearest is also the RHUs. However, in Tabuk, the provincial hospital ranked first across all income groups except for those at P2501-5000 and above P20000 who said the nearest facility is the private hospital. (Appendix 9 Tables 9.5 to 9.6).
33
Health Sector Reform Technical Assistance Project
By age group, those ages 18-30, 40-51 in Rizal are nearest to the RHU; while those at 31-39 and 53+, to the district hospitals. In Tabuk, the patter is proximity to the provincial and private hospitals across ages. (Appendix 9 Tables 9.7 and 9.8) On the variable of education, the district hospital is nearest to those with elementary and high school background with the RHU coming second in rank. Generally, college graduates were near the RHU in Rizal. However, in Tabuk, the private and provincial hospitals are closest to elementary and college students while the reverse apply to the college, postgraduate and vocational graduates. (Appendix 9 Tables 9.9 and 9.10) By sex, males and females in Rizal were nearest to the RHU. In Tabuk, they are near to provincial and private hospitals. (Appendix 9 Tables 9.11 and 9.12)
• Reference Facility. On the variable of income, the reference facility in Rizal
across income groups is not a discernible pattern as the respondents ranked the RHU, district hospital, private hospital. By age, the nearest reference facility is the RHU and the district hospital. By education, it is the district hospital, then the private hospital, and then the RHU. (Appendix 9 Tables 9.23, 9.25, 9.27, 9.29, 9.31)
Comparatively, there was a consistent pattern among Tabuk respondents for the provincial and private hospital as their nearest reference facility across the variables of income, age, sex, education. (Appendix 9 Tables 9. 24, 9.26, 9.28, 9.30)
• Reference Facility by Service Satisfaction. Majority of Rizal respondents
ranked the district hospital and the private hospital respectively on service satisfaction. In Tabuk, majority ranked the provincial hospital first, the pri-vate hospital second. In both sites, the RHU came a poor third among only a very small percent of respondents. (Appendix 9 Tables 9.21 and 9.22).
• Health Seeking Behavior. On the variable of sex, Rizal female respondents
chose the district and consult the private practitioner; while the males chose either to go to the RHU or self-medicate. In Tabuk, the females go to the provincial hospital or next to the private practitioner; the males preferred the private practitioner and then the provincial hospital. (Appendix 9 Tables 9.23 and 9.24).
By age, the Rizal ages 18-30 ranked the private practitioner and the rural health unit no. 1 and the district hospital next; those across the groups from 31 to 53+ ranked the district hospital first and consulting the practitioner sec-ond. In Tabuk, it is either the provincial hospital first or the private practitio-ner while third health seeking behavior is either self-medication or visit to the RHU. (Appendix 9 Tables 9.25 and 9.26)
Across educational groups, the first health seeking behavior in Rizal is the district hospital for those with elementary and high school background while
34
Health Sector Reform Technical Assistance Project
those in college prefer to consult the private practitioner, then the district hospital, and the RHU. In Tabuk, the practices generally point to the choice between provincial hospital, the practitioner, the self or the RHU. (Appendix 9 Tables 9.27 and 9.28). For lower income groups in Rizal, the first rank behavior is to go to the RHU or district hospital, or self-medicate, or go to the private practitioner while those at incomes of P5001 go to the district hospital or self medicate, while those above P10000 income go to the private practitioner first and then to the district hospital. On the other hand, those in Tabuk at all income groups go either first or second in choice to the provincial hospital or the private practi-tioner. (Appendix 9 Tables 9.29 to 9.32).
Household FGD respondents claimed that they usually apply first aid and self-medicate. They use herbal medicines or ordinary medicines from drug-stores. If they have fever, they do a sponge bath but consult a doctor if the fever lasts for two days. However, they clarified that this behavior depends upon the ailment. They can go to the RHU and BHS but some respondents averred that there are no medicines and would have to be referred to other hospitals whether public or private depending on patient's preference. Some have gone to the provincial hospital but as they would have to buy medicines and supplies outside the hospital, they eventually prefer to go to the private hospital where they are given more care.
Proximity and Accessibility. The Tabuk based provincial hospital and RHUs are accessible to those in the nearby areas since transportation and road networks are available. Time to reach these facilities have been estimated to be some 30 minutes to one hour and even shorter in the case of BHS. But this is not the case in the other parts of the province such as in Rizal and Tanudan due to the lack of road networks. This is even farther from the residents of the other mu-nicipalities, taking a day or two, and even hiking at some parts of the route on dirt road until the point where transportation is available. Consequently, Tin-glayan deemed it necessary and convenient to join the nearby municipalities of the Mt. Province for Bontok General Hospital as core referral hospital.
2.3 Composition and Nature of Health Services Health Programs. By process and procedure, the provincial government usually asks the health centers to prepare their local plans for programs based on local conditions that are put together by the Municipal Health Officer, after which all the municipal plans are aggregated into a provincial health plan and programs. Since devolution, there is no dictation from the central department on health but the national programs are presented to the province that has found these to be relevant to its own health needs and demands. Hence, the health centers provide parallel programs -- Nutrition Program, Family Planning Program, Control of Diarrheal Diseases Program, Control of Acute Respiratory Infection, Malaria Control Program, Tuberculosis and Leprosy Control Program, Under Five Program, and Dental Health Program. The province has added Environ-mental Health Program and IEC. Also, the RHUs have offered laboratory services, consultation, minor surgery, and disease prevention, control of locally endemic diseases. They have continued the reporting and recording of the

35
Health Sector Reform Technical Assistance Project
FHSIS, follow-up of cases, collaboration with NGOs, and monitoring of com-munity health. The provincial hospital has rendered curative and preventive health care, with minimum rehabilitative health care. Appendix 8.17 sows the mix of services under medical, nursing, laboratory, pharmacy, dental, dietary, as well as training and administrative services. The district and municipal hospitals provide OPD services, minor surgeries, OB-GYN and childbirth deliveries, as well as primary health care services. Quality of Health Programs and Services. The province has set indicators for the programs mentioned above to determine accomplishment of targets in hospitals while the municipal local governments monitor the programs at the RHUs and the BHS. At all levels the quality of health programs is limited by major operational problems emanating from lack of funds and personnel, inadequate equipment and machines (in the case of hospitals), and poor facilities (including toilets, water supply, infrastructure). The provincial, district, and municipal hospitals have recently been downgraded. Consequently, the health officials reported that the Kalinga Provincial Hospital aims to be upgraded to a tertiary level hospital and a training and research venue. On the other hand, the other district hospitals at various sites aim at upgrading to secondary hospital status; the Tanudan municipal hospital, to a district hospital (See also District Hospital Plans 2001). The Provincial Health Office has identified the problems of the hospital system including its strengths, weaknesses, opportunities, and strengths; and has prepared the corresponding strategic and operational plans. (Refer to the Kalinga Provincial Hospital Strategic Plan 2001-2005'; Integrated Annual Provin-cial Health Plan 2000; Provincial Health Plan and Operational System 2001) The community residents raised their dissatisfaction in the FGD over the inade-quacy of information, medicines, staff, and poor sanitary conditions in govern-ment hospitals and health centers. They would have to wait for a doctor for even as long as 30 minutes to an hour and buy medicines outside the hospital or medicines would be given in small doses. Hence, they preferred to go to the private hospital in serious cases because doctors can easily attend to them and there are enough medicines. Also in the private hospital, their needs are easily met and all they have to do is pay when they get discharged. But as already pointed out, the communities go to the provincial and district hospitals even for primary health care when these are nearer to them. Hence the construction of RHUs and BHS close to communities for respective catchment areas is per-ceived to be a necessary intervention. According to some FGD participants (13) from an area in Tabuk, the referral system is not strictly followed as the health providers at the BHS and RHU would refer them to a hospital, but not necessarily the provincial hospital and it would depend on the patient's choice where to go. They generally prefer the private hospital because the patient is given immediate attention. However, for some health services like immunization, or problems like asthma and blood pressure, they go to the health facility. Usually the common problems in the family and

36
Health Sector Reform Technical Assistance Project
community are malaria, colds, cough, asthma, and even tuberculosis. There are medicines in the RHU for tuberculosis but usually there is not enough supply. They do not participate in the BHS or RHUs or provincial hospital health projects because the do are not aware of any announcements or of any projects.
2.4 Management and Support Systems While there are two other health zones, the Bumilgan Zone and the Chico River Zone, this study focused on Lin-awa District Health Zone. However, man-agement and support systems were set up at the provincial level, that is, at the Provincial Health Office, for the operations of the three zones. Structures were set-up for policymaking, integrated planning and development, financing, and operations monitoring. Structures. Provincial Health Board is the and the respective District Health Boards are the main structures for policy making at the provincial and district levels respectively for the health zones by reason of the Memorandum of Agreement. However, the Local Health Board of the municipality is the policy and decision body mandated by the Local Government Code. Hence, the decisions of the DHB must be relayed for approval to the LHB by the by the Sanggunian Bayan member who is chair of the committee on Health. The main driving force for management is the Provincial Health Office with a Technical Section with devolved DOH personnel that can provide the technical assistance. The Department of Health-Regional Health Office for CAR is repre-sented by the Provincial Health Team with retained DOH Reps assigned to each of the health zone member municipalities for liaison, monitoring, health advo-cacy, and other related functions. As previously mentioned, the main five-year ICHSP has provided the main support system programs managed by a contrac-tual staff constituting the Provincial Support Unit. With this set-up the province through its provincial health officers has driven the support systems that include integrated planning and development, policy making, health financing, health human resources development, infrastructure development for the hospitals and public health units. Integrated Planning and Development. The initiative in integrated planning and development resulted in the annual district health plan that awaits to be fully operational within the zone. The first major output of the Lin-awa District Health Zone was an annual district health plan. Within the zone, the plan aimed at reducing prevalence of existing diseases, institutionalizing the district health system, upgrading all health facilities, and adopting a health care financing scheme to support the district health system (Lin-awa Annual District Health Plan 2000). Its strategies include: LGU coordination and collaboration in policy making, linkaging with NGO and the private sector, intensified disease surveil-lance, strict implementation of policies and protocols on health programs, IEC, and health manpower development and training. The planning process was participated by the members of the District Health Board, with complete attendance of the mayors, municipal health officers, and council health committee officers. The local health plans were consolidated and

37
Health Sector Reform Technical Assistance Project
integrated into a new strategic and operational plan for the zone. For the purposes of implementing the plan, the Lin-awa municipalities started in 2000 with medical mission projects with sharing of personnel and costs. Local executives commented that the concept, approach, and system are new and barely on take-off stage. The two-year experience has surfaced critical con-cerns that need re-examining for the zone and the system to be sustained. Policy Making. The District Health Board was the new structure established for the purposes of the district health zone. Although rationalized within the context of the Local Government Code, it does not have the same powers as the mu-nicipal Local Health Board. Nonetheless, the district health board provided an opportunity for coordination and collaboration by resource sharing that has been necessitated by the inadequacy of the LGUs budget. Its leadership was placed in the hands the three mayors of the zone as co-chairs. The Mayor of Tabuk was selected as the first chair on the basis of Tabuk’s central role in the province and in the zone. Tabuk is a first class municipality while Tanudan is fifth class and Rizal is sixth class municipality. The resources and capacities of the Tabuk municipal LGU was recognized and the local executive, the Mayor, was willing to help. However, in March 2001, the DHB decided to implement the rotation of the chair and the hosting of the meeting to address the problems of non-participation in meetings by the local executives of other municipalities. The Lin-awa District Health Board has met only twice since 2000 and the early part of 2001, which accounts for the perception that it has not been functional as expected. The May elections and the change in local officials can also change the leadership configuration and there is quite an apprehension about the matter. At the provincial level, the Provincial Health Board has not been maximized due to the problems with three contenders for the post of Governor. The Sanggunian Panlalawigan representative joined the study tour to the district health system in South Cotabato and the familiarity has helped advocate the zone in the council. The first incumbent governor was committed to implementing the district health system in the province and the Vice-Mayor in his capacity as Acting Governor provided the authority during the period of the political controversy. The major part played by the provincial and local councils were in approving the Memorandum of Agreement on the establishment of the zone, the prioritization and budget allocation for health, and adoption of the PhilHealth program in support of the district health system. Financing and Budgeting. The member LGUs in the Lin-awa Zone adopted co-sharing of costs in the common medical mission projects, without any transfer of funds, but by merely using their respective budget allocation for health. In the medical mission in Rizal for example, Rizal used its budget to pay for medi-cines, transportation and gas while Tabuk and Tanudan sent doctors and health staff. To accomplish the zone objective on the financial support system for indigents, the province enrolled 1000 families in the PhilHealth Indigency Program (Appen-
38
Health Sector Reform Technical Assistance Project
dix 8): 600 families in Tanudan and 1000 in Tabuk for which the LGUs gave counterpart funds (Tabuk gave P594,000). Within the ICHSP, the Ambigatton Cooperative Pharmacy was organized at the provincial level for health care financing in the purchase of medicines. The Lingap sa Mahirap program and the DSWD have also been sources of support for indigents. The Ambigatton Cooperative was traced to the monthly "Kumustahan sa Provin-cial Hospital" when the health workers association proposed to set up a multipur-pose cooperative (cooperative pharmacy) to address problems with high costs and shortage of medicines and medical supplies. In November 1999, an obser-vation tour was conducted in Palawan and the name Ambigatton (meaning, morning star in Kalinga) Multipurpose Cooperative was adopted (see Appendix 13). With technical and organizational assistance from DOH-CAR, the Bumilgan Multipurpose cooperative was subsequently set up. The province also launched community based health insurance schemes man-aged by the BHW for payment of piso-piso araw- araw (one peso daily) or P30 monthly. The Bumilgan Medical Assistance Fund, the Rizal Barangay Health Worker Multipurpose Cooperative, and the Abbuyog Medical Assistance Fund (Tanudan BHW Funds) were organized. Chiefs of the hospitals underscored the need to evaluate the policy of remitting their income to the province and instead retain the funds as incentive for hospi-tals and to augment the provincial budget allocation. The hospital’s income can be directly plowed back for improvements. Human Resources. The staff in hospitals and health centers, including devolved personnel, have received the salaries according to the Magna Carta and salary standardization policies, except that certain benefits like the hazard pay have not been released due to shortage of funds. For the Lin-awa Zone, there has been a sharing of human resources during medical missions, and in the case of the Tanudan Municipal Hospital, the municipal health officer has rendered services to assist the chief of the hospital. The Sanggunian Panlalawigan also authorized the setting up of a Health Human Resource Management and Development Center at the Office of Health Ser-vices. This will look into health manpower capacities, recruitment, deployment, training and development in an attempt to de-politicize and instead to profession-alize the health staff. Referral System. As pointed out earlier, the referral system does not follow the regular chain because patients choose to go directly to the district hospital and the provincial hospital due to proximity, availability of transportation, and quality of health services. This practice has been reinforced by the hospitals by provid-ing primary health services since there is not much capacity for secondary and tertiary health care services. Moreover, the referral system has not been closely monitored.

39
Health Sector Reform Technical Assistance Project
The situation is addressed by the plan and initial efforts to upgrade provincial and district hospital facilities and capacities and to repair/construct new RHUs and BHS with funds from the ICHSP. By March 2001, the DHB approved the use of a referral tracking system using a form that will supply information to each unit even when the patient skips the chain (Appendix 12- Sustainability Updates). In the same meeting it was decided that the Provincial Health Office allocate some funds be given to the Tanudan Memorial Hospital and Juan M. Duyan Memorial Hospital to support the upgrading of the facilities since the Tanudan and Rizal municipalities do not use the Tabuk- based provincial hospital . This will help motivate the municipalities to remain within the Lin’awa Zone. This will also address the non-utilization of the Kalinga Provincial Hospital by the above- mentioned municipalities as shown in the results of the quick survey. Management and Information System. Information about the referral chain has not been widely disseminated to the health personnel and community. There has been no tight tracking of patients' movement to and from the referral hospital until March 2001 where the District Health Board, during the said meeting, adopted a new referral form and system for the Lin’awa Zone. Information has also been lacking about the services offered at different levels of the referral system. As mentioned, a new tracking form was designed for the referral system and will be effective by March 2001. The database for health personnel will also be done by the newly organized Health Human Resource Management Center.
2.5 Community Participation The Sinangpad is a federation of non-government organizations linked to the ICHSP. There are 24 enlisted NGOs involved in different programs for health in Kalinga Province (Appendix 14-Sinangpad). The ICHSP prepared and used the NGO/PO Profile Form to gather information on the NGOs’ activities; the Capabil-ity Assessment Tool to assess the NGOs’ strengths and weaknesses; and the Self-Awareness Questionnaire to determine the NGOs’ skills in undertaking community health development work. NGO representatives attended meetings called for by the ICHSP, the Provincial Health Board, and the District Health Boards. Through the Small Grant Schemes of ICHSP, NGOs were selected, based on proposals they submitted, to work on specific community health projects with funding from AUSAID. In specific sites, the NGOs carried out projects such as school based community health contests, health promotion approaches, Botika sa Barrio, Family Planning and Reproductive Health, medical and dental missions, community organizing and mobilization, Information-Education Campaigns, and preparation of a community health plan. The Ausaid areas are the sites where the Small Grant Scheme has been applied on projects. These are Lubuagan, Balbalan, Tanu-dan, Tabuk, Pasil, and Tinglayan.
40
Health Sector Reform Technical Assistance Project
3. ILHZ Gains and Challenges In two years, modest gains can be observed in the Lin-awa zone, particularly in terms of the following: • Indigenization of the concept and approach indicating a sense of ownership
by the province, and sensitivity to cultural, geographic, socio-political fac-tors;
• Proactive creativity for modeling alternative district health zones and systems; • Integration of health and political systems through the functionality of the
District Health Board and the Expanded Provincial Health Board, despite the slow pace of conducting meetings and implementing district health zone poli-cies and plans, not only within levels of government within the province (inter municipal, vertical municipal and provincial, inter provincial levels of govern-ment);
• Integration of health services through the referral system, despite the break in
the chain; thereby, raising issues on the very nature of the referral system and its adaptation to local constraints of geography, topography, terrain, mul-tiethnicity, and multicultural conditions in the province or sites;
• Linkages with non-government organizations within the province and exter-
nal funding organizations through the Department of Health at national and regional levels for the support systems to institutional the district health sys-tem;
• Political Commitment of local leadership with the corollary funding support,
even if the amounts may not fully cover all costs; • Resource sharing within the bounds of the legal and financial system of
government; • Implementation of support systems, such as the health human resources
management center, health financing cooperatives (cooperative pharmacy, community based health financing) for the operationalization of the district health system;
• Driving force and advocacy of the Provincial Health Office (Provincial Health
Officers) through periods of political uncertainties and constraints to initiate, implement, expand, and sustain the inter-local health zones;

41
Health Sector Reform Technical Assistance Project
IV Analysis: Best Practices,
Strengths and Weaknesses 1. Best Practices Kalinga Province is an example of the best practices in: • Local adaptation, modeling, and indigenization of the WHO and the DOH
models as seen in the clustering of municipalities and the referral system. • Implementation of integrated support systems to institutionalize the district
health system through collaboration with the DOH at the national level, the RHO at the regional level, and external funding organizations.
• Health planning and development that takes serious account of local geog-
raphy, terrain, and culture. • Financing the Indigency Program in cooperation with Phil Health to give
people access to health care and help sustain the district health system; community based health financing through cooperatives.
• Driving force and advocacy of the Provincial Health Office (Provincial Health
Officers) through periods of political uncertainties and constraints to initiate, implement, expand, and sustain the inter-local health zones.
2. Strengths and Weaknesses However, the system is not without its weaknesses and strengths, success and failures. Specifically, the Lin-awa District Health Zone has faced difficulties in its early stages at the Lin-awa zone. These were:
• The uncertainties about the local executive’s authority at the provincial level
stalled the process of implementation. • The rotation of mayors as co-chairs of the District Health Board has not
optimized the work of the zone because local executives have not attended meetings.

42
Health Sector Reform Technical Assistance Project
• One weak area in the system pertains to the vague and unclear roles of the DOH representative and therefore the gaps in performance of monitoring and liaison related to the district health system.
• The District Health Board and the Provincial Health Board moved fast at the
beginning but slowed down by the early part of the next year of operation, with the medical and health staff of health centers and the hospitals as the more consistent in pursuing the work of the zone.
• Hospitals were not prepared to provide the secondary and tertiary level of
health care that it was expected to do for the zone and in fact were down-graded.
• The most important and crucial issue consists in the very nature of the
geography, terrain, culture of Kalinga Province that most be understood more deeply for better interventions in structure, policies, plans, and pro-grams.
3. Patterns and Lessons for Sustainability and Replication Given the short time, the case study is useful to discern positive patterns and lessons for sustainability and replication, such as the following. • The referral system is taking place despite the fact that this is not the ex-
pected and normal chain that starts from the BHS, to the RHU, to the District, and to the Provincial Hospital by the very nature of the terrain, inadequate transportation and road networks.
• Hospitals are undergoing upgrading processes for capacity building, to do its
part in the referral system. • There are structures in place—the Provincial Health Board and the District
Health Board, that wait to be reinforced and strengthened to carry its func-tions ably.
The provincial health officers have acted as the driving force for the operationali-zation of the district health system. Upon debriefing for this case study, they immediately moved to convene the Lin-awa Zone District Health Board to address the problems raised. In its meeting of March 8, 2001, the board decided on the measures to sustain the Lin-awa zone. At this point, the recent (March 8, 2001) policies, actions, and agreements among the DHB members can be considered as sustainability measures since by these the threats have been overcome and the continuance of the Lin-awa is assured. : • The DHB will implement the policy that three (3) mayors shall be Co-Chairs of
the DHB and meetings shall be hosted and presided on rotation by the re-spective mayors. The regular meeting is every 3rd Thursday of the 1st month

43
Health Sector Reform Technical Assistance Project
of each quarter. The MHO and staff will be the Secretariat and responsible for logistics.
• The DHB will be constituted to include the SP on health of the province and
the SB on health, MPDO, NGO reps, MHOs, COHs, DOH representatives in Tabuk, Tanudan, Rizal. The functions will operate as revised during this March 8, 2001 meeting.
• Schedules will be followed for performance review in 2nd week of December
and submission of health plan for the next year is every July, while district health plans to be done every September. Calendar of activities was set within a year for presentation of annual health plans, finalization of annual district plans and performance review.
• A Trust Fund will be established with contribution by each established RHU of
P100,000/year; the hospital of P100,000/year; and core referral hospital of P200,000/year.
• Project proposals will be submitted for approval and funding by the DHB. • Each health facility will develop health care financing. • A unified referral system will be adopted in the zone and the staff will be
oriented in a seminar. • Health personnel in Lin-awa shall participate in activities during calamity,
disaster, and epidemics within the zone.

44
Health Sector Reform Technical Assistance Project
V Conclusions and
Recommendations The strategic value added of the IHLZ lies in the fact that it has “re-integrated” the health system after the adverse effects of devolution have been undeniably determined and the complexities of devolution have been somehow understood. It may be viewed as a creative approach that stands validation in Philippine setting, particularly in Kalinga, where conditions are different from the rest of the Philippines. Kalinga belongs to the Cordillera Administrative Region, the formation of which is an indication of its critical role in national and regional political and administrative integration and development. The three models can be examined for replication when conditions in other sites parallel those in the respective zones. Lin-awa Zone is a model for contiguous lowland municipalities. Chico River District is an inter-province model; Bumil-gan (Balbalan) District is a case of a vertical model between municipality and province. These two are for mountainous areas, and where transportation and road links are weak such that a contiguous model will not apply. Finally, the Kalinga case raises the following policy issues: • The unilinear referral chain that cannot be observed during transition period
where hospitals are upgrading and patients prefer to go to facilities based on accessibility, location , culture , services and capacities of the health facility.
• To upgrade hospitals raised the issue of revenue retention, from income
derived from their services • With respect to the Provincial Health Board and the District Health Board, the
issue of leadership presents the options favoring the health officials than po-litical leaders in the position of chair; and
• On health financing, the legal aspects of LGU budget allocation and resource
generation must be explored to fund the health zones In a macro scale, the Kalinga experience can be explored when considering the local health zone component of the Health Sector Reform Agenda. The per-formance of the health sector under devolution hinges on the synergy of health stakeholders in the local health system and in convergence zones to counter-act

45
Health Sector Reform Technical Assistance Project
the fragmentation in the early years of devolution. There is a need to bring down health objectives from the national to the local level in a coordinated and inte-grated way, as well as, to pool resources and capacities of various stake-holders. The Kalinga experience can be compared with the other cases to extract a more general pattern of how local health systems can achieve positive results for the people’s health. It has made possible the linkages of the national, regional, and local government units and within its jurisdiction, the integration of public health units and hospitals. Given this take-off and its results, the inter-local health system or district health system can be optimized. Policies, even legislative action, can ensure that the gains will be pursued.

46
Health Sector Reform Technical Assistance Project
References Compilation of Papers, Provincial Models and Reference Materials on the District
Health System. Management Sciences for Health-Health Sector Reform Technical Assistance Project, August 1999.
Frerichs RR, Tar Tar K. “Computer-Assisted Rapid Surveys in Developing
Countries.” Public Health Reports 1989: 104(1): 14-23. __________. “Use of Rapid Survey Methodology to Determine Immunization
Coverage in Rural Burma.” Journal of Tropical Pediatrics 1988: 34: 125-130. The Best of Health 2000. Integrated Provincial Health Office, Province of South
Cotabato, July 2000. Establishing the Inter Local Health System in South Cotabato. Integrated Com-
munity Health Services, an Australian AID-assisted Project, April 2000. A Project Status Report. South Cotabato. Integrated Community Health Ser-
vices, an Australian AID-assisted Project, December 2000. Kalumba K. Towards an Equity-Oriented Policy of Decentralization in Health
Systems Under Conditions of Turbulence: The Case of Zambia. Geneva: World Health Organization.
1995 Census of Population, Report No. 2 – 83-K (South Cotabato) Socio Eco-
nomic and Demographic Characteristics. Manila: National Statistics Office, March 1997.
1995 Census of Population, Report No. 1 – K (Southern Mindanao) – Population
by Province, City/Municipality and Barangay. Manila: National Statistics Of-fice, August 1996.
Local Health Systems in the Americas: An Ongoing Social Strategy. Pan Ameri-
can Health Organization, World Health Organization, 1993. Strengthening the Implementation of Local Health Systems. Pan American
Health Organization, World Health Organization and W.K Kellogg Founda-tion, 1992.
Van Lerbergh, W. and Lafort, Y. The Role of the Hospital in the District: Deliver-
ing or Supporting Primary Health Care? Geneva: World Health Organization, [n.d.].
District Health Facilities: Guidelines for Development and Operations. World
Health Organization, Regional Publications, Western Pacific Series No. 22, 1998.
The Role of Local Government in Health: Comparative Experiences and Major
Issues. World Health Organization, South Cotabato, 1997.

47
Health Sector Reform Technical Assistance Project
Glossary Core Referral Hospital. The term core referral hospital indicates the main hospital for an ILHZ and its catchment population. Such hospital is the main point of referral for hospital services from the community, private medical practi-tioners, and public health services at Barangay Health Stations (BHS) and Rural Health Units (RHU). The minimum services provided at a core referral hospital include outpatient services, laboratory and radiological diagnostic services, inpatient care, and surgical services sufficient to provide emergency care for basic life threatening conditions, obstetrics and trauma. Referrals to and from the core referral hospital are managed in accordance with a referral system that delineates the levels of diagnostic, surgical and medical services appropriate for the referral hospital and the other health service provid-ers in the ILHZ. In most cases, the core referral hospitals are private sector facilities. (AusAID) District Health System. The World Health Organization defines the District Health System as “a more or less contained segment of the national health system which comprises a well defined administrative and geographic area either rural or urban and al institutions and sectors whose activities contribute to improve health”. It is subdivided into three levels of referral namely primary (barangay health stations and rural health units), secondary (district hospitals) and tertiary (Regional hospitals) that have distinct yet complementary functions. Inter Local Health Zone (ILHZ) and Inter Local Health System (ILHS). The ILHZ is the nationally endorsed unit for local health service management and delivery in the Philippines. This system is inspired by the concept of the District Health System (DHS), a generic term developed by the WHO to describe an integrated health management and delivery system based on defined administrative and geographical area known as health districts. The DHS has been applied in many developed and developing countries throughout the world, primarily in countries where responsibility for health services has been decentralized from national to local health authorities. In post-devolution Philippines, “health districts” have been variously referred to as Inter-Local Health Districts (ILHD), Local Area Health Development Zones (LADHZ) and Area Health Zones (AHZ). At the national level, EO No. 205 of January 2000 established Inter-Local Health Zones (ILHZ) throughout the Philippines. The component parts of an ILHZ are connected through health service manage-ment, delivery and referral systems. When all ILHZs within a province are linked together they form the basis of the province-wide ILHS. Despite local variations in name, the overall concept remains constant: creation of an ILHS by clustering municipalities into ILHZs. Each ILHZ has a defined population within a defined geographical area and comprises a central (or “core”) referral hospital and a number of primary level facilities such as RHUs and BHS.
48
Health Sector Reform Technical Assistance Project
In addition to government health services ILHZs are inclusive of all other stake-holders and sectors involved in the delivery of health services or the promotion of health, including community-based NGOs and the private health sector. (AusAID) Health Covenant 1999. The Health Covenant between the Department of Health, League of Provinces of the Philippines, the Department of Interior and Local Government and the Union of Local Authorities in the Philippines was forged in a workshop. ILHZ, DHS. Philippines National Assembly referred to this as ILHDs. In post devolution, Philippines refers to “both districts.” EO 205 of 2000 provides for the establishment of IHLZ, this made it a national strategy. ILHZ Board. Establishment of ILHZ has facilitated linkages between municipal and provincial decision-making bodies through the broad membership of ILHZ boards. The main purpose of ILHZ board is to facilitate inter-LGU cooperation and coordination. (AusAID) Referral System. It is a set of activities undertaken by the health care provider or facility in response to its inability to provide the necessary intervention to a patient’s need. It is done from the community to the Rural Health Unit, from the Rural Health Unit to the hospital and within the hospital internal system and vice versa. It involves not only direct patient care but also support services such as transportation to transfer patients from one health facility to another. Also communication systems need to be established among different facilities. Sanggunian. The sanggunian is the legislative branch of local government units while the governor/mayors] represent the executive branch. The sanggunian panlalawigan is the provincial legislative assembly and at the municipal level, the sanggunian bayan is the legislative body. Every sanggunian has a committee on health and the chairperson is a member of the municipality or provincial local health board.
49
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
List of Appendices Appendix 1. Sources of Data. ........................................................................... 50
Appendix 2. List of FGD and KII Participants in Kalinga. .................................. 52
Appendix 3. Sampling Frame for Kalinga.......................................................... 55
Appendix 4. Area Maps. ................................................................................... 56
Appendix 5. Mandates and Memorandums of Agreement. ............................... 57
Appendix 6. Organizational Structure. ............................................................... 58
Appendix 7. Site Characteristics. ....................................................................... 63
Appendix 8. Health Indices. ............................................................................... 67
Appendix 9. Quick Survey Results..................................................................... 81
Appendix 10. Integrated Community Health Service Project............................ 101
Appendix 11. Kalinga Milestones in IHLZ Development................................... 102
Appendix 12. Sustainability Interventions. ....................................................... 106
Appendix 13. Ambigatton Multi-purpose Cooperative. .................................... 107
Appendix 14. Non-Government Organization – Sinangpad.............................. 108

50
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 1. Sources of Data. 1) Provincial Government
• Annual Accomplishment Reports – 1993, 1994, 1996, 1997, 1999 • Mid-Term Provincial Development Plan 1993-1998 • Mid-Term Provincial Development Plan 1999-2000 • Organizational Structure (HMRO file) • Provincial Staffing (HMRO file) • Provincial Income, Budget and Allotment for Health – 1993-2001
2) Provincial Health Office
• Integrated Annual Provincial Health Plan Volume II • Individual RHU Catch Up Plan for 2000 • Provincial Health Annual Report for 2000 • Kalinga Provincial Strategic Plan for 2001-2005 • RHU Operational Plan for 2001 • Provincial Health Plan for 2001 • District Hospital Plan for 2001 • Mortality Surveillance, Leading Causes of Mortality, 1991-2000 • Vital Statistics – 1996-1999 • Morbidity Surveillance, Disease Occurrences, 1995-2000 • Hospital Staffing • Sangguniang Panlalawigan Resolution 2000-301 on establishment of
HHRMDC • DOH Administrative Order No. 9-A series 1999 • Articles of Cooperation of Ambigatton Multi-Purpose Cooperative • ICHSP Maps of Kalinga and the different Health Facilities • Health Journal: Chico River Health District • Program Appropriation by Object, Local Budget Preparation Form 152 • PHIC document on status of Indigent Program in Kalinga
3) Kalinga Provincial Hospital
• Hospital Statistical Reports- 1990- June 2000 • Hospital Organizational Chart • Kalinga Provincial Hospital Work and Financial Plan 1999
4) Integrated Community Health Services Project Office
• ICHSP brochure • Mid- Term Review Report for 2000
5) Lina-wa Zone
• Lina-wa Report • Memorandum of Agreement • Minutes of Meeting • List of SINAGPAD NGOs • Minutes of SINAGPAD Meetings

51
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
6) Tanudan Municipality Data • Budget –1996- 2001 • 2001 PhilHealth Contribution
7) Tabuk Municipality Data
• Organizational Structure of RHUs • Catchment Areas • Executive Summary of the Accomplishment Report 1999 • Profile of Tabuk • Development Plan 1999-2004
8) Rizal Municipality Data
• Medium Term Plan 1999-2004 • Vital Statistics- 1996-2000 • Budget- 1993-2001 • PhilHealth Contributions for 2001 • Annual Report 1997 • Juan Duyan District Hospital Services
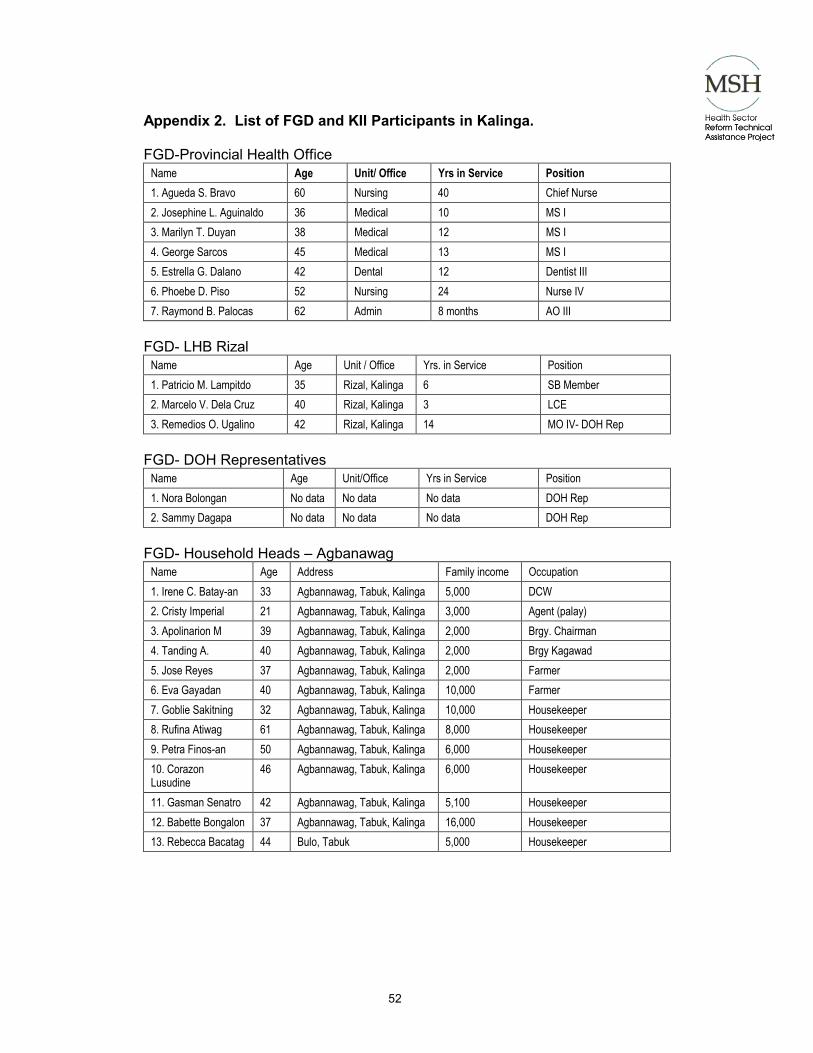
52
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 2. List of FGD and KII Participants in Kalinga. FGD-Provincial Health Office
Name Age Unit/ Office Yrs in Service Position 1. Agueda S. Bravo 60 Nursing 40 Chief Nurse 2. Josephine L. Aguinaldo 36 Medical 10 MS I 3. Marilyn T. Duyan 38 Medical 12 MS I 4. George Sarcos 45 Medical 13 MS I 5. Estrella G. Dalano 42 Dental 12 Dentist III 6. Phoebe D. Piso 52 Nursing 24 Nurse IV 7. Raymond B. Palocas 62 Admin 8 months AO III
FGD- LHB Rizal
Name Age Unit / Office Yrs. in Service Position 1. Patricio M. Lampitdo 35 Rizal, Kalinga 6 SB Member 2. Marcelo V. Dela Cruz 40 Rizal, Kalinga 3 LCE 3. Remedios O. Ugalino 42 Rizal, Kalinga 14 MO IV- DOH Rep
FGD- DOH Representatives
Name Age Unit/Office Yrs in Service Position 1. Nora Bolongan No data No data No data DOH Rep 2. Sammy Dagapa No data No data No data DOH Rep
FGD- Household Heads – Agbanawag
Name Age Address Family income Occupation 1. Irene C. Batay-an 33 Agbannawag, Tabuk, Kalinga 5,000 DCW 2. Cristy Imperial 21 Agbannawag, Tabuk, Kalinga 3,000 Agent (palay) 3. Apolinarion M 39 Agbannawag, Tabuk, Kalinga 2,000 Brgy. Chairman 4. Tanding A. 40 Agbannawag, Tabuk, Kalinga 2,000 Brgy Kagawad 5. Jose Reyes 37 Agbannawag, Tabuk, Kalinga 2,000 Farmer 6. Eva Gayadan 40 Agbannawag, Tabuk, Kalinga 10,000 Farmer 7. Goblie Sakitning 32 Agbannawag, Tabuk, Kalinga 10,000 Housekeeper 8. Rufina Atiwag 61 Agbannawag, Tabuk, Kalinga 8,000 Housekeeper 9. Petra Finos-an 50 Agbannawag, Tabuk, Kalinga 6,000 Housekeeper 10. Corazon Lusudine
46 Agbannawag, Tabuk, Kalinga 6,000 Housekeeper
11. Gasman Senatro 42 Agbannawag, Tabuk, Kalinga 5,100 Housekeeper 12. Babette Bongalon 37 Agbannawag, Tabuk, Kalinga 16,000 Housekeeper 13. Rebecca Bacatag 44 Bulo, Tabuk 5,000 Housekeeper
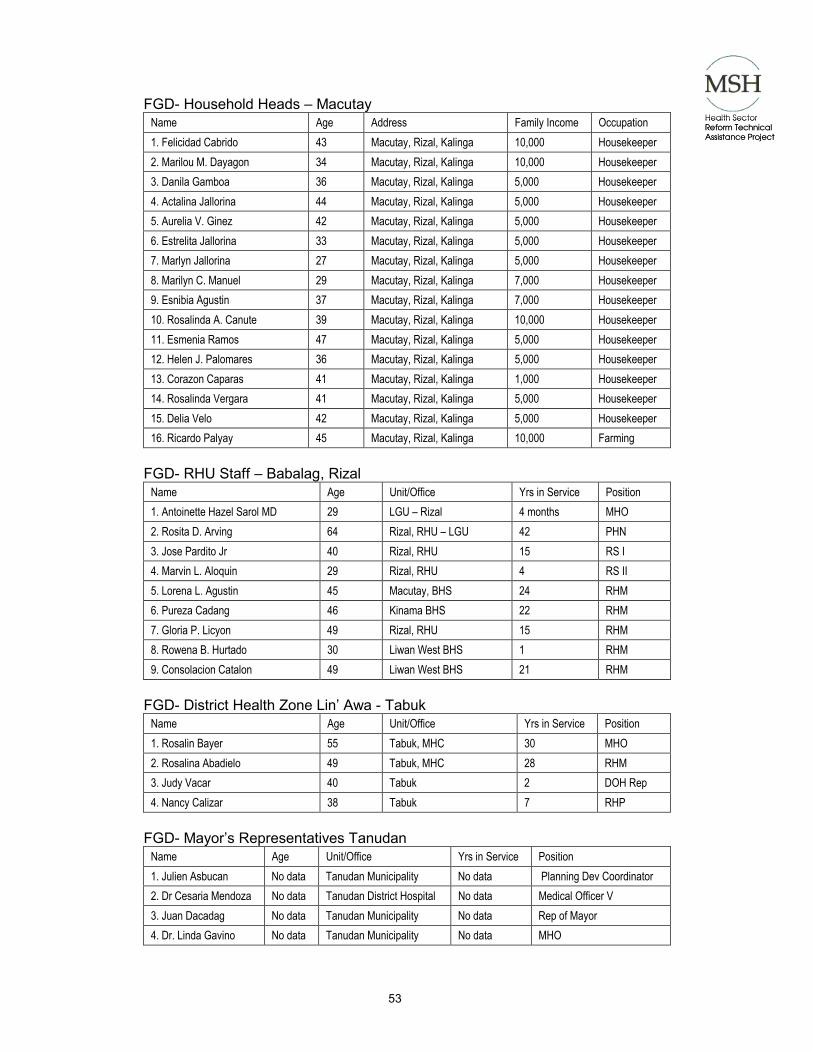
53
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
FGD- Household Heads – Macutay Name Age Address Family Income Occupation 1. Felicidad Cabrido 43 Macutay, Rizal, Kalinga 10,000 Housekeeper 2. Marilou M. Dayagon 34 Macutay, Rizal, Kalinga 10,000 Housekeeper 3. Danila Gamboa 36 Macutay, Rizal, Kalinga 5,000 Housekeeper 4. Actalina Jallorina 44 Macutay, Rizal, Kalinga 5,000 Housekeeper 5. Aurelia V. Ginez 42 Macutay, Rizal, Kalinga 5,000 Housekeeper 6. Estrelita Jallorina 33 Macutay, Rizal, Kalinga 5,000 Housekeeper 7. Marlyn Jallorina 27 Macutay, Rizal, Kalinga 5,000 Housekeeper 8. Marilyn C. Manuel 29 Macutay, Rizal, Kalinga 7,000 Housekeeper 9. Esnibia Agustin 37 Macutay, Rizal, Kalinga 7,000 Housekeeper 10. Rosalinda A. Canute 39 Macutay, Rizal, Kalinga 10,000 Housekeeper 11. Esmenia Ramos 47 Macutay, Rizal, Kalinga 5,000 Housekeeper 12. Helen J. Palomares 36 Macutay, Rizal, Kalinga 5,000 Housekeeper 13. Corazon Caparas 41 Macutay, Rizal, Kalinga 1,000 Housekeeper 14. Rosalinda Vergara 41 Macutay, Rizal, Kalinga 5,000 Housekeeper 15. Delia Velo 42 Macutay, Rizal, Kalinga 5,000 Housekeeper 16. Ricardo Palyay 45 Macutay, Rizal, Kalinga 10,000 Farming
FGD- RHU Staff – Babalag, Rizal
Name Age Unit/Office Yrs in Service Position 1. Antoinette Hazel Sarol MD 29 LGU – Rizal 4 months MHO 2. Rosita D. Arving 64 Rizal, RHU – LGU 42 PHN 3. Jose Pardito Jr 40 Rizal, RHU 15 RS I 4. Marvin L. Aloquin 29 Rizal, RHU 4 RS II 5. Lorena L. Agustin 45 Macutay, BHS 24 RHM 6. Pureza Cadang 46 Kinama BHS 22 RHM 7. Gloria P. Licyon 49 Rizal, RHU 15 RHM 8. Rowena B. Hurtado 30 Liwan West BHS 1 RHM 9. Consolacion Catalon 49 Liwan West BHS 21 RHM
FGD- District Health Zone Lin’ Awa - Tabuk
Name Age Unit/Office Yrs in Service Position 1. Rosalin Bayer 55 Tabuk, MHC 30 MHO 2. Rosalina Abadielo 49 Tabuk, MHC 28 RHM 3. Judy Vacar 40 Tabuk 2 DOH Rep 4. Nancy Calizar 38 Tabuk 7 RHP
FGD- Mayor’s Representatives Tanudan
Name Age Unit/Office Yrs in Service Position 1. Julien Asbucan No data Tanudan Municipality No data Planning Dev Coordinator 2. Dr Cesaria Mendoza No data Tanudan District Hospital No data Medical Officer V 3. Juan Dacadag No data Tanudan Municipality No data Rep of Mayor 4. Dr. Linda Gavino No data Tanudan Municipality No data MHO
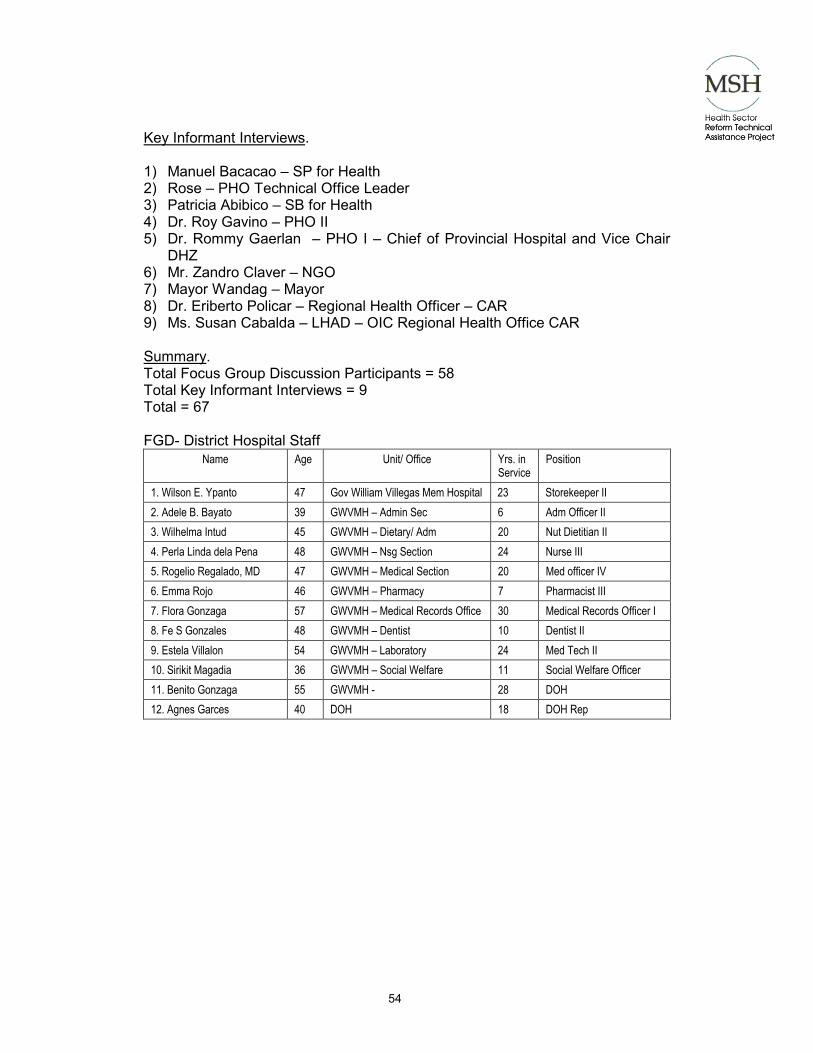
54
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Key Informant Interviews. 1) Manuel Bacacao – SP for Health 2) Rose – PHO Technical Office Leader 3) Patricia Abibico – SB for Health 4) Dr. Roy Gavino – PHO II 5) Dr. Rommy Gaerlan – PHO I – Chief of Provincial Hospital and Vice Chair
DHZ 6) Mr. Zandro Claver – NGO 7) Mayor Wandag – Mayor 8) Dr. Eriberto Policar – Regional Health Officer – CAR 9) Ms. Susan Cabalda – LHAD – OIC Regional Health Office CAR Summary. Total Focus Group Discussion Participants = 58 Total Key Informant Interviews = 9 Total = 67 FGD- District Hospital Staff
Name Age Unit/ Office Yrs. in Service
Position
1. Wilson E. Ypanto 47 Gov William Villegas Mem Hospital 23 Storekeeper II 2. Adele B. Bayato 39 GWVMH – Admin Sec 6 Adm Officer II 3. Wilhelma Intud 45 GWVMH – Dietary/ Adm 20 Nut Dietitian II 4. Perla Linda dela Pena 48 GWVMH – Nsg Section 24 Nurse III 5. Rogelio Regalado, MD 47 GWVMH – Medical Section 20 Med officer IV 6. Emma Rojo 46 GWVMH – Pharmacy 7 Pharmacist III 7. Flora Gonzaga 57 GWVMH – Medical Records Office 30 Medical Records Officer I 8. Fe S Gonzales 48 GWVMH – Dentist 10 Dentist II 9. Estela Villalon 54 GWVMH – Laboratory 24 Med Tech II 10. Sirikit Magadia 36 GWVMH – Social Welfare 11 Social Welfare Officer 11. Benito Gonzaga 55 GWVMH - 28 DOH 12. Agnes Garces 40 DOH 18 DOH Rep
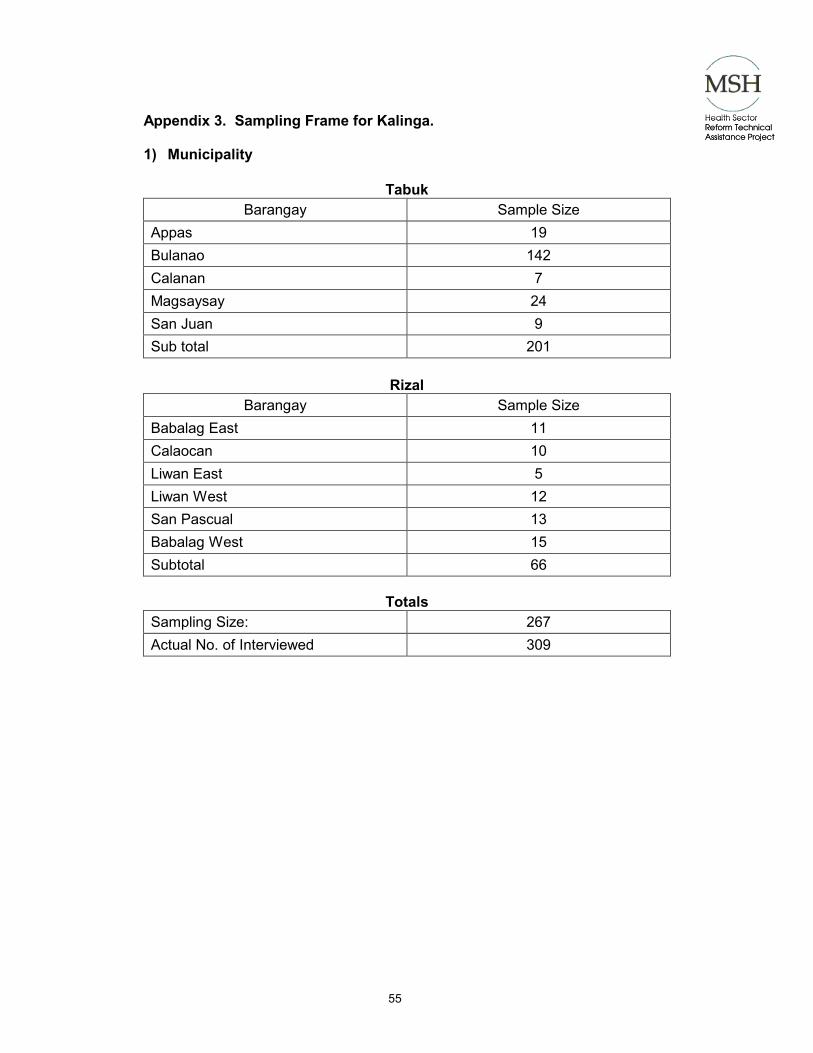
55
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 3. Sampling Frame for Kalinga. 1) Municipality
Tabuk Barangay Sample Size
Appas 19 Bulanao 142 Calanan 7 Magsaysay 24 San Juan 9 Sub total 201
Rizal
Barangay Sample Size Babalag East 11 Calaocan 10 Liwan East 5 Liwan West 12 San Pascual 13 Babalag West 15 Subtotal 66
Totals
Sampling Size: 267 Actual No. of Interviewed 309
56
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 4. Area Maps. (Note: available in hardcopy only.) 4-1. Lin-awa Zone in Kalinga 4-2. Catchment Municipalities in Kalinga 4-3. Lin-awa Zone, Chico River district and Balbal-an District Network of Health
Facilities

57
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 5. Mandates and Memorandums of Agreement. (Note: Available in hardcopy only.) 5-1. Executive Order 205. 5-2. Lin-awa Zone Memorandum of Agreement. 5-3. Chico River Memorandum of Agreement. 5-4. Sangguniang Panlalawigan Resolution No. 2000-301.

58
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 6. Organizational Structure.
6-1. Lin-awa.
6-2. Lin-awa District Health Board.
Kalinga Provincial Hospital
Municipality of TabukMunicipal Health Office
Municipality of TanudanMunicipal Health Office
Municipality of RizalMunicipal Health Office
Lin’awa Zone Health Board
BHS BHS BHS BHS BHS BHS BHS BHS BHS
RHU RHU RHU RHU RHU
Kalinga Provincial Hospital
Municipality of TabukMunicipal Health Office
Municipality of TanudanMunicipal Health Office
Municipality of RizalMunicipal Health Office
Lin’awa Zone Health Board
BHS BHS BHS BHS BHS BHS BHS BHS BHS
RHU RHU RHU RHU RHU
Mayor
Provincial Health Officer
KalingaProvincial Hospital
Chief of Hospital
Juan M DuyanMemorial District
HospitalChief of Hospital
TanudanMunicipal Hospital
Chief of Hospital
Sangguniang Panlalawigan (2)
Sangguniang Bayan Members (2)
NGO Representative
DOH Representative
Mayor
Provincial Health Officer
KalingaProvincial Hospital
Chief of Hospital
Juan M DuyanMemorial District
HospitalChief of Hospital
TanudanMunicipal Hospital
Chief of Hospital
Sangguniang Panlalawigan (2)
Sangguniang Bayan Members (2)
NGO Representative
DOH Representative

59
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
6-3. Tabuk RHU.
6-4. Rizal RHU.
Mayor
Municipal Health Officer
Rural Health Physician I Rural Health Physician II Rural Health Physician III
PHN Dentist RHI
Dental Aide
RHM (5)
BHWs
PHN RHI MT
RHM (7)
BHWs
PHN
RHM (6)
BHWs
RHI
Mayor
Municipal Health Officer
Rural Health Physician I Rural Health Physician II Rural Health Physician III
PHN Dentist RHI
Dental Aide
RHM (5)
BHWs
PHN RHI MT
RHM (7)
BHWs
PHN
RHM (6)
BHWs
RHI
Mayor
Municipal Health Officer
Public Health Nurse Sanitary InspectorSanitary Inspector
Casual MidwifeRomualdez BHS
RHM Kinama
RHM MacutayRHM MHC
RHM Liwan West
RHM Liwan East
Casual MidwifeCalaocan BHS
Mayor
Municipal Health Officer
Public Health Nurse Sanitary InspectorSanitary Inspector
Casual MidwifeRomualdez BHS
RHM Kinama
RHM MacutayRHM MHC
RHM Liwan West
RHM Liwan East
Casual MidwifeCalaocan BHS

60
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
6-5. Provincial Hospital.
Provincial Health Officer 2
Provincial Health Officer 1
Medical Services
Nursing Services
Admin & SupportServices
Technical Section
MS 3
MS 2
MO 4
MO 3
MS 2
Dental
Pharmacy
Lab
X-ray
RN 5
RN 4
RN 3
RN 2
RN 1
NA
Utility Worker
Laundry Woman
AO 3
Cashier
RN 2 – NTPCoor.
Record Officer
Storekeeper
Mechanic
Clerks
Security
Carpenter
Driver
NutritionDietician
Soc. Worker 1
Dormitory Mgr
Comm.Equip. Oprtr 2
Record Officer
Clerk
Clerk
Clerk
Clerk
MO 4
RN 4 EPI
RN 2 NTP
Nutri.Coor 2
FHSISCoor.
N/D 4
MW 4 FP
RN 1CORECOLDCHAINCoor.
SI 4 CDD
RN 1Prev
Nephro
Hepo 1
Source: Kalinga Hospital Nursing Service.
Provincial Health Officer 2
Provincial Health Officer 1
Medical Services
Nursing Services
Admin & SupportServices
Technical Section
MS 3
MS 2
MO 4
MO 3
MS 2
Dental
Pharmacy
Lab
X-ray
RN 5
RN 4
RN 3
RN 2
RN 1
NA
Utility Worker
Laundry Woman
AO 3
Cashier
RN 2 – NTPCoor.
Record Officer
Storekeeper
Mechanic
Clerks
Security
Carpenter
Driver
NutritionDietician
Soc. Worker 1
Dormitory Mgr
Comm.Equip. Oprtr 2
Record Officer
Clerk
Clerk
Clerk
Clerk
MO 4
RN 4 EPI
RN 2 NTP
Nutri.Coor 2
FHSISCoor.
N/D 4
MW 4 FP
RN 1CORECOLDCHAINCoor.
SI 4 CDD
RN 1Prev
Nephro
Hepo 1
Source: Kalinga Hospital Nursing Service.

61
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
6-6. Provincial Health Board.
Governor
Provincial Health Officer II
Chief of CO-Referral Hospitals
Juan Duyan Memorial Hospital Tanudan Municipal Hospital
NGO Rep DOH Rep
Sangguniang PanlalawiganChair of Committee on Health
Sangguniang Bayan Members (3)Chair of Committee on Health
Provincial Health Team Leader

62
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
6-7. Provincial Government.

63
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 7. Site Characteristics.
7-1. Land Area by Municipality, 1995. Province/ Municipality Land Area (sq. km.) % Distribution
Kalinga 3,119.4 100.0 Balbalan 550.0 17.63 Lubuagan 329.5 10.56 Pasil 188.0 6.03 Pinukpuk 694.1 22.25 Rizal 177.5 5.69 Tabuk 641.7 20.57 Tanudan 349.1 11.19 Tinglayan 189.5 6.06
Source: Provincial Medium Term Development Plan, 1999-2004.
7-2. Population by Municipalities, Kalinga 1990 and 1995. Province/ Municipality 1995 Annual Average Growth Rate % Distribution (1995 Pop’n)
Kalinga 154,145 2.23 100.0 Balbalan 11,742 2.77 7.62 Lubuagan 9,897 1.40 6.42 Pasil 8,935 3.15 5.80 Pinukpuk 23,057 2.60 14.95 Rizal 12,173 2.12 7.90 Tabuk 63,507 1.98 41.20 Tanudan 11,243 3.57 7.29 Tinglayan 13,591 1.37 8.82
Source: Provincial Medium Term Development Plan, 1999-2004.
7-3. Population Density by Municipality, Kalinga, 1995. Province/ Municipality Total Population in 1995 Population Density
Kalinga 154,145 50 Balbalan 11,742 21 Lubuagan 9,897 30 Pasil 8,935 47 Pinukpuk 23,057 33 Rizal 12,173 68 Tabuk 63,507 98 Tanudan 11,243 32 Tinglayan 13,591 71
Source: Provincial Medium Term Development Plan, 1999-2004.

64
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
7-4. Total Population by Age Group and Percent Distribution Kalinga, 1990 and 1995.
1990 1995 Age Group
Number % Dist. Number % Dist. Growth Rate # of Persons
Under 1 year Old 4853 3.54 4686 3.04 0.65 1-14 Year Old 53367 38.94 58418 37.9 1.71 15-64 Year Old 74722 54.51 86013 55.81 2.68 65 & Over 4132 3.01 5010 3.25 3.68 Total 137074 100.00 154145 100.00 2.23 Source: Provincial Medium Term Development Plan 1999-2004
7-5. Population Growth Rate by Sex and by Municipality Kalinga, 1990-1995. 1990 1995 Growth Rate Province/
Municipality Total Male Female Total Male Female Male Female
KALINGA 137074 69760 67314 154145 78817 75328 2.32 2.13
Balbalan 10149 5225 4924 11742 6088 5654 3.91 2.63
Lubuagan 9190 4700 4490 9897 5113 4789 1.59 1.22
Pasil 7573 3846 3727 8935 4546 4389 3.19 3.12
Pinukpuk 20105 10328 9777 23057 11895 11162 2.69 2.52
Rizal 10886 5607 5279 12173 6256 5917 2.08 2.16
Tabuk 57208 29011 28197 63507 32420 31087 2.11 1.85
Tanudan 9324 4718 4606 11243 5674 5569 3.52 3.63
Tinglayan 12639 6325 6314 13591 6825 6766 1.44 1.31 Source: Provincial Medium Term Development Plan 1999-2004
7-6. Local Government Income, Provincial Government of Kalinga 1996-1997. Sources of Income 1996 1997 Growth Rate % Distribution 1997
Local Income 9,089,593.65 8,996,123.40 1.03 6.13 Property Taxes 444,702.60 475,735.20 3.43 Taxes on Goods and Services 470,045.46 660,799.67 18.57 Operating and Miscellaneous Income 8,174,845.59 7,848,530.83 2.02 Capital Revenue 1,945 11,057.70 IRA 104,537,919.00 137,854,590.54 31.87 93.87 Total 113,627,512.70 146,850,713.90 29.24 100.00 Source: Annual Report, Provincial Government of Kalinga, 1997

65
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
7-7. Local Government Expenditure by Object, Kalinga, 1996-1997. Object of Expenditure 1996 1997 Growth Rate % % Distribution 1997
Personnel Services 67,971,267.65 99,034,430.24 45.70 67.92 Maintenance & Other Operating Expenses 34,369,124.69 46,778,861.48 36.10 32.08 Total 102,340,392.30 145,813,219.72 42.48 100.00 Source: Annual Report, Provincial Government of Kalinga, 1997
7-8. Local Government Expenditure by Function, Kalinga, 1996-1997. Expenditure by Function 1996 1997 Growth Rate % Percent Distribution1997
Development Admin. 28,458,901.17 43,425,547.07 23 29.78 Social Services 46,781,242.72 61,290,813.89 12 42.03 Economic Services 35,001,225.88 41,096,930.74 8 28.19 Total 112,241,369.77 145,813,291.72 14 100.00 Source: Provincial Medium Term Development Plan 1999-2004
7-9. Employment Distribution by Major Industry Kalinga, 1995. Industry Number % Distribution
Agriculture, forestry, fishery 47,199 77.88
Manufacturing 736 1.18
Electricity, Gas, Water 53 0.09
Construction 872 1.40
Trade 2,023 3.25
Services 11,294 18.16
Not Stated 23 0.04
Total 62,200 100.00 Source: Provincial Medium Term Development Plan 1999-2004

66
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
7-10. Number of Personnel by Department/Office, Kalinga, 1997. Department/Office # of Regular Employees
Provincial Governor's Office 6
ENR 9
Warden 17
Office of the Vice Governor/Sangguniang Panlalawigan 12
Office of the Provincial Secretary 13
Provincial Administrator's Office 24
Provincial Planning and Development Office 17
General Services Office 68
Provincial Budget office 11
Provincial Accountant 14
Provincial Treasury Office 39
Provincial Attorney's Office 4
Provincial Assessor's Office 25
Provincial Social Welfare and Development Office 8
Provincial Agriculturist's Office 58
Provincial Veterinary Office 19
Provincial Engineering Office 77
Provincial Cooperative and Development Office 4
Provincial Health Office 175
Kalinga District Hospital 57
Western District Hospital 30
Pinukpuk District Hospital 35
Juan M. Duyan District Hospital 39
Tanudan Municipal Hospital 19
TOTAL 780 Source: Provincial Medium Term Development Plan 1999-2004

67
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 8. Health Indices.
8-1. Crude Birth Rate, Crude Death Rate, Infant Mortality Rate and Maternal Mortality Rate, Kalinga, 1995-2000.
Indices 1995 1996 1997 1998 1999 2000
CBR (per 1000 pop'n) 24.54 26.58 22.99 21.8 21.7 22.7
CDR (per 1000 pop'n 2.96 3.29 3.33 3.02 3.27 3.6
IMR (per 1000 LB) 15.79 18.54 19.98 16.16 21.1 19.19
MMR (per 1000 LB) 1.24 1.38 0.54 0.56 1.33 1.02 Source: Provincial Health Office.
8-2. Leading Causes of Maternal Mortality, Kalinga, 1995-2000. 1995 1996 1997 1998 1999 2000
Diseases No. Rate No. Rate No. Rate No. Rate No. Rate No. Rate
Post Partum Hemorrhage 3 0.53 5 1.38 2 0.53 1 0.28 3 0.8 1 0.25
Hypertension 2 0.36
Retained Placenta 1 0.18 1 0.28
RHD 1 0.18
Septicemia 2 0.53
Post Abortion Hemorrhage 1 0.25
Uterine Atony 1 0.25
Sepsis 2ndary to Trauma 1 0.25 Source: Provincial Health Office.
8-3. Leading Causes of Infant Mortality Rate/ 1000 Live Births, Kalinga, 1997. 5 year Average 1997
Diseases No. Rate No. Rate
Pneumonia 31 5.77 14 3.78 Prematurity 4 0.74 9 2.43 Congenital Anomaly 4 0.74 5 1.35 Malaria 10 1.86 3 0.81 Measles 3 0.81 Diarrhea 3 0.81 Congenital Heart Disease 3 0.54 3 0.81 Sepsis Neonatorum 1 0.81 2 0.54
Source: Provincial Medium Term Development Plan, 1999-2004.

68
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-4. Leading Causes Of Mortality Rate/1000 Population, Kalinga, 1997 5 Year Average 1997
Diseases No. Rate No. Rate
Pneumonia 42 69.2 73 44.33 Pulmonary 54 27.13 67 40.68 Hypertension 38 16.93 41 24.89 Accidents 53 26.69 36 21.86 Peptic Ulcer Disease 24 13.4 29 17.61 CVD 64 37.38 29 17.61 Cancer 33 14.7 28 17 Assault 23 12.8 24 14.57 Malaria 39 18.65 17 10.32 Old 12 5.3 11 6.77 Bronchial Asthma 10 6.07
Source: Provincial Medium Term Development Plan, 1999-2004.
8-5. Leading Causes Of Morbidity Rate/1000 Population, Kalinga, 1997 5 Year Average 1997
Diseases No. Rate No. Rate
Bronchitis/ Bronchiolitis 6584 3364.2 5411 3285.67 Malaria 4852 3337.5 4196 2574.89 Diarrhea 5050 2521.4 4004 24.31.31 Pneumonia 4048 1907.3 3602 2187.21 Influenza 2762 1254.6 2311 7 PTB 805 203.8 494 288.97 Measles 448 272.03 Dysentery 107 47.2 308 187.02 Chickenpox 704 228.8 268 163.74 Conjunctivitis 135 65.8 186 112.94 ARI 194 116.1 178 108.08 Diseases of the Heart 84 88.35 169 103.62
Source: Provincial Medium Term Development Plan, 1999-2004.
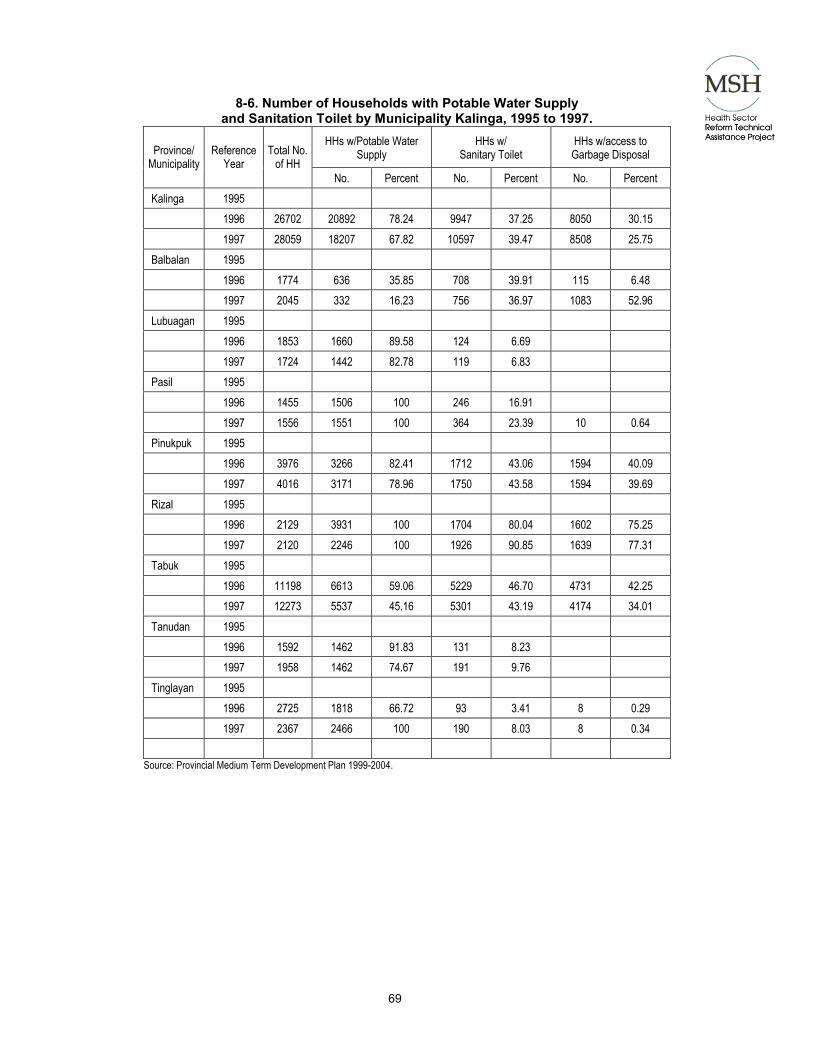
69
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-6. Number of Households with Potable Water Supply and Sanitation Toilet by Municipality Kalinga, 1995 to 1997.
HHs w/Potable Water Supply
HHs w/ Sanitary Toilet
HHs w/access to Garbage Disposal Province/
Municipality Reference
Year Total No.
of HH No. Percent No. Percent No. Percent
Kalinga 1995 1996 26702 20892 78.24 9947 37.25 8050 30.15 1997 28059 18207 67.82 10597 39.47 8508 25.75 Balbalan 1995 1996 1774 636 35.85 708 39.91 115 6.48 1997 2045 332 16.23 756 36.97 1083 52.96 Lubuagan 1995 1996 1853 1660 89.58 124 6.69 1997 1724 1442 82.78 119 6.83 Pasil 1995 1996 1455 1506 100 246 16.91 1997 1556 1551 100 364 23.39 10 0.64 Pinukpuk 1995 1996 3976 3266 82.41 1712 43.06 1594 40.09 1997 4016 3171 78.96 1750 43.58 1594 39.69 Rizal 1995 1996 2129 3931 100 1704 80.04 1602 75.25 1997 2120 2246 100 1926 90.85 1639 77.31 Tabuk 1995 1996 11198 6613 59.06 5229 46.70 4731 42.25 1997 12273 5537 45.16 5301 43.19 4174 34.01 Tanudan 1995 1996 1592 1462 91.83 131 8.23 1997 1958 1462 74.67 191 9.76 Tinglayan 1995 1996 2725 1818 66.72 93 3.41 8 0.29 1997 2367 2466 100 190 8.03 8 0.34
Source: Provincial Medium Term Development Plan 1999-2004.

70
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-7. Hospital Occupancy Rate, Total Admission and Discharge, Total Out-Patient
Attended and Referrals Sent, Kalinga Provincial Hospital, 1990-2000.

71
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-8. Hospital Bed Capacity and Number of Beds per Service,
Kalinga Provincial Hospital 1990-2000. 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Jan.-June 2000
Bed Capacity
Authorized 100 100 100 100 100 100 100 100 100 100 100
Actual/ Implementing 100 100 100 100 100 100 100 100 100 100 100
Type of Service
Medicine 35 35 25 35 30 30 30 30 30 30 30
Pediatrics 35 35 35 35 30 30 30 30 30 30 30
Surgery
a. Pediatrics 5 15 15 15 10 10 10 10 10 10 10
b. Adult 10 15 15 15 15 15 15 15 15 15 15
Obstetrics 10 0 0 0 10 10 10 10 10 10 10
Gynecology 5 0 0 0 5 5 5 0 0 0 0
Newborn 0 0 0 0 0 0 0 5 5 5 5 Source: Kalinga Provincial Hospital Annual Reports, 1990-2000.
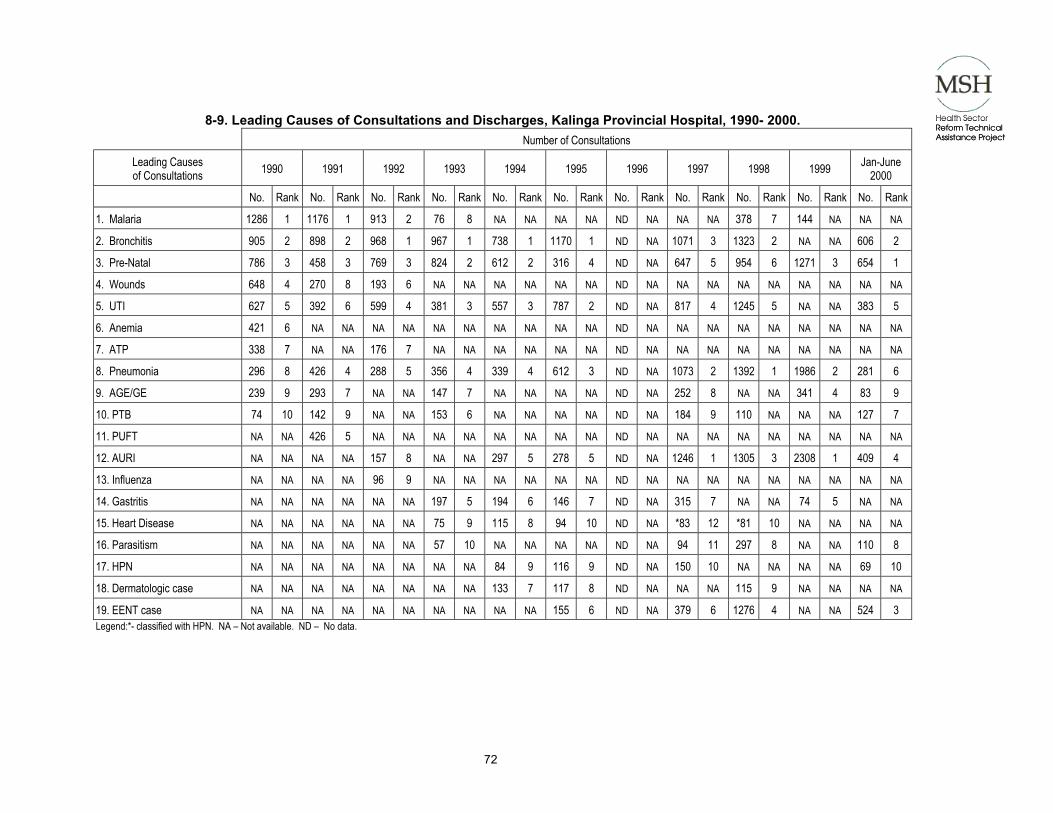
72
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-9. Leading Causes of Consultations and Discharges, Kalinga Provincial Hospital, 1990- 2000.
Number of Consultations
Leading Causes of Consultations 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Jan-June
2000
No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank
1. Malaria 1286 1 1176 1 913 2 76 8 NA NA NA NA ND NA NA NA 378 7 144 NA NA NA
2. Bronchitis 905 2 898 2 968 1 967 1 738 1 1170 1 ND NA 1071 3 1323 2 NA NA 606 2
3. Pre-Natal 786 3 458 3 769 3 824 2 612 2 316 4 ND NA 647 5 954 6 1271 3 654 1
4. Wounds 648 4 270 8 193 6 NA NA NA NA NA NA ND NA NA NA NA NA NA NA NA NA
5. UTI 627 5 392 6 599 4 381 3 557 3 787 2 ND NA 817 4 1245 5 NA NA 383 5
6. Anemia 421 6 NA NA NA NA NA NA NA NA NA NA ND NA NA NA NA NA NA NA NA NA
7. ATP 338 7 NA NA 176 7 NA NA NA NA NA NA ND NA NA NA NA NA NA NA NA NA
8. Pneumonia 296 8 426 4 288 5 356 4 339 4 612 3 ND NA 1073 2 1392 1 1986 2 281 6
9. AGE/GE 239 9 293 7 NA NA 147 7 NA NA NA NA ND NA 252 8 NA NA 341 4 83 9
10. PTB 74 10 142 9 NA NA 153 6 NA NA NA NA ND NA 184 9 110 NA NA NA 127 7
11. PUFT NA NA 426 5 NA NA NA NA NA NA NA NA ND NA NA NA NA NA NA NA NA NA
12. AURI NA NA NA NA 157 8 NA NA 297 5 278 5 ND NA 1246 1 1305 3 2308 1 409 4
13. Influenza NA NA NA NA 96 9 NA NA NA NA NA NA ND NA NA NA NA NA NA NA NA NA
14. Gastritis NA NA NA NA NA NA 197 5 194 6 146 7 ND NA 315 7 NA NA 74 5 NA NA
15. Heart Disease NA NA NA NA NA NA 75 9 115 8 94 10 ND NA *83 12 *81 10 NA NA NA NA
16. Parasitism NA NA NA NA NA NA 57 10 NA NA NA NA ND NA 94 11 297 8 NA NA 110 8
17. HPN NA NA NA NA NA NA NA NA 84 9 116 9 ND NA 150 10 NA NA NA NA 69 10
18. Dermatologic case NA NA NA NA NA NA NA NA 133 7 117 8 ND NA NA NA 115 9 NA NA NA NA
19. EENT case NA NA NA NA NA NA NA NA NA NA 155 6 ND NA 379 6 1276 4 NA NA 524 3 Legend:*- classified with HPN. NA – Not available. ND – No data.

73
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Number of Discharges (Final Diagnosis) Leading Causes of Discharges 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Jan-June
2000 No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank No. Rank
1. Malaria 1028 1 953 1 1016 2 851 3 1089 1 1165 1 233 3 164 5 518 4 78 10 46 8 2. Bronchitis 826 2 488 5 416 5 265 6 223 7 NA NA 145 6 203 4 292 7 195 5 96 4 3. Pneumonia 532 3 742 2 728 3 858 2 695 2 946 2 439 1 852 1 884 1 746 1 327 1 4. PUFT 485 4 498 3 NA NA NA NA NA NA NA NA NA NA NA NA NA NA 96 7 NA NA
5. Newborn/Post Partum/CS 470 5 498 4 1032 1 1283 1 NA NA NA NA NA NA NA NA NA NA 418 4 NA NA
6. UTI 322 6 231 7 407 6 287 5 525 3 712 3 193 4 444 3 599 3 621 2 324 2 7. AGE/ GE 305 7 416 6 573 4 484 4 480 4 386 4 267 2 525 2 620 2 472 3 318 3 8. Anemia 169 9 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA
9. ATP 139 10 NA NA 97 7 NA NA NA NA NA NA 43 7 34 NA NA NA 79 9 NA NA
10. Infected Wound/ Wounds 102 11 NA NA NA NA 103 8 312 5 319 6 175 5 156 6 322 5 132 6 NA NA
11. HPN NA NA 60 8 NA NA NA NA NA NA 37 10 17 10 NA NA NA NA NA NA 28 9 12. Measles NA NA 49 9 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA
13. PTB NA NA 41 10 NA NA NA NA 154 9 64 8 40 7 73 9 NA NA 75 11 13 10 14. PUD NA NA NA NA 80 8 NA NA 74 10 NA NA NA NA NA NA NA NA NA NA NA NA
15. Heart Diseases NA NA NA NA 74 10 114 7 203 8 NA NA NA NA 95 7 NA NA NA NA NA NA
16. Influenza NA NA NA NA 77 9 NA NA NA NA 50 9 NA NA NA NA NA NA NA NA NA NA
17. Abortion NA NA NA NA NA NA 53 10 NA NA NA NA NA NA 93 8 65 9 86 8 67 6 18. Typhoid Fever NA NA NA NA NA NA 93 9 263 6 353 5 NA NA 71 11 NA NA NA NA NA NA
19. EENT case NA NA NA NA NA NA NA NA NA NA 199 7 NA NA NA NA NA NA NA NA NA NA
20. Gastritis NA NA NA NA NA NA NA NA NA NA NA NA 22 8 72 10 NA NA NA NA NA NA
21. Cerebral Concussion NA NA NA NA NA NA NA NA NA NA NA NA 20 9 NA NA NA NA NA NA NA NA
22. URTI NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 251 6 NA NA NA NA
23. Dengue Fever NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 135 8 66 12 NA NA
24. Sepsis Neonatorum NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 93 5 25. Fracture NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 46 7 Source: Kalinga Provincial Hospital Report, 1990- Jan.-June 2000
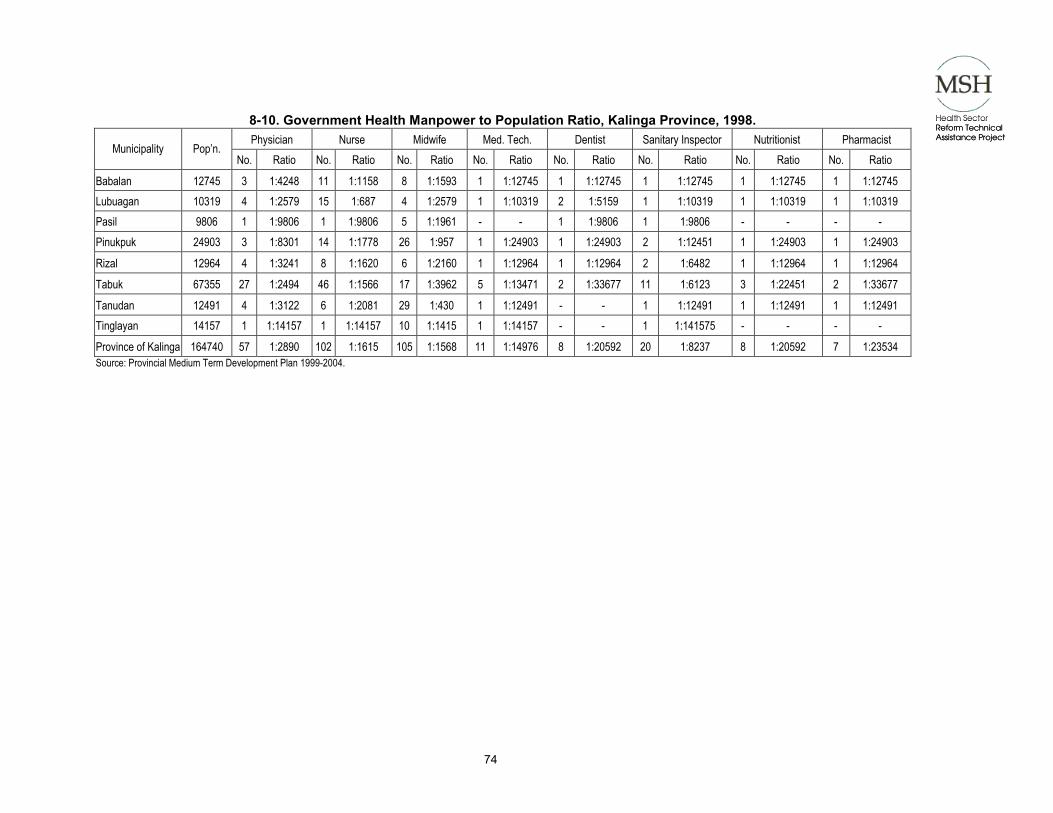
74
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-10. Government Health Manpower to Population Ratio, Kalinga Province, 1998. Physician Nurse Midwife Med. Tech. Dentist Sanitary Inspector Nutritionist Pharmacist
Municipality Pop’n. No. Ratio No. Ratio No. Ratio No. Ratio No. Ratio No. Ratio No. Ratio No. Ratio
Babalan 12745 3 1:4248 11 1:1158 8 1:1593 1 1:12745 1 1:12745 1 1:12745 1 1:12745 1 1:12745 Lubuagan 10319 4 1:2579 15 1:687 4 1:2579 1 1:10319 2 1:5159 1 1:10319 1 1:10319 1 1:10319 Pasil 9806 1 1:9806 1 1:9806 5 1:1961 - - 1 1:9806 1 1:9806 - - - - Pinukpuk 24903 3 1:8301 14 1:1778 26 1:957 1 1:24903 1 1:24903 2 1:12451 1 1:24903 1 1:24903
Rizal 12964 4 1:3241 8 1:1620 6 1:2160 1 1:12964 1 1:12964 2 1:6482 1 1:12964 1 1:12964
Tabuk 67355 27 1:2494 46 1:1566 17 1:3962 5 1:13471 2 1:33677 11 1:6123 3 1:22451 2 1:33677
Tanudan 12491 4 1:3122 6 1:2081 29 1:430 1 1:12491 - - 1 1:12491 1 1:12491 1 1:12491 Tinglayan 14157 1 1:14157 1 1:14157 10 1:1415 1 1:14157 - - 1 1:141575 - - - -
Province of Kalinga 164740 57 1:2890 102 1:1615 105 1:1568 11 1:14976 8 1:20592 20 1:8237 8 1:20592 7 1:23534 Source: Provincial Medium Term Development Plan 1999-2004.
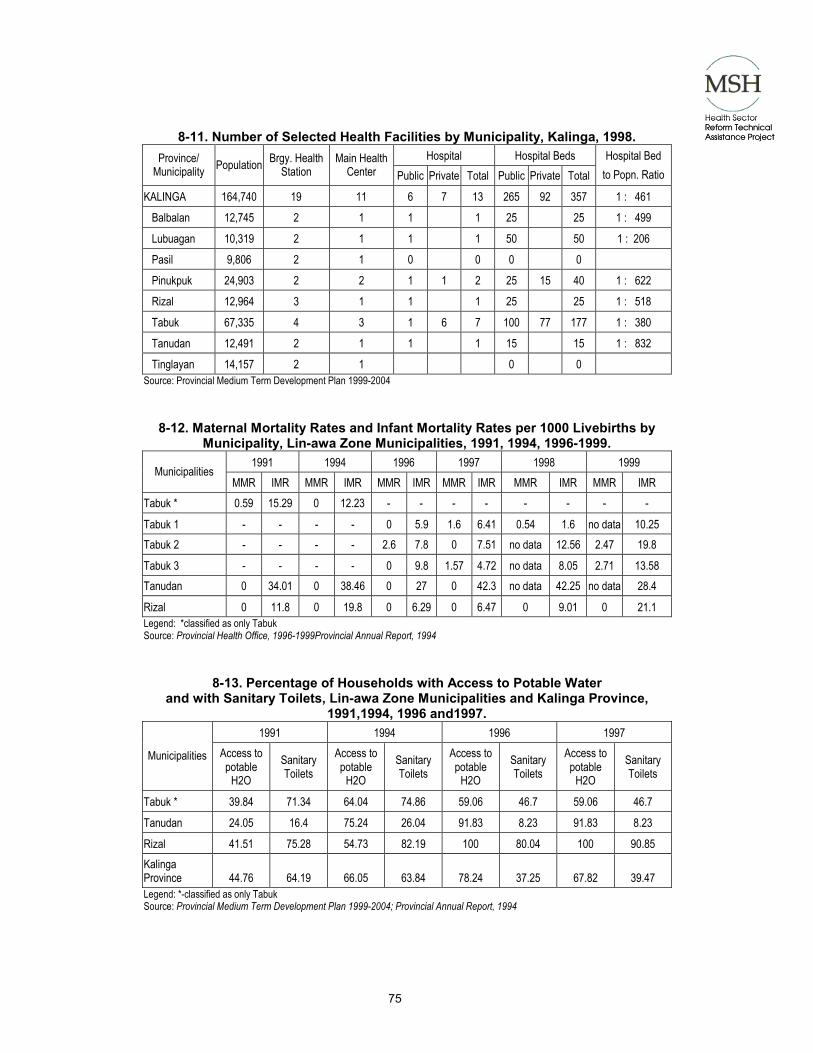
75
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-11. Number of Selected Health Facilities by Municipality, Kalinga, 1998. Hospital Hospital Beds Province/
Municipality Population Brgy. Health Station
Main Health Center Public Private Total Public Private Total
Hospital Bed to Popn. Ratio
KALINGA 164,740 19 11 6 7 13 265 92 357 1 : 461
Balbalan 12,745 2 1 1 1 25 25 1 : 499
Lubuagan 10,319 2 1 1 1 50 50 1 : 206
Pasil 9,806 2 1 0 0 0 0
Pinukpuk 24,903 2 2 1 1 2 25 15 40 1 : 622
Rizal 12,964 3 1 1 1 25 25 1 : 518
Tabuk 67,335 4 3 1 6 7 100 77 177 1 : 380
Tanudan 12,491 2 1 1 1 15 15 1 : 832
Tinglayan 14,157 2 1 0 0 Source: Provincial Medium Term Development Plan 1999-2004
8-12. Maternal Mortality Rates and Infant Mortality Rates per 1000 Livebirths by Municipality, Lin-awa Zone Municipalities, 1991, 1994, 1996-1999.
1991 1994 1996 1997 1998 1999 Municipalities
MMR IMR MMR IMR MMR IMR MMR IMR MMR IMR MMR IMR Tabuk * 0.59 15.29 0 12.23 - - - - - - - -
Tabuk 1 - - - - 0 5.9 1.6 6.41 0.54 1.6 no data 10.25 Tabuk 2 - - - - 2.6 7.8 0 7.51 no data 12.56 2.47 19.8
Tabuk 3 - - - - 0 9.8 1.57 4.72 no data 8.05 2.71 13.58 Tanudan 0 34.01 0 38.46 0 27 0 42.3 no data 42.25 no data 28.4
Rizal 0 11.8 0 19.8 0 6.29 0 6.47 0 9.01 0 21.1 Legend: *classified as only Tabuk Source: Provincial Health Office, 1996-1999Provincial Annual Report, 1994
8-13. Percentage of Households with Access to Potable Water and with Sanitary Toilets, Lin-awa Zone Municipalities and Kalinga Province,
1991,1994, 1996 and1997. 1991 1994 1996 1997
Municipalities Access to potable
H2O Sanitary Toilets
Access to potable
H2O Sanitary Toilets
Access to potable
H2O Sanitary Toilets
Access to potable
H2O Sanitary Toilets
Tabuk * 39.84 71.34 64.04 74.86 59.06 46.7 59.06 46.7
Tanudan 24.05 16.4 75.24 26.04 91.83 8.23 91.83 8.23
Rizal 41.51 75.28 54.73 82.19 100 80.04 100 90.85 Kalinga Province 44.76 64.19 66.05 63.84 78.24 37.25 67.82 39.47 Legend: *-classified as only Tabuk Source: Provincial Medium Term Development Plan 1999-2004; Provincial Annual Report, 1994

76
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-14. Budget for Health, Kalinga, 1993-2001.

77
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-15. Ranking of Unmet Minimum Basic Needs, Kalinga Province,1996. Rank Minimum Basic Needs Percent
1 Families with income above subsistence threshold Level 79.61
2 Other members of the family 18 years & above employed 71.02
3 Couples Practicing family planning in the last 6 months 67.96
4 Children aged 3-6 attending day care/ pre-school 66.54
5 Solo parent availing of health services 60.15
6 Access to sanitary toilets(watersealed, antipolo, flushed) 49.48
7 Children 13-16 years old in high school 47.53
8 Deliveries attended by trained personnel 45.5
9 0-1 years old fully immunized 36.99
10 Couples with access to family planning 36.44
11 Infants breastfed for at least 4 months 34.69
12 No severely and moderately underweight children 34.22
13 Pregnant women given at least 2 doses of tetanus toxoid 33.83
14 Pregnant & Lactating mothers provided with Iron & Iodine supplements 33.46
15 Children 6-12 years old in elementary school 29.77
16 Access to potable water (faucet/deepwell) within 250 m 27.61
17 Family members 10 years and above able to read and write 26.92
18 Newborns with birth weight of at least 2.5 kgs. 25.86
19 No child below 7 years old left unattended 24.53
20 Family members involved in at least 1 people's organization 23.36
21 Not more than 1 diarrhea episodes per child under 5 yr. Old 22.23
22 Head of family employed 21.65
23 Children 18 years old & below not engaged in hazardous occupation 18.42
24 Housing durable for at least 5 years 18.28
25 No family member displaced by natural disaster 17.08
26 Family members with basic clothing (at least 3 sets) 13.97
27 Family members able to vote at elections 13.18
28 No family member victimized by crime against property (theft) 7.71
29 No family members victimized by crime against person (rape, murder) 2.49
30 House owned, rented or shared 2.02
31 No incidence of domestic violence 1.97
32 No deaths in family due to preventable causes w/in the year 1.69
33 No family member victimized by armed conflict 1.49 Source: Provincial Medium Term Development Plan 1999-2004.

78
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-16. Provincial Environment to PhilHealth Indigent Program Center.
(Note: available in hardcopy only.)

79
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
8-17. Hospital and Rural Health Unit Mix of Services.
Mix of Services of the Tertiary Provincial Hospital 1) Medical:
• Medicine Cardiology Hematology Pulmonary Infectious Disease Gastroentorology Oncology • Surgery General Urology Orthopedics Oncology • EENT Opthalmology • OB-GYNE Fertility STD Clinics Oncology Ultrasonology • Pediatrics Cardiology Infectious Disease Neonatology/Perinatology Pulmonology • Radiology Nuclear Medicine Ultrasonology • Anesthesia Regional Anesthesia Management of Pain • Pathology Anatomic Clinical Forensic • Psychiatry General • ER
2) Nursing:
• Medicine Critical Care Adult CCU ICU Renal Pulmonary • Surgery Critical Care OR/DR • OB-GYNE Critical Care OR/DR • Pediatrics Critical Care Renal Neonatology Perinatology Pulmonary • CSR Antiseptic/Asepsis • ER
3) Laboratory:
• Hematology • Blood Banking • AIDS/STD • Water Analysis • Culture and Sensitivity
4) Pharmacy:
• Clinical Pharmacy 5) Dental: • Orthodentology 6) Dietary: • Therapeutic Diet Preparation

80
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
7) Administrative: • Computer Literacy and Troubleshooting • Bromidical Engineering • Equipment Maintenance and Troubleshooting • Waste Management • Housekeeping, Janitorial • Laundering 8) Technical Staff: • Training • Technical Supervision/Monitoring 9) Training:
• Midwifery Affiliate • Technical Programs (Updates and Skills) for both Hospital/Field Health Staff
Mix of Services of the RHU 1. Priority DOH programs (FP/RH services, EPI, Nutrition, CARI, Malaria Control TB
Control, CDD)
2. Maternal and Child Health
3. NCDC
4. Dental Services
5. Laboratory Services
6. Consultation
7. Minor Surgery
8. Disease Prevention
9. Control of locally endemic diseases
10. Attend Medical/surgical emergencies
11. Prompt referral of major cases
12. Supervision
13. Proper reporting and recording of FHSIS
14. Thorough follow-up of cases
15. Local Health Board
16. Tap or network with NGOs
17. Encourage and support livelihood project
18. Help/Contribute to Community Health Plan
19. Monitor health of community
20. Medico-legal

81
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 9. Quick Survey Results.
9-1. Sex Distribution by Municipality, Kalinga Province, 2001. Rizal Tabuk Total
Sex Freq Percent Freq Percent Freq Percent
Female 72 85.71 176 77.88 248 80.00 Male 9 10.71 46 20.35 55 17.74 No Response 3 3.57 4 1.77 7 2.26 Total 84 100.00 226 100.00 310 100.00
9-2. Age Distribution by Municipality, Kalinga Province,2001. Rizal Tabuk Total
Age Group Freq Percent Freq Percent Freq Percent
18 - 30 27 32.14 72 31.86 99 31.94 31 -39 20 23.81 68 30.09 88 28.39 40 - 52 18 21.43 53 23.45 71 22.90
53+ 19 22.62 33 14.60 52 16.77 Total 84 100.00 226 100.00 310 100.00
9-3. Income by Municipality, Kalinga Province,2001. Rizal Tabuk Total
Income Freq Percent Freq Percent Freq Percent
less than 2500 17 20.24 35 15.49 52 16.77 2501 - 5000 38 45.24 89 39.38 127 40.97 5001 - 10000 20 23.81 50 22.12 70 22.58 10001 - 20000 9 10.71 45 19.91 54 17.42
> 20000 0 0.00 7 3.10 7 2.26 Total 84 100.00 226 100.00 310 100.00
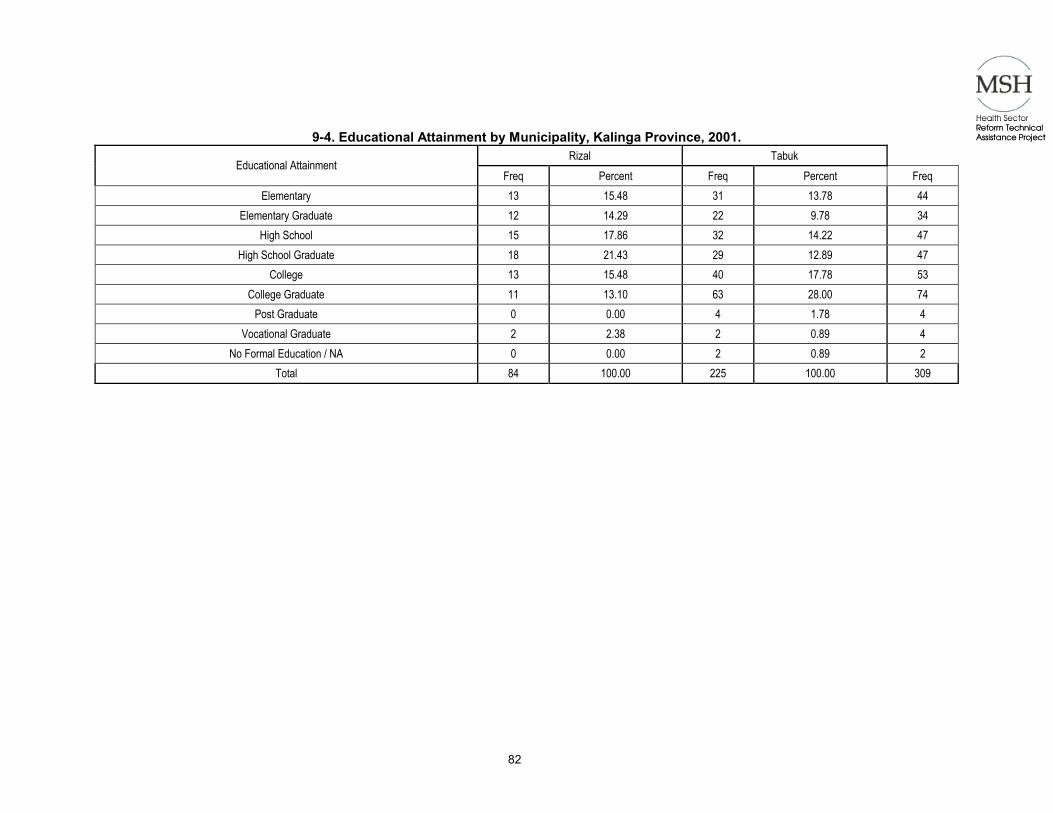
82
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-4. Educational Attainment by Municipality, Kalinga Province, 2001. Rizal Tabuk
Educational Attainment Freq Percent Freq Percent Freq
Elementary 13 15.48 31 13.78 44 Elementary Graduate 12 14.29 22 9.78 34
High School 15 17.86 32 14.22 47 High School Graduate 18 21.43 29 12.89 47
College 13 15.48 40 17.78 53 College Graduate 11 13.10 63 28.00 74
Post Graduate 0 0.00 4 1.78 4 Vocational Graduate 2 2.38 2 0.89 4
No Formal Education / NA 0 0.00 2 0.89 2 Total 84 100.00 225 100.00 309

83
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-5. Nearest Health Facility by Income, Rizal, Kalinga Province, 2001.
< 2500 2501-5000 5001-10000 Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank District Hospital 7 41.18 2 16 42.11 1 9 45.00 2
Provincial Hospital 0 0.00 4 0 0.00 5 0 0.00 4 Private Hospital 0 0.00 4 2 5.26 4 0 0.00 4
Rural Health Unit 9 5.88 1 15 13.16 2 10 5.00 1 Barangay Health Station 1 5.88 3 5 13.16 3 1 5.00 3 Other District Hospital 0 0.00 4 0 0.00 5 0 0.00 4
Total 17 100.00 38 100.00 20 100.00
10001-20000 >20000 Total Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent District Hospital 3 33.33 2 0 0.00 1 35 41.67
Provincial Hospital 0 0.00 4 0 0.00 1 0 0.00 Private Hospital 1 11.11 3 0 0.00 1 3 3.57
Rural Health Unit 5 0.00 1 0 0.00 1 39 46.43 Barangay Health Station 0 0.00 4 0 0.00 1 7 8.33 Other District Hospital 0 0.00 4 0 0.00 1 0 0.00
Total 9 100.00 0 0.00 84 100.00
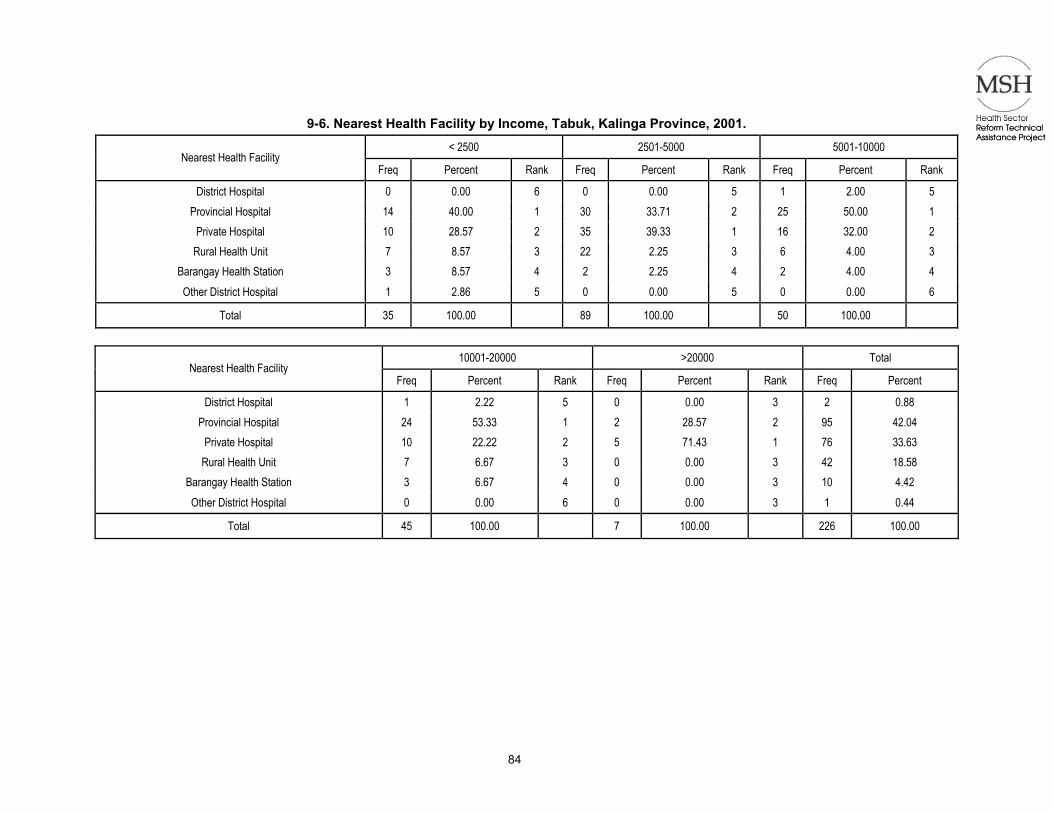
84
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-6. Nearest Health Facility by Income, Tabuk, Kalinga Province, 2001.
< 2500 2501-5000 5001-10000 Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank District Hospital 0 0.00 6 0 0.00 5 1 2.00 5
Provincial Hospital 14 40.00 1 30 33.71 2 25 50.00 1 Private Hospital 10 28.57 2 35 39.33 1 16 32.00 2
Rural Health Unit 7 8.57 3 22 2.25 3 6 4.00 3 Barangay Health Station 3 8.57 4 2 2.25 4 2 4.00 4 Other District Hospital 1 2.86 5 0 0.00 5 0 0.00 6
Total 35 100.00 89 100.00 50 100.00
10001-20000 >20000 Total Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent District Hospital 1 2.22 5 0 0.00 3 2 0.88
Provincial Hospital 24 53.33 1 2 28.57 2 95 42.04 Private Hospital 10 22.22 2 5 71.43 1 76 33.63
Rural Health Unit 7 6.67 3 0 0.00 3 42 18.58 Barangay Health Station 3 6.67 4 0 0.00 3 10 4.42 Other District Hospital 0 0.00 6 0 0.00 3 1 0.44
Total 45 100.00 7 100.00 226 100.00
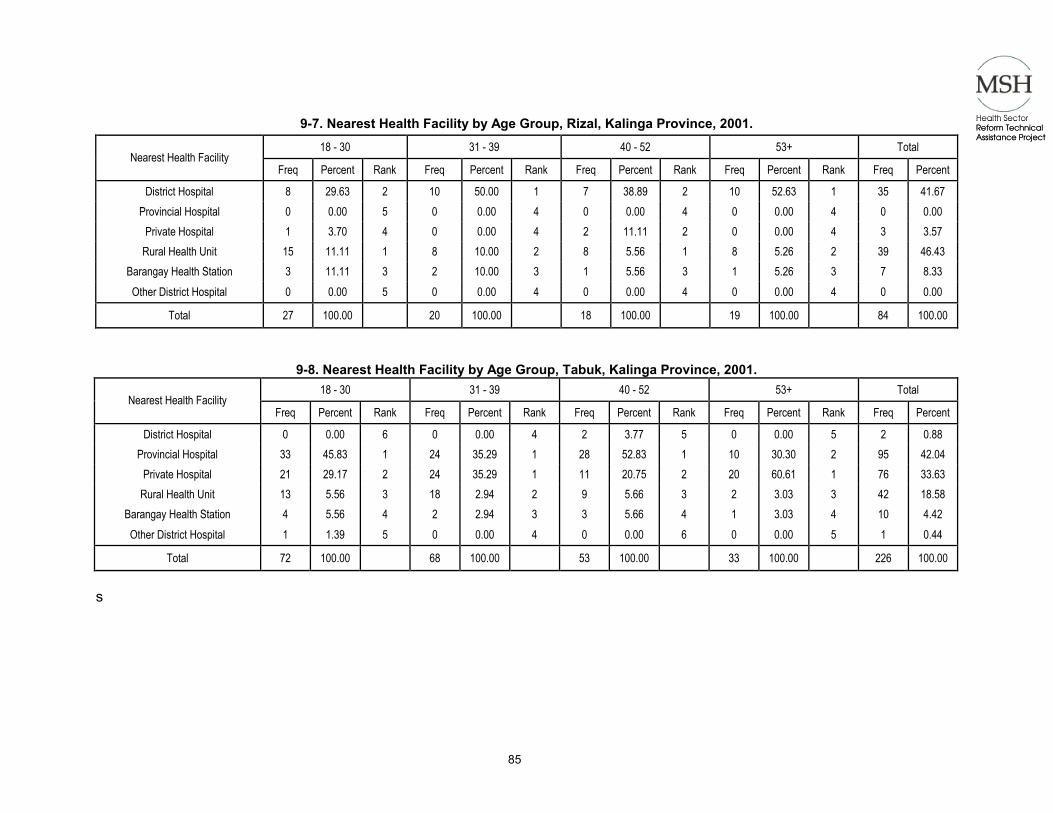
85
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-7. Nearest Health Facility by Age Group, Rizal, Kalinga Province, 2001.
18 - 30 31 - 39 40 - 52 53+ Total Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent District Hospital 8 29.63 2 10 50.00 1 7 38.89 2 10 52.63 1 35 41.67
Provincial Hospital 0 0.00 5 0 0.00 4 0 0.00 4 0 0.00 4 0 0.00 Private Hospital 1 3.70 4 0 0.00 4 2 11.11 2 0 0.00 4 3 3.57
Rural Health Unit 15 11.11 1 8 10.00 2 8 5.56 1 8 5.26 2 39 46.43 Barangay Health Station 3 11.11 3 2 10.00 3 1 5.56 3 1 5.26 3 7 8.33 Other District Hospital 0 0.00 5 0 0.00 4 0 0.00 4 0 0.00 4 0 0.00
Total 27 100.00 20 100.00 18 100.00 19 100.00 84 100.00
9-8. Nearest Health Facility by Age Group, Tabuk, Kalinga Province, 2001. 18 - 30 31 - 39 40 - 52 53+ Total
Nearest Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 0 0.00 6 0 0.00 4 2 3.77 5 0 0.00 5 2 0.88 Provincial Hospital 33 45.83 1 24 35.29 1 28 52.83 1 10 30.30 2 95 42.04
Private Hospital 21 29.17 2 24 35.29 1 11 20.75 2 20 60.61 1 76 33.63 Rural Health Unit 13 5.56 3 18 2.94 2 9 5.66 3 2 3.03 3 42 18.58
Barangay Health Station 4 5.56 4 2 2.94 3 3 5.66 4 1 3.03 4 10 4.42 Other District Hospital 1 1.39 5 0 0.00 4 0 0.00 6 0 0.00 5 1 0.44
Total 72 100.00 68 100.00 53 100.00 33 100.00 226 100.00 s

86
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-9. Nearest Health Facility by Educational Attainment, Rizal, Kalinga Province, 2001.
Elementary Elementary Graduate High School High School Graduate Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank District Hospital 6 35.29 1 6 50.00 1 9 60.00 1 4 22.22 2
Provincial Hospital 0 0.00 4 0 0.00 2 0 0.00 4 0 0.00 4 Private Hospital 1 5.88 3 0 0.00 2 0 0.00 4 1 5.56 3
Rural Health Unit 5 5.88 2 6 50.00 1 5 6.67 2 12 5.56 1 Barangay Health Station 1 5.88 3 0 0.00 2 1 6.67 3 1 5.56 3 Other District Hospital 0 0.00 4 0 0.00 2 0 0.00 4 0 0.00 4
Total 17 100.00 12 100.00 15 100.00 18 100.00
College College Graduate Post graduate Vocational Graduate No Formal School / NA Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank District Hospital 4 30.77 2 5 45.45 1 0 0.00 1 1 50.00 1 0 0.00 1
Provincial Hospital 0 0.00 4 0 0.00 3 0 0.00 1 0 0.00 2 0 0.00 1 Private Hospital 0 0.00 4 1 9.09 2 0 0.00 1 0 0.00 2 0 0.00 1
Rural Health Unit 6 46.15 1 5 45.45 1 0 0.00 1 0 0.00 2 0 0.00 1 Barangay Health Station 3 23.08 3 0 0.00 3 0 0.00 1 1 50.00 1 0 0.00 1 Other District Hospital 0 0.00 4 0 0.00 3 0 0.00 1 0 0.00 2 0 0.00 1
Total 13 100.00 11 100.00 0 0.00 2 100.00 0 0.00
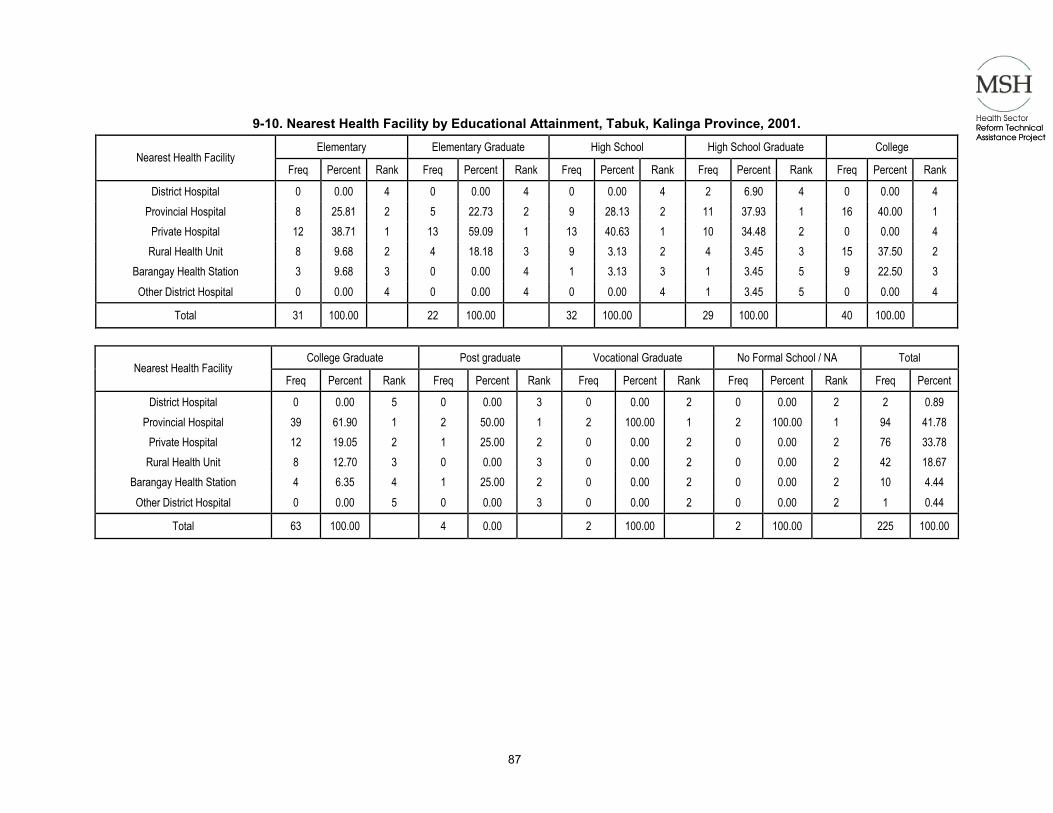
87
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-10. Nearest Health Facility by Educational Attainment, Tabuk, Kalinga Province, 2001.
Elementary Elementary Graduate High School High School Graduate College Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank District Hospital 0 0.00 4 0 0.00 4 0 0.00 4 2 6.90 4 0 0.00 4
Provincial Hospital 8 25.81 2 5 22.73 2 9 28.13 2 11 37.93 1 16 40.00 1 Private Hospital 12 38.71 1 13 59.09 1 13 40.63 1 10 34.48 2 0 0.00 4
Rural Health Unit 8 9.68 2 4 18.18 3 9 3.13 2 4 3.45 3 15 37.50 2 Barangay Health Station 3 9.68 3 0 0.00 4 1 3.13 3 1 3.45 5 9 22.50 3 Other District Hospital 0 0.00 4 0 0.00 4 0 0.00 4 1 3.45 5 0 0.00 4
Total 31 100.00 22 100.00 32 100.00 29 100.00 40 100.00
College Graduate Post graduate Vocational Graduate No Formal School / NA Total Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 0 0.00 5 0 0.00 3 0 0.00 2 0 0.00 2 2 0.89 Provincial Hospital 39 61.90 1 2 50.00 1 2 100.00 1 2 100.00 1 94 41.78
Private Hospital 12 19.05 2 1 25.00 2 0 0.00 2 0 0.00 2 76 33.78 Rural Health Unit 8 12.70 3 0 0.00 3 0 0.00 2 0 0.00 2 42 18.67
Barangay Health Station 4 6.35 4 1 25.00 2 0 0.00 2 0 0.00 2 10 4.44 Other District Hospital 0 0.00 5 0 0.00 3 0 0.00 2 0 0.00 2 1 0.44
Total 63 100.00 4 0.00 2 100.00 2 100.00 225 100.00

88
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-11. Nearest Health Facility by Sex, Rizal, Kalinga Province, 2001.
Female Male No Response Total Nearest Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent District Hospital 31 43.06 2 4 44.44 1 0 0.00 3 35 41.67
Provincial Hospital 0 0.00 5 0 0.00 4 0 0.00 3 0 0.00 Private Hospital 3 4.17 4 0 0.00 4 0 0.00 3 3 3.57
Rural Health Unit 34 5.56 1 3 33.33 2 2 66.67 1 39 46.43 Barangay Health Station 4 5.56 3 2 22.22 3 1 33.33 2 7 8.33 Other District Hospital 0 0.00 5 0 0.00 4 0 0.00 3 0 0.00
Total 72 100.00 9 100.00 3 100.00 84 100.00
9-12. Nearest Health Facility by Sex, Tabuk, Kalinga Province, 2001. Female Male No Response Total
Nearest Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 2 1.14 2 0 0.00 5 0 0.00 3 2 0.88 Provincial Hospital 70 39.77 1 24 52.17 1 1 25.00 2 95 42.04
Private Hospital 56 31.82 2 18 39.13 2 2 50.00 1 76 33.63 Rural Health Unit 38 5.11 3 3 6.52 3 1 0.00 2 42 18.58
Barangay Health Station 9 5.11 4 1 2.17 4 0 0.00 3 10 4.42 Other District Hospital 1 0.57 6 0 0.00 5 0 0.00 3 1 0.44
Total 176 100.00 46 100.00 4 100.00 226 100.00
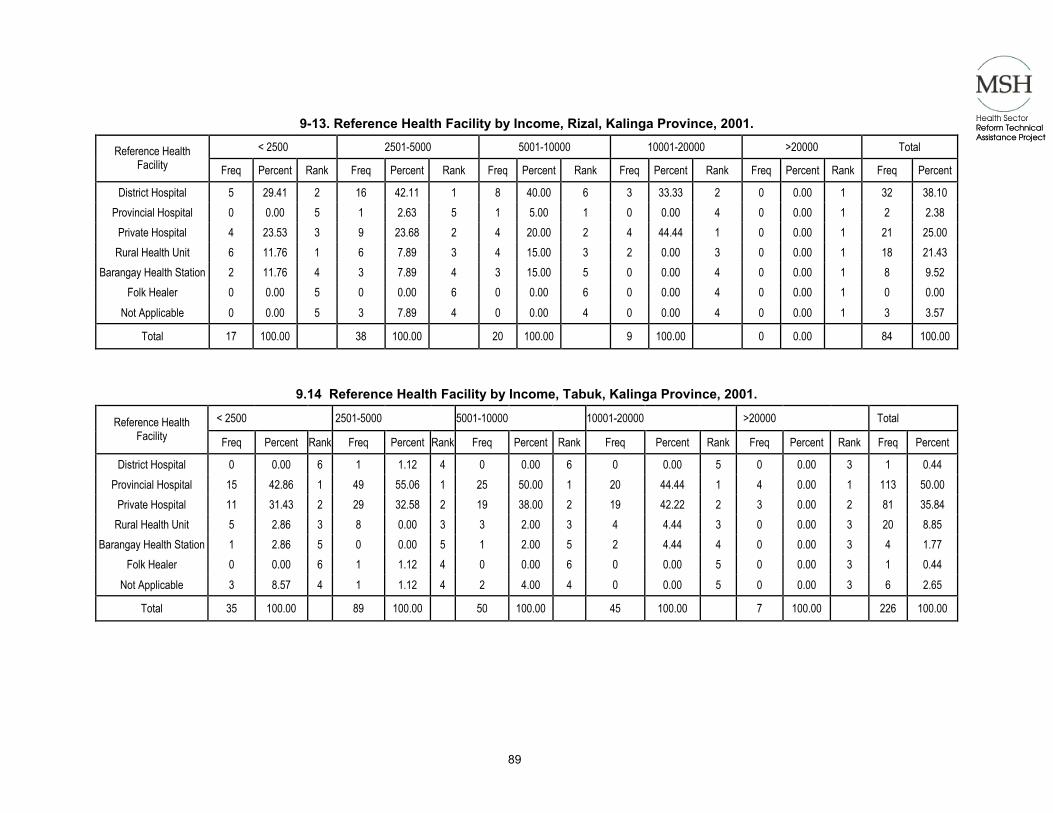
89
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-13. Reference Health Facility by Income, Rizal, Kalinga Province, 2001.
< 2500 2501-5000 5001-10000 10001-20000 >20000 Total Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 5 29.41 2 16 42.11 1 8 40.00 6 3 33.33 2 0 0.00 1 32 38.10 Provincial Hospital 0 0.00 5 1 2.63 5 1 5.00 1 0 0.00 4 0 0.00 1 2 2.38
Private Hospital 4 23.53 3 9 23.68 2 4 20.00 2 4 44.44 1 0 0.00 1 21 25.00 Rural Health Unit 6 11.76 1 6 7.89 3 4 15.00 3 2 0.00 3 0 0.00 1 18 21.43
Barangay Health Station 2 11.76 4 3 7.89 4 3 15.00 5 0 0.00 4 0 0.00 1 8 9.52 Folk Healer 0 0.00 5 0 0.00 6 0 0.00 6 0 0.00 4 0 0.00 1 0 0.00
Not Applicable 0 0.00 5 3 7.89 4 0 0.00 4 0 0.00 4 0 0.00 1 3 3.57 Total 17 100.00 38 100.00 20 100.00 9 100.00 0 0.00 84 100.00
9.14 Reference Health Facility by Income, Tabuk, Kalinga Province, 2001. < 2500 2501-5000 5001-10000 10001-20000 >20000 Total Reference Health
Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent District Hospital 0 0.00 6 1 1.12 4 0 0.00 6 0 0.00 5 0 0.00 3 1 0.44
Provincial Hospital 15 42.86 1 49 55.06 1 25 50.00 1 20 44.44 1 4 0.00 1 113 50.00 Private Hospital 11 31.43 2 29 32.58 2 19 38.00 2 19 42.22 2 3 0.00 2 81 35.84
Rural Health Unit 5 2.86 3 8 0.00 3 3 2.00 3 4 4.44 3 0 0.00 3 20 8.85 Barangay Health Station 1 2.86 5 0 0.00 5 1 2.00 5 2 4.44 4 0 0.00 3 4 1.77
Folk Healer 0 0.00 6 1 1.12 4 0 0.00 6 0 0.00 5 0 0.00 3 1 0.44 Not Applicable 3 8.57 4 1 1.12 4 2 4.00 4 0 0.00 5 0 0.00 3 6 2.65
Total 35 100.00 89 100.00 50 100.00 45 100.00 7 100.00 226 100.00
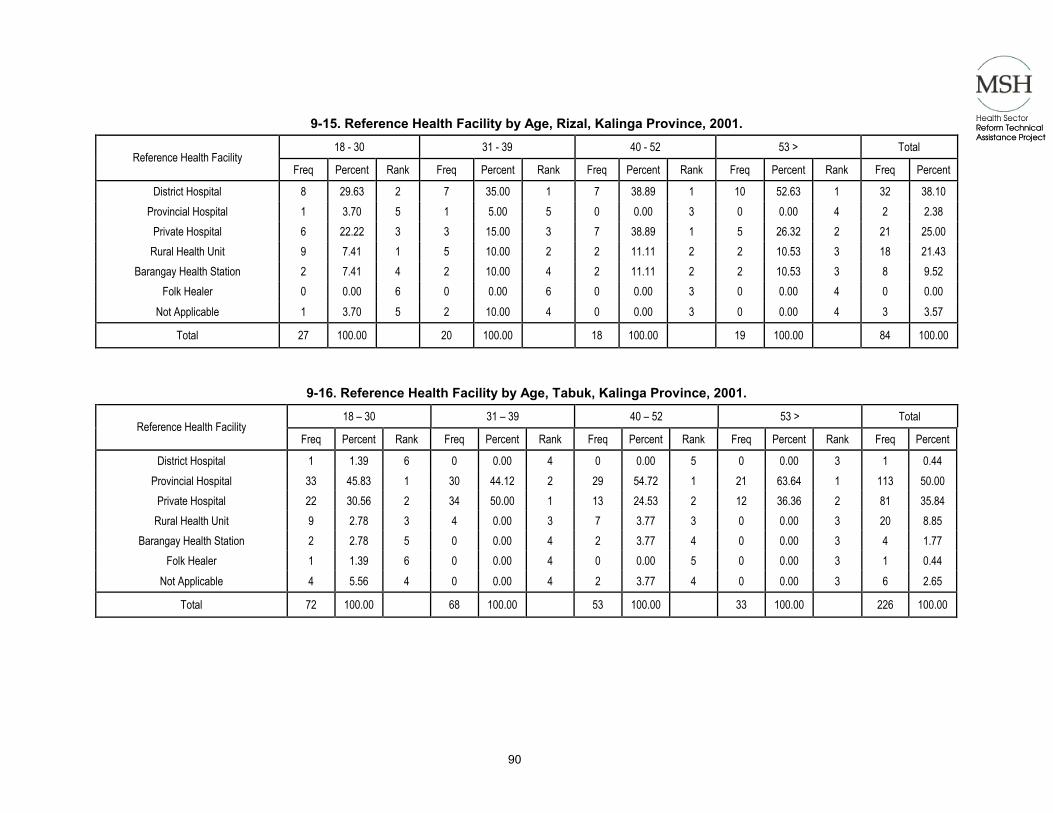
90
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-15. Reference Health Facility by Age, Rizal, Kalinga Province, 2001.
18 - 30 31 - 39 40 - 52 53 > Total Reference Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 8 29.63 2 7 35.00 1 7 38.89 1 10 52.63 1 32 38.10 Provincial Hospital 1 3.70 5 1 5.00 5 0 0.00 3 0 0.00 4 2 2.38
Private Hospital 6 22.22 3 3 15.00 3 7 38.89 1 5 26.32 2 21 25.00 Rural Health Unit 9 7.41 1 5 10.00 2 2 11.11 2 2 10.53 3 18 21.43
Barangay Health Station 2 7.41 4 2 10.00 4 2 11.11 2 2 10.53 3 8 9.52 Folk Healer 0 0.00 6 0 0.00 6 0 0.00 3 0 0.00 4 0 0.00
Not Applicable 1 3.70 5 2 10.00 4 0 0.00 3 0 0.00 4 3 3.57 Total 27 100.00 20 100.00 18 100.00 19 100.00 84 100.00
9-16. Reference Health Facility by Age, Tabuk, Kalinga Province, 2001. 18 – 30 31 – 39 40 – 52 53 > Total
Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 1 1.39 6 0 0.00 4 0 0.00 5 0 0.00 3 1 0.44 Provincial Hospital 33 45.83 1 30 44.12 2 29 54.72 1 21 63.64 1 113 50.00
Private Hospital 22 30.56 2 34 50.00 1 13 24.53 2 12 36.36 2 81 35.84 Rural Health Unit 9 2.78 3 4 0.00 3 7 3.77 3 0 0.00 3 20 8.85
Barangay Health Station 2 2.78 5 0 0.00 4 2 3.77 4 0 0.00 3 4 1.77 Folk Healer 1 1.39 6 0 0.00 4 0 0.00 5 0 0.00 3 1 0.44
Not Applicable 4 5.56 4 0 0.00 4 2 3.77 4 0 0.00 3 6 2.65 Total 72 100.00 68 100.00 53 100.00 33 100.00 226 100.00

91
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-17. Reference Health Facility by Sex, Rizal, Kalinga Province, 2001.
Female Male No Response Total Reference Health Facility
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent District Hospital 29 40.28 1 3 33.33 1 0 0.00 3 32 38.10
Provincial Hospital 2 2.78 5 0 0.00 4 0 0.00 3 2 2.38 Private Hospital 19 26.39 2 2 22.22 2 0 0.00 3 21 25.00
Rural Health Unit 15 6.94 3 2 11.11 2 1 66.67 2 18 21.43 Barangay Health Station 5 6.94 4 1 11.11 3 2 66.67 1 8 9.52
Folk Healer 0 0.00 6 0 0.00 4 0 0.00 3 0 0.00 Not Applicable 2 2.78 5 1 11.11 3 0 0.00 3 3 3.57
Total 72 100.00 9 100.00 3 100.00 84 100.00
9-18. Reference Health Facility by Sex, Tabuk, Kalinga Province, 2001. Female Male No Response Total
Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 1 0.57 6 0 0.00 6 0 0.00 1 1 0.44 Provincial Hospital 88 50.00 1 21 45.65 1 0 0.00 1 113 50.00
Private Hospital 62 35.23 2 19 41.30 2 0 0.00 1 81 35.84 Rural Health Unit 18 2.27 3 2 0.00 4 0 0.00 1 20 8.85
Barangay Health Station 4 2.27 4 0 0.00 6 0 0.00 1 4 1.77 Folk Healer 0 0.00 7 1 2.17 5 0 0.00 1 1 0.44
Not Applicable 3 1.70 5 3 6.52 3 0 0.00 1 6 2.65 Total 176 100.00 46 100.00 0 0.00 226 100.00

92
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-19. Reference Health Facility by Education, Tabuk, Kalinga Province, 2001.
Elementary Elementary Graduate High School High School Graduate Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent rank
District Hospital 0 0.00 4 0 0.00 5 0 0.00 4 0 0.00 4 Provincial Hospital 18 58.06 1 12 54.55 1 12 37.50 1 14 48.28 1
Private Hospital 11 35.48 2 7 31.82 2 12 37.50 1 10 34.48 2 Rural Health Unit 1 0.00 3 2 0.00 3 6 0.00 2 5 0.00 3
Barangay Health Station 0 0.00 4 0 0.00 5 0 0.00 4 0 0.00 4 Folk Healer 0 0.00 4 0 0.00 5 0 0.00 4 0 0.00 4
Not Applicable 1 3.23 3 1 4.55 4 2 6.25 3 0 0.00 4 Total 31 100.00 22 100.00 32 100.00 29 100.00
College College Graduate Post Graduate Vocational Graduate Not Applicable Total Reference Health
Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 1 2.50 4 0 0.00 5 0 0.00 3 0 0.00 2 0 0.00 2 1 0.44 Provincial Hospital 22 55.00 1 30 47.62 1 0 0.00 3 2 100.00 1 2 100.00 1 112 49.78
Private Hospital 13 32.50 2 25 39.68 2 3 75.00 1 0 0.00 2 0 0.00 2 81 36.00 Rural Health Unit 2 2.50 3 4 3.17 3 0 25.00 3 0 0.00 2 0 0.00 2 20 8.89
Barangay Health Station 1 2.50 4 2 3.17 4 1 25.00 2 0 0.00 2 0 0.00 2 4 1.78 Folk Healer 1 2.50 4 0 0.00 5 0 0.00 3 0 0.00 2 0 0.00 2 1 0.44
Not Applicable 0 0.00 5 2 3.17 4 0 0.00 3 0 0.00 2 0 0.00 2 6 2.67 Total 40 100.00 63 100.00 4 100.00 2 100.00 2 100.00 225 100.00
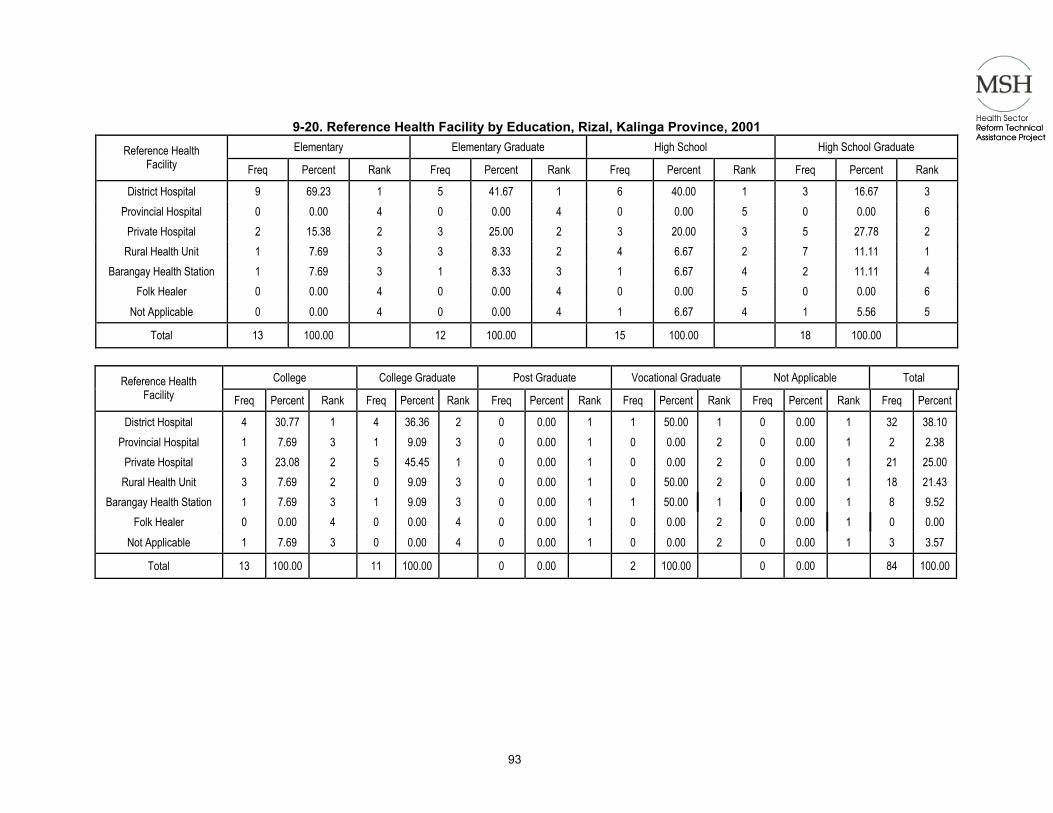
93
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-20. Reference Health Facility by Education, Rizal, Kalinga Province, 2001 Elementary Elementary Graduate High School High School Graduate Reference Health
Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank District Hospital 9 69.23 1 5 41.67 1 6 40.00 1 3 16.67 3
Provincial Hospital 0 0.00 4 0 0.00 4 0 0.00 5 0 0.00 6 Private Hospital 2 15.38 2 3 25.00 2 3 20.00 3 5 27.78 2
Rural Health Unit 1 7.69 3 3 8.33 2 4 6.67 2 7 11.11 1 Barangay Health Station 1 7.69 3 1 8.33 3 1 6.67 4 2 11.11 4
Folk Healer 0 0.00 4 0 0.00 4 0 0.00 5 0 0.00 6 Not Applicable 0 0.00 4 0 0.00 4 1 6.67 4 1 5.56 5
Total 13 100.00 12 100.00 15 100.00 18 100.00
College College Graduate Post Graduate Vocational Graduate Not Applicable Total Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 4 30.77 1 4 36.36 2 0 0.00 1 1 50.00 1 0 0.00 1 32 38.10 Provincial Hospital 1 7.69 3 1 9.09 3 0 0.00 1 0 0.00 2 0 0.00 1 2 2.38
Private Hospital 3 23.08 2 5 45.45 1 0 0.00 1 0 0.00 2 0 0.00 1 21 25.00 Rural Health Unit 3 7.69 2 0 9.09 3 0 0.00 1 0 50.00 2 0 0.00 1 18 21.43
Barangay Health Station 1 7.69 3 1 9.09 3 0 0.00 1 1 50.00 1 0 0.00 1 8 9.52 Folk Healer 0 0.00 4 0 0.00 4 0 0.00 1 0 0.00 2 0 0.00 1 0 0.00
Not Applicable 1 7.69 3 0 0.00 4 0 0.00 1 0 0.00 2 0 0.00 1 3 3.57 Total 13 100.00 11 100.00 0 0.00 2 100.00 0 0.00 84 100.00
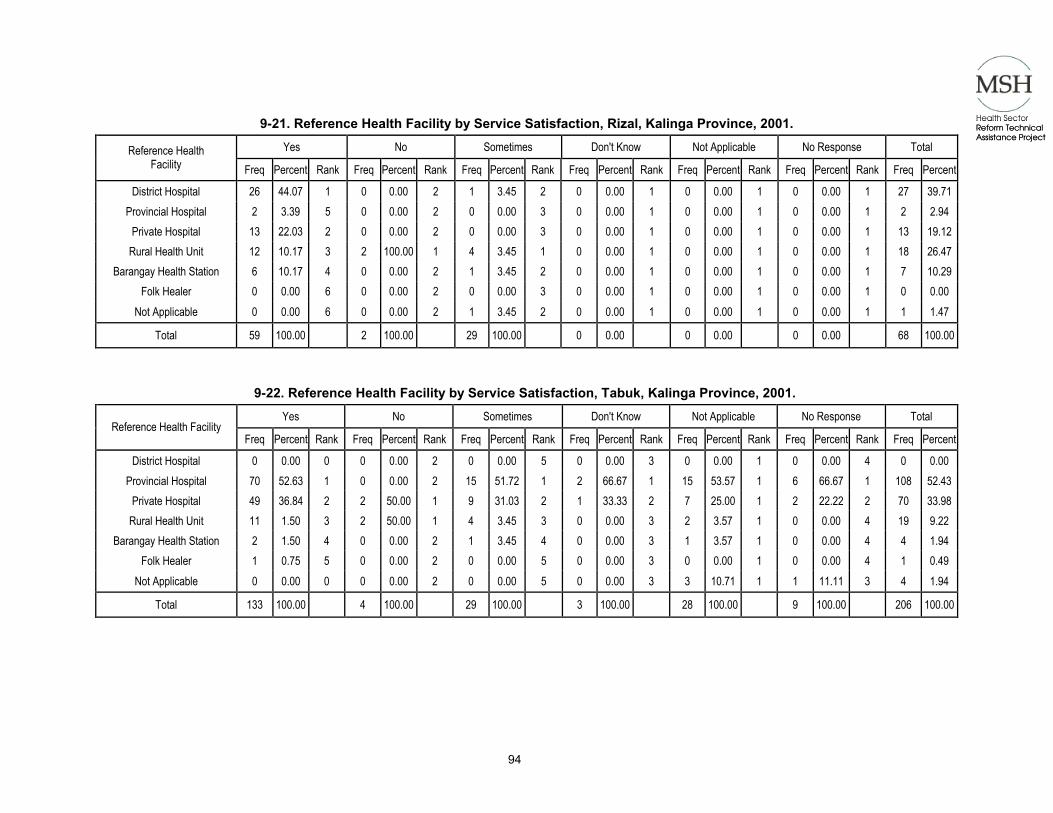
94
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-21. Reference Health Facility by Service Satisfaction, Rizal, Kalinga Province, 2001.
Yes No Sometimes Don't Know Not Applicable No Response Total Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 26 44.07 1 0 0.00 2 1 3.45 2 0 0.00 1 0 0.00 1 0 0.00 1 27 39.71Provincial Hospital 2 3.39 5 0 0.00 2 0 0.00 3 0 0.00 1 0 0.00 1 0 0.00 1 2 2.94
Private Hospital 13 22.03 2 0 0.00 2 0 0.00 3 0 0.00 1 0 0.00 1 0 0.00 1 13 19.12Rural Health Unit 12 10.17 3 2 100.00 1 4 3.45 1 0 0.00 1 0 0.00 1 0 0.00 1 18 26.47
Barangay Health Station 6 10.17 4 0 0.00 2 1 3.45 2 0 0.00 1 0 0.00 1 0 0.00 1 7 10.29Folk Healer 0 0.00 6 0 0.00 2 0 0.00 3 0 0.00 1 0 0.00 1 0 0.00 1 0 0.00
Not Applicable 0 0.00 6 0 0.00 2 1 3.45 2 0 0.00 1 0 0.00 1 0 0.00 1 1 1.47 Total 59 100.00 2 100.00 29 100.00 0 0.00 0 0.00 0 0.00 68 100.00
9-22. Reference Health Facility by Service Satisfaction, Tabuk, Kalinga Province, 2001. Yes No Sometimes Don't Know Not Applicable No Response Total
Reference Health Facility Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
District Hospital 0 0.00 0 0 0.00 2 0 0.00 5 0 0.00 3 0 0.00 1 0 0.00 4 0 0.00 Provincial Hospital 70 52.63 1 0 0.00 2 15 51.72 1 2 66.67 1 15 53.57 1 6 66.67 1 108 52.43
Private Hospital 49 36.84 2 2 50.00 1 9 31.03 2 1 33.33 2 7 25.00 1 2 22.22 2 70 33.98Rural Health Unit 11 1.50 3 2 50.00 1 4 3.45 3 0 0.00 3 2 3.57 1 0 0.00 4 19 9.22
Barangay Health Station 2 1.50 4 0 0.00 2 1 3.45 4 0 0.00 3 1 3.57 1 0 0.00 4 4 1.94 Folk Healer 1 0.75 5 0 0.00 2 0 0.00 5 0 0.00 3 0 0.00 1 0 0.00 4 1 0.49
Not Applicable 0 0.00 0 0 0.00 2 0 0.00 5 0 0.00 3 3 10.71 1 1 11.11 3 4 1.94 Total 133 100.00 4 100.00 29 100.00 3 100.00 28 100.00 9 100.00 206 100.00

95
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-23. Health Seeking Behavior by Sex, Rizal, Kalinga Province, 2001.
Female Male No Response Total Health Seeking Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
Consult Private Practitioner 20 27.78 2 2 22.22 2 0 0.00 3 22 26.19 Folk Healer 0 0.00 6 0 0.00 4 0 0.00 3 0 0.00
Barangay Health Station 5 6.94 5 0 0.00 4 1 33.33 2 6 7.14 Rural Health Unit 12 16.67 3 1 11.11 3 2 66.67 1 15 17.86
Self Medicate 8 11.11 4 3 33.33 1 0 0.00 3 11 13.10 Go to District Hospital 27 37.50 1 3 33.33 1 0 0.00 3 30 35.71
Go to Provincial Hospital 0 0.00 6 0 0.00 4 0 0.00 3 0 0.00 Herbal Medicines 0 0.00 6 0 0.00 4 0 0.00 3 0 0.00
Total 72 100.00 9 100.00 3 100.00 84 100.00
9-24. Health Seeking Behavior by Sex, Tabuk, Kalinga Province, 2001. Female Male No Response Total Health Seeking
Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Consult Private Practitioner 65 36.93 2 19 41.30 1 0 0.00 2 84 37.17
Folk Healer 4 2.27 4 4 8.70 3 0 0.00 2 8 3.54 Barangay Health Station 2 1.14 5 1 2.17 5 0 0.00 2 3 1.33
Rural Health Unit 15 8.52 3 1 2.17 5 0 0.00 2 16 7.08 Self Medicate 15 8.52 3 2 4.35 4 0 0.00 2 17 7.52
Go to District Hospital 1 0.57 6 2 4.35 4 0 0.00 2 3 1.33 Go to Provincial Hospital 73 41.48 1 16 34.78 2 4 100.00 1 93 41.15
Herbal Medicines 1 0.57 6 1 2.17 5 0 0.00 2 2 0.88 Total 176 100.00 46 100.00 4 100.00 226 100.00
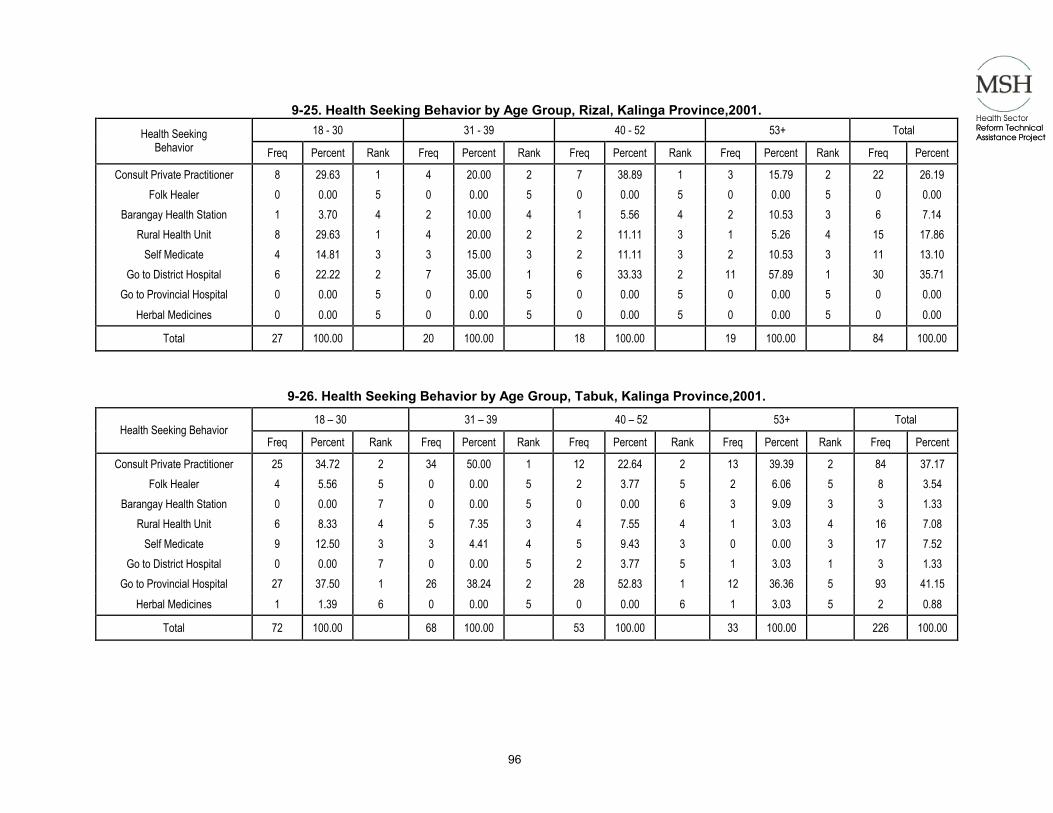
96
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-25. Health Seeking Behavior by Age Group, Rizal, Kalinga Province,2001. 18 - 30 31 - 39 40 - 52 53+ Total Health Seeking
Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Consult Private Practitioner 8 29.63 1 4 20.00 2 7 38.89 1 3 15.79 2 22 26.19
Folk Healer 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 Barangay Health Station 1 3.70 4 2 10.00 4 1 5.56 4 2 10.53 3 6 7.14
Rural Health Unit 8 29.63 1 4 20.00 2 2 11.11 3 1 5.26 4 15 17.86 Self Medicate 4 14.81 3 3 15.00 3 2 11.11 3 2 10.53 3 11 13.10
Go to District Hospital 6 22.22 2 7 35.00 1 6 33.33 2 11 57.89 1 30 35.71 Go to Provincial Hospital 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00
Herbal Medicines 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 Total 27 100.00 20 100.00 18 100.00 19 100.00 84 100.00
9-26. Health Seeking Behavior by Age Group, Tabuk, Kalinga Province,2001. 18 – 30 31 – 39 40 – 52 53+ Total
Health Seeking Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
Consult Private Practitioner 25 34.72 2 34 50.00 1 12 22.64 2 13 39.39 2 84 37.17 Folk Healer 4 5.56 5 0 0.00 5 2 3.77 5 2 6.06 5 8 3.54
Barangay Health Station 0 0.00 7 0 0.00 5 0 0.00 6 3 9.09 3 3 1.33 Rural Health Unit 6 8.33 4 5 7.35 3 4 7.55 4 1 3.03 4 16 7.08
Self Medicate 9 12.50 3 3 4.41 4 5 9.43 3 0 0.00 3 17 7.52 Go to District Hospital 0 0.00 7 0 0.00 5 2 3.77 5 1 3.03 1 3 1.33
Go to Provincial Hospital 27 37.50 1 26 38.24 2 28 52.83 1 12 36.36 5 93 41.15 Herbal Medicines 1 1.39 6 0 0.00 5 0 0.00 6 1 3.03 5 2 0.88
Total 72 100.00 68 100.00 53 100.00 33 100.00 226 100.00

97
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-27. Health Seeking Behavior by Education, Rizal, Kalinga Province, 2001.
Elementary Elementary Graduate High School High School Graduate Health Seeking Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank
Consult Private Practitioner 2 15.38 2 3 25.00 2 4 26.67 2 4 22.22 2 Folk Healer 0 0.00 4 0 0.00 4 0 0.00 5 0 0.00 5
Barangay Health Station 1 7.69 3 0 0.00 4 1 6.67 4 2 11.11 4 Rural Health Unit 1 7.69 3 2 16.67 3 2 13.33 3 7 38.89 1
Self Medicate 1 7.69 3 0 0.00 4 2 13.33 3 2 11.11 4 Go to District Hospital 8 61.54 1 7 58.33 1 6 40.00 1 3 16.67 3
Go to Provincial Hospital 0 0.00 4 0 0.00 4 0 0.00 5 0 0.00 5 Herbal Medicines 0 0.00 4 0 0.00 4 0 0.00 5 0 0.00 5
Total 13 100.00 12 100.00 15 100.00 18 100.00
College College Graduate Post graduate Vocational Graduate Health Seeking Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank
Consult Private Practitioner 4 30.77 1 5 45.45 1 0 0.00 1 0 0.00 2 Folk Healer 0 0.00 4 0 0.00 5 0 0.00 1 0 0.00 2
Barangay Health Station 0 0.00 4 1 9.09 4 0 0.00 1 1 50.00 1 Rural Health Unit 3 23.08 2 0 0.00 3 0 0.00 1 0 0.00 2
Self Medicate 4 30.77 1 2 18.18 5 0 0.00 1 0 0.00 2 Go to District Hospital 2 15.38 3 3 27.27 2 0 0.00 1 1 50.00 1
Go to Provincial Hospital 0 0.00 4 0 0.00 5 0 0.00 1 0 0.00 2 Herbal Medicines 0 0.00 4 0 0.00 5 0 0.00 1 0 0.00 2
Total 13 100.00 11 100.00 0 0.00 2 100.00

98
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Elementary Elementary Graduate High School High School Graduate Health Seeking
Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Consult Private Practitioner 11 35.48 11 8 36.36 2 11 34.38 2 12 41.38 2
Folk Healer 2 6.45 4 0 0.00 4 2 6.25 4 0 0.00 5 Barangay Health Station 0 0.00 6 0 0.00 4 1 3.13 5 0 0.00 5
Rural Health Unit 1 3.23 5 2 9.09 3 4 12.50 3 2 6.90 3 Self Medicate 4 12.90 3 0 0.00 4 2 6.25 4 0 0.00 5
Go to District Hospital 1 3.23 5 0 0.00 4 0 0.00 6 1 3.45 4 Go to Provincial Hospital 10 32.26 2 12 54.55 11 12 37.50 1 14 48.28 1
Herbal Medicines 2 6.45 4 0 0.00 4 0 0.00 6 0 0.00 5 Total 31 100.00 22 100.00 32 100.00 29 100.00
College College Graduate Post graduate Vocational Graduate Health Seeking
Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Consult Private Practitioner 10 25.00 2 27 42.86 1 4 100.00 1 0 0.00 2 1
Folk Healer 1 2.50 5 3 4.76 4 0 0.00 2 0 0.00 2 0 Barangay Health Station 0 0.00 6 2 3.17 5 0 0.00 2 0 0.00 2 0
Rural Health Unit 4 10.00 4 3 4.76 4 0 0.00 2 0 0.00 2 0 Self Medicate 6 15.00 3 4 6.35 3 0 0.00 2 0 0.00 2 1
Go to District Hospital 1 2.50 5 0 0.00 6 0 0.00 2 0 0.00 2 0 Go to Provincial Hospital 18 45.00 1 24 38.10 2 0 0.00 2 2 100.00 1 0
Herbal Medicines 0 0.00 6 0 0.00 6 0 0.00 2 0 0.00 2 0 Total 40 100.00 63 100.00 4 100.00 2 100.00 2

99
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-29. Health Seeking Behavior by Income, Rizal, Kalinga Province, 2001
< 2500 2501-5000 5001-10000 10001-20000 >20000 Total Health Seeking Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
Consult Private Practitioner 5 29.41 2 10 26.32 2 3 15.00 3 4 44.44 1 0 0.00 1 22 26.19 Folk Healer 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 4 0 0.00 1 0 0.00
Barangay Health Station 1 5.88 4 3 7.89 4 2 10.00 4 0 0.00 4 0 0.00 1 6 7.14 Rural Health Unit 6 5.88 1 5 13.16 3 3 20.00 3 1 11.11 3 0 0.00 1 15 17.86
Self Medicate 1 5.88 4 5 13.16 2 4 20.00 2 1 11.11 3 0 0.00 1 11 13.10 Go to District Hospital 4 23.53 3 15 39.47 1 8 40.00 1 3 33.33 2 0 0.00 1 30 35.71
Go to Provincial Hospital 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 4 0 0.00 1 0 0.00 Herbal Medicines 0 0.00 5 0 0.00 5 0 0.00 5 0 0.00 4 0 0.00 1 0 0.00
Total 17 100.00 38 100.00 20 100.00 9 100.00 0 0.00 84 100.00
9-30. Health Seeking Behavior by Income, Tabuk, Kalinga Province, 2001.
< 2500 2501-5000 5001-10000 10001-20000 >20000 Total Health Seeking Behavior
Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
Consult Private Practitioner 10 28.57 2 31 34.83 1 15 30.00 2 25 55.56 1 3 42.86 2 84 37.17 Folk Healer 3 8.57 3 1 1.12 4 2 4.00 5 2 4.44 4 0 0.00 3 8 3.54
Barangay Health Station 1 2.86 5 1 1.12 4 1 2.00 6 0 0.00 6 0 0.00 3 3 1.33 Rural Health Unit 2 8.57 4 10 5.62 2 3 12.00 4 1 6.67 5 0 0.00 3 16 7.08
Self Medicate 3 8.57 3 5 5.62 3 6 12.00 3 3 6.67 3 0 0.00 3 17 7.52 Go to District Hospital 1 2.86 5 0 0.00 5 1 2.00 6 1 2.22 5 0 0.00 3 3 1.33
Go to Provincial Hospital 14 40.00 1 0 0.00 5 22 44.00 1 13 28.89 2 4 57.14 1 93 41.15 Herbal Medicines 1 2.86 5 1 1.12 4 0 0.00 7 0 0.00 6 0 0.00 3 2 0.88
Total 35 100.00 89 100.00 50 100.00 45 100.00 7 100.00 226 100.00

100
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
9-31. Health Seeking Behavior by Service Satisfaction, Rizal, Kalinga Province, 2001. YES NO Sometimes Don't Know Not Applicable Total Health Seeking
Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq PercentConsult Private Practitioner 14 23.73 2 1 50.00 1 0 0.00 3 0 0.00 1 0 0.00 1 15 22.06
Folk Healer 0 0.00 6 0 0.00 2 0 0.00 3 0 0.00 1 0 0.00 1 0 0.00 Barangay Health Station 5 8.47 5 0 0.00 2 1 14.29 2 0 0.00 1 0 0.00 1 6 8.82
Rural Health Unit 11 11.86 3 1 50.00 1 2 28.57 1 0 0.00 1 0 0.00 1 14 20.59 Self Medicate 7 11.86 4 0 0.00 2 2 28.57 1 0 0.00 1 0 0.00 1 9 13.24
Go to District Hospital 22 37.29 1 0 0.00 2 2 28.57 1 0 0.00 1 0 0.00 1 24 35.29 Go to Provincial Hospital 0 0.00 6 0 0.00 2 0 0.00 3 0 0.00 1 0 0.00 1 0 0.00
Herbal Medicines 0 0.00 6 0 0.00 2 0 0.00 3 0 0.00 1 0 0.00 1 0 0.00 Total 59 100.00 2 100.00 7 100.00 0 0.00 0 0.00 68 100.00
9-32. Health Seeking Behavior by Service Satisfaction, Tabuk, Kalinga Province, 2001. YES NO Sometimes Don't Know Not Applicable Health Seeking
Behavior Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent Rank Freq Percent
Consult Private Practitioner 48 36.09 2 1 25.00 1 7 24.14 2 0 0.00 3 12 42.86 1 5 55.56 Folk Healer 5 3.76 3 0 0.00 2 0 0.00 5 0 0.00 3 1 0.00 3 1 0.00
Barangay Health Station 1 0.75 5 0 0.00 2 1 3.45 4 0 0.00 3 1 0.00 3 0 0.00 Rural Health Unit 7 9.02 4 1 25.00 1 4 3.45 3 0 33.33 3 2 0.00 2 1 0.00
Self Medicate 12 9.02 3 1 25.00 1 1 3.45 4 1 33.33 2 0 0.00 4 1 0.00 Go to District Hospital 1 0.75 5 0 0.00 2 1 3.45 4 0 0.00 3 0 0.00 4 0 0.00
Go to Provincial Hospital 57 42.86 1 1 25.00 1 15 51.72 1 2 66.67 1 12 42.86 1 1 11.11 Herbal Medicines 2 1.50 5 0 0.00 2 0 0.00 5 0 0.00 3 0 0.00 4 0 0.00
Total 133 100.00 4 100.00 29 100.00 3 100.00 28 100.00 9 100.00
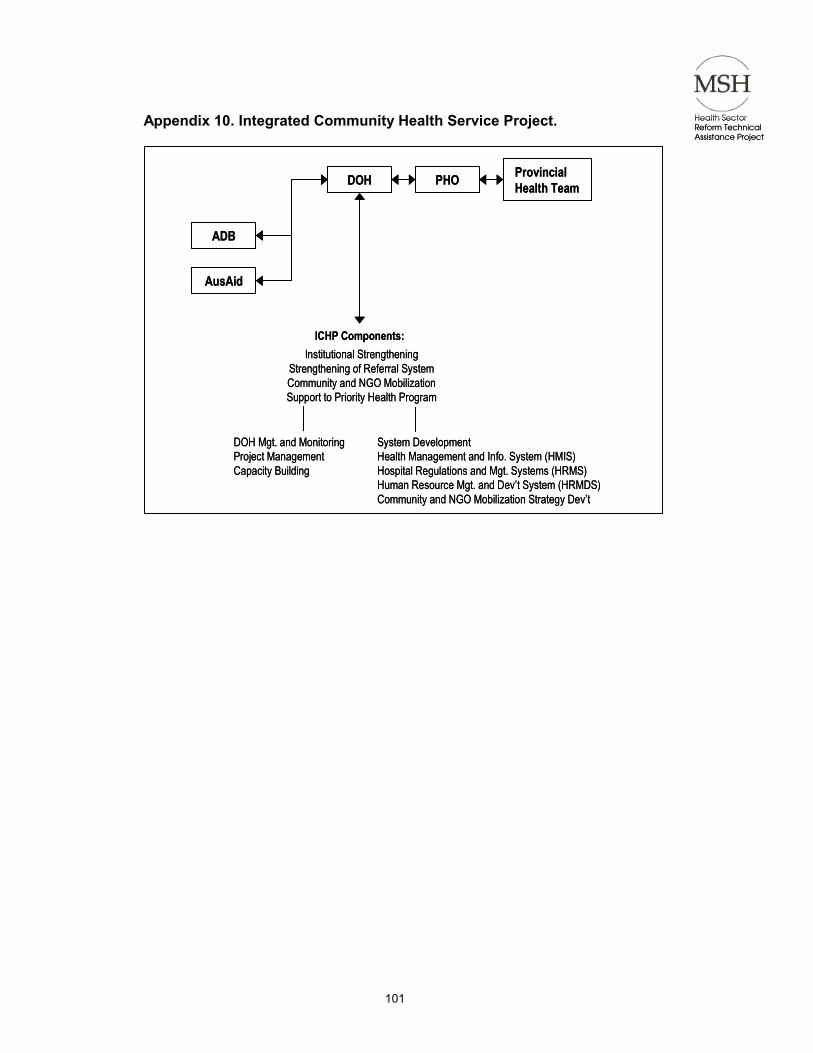
101
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
Appendix 10. Integrated Community Health Service Project.
DOH PHO Provincial Health Team
ADB
AusAid
ICHP Components:Institutional Strengthening
Strengthening of Referral SystemCommunity and NGO MobilizationSupport to Priority Health Program
DOH Mgt. and MonitoringProject ManagementCapacity Building
System DevelopmentHealth Management and Info. System (HMIS)Hospital Regulations and Mgt. Systems (HRMS)Human Resource Mgt. and Dev’t System (HRMDS)Community and NGO Mobilization Strategy Dev’t
DOH PHO Provincial Health Team
ADB
AusAid
ICHP Components:Institutional Strengthening
Strengthening of Referral SystemCommunity and NGO MobilizationSupport to Priority Health Program
DOH Mgt. and MonitoringProject ManagementCapacity Building
System DevelopmentHealth Management and Info. System (HMIS)Hospital Regulations and Mgt. Systems (HRMS)Human Resource Mgt. and Dev’t System (HRMDS)Community and NGO Mobilization Strategy Dev’t

Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
102
Appendix 11. Kalinga Milestones in IHLZ Development.
KEY STEPS IN ILHZ DEVELOPMENT
PRE-DEVOLUTION 1984-1992
DEVOLUTION 1992-1998
POST-DEVOLUTION 1999 - PRESENT
Implementation of the WHO-inspired District Health System
PREPARATORY ACTIVITIES Conceptualization of the idea
Identified factors affecting the delivery of health services: poor communication, transportation, difficult terrain, constraints of mobility and inaccessibility and high health cost in relation to low income profile of municipalities especially those belonging to 4th and 5th class The devolution has also broken the chain of integration as a result of administration and control over the health facilities and where management of hospitals are within the Provincial Government while that of the Rural Health Units and Barangay Health Stations are under the Municipal Government Conceptualization of the Balbalan Zone (1994) ICHSP Conceptualization (November 1995) Kalinga Apayao separated by RA 7878 (1995)
DOH rationalized the national health system through the drafting of the Health Sector Reform Agenda (January 2000) DOH took the initiative to conceptualize the District Health System with Inter-LGU cooperation (2000)
Developing the concept paper
Preparation for the Balbalan MOA; one hospital and one municipality model within the province of Kalinga Apayao (1993)
Finalizing proposals to provincial government, DOH, and AUSAID
Inception of the AUSAID/ ADB supported Integrated Community Health Services Project (ICHSP) (1997)
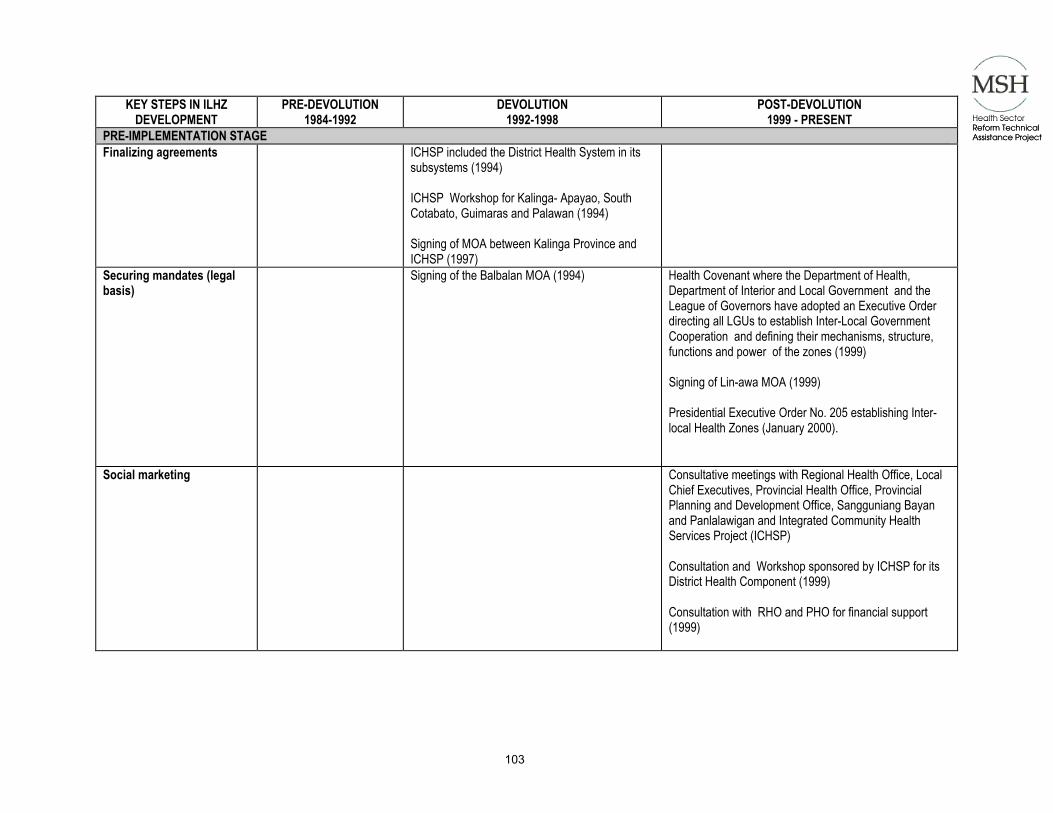
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
103
KEY STEPS IN ILHZ DEVELOPMENT
PRE-DEVOLUTION 1984-1992
DEVOLUTION 1992-1998
POST-DEVOLUTION 1999 - PRESENT
PRE-IMPLEMENTATION STAGE Finalizing agreements ICHSP included the District Health System in its
subsystems (1994) ICHSP Workshop for Kalinga- Apayao, South Cotabato, Guimaras and Palawan (1994) Signing of MOA between Kalinga Province and ICHSP (1997)
Securing mandates (legal basis)
Signing of the Balbalan MOA (1994) Health Covenant where the Department of Health, Department of Interior and Local Government and the League of Governors have adopted an Executive Order directing all LGUs to establish Inter-Local Government Cooperation and defining their mechanisms, structure, functions and power of the zones (1999) Signing of Lin-awa MOA (1999) Presidential Executive Order No. 205 establishing Inter-local Health Zones (January 2000).
Social marketing
Consultative meetings with Regional Health Office, Local Chief Executives, Provincial Health Office, Provincial Planning and Development Office, Sangguniang Bayan and Panlalawigan and Integrated Community Health Services Project (ICHSP) Consultation and Workshop sponsored by ICHSP for its District Health Component (1999) Consultation with RHO and PHO for financial support (1999)

Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
104
KEY STEPS IN ILHZ DEVELOPMENT
PRE-DEVOLUTION 1984-1992
DEVOLUTION 1992-1998
POST-DEVOLUTION 1999 - PRESENT
Planning for implementa-tion
Tour to South Cotabato and Palawan for Health Coopera-tive (1999) Conceptualization of Ambigatton Multipurpose Coopera-tive (1999)
IMPLEMENTATION STAGE Phased and province-wide dissemination of the IHS
District Health Board and Provincial Health Board Meetings; Project Activities include medical mission in Municipality of Rizal and Kalinga Provincial Hospital Advocacy and sustained implementation of MOA in spite of political instability at governor’s level
Development of financing options
Installation of support systems such as the PhilHealth Indigent Program (2001) and Ambigatton Multi-purpose Cooperative (2000) And its expansion to: (2000-2001) Bumilgan Multipurpose Cooperative Rizal Barangay Health Workers’ Multi-purpose Coopera-tive Community Based Health Insurance in Rizal (managed by BHWs; a system of “piso-piso araw- araw”)
Monitoring and evaluation of the pilot and expansion areas
Setting of Chico River (July 2000) and the Balbalan (Bumilgan) Health Zones (MOA signed in 1994)
Achievements District Health Plans Medical and Surgical Missions PhilHealth Insurance enrollment Ambigatton Multi-Purpose Cooperative and its expansions to other areas Support of ICHSP

Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
105
KEY STEPS IN ILHZ DEVELOPMENT
PRE-DEVOLUTION 1984-1992
DEVOLUTION 1992-1998
POST-DEVOLUTION 1999 - PRESENT
Sustainability Updates
As of March 2001: Reconvening the District Health Board of the Lin-awa Zone (March 3, 2001) where decisions on the interven-tions for sustainability were made. These include: Rotation of Mayors as host and chairperson Review and reemphasis on functions of the DHB Approval of a better referral tracking system and form Conceptualization of MOH to transfer funds of PHO to Tanudan Municipal Hospital and Juan M. Duyan Memorial Hospital based on Balbalan MOA Scheduled regular meetings for the DHB: 3rd Thursday of first month of each quarter where hosting of meeting is on rotation basis Preparation of operational plans every July and district health plan every September Aside from regular health budget allocation of each municipality a Trust Fund of the DHB shall be established with the following recommended contributions from each hospital and RHU: P100, 000 from each hospital per year and P100,000 from each RHU per year; core referral hospital shall contribute P200,000 per year; funds shall be used solely for projects and activities of the Lin-awa Zone as approved by the DHB

Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
106
Appendix 12. Sustainability Interventions. (Note: available in hardcopy only.)
Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
107
Appendix 13. Ambigatton Multi-purpose Cooperative. (Note: available in hardcopy only.)

Health Sector Reform Technical Assistance Project
Health Sector Reform Technical Assistance Project
108
Appendix 14. Non-Government Organization – Sinangpad. (Note: available in hardcopy only.)





























